Embed Size (px)
Citation preview

Acute ischemic stroke
thrombolysis outside
the license
Dr André
PeetersService de NeurologieCliniques Universitaires Saint-Luc / U.C.L.1200 BRUXELLES

Patient JG (♀
86
)
• Medical
history
– AHT, R/ , Emconcor
2.5 mg, Lasix
40 mg
– AF paroxystic
R/ Apocard
150 mg (refuses OAC)
– basocellular
carcinoma, surgery
D-3
• Actual
condition
– 09:30 left
hemiparesis
– 11:12 admission : NIHSS 6
• Ancillary
tests
– INR: 0.90, platelets
232.000
– MRI: exclusion ICH, occlusion R ACM, DWI/PWI mismatch

Contra-indications:
Situations
with
a high risk of haemorrhage
such
as:known
haemorrhagic
diathesis; concomitant oral
anticoagulants; manifest
or
recent severe
or
dangerous
bleeding; known
history
of or
suspectedintracranial
haemorrhage; suspected
subarachnoid
haemorrhage
or
condition
after
subarachnoid
haemorrhage
from
aneurysm; history
of CNSdamage; within
10 days
of traumatic external
heart
massage, obstetrical
delivery, recent puncture
of a non-compressible
blood-vessel; severeuncontrolled
arterial
hypertension; bacterial
endocarditis, pericarditis;
acute pancreatitis; documented
ulcerative
gastrointestinal
disease
duringthe last 3 months, oesophageal
varices, arterial
aneurysms, arterial/venous
malformations; neoplasm
with
increased
bleeding
risk; severe
liverdisease, including
hepatic
failure, cirrhosis, portal hypertension
and active
hepatitis; major surgery
or
significant trauma in past 3 months; symptomonset
more than
3 hours
or
unknown; minor neurological
deficit
or
symptoms
rapidly
improving
before
infusion
start; severe
stroke;seizure
at onset
of stroke; evidence
of ICH on
CT-scan; symptoms
of subarachnoid
haemorrhage; heparin
within
previous
48 hours
and elevated
thromboplastintime; history
of stroke
and concomitant diabetes; prior stroke
within
last 3
months; platelet
count
<100,000/mm3; systolic
blood
pressure
>185 or
diastolic>110 mmHg, or
aggressive
management necessary
to reduce
BP to these limits;
blood
glucose <50 or
>400mg/dL; for
age
18–80 years
only.

IV Thrombolysis : off-label
• Recent
(major) surgery
– relative small
or low
risk
procedure
– accessible site
– amenable
to conservative R of bleeding
complications
Stroke 2007;38:2612-2618

IV Thrombolysis : off-label
• Mild
or rapidly
improving
symptoms
– substantial
number
have poor
outcomes
– mild
symptoms
can
be
very
disabling
– observational
studies: IVT associated
with
good outcome
Stroke 2007;38:2612-2618

Patient JG (♀
86
)
• IV thrombolysis
at
12:30 (DNT: 78 min)
• Evolution
– 13:30 NIHSS 3
– Frontal hematoma
– D5 leaves
the hospital, NIHSS 0
– Outpatient
clinic
after
6 weeks
• hematoma
entirely
recovered
• R/ dabigatran
2 x 100 mg

IV Thrombolysis : off-label
• > 80 years
– Stroke 2000;31:370-375
– Neurology
2005;65:1795-1798
– J Neurol
Neurosurg
Psychiatry
2006;77:375-377
– J Neurol
Neurosurg
Psychiatry
2007;78:690-693
– Cerebrovasc
Dis. 2008;25:129-135
– Stroke 2010;41:1833-1835
– K Lees (Vista)

Stroke 2010, 41:2840-2848

IV Thrombolysis : off-label
• > 80 years
– no increased
risk
of symptomatic
intracranial
hemorrhage
– chance of favorable outcome
at
3 months
is
50 % less
– in-hospital
†
D7 : 13 % (80 plus) versus 11 % (< 80)
Derex L, Nighoghossian N. Nat Rev Neurol 2009;5:506Uyttenboogaart M et al. Age Ageing 2007;36:577

IV Thrombolysis : off-label
• Prospective studies
in > 80 years
– IST-3 (presented
at
ESC Lisbon
22-25 May 2012)
• Inclusion < 6 h
• 1617/3035 patients aged
> 80 years
– TESPI (Thrombolysis
in Elderly
Stroke Patients in Italy)

IV Thrombolysis : off-label
• > 80 years, –
with
↑
age, ↑
risk
of dementia
& microbleeds
• National Inpatient
Sample
Database
–
35.557 patients, 207 with
dementia
received
IVT–
no increased
risk
of ICH or death
• «
Add
life to years
> add
years
to life
»
Neurology 2011;76:1575–1580

Contra-indications:
Situations
with
a high risk of haemorrhage
such
as:known
haemorrhagic
diathesis; concomitant oral
anticoagulants; manifest
or
recent severe
or
dangerous
bleeding; known
history
of or
suspectedintracranial
haemorrhage; suspected
subarachnoid
haemorrhage
or
condition
after
subarachnoid
haemorrhage
from
aneurysm; history
of CNSdamage; within
10 days
of traumatic external
heart
massage, obstetrical
delivery, recent puncture
of a non-compressible
blood-vessel; severeuncontrolled
arterial
hypertension; bacterial
endocarditis, pericarditis;
acute pancreatitis; documented
ulcerative
gastrointestinal
disease
duringthe last 3 months, oesophageal
varices, arterial
aneurysms, arterial/venous
malformations; neoplasm
with
increased
bleeding
risk; severe
liverdisease, including
hepatic
failure, cirrhosis, portal hypertension
and active
hepatitis; major surgery
or
significant trauma in past 3 months; symptomonset
more than
3 hours
or
unknown; minor neurological
deficit or
symptoms
rapidly
improving
before
infusion
start; severe
stroke;seizure
at onset
of stroke; evidence
of ICH on
CT-scan; symptoms
of subarachnoid
haemorrhage; heparin
within
previous
48 hours
and elevated
thromboplastintime; history
of stroke
and concomitant diabetes; prior stroke
within
last 3
months; platelet
count
<100,000/mm3; systolic
blood
pressure
>185 or
diastolic>110 mmHg, or
aggressive
management necessary
to reduce
BP to these limits;
blood
glucose <50 or
>400mg/dL; for
age
18–80 years
only.

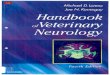
IV thrombolysis
Lancet 2004;363:768-74
> 4,5 tim> 4,5 timNNT 3
NNT 7
NNT 14
off-label !

IV Thrombolysis : off-label
• Wake-up
stroke
–
about 25% AIS awaken
with
their
deficits–
stroke onset
defined
as last-seen-normal time
–
early
morning
peak
occurrence AIS •
CT
• MRI (PRE-FLAIR)
–
retrospective
study
thrombolysis
in WUS patients •
Treated
WUS (n=46) outcome
> non-treated
WUS (n=34)
and similar
to < 3h-treated
patients
Stroke 2009;40;827-832

PRE-FLAIR
Lancet Neurol 2011; 10: 978–86

PRE-FLAIR
Lancet Neurol 2011; 10: 978–86
moderate sensitivity
(62%) but
good
specificity
(78%) in the identification
of patients
in the < 4.5 h window

«
Selecting
patients by tissue-window
rather
than
by time window
»

Contra-indications:
Situations
with
a high risk of haemorrhage
such
as:known
haemorrhagic
diathesis; concomitant oral
anticoagulants; manifest
or
recent severe
or
dangerous
bleeding; known
history
of or
suspectedintracranial
haemorrhage; suspected
subarachnoid
haemorrhage
or
condition
after
subarachnoid
haemorrhage
from
aneurysm; history
of CNSdamage; within
10 days
of traumatic external
heart
massage, obstetrical
delivery, recent puncture
of a non-compressible
blood-vessel; severeuncontrolled
arterial
hypertension; bacterial
endocarditis, pericarditis;
acute pancreatitis; documented
ulcerative
gastrointestinal
disease
duringthe last 3 months, oesophageal
varices, arterial
aneurysms, arterial/venous
malformations; neoplasm
with
increased
bleeding
risk; severe
liverdisease, including
hepatic
failure, cirrhosis, portal hypertension
and active
hepatitis; major surgery
or
significant trauma in past 3 months; symptomonset
more than
3 hours
or
unknown; minor neurological
deficit or
symptoms
rapidly
improving
before
infusion
start; severe
stroke;seizure
at onset
of stroke; evidence
of ICH on
CT-scan; symptoms
of subarachnoid
haemorrhage; heparin
within
previous
48 hours
and elevated
thromboplastintime; history
of stroke
and concomitant diabetes; prior stroke
within
last 3
months; platelet
count
<100,000/mm3; systolic
blood
pressure
>185 or
diastolic>110 mmHg, or
aggressive
management necessary
to reduce
BP to these limits;
blood
glucose <50 or
>400mg/dL; for
age
18–80 years
only.

IV Thrombolysis: BP & INR
• Usefulness
BP count before
IVT (Stroke. 2007;38:1639-1640)
– unsuspected
platelet
count 100 000 was
found
in 0.3%
• Usefulness
clotting
test < IVT
(Neurology 2009;73;1957-1962)
– Unsuspected
coagulopathy
was
found
in 0.4 %
– Coagucheck

IV Thrombolysis : off-label
• Use of oral anticoagulants
– INR < 1.7
– 7 studies
with
3631 patients -
6.6% on warfarin
• risk
of symptomatic
ICH is
increased
• no difference
in mortality
or functional
outcome
Int Stroke J 2011;6:568

Patient GD (1)
• Medical
history
– AF, R/ Sintrom, Lanoxin, Emconcor
– TIA 08/2006
– AIS 12/2006, R/ IA thrombolysis (20 mg rt-PA)
• Actual
condition
– 15:15 loss
of consciousness
– 15:35 admission : conscious, GCS 14/15, no motor
deficit
– 16:20 mydriasis
R, anarthria, hemiplegia
L, NIHSS 18
• Ancillary
tests
– INR: 2.25
– Brain
CT




Patient GD (2)
• Evolution (24 H)–
GCS 4 → 14/15, recovers
L hemiplegia
and R mydriasis
– Oculomotor
palsy
and ataxia
• Evolution (3M)–
Oculomotor
palsy, mRS
2

Contra-indications:
Situations
with
a high risk of haemorrhage
such
as:known
haemorrhagic
diathesis; concomitant oral
anticoagulants; manifest
or
recent severe
or
dangerous
bleeding; known
history
of or
suspectedintracranial
haemorrhage; suspected
subarachnoid
haemorrhage
or
condition
after
subarachnoid
haemorrhage
from
aneurysm; history
of CNSdamage; within
10 days
of traumatic external
heart
massage, obstetrical
delivery, recent puncture
of a non-compressible
blood-vessel; severeuncontrolled
arterial
hypertension; bacterial
endocarditis, pericarditis;
acute pancreatitis; documented
ulcerative
gastrointestinal
disease
duringthe last 3 months, oesophageal
varices, arterial
aneurysms, arterial/venous
malformations; neoplasm
with
increased
bleeding
risk; severe
liverdisease, including
hepatic
failure, cirrhosis, portal hypertension
and active
hepatitis; major surgery
or
significant trauma in past 3 months; symptomonset
more than
3 hours
or
unknown; minor neurological
deficit or
symptoms
rapidly
improving
before
infusion
start; severe
stroke;seizure
at onset
of stroke; evidence
of ICH on
CT-scan; symptoms
of subarachnoid
haemorrhage; heparin
within
previous
48 hours
and elevated
thromboplastintime; history
of stroke
and concomitant diabetes; prior stroke
within
last 3
months; platelet
count
<100,000/mm3; systolic
blood
pressure
>185 or
diastolic>110 mmHg, or
aggressive
management necessary
to reduce
BP to these limits;
blood
glucose <50 or
>400mg/dL; for
age
18–80 years
only.

IV Thrombolysis : off-label
• Prior stroke and diabetes
–
SITS-ISTR and VISTA (prospective)
–
29,500 patients •
5,411 (18.5%) had
DM
• 5,019 had
prior
stroke (17.1%)
• 1,141 (5.5%) had
both
–
Outcomes
from
thrombolysis
are better
than
the controls among
patients with
DM, prior
stroke, or both
Neurology 2011;77:1866–1872

IV Thrombolysis : off-label•
Early
infarct
signs
> 1/3 MCA territory
– IST-3 (presented
at
ESC Lisbon
22-25 May 2012)
JAMA. 2001;286:2830-2838

IV Thrombolysis : off-label
• Seizure
– exclusion criterion
in RCT (postictal
Todd’s
paralysis
= stroke mimic)
– however, if AIS is
confirmed, these
patients can
be
thrombolysed
Stroke 2007;38:2612-2618

IV Thrombolysis : off-label
• Cervical artery
dissection
– 180 patients (14 retrospective
series
/ 22 case reports)*
• safety
& outcome
similar
to non-CAD
– 16 ICAD / 625 IVT
• outcome
less
favorable ?**
– ↑
re-occlusion rates in tandem-occlusion
* Stroke. 2011;42:2515-2520
** Int J Stroke 2012;7:7-13

Stroke 2007;38;2270-2274

IV Thrombolysis : off-label
• Intracranial
aneurysm
(and arteriovenous malformation)
– Is this
aneurysm
an incidental
finding? (AIS not due to vasospasm)
• Yes
consider
IVT
• No consider
thrombectomy
Stroke 2007;38:2612-2618

IV Thrombolysis : off-label
• Intracranial
aneurysm
(and arteriovenous malformation)
– Brain
imaging
is
ment to exclude
ICH/SAH > to show AIS (EIS)
• subtle
SAH, cortical CVT, traumatic
lesions
(fall
due to stroke)
Stroke 2007;38:2612-2618

AJNR 2010;31:1355– 62

IV Thrombolysis : off-label
• Recent
myocardial
infarction
?
• Cardiac
thrombus ?
Stroke 2007;38:2612-2618

IVT off-label : conclusions
1. More experience
in off-label use of IVT
2. In relatively
safe
situations: informed
consent → IVT
3. In relatively
high
risk
situations: informed
consent → IAT
Acknowledgements: J De Keyser 10th Symposium BSC 12 Dec 2011