Embed Size (px)
Citation preview

06 (2007) 305–310www.elsevier.com/locate/ygyno
Gynecologic Oncology 1
UCN-01 in combination with topotecan in patients with advancedrecurrent ovarian cancer: A study of the Princess Margaret
Hospital Phase II consortium
Stephen Welch a, Hal W. Hirte b,⁎, Mark S. Carey c, Sebastian J. Hotte b, Ming-Sound Tsao a,Shirley Brown a, Gregory R. Pond a, Janet E. Dancey d, Amit M. Oza a
a Princess Margaret Hospital, Toronto, Ontario, Canada M56 2M9b Juravinski Cancer Centre, 699 Concession St., Hamilton, ON, Canada L8V 5C2
c London Regional Cancer Program, London, Ontario, Canada N6A 4L6d Cancer Therapy Evaluation Program, National Cancer Institute, Bethesda, Maryland 20852, USA
Received 31 October 2006Available online 29 May 2007
Abstract
Background and objective. UCN-01 is a staurosporine analogue shown to abrogate the G2 checkpoint through inhibition of cyclin-dependentkinases. Preclinical evidence suggests synergy between UCN-01 and cytotoxic chemotherapy. Topotecan is an active agent in ovarian cancer. Thisphase II study was conducted to investigate the safety and efficacy of topotecan and UCN-01 in patients with advanced ovarian cancer.
Methods. A two-stage phase II trial was designed for patients with advanced ovarian cancer with progressive disease despite prior treatmentwith platinum and paclitaxel. Patients with advanced ovarian cancer were treated with topotecan, 1 mg/m2 IV, days 1 to 5, and UCN-01 70 mg/m2
on day 1 of the first cycle, and 35 mg/m2 on day 1 of all subsequent cycles. Treatment was repeated on a 3-week cycle. The primary objective ofthis study was objective response rate while secondary objectives included rates of stable disease, duration of response, progression-free andoverall survival, as well as toxicity. Tumor biopsy specimens were also collected where possible for molecular correlative studies.
Results. Twenty-nine patients are evaluable for toxicity and efficacy. Three patients (10%) achieved a partial response. The median time toprogression was 3.3 months (95% CI 1.5–NA), and the median overall survival was 9.7 months (95% CI: 7.5–15.3). The most common grade 3–4toxicities were neutropenia (79%), anemia (41%), thrombocytopenia (14%), hyperglycemia (10%), and pain (10%).
Conclusion. The combination of UCN-01 and topotecan is generally well tolerated, however, this combination is not considered to havesignificant antitumor activity against advanced ovarian cancer.© 2007 Elsevier Inc. All rights reserved.
Keywords: Ovarian cancer; Topotecan; UCN-01; Cyclin-dependent kinase modulator
Introduction
Ovarian cancer is the fifth leading cause of cancer-relateddeath in North America. For all but a minority of patients withoperable ovarian cancer, post-operative combination che-motherapy with platinum and taxane has become the standardof care. Despite this intervention, the majority of patients withstage III/IV disease relapse and ultimately die from their
⁎ Corresponding author. Fax: +1 905 575 6326.E-mail address: [email protected] (H.W. Hirte).
0090-8258/$ - see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.ygyno.2007.02.018
disease. The intent of chemotherapy in these patients is topalliate symptoms and to provide control of disease.
Topotecan, an inhibitor of topoisomerase I, has shownconsiderable efficacy in advanced ovarian cancer, with responserates as high as 33%, with comparable efficacy to agents such aspaclitaxel or liposomal doxorubicin [1–3]. Topotecan exerts itscytotoxic effect by causing single- and double-stranded breaksin DNA [4]. In theory, cells damaged by the effects of topotecancould undergo cell cycle arrest and subsequent DNA repair inorder to survive.
7-Hydroxystaurosporine (UCN-01) is a staurosporine analo-gue isolated from the culture broth of Streptomyces species [5].

306 S. Welch et al. / Gynecologic Oncology 106 (2007) 305–310
UCN-01 has also been shown to inhibit the activity of cdk1 andcdk2 [6–8]. This inhibition leads to the activation of cyclinB/cdc2 and marked abrogation of the G2-phase checkpoint,promoting cells to undergo early mitosis and subsequentapoptotic death, rather than cell cycle arrest.
Preclinical models have demonstrated synergistic activity ofUCN-01 with a number of cytotoxic agents [9,10], includingtopotecan [11,12]. Several phase I studies have been conductedwith UCN-01 as a single agent, and in combination withcytotoxic chemotherapy [13–15]. Our group has conducted aphase I study of UCN-01 and topotecan [16]. The mostfrequent toxicities seen were myelosuppression, hyperglycemiaand constipation. Among the 22 response-evaluable patients inthis study, 10 patients had ovarian cancer, and of these, 1 had aconfirmed partial response and another had an unconfirmedpartial response. The recommended phase II dose level(RPTD) was expanded to obtain optimal safety information,concentrating only on patients with advanced ovarian cancer.
We have conducted a single-arm, open-label phase II studyof this novel combination in recurrent ovarian cancer patientswho have progressed despite platinum-based therapy. Inaddition to the 18 patients accrued exclusively to the phase IIstudy, we have included in this analysis the results of the 11evaluable ovarian cancer patients accrued to the expandedcohort of the phase I study.
Materials and methods
Patient eligibility
All patients had histologically confirmed ovarian epithelial cancer, primaryperitoneal carcinoma or fallopian tube cancer with measurable disease, asdefined by the Response Evaluation Criteria in Solid Tumors (RECIST).Included patients were those whose cancers had recurred or persisted despiteinitial platinum-based chemotherapy. Patients enrolled to the phase II studycould have received no more than 2 prior chemotherapy regimens, and had tohave received at least one prior regimen containing carboplatin or cisplatin.Patients were considered potentially platinum-sensitive if the platinum-freeinterval was greater than 6 months. Patients whose disease progressed whilebeing treated with platinum were considered platinum-refractory. All otherpatients were considered platinum-resistant. Prior treatment with topotecan orany other topoisomerase I inhibitor was prohibited. Eligible patients had to havecompleted any chemotherapy, radiotherapy or surgery at least 4 weeks prior tohaving given written informed consent. Other inclusion criteria included: ECOGperformance status of 0, 1 or 2 (or Karnofsky scale≥60%), life expectancy>12weeks, adequate hematologic function (leukocytes ≥3×109/l, absoluteneutrophil count ≥1.5×109/l, platelets ≥100×109/l), hepatic function (totalbilirubin≤upper limit of normal, transaminases ≤2.5×upper limit of normal),and renal function (serum creatinine≤upper limit of normal or creatinineclearance≥50 ml/min/1.73 m2). Women of childbearing potential were alsorequired to have a negative pregnancy test prior to enrolment and had to agree touse adequate contraception. Further exclusion criteria included the following:concurrent use of any other investigational agents, known brain metastases,history of allergic reactions to compounds of similar composition to UCN-01 ortopotecan, history of coronary artery disease, mediastinal radiation, orsymptomatic cardiorespiratory disease. Patients with uncontrolled intercurrentillness, such as active infection, or psychiatric illness that would likely limitcompliance with study requirements, were also excluded. As UCN-01 has beenassociated with hyperglycemia, patients with insulin-dependent diabetesmellitus were excluded. Patients with diabetes mellitus who were diet-controlledor treated with oral hypoglycemic agents were entered at the discretion of theinvestigator.
Treatment plan
UCN-01 and topotecan were administered on an outpatient basis on the firstday of every 3-week cycle. Patients received topotecan alone, daily on days 2–5.For cycle 1, UCN-01 was administered as a 3-h infusion, at a dose of 70 mg/m2.For subsequent cycles, the dose of UCN-01 was reduced to 35 mg/m2 due to itsprolonged half-life. Blood glucose was measured 24 h after UCN-01 infusion.Topotecan (Hycamptin, SmithKline Beecham) was delivered intravenously over30 min, at a dose of 1 mg/m2. On day 1 of each cycle, patients received 1 l ofintravenous saline hydration as well as prophylactic antiemetics withdexamethasone, 4 mg, and a 5-HT3 antagonist by intravenous route. On days2–5 of each cycle, patients received further prophylactic antiemetics withprochlorperazine, metoclopramide, or domperidone, according to institutionalpolicy.
Patients with stable disease continued on treatment to a maximum of 6cycles, or until disease progression, unacceptable adverse event, or patientwithdrawal from study. Patients with complete response or stable partialresponse continued for 2 further cycles after documentation of response inabsence of previously described criteria for discontinuation.
Evaluations during treatment
Pre-treatment evaluations conducted within 7 days of start of protocoltherapy included informed consent, complete history and physical examination,baseline laboratory studies (complete blood count and differential, serumchemistry, and CA-125), electrocardiogram, and pulmonary function tests.Radiologic evaluation of disease by means of computed tomography of thechest, abdomen and pelvis was also required within 4 weeks of the start ofprotocol therapy.
During treatment, patients were evaluated by a physician every cycle toassess for toxicity, graded according to the National Cancer Institute CommonToxicity Criteria for Adverse Events (CTCAE) version 3.0. Disease responsewas assessed every 2 cycles by repeated tumor imaging via computedtomography. Response to therapy was evaluated according to RECIST criteria.
Dose adjustments
Dose adjustments were made according to the worst toxicity experienced bythe patient in the previous treatment cycle. In the event of a grade 3 or 4 toxicity,UCN-01 and topotecanwere held until toxicity resolved to grade 1 or less. If therewas no such recovery after 2 weeks off therapy, patients were removed fromstudy. A 25% dose reduction of topotecan was used in subsequent cycles afterresolution of grade 3 or 4 hematologic toxicity, whereas a 50% dose reductionwas used for grade 3 or 4 non-hematologic toxicity. Due to its long half-life, thedose of UCN-01 was reduced by 50% for the second cycle for all patients. In theevent of a grade 3 or 4 non-hematologic toxicity in cycle 1, the UCN-01 dose wasreduced by 75%. In the event of grade 3 or 4 non-hematologic toxicity insubsequent cycles, UCN-01 was delivered at 50% of the previous dose. Ashyperglycemia is a known toxicity for UCN-01 and not for topotecan, the dose ofUCN-01 only was reduced in the event of grade 3 or 4 hyperglycemia.
Correlative studies of tumor biopsies
The purpose of correlative studies was to assess molecular changes in tumortissue and to correlate these changes with one another and with clinical outcome.Patients were asked to provide separate consent to have investigators collectpaired tumor biopsies, one at baseline and another just prior to the second cycleof treatment. These fresh tumor samples were snap frozen and stored forcorrelative studies.
Immunohistochemical staining was performed for the following biomarkers:p53, Ki-67, and phospho-H2AX. Strong staining for p53 was considered asurrogate marker for p53 mutation. Changes in Ki-67 were intended to reflectthe cell cycle checkpoint effect, with high levels of Ki-67 representing cellsprogressing through mitosis. Phospho-H2Ax is a marker for DNA double-stranddamage and repair, with higher levels expected after treatment with topotecan.
Tumor biopsies taken prior to and after one cycle of treatment with UCN-01were collected into 10% neutral buffered formalin, fixed overnight before being

Table 1Patient baseline demographics (n=29)
Median (range) age 55 (23–72)PS 0:1:2 10:16:3Malignancy Ovarian 22
Peritoneal neoplasm 4Female reproductive 2NeoplasmFallopian tube 1
#Prior regimens 1:2:3:4 15:12:1:1Prior therapy Adjuvant CT 9
Systemic CT 25RT 4
Platinum-free interval, months (n=28) Median (range) 3.2 (0.7–23.7)Classification of relapse (n=28) Platinum-sensitive 5 (17.9%)
Platinum-resistant 11 (39.3%)Platinum-refractory 12 (42.9%)
307S. Welch et al. / Gynecologic Oncology 106 (2007) 305–310
transferred to 70% ethanol and shipped for processing into paraffin blocks.Sections of 4-μm thickness were cut onto Surgipath x-tra slides. Sections weredewaxed in xylene and rehydrated through graded alcohol. Antigen retrieval wasperformed in a Milestone T/T Mega microwave oven for 10 min at 120 °C in10 mM citrate buffer, pH 6.0. After cooling, endogenous peroxidase and biotinactivities were blocked respectively using 3% hydrogen peroxide and biotinblocking kit (Vector Laboratories). For detection of p53 and pH2Ax, slides wereincubated at room temperature overnight with antibody (p53: Pab1801, VectorLaboratories; pH2Ax: JBW301, Upstate) in a moist chamber. For detection ofKi-67, slides were incubated for 1 h with antibody (MIB-1, Dako Cytomation) atroom temperature in a moist chamber. For all assays, this was followed withbiotinylated linking reagent (ID Labs Inc.) and HRP-conjugated ultrastreptavidin labeling reagent (ID Labs Inc.) for 30 min each. Color developmentwas done with freshly prepared NovaRed solution (Vector Laboratories) andcounterstained with Mayer's hematoxylin. Finally, sections were dehydratedthrough graded alcohols, cleared in xylene, and mounted in Permount (FisherScientific).
For each tumor biopsy, selected targeted areas of expression were evaluated.Areas were subjectively contoured and staining intensity was graded by onepathologist (M.-S.T.). For H2Ax and Ki-67, cells were graded as negative (0),weak positive (1+), positive (2+), or strongly positive (3+). The proportion ofcells at least positive (2+/3+) was assessed and correlated with outcome. Forp53, samples were graded as either 3+ or negative for p53 expression.
Statistical considerations
The primary objective of this study was to determine the objective responserate by RECIST criteria. Secondary objectives included rates of stable disease,duration of response, progression-free and overall survival, as well as toxicity.The protocol was devised in two stages with a two-stage maximum of 33patients in order to distinguish a meaningful response rate of 35% from a nullrate of 15% with α=0.10 and β=0.10 using the optimal design of Simon [17]. If4 or more objective responses were observed among the first 19 evaluablepatients in stage I, the trial would have continued to stage II to accrue a further14 evaluable patients. The regimen would be considered for further evaluation if8 or more objective responses were observed among the total of 33 evaluablepatients on trial.
Descriptive statistics were used to summarize patient characteristics,outcomes and adverse events. The Kaplan–Meier method was used to estimatesurvival and time to progression outcomes. Survival was defined from the datea patient first received treatment to the date of death, or last follow-up date thepatient was confirmed to be alive. Time to progression (TTP) was defined fromthe date a patient first received treatment to the first observed date of objectiveor clinical progression. Patients who withdrew or completed the 6 cycles oftreatment as per protocol were censored on the date they came off-study for theTTP analysis. CA-125 response was defined as an on-treatment CA-125measurement ≥50% smaller than the baseline CA-125 measurement. 95%Confidence intervals (CI) were constructed using exact methods wherepossible.
For correlative studies, the difference from pre-treatment to post-treatmentwas calculated for each value and a Wilcoxon rank-sum test was used to testwhether the marker expression changed significantly due to treatment.Spearman correlation coefficients were used to determine a relationship betweenchange in biomarker expression and time to progression, objective tumorresponse and overall survival. Association between baseline p53 and objectiveresponse, time to progression and overall survival was investigated usingWilcoxon rank-sum test.
Results
Patient characteristics
Twenty-nine patients were evaluable for this study, including11 patients with advanced ovarian carcinoma, treated at theRPTD in the expansion cohort of our phase I trial [16]. All 29patients were treated with the same dose and schedule of UCN-
01 and topotecan. Patients were enrolled between April 2003and October 2004 at 3 cancer centers in Canada. Table 1describes the patient characteristics at study entry. The medianage was 55 years (range: 23–72) and 90% were rated as EasternCooperative Oncology Group performance status 0 or 1. Allpatients had received prior chemotherapy. Two of the 29patients, both of which were in the expansion cohort of thephase I trial, had received more than 2 prior chemotherapyregimens.
Treatment duration
A total of 139 cycles of treatment were given to the 29patients (median 4, range: 1–13). Ten patients completed atleast 6 cycles of treatment, including one patient who completed13 cycles and another who completed 11 cycles. Reasons fordiscontinuation of treatment included: disease progression (17),completion of mandated six cycles (10), withdrawal of consent(1) and complicating disease (1).
Toxicities
Treatment with UCN-01 and topotecan was generallytolerated well and there were no treatment-related deaths. Allgrade 3 or 4 adverse events, regardless of attribution, occurringin at least 3 patients are listed in Table 2. Grade 3 or 4 toxicitiesdeemed at least possibly related to study treatment wereprimarily hematologic, including neutropenia, leucopenia,anemia, thrombocytopenia, febrile neutropenia, and lymphope-nia. The most common non-hematologic grade 3+ treatment-related toxicity was hyperglycemia.
Efficacy
Twenty-six of the 29 patients were evaluable for objectiveresponse by RECIST criteria. One patient was found, uponindependent review, to not have measurable disease at baseline.This patient is considered evaluable for toxicity, but inevaluablefor response, follow-up or survival. A second patient withdrewconsent prior to their first imaging follow-up. A third patient
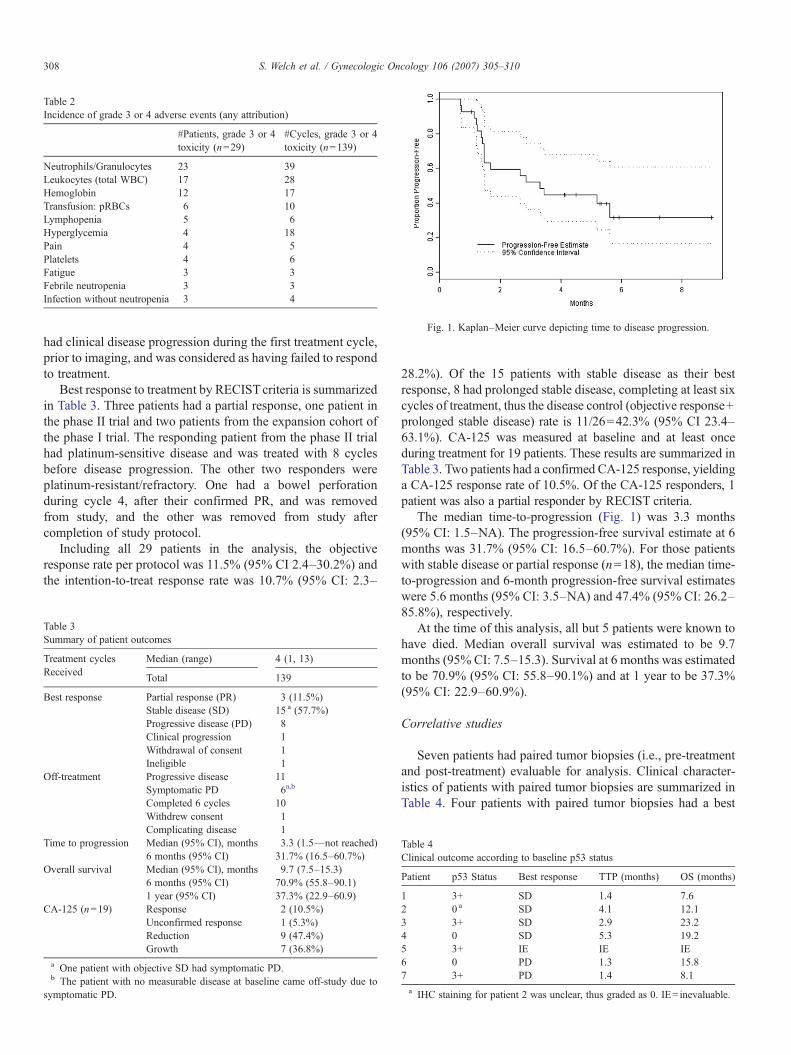
Fig. 1. Kaplan–Meier curve depicting time to disease progression.
Table 2Incidence of grade 3 or 4 adverse events (any attribution)
#Patients, grade 3 or 4toxicity (n=29)
#Cycles, grade 3 or 4toxicity (n=139)
Neutrophils/Granulocytes 23 39Leukocytes (total WBC) 17 28Hemoglobin 12 17Transfusion: pRBCs 6 10Lymphopenia 5 6Hyperglycemia 4 18Pain 4 5Platelets 4 6Fatigue 3 3Febrile neutropenia 3 3Infection without neutropenia 3 4
308 S. Welch et al. / Gynecologic Oncology 106 (2007) 305–310
had clinical disease progression during the first treatment cycle,prior to imaging, and was considered as having failed to respondto treatment.
Best response to treatment by RECISTcriteria is summarizedin Table 3. Three patients had a partial response, one patient inthe phase II trial and two patients from the expansion cohort ofthe phase I trial. The responding patient from the phase II trialhad platinum-sensitive disease and was treated with 8 cyclesbefore disease progression. The other two responders wereplatinum-resistant/refractory. One had a bowel perforationduring cycle 4, after their confirmed PR, and was removedfrom study, and the other was removed from study aftercompletion of study protocol.
Including all 29 patients in the analysis, the objectiveresponse rate per protocol was 11.5% (95% CI 2.4–30.2%) andthe intention-to-treat response rate was 10.7% (95% CI: 2.3–
Table 3Summary of patient outcomes
Treatment cyclesReceived
Median (range) 4 (1, 13)
Total 139
Best response Partial response (PR) 3 (11.5%)Stable disease (SD) 15 a (57.7%)Progressive disease (PD) 8Clinical progression 1Withdrawal of consent 1Ineligible 1
Off-treatment Progressive disease 11Symptomatic PD 6a,b
Completed 6 cycles 10Withdrew consent 1Complicating disease 1
Time to progression Median (95% CI), months 3.3 (1.5—not reached)6 months (95% CI) 31.7% (16.5–60.7%)
Overall survival Median (95% CI), months 9.7 (7.5–15.3)6 months (95% CI) 70.9% (55.8–90.1)1 year (95% CI) 37.3% (22.9–60.9)
CA-125 (n=19) Response 2 (10.5%)Unconfirmed response 1 (5.3%)Reduction 9 (47.4%)Growth 7 (36.8%)
a One patient with objective SD had symptomatic PD.b The patient with no measurable disease at baseline came off-study due to
symptomatic PD.
28.2%). Of the 15 patients with stable disease as their bestresponse, 8 had prolonged stable disease, completing at least sixcycles of treatment, thus the disease control (objective response+prolonged stable disease) rate is 11/26=42.3% (95% CI 23.4–63.1%). CA-125 was measured at baseline and at least onceduring treatment for 19 patients. These results are summarized inTable 3. Two patients had a confirmed CA-125 response, yieldinga CA-125 response rate of 10.5%. Of the CA-125 responders, 1patient was also a partial responder by RECIST criteria.
The median time-to-progression (Fig. 1) was 3.3 months(95% CI: 1.5–NA). The progression-free survival estimate at 6months was 31.7% (95% CI: 16.5–60.7%). For those patientswith stable disease or partial response (n=18), the median time-to-progression and 6-month progression-free survival estimateswere 5.6 months (95% CI: 3.5–NA) and 47.4% (95% CI: 26.2–85.8%), respectively.
At the time of this analysis, all but 5 patients were known tohave died. Median overall survival was estimated to be 9.7months (95% CI: 7.5–15.3). Survival at 6 months was estimatedto be 70.9% (95% CI: 55.8–90.1%) and at 1 year to be 37.3%(95% CI: 22.9–60.9%).
Correlative studies
Seven patients had paired tumor biopsies (i.e., pre-treatmentand post-treatment) evaluable for analysis. Clinical character-istics of patients with paired tumor biopsies are summarized inTable 4. Four patients with paired tumor biopsies had a best
Table 4Clinical outcome according to baseline p53 status
Patient p53 Status Best response TTP (months) OS (months)
1 3+ SD 1.4 7.62 0 a SD 4.1 12.13 3+ SD 2.9 23.24 0 SD 5.3 19.25 3+ IE IE IE6 0 PD 1.3 15.87 3+ PD 1.4 8.1a IHC staining for patient 2 was unclear, thus graded as 0. IE= inevaluable.

309S. Welch et al. / Gynecologic Oncology 106 (2007) 305–310
objective response of stable disease, 2 patients had a bestobjective response of progressive disease, and 1 patient wasinevaluable due to lack of measurable disease at baseline. Noassociation was observed between p53 and response, time-to-progression, or overall survival. In addition, neither change inphospho-H2Ax nor Ki-67 was found to be a statisticallysignificant predictor of response, time-to-progression, or overallsurvival in this study (data not shown).
Discussion
In patients with advanced ovarian cancer who haveprogressed after platinum-based chemotherapy, topotecan isone of a number of options for palliative chemotherapy. Agentsused in this setting have only modest activity. Several dosingschedules of topotecan have been advocated. The schedule ofdaily topotecan for 5 consecutive days was chosen for this studyas it has been suggested to be less myelotoxic and moretolerable than other schedules in a randomized study [18]. Thedose of 1 mg/m2 was the recommended phase II dose from thepreviously described phase I trial [16].
There is good theoretical rationale for combining cell cycleactive compounds, such as UCN-01 or flavopiridol, withcytotoxic chemotherapies with cell cycle phase specificity.Topotecan inhibits topoisomerase I and has selective toxicity forcells in S phase [4]. Since UCN-01 has shown markedabrogation of the G2 checkpoint, it is reasonable to combineUCN-01 with topotecan in order to prevent cells fromundergoing cell cycle arrest and potential DNA repair afterexposure to topotecan. Cells would then be prompted toundergo mitotic catastrophe or apoptosis. Synergy betweenUCN-01 and chemotherapy has been shown in vitro. Increasedcytotoxicity is seen in cells containing mutant p53 genes inmany, but not all, reports. Phase I clinical trials have previouslydemonstrated the feasibility and tolerability of UCN-01, assingle agent and in combination with chemotherapy. UCN-01has an unexpectedly long and variable half-life [13,16].
In terms of toxicity, the observed incidence of severehematologic toxicity is not out of keeping with prior trials oftopotecan in this patient population. UCN-01 has not beenassociated with significant myelosuppression when used as asingle agent [13]. There were 3 patients on this study withfebrile neutropenia (grade 3) and there were no toxic deaths.Hyperglycemia is a known toxicity of UCN-01; for this reason,patients with diabetes mellitus requiring insulin were excluded.Hyperglycemia was easily manageable in this study. Theetiology of UCN-01-induced hyperglycemia is unclear, butinhibition of AKT and downstream insulin-receptor pathwaysare the most probable causes [19].
A standard two-stage phase II clinical trial was employed inthis clinical trial. In this patient population, a response rate ofapproximately 10–15% would be expected with topotecanalone. With only 1 responder among 19 evaluable patients in thefirst stage of the phase II protocol, it was unlikely that asignificant improvement in the primary endpoint, response rate,would have been shown if accrual were to continue to include33 patients on study. Thus, the study was stopped after stage I
and this combination has been deemed insufficiently active inthis patient population.
Despite encouraging preclinical observations, our resultsindicate that the addition of UCN-01 to topotecan does notenhance activity over topotecan alone in ovarian cancer. A trialof UCN-01 in combination with topotecan is ongoing in smallcell lung cancer, and the results of these trials are awaited.UCN-01 treatment in ovarian cancer cell lines results in thereversal of cisplatin resistance [10]. Phase I studies haveconfirmed the tolerability of UCN-01 and cisplatin [15], thusthis combination may be a viable option for future study inovarian cancer.
It is plausible that the scheduling of UCN-01 with topotecannegated any possible synergy. Sequential treatment of atopoisomerase inhibitor followed by UCN-01 results inincreased cytotoxicity by apoptosis assay as compared toconcurrent treatment in a colon carcinoma model [11].Flavopiridol, another cell cycle active drug that inhibitscyclin-dependent kinases, has undergone phase I study,administered sequentially after irinotecan with promisingantitumor effect [20]. Future investigators exploring thecombination of UCN-01 and cytotoxic chemotherapy mayconsider sequential treatment to test this hypothesis. However,the unusually long half-life of UCN-01 [13,16] is likely toobscure any potential benefit to sequence specificity in all butthe first cycle of treatment [15].
It has been suggested that tumor cells defective in p53function rely on cell cycle arrest in G2 phase for protection aftercamptothecin-induced DNA damage, whereas tumor cells withpreserved p53 function arrest are protected from such damageby arrest in G0/G1 phase. Since UCN-01 abrogates the G2-phase checkpoint, UCN-01 added to a camptothecin analoguewould be expected to be more effective in cells with mutant p53.Conversely, flavopiridol, a novel inhibitor of cyclin-dependentkinases, in combination with irinotecan, appears to be moreactive in patients with wild-type p53 than those with mutant p53[20]. A strategy of selecting either UCN-01 or flavopiridol tocombine with cytotoxic chemotherapy, depending on p53status, is an appealing one [21], but would require furtherconfirmatory evidence in prospective clinical trials. The notionof a preferential anti-cancer effect of UCN-01 in combinationwith chemotherapy depending on p53 function is supported bysome [12,22] but not all preclinical studies [23,24]. Sequentialtreatment of colon cancer cell lines with UCN-01 and SN-38, atopoisomerase I inhibitor, markedly enhances cytotoxicity, inpart by induction of apoptosis, in mutant p53 cells, but not wildtype. On the other hand, concurrent treatment with UCN-01 andSN-38 results in amplified DNA damage response andaugmentation of clonogneic inhibition that is independent ofp53 status [11].
The limited results of our study in 7 patients do not supportp53 status as a predictive marker for concurrent treatment ofovarian cancer with UCN-01 and topotecan, as we observed nocorrelation between p53 status and outcome (Table 4). Inter-pretation of these results should be made with caution, as thenumber of biopsy samples was small and there were no objectiveresponses in patients from whom the samples were collected.

310 S. Welch et al. / Gynecologic Oncology 106 (2007) 305–310
In summary, the combination of topotecan with UCN-01 wastolerated reasonably well in a cohort of advanced ovariancancer, but did not appear to have sufficient antitumor activityin this patient population to warrant further study.
Acknowledgments
This study has been supported by a clinical trials contractfrom the US National Cancer Institute, #N01-CM-1701.
This study was previously presented in part at the 2003AACR meeting in Washington, DC, the 2003 NCI-AACR-EORTCmeeting in Boston, Massachusetts, and the 2005 ASCOmeeting in Orlando, Florida.
References
[1] Creemers GJ, Bolis G, Gore M, Scarfone G, Lacave AJ, Guastalla JP, et al.Topotecan, an active drug in the second-line treatment of epithelial ovariancancer: results of a large European phase II study. J Clin Oncol 1996;14:3056–61.
[2] Gordon AN, Fleagle JT, Guthrie D, Parkin DE, Gore ME, Lacave AJ.Recurrent epithelial ovarian carcinoma: a randomized phase III study ofpegylated liposomal doxorubicin versus topotecan. J Clin Oncol 2001;19:3312–22.
[3] ten Bokkel Huinink W, Gore M, Carmichael J, Gordon A, Malfetano J,Hudson I, et al. Topotecan versus paclitaxel for the treatment of recurrentepithelial ovarian cancer. J Clin Oncol 1997;15:2183–93.
[4] Del Bino G, Lassota P, Darzynkiewicz Z. The S-phase cytotoxicity ofcamptothecin. Exp Cell Res 1991;193:27–35.
[5] Takahashi I, Saitoh Y, Yoshida M, Sano H, Nakano H, Morimoto M, et al.UCN-01 and UCN-02, new selective inhibitors of protein kinase C: II.Purification, physico-chemical properties, structural determination andbiological activities. J Antibiot (Tokyo) 1989;42:571–6.
[6] Akinaga S, Nomura K, Gomi K, Okabe M. Effect of UCN-01, a selectiveinhibitor of protein kinase C, on the cell-cycle distribution of humanepidermoid carcinoma, A431 cells. Cancer Chemother Pharmacol 1994;33:273–80.
[7] Graves PR, Yu L, Schwarz JK, Gales J, Sausville EA, O'Connor PM, et al.The Chk1 protein kinase and the Cdc25C regulatory pathways are targetsof the anticancer agent UCN-01. J Biol Chem 2000;275:5600–5.
[8] Busby EC, Leistritz DF, Abraham RT, Karnitz LM, Sarkaria JN. Theradiosensitizing agent 7-hydroxystaurosporine (UCN-01) inhibits theDNA damage checkpoint kinase hChk1. Cancer Res 2000;60:2108–12.
[9] Husain A, Yan XJ, Rosales N, Aghajanian C, Schwartz GK, Spriggs DR.UCN-01 in ovary cancer cells: effective as a single agent and in com-bination with cis-diamminedichloroplatinum(II)independent of p53 status.Clin Cancer Res 1997;3:2089–97.
[10] Monks A, Harris ED, Vaigro-Wolff A, Hose CD, Connelly JW, SausvilleEA. UCN-01 enhances the in vitro toxicity of clinical agents in humantumor cell lines. Invest New Drugs 2000;18:95–107.
[11] Tse AN, Schwartz GK. Potentiation of cytotoxicity of topoisomerase ipoison by concurrent and sequential treatment with the checkpointinhibitor UCN-01 involves disparate mechanisms resulting in either p53-independent clonogenic suppression or p53-dependent mitotic catastrophe.Cancer Res 2004;64:6635–44.
[12] Shao RG, Cao CX, Shimizu T, O'Connor PM, Kohn KW, Pommier Y.Abrogation of an S-phase checkpoint and potentiation of camptothecincytotoxicity by 7-hydroxystaurosporine (UCN-01) in human cancer celllines, possibly influenced by p53 function. Cancer Res 1997;57:4029–35.
[13] Dees EC, Baker SD, O'Reilly S, Rudek MA, Davidson SB, AylesworthC, et al. A phase I and pharmacokinetic study of short infusions of UCN-01 in patients with refractory solid tumors. Clin Cancer Res 2005;11:664–71.
[14] Kortmansky J, Shah MA, Kaubisch A, Weyerbacher A, Yi S, Tong W,et al. Phase I trial of the cyclin-dependent kinase inhibitor and proteinkinase C inhibitor 7-hydroxystaurosporine in combination with Fluor-ouracil in patients with advanced solid tumors. J Clin Oncol 2005;23:1875–84.
[15] Lara Jr PN, Mack PC, Synold T, Frankel P, Longmate J, Gumerlock P, et al.The cyclin-dependent kinase inhibitor UCN-01 plus cisplatin in advancedsolid tumors: a California cancer consortium phase I pharmacokinetic andmolecular correlative trial. Clin Cancer Res 2005;11:4444–50.
[16] Hotte SJ, Oza A, Winquist EW, Moore M, Chen EX, Brown S, et al. PhaseI trial of UCN-01 in combination with topotecan in patients with advancedsolid cancers: a Princess Margaret Hospital Phase II Consortium study.Ann Oncol 2006;17:334–40.
[17] Simon R. Optimal two-stage designs for phase II clinical trials. ControlClin Trials 1989;10:1–10.
[18] Hoskins P, Eisenhauer E, Beare S, Roy M, Drouin P, Stuart G, et al.Randomized phase II study of two schedules of topotecan in previouslytreated patients with ovarian cancer: a National Cancer Institute of CanadaClinical Trials Group study. J Clin Oncol 1998;16:2233–7.
[19] Kondapaka SB, Zarnowski M, Yver DR, Sausville EA, Cushman SW. 7-Hydroxystaurosporine (UCN-01) inhibition of Akt Thr308 but not Ser473phosphorylation: a basis for decreased insulin-stimulated glucose trans-port. Clin Cancer Res 2004;10:7192–8.
[20] Shah MA, Kortmansky J, Motwani M, Drobnjak M, Gonen M, Yi S, et al.A phase I clinical trial of the sequential combination of irinotecan followedby flavopiridol. Clin Cancer Res 2005;11:3836–45.
[21] Schwartz GK. Development of cell cycle active drugs for the treatment ofgastrointestinal cancers: a new approach to cancer therapy. J Clin Oncol2005;23:4499–508.
[22] Wang Q, Fan S, Eastman A, Worland PJ, Sausville EA, O'Connor PM.UCN-01: a potent abrogator of G2 checkpoint function in cancer cells withdisrupted p53. J Natl Cancer Inst 1996;88:956–65.
[23] Yu Q, La Rose J, Zhang H, Takemura H, Kohn KW, Pommier Y. UCN-01inhibits p53 up-regulation and abrogates gamma-radiation-induced G(2)-M checkpoint independently of p53 by targeting both of the checkpointkinases, Chk2 and Chk1. Cancer Res 2002;62:5743–8.
[24] Hirose Y, Berger MS, Pieper RO. Abrogation of the Chk1-mediated G2checkpoint pathway potentiates temozolomide-induced toxicity in a p53-independent manner in human glioblastoma cells. Cancer Res 2001;61:5843–9.