Embed Size (px)
Citation preview

Trombociti i koronarna bolest
Prof. dr. sc. Mislav Vrsalović FESC, FSVM
Trombociti - interdisciplinarni pristup Zagreb, 11. studenoga 2017.

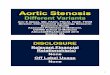
Atherothrombosis* is the
Leading Cause of Death Worldwide1
* Atherothrombosis defined as ischemic heart disease and cerebrovascular disease. 1 The World Health Report 2001. Geneva. WHO. 2001.
22.3
19.3
12.6
9.7
9
6.3
0 5 10 15 20 25 30
Atherothrombosis*
Infectious Disease
Cancer
Injuries
Pulmonary Disease
AIDS
Causes of Mortality (%)

Atherothrombosis Significantly
Shortens Life
Analysis of data from the Framingham Heart Study.
Peeters A, et al. Eur Heart J. 2002;23:458-466.
Atherothrombosis reduces life expectancy by around
8-12 years in patients aged over 60 years1
Average Remaining Life Expectancy at Age 60 (Men)
0
4
8
12
16
20
Healthy
Years
History of AMI
-9.2
years
History of Cardiovascular Disease
-7.4
years
History of Stroke
-12
years

Cerebral Ischemic stroke
Transient ischemic attack
Cardiac Myocardial infarction
Angina pectoris (stable, unstable)
Peripheral Arterial Disease
Critical limb ischemia, claudication
Clinical Manifestations of Atherothrombosis

Common Underlying Atherothrombotic
Disease Process
MI, myocardial infarction; PAD, peripheral arterial disease; CV, cardiovascular.
Ness J, et al. J Am Geriatr Soc. 1999;47:1255-1256.
Schafer AI. Am J Med. 1996;101:199-209.
Atherothrombotic Events (MI, Stroke, or CV Death)
Plaque
Rupture
Platelet
Adhesion,
Activation, and
Aggregation
Thrombus
Formation
MI Atherothrombotic
Stroke PAD Unstable Angina

Risk of a Second Atherothrombotic Event
Increased Risk vs General Population (%)
Original Event MI Stroke
MI 5-7 times
greater risk
(includes death)*
3-4 times greater risk
(includes TIA)
Stroke 2-3 times
greater risk (includes angina and sudden
death)*
9 times
greater risk
PAD 4 times
greater risk*
2-3 times greater risk
(includes TIA)
* Death documented within 1 hour of an event attributed to CHD.
Note:This chart is based on epidemiologic data and is not intended to provide a direct basis for
comparison of risks between event categories.
MI, myocardial infarction; TIA, transient aschemic attack, PAD, peripheral artery disease.
Adult Treatment Panel II. Circulation. 1994;89:1333-1363.
Kannel, WB. J Cardiovasc Risk. 1994;1:333-339.
Wilterdink, JI, et al. Arch Neurol. 1992;49:857-863.
Crique, MH, et al. N Engl J Med. 1992;326:381-386.

Unstable
angina
MI
Ischemic
stroke/TIA
Critical leg
ischemia
Intermitent
claudication
CV death
ACS
Atherosclerosis
Stable angina/
Intermittent claudication
Atherothrombosis: A Generalized and
Progressive Process
Thrombosis
Adapted from Libby P. Circulation. 2001;104:365-372.

Atherothrombosis: Thrombus Superimposed on
Atherosclerotic Plaque
Adapted from Falk E, et al. Circulation. 1995;92:657-671.

Characteristics of Unstable and
Stable Plaque
Thin
fibrous cap
Inflammatory
cells
Few
SMCs
Eroded
endothelium Activated
macrophages
Thick
fibrous cap
Lack of
inflammatory
cells
Foam cells
Intact
endothelium
More
SMCs
Libby P. Circulation. 1995;91:2844-2850.
Unstable Stable

Plaque Rupture
Andrew Farb, MD by permission.

Impaired Fibrinolysis
Fibrinogen Diabetes Mellitus
Cholesterol
Smoking Cap Fatigue
Atheromatous Core (size/consistency)
Cap Inflammation
Homocysteine
Plaque Rupture
Cap Thickness/
Consistency
Systemic Factors Local Factors
Risk Factors for Plaque Rupture
Fuster V, et al. N Engl J Med. 1992;326:310-318.
Falk E, et al. Circulation. 1995:92:657-671.


Akutni
koronarni
sindrom

Smrtnost bolesnika s AKS je i dalje visoka
Smrtnost bolesnika s AKS-om kod kojih je napravljena PCI u prvoj godini
nakon dijagnoze1
AKS – akutni koronarni sindrom; NAP – nestabilna angina pektoris
NSTEMI – infarkt miokarda bez ST elevacije; STEMI – infarkt miokarda sa ST elevacijom
- Svakih 12 sati u Hrvatskoj umru najmanje 2 osobe zbog AKS-a.2

ACS: Tip of the Atherothrombotic “Iceberg”
ACS, acute coronary syndrome; UA, unstable angina; NSTEMI, non-ST-segment elevation myocardial
infarction; STEMI, ST-segment elevation myocardial infarction.
Adapted from Goldstein JA. J Am Coll Cardiol. 2002;39:1464-1467.
Clinical
Subclinical
Presence of Multiple Coronary Plaques
Vascular Inflammation
Persistent Hyperreactive
Platelets
Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)

Hemostatic Plug Formation
Thrombin
AGGREGATION
Fibrin
Hemostatic
Clot
Clotting Platelet Aggregation
0 min 10 min 5 min
SECONDARY
PRIMARY
COAGULATION
Adapted from Ferguson JJ, et al. Antiplatelet Therapy in Clinical Practice. 2000:15-35.


1. Platelet Adhesion
2. Platelet Activation
Platelet
GP Ib
Plaque rupture Activated Platelet
GP IIb/IIIa
ASA, acetylsalicyclic acid.
Cannon and Braunwald, Heart Disease. 2001.
TxA2
Fibrinogen
GP IIb/IIIa Inhibitors
ASA, Clopidogrel/Ticlopidine
Platelets Role in Thrombosis

Thrombin Serotonin Epinephrine Collagen Activation
Activated
Platelet
COX
Degranulation
Aspirin
Gp IIb/IIIa
fibrinogen
receptor
To neighboring
platelet
Clopidogrel
Ticlopidine
Platelet agonists
ADP ATP serotonin calcium magnesium
Adhesive proteins
thrombospondin
fibrinogen
p-selectin
vWF
Coagulation factors
factor V factor XI PAI-1
Inflammatory factors
platelet factor 4
CD 154 (CD 40 ligand)
PDGF
IV Gp IIb/IIIa Inhibitors
TXA, thromboxane; PDGF, platelet-derived growth factor.

Platelet Hyperreactivity Following ACS
Predicts 5-Year Outcomes
Platelet Aggregability Status
0
10
20
30
40
50 Death
Cardiac Events
10.3
6.4
14.9
24.1
46.2
34.6
Pati
en
ts (
%)
*RR=1.6
(CI 0.5-5.5)
Negative
(n=94)
*RR=1.6
(CI 0.7-3.5)
*RR=5.4
(CI 2.2-13.4)
*RR=3.1
(CI 1.6-5.8)
Intermediate
(n=29)
Positive
(n=26)
ACS, acute coronary syndrome.
* Relative risk compared to group with negative aggregation.
Adapted from Trip MD, et al. N Engl J Med. 1990;322:1549-1554.

Terapija AKS
Antiishemijski lijekovi
Antikoagulansi
-UFH ili LMWH
-fondaparinux
-bivalirudin
Antiagregacijska th.
-ASK
-klopidogrel
-Gp IIb/IIIa inhibitori
Revaskularizacija


Antitrombocitna terapija: klopidogrel – preko 10 godina životnog iskustva na širokom spektru
bolesnika
10 kliničkih ispitivanja uključijući preko 130.000 bolesnika
Učinkovitost i sigurnost klopidogrela dokazana je na preko 130
milijuna bolesnika u svijetu
Okosnica antitrombocitne terapije
Prasugrel i tikagrelor – novi antitrombotici
Approved 2011


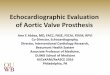
Antiplatelet Mechanism of Action
Aspirin blocks cyclooxygenase, the enzyme that mediates the first step in the biosynthesis of prostaglandins and thromboxanes from arachidonic acid, preventing platelet aggregation
The P2Y12 (ADP) receptor blockers (clopidogrel, etc.) block the binding of adenosine diphosphate (ADP) to a platelet receptor P2Y12, thereby inhibiting activation of the glycoprotein (GP) IIb/IIIa complex and platelet aggregation
Anti-GP IIb/IIIa antibodies and receptor antagonists inhibit the final common pathway of platelet aggregation (the cross-bridging of platelets by fibrinogen binding to the GP IIb/IIIa receptor)

Aspirin
Platelets do not synthesize new enzymes functional defect induced by aspirin persists for the life of the platelet (nonreversible)
In ACS, including Unstable Angina and NSTEMI: reduction in the combined endpoints of subsequent nonfatal MI, nonfatal stroke, and vascular death Give first dose in ACS of 162-325mg, crushed or chewed, as soon as possible in ACS
ASA has rapid and immediate antithrombotic effect
Discharge patient on ASA 75-100mg daily and to be continued indefinitely for secondary prevention
Side effects: GI intolerance, worsening of preexistent bleeding
Primary Prevention
1. Benefit of ASA must be weighed against risk of bleeding 1. Risk of bleeding likely to outweigh benefits in patients w/ Framingham 10 year risk scores < 10%
2. Consider in patients with DMII and those with CKD as well as patients w/ Framingham risk scores > 10%

ADP receptor antagonists (P2Y12
receptor blockers) Ticlopidine: rarely used anymore due to risk of thrombocytopenia, neutropenia, GI upset and TTP-HUS
Clopidogrel: DAPT with Clopidogrel and ASA was superior compared to ASA alone in patients w/ NSTEMI 3 limitations to the use of clopidogrel Delayed onset of action
Large individual variability in platelet response due to mutation in CYP2C19 allele decreased platelet inhibition and increase in ischemic events
Inhibitory effect on platelets is Irreversible
Prasugrel: more rapid onset of action and achieves higher degrees of platelet inhibition than clopidogrel Compared with Clopidogrel, 19% reduction in cardiovascular
death/MI/stroke when given at time of planned PCI, however bleeding risk greatly increased (including life-threatening bleed)
Contraindicated in patients w/ history of stroke, age > 75 years, or weight < 60 kg

Ticagrelor
Binds reversibly to the P2Y12 platelet
receptor
More rapid onset of action than clopidogrel
More intense platelet inhibition than
clopidogrel
Data reveals better *efficacy* than clopidogrel
with reduction in cardiovascular death, MI,
stroke in patients with ACS

Klopidogrel: preko 10 godina kliničkog
iskustva
Indikacija
nakon IM, CVI ili
dokazane PAB
Publicirana ispitivanja
Godina publikacije
CAPRIE
1996
CAPRIE CAPRIE CAPRIE
CLASSICS CLASSICS CLASSICS
CURE
(PCI-CURE)
CURE
(PCI-CURE)
CREDO
2000 2001 2002
CAPRIE CAPRIE CAPRIE CAPRIE CAPRIE
CLASSICS CLASSICS CLASSICS CLASSICS CLASSICS
CURE
(PCI-CURE)
CURE
(PCI-CURE)
CURE
(PCI-CURE)
CURE
(PCI-CURE)
CURE
(PCI-CURE)
CREDO CREDO CREDO CREDO CREDO
2004 2004 2006 2005 2005
MATCH MATCH MATCH MATCH MATCH
CLARITY CLARITY CLARITY CLARITY
COMMIT
CCS2
COMMIT
CCS2
COMMIT
CCS2
CHARISMA CHARISMA
CARESS
2009
CARESS CARESS CARESS CARESS
MATCH
CREDO
CURE
(PCI-CURE)
CLASSICS
CAPRIE CAPRIE
CLASSICS
CURE
(PCI-CURE)
CREDO
MATCH
CLARITY
COMMIT
CCS2
CHARISMA
2009
CARESS
CURRENT CURRENT
ACTIVE
Indikacija u
UA/NSTEMI
Indikacija u
STEMI
Indikacija u AF
~130,000 bolesnika liječenih klopidogrelom u 10 kliničkih ispitivanja
~130 milijuna bolesnika liječenih u svakodnevnoj kliničkoj praksi
1. Data on file
2. IMS data MAT 12/10

Klopidogrel: manje združenih događaja
KV smrti, IM ili CVI nakon PCI
Meta analiza PCI-CURE, PCI-CLARITY i CREDO: konzistentan povoljan učinak liječenja klopidogrelom
na KV smrti, IM ili moždani udar nakon PCI: 28% smanjenje događaja u bolesnika koji nisu primali GP
IIb/IIIa inhibitor u vrijeme PCIa i 31% smanjenje događaja u bolesnika liječenih GP IIb/IIIa inhibitorom
Sabatine MS et al. Am Heart J 2008;155:910–917.
KV-kardiovaskularni, IM-infarkt miokarda, MU-moždani udar, PCI-perkutana koronarna intervencija

Klopidogrel: bez signifikantnog povećanja broja
TIMI velikih ili manjih krvarenja nakon PCI
Meta-analiza PCI-CURE, PCI-CLARITY i CREDO: Primjena klopidogrela nije bila povezana sa
signifikantnim porastom kompozitnog ishoda TIMI major i minor krvarenja, bez obzira na primjenu
GP IIb/IIIa inhibitora
Sabatine MS et al. Am Heart J 2008;155:910–917.

Zašto je krvarenje važno?
Smrtnost i krvarenje u bolnici nakon PCI
Peterson ED ACC 2007
Mehta SR ACC 2007 PCI-perkutana koronarna intervencija
• krvarenja u bolnici usko koreliraju sa smrtnošću nakon PCI

COMMIT: klopidogrel smanjuje
kombinirani ishod smrti, IM ili CVI za 9%
u STEMI D
og
ađ
aji
(%
)
Chen ZM. Lancet 2005;366:1607–21
klopidogrel (9.3%)
RRR=9%
P=0.002
Placebo (10.1%)
0 0 7 14 21 28
2
4
6
8
10
Dani od randomizacije
Clopidogrel Placebo Odds ratio & 95% CI
Clopid. better Placebo better (22,958) (22,891)
Hour
to entry
0-6
7-12
13-24
ALL
776 (9.3%)
672 (9.7%)
666 (8.8%)
2125 (9.3%)
904 (10.9%)
735 (10.7%)
666 (8.7%)
2311 (10.1%) 9% SE 3
(2P = 0.002)
0.4 0.6 0.8 1.0 1.2 1.4 1.6

CURRENT OASIS 7:
Klopidogrel dvostruka vs standardna doza:
primarni ishod - PCI bolesnici
Dani
Ku
mu
lati
vn
i ri
zik
0.0
0
.01
0
.02
0
.03
0
.04
0 3 6 9 12 15 18 21 24 27 30
Klopidogrel standardna doza
Klopidogrel dvostruka doza
HR 0.86
95% CI 0.74-0.99
P=0.039
14%
RRR
CV smrt, IM ili moždani udar
Mehta SR, et al. Lancet 2010;376:1233–1243

CURRENT OASIS 7:
Klopidogrel dvostruka vs standardna doza Stent tromboza (potvrđena angiografski)
0 3 6 9 12 15 18 21 24 27 30
Dani
Ku
mu
lati
vn
i ri
zik
0.0
0
.00
4
0.0
08
0
.01
2 Klopidogrel standardna doza
Klopidogrel dvostruka doza
46%
RRR
HR 0.54
95% CI 0.39-0.74
P=0.0001
Mehta SR, et al. Lancet 2010;376:1233–1243

Što je s novim antitrombocitnim lijekovima?
• učinkovitost: početak djelovanja
• sigurnost: krvarenja

Prasugrel vs klopidogrel: PCI bolesnici smanjenje događaja uz veći rizik od krvarenja
TRITON TIMI: Wiviott, N Engl J Med 2007;357:2001-15

Prasugrel vs klopidogrel: “TRILOGY ACS”
bez razlike u događajima
Medikamentozno liječeni visokorizični bolesnici sa UA/NSTEMI
(bez revaskularizacije)
nema razlike u
kompozitnim
događajima (KV smrt,
IM, CVI) između
prasugrela i
klopidogrela u prvoj
godini
http://www.theheart.org/article/1437675.do?utm_medium=email&utm_source=20120825_ESC2012_en_world&utm_campaign=newsletter;
http://spo.escardio.org/sessiondetails.aspx?eevtid=54&fp=401&doc=webcast

Tikagrelor vs klopidogrel:
smanjenje događaja uz veći rizik od ne-CABG
krvarenja i fatalnih intrakranijalnih krvarenja
PLATO: Walletin, N Engl J Med 2009;361:1-13

Ograničenja prilikom upotrebe novih
antitrombotičkih lijekova
PRASUGREL
• u bolesnika s visokim rizikom od
krvarenja, osobito:
- bolesnici stariji od 75 godina
- bolesnici lakši od 60 kg
• kontraindikacija - CVI/TIA u
anamnezi
TIKAGRELOR • kontraindikacija – intrakranijalno
krvarenje u anamnezi
• posebna upozorenja – povećani
rizik od krvarenja
- Povećani rizik od ne-CABG
krvarenja (AKS bolesnici na
tikagreloru i ASK)
• češća pojava dispneja (oprez
kod bolesnika s astmom i
KOPB-om)
• suradljivost - 2 tbl. na dan
(doza održavanja)
MU-moždani udar, TIA-tranzitorna ishemična ataka; ASK-acetilsalicilna kiselina

42
ESC smjernice za liječenje NSTEMI
- P2Y12 inhibitori
Grupa I , razina B
The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without ST-segment elevation of the European
Society of Cardiology (ESC). ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-
segment elevation. European Heart Journal. Published online 26 August 2011
a50% inhibicija agregacije trombocita

TIKAGRELOR: Prvi i jedini odobreni CPTP
TIKAGRELOR
pripada novoj kemijskoj skupini; ciklo-pentil-triazolo-pirimidina (CPTP)
je aktivna supstanca, ne zahtjeva prethodnu pretvorbu u aktivan oblik
je selektivni antagonist receptora adenozin difosfata (ADP)
Vezuje se direktno i reverzibilno na P2Y12 receptore i na taj način sprječava ADP-om posredovanu aktivaciju i agregaciju trombocita
Tienopiridini (klopidogrel) zahtjevaju prethodnu pretvorbu u aktivan oblik i vezuju se ireverzibilno za P2Y12 receptor
P2Y12 receptor
na trombocitu
BRILIQUE
ADP mjesto
vezanja
Husted S, et al. Eur Heart J. 2006;27:1038–1047.
Gurbel PA, et al. Expert Opin Drug Metab Toxicol. 2009;5(8):989–1004.
Van Giezen JJ, et al. J Thromb Haemost. 2009;7:1556–1565.

TIKAGRELOR: Nije potrebna prethodna aktivacija
BRILIQUE:
NIJE POTREBNA PRETHODNA
AKTIVACIJA LIJEKA
Klopidogrel:
PREDLIJEK – ZAHTJEVA PRETHODNU
PRETVORBU U AKTIVAN OBLIK
Aktivan oblik
Intermedijarni metabolit
Predlijek
Prilagođeno iz Schomig A. N Engl J Med. 2009;361:1108–1111.

0
20
40
60
80
100
0 2 4 6 8 10 12 14 16 18 20 22 24
TIKAGRELOR - Brz početak djelovanja
*
*
* *
*
BRILIQUE (n=54)
Klopidogrel (n=50)
Placebo (n=12)
Prilagođeno iz Gurbel PA, et al. Circulation. 2009;120:2577–2585.
BRILIQUE 180-mg udarna doza kod stabilnih CAD pacijenata
Klopidogrel 600-mg udarna doza kod stabilnih CAD pacijenata
Inh
ibic
ija a
gre
ga
cij
e t
rom
bo
cit
a (
IPA
)
Udarna doza
Vrijeme (sati)
BRILIQUE
Klopidogrel *P<0.0001 BRILIQUE vs
klopidogrel Placebo
Veza između IPA i kliničke aktivnosti još nije potvrđena

Klinička farmakologija: TIKAGRELOR i klopidogrel
Gurbel PA, et al. Circulation. 2009;120:2577–2585.
Sažetak opisa svojstava lijeka Brilique (BRILIQUE)
PLAVIX® [Uputa o lijeku, Hrvatska]..
TIKAGRELOR Klopidogrel
Kemijska klasa CPTP tienopiridini
Reverzibilna inhibicija P2Y12 receptora DA NE
PD varijabilnost CYP2C19 genotipa NE DA
Doziranje 2 puta dnevno (bid) jednom dnevno (qd)
Srednja inhibicija agregacije trombocita
nakon 30 min 41% 8%
Srednja inhibicija agregacije trombocita
nakon 2 sata 89% 38%

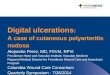
TIKAGRELOR ima dvostruki mehanizam djelovanja:
antitrombocitni učinak i pojačan adenozinski odgovor
Inhibicija receptora P2Y12 1,2
Antitrombocitni učinak
Inhibicija ENT-1 transportera3,4,5
Poboljšan lokalni adenozinski
odgovor može rezultirati:*
Dodatna inhibicija
agregacije/aktivacije
trombocita
Kardioprotekcija6
Vazodilatacija5,7,8
Modulacija upale
Dispneja7
Figure adapted from Nylander S, et al. (2013).
AC, adenylyl cyclase; ADP, adenosine diphosphate; cAMP, cyclic adenosine monophosphate; ENT, equilibrative nucleoside transporter.
References in slide notes.
Eritrocit
Adenozin
cAMP
Trombocit
ADP
ENT-1
Tikagrelor
AC
Gi Gs
A2A P2Y12
Aktivacija/agregacija trombocita
1. van Giezen JJJ, et al. J Thromb Haemost 2009;7:1556–1565.
2. Wallentin L. Eur Heart J 2009;30:1964–1977.
3. Nylander S, et al. J Thromb Haemost 2013;11:1867–1876.
4. Armstrong D, et al. J Cardiovasc Pharmacol Ther; In press.
5. van Giezen JJJ, et al. J Cardiovasc Pharmacol Ther 2012;17:164–172.
6. Wang K, et al. Thromb Haemost. 2010;104:609-17.
7. Wittfeldt A, et al. J Am Coll Cardiol 2013;61:723–727.
8. Alexopoulos D, et al. Circ Cardiovasc Interv 2013;19:5121–5126.

TIKAGRELOR: Smanjenje kardiovaskularne
smrtnosti u bolesnika s AKS-om
ARR – apsolutno smanjenje rizika; RRR – relativno smanjenje rizika; HR – omjer rizika
NNT – potreban broj liječenih osoba da bismo spriječili jedan događaj
CI – interval pouzdanosti
Wallentin L, et al.N Engl J Med. 2009;361:1045-1057.

TIKAGRELOR ne pokazuje značajne razlike u cjelokupnom
broju teških, smrtonosnih i po život opasnih krvarenja
Učestalost krvarenja definirano po PLATO-u i TIMI-ju *
* TIMI – tromboliza kod infarkta miokarda
Wallentin L, et al. N Engl J Med. 2009;361:1045–1057.