-
7/28/2019 Case History Surgery Chole Cystitis
1/23
First Moscow State Medical University
MEDICAL FACULTY
Division of Foreign Students with Instruction Conducted in
English
Department of Surgery
CASE HISTORY
By Mardiana Kamal
Medical Faculty, English Medium, Group 93
Supervisor: , MD PhD
MOSCOW 2012
-
7/28/2019 Case History Surgery Chole Cystitis
2/23
Personal data of the patient
Name :
Age : 80 years old
Date of birth : 11.11.1931
Sex : Female
Weight : 60 kg
Height : 156 cm
Occupation : Pensioner
Marital status : Married
Department : Surgery
Date of Admission : 11.03.2012
COMPLAINTS
The patient complained of feeling heaviness in region of under
right costal arc, periodically appeared
pain after eating fatty food.
ANAMNESIS MORBIThe patient, , was admitted to the 79th Hospital
on 11.03.2012 with the
complaints of feeling heaviness in region of in region of under
right costal arch, already 5 years. On the
same day, she went to the polyclinic, was asked to go to the
hospital and she was admitted.
Investigations were performed: Ultrasound investigation of
abdominal cavity revealed concrement in
gall bladder.
ANAMNESIS VITAE
Anamnesis familiae
The patient is widowed and has 1 child. Her daughter was also
admitted to the hospital two years ago
with the same complaints.
Physical abnormalities: The patient grew normally without any
physical abnormality.
Previous medical history
The patient had never been admitted to any hospitals before.
Although, she has diagnosed previous
case of ARVI, Ischemic Heart Disease, Arterial Hypertension, and
Chronic Obstructive Pulmonary
Disease. No information on usage of medical preparations.
Epidemiological anamnesis: She does not have any current
infection. She seldom has tonsilits.
Harmful habits: Patient does not smoke or drink
Previous blood transfusion: Patient had previous no blood
transfusion
Allergic history: There is no known allergy in this patient.
STATUS PREASENS
The patients condition is satisfactory. She is well and alert.
She is coherent and fluent.
-
7/28/2019 Case History Surgery Chole Cystitis
3/23
CONSTITUTION
The patient had a normal constitution.The external features of
the body correlates to her age.
POSTURE
The patient was normal and active. She did not have any
discomfort during inspection and was not
assuming a forced position.
Height 1.56 m, weight 60kg.
BMI = 23 - normal
SKIN
The patient got a clear pink skin. There were no
hyperpigmentations of the skin. The skin was evenly
colored with no jaundice. There were no abnormal discolorations
of the mucous membranes. The skin of
the patient was dry.
SUBCUTANEOUS FAT
Patients subcutaneous fats are uniformly distributed. There is
no excessive fat accumulation. Wasting
was also not noticed in this patient.
EDEMA
No edema was visible in this patient. The eye lids appear normal
with no narrowing of the slits. The
patients ankle and legs were checked and there was no pitting
edema. Acsites was absentand no
generalized form of edema was found in this patient
(anasarca).
LYMPH NODES
Regions Visual inspection Palpation Characters
Submandibular Not visible Palpable, not enlarged
(0.5cm)
Mobile without
skin attachment
Cervical Not visible Palpable, not enlarged(0.5cm)
Mobile withoutskin attachment
Supraclavicular Not visible Not palpable -
Axillary Not visible Palpable, not enlarged
(0.5cm)
Mobile without
skin attachment
MUSCULAR SYSTEM
There were no local atrophies of the skeletal musculature
observed in this patient. There was no
functional skeletal muscle dysfunction (cramps).
BONESThe bones of the skull, chest, spine and extremities were
normal without any abnormal bulge or
deformities. Patients general bone configuration is normal.
There is no abnormal growth or elongation
(gigantism) of the patients bone structures.
-
7/28/2019 Case History Surgery Chole Cystitis
4/23
RESPIRATORY SYSTEM
Inspection of the chest
The patient was examined in an upright sitting position in her
room. The patients clavicles and the
shoulder blades are at the same level and the supra-clavicular
fossa and the sub-clavicular are equally
pronounced on each sides.
Respiratory movements:
The respiratory movements of the patient were normal since the
patient was not assuming a forced
position and there was no evidence of involvement of the
accessory respiratory muscles.
Respiratory type: The respiratory type was thoraxic
breathing.
Respiratory rate: 15 breaths per minute.
Respiratory rhythm: Rhythmic of uniform depth and equal length
of the inspiration and expiration.
Constitution: The patient had a normostenic constituition. The
costal angle is not more than 90 degrees.
Pain and tenderness:
Pain and tenderness (both local and diffuse) are absent in the
patients thoracic region.
Elasticity (resilience):
The patients chest is of normal decreased elasticity.
Vocal fremitus:Vocal fremitus normal in this patient. The vocal
fremitus was about the same intensity with no changes
in symmetrical parts of the thoracic cavity.
Percussion of the chest:
Comparative percussion:
Pulmonic sound with an admixture of tympani. The so-called
hyper-resonant sound is heard in
symmetrical points of patients thoracic cavity.
Topographic percussion:
Upper borders of the lungs:
Borders of the lungs Right lung Left lung
Upper anterior border 3 cm above the clavicle 3 cm above the
clavicle
Upper posterior border Spinous process of the 7th
cervical vertebra
Spinous process of the 7th
cervical vertebra
Kroenigs area normal normal
The lower borders of the lungs:
Topographic lines Right lung Left lung
Linea parasternalis 5th
intercostals space -
Linea midclavicularis 6th
rib -
Linea axillaris anterius 7th rib 7th rib
Linea axillaries medius 8th rib 8th rib
-
7/28/2019 Case History Surgery Chole Cystitis
5/23
Linea axillaris posterius 9th rib 9th rib
Linea scapularis 10th rib 10th rib
Linea paraspinalis Spinous process of the 11th
thoracic vertebra
Spinous process of the 11th
thoracic vertebra
Mobility of the lower lung borders:
Mobility of the lower lung borders are without any
peculiarities, with normal parameters.
Auscultation of the lungs:
Vesicular breathing:
The patient had clear vesicular breathing with normal
inspiration and expiration phases.
Bronchial breathing:
Bronchial breathing is heard over the larynx, and trachea.
Bronchophony:
Normal bronchophony. The loud whispering voice of the patient is
audible on both side of the chest in
symmetrical points.
CARDIOVASCULAR SYSTEM
General inspection of the cardiovascular system:
Patient appears calm with no signs of breathlessness, anxiety or
discomfort.
Examination of the neck region:
No carotid shudder is felt.
Neck veins are not visible.
Arterial blood pressure: 140/80 mmHg
Pulse Rate : 78 beat per minute
Palpation of the apex beat: Apex beat in this patient was not
palpable.
Palpation of the pulse:
Carotid artery:
- Pulse not visible, but felt- Regular pulse with regular
resistance and strengthAxillary artery:
- Pulse not visible, but felt- Regular pulse with regular
resistance and strengthInguinal artery:
- Pulse not visible, but felt- Regular pulse with regular
resistance and strengthPopliteal artery:
- Pulse not visible, but felt- Regular pulse with regular
resistance and strengthTibialis posterior:
- Pulse not visible, but felt- Regular pulse with regular
resistance and strengthDorsalis pedis:
- Pulse not visible, but felt- Regular pulse with regular
resistance and strength
-
7/28/2019 Case History Surgery Chole Cystitis
6/23
Palpations of apex beat: palpated 2cm medial to the left
midclavicular line.
Auscultation:
Points S1 S2 S3 S4
1st
point Normal Normal _ _
2nd point Normal Normal _ _
3rd point Normal Normal _ _
4th point Normal Normal _ _
Botkin-erbs point Normal Normal _ _
Auscultatory findings: No pathologies were found
Percussion of the heart:
Relative heart dullness:
Relative borders of the heart Dullness levels
Right border 3 cm laterally to the right edge of the
sternum
Left border 1 cm medially from the midclavicular line
Upper border 3rd
intercostals space
Absolute heart dullness:
Absolute borders of the heart Dullness levels
Right border Left edge of the sternum
Left border 1 cm from the relative heart dullness
Upper border 4th
intercostals space
Configuration of the vascular bundle:
The configuration of the vascular bundle is without any
peculiarities.
Configuration and assessment (shape) of the heart dullness:The
heart dullness is relatively normal with no mitral or aortic
(so-called sitting duck or boot shaped)
configuration of the heart dullness.
-
7/28/2019 Case History Surgery Chole Cystitis
7/23
URINARY SYSTEM
Inquiry:
Patient had no complains. She has no pain or any discomfort in
her lumbar region. The patients
micturation is normal with no pain of discomfort during this
process.
Physical examination:
Inspection:
There are no physical signs of fetor uremicus. There is no
abnormal swelling or protrusion in the
patients loin region.
Palpation:
The kidneys were impalpable. No tenderness over renal
ENDOCRINE SYSTEM
Physical examination:
Inspection:
Patients general outlook does not indicate any endocrinal
abnormalities.Patients mental and
emotional state was normal. Her sleeping patterns have not
changed.
CENTRAL NERVOUS SYSTEM
Inquiry:
Consciousness : conscious and alert
Headache : absent
Dizziness : absent
Sleeping disorders : absent
Memory status : Normal
STATUS LOCALIS (Digestive system)
Physical examination of the gastrointestinal tract:
Inspection:The general appearance of the patient is satisfactory
and there is no evidence of poor nutritional state
or cachexia.
Oral cavity: no foul smell or any other unpleasant odor.
State of the teeth : no cavities were present.
State of the gums: pink color without hemorrhages, no ulceration
and no purulent inflammation.
State of the tongue: the tongue is clean and moist with visible
papillae.
Palpation of the Stomach: soft, without pain
Schutkin-Blumberg sign : Negative
Peritoneal signs : Negative
Ortner sign : Negative
Auscultation : normal bowel sounds
-
7/28/2019 Case History Surgery Chole Cystitis
8/23
LIVER AND THE GALL BLADDER
Physical examination:
The inspection was carried out during the day in a room with
proper light settings. The habitusof the patient was normal. No
icteric of the sclera. Normal pinkish colour of all parts of the
tongue,
palms and soles.
Skin:
No abnormal discoloration of the skin. Few scratch marks were
revealed during inspection. No hemorrhagic diathesis. No spider
angiomatas.Percussion of the liver:
Topographic lines Superior liver borders Inferior liver
borders
Linea axillaris anterior
dextra
7th rib 10th rib
Linea midclavicularis dextra 6th rib Arcus costalis
Linea parasternalis dextra Superior edge of the 6th
rib 2 cm below the interior
edge of the right costal arch
Lines mediana anterior _ 3 cm below the base of the
xiphoid process
The left border of the liver dullness was on the linea
parastenalis sinistra.
Palpation of the liver and gallbladder:
Palpation of the liver: Palpation was not performed due to
post-operative drainage at right hypogastric
region.
Gall bladder
Murphys sign Negative
Otners sign Negative
Georgivsky- de musses sign Negative
Spleen
Palpation of the Spleen:
The spleen was impalpable.
Percussion of the spleen:
Axis Measurements
Transverse axis 5.5 cm
Long axis 7 cm
-
7/28/2019 Case History Surgery Chole Cystitis
9/23
PRESUMPTIVE DIAGNOSIS
Chronic Cholecystitis.
Methods of investigations
Common blood count Biochemical blood test Common urine test
Prothrombin index HBs Ag, antiHCV, HIV test Ultrasound examination
Oesophagogastroduodenoscopy ECGInstrumental and laboratory
methods
General analysis of the blood
Date of the sample: 13.03.2012
Parameters Obtained results
WBC 11.1 10^9 /l
RBC 4.21 10^12 /l
HGB 116 g/l
Hematocrit 37.4
Platelet 182 10^9/l
Mean Corpuscular Volume 89 fl
Mean Corpuscular Hemoglobin 27.5 pg
MCHC 311 g/l
Lymphocyte 26 %
Monocyte 6 %
Granulocyte 69 %
Biochemical Analysis of the Blood
Date: 13.03.2012
Parameters Results
Total Protein 63 g/l
Albumin 38g/l
Urea 6.3 mmol/l
Total bilirubin 9.9 micromol
Iron 6.6 mmol.l
Creatinine 101.1 micromol/l
Cholesterin 6.1 mmol/l
Tryglyceride 1.04 mmol/l
-
7/28/2019 Case History Surgery Chole Cystitis
10/23
AST 46 E/l
ALT 38 E/l
a-Amylase 27 E/l
Alkaline Phosphotase 160 E/l
Glucose 4.1 mmol/l
General analysis of patients urine sample
Date of sample: 14.09.2011
Properties Results
Color yellow
Transparency clear
Urine pH 6.0 - acidic
Reactivity to blood negative
Protein 0.5 g/l
Ketone body 4 mmol/l
Bilirubin Pigments 8.5 umol/l
Urobilin 34 umol/l
Leucocytes 250 Leu/uL
Prothrombin index (13.03.2012) : 84%
HBs Ag test : Negative
antiHCV test : Negative
HIV test : Negative
ULTRASONOGRAPHY INVESTIGATIONSDate 11.03.2012
Concrement in gall bladder. Chronic calculous cholecystitis,
bile duct not dilated.
Date : 13.03.2012
Separated from subdiaphragmatic peritoneum on the right and
left, obstructive, near the spleen in the
lateral left and right canals. In pelvic cavity, no
peculiarities identified.
Intrahepatic bile ducts are not dilated. In region of
gallbladder, fluid delineated structures are not
identified. Hepaticocholedochus : 5.5 6mm
Liver:Parenchyma : Changed
Focal changes : None
Intrahepatic duct : Poor
Gallbladder:
Deformed, Size increased, wall is without changes. Contents are
non-homogenous. Palpation in region
of gallbladder is without pain. Common bile duct is without
changes.
-
7/28/2019 Case History Surgery Chole Cystitis
11/23
Pancreas:
Normal value, not dilated, no focal changes
Spleen :
No significant changes
Conclusion : Cholelithiasis. Chronic Calculous
Cholecystitis.
ENDOSCOPIC INVESTIGATIONS
Esophagogastroduodenoscopy:
Date: 12.09.2011
Patients throat was anesthetized with 10 % of lidocaine. There
was no obstacle in the passage of the
fiberscope. The esophageal lumen was free. The opening at the
esophagealgastric junction not
deformed. Mucosa is pale-pink. There are no pathogenic changes
in the esophagus. Cardiac sphincter
does not close completely. Evacuation from oesophagus is normal.
Empty stomach with mucous. Folds
in normal form, during insufflation of air expanded
satisfactorily. Peristalsis symmetrical. Mucosal focal
hyperaemia. Angle of stomach, antral part without peculiarities.
Evacuation is normal. Duodenum iswithout peculiarities. Mucosal
layers is without defect. Postbulbar part is normal.
Conclusion : Chronic Gastroduodenitis
ELECTROCARDIOGRAPHIC INVESTIGATIONS
Sinus rhythm with no signs of current attact of coronary heart
disease.
CLINICAL DIAGNOSIS
Chronic Calculous Cholecystitis
LAPAROSCOPIC CHOLECYSTECTOMY
Under endotracheal anaesthasia, impositioned pneumoperitoneum
and administrated trocar in typical
points.
Video revision : No effusion in peritoneal cavity. Gall bladder
normal size. Wall is thickened, fused and
sealed to duodenum. Bile duct is visually not dilated. Fusion is
dissected, removed bladder duct and
artery, clipping and separately crossed. Bladder is separated
from position with coagulation after.
Hemostasis in course of operation. Bladder is extracted from
peritoneal cavity through paraumbilical
puncture. Peritoneal cavity drained. Removed pneumoperitoneum.
Suture on punctures.
MEDICATION
1. Ketorol 1.0 / D2. Ceftriaxone 1.0 2x/D3. Analgia 50% 2.0 (if
pain arises)
-
7/28/2019 Case History Surgery Chole Cystitis
12/23
CONCLUSION
The patient was diagnosed with chronic calculous
cholecystitis.
The diagnosis in this patient was confirmed through instrumental
investigation by ultrasonography of
the right hypochondriac region. Diagnosis was also achieved with
relation to patients symptom of
feeling heaviness in region under costal arch.
During ultrasonography on 11.03.2012, concrement in gall bladder
was revealed. Chronic
calculous cholecystitis was the presumptive diagnoses. During
ultrasonography on 13.03.2012, signs of
Intrahepatic bile ducts are not dilated. In region of
gallbladder, fluid delineated structures are not
identified. Hepaticocholedochus : 5.5 6mm. The was also an
increase of urobilin in her urine test.
Patients with choledocholithiasis may be completely
asymptomatic; symptoms occur
when the stones obstruct the CBD. The ultrasonography confirmed
the diseases.
In the hospital, the patient had undergone laparoscopic
cholecystectomy under
anesthesia as treatment.
DIFFERENTIAL DIAGNOSIS
Acute gastritis Amoebic hepatic abcess Appendicitis Biliary
colic Cholangitis Cholangiocarcinoma Acute pancreatitis
Nephrolithiasis Gastric ulcer Peptic ulcer disease
-
7/28/2019 Case History Surgery Chole Cystitis
13/23
CHRONIC CALCULOUS CHOLECYSTITIS
Chronic cholecystitis is gallbladder
inflammation that has lasted a long time. It
almost always results from gallstones. It is
characterized by repeated attacks of pain
(biliary colic). In chronic cholecystitis, the
gallbladder is damaged by repeated attacks of
acute inflammation, usually due to gallstones,
and may become thick-walled, scarred, and
small. The gallbladder usually contains sludge
(microscopic particles of materials similar to
those in gallstones) or gallstones that block its
opening into the cystic duct or reside in the
cystic duct itself.
PATHOPHYSIOLOGY
Gallstones result from supersaturation of cholesterol in the
bile, which acts as an irritant, producing
inflammation in the gallbladder, and which precipitates out of
bile, causing stones. Risk factors include
gender (women four times as like to develop cholesterol stones
as men), age (older than age 40),
multiple parity, obesity, use of estrogen and
cholesterol-lowering drugs, bile acid malabsorption with GI
disease, genetic predisposition, rapid weight loss. Pigment
stones occur when free bilirubin combines
with calcium. These stones occur primarily in patients with
cirrhosis, hemolysis, and biliary infections.
Acute cholecystitis is caused primarily by gallstone obstruction
of the cystic duct with edema,
inflammation, and bacterial invasion. It may also occur in the
absence of stones, as a result of major
surgical procedures, severe trauma, or burns.
Chronic cholecystitis results from repeated attacks of
cholecystitis, presence of stones, or chronic
irritation. The gallbladder becomes thickened, rigid, fibrotic,
and functions poorly.
-
7/28/2019 Case History Surgery Chole Cystitis
14/23
CLINICAL PRESENTATION
Recurrent episodes of biliary pain in the right upper abdomen,
sometimes in epigastrium, often with
irradiation to the right scapular region. Biliary pains may be
in the right hypochondrium, frequently or
occasionally, of different intensity and duration, related to
intake of fatty meals.
1. In addition, a biliary pain may occur with one or more of the
following symptoms:a. regular or periodical feeling of bitter
tasteb. nausea, sometimes vomitingc. regular or periodical
abdominal bloating and borborygmusd. unstable stool with
constipation or diarrhea prevailing2. Impaired gallbladder
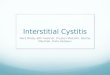
emptying.3. According to ultrasound examination, thickening of the
gallbladder wall up to 3-4 mm and presenceof gallstones in the
gallbladder lumen.
-
7/28/2019 Case History Surgery Chole Cystitis
15/23
Chronic cholecystitis on ultrasonography
MEDICATION
For acute cholecystitis, initial treatment includes bowel rest,
intravenous hydration, analgesia, and
intravenous antibiotics. For mild cases of acute cholecystitis,
antibiotic therapy with a single broad-
spectrum antibiotic is adequate.
The current Sanford guide recommendations include
piperacillin/tazobactam (Zosyn, 3.375 g IV q6h or 4.5 g IV q8h),
ampicillin/sulbactam (Unasyn, 3 g IV q6h), or meropenem (Merrem, 1
g IV q8h).In severe life-threatening cases, the Sanford Guide
recommends
imipenem (500 mg IV q6h) third-generation cephalosporin plus
Flagyl (1 g IV loading dose followed by 500 mg IV q6h).Pathogenetic
treatment of patients with chronic calculous cholecystitis
Accordingly, treatment of chronic calculous cholecystitis (with
biliary pain) aiming for prophylactics of
the acute calculous cholecystitis, duodeno-gastral reflux,
antral atrophic (bile-acid-dependent) gastritis
and chronic biliary pancreatitis includes:
1. Celecoxib - 100 mg, 2 times a day after meal for 5-7 days,
after which2. Ursodeoxycholic acid - 750 mg, once a day (in the
evening) for 3 month.Celecoxib is a selective inhibitor of COX-2.
Inhibiting COX-2 activity in the smooth muscle cells of
thegallbladder wall and cystic duct it brings relief of the biliary
pain within 3-5 days, restoration of the
evacuation function of the gallbladder and the
gallbladder-dependent output of biliary cholesterol,
active and passive passage of the hepatic bile into the
gallbladder, and decrease in the gallbladder-
independent enterohepatic circulation of bile acids, biliary
cholesterol and biliary bilirubin.
Celecoxib, a selective inhibitor of COX-2, inhibiting COX-2
activity in the epithelial cells of the gallbladder
mucosa causes inhibition of the glycoprotein mucin
hypersecretion into the gallbladder lumen,
-
7/28/2019 Case History Surgery Chole Cystitis
16/23
concentration of glycoprotein biliary mucin in gallbladder bile
and viscosity of gallbladder bile, which
prevents formation of biliary sludge.
Low COX-2 activity in the epithelial cells of the gallbladder
mucosa helps restoring the absorption
function of the gallbladder (absorption of water and biliary
cholesterol from phospholipid vesicles),
which results in increase of concentration of total bile acids
and decrease of concentration of biliary
cholesterol in the gallbladder bile. Also, low COX-2 activity in
the epithelial and smooth muscle cells of
the gallbladder infundibulum helps lowering the risk of
development of acute calculous cholecystitis.
Ursodeoxycholic acid, is a hydrophilic hepatoprotective bile
acid. It helps in dissolving the cholesterol
monohydrate crystals in the gallbladder, decrease of
lithogenicity of gallbladder and hepatic bile,
disappearance of the chronic bland intrahepatic cholestasis
(i.e. results in the restoration of the
accumulation and excretion functions of liver) and in some
patients helps in dissolving cholesterol
gallstones.
Celecoxib and Ursodeoxycholic acid, blocking main pathogenetic
mechanisms of gallstones formation,
help in slowing down the growth of cholesterol gallstones and
lower the risk of acute calculous
cholecystitis. In some patients the chronic calculous
cholecystitis can transfer into the gallstone disease(without
biliary pain) or the silent gallstones group.
Estimated effectiveness is 95%.
Remission period is 18-24 months.
Contraindications for Celecoxib:
allergic reactions (nettle-rash, bronchial spasm) to
acetylsalicylic acid or other NSAIDs (inanamnesis);
3rd trimester of pregnancy; high sensitivity to sulphonamides;
high sensitivity to any component of the
preparation.Contraindications for Ursodeoxycholic acid: high
sensitivity to the preparation; acute inflammatory diseases of the
gallbladder and the bile ducts; ulcerative colitis; Crones
disease.
MANAGEMENT
Patients should be fasted, rehydrated with intravenous fluids,
and given oxygen therapy and adequate
analgesia. Indometacin (25 mg three times daily for a week) can
reverse the inflammation of the gallbladder and the contractile
dysfunction seen in the early stages (first 24 hours) of
cholecystitis. The
prokinetic action of indometacin will also improve postprandial
emptying of the gall bladder in patients
with gallbladder disease. A single intramuscular dose of
diclofenac (75 mg) may substantially decrease
the rate of progression to acute cholecystitis in patients with
symptomatic gall stones.Because of the
risk of superimposed infection, intravenous antibiotics should
be started empirically if the patient has
systemic signs or if no improvement is seen after 12-24 hours. A
second generation or newer
cephalosporin should be used (for example, cefuroxime 1.5 g
every 6-8 hours) with metronidazole (500
-
7/28/2019 Case History Surgery Chole Cystitis
17/23
mg every 8 hours). Non-operative managementsolvent dissolution
therapy or extracorporeal
shockwave lithotripsyhas been used with variable results to
treat chronic cholecystitis in patients unfit
for surgery, but it has no place in the management of acute
cholecystitis.
TREATMENT
For patients with symptomatic gallstones and suspected common
bile duct stones, either preoperative
endoscopic cholangiography or an intraoperative cholangiogram
will document the bile duct stones. If
an endoscopic cholangiogram reveals stones, sphincterotomy and
ductal clearance of the stones is
appropriate, followed by a laparoscopic cholecystectomy. An
intraoperative cholangiogram at the time
of cholecystectomy will also document the presence or absence of
bile duct stones.
Laparoscopic
common bile duct exploration via the cystic duct or with formal
choledochotomy allows the stones to be
retrieved in the same setting (see Choledochal Exploration). If
the expertise and/or the instrumentation
for laparoscopic common bile duct exploration are not available,
a drain should be left adjacent to the
cystic duct and the patient scheduled for endoscopic
sphincterotomy the following day. An open
common bile duct exploration is an option if the endoscopic
method has already been tried or is, for
some reason, not feasible. If a choledochotomy is performed, a T
tube is left in place. Stones impacted in
the ampulla may be difficult for both endoscopic ductal
clearance as well as common bile duct
exploration (open or laparoscopic). In these cases the common
bile duct is usually quite dilated (about 2
cm in diameter). A choledochoduodenostomy or a Roux-en-Y
choledochojejunostomy may be the best
option under this circumstance.
-
7/28/2019 Case History Surgery Chole Cystitis
18/23
OPERATIVE APPROACH
Surgery is indicated if the patient's condition deteriorates or
when generalised peritonitis or
emphysematous cholecystitis is present. These features suggest
gangrene or perforation of the gall
bladder.
Cholecystectomy
Patients with cholecystitis who undergo early laparoscopic
cholecystectomy (before symptoms have
lasted 72-96 hours) have lower complication rates and lower
conversion rates than open
cholecystectomy and shorter hospital stays than those undergoing
interval surgery.
Surgery for cholecystitis also has a lower conversion rate than
delayed surgery (which is
performed during the index admission after conservative
management and after symptoms have lasted
3-5 days). Early surgery also avoids complications when
conservative treatment fails. A long time
between onset of symptoms and presentation is associated with
advanced disease.
Early laparoscopic surgery is safe and feasible in patients with
acute or chronic cholecystitis. If early
interventionless than 72 hours after symptoms startedcan be
achieved, oedema planes present
during this period allow the gall bladder to be dissected
laparoscopically. Although it is desirable tooperate within this
time period, it is often difficult to do so in clinical practice.
By the time inflammation
has been present for more than 72 hours, features of chronic
inflammation (such as fibrosis)
predominate and make it more difficult to dissect the gall
bladder.
Contraindications for laparoscopic cholecystectomy include the
following:
High risk for general anesthesia Morbid obesity Signs of
gallbladder perforation, such as abscess, peritonitis, or fistula
Giant gallstones or suspected malignancy End-stage liver disease
with portal hypertension and severe coagulopathy
-
7/28/2019 Case History Surgery Chole Cystitis
19/23
-
7/28/2019 Case History Surgery Chole Cystitis
20/23
Percutaneous cholecystostomy
Percutaneous cholecystostomy is a minimally invasive procedure
that can benefit patients with serious
comorbidity who are at high risk from major surgery.
Percutaneous cholecystostomy can be performed
at the bedside under local anaesthetic and is suitable for
patients in intensive care units and those with
burns. It is the definitive treatment in patients with
acalculous cholecystitis or it may be used as a
temporising measureto drain infected bile and delay the need for
definitive treatment.
Percutaneous cholecystostomy. A pigtail catheter has been placed
through the abdominal wall, the right
lobe of the liver, and into the gallbladder.
-
7/28/2019 Case History Surgery Chole Cystitis
21/23
Percutaneous cholecystostomy gives clinical improvement in about
three quarters of patients. Mortality
after this procedure is related to comorbidity (for example,
pneumonia or myocardial infarction) or pre-
existing sepsis. An incomplete or poor response to
cholecystostomy within the first 48 hours may
indicate causes of sepsis other than cholecystitis, inadequate
antibiotic coverage, possible complications
(such as dislodgement of the drainage tube), or necrosis of the
wall of the gall bladder.
Patients can undergo cholecystectomy after percutaneous
cholecystostomy. In patients unfit to be given
a general anaesthetic, the drain can be left in place for more
than six weeks to allow radiological
extraction of calculi at a later date.
Risks
The overall risk of laparoscopic gallbladder surgery is very
low. The most serious possible complicationsinclude:
Infection of an incision. Internal bleeding. Injury to the
common bile duct. Injury to the small intestine by one of the
instruments used during surgery. Risks of general
anesthesia.Recovery is much faster and less painful after
laparoscopic surgery than after open surgery.
The hospital stay after laparoscopic surgery is shorter than
after open surgery. People generally gohome the same day or the
next day, compared with 2 to 4 days or longer for open surgery.
Recovery is faster after laparoscopic surgery. You will spend
less time away from work and other activities after laparoscopic
surgery (about 7 to10 days compared with 4 to 6 weeks).
-
7/28/2019 Case History Surgery Chole Cystitis
22/23
POSTCHOLECYSTECTOMY SYNDROME
Postcholecystectomy syndrome sometimes occurs when abdominal
symptoms develop after surgery to
remove the gallbladder(cholecystectomy). Between 5% and 40% of
people who have
thegallbladder removed may experience this syndrome.
Symptoms of postcholecystectomy syndrome may include: Upset
stomach, nausea, and vomiting. Gas, bloating, and diarrhea.
Persistent pain in the upper right abdomen You can ease diarrhea by
taking the medicine cholestyramine. If pain continues, you may have
a problem caused by something other than the gallbladder ora
gallstone. Other possible causes of abdominal pain include
irritable bowel syndrome, stomach (peptic)
ulcers, pancreatitis, or abdominal pain from an unknown
cause.
COMPLICATIONS
(1) Gangrenous cholecystitisGangrenous cholecystitis occurs in
2-30% of cases of acute cholecystitis. Men aged over 50 with a
history of cardiovascular disease and leucocytosis (>17 000
leucocytes/ml) have the highest risk of
gangrene of the gall bladder.Gangrene occurs most commonly at
the fundus because the vascular
supply often becomes compromised. Urgent laparoscopic
cholecystectomy should be considered in
patients at high risk of gangrene, and the surgeon should have a
low threshold for conversion to open
cholecystectomy during the procedure.
(2) Gallbladder perforationThe gall bladder is perforated in 10%
of cases of acute cholecystitisusually in patients who sought
medical attention after a delay or in those who do not respond
to conservative management.
Perforation most commonly occurs at the fundus. After the gall
bladder has perforated, patients may
experience transient relief of their symptoms because the gall
bladder decompresses, but peritonitis
then develops.
Free perforation presents with generalised biliary peritonitis
and is associated with a mortality of 30%.
Localised perforation, with the formation of pericholecystic
abscesses, is more common, because the
adherent viscera adjacent to the perforation tend to localise
spillage of the contents of the gall bladder.
A mass may be palpable in patients with localised perforation,
and computed tomography is the most
useful investigation.
(3) Cholecystoenteric fistulasAn acutely inflamed gall bladder
may create a cholecystoenteric fistula by adhering to and causing
aperforation in other parts of the gastrointestinal tract. The most
common sites for fistulas are the
duodenum and the hepatic flexure of the colon. Decompression of
the gall bladder because of a fistula
may cause resolution of the acute cholecystitis. Air in the
biliary tree (pneumobilia) can be seen on
abdominal radiographs, and imaging enhanced with contrast agents
may show fistulas.
(4) Gallstone ileusGallstone ileusobstruction of the small
intestine caused by a gall stone passing from the biliary tract
into the intestinal tract through a fistulashould be considered
in elderly patients with no obvious
-
7/28/2019 Case History Surgery Chole Cystitis
23/23
cause for the intestinal obstruction. Patients may not have a
history of cholecystitis. Mortality (15-20%)
is attributed to delays before surgery is performed or to
coexisting medical illnesses. Classic findings on
abdominal radiographs include pneumobilia, intestinal
obstructions, and gall stones in unusual sites.
PROGNOSIS
For uncomplicated cholecystitis, the prognosis is excellent,
with a very low mortality rate. In patients who are critically ill
with cholecystitis, the mortality rate approaches 50-60%,
especially inthe setting of gangrene or empyema.
Once complications such as perforation/gangrene develop, the
prognosis becomes less favorable. Inpatients who are critically ill
with acalculous cholecystitis and perforation or gangrene, the
mortality rate
can be as high as 50-60%.
TREATMENT FOR PATIENT
Laparoscopic cholecystectomy was done to remove inflamed
choledocus. It was successful to stop
patients complaints and to prevent complications in the
future.
POSTOPERATIVE PERIOD
Patient spent his post-operative period in the surgical ward.
Her general condition was good with
disappearance of main complaints. Prognosis is good with no
post-operative complication and she will
be discharge on 19/03/2012.
RECOMMENDATION
1. Patient should be managed and monitored with correction of
fluid and electrolyte abnormalities,Antibiotics for complicating
infections, performing imaging studies as appropriate (eg,
ultrasound, HBS)
and lab data for follow-up care.
2. Patient should maintain healthy life style

















![Interstitial cystitis[1]](https://img.pdfslide.us/doc/110x75/55a728d31a28ab885e8b4702/interstitial-cystitis1.jpg)