Embed Size (px)
Citation preview

included studies that compare the diagnostic accuracy of cystic fluid CEAwith the histologicaldiagnosis. We requested further information from the authors if any clarification was needed.Pooled estimates of sensitivity, specificity, likelihood ratio (LR) and diagnostic odds ratio(DOR) were calculated using random-effects models. Summary receiver-operating character-istic (sROC) curves were used to analyze the diagnostic accuracy of cystic fluid CEA indistinguishing benign and malignant pancreatic cysts. Results: Of 842 articles, 8 studies (n=504) met the inclusion criteria. The cut-off for determining malignant cyst ranged from109.9 - 6,000 ng/ml among various studies. The pooled estimates of intracystic CEA levelin prediction of malignant pancreatic cysts were poor, with a pooled sensitivity of 63%(95% CI, 55-69), pooled specificity of 63% (95% CI, 57-68). The positive LR was 1.89(95% CI, 1.13-3.16) and the negative LR was 0.62 (95% CI, 0.40-0.97). The DOR was 3.84(95% CI, 1.37-10.74). Heterogeneity was observed (I2 = 76%, p , 0.0001). The area underthe sROC curve was 0.70 with an SE of 0.09. The maximum joint sensitivity and specificity(Q* value) was 0.66 with an SE of 0.07. In subgroup analysis of patients with mucinouscysts (mucinous cystic neoplasm and IPMN) (5 studies, 227 patients), the pooled sensitivityof intracystic CEA level in prediction of malignant pancreatic cysts was 65% (95% CI, 57-73), with the pooled specificity of 66% (95% CI, 59-72) and DOR of 4.74 (95% CI, 1.46-15.37). Conclusion: This meta-analysis suggested that the accuracy of intracystic CEA levelin differentiating benign and malignant pancreatic cysts was poor. The decision to performsurgical resection for pancreatic cystic lesions including IPMN should not be based solelyon a very high intracystic CEA level.
Tu1226
In Vivo Characterization of Pancreatic Serous Cystadenomas by Needle-BasedConfocal Laser Endomicroscopy (nCLE). Intra and Inter Observer Agreement -Contact StudyBertrand Napoleon, Bertrand Pujol, Anne-Isabelle Lemaistre, Fabrice Caillol, DamienLucidarme, Bernard Filoche, Blandine Mialhe-Morellon, Fabien Fumex, Vincent Lepilliez,Marc Giovannini
Introduction: nCLE enables microscopic observation of solid organs, in vivo and in real-time, during an EUSFNA procedure. A prospective multicentric french study (CONTACT)aims at assessing the diagnostic performance of nCLE for the diagnosis of pancreatic cysts.The chosen interpretation criteria have been defined during a previous study (INSPECT),but the definition of complementary criteria was considered after the inclusion of the first10 patients. 2 investigators and 2 pathologists reviewed the 10 recordings and identified anew aspect: the superficial vascular networking (SVN). It matches the serous cystadenoma(SCA) histology. The aim of this preliminary study is to validate this criteria by assessingits diagnostic performance for the diagnosis of SCA, as well as the inter (IOA) and intraobserver agreements. Materials and methods:Over 6 months, 18 patients without chronicpancreatitis and with a lonely pancreatic cyst . 2cm large were enrolled. Following EUSexamination, the nCLE miniprobe was introduced in a 19G needle and real-time videosequences of the cyst wall were recorded.Fluid obtained by FNAwas analyzed. Final diagnosisof SCA (n=8) was based on the following characteristics: -transsonor fluid, absence of nodule,parietal vegetations or solid tumor on EUS, -absence of cytologic criteria suggesting amucinous lesion +/- SCA cells, -intracystic tumoral marker CEA , 5.The other lesions wereconsidered as mucinous cystadenoma (n=5,proven by surgery),IPMN (n=3),pseudocysts (n=2). IOA was evaluated by 6 investigators (4 experts,2 beginners) who reviewed a set of 18video sequences (8 SCA and 10 non SCA) in a randomized order after a basic training onimage interpretation (2 cases, one with SVN). The intraobserver agreement was evaluated,in parallel, by 1 beginner and 1 expert who reviewed twice the same set in a different order.Following this evaluation, a joint review was done for cases for which a discrepancy ofinterpretation was observed. A final consensus for the diagnosis was proposed if possible.Results:The intraobserver agreement was excellent and identical for the beginner and theexpert (κ 0.87).The IOA was good to excellent ( κ 0.69). In 72% of cases the agreementbetween the 6 observers was complete.A final consensus was obtained in the 28% remainingcases.Compared to the final diagnosis, the accurracy, sensitivity, specificity, PPV and NPVfor the diagnosis of SCA by nCLE were respectively 83%, 62.5%, 100%, 100% and 77%.Conclusion: The presence of SVN is a histological particularity of SCA, which can behighlighted by nCLE. The specificity and PPV of the sign is 100% in this preliminary series.Its presence could avoid unnecessary surgery for SCA. The second phase of the study shouldenable to validate prospectively this sign and confirm the interest of nCLE for the diagnosisof pancreatic cystic tumors.
Tu1227
Long-Term Follow up of Branch Duct Intraductal Papillary MucinousNeoplasms of the Pancreas: A Single Center ExperienceManabu Osanai, Hiroyuki Maguchi, Kei Yane, Toshifumi Kin, Ryo Takaki, KazuyukiMatsumoto, Tomoaki Matsumori, Katsushige Gon, Akio Katanuma, Kuniyuki Takahashi
BACKGROUND& AIMS; In the IPMN/MCN international consensus guidelines, branch ductIPMN (BD-IPMN) have changed from rather early resection to more deliberate observation.However, long term follow-up result of BD-IPMN has been limited, the aim of this studywas to clarify the natural history of BD-IPMN. METHODS; 582 patients with BD-IPMNswere treated in our institute from 1997 to 2012. 116 patients with BD-IPMNs with morethan 5 years imaging follow-up were identified and their cases reviewed. Evaluation pointswere 1) initial clinical data, 2) progression rate, 3) incidence of ordinary pancreatic cancer,and 4) outcomes. RESULTS; 1)Mean observation period was 90 months (61 to 185 months)(M:F=41:75; median age, 66y). The initial mean size of the cystic lesion is 19.9mm (10~45),diameter of the main pancreatic duct (MPD) is 3.0mm (2~10). 97 patients (86%) had nomural nodules, while 19 patients initially had mural nodules (1~9mm, mean 3.5mm). 2)Twenty-one patients (18.1%) exhibited progression with an increasing cyst size, MPD diame-ter, or appearance and/or enlargement of mural nodules. Surgical resection was performedin 7 (33.3%) of 21 patients with progression and 5 (5.3%) of 95 patients without changes.Pathological diagnosis; with progression group was 5 adenoma, 1 carcinoma in situ, and 1invasive IPMC, without progression group was 4 adenoma and 1 minimally invasive IPMC.3) Two patients died of extrapancreatic malignancies, 2 patients died of newly developed
S-797 AGA Abstracts
ductal carcinoma of the pancreas, and 3 patients died of other benign diseases. Thus, nopatients died of IPMN itself during the follow-up period. CONCLUSION; Of 116 BD-IPMNs,morphological change was observed in 18.1% during the mean follow-up period of 90months and no patients died of IPMN itself. This suggests that observation may be areasonable approach to BD-IPMNs until morphological changes.
Tu1228
High Prevalence of Cystic Pancreatic Lesions in Patients With Advanced LiverDiseaseSeth N. Sclair, Emmanuel Coronel, Simon Abramson, David Jativa, Victor J. Casillas, PaulMartin, Beatrice L. Madrazo
Background: Routine abdominal imaging frequently uncovers unsuspected masses. Recentstudies report a prevalence of incidentally detected pancreatic cystic lesions (PCL) in thegeneral population of 2.4% to 2.6% (De Jong 2010, Laffan 2008). We have observedincreasing numbers of PCL in cirrhotic patients receiving routine abdominal imaging forhepatocellular carcinoma surveillance. The aim of this study is to establish PCL prevalencein patients with advanced liver disease. Methods: This was a cross-sectional study comparingthree groups of cirrhotic patients: 1) "Clinic" (hepatology clinic patients, 2010-11), 2) "MRI"(consecutive patients with cirrhosis and abdominal MRI, 2009-11), and 3) "Transplant"(liver transplant recipients, 2010-11). Patients with cirrhosis and CT and MR imaging studieswere included. For liver-transplanted patients, only pre-transplant images were considered.Key exclusions were age ,18y, history of pancreatitis, and polycystic liver and/or kidneydisease. One imaging study per eligible patient was blindly reviewed by a team of radiologists.We calculated PCL prevalence in each group and also correlated PCL prevalence with Modelof End Stage Liver Disease (MELD) score and etiology of liver disease. Statistical analysiswas performed using 3x2 Chi-square, Fisher exact, and Mann Whitney tests. Results: Seven-hundred and twenty-three patients were screened and 585 were eligible (cirrhosis with CTor MR scans). From these 585 patients, 65 were excluded due to age, pancreatitis, andpolycystic liver and/or kidney disease. Two-hundred and twenty-eight patients were in theClinic group, 150 in the MRI group, and 142 in the Transplant group. Mean age was 59,57, and 56 in the 3 groups, respectively. Male patients comprised 69%, 55%, and 75% ofthe 3 groups, respectively. Key results are listed in tables 1 and 2. Additionally, medianMELD score and interquartile range in patients with cysts (n=43) was 15 (10-18) andwithout cysts (n=457) was 11 (9-15), p=.03. PCL prevalence in patients with non-alcoholicsteatohepatitis (NASH) related cirrhosis was 1/64 (1.6%) compared to PCL prevalence of42/456 (9.2%) in all other liver disease (p ,.05). Discussion: Overall, there is a markedincrease in PCL prevalence in our cirrhosis cohorts compared to the non-cirrhotic population.The prevalence of PCL is highest in adult cirrhotic patients who underwent liver transplanta-tion. Further, there is a statistically significant association with increasing MELD score andPCL prevalence. The prevalence of PCL in patients with NASH-cirrhosis is similar to theprevalence in the non-cirrhotic population, while PCL prevalence is higher in patients withcirrhosis from viral hepatitis, alcoholic, and other liver disease. Prospective studies are neededto define pathogenesis and management of these incidental lesions in cirrhotic patients.Table 1 - Prevalence of PCL by Cirrhosis Cohort
Table 2 - Prevalence of PCL by MELD Score
Twenty patients had missing labs and therefore were excluded from the MELD sub-analysis.
Tu1229
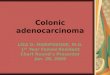
Pancreatic Cyst Prevalence and the Risk of Mucin-Producing Adenocarcinomain United States AdultsTimothy B. Gardner, Lisa M. Glass, Stuart R. Gordon
BACKGROUND & AIMS: The presence of a pancreatic cyst often prompts concern, althoughthe rate of malignant transformation to mucin-producing adenocarcinoma is not known.We aimed to determine the prevalence rate of mucin-producing adenocarcinoma in UnitedStates adults with pancreatic cysts. METHODS: This retrospective, population-based cross-sectional study calculated the annual number of mucin-producing adenocarcinomas usingthe SEER 18 database and the 2010 United States census. The overall prevalence rate ofcysts in the population was found using data from large cross-sectional imaging studies ofincidental cyst prevalence. Prevalence rates were then calculated by dividing the annualnumber ofmucin-producing adenocarcinomas by the cyst prevalence rate. RESULTS: Between2005 and 2009, 1,336 mucin-producing adenocarcinomas were estimated to be foundannually in a United States adult population of 137,154,960. The total number of pancreascysts, given a cyst prevalence rate of 2.5%, was 4,110,737. Therefore, the prevalence ofmucin-producing adenocarcinoma arising in patients with pancreatic cysts was 32.5 per100,000 (95% C.I. 21.8, 43.2). The prevalence rate was 31.2 per 100,000 (20.3, 42.1) infemales and 34.0 per 100,000 (22.6, 45.4) in males. As expected, the rate of malignanttransformation increased linearly with advancing age (highest 45.1 per 100,000 in 80-84year old males). CONCLUSION: Malignant transformation of pancreatic cysts into mucin-producing adenocarcinoma in United States adults is a very rare event. Current clinical
AG
AA
bst
ract
s

AG
AA
bst
ract
sguidelines and resource allocation for pancreatic cyst disease should be reconsidered giventhese findings.Annual crude and age-specific prevalence rates of mucin-producing adenocarcinoma in 40-84 year old United States patients with pancreatic cysts
Tu1230
Malignant Predictors for Branch Duct Type IPMNSeiko Hirono, Masaji Tani, Manabu Kawai, Ken-ichi Okada, Motoki Miyazawa, AtsushiShimizu, Yuji Kitahata, Masaki Ueno, Shinya Hayami, Hiroki Yamaue
Introduction: The indications for resection of the branch duct type IPMNhave been controver-sial, because branch duct type IPMN generally has a low risk of malignancy, althoughsurgical resection is required for all main duct type IPMN, because of its high malignantpotential. Therefore, in this study, we identified predictors of malignancy to determineindications for surgery for the patients with branch duct type IPMN. Methods: We retrospec-tively analyzed the clinicopathological factors of 162 patients who underwent resection forbranch duct type IPMN at Wakayama Medical University Hospital from July 1999 to October2012, to identify predictors of the malignant behavior of this neoplasm. For the purposeof the analyses, we classified IPMN with adenoma as a benign IPMN group, whereasnoninvasive and invasive IPMC were classified as a malignant IPMN group. The ROC curveswere used to determine the cutoff levels for the tumor size, main pancreatic duct (MPD)size, mural nodule size, and CEA level in the pancreatic juice to differentiate between benignand malignant IPMN in the patients with the branch duct type IPMN. Results: Of 162patients, 60 patients (37%) had adenoma, 53 patients (33%) had noninvasive IPMC, and49 patients (30%) had invasive IPMC. The areas under curve for the tumor size, MPD size,mural nodule size, and CEA level in the pancreatic juice were 0.612, 0.711, 0.819, and0.920, respectively, and the determined cutoff levels for the differentiation between benignand malignant IPMNs were 30 mm, 5 mm, 5 mm and 30 ng/ml, respectively. We found 6significant predictors for malignancy in the branch duct type IPMN in a univariate analysis;jaundice (P,0.01), MPD size .5mm (P,0.01), mural nodule size .5mm (P,0.01), elevatedserum CA19-9 level (P,0.01), positive cytology in the pancreatic juice (P=0.02), and CEAlevel in the pancreatic juice .30ng/ml (P,0.01). In a multivariate analysis, a mural nodulesize .5mm (P,0.01, odds ratio (95% CI); 12.9 (2.3-70)) and a CEA level in the pancreaticjuice .30ng/ml (P,0.01, odds ratio (95% CI); 299 (18-5067)) were independent factorsassociated with malignancy. When the combination of a mural nodule size .5mm and aCEA level in the pancreatic juice .30ng/ml is used, the positive predictive value was 100%(45/45), and the negative predictive value was 96.6% (28/29). Conclusion: We identifiedtwo useful predictive factors for malignancy in branch duct type IPMN; a mural nodule size.5mm and a CEA level in the pancreatic juice obtained by preoperative ERP .30ng/ml.
Tu1231
Dominant Cyst Size and Progression Rate Should Guide Management ofPatients With Multifocal IPMNRussell Rosenblatt, Irene Epelboym, John M. Poneros, Amrita Sethi, Charles J. Lightdale,John D. Allendorf, John A. Chabot, Tamas A. Gonda
Background Benign and premalignant cystic lesions of the pancreas are being identified withincreased frequency with widespread use of abdominal cross-sectional imaging. While mostare benign, intraductal papillary mucinous neoplasms (IPMN) carry a risk of malignanttransformation. Consensus guidelines exist for management of solitary IPMN, however themanagement of multifocal disease is less clear. The purpose of this study was to describethe natural history, impact of location, and risk of parallel progression of multifocal IPMN inan intermediate risk patient population. Methods We retrospectively reviewed demographiccharacteristics as well as cyst location, size, and imaging features of all patients in ourendoscopic surveillance database who were known to have discrete multiple IPMN. Wecompared this population to a control group of patients with unifocal IPMN. Continuousvariables were compared using Student's t-test and categorical variables were comparedusing chi square test. Results Between 1998 and 2012, 644 patients underwent endoscopicsurveillance at our institution; 90 (14%) had multifocal IPMN with 34 being followed withat least 2 endoscopic ultrasounds for at least 1 year. All patients had at least 2 lesions and11 (32.4%) had 3 or more. Twelve (35.3%) were located in non-adjacent pancreatic segments.Compared with 21 unifocal IPMN patients, differences in age (72.5 vs 76, p=0.903) and
S-798AGA Abstracts
gender (29.4% vs 38.1% male, p=0.505) were not statistically significant. Median dominantcyst size at presentation for multifocal was 11mm compared with 14mm for unifocal, p=0.558. Over a median follow-up time of 21 months for both groups, dominant cyst sizechanged from 11 to 12mm in multifocal compared with 14 to 13mm in unifocal group, p=0.842. Greater than 10% increase in cyst size was observed in 13(38.2)% of multifocalcompared with 4(19.1%) unifocal lesions, p=0.135. At presentation, median size of secondcyst in multifocal group was 6mm, with 7(20.6%) showing no change and 14 (41.2%)decreasing in size over the surveillance period. Most of the remaining cysts, median 7mmat presentation, remained stable in size. Only 1(3%) of dominant while none of the secondand third progressed beyond 30mm. Conclusions In patients with multifocal IPMN,meaning-ful size increase over timemainly occurs in the dominant (largest) lesion.While demographicsand cyst growth rates are not significantly different compared with unifocal disease, over athird occur in non-contiguous locations within the pancreas, presenting a potential challengeif surgical resection is eventually considered. In this intermediate risk population, incidenceof cyst size progression beyond resection criteria is low overall and not significantly differentthan that of unifocal lesions, arguing for continued endoscopic surveillance guided by growthof the dominant cyst.
Tu1232
How Should We Follow Branch Duct IPMN Cases? Along "InternationalConsensus Guidelines 2012 for the Management of IPMN and MCN of thePancreas"Daisuke Masuda, Takeshi Ogura, Akira Imoto, Ken Narabayashi, Sadaharu Nouda,Takanori Kuramoto, Kumi Ishida, Yosuke Abe, Toshihisa Takeuchi, Takuya Inoue, SatoshiTokioka, Michiaki Takii, Eiji Umegaki, Kazuhide Higuchi
Background and Aim: New International Consensus Guidelines for IPMN were publishedin 2012. We have several unsolved problems on diagnosis of IPMN subtypes or follow-upperiods of non-resected cases. In this study we evaluated how to follow up branch ductcases of IPMN Methods: We studied retrospectively our branch duct cases of IPMN alongthe new IPMN guidelines. We classified branch duct IPMN in three criteria; "high-riskstigmata", "worrisome features" or "no high-risk or worrisome features" on the respect ofimaging findings, and studied on imaging findings, cyto-pathological yields, resection andfollow-up cases. Subjects: Subjects were 302 branch duct IPMN cases (Mean ages; 67.8±0.5years, gender; male/female 145/157) in Osaka Medical College Hospital from 1995 to 2012.We had 31 "high-risk stigmata (HRS)", 55 "worrisome features (WF)", 216 "no high-riskor worrisome features (NHW)". HRS had 6 obstructive jaundice, 15 MPD ^10mm, 24solid component . Results: 1) MPD diameter; HRS: 8.4±1.2mm, WF: 4.6±0.2mm, NHW:2.7±0.1mm (HRS:WF p=0.0002, HRS:NHW p,0.0001, WF:NHW p,0.0001). Cyst size;HRS: 35.5±4.0mm, WF: 21.1±1.7mm, NHW: 16.1±0.1mm (HRS:WF p=0.0003, HRS:NHWp,0.0001, WF:NHW p=0.0003). Mural nodule diameter; HRS: 14.3±1.3mm, WF:4.4±0.3mm (HRS:WF p,0.0001). 2) Cyto-Pathological suspicious or positive rate; HRS;72.2% (13/18), WF; 42.9% (12/28), NHW; 18.8% (6/32) (HRS:WF p=0.0663, HRS:NHWp,0.0001, WF:NHW p=0.0232). 3) Resection / Follow; HRS: 48.4%(15/31) / 51.6%(16/31), WF: 20%(11/55) / 80%(44/55), NHW: 2.8%(6/216) / 97.2%(210/216) (HRS:WF p=0.0059, HRS:NHW p,0.0001, WF:NHW p,0.0001). 4) In 32 resection cases, we have 6invasive ductal cancer (ICD), 13 non invasive ductal cancer (NICD), 10 adenoma (AD), 3dysplasia (DY). We had 15 cases in HRS (ICD33.3%, NICD53.3%, AD 13.3%), had inWF 11 cases (NICD36.4%, AD45.5%, DY18.2%), and had in NHW 6 cases (ICD 16.7%,NICD16.7%, AD50.0%, DY16.7%). 5) In 270 follow-up cases, we had 40 exacerbation ofimaging findings in 984 days. Exacerbation rate was 68.8% in HRS, 15.9% in WF, and 10.5%in NHW (HRS:WF p,0.0001, HRS:NHW p,0.0001, WF:NHW p=0.3028). Exacerbationduration were 572 days in HRS, 1250 days in WF, 1074 days in NHW (HRS/WF: p=0.0395, HRS/NHW: p=0.1065, WF/NHW: p=0.6620). Conclusions: HRS cases had highermalignancy than WF or NHW, so HRS should be treated as malignancy along new guideline.But in NHW we had also 2 cancer in resection cases, furthermore 10.5% of NHW casesexacerbated in 1073 days, so we thought that careful follow-up is also needed for NHW cases.
Tu1233
The Clinical Outcome of Incidental Pancreatic Cystic Neoplasms in ElderlyPatientsSung Ho Kim, Jae Seon Kim, Hyejin Noh, Beom Jae Lee, Jong-Jae Park, Young-Tae Bak
Background/Aims: Incidental pancreatic cystic neoplasms (PCNs) are increasingly foundowing to the recent advances and more availability of the diagnostic modalities. Surgery isrecommended when the main pancreatic duct is ≥10 mm in diameter, or enhancing solidcomponent is found within the cyst. Surgery is also considered when one of the followingalarm features is present: A cyst of .3 cm in size, a thickened/enhancing cyst wall, a mainduct of 5-9 mm in diameter, a non-enhancing mural nodule, or an abrupt change in caliberof pancreatic duct with distal pancreatic atrophy. Considering the high risk of perioperativemorbidity, making decision for surgical operation in elderly patients is still very difficult.The aim of this study was to elucidate the clinical outcome of PCNs in patients with 65years or older in age. Methods: Patients who underwent either surgical operations or clinicalfollow-ups for longer than 1 year for radiologically proven PCNs between April 1997 andMarch 2006 were included and analyzed retrospectively. Results: Among 90 patients withincidental PCNs, 38 (surgery 10, follow-up 28) were 65 years or older (the older group)and 52 (surgery 25, follow-up 27) were younger than 65 years (the younger group). Theaverage follow-up duration was 31±18 months. Among 28 follow-up cases of the oldergroup, 21 had no alarm features, 7 had alarm features without undergoing surgery due tothe possibility of developing perioperative morbidity, and 2 case refused surgery. Among27 follow-up cases of the younger group, 19 had no risk factors, and 8 cases refused surgery.Postoperative morbidity developed in 4 of 10 cases (40.0%; splenic vessel rupture 1, abscess1, pleural effusion 1 and obstructive jaundice 1) of the older group and in 5 of 25 cases(20.0%; gastrointestinal bleeding 1, abscess 2, and pseudocyst 2) of the younger group (p=0.393). 1 case in the younger group experienced a recurrence of PCN 9 years after theinitial surgery. In 55 cases of the follow-up group, the diameter of PCNs increased in 6 of28 cases (21.4%) in the older group and 4 of 27 cases (14.8%) in the younger group (P=