Embed Size (px)
Citation preview
TREATMENT OF SUBMACULARHAEMORRHAGES
TVRS, June 2015.
Thanos Vakalis,Ophthalmica Institute,
Thessaloniki.
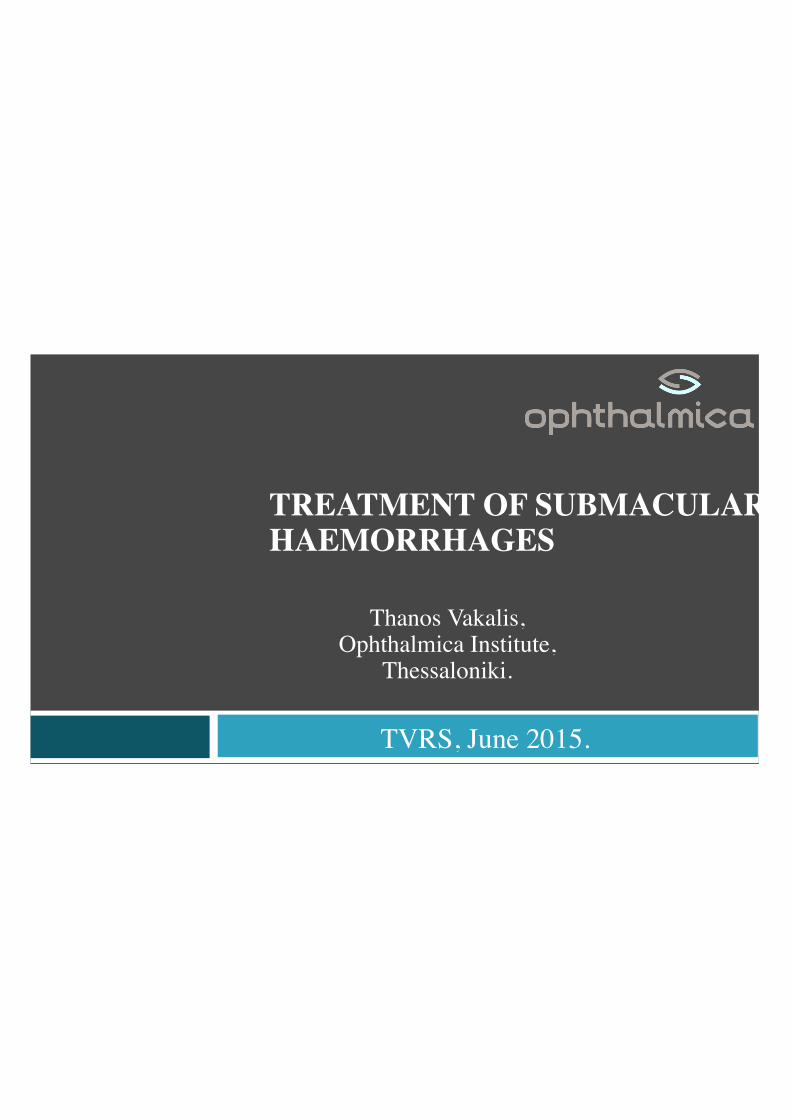
Macroaneurysm rupture, VA: FC

Fibrinolysis of experimental subretinal haemorrhage without removal using tissue plasminogenactivator. Morse LS et al, B J Ophthalmol 1994.
Photomicroscopy 2 weeks after SMH
Treatment
Visual Recovery• Thrombolysis• Removal of blood from macula• Causative treatment
Treatment
• R-TPA• Gas injection• Anti VEGF Treatment

r-TPA
rTPA
Molecular weight 70 Kda Toxicity in high doses Safe for subretinal use
Intravitreal gas and TPA: an outpatient procedure for submacular hemorrhage.Heriot WJ, AAO Annual Vitreoretinal Update, 1996.
Therapeutic options
Intravitreal injection of gas & tpa
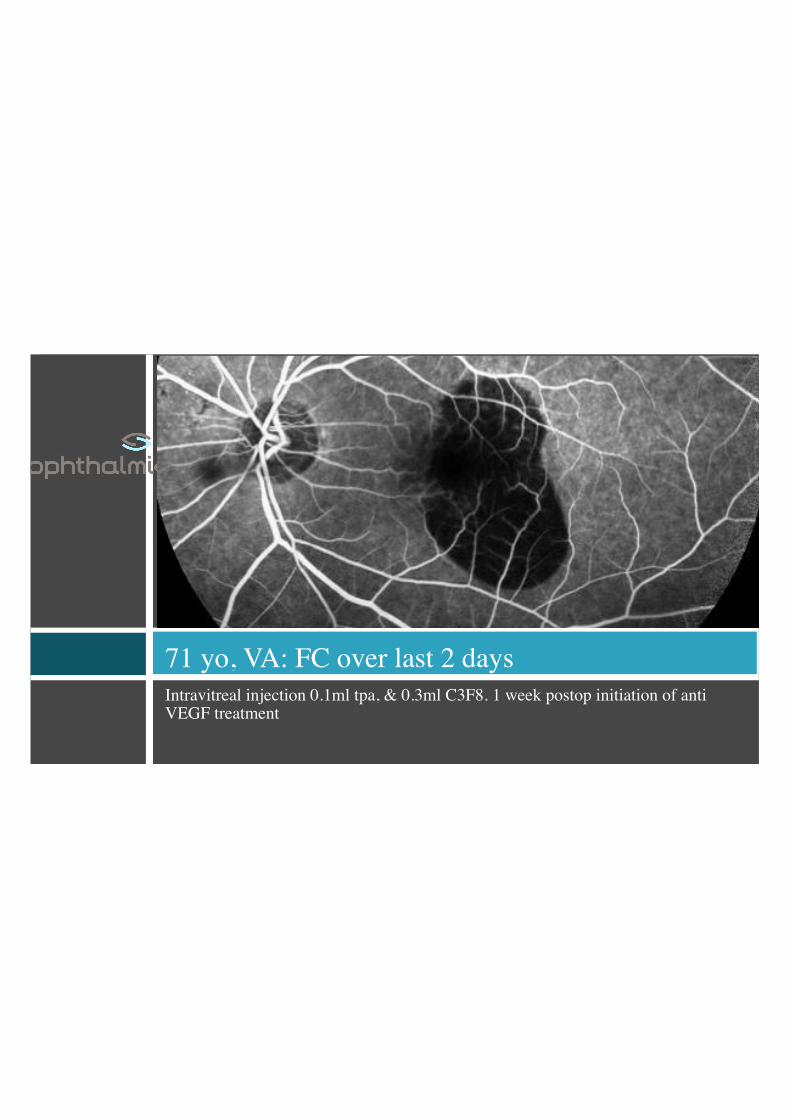
Intravitreal injection 0.1ml tpa, & 0.3ml C3F8. 1 week postop initiation of antiVEGF treatment
71 yo, VA: FC over last 2 days

10 days postopVA: 1/10
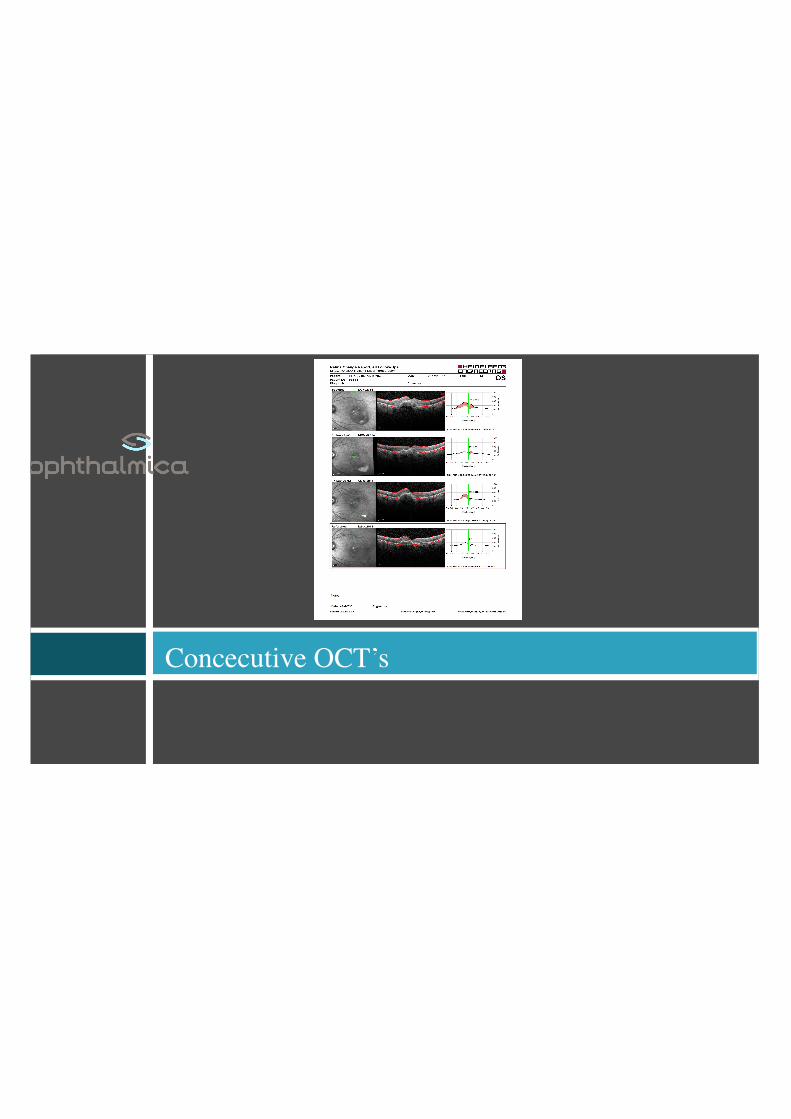
Concecutive OCT’s
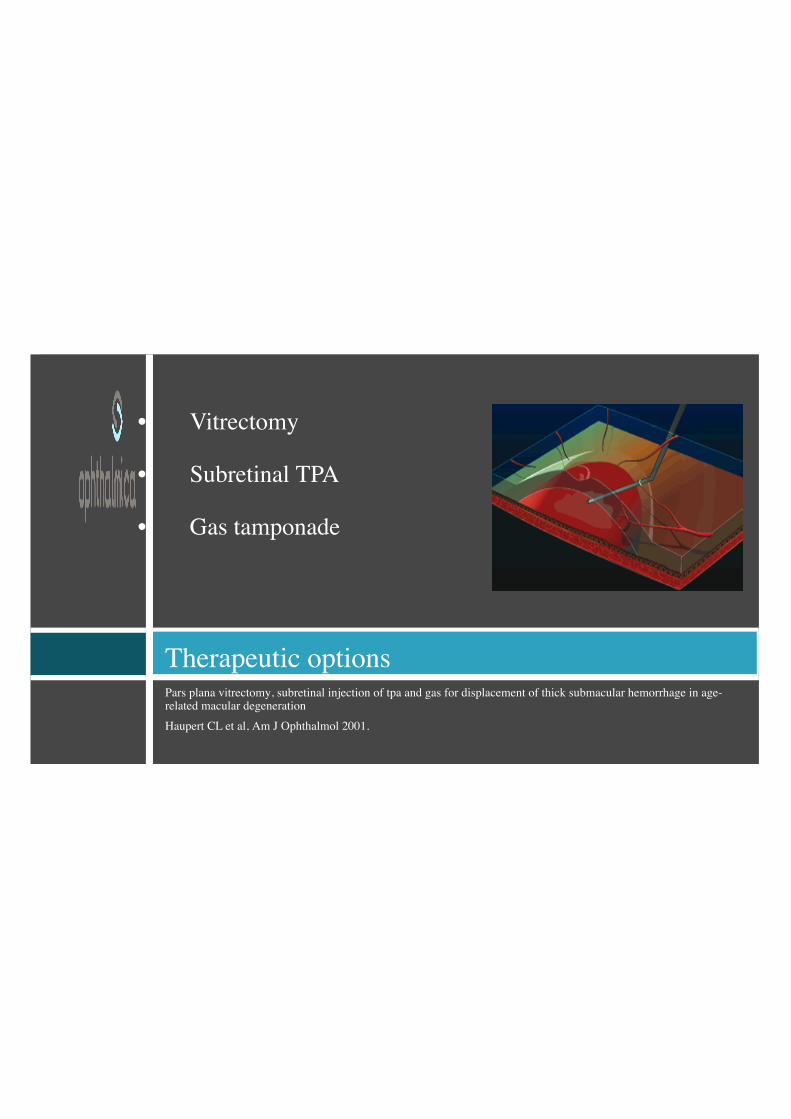
Pars plana vitrectomy, subretinal injection of tpa and gas for displacement of thick submacular hemorrhage in age-related macular degenerationHaupert CL et al, Am J Ophthalmol 2001.
Therapeutic options
• Vitrectomy
• Subretinal TPA
• Gas tamponade
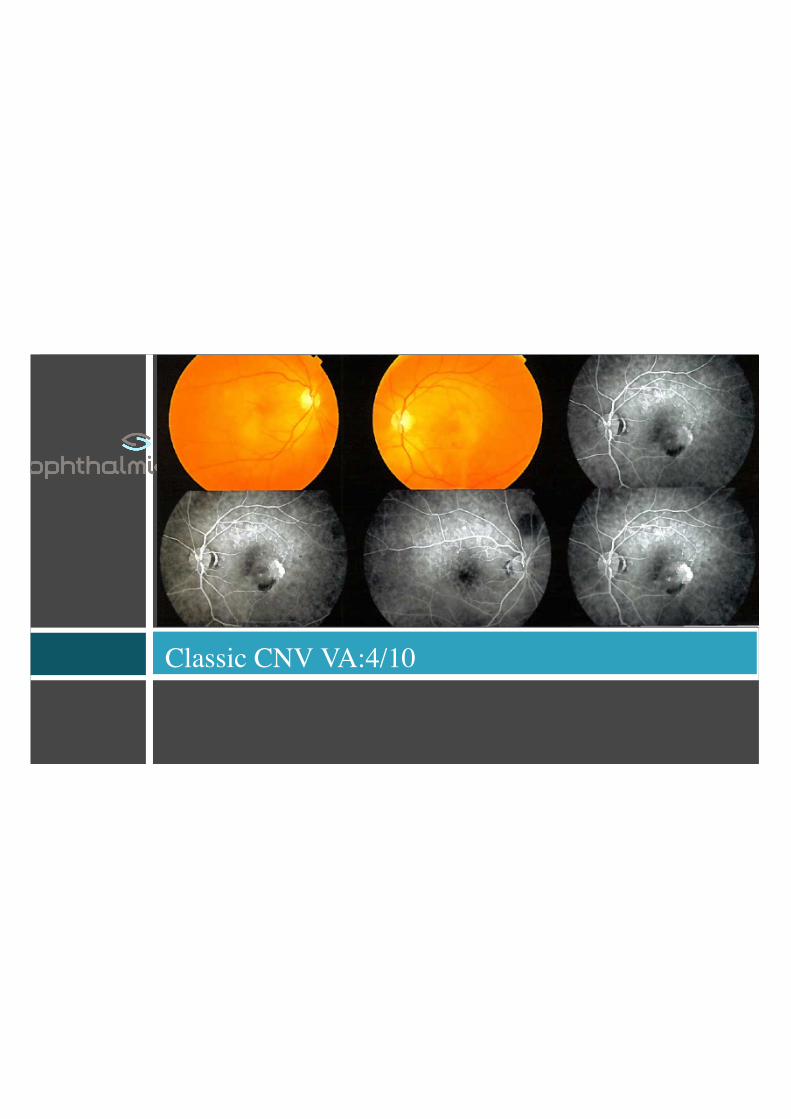
Classic CNV VA:4/10

1 day post antiVEGF VA: HM
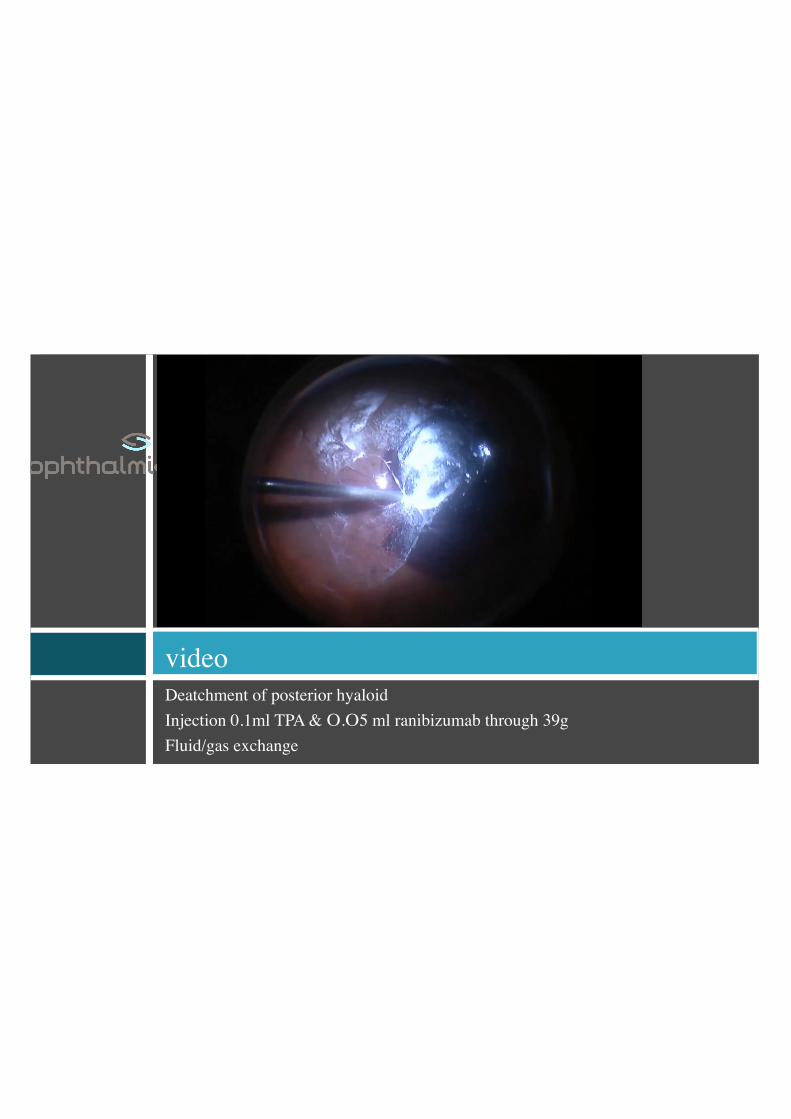
Deatchment of posterior hyaloidInjection 0.1ml TPA & Ο.Ο5 ml ranibizumab through 39gFluid/gas exchange
video
2 weeks postop

POSTOP OCT VA: FC

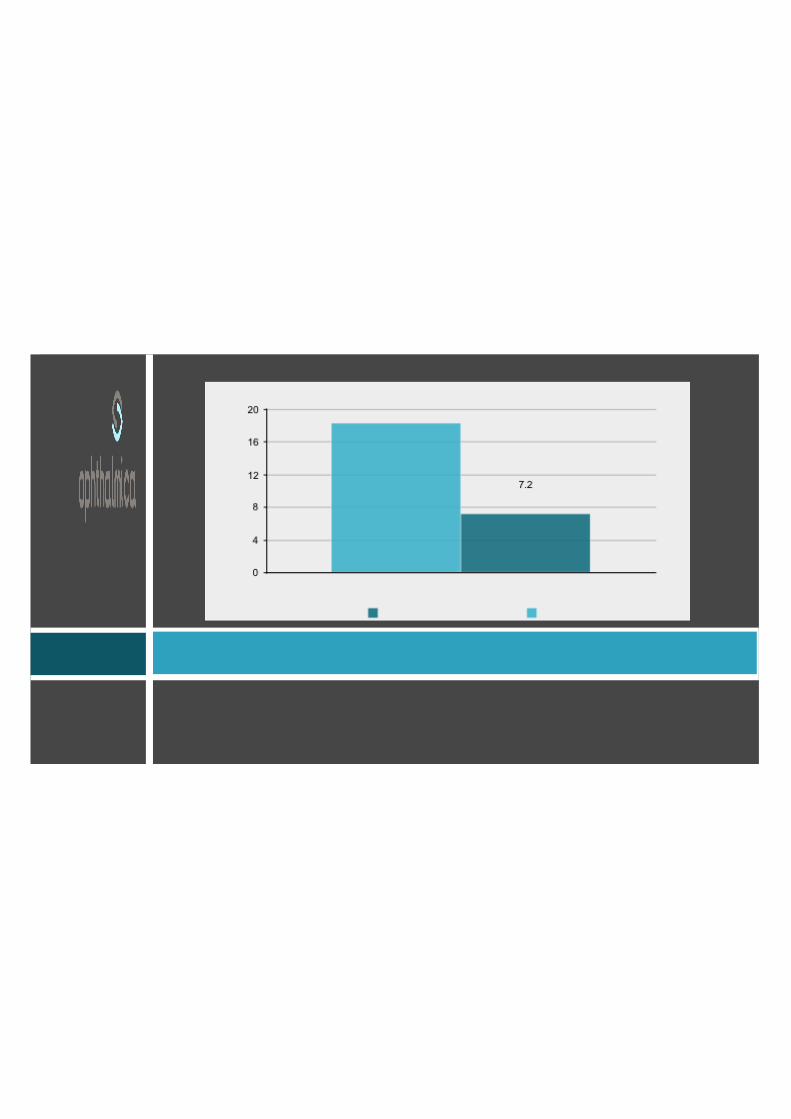
Ophthalmica series
13 patients, 14 eyesFollow up 3 to 25moΟ.Ο. HM -1/20 ECC. FIXATION.
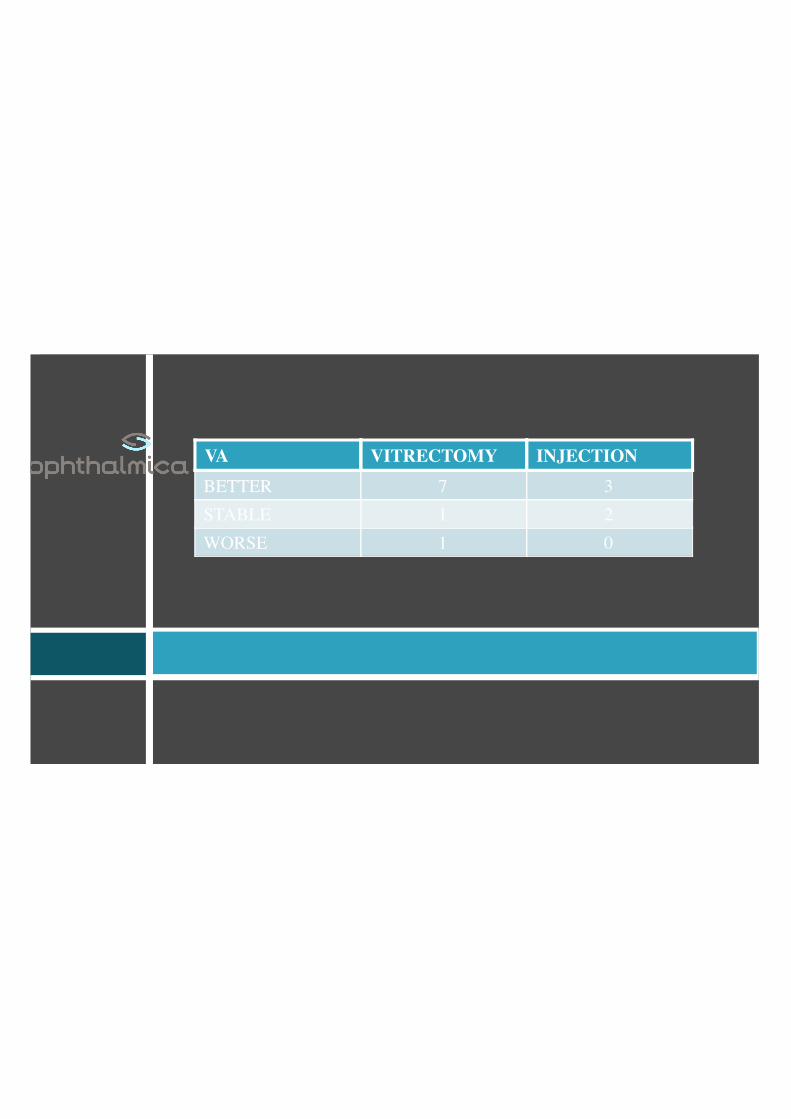
VA VITRECTOMY INJECTIONBETTER 7 3STABLE 1 2WORSE 1 0
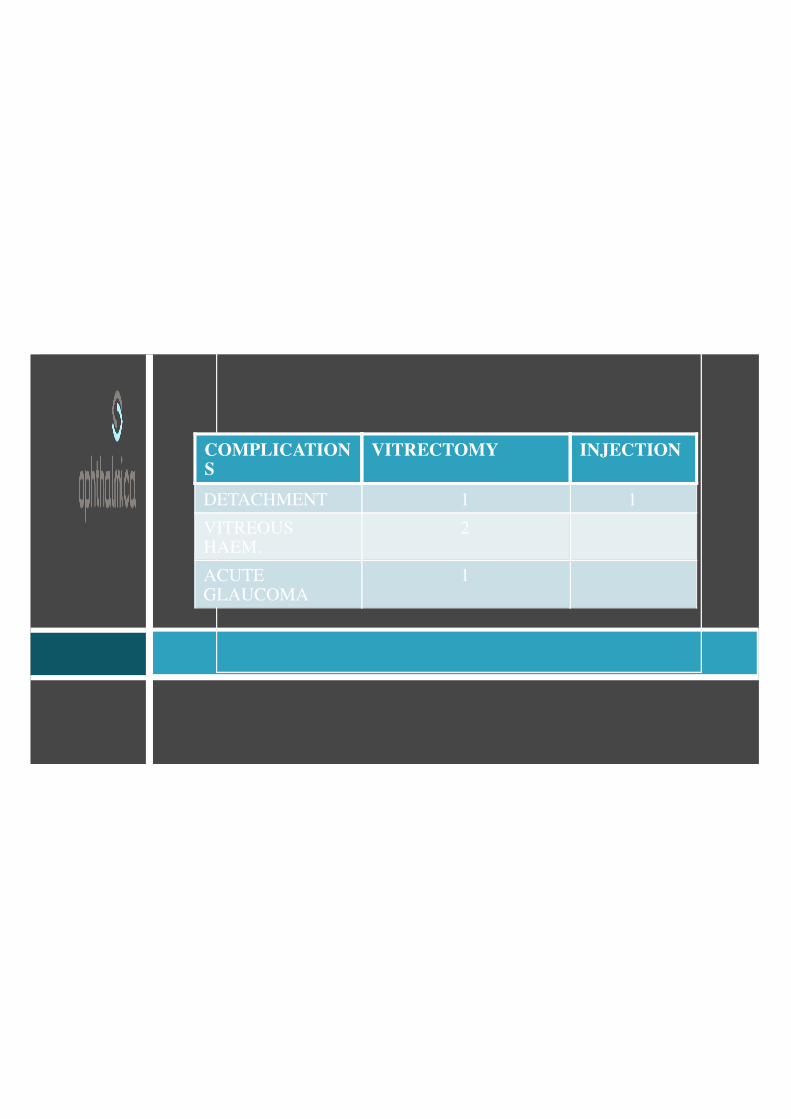
COMPLICATIONS
VITRECTOMY INJECTION
DETACHMENT 1 1VITREOUSHAEM.
2
ACUTEGLAUCOMA
1

Literature review of recombinant tpa used for reset-onset submacular hemorrhage displacement in age-related macular degenerationJT van Zeeburg, JC van Meurs, Ophthalmologica 2013.
LITERATURE REVIEW
38 recent studies1185 eyesHaemorrhage dislocation 60%Significant change in VA
THERAPEUTIC DILEMMAS
Anti VEGF Timing Choice Visual rehabilitation

Management of thick submacular hemorrhage with subretinal tissueplasminogen activator and pneumatic displacement for age-related maculardegeneration.Chang W, Am J Ophthalmol 2014.
Anti VEGF
Pre & post operative use appears to Reduce risk of recurrent haemorrhage Better final VA

Intravitreal anti-vascular endothelial growth factor for submacularhemorrhage from choroidal neovascularization.Kim JH,Ophthalmology 2014
AntiVEGF
Also effective as monotherapy? Only small and shallow bleeds
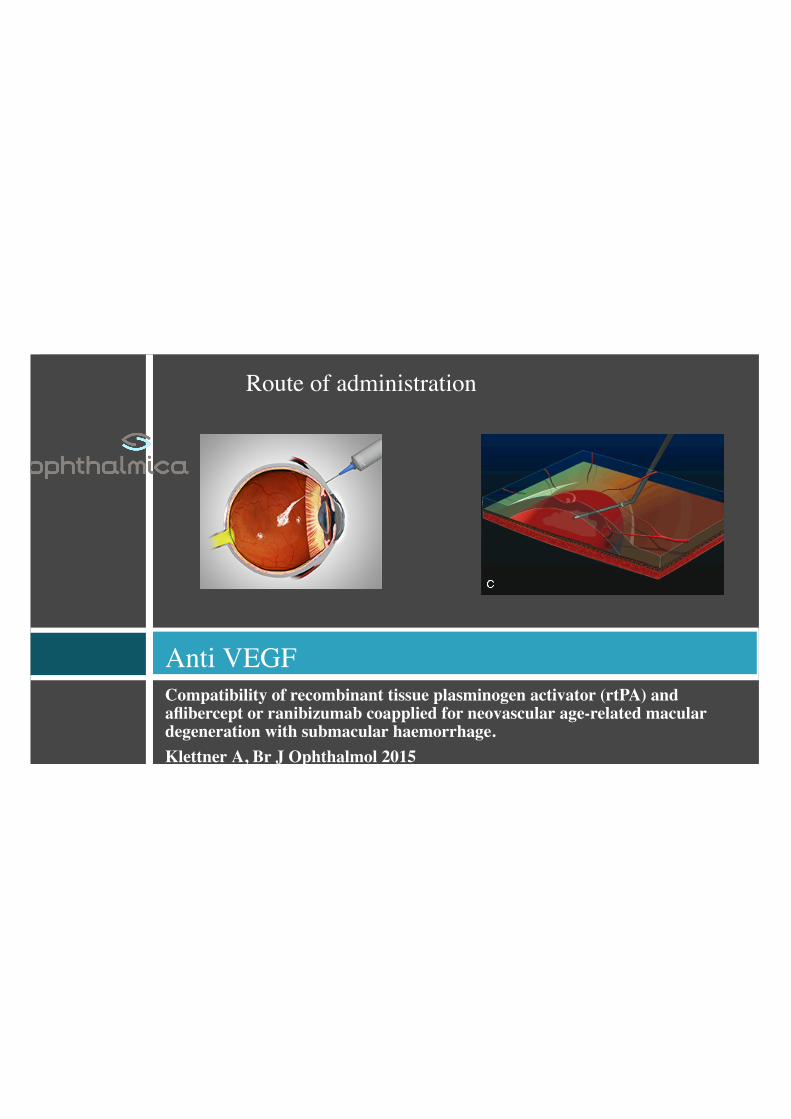
Compatibility of recombinant tissue plasminogen activator (rtPA) andaflibercept or ranibizumab coapplied for neovascular age-related maculardegeneration with submacular haemorrhage.Klettner A, Br J Ophthalmol 2015
Anti VEGF
Route of administration

Compatibility of recombinant tissue plasminogen activator (rtPA) andaflibercept or ranibizumab coapplied for neovascular age-related maculardegeneration with submacular haemorrhage.Klettner A, Br J Ophthalmol 2015
Anti VEGF
Dosing in eyes with gas? Full Dosing appears to be well tolerated
Management of thick submacular hemorrhage with subretinal tissueplasminogen activator and pneumatic displacement for age-related maculardegeneration.Chang W, Am J Ophthalmol 2014.
TIMING
Experimentally irreversible damage within 1 week. In studies clinical recovery even after 1 month Immidiate initiation does not reduce rate of fibrinolysis
Literature review of recombinant tpa used for reset-onset submacularhemorrhage displacement in age-related macular degenerationJT van Zeeburg, JC van Meurs, Ophthalmologica 2013.
Vitrectomy or injection
Both efficacious Similar complication rate Trend is recent studies towards vittrectomy Superiority of vitrectomy only in larger haemorrhages

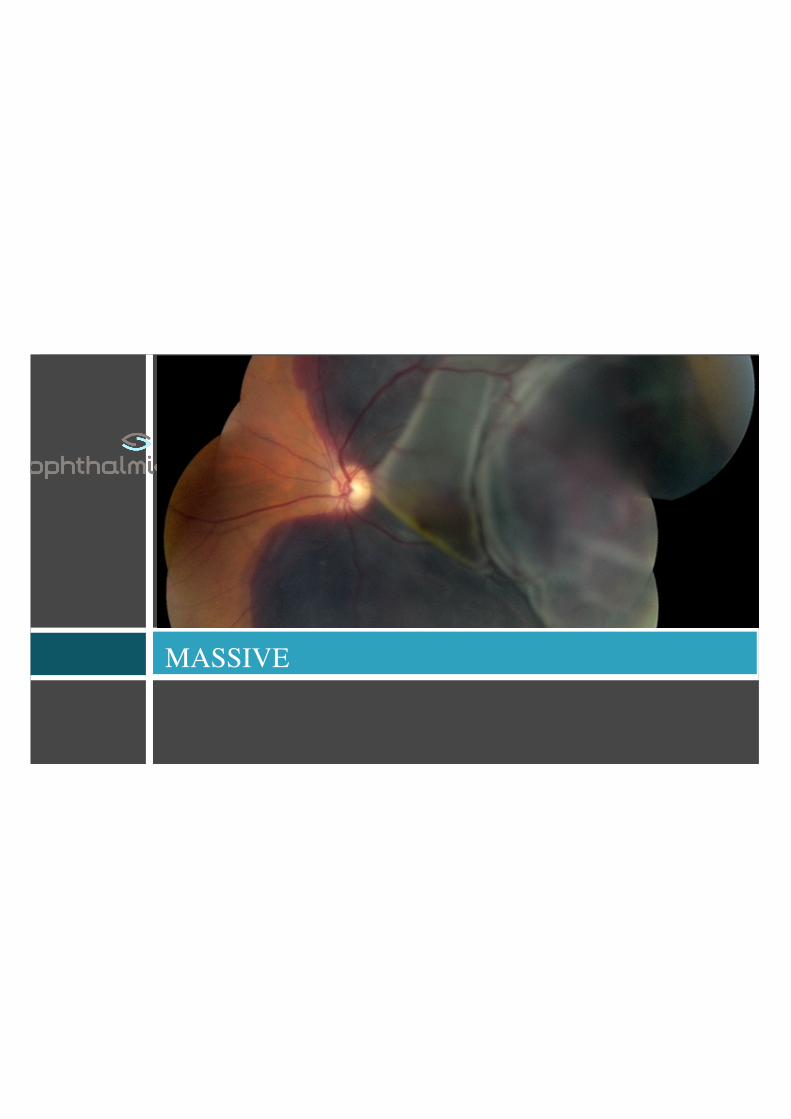
MASSIVE

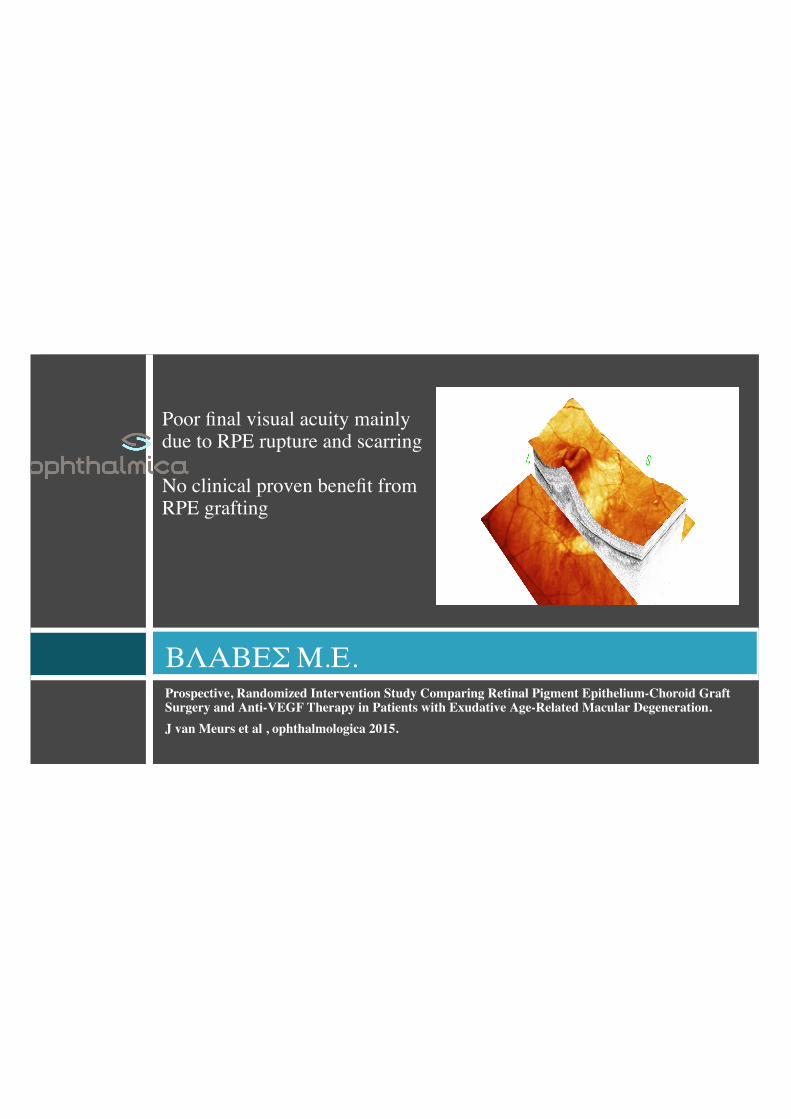
Prospective, Randomized Intervention Study Comparing Retinal Pigment Epithelium-Choroid GraftSurgery and Anti-VEGF Therapy in Patients with Exudative Age-Related Macular Degeneration.J van Meurs et al , ophthalmologica 2015.
ΒΛΑΒΕΣ Μ.Ε.
Poor final visual acuity mainlydue to RPE rupture and scarring No clinical proven benefit fromRPE grafting

CONCLUSIONS
Visual rehabilitation possible Anti VEGF plays key role Comparable results with less invasive methods Vitrectomy should be reserved for larger haemorrhages Effort should be made for early intervention

ΕΥΧΑΡΙΣΤΩ