Embed Size (px)
Citation preview

Platinum Priority – Pelvic PainEditorial by George A. Barbalias on pp. 366–368 of this issue
Trigonal Injection of Botulinum Toxin A in Patients with
Refractory Bladder Pain Syndrome/Interstitial Cystitis
Rui Pinto a,b, Tiago Lopes a, Barbara Frias b,c, Andre Silva a,b, Joao Alturas Silva a,b,Carlos Martins Silva a,b,c, Celia Cruz b,c, Francisco Cruz a,b,c,*, Paulo Dinis a,b,c
a Department of Urology, Hospital de Sao Joao, Portugalb Faculty of Medicine, University of Porto, Portugalc Institute of Histology and Embryology (Faculty of Medicine of Porto) and Instituto de Biologia Molecular e Celular, University of Porto, Portugal
E U R O P E A N U R O L O G Y 5 8 ( 2 0 1 0 ) 3 6 0 – 3 6 5
avai lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Article info
Article history:
Accepted February 23, 2010Published online ahead ofprint on March 6, 2010
Keywords:
Bladder pain syndrome
Interstitial cystitis
Botulinum toxin
NGF
BDNF
Bladder trigone
Pain
Abstract
Background: Bladder pain syndrome/interstitial cystitis (BPS/IC) is a chronic dis-
ease without an effective treatment, characterized by pain during bladder filling.
Most nociceptive bladder afferents course in the trigone.
Objective: To evaluate efficacy and tolerability of trigonal injection of botulinum
toxin A (BoNTA) in patients with BPS/IC. Urine concentration of nerve growth factor
(NGF) and brain-derived neurotrophic factor (BDNF) were also evaluated.
Design, setting, and participants: Women with refractory BPS/IC were included in
an open, exploratory study.
Intervention: Under sedation, 100 U of BoNTA (Botox) were injected in 10 trigonal
sites (10 U per 1 ml saline). Retreatment was allowed 3 mo after injection.
Measurements: Pain, urinary frequency, O’Leary-Sant score (OSS), quality of life,
(QoL), and urodynamic testing at 1 and 3 mo and every 3 mo thereafter. Urine NGF
and BDNF were assessed at the same points. Patients who were retreated were
evaluated every 3 mo.
Results and limitations: All patients reported subjective improvement at 1- and
3-mo follow-up. Pain, daytime and nighttime voiding frequency, OSS, and QoL
improved significantly. Bladder volume to first pain and maximal cystometric
capacity more than doubled. Treatment remained effective in >50% of the patients
for 9 mo. Retreatment was also effective in all cases, with similar duration. A
significant, transient reduction in urinary NGF and BDNF was observed. No cases of
voiding dysfunction occurred.
The low number of patients and the lack of a placebo arm are obvious limitations
of this study.
Conclusions: Trigonal injection of BoNTA is a safe and effective treatment for
refractory BPS/IC.
soc
. H513r@m
# 2010 European As
* Corresponding authorPortugal. Fax: +351 225E-mail address: cruzfjm
0302-2838/$ – see back matter # 2010 European Association of Urology. Publis
iation of Urology. Published by Elsevier B.V. All rights reserved.
ospital S. Joao, Faculty of Medicine of Porto and IBMC of Porto, Porto,655.ed.up.pt (F. Cruz).
hed by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2010.02.031

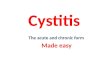
Fig. 1 – Location of trigonal injection sites. Each site was injected withbotulinum toxin A, 10 U per 1 ml saline.
E U R O P E A N U R O L O G Y 5 8 ( 2 0 1 0 ) 3 6 0 – 3 6 5 361
1. Introduction
The International Continence Society (ICS) has defined
painful bladder syndrome as the complaint of suprapubic
pain related to bladder filling accompanied by other
symptoms such as daytime and nighttime voiding fre-
quency in the absence of a proven urinary infection or other
obvious pathology [1]. The European Society for the Study of
Interstitial Cystitis (ESSIC), in an attempt to use a consistent
pain syndrome terminology, has preferred the term bladder
pain syndrome (BPS). BPS is defined as pelvic pain, pressure,
or discomfort perceived to be related to the urinary bladder,
accompanied by at least one other urinary symptom such as
a persistent urge to void or increased daytime and
nighttime voiding frequency [2]. The definition of interstitial
cystitis (IC) should probably be restricted to cases that
include typical cystoscopic and histologic features [1,2]. In
this paper, the designation BPS/IC will be used.
The etiology of BPS/IC is unknown. Therefore, BPS/IC
management is directed to pain relief, as bladder pain is
believed to drive both voiding frequency and nocturia.
Botulinum toxin A (BoNTA) has been shown to decrease
noxious input [3,4]. The analgesic effect of BoNTA pre-
sumably results from decreased neuropeptide release at
peripheral extremities [5], and glutamate, substance P, and
calcitonin gene-related peptides from the central endings of
bladder sensory nerves [5]. In the first case, neurogenic
inflammation is prevented, and in the second, nociceptive
transmission becomes inhibited at the spinal cord.
Most nociceptive bladder afferents are concentrated in
the trigone [6]. This may suggest that previous studies that
injected the entire bladder of BPS/IC patients with BoNTA
[7,8] placed most of the neurotoxin far from the nociceptive
fibers and increased the risk of decreasing detrusor
contractility. The hazard of vesicoureteral reflux after
trigonal BoNTA is nonexistent [9]. Therefore, we undertook
a pilot study evaluating the effectiveness, safety, and
duration of treatment/retreatment of BPS/IC patients with
BoNTA applied exclusively to the trigone. Additionally, the
urine concentration of two neurotrophic factors known to
influence the activity of nociceptive afferent fibers—nerve
growth factor (NGF) and brain-derived neurotrophic factor
(BDNF)—was assessed. The urinary levels of NGF were
previously shown to be increased in BPS/IC patients [10].
However, BDNF, an equally ubiquitous neurotrophin, has
never been investigated in this disease.
2. Material and methods
Twenty-six women with BPS/IC gave written informed consent to
receive BoNTA, a practice that has been approved by the ethics
committee of our institution in refractory cases. Patients were informed
about the possible complications of BoNTA administration, including the
necessity of occasional self-catheterization.
All patients had experienced symptoms for >6 mo and had
undergone cystoscopy with hydrodistension and bladder biopsy under
general anesthesia. Previous unsuccessful treatments included oral
pentosan polysulphate, amitriptyline, intravesical heparinoids, and
intravesical dimethyl sulfoxide. Two patients had had intravesical
resiniferatoxin 2 yr previously. Pregnancy, neurologic diseases, urinary
tract infections (UTIs), aminoglycoside use, bladder outlet obstruction,
detrusor overactivity, urinary incontinence, bladder stones, and previous
pelvic radiotherapy were exclusion criteria.
All patients were evaluated by history, physical examination, serum
biochemistry, urinalysis, urine culture and cytology, and imaging
assessing the upper and lower urinary tracts. Pain intensity was scored
using a 10-point visual analog scale (VAS). Patients provided a 3-d
voiding frequency volume chart [11], and the O’Leary-Sant score (OSS)
was used to assess symptoms and problems. Quality of life (QoL) was
evaluated using question 8 of the International Prostate Symptoms
Score. Pressure-flow studies (Dantec Dynamics Ltd., Bristol, England),
followed ICS directives. A 6-French dual-channel catheter was used,
infusing saline at room temperature (25 ml/min). Bladder volumes for
first sensation/pain of bladder filling, maximum cystometric capacity,
maximum urinary flow rate during voiding phase (Qmax), bladder
contractility index, and postvoid residual (PVR) volume were assessed.
BoNTA (Allergan, Irvine, CA, USA) was injected under light sedation
through a 23-gauge needle (Coloplast A/S, Humlebaek, Denmark)
inserted 3 mm into the trigonal wall underneath cystoscopic control.
A total of 100 U was distributed throughout 10 sites (10 U per 1 ml saline,
Fig. 1). Patients received prophylactic ciprofloxacin; specifically, 500 mg
twice a day for 3 d.
After 2 wk, PVR volume and muscle weakness were assessed. Urine
was collected for culture. Patients were further evaluated at 1 and 3
mo and every 3 mo thereafter using VAS for pain, a 3-d voiding chart,
OSS, QoL, and urodynamic investigations, as performed at baseline.
Patients could ask for retreatment after the 3-mo visit if they reported
symptom reappearance and OSS and VAS confirmed a return to
baseline values.
Urinary NGF and BDNF were also measured in the last 10 patients, at
baseline and at 1, 3, and 6 mo after BoNTA injection. Urine samples were
collected at a full bladder sensation, immediately put on ice, and
centrifuged (3000 rpm; 10 min at 4 8C). The supernatant was collected in
1.5-ml tubes and stored at �80 8C. NGF and BDNF concentrations were
determined by ELISA (Emax Immunoassay System, Promega, Madison,
WI, USA), with a minimum sensitivity of 3.9 pg/ml and 7.8 pg/ml,
respectively, following the manufacturer’s instructions. Briefly, 96-well
plates were coated with anti-NGF/BDNF polyclonal antibodies. Urine or
NGF/BDNF standards were added to each well, and plates were
incubated. After several washes, anti-NGF/BDNF monoclonal antibodies
were added, and plates were again incubated. After thorough washes,
the amount of bound monoclonal antibody was detected using
immunoglobulin G–horseradish peroxidase-conjugated antibody. The
unbound conjugate was washed out, followed by a 10-min incubation
with a 100 ml substrate solution at room temperature. Hydrochloric acid
was added to terminate the reactions. Color change was measured with a
Synergy HT Microplate Reader (Bio-Tek Instruments, Winooski, VT, USA)

Table 1 – Classification of patients according to European Society for the Study of Interstitial Cystitis criteria [2]
Bladder pain syndrome classification Biopsy
X (not done) A (normal) B (inconclusive) C (positive)
Cystoscospy with hydrodistension X (not done) 0 0 0 0
1 (normal) 0 0 0 0
2 (glomerulations) 0 1 1 6
3 (Hunner’s lesion) 0 1 2 15
Table 2 – Data at baseline and after first and second treatments
First treatmentbaseline
First treatment,first month
First treatment,third month
Secondtreatmentbaseline
Secondtreatment,
third month
Pain visual analog scale (0–10) 5.8 � 1.8 2.1 � 0.3* 1.7 � 0.8* 4.3 � 0.6 1.6 � 0.6*
Daytime frequency 11.4 � 3.6 5.5 � 1.2* 4.7 � 0.9* 8 � 2 5 � 2*
Nighttime frequency 5.5 � 1.9 2.7 � 1.1* 2.1 � 0.7* 4.3 � 0.6 3 � 1*
O’Leary-Sant score for symptoms (0–20) 15.6 � 3 8.4 � 1.1* 6.8 � 1.2* 11.3 � 1.2 7.5 � 1.5*
O’Leary-Sant score for problems (0–16) 13.4 � 3.4 4.9 � 2.1* 4.6 � 1.3* 7 � 3 5 � 2.6*
Quality of life (0–6) 5.1 � 0.9 1.8 � 0.4* 0.7 � 0.5* 4 � 0.6 1.7 � 0.6*
Bladder volume for first sensation/pain (ml) 44 � 20 104 � 23* 107.5 � 20.8* 44 � 14 90 � 23*
Maximum cystometric capacity (ml) 106 � 42 244 � 56* 279 � 82* 139 � 33 214 � 61*
Bladder contractility index
(PdetQmax + 5 � Qmax)
70.2 � 42 78 � 15.2 80.8 � 14 70.5 � 13.5 82 � 13.5
Maximum urinary flow rate (ml/s) 13.3 � 1.8 14.6 � 2.8 15.3 � 2.5 13.1 � 2.4 15.4 � 2.8
Postvoid residual volume (ml) 3.1 � 4.3 10.9 � 4.9 13.8 � 6.3 12 � 4.5 12.4 � 6.7
* p < 0.05.
E U R O P E A N U R O L O G Y 5 8 ( 2 0 1 0 ) 3 6 0 – 3 6 5362
at 450 nm. All samples were run in duplicate, and values were averaged.
NGF and BDNF levels were normalized to the urinary concentration of
creatinine.
Results are presented as mean values plus or minus standard
deviations. A paired t test was used for intragroup comparisons. A
Wilcoxon test for nonparametric data was used for multiple compar-
isons. Kaplan-Meyer plots were applied to the duration of treatment. A p
value of <0.05 was considered statistically significant. Analysis of data
was performed using IBM SPSS v.18.0 for the Macintosh (SPSS Inc., an
IBM Company, Chicago, IL, USA).
3. Results
Patients had a mean age of 48.1 � 13 yr. All patients had
typical cystoscopic findings, and the majority had positive
findings in bladder samples. The ESSIC classification for all 26
patients is presented in Table 1.
Fig. 2 – O’Leary-Sant score for symptoms (0–20) and problems (0–16) at baseli* = p < 0.05.
Symptoms were present for 5 � 2 yr. Table 2 shows VAS
value, daytime and nighttime voiding frequency, OSS and QoL
scores, and urodynamic parameters at baseline. No patient
had detrusor overactivity.
After 2 wk of treatment, no patients reported voiding
difficulties, high PVR, or UTI. Urine cultures were all
negative.
Sixteen patients were followed for 2 yr. The last 10 cases
had a follow-up of 6 mo. At 1-mo and 3-mo follow-up,
voiding difficulties—namely, hesitancy, a weak or inter-
mittent stream, or high PVR (Table 2)—were not observed.
UTIs did not occur. A marked decrease in OSS symptoms and
problems at 1 and 3 mo was observed (Fig. 2). In addition,
pain intensity, daytime and nighttime voiding frequency,
and QoL decreased significantly, whereas bladder volume to
first pain sensation and maximum cystometric capacity
increased significantly (Table 2). Bladder contractility
ne and after first treatmen.

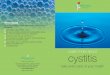
Fig. 3 – Kaplan-Meyer plot for duration of first and second treatment. Thetwo curves overlap in most of their extension (in the first treatments, 10patients currently have only 6-mo follow-up).
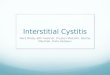
Fig. 5 – Urine concentration (pg/mg) of nerve growth factor (NGF) andbrain-derived neurotrophic factor (BDNF) at baseline and aftertreatment.* = p < 0.05.
E U R O P E A N U R O L O G Y 5 8 ( 2 0 1 0 ) 3 6 0 – 3 6 5 363
index, Qmax, and PVR were not changed (Table 2). At 6-mo
follow-up, 3 of 26 patients requested retreatment. At 9 mo, 4
of 13 patients made the same request. At 12-mo follow-up,
nine patients that reached this visit were retreated.
Considering only the patients followed-up to retreatment
(16 for the first treatment and 16 for the second treatment),
the average duration of clinical improvement was 10.1� 2.4
mo after the first treatment and 10.3 � 2.2 after retreatment.
Sixteen patients were retreated. Before reinjection, OSS
symptom and problem score, VAS, daytime and nighttime
voiding frequency, and QoL were slightly inferior to baseline
values at presentation. Although not accompanied by
hydrodistension, the appearance of the mucosa was similar
to baseline at reinjection cystoscopy. A significant improve-
ment was nevertheless detected in all these parameters at
the 3-mo visit (Table 2). No cases of voiding dysfunction
were reported. Five UTIs were detected. All 16 patients were
observed at the 6-mo visit, and 2 asked for a third BoNTA
injection. At the 9-mo visit, 5 of the 14 remaining patients
Fig. 4 – O’Leary-Sant symptom and problem combined score of all patientsdistributed by tertiles after first and second treatment. A score <14 isfound in normal subjects [11].
also asked for retreatment. At 12 mo, all the remaining nine
patients asked for a third injection (Fig. 3).
OSS applied to normal individuals shows combined
scores below 14 [12]. Using this criteria, all patients had a
combined OSS score below 14 after the first treatment, and
only one had a score above that cut off after the second
treatment (Fig. 4, Table 2).
NGF changed from 16.4 � 11.2 pg/mg at baseline to
2.2 � 2.1, 6.1 � 3.5, and 16.2 � 11.7 pg/mg after 1, 3, and 6 mo,
respectively ( p < 0.05 at first and third months). BDNF
changed from 39.9 � 35.3 to 13 � 9.5, 25.9 � 9.5, and
28.3 � 12.7, respectively, at the same time points ( p < 0.05
at the first month) (Fig. 5). At 1 mo, a strong correlation was
found between the absolute decrease in NGF and BDNF
concentration and the absolute decrease of pain intensity in
the VAS (Fig. 6).
4. Discussion
This work showed that trigonal injection of BoNTA
improved lower urinary tract symptoms, including pain
and frequency, in the entire cohort. More than half the
patients reported symptom improvement during at least
the first 9 mo of treatment. At 1-yr follow-up, all patients
requested retreatment, which was as effective and safe
during a similar period of time. At reinjection, the

Fig. 6 – Correlation between the absolute decrease of urinaryconcentration of nerve growth factor (D NGF) and brain-derivedneurotrophic factor (D BDNF) and absolute decrease of pain intensity (D
VAS; VAS = visual analog scale) at 1-mo follow-up.R2 = multivariate coefficient of determination.
E U R O P E A N U R O L O G Y 5 8 ( 2 0 1 0 ) 3 6 0 – 3 6 5364
cystoscopic appearance of the mucosa was similar to that at
baseline. As interim cystoscopies were not planned, we do
not know whether BoNTA treatment improved mucosa
appearance in parallel with symptom regression.
The trigone contains a dense suburothelial network of
nociceptive fibers [6] that participate in pain generation and
neurogenic inflammation [4,5,13]. This network is mark-
edly increased in BPS/IC patients [14]. BoNTA blocks the
release of neurotransmitters from those fibers [5]. In
addition, BoNTA reduces TRPV1 trafficking from the
cytoplasm to the cell membrane of sensory neurons [15].
As a consequence, a marked analgesic effect of BoNTA can
be expected. BoNTA also decreases adenosine triphosphate
(ATP) release from the bladder [16], providing an additional
explanation for the analgesic effect. ATP is released from
urothelial cells [17,18] and causes pain after binding
purinergic receptors in suburothelial sensory fibers [19].
Urothelium from BPS/IC patients [20] releases more ATP
than control urothelium. The mechanism leading to ATP
release impairment is, however, unclear. Urothelium, in
contrast to sensory nerves, does not express SV2 or SNAP-25
[21], precluding the direct action of BoNTA. Future studies
will elucidate this phenomenon.
BoNTA reduces the urine concentration of NGF [10], a
neurotrophic agent essential for the growth and main-
tenance of a large subset of nociceptors. As NGF has noxious
effects [22], its reduction in the urine can also contribute to
a decrease in bladder pain. The present study confirmed
NGF reduction but added the novel information that BDNF,
another ubiquitous neurothrophin with nociceptive activity
[23], is also decreased upon BoNTA treatment. NGF is
released from urothelial [24] and smooth muscle cells [25],
whereas BDNF immunoreactivity was observed in urothelial
cells [26] and in sensory fibers [23]. The mechanism for
such a decrease is unknown, and any explanation at this
time can be considered only speculative. It is, however,
interesting to observe that whole bladder [10] or trigonal
injections (as done in this study) might cause a similar
neurothrophin decrease. However, this decrease might be
the consequence of sensory fiber concentration in the
trigone.
Previous studies with BoNTA in BPS/IC patients have
reported conflicting results. Giannantoni [7] injected 200 U
of BoNTA in 20 sites in 15 patients. However, only 60 U were
applied in the trigone, helping to explain the short
antinociceptive effect observed. Pain recurred in 73% of
the patients at 5 mo. Kuo et al. [8] injected 100 or 200 U in
40 sites in the posterior and lateral walls, combined with
hydrodistension. Curiously, 71% of the patients still showed
improvement at 6 mo, 55% at 12 mo, and 30% at 24 mo. This
surprisingly long-lasting effect might be attributable to
hydrodistension. However, the treated population might
also differ between the Kuo et al study [8] and this one. Pain
was less intense and occurred at bladder volumes of 150 ml
in the Kuo et al study [8]. In ours, pain appeared at volumes
of <50 ml. Furthermore, no cases of ulcerative disease were
included by Kuo et al. [8]. Thus, patients enrolled in our
study might have had a more severe form of BPS/IC and
therefore responded to BoNTA for shorter periods. The use
of a common classification system such as the ESSIC model
might help in future comparisons [2,27].
Restraining BoNTA to the trigone might have prevented
voiding dysfunction, a result often reported by other studies
that injected the whole bladder [7,8]. As a fixed part of the
bladder, predominantly innervated by sympathetic nerves,
the human trigone does not contract during voiding [28].
Although some BoNTA could have diffused from the trigone
to the lateral walls, in fact, there was no clinical or
urodynamic evidence of poor emptying. Stress urinary
incontinence eventually caused by BoNTA diffusion to
adjacent sphincteric structures did not occur. Although UTIs
were not observed after the first treatment, five patients
developed UTIs after reinjection. This is a concern, as UTIs
might worsen BPS/IC symptoms [29].
The duration of clinical improvement was comparable to
that reported in detrusor overactivity [3,30]. Nevertheless,
BPS/IC being a chronic disease, retreatments are foresee-
able. In patients retreated through the duration of this
study, BoNTA has remained effective. This is an important
consideration for BPS/IC patients, because BoNTA injections
have no curative effect. Although reinjections every 8–10
mo might constitute a major burden to patients and health
systems, detrusor overactivity is being managed cost
effectively with repeated injections for >8 yr [3,30].
5. Conclusions
Trigonal injection of 100 U BoNTA improves BPS/IC
symptoms without significant complications. Reinjections
remain effective. The low number of patients and the lack of

E U R O P E A N U R O L O G Y 5 8 ( 2 0 1 0 ) 3 6 0 – 3 6 5 365
a placebo arm are obvious limitations of this study.
Therefore, placebo-controlled dose-escalating studies are
warranted.
Author contributions: Francisco Cruz had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Dinis, F. Cruz, Pinto.
Acquisition of data: Pinto, Lopes, Frias, J.A. Silva, C.M. Silva.
Analysis and interpretation of data: Pinto.
Drafting of the manuscript: Pinto.
Critical revision of the manuscript for important intellectual content: F. Cruz,
Dinis, C. Cruz.
Statistical analysis: Pinto.
Obtaining funding: Dinis, F. Cruz.
Administrative, technical, or material support: None.
Supervision: Dinis, F. Cruz.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest, including
specific financial interests and relationships and affiliations relevant
to the subject matter or materials discussed in the manuscript
(eg, employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: F. Cruz is a consultant with
Allergan, Astellas, and Recordati.
Funding/Support and role of the sponsor: This work was funded by
INComb FP7 HEALTH project no. 223234 and the Portuguese Association
of Urology.
References
[1] Abrams P, Cardozo L, Fall M, et al. The standardisation of terminol-
ogy of lower urinary tract function: report from the Standardisation
Sub-committee of the International Continence Society. Neurourol
Urodyn 2002;21:167–78.
[2] Van de Merwe JP, Nordling J, Bouchelouche P, et al. Diagnostic
criteria, classification, and nomenclature for painful bladder
syndrome/interstitial cystitis: an ESSIC proposal. Eur Urol 2008;
53:60–7.
[3] Apostolidis A, Dasgupta P, Denys P, et al. Recommendations on the
use of botulinum toxin in the treatment of lower urinary tract
disorders and pelvic floor dysfunctions: a European consensus
report. Eur Urol 2009;55:100–20.
[4] Chuang YC, Yoshimura N, Huang CC, et al. Intravesical botulinum
toxin A administration produces analgesia against acetic acid
induced bladder pain response in rats. J Urol 2004;172:1529–32.
[5] Rapp DE, Turk KW, Bales GT, et al. Botulinum toxin type A inhibits
calcitonin gene-related peptide release from isolated rat bladder. J
Urol 2006;175:1138–42.
[6] Avelino A, Cruz C, Nagy I, et al. Vanilloid receptor 1 expression in the
rat urinary tract. Neuroscience 2002;109:787–98.
[7] Giannantoni A, Porena M, Costantini E, et al. Botulinum A toxin
intravesical injection in patients with painful bladder syndrome:
1-yr follow-up. J Urol 2008;179:1031–4.
[8] Kuo HC, Chancellor MB. Comparison of intravesical botulinum toxin
type A injections plus hydrodistension with hydrodistension alone
for the treatment of refractory interstitial cystitis/painful bladder
syndrome. BJU Int 2009;1:1–5.
[9] Karsenty G, Elzayat E, Delapparent T, et al. Botulinum toxin type A
injections into the trigone to treat idiopathic overactive bladder do
not induce vesicoureteral reflux. J Urol 2007;177:1011–4.
[10] Liu HT, Tyagi P, Chancellor MB, et al. Urinary nerve growth factor
level is increased in patients with interstitial cystitis/bladder pain
syndrome and decreased in responders to treatment. BJU Int
2009;104:1476–81.
[11] Nordling J, Anjum FH, Bade JJ, et al. Primary evaluation of patients
suspected of having interstitial cystitis (IC). Eur Urol 2004;45:
662–9.
[12] O’Leary MP, Grannum RS, Floyd JF, et al. The Interstitial Cystitis
Symptom Index and Problem Index. Urology 1997;49:58–63.
[13] Dinis P, Charrua A, Avelino A, et al. Intravesical resiniferatoxin
decreases spinal c-fos expression and increases bladder volume
to reflex micturition in rats with chronic inflamed urinary bladders.
BJU Int 2004;94:153–7.
[14] Mukerji G, Yiangou Y, Agarwal SK, et al. Transient receptor potential
vanilloid receptor subtype 1 in painful bladder syndrome and its
correlation with pain. J Urol 2006;176:797–801.
[15] Morenilla-Palao C, Planells-Cases R, Garcıa-Sanz N, et al. Regulated
exocytosis contributes to protein kinase C potentiation of vanilloid
receptor activity. J Biol Chem 2004;279:25665–72.
[16] Khera M, Somogyi GT, Kiss S, et al. Botulinum toxin A inhibits ATP
release from bladder urothelium after chronic spinal cord injury.
Neurochem Int 2004;45:987–93.
[17] Birder LA, Barrick SR, Roppolo JR, et al. Feline interstitial cystitis
results in mechanical hypersensitivity and altered ATP release from
bladder urothelium. Am J Physiol Renal Physiol 2003;285:423–9.
[18] Charrua A, Reguenga C, Cordeiro JM, et al. Functional transient
receptor potential vanilloid 1 is expressed in human urothelial
cells. J Urol 2009;182:2944–50.
[19] Cockayne DA, Hamilton SG, Zhu QM, et al. Urinary bladder hypore-
flexia and reduced pain-related behaviour in P2X3-deficient mice.
Nature 2000;407:1011–5.
[20] Sun Y, Keay S, De Deyne PG, et al. Augmented stretch activated
adenosine triphosphate release from bladder uroepithelial cells in
patients with interstitial cystitis. J Urol 2001;166:1951–6.
[21] Coelho A, Dinis P, Pinto R, et al. Distribution of the high-affinity
binding site and intracellular target of botulinum toxin type A in
the human bladder. Eur Urol 2010;57:884–90.
[22] Dyck PJ, Peroutka S, Rask C, et al. Intradermal recombinant human
nerve growth factor induces pressure allodynia and lowered heat–
pain threshold in humans. Neurology 1997;48:501–5.
[23] Merighi A, Salio C, Ghirri A, et al. BDNF as a pain modulator. Prog
Neurobiol 2008;85:297–317.
[24] Koltzenburg M, Torebjork HE. Pain and hyperalgesia in acute
inflammatory and chronic neuropathic conditions. Lancet 1995;
345:1111.
[25] Clemow DB, Steers WD, Tuttle JB. Stretch-activated signaling of
nerve growth factor secretion in bladder and vascular smooth
muscle cells from hypertensive and hyperactive rats. J Cell Physiol
2000;183:289–300.
[26] Pinto R, Frias B, Allen S, et al. Sequestration of BDNF by intravenous
delivery of TrkB-Ig2 reduces bladder overactivity and noxious input
in animals with chronic cystitis. Neuroscience 2010;166:907–16.
[27] Fall M, Oberpenning F, Peeker R. Treatment of bladder pain syn-
drome/interstitial cystitis 2008: can we make evidence-based
decisions? Eur Urol 2008;54:65–78.
[28] Shafik A. Role of the trigone in micturition. J Endourol 1998;12:
273–7.
[29] Warren JW, Brown V, Jacobs S, et al. Urinary tract infection and
inflammation at onset of interstitial cystitis/painful bladder
syndrome. Urology 2008;71:1085–90.
[30] Del Poppolo G, Filocamo MT, Li Marzi V, et al. Neurogenic detrusor
overactivity treated with English botulinum toxin A: 8-yr experi-
ence of one single centre. Eur Urol 2008;53:1013–20.