-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
1/17
Page | 0
Transdermal and Oral Hormone Replacement Therapy and The
Incidence
of Vein Thromboembolism Among Postmenopausal Women
Rizky umara Anindhita
!"!#!$#%&%
'akarta %!&&
Abstract#
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
2/17
Page | 1
The pathophysiology of vascular disorder are briefly reviewed
within the context of
the relevance and safety of hormone replacement therapy.
Estimation of data from the medical
articles in relevance to the topic and the results of several
investigation studies suggest that
selective hormone replacement therapy is necessary for the
majority of postmenopausal
women. The key to overcome the benefits-risks profile is
individualization of hormone
replacement therapy, especially regarding the selection of the
route of administration of
hormone replacement therapy
The route of hormone replacement therapy administration is an
important determinant
of the risk of vein thromboembolism event in postmenopausal
women using hormone therapy.
ral route of administration of hormone replacement therapy are
associated with a
higher risk of vein thromboembolism among postmenopausal women.
This contributes an
epidemiological evidence that transdermal route of
administration may be safe with respect to
vein thromboembolism risk.
!E" #$%&' (ormone replacement therapy, )ein thromboembolism,
)ascular disorder
Introduction#
)enous thromboembolism is one of the vascular diseases of the
extremities which is
affecting *,+ per * persons every year*. This condition often
has a potential fatal
outcome, approximately +/ to */ of cases, which is worsen by the
fact that individuals who
have had a first event of venous thromboembolism are at high
risk for the second event *.
%ata about the incidence of venous thromboembolism among
postmenopausal women
has shown an increased within the past few years. This has been
correlated to administration
of hormone replacement therapy, which is taken by the
postmenopausal women to overcome
the severe climacteric symptoms.
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
3/17
Page | 2
0rom the recent epidemiological data, it suggests that different
routes of
administration of hormone replacement therapy expose different
amount of risk of the
incidence of vein thromboembolism. 1 concieve that the use of
oral administration are
associated with higher risk of vein thromboembolism among
postmenopausal women. This
thought is based upon the experimental study that was conducted
in the 2nited &tates of
3merica which concluded that the use of oral administration
increases the incidence of vein
thromboembolism, whereas the transdermal administration may be
safe with respect to vein
thromboembolism risk.
Hormone replacement as the treatment of menopause
Hormone replacement therapy and its use#
(ormone replacement therapy is a treatment for women who undergo
menopause, a
part of the aging process which embraces the transition from the
reproductive to the non-
reproductive phase of life4. The menopause age varies with race
and socioeconomic
conditions, but in western Europe and the 2&3 the average
age of onset is +* years 4. 1n
outline, the condition of menopause reflects the status of
women5s ovarium organ which is
one of the female reproductive system, it shows that the number
of ovum to be ovulated has
decreased, thus this women will experience hormonal changes.
0rom the aspect of physiology and anatomy, female5s reproductive
system involves
three hormone-secreting organ, they are the hypothalamus,
anterior pituitary gland, and the
ovarium. (ypothalamus produces gonadotropin-releasing hormone
6n$(, which will affect
the anterior pituitary gland to produce follicle-stimulating
hormone 0&( and luteinizing
hormone 7(. These hormones will inturn affect the ovarium to
produce estrogen that will be
used in the formation and development endometrium of the uterus
in follicular phase and to
be secreted to the blood. These three organ that is discussed,
which is also called the
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
4/17
Page | 3
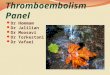
(ig#& (eedback )echanism *ithin the HP+ a,is
hypothalamus-pituitary-gonadal axis (86
axis plays a role to each other, which means
that there is a feedback mechanism within
this axis (ig#&*4. The estrogen produced
by the ovarium will affect the amount of
gonadotropin-releasing hormone, when there
is low estrogen level in the blood, this will
induced the hypothalamus to produce higher
level of gonadotropin-releasing hormone
which inturn causing the anterior pituitary
gland to produce high level of follicle-
stimulating hormone and luteinizing
hormone. 1n the other hand, when there is
high estrogen level, this will suppressed the
production of gonadotropin-releasing hormone and also causing
the level of follicle-
stimulating hormone and luteinizing hormone to become lower.
%uring the menopausal condition, there is a marked reduction in
ovarian production of
estrogen4. This is correlated by the fact that the number of
ovarian follicle is decreased in
time by the age. This absence of significant estrogen production
results in excessive release of
follicle-stimulating hormone and luteinizing hormone. These
variation in the circulating levels
of estrogen in the menopausal condition, accounts for the
variation in severity of menopausal
symptoms.
The symptoms in menopause can be divided into several groups
which is shown below
in Table#&4.
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
5/17
Page | 4
Table#&4# -ymptoms and -igns of The .limacteric
/menopause0
Vascular disturbances (ot flushes which consist of flushes
and
perspiration. This is associated with increased
in skin temperature and also associated in
some way with high level of gonadotropin-
releasing hormone..hanges in target organ response 9essation of
menstruation.
)aginal walls lose their rugosity and become
smooth and atrophic.
9ervix diminishes in size and decreased
production of cervical mucus.
2terus shrink in size.
Endometrium becomes atrophic.
1pidermal appendages &kin becomes thinned and wrinkled.
7oss of scalp, pubic, and axillary hair.
2one changes 7oss of trabecular bone which causes
osteoporosis. This is associated with
increased bone resorption.
.ardio3ascular complication 1ncrease in coronary heart
disease.
1ncrease of serum cholesterol level.
Psychological and emotional symptoms &evere emotional
disorder, such as depression
and anxiety.
Other symptoms and signs 3norexia, excessive fatigue,
nausea,
vomiting, and bowel disorders.
#omen who are experiencing those symptoms and signs and cannot
stand the severity
of them, are advised to take estrogen therapy as a hormone
replacement therapy to overcome
those symptoms and signs. :y taking the external source of
estrogen, it will increase the level
of estrogen in the blood and so will cause a feedback to
hypothalamus which will decrease the
production of gonadotropin-releasing hormone and so
follicle-stimulating hormone and
luteinizing hormone produced by anterior pituitary gland. This
hormonal therapy mechanism
will correct the hormonal changes that occur in menopausal
women. 3s by its name, hormone
replacement therapy is to take in hormone form external source
to replace the endogenous
hormone of the body.
Transdermal route of administration#
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
6/17
Page | 5
&ystemic estrogen can be administered trandermally and it is
usually used by women
who cannot tolerate or take oral forms because of nausea and
other health issues ;. There are
many kind of estrogen that can be administered transdermally, as
listed below in Table#%;.
Table#%;# Patch 4o* dose
/mg0
-tandard
dose /mg0
)edium
dose /mg0
Higher
dose /mg0
Highest
dose /mg0
Alora .+ .4+ *.4+ 4.+
Ortho61st /estrone0 .>4+ *.4+
Premarin /con5ugated e9uine estrogen0 .; .>4+ .? *.4+ 4.+
0rom the article titled 3ge-3djusted 7ong-Term Estrogen Therapy'
9ardiovascular
(ealth and %isease, it is stated, under sub-chapter of clinical
trials on hemostasis and venous
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
7/17
Page | 6
thrombosis, that hormone replacement therapy which is
administered orally will undergo first-
pass metabolism in the liver and this process has an effect on
the production of procoagulant
factors that are synthesized in the liver. Therefore avoidance
of the entero-hepatic first-pass
effect is associated with a more limited change in the
hemostatic profile.
@ost of the changes in the hemostatic profiles result from oral
estrogen usage, such as
conjugated e=uine estrogen 9EE, estradiol E4, or esterified
estrogen EE. These changes
include an increase in the levels of tissue activator
fibrinolysis inhibitor antigen, protein 9, %-
dimer, and factors )11, 1A, A indicators of increased
coagulation, and a decrease in the level
of protein &, antithrombin anticoagulation, and tissue
plasminogen activators fibrinolysis
B. 3ll of this changes will create a condition called
hypercoagulability state which favours the
formation of venous thrombus.
The degree to which estrogen as hormone replacement therapy
increases the risk of
venous thrombosis will vary primarily with the dose of estrogen
and the route of estrogen
therapy and this explains why there is a higher incidence of
venous thrombosis in oral route of
administration of estrogen therapy compared to transdermal
route.
Vein thromboembolism#
+eneral in3estigation of 3ein thromboembolism and its
pathophysiology
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
8/17
Page | 7
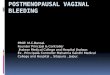
(ig#% 2lood .oagulation .ascade
)ein thromboembolism belongs to the group of vascular disease of
the extremities which is
characterized by the presence of
thrombus and inflammatory
response in the vessel wall+. This
vein disorder is subdivided into
two form' deep venous thrombosis
and superficial venous thrombosisC
the difference between these two
form of venous thrombosis is that
the location of the vein, one is in
near the skin surface superficial
and the other lays deep down the
tissue deep. 3ccording to
)irchow5*D+> there are three
factors which contribute to the
formation of venous thrombosis'
disruption of the blood flow
stasis, vascular damage, and hypercoagulability. The damage of
the vascular component will
trigger the activation of coagulation cascade by releasing
tissue factor which activates the
extrinsic pathway and prekallikrein which activates the
intrinsic pathway. :oth of these
pathways will lead to the formation of fibrin clot which later
on will trap the blood corpuscle
and form a thrombus (ig#%0**. This thrombus will keeps on
developing, as long as the
coagulation cascade is activated, and it will cause obstruction
in the lumen of the blood vessel
and thus disturbing the flow of the blood. Thrombus that is
formed can be anchored on the
wall of the blood vessel, as described before, or it can be
detached from the wall of the blood
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
9/17
Page | 8
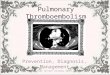
(ig# " Imbalance Hemostatic 4eading to Hypercoagulability
vessel and will flow with the blood, this is called
thromboembolus and the obstruction of a
blood vessel by an embolus is called embolism. This embolus can
pass through the
bloodstream to the heart and may get lodge in an artery and may
cause blood flow obstruction
which if it is not treated it may lead to organ damage and even
death >.
1n condition where the flow of the blood is slowed or stopped
stasis, the tissue of the
blood becomes inade=uately perfused with oxygen and nutrients.
Therefore this condition will
cause the damaged of blood vessels which will trigger the
activation of coagulation cascade
and will form thrombus, later on.
(ypercoagulability can be defined as a group of inherited or
ac=uired conditions
associated with a predisposition to venous thrombosis
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
10/17
Page | 9
>#0 Pregnancy#
?#0 1strogen use ; as replacement therapy or contraception#
7#0 Hypercoagulability ; resistance to acti3ated protein .<
deficiency antithrombin III#
$#0 Venulitis ; thromboangitis obliterans< 2ehcet@s
disease#
#0 Pre3ious deep 3ein thrombosis#
Pathophysiology of hormone replacement therapy6inducing63ein
thromboembolism#
(emostasis of our blood clotting is controlled by two mechanism'
coagulation
cascadeC that has an intrinsic and extrinsic pathway, a number
of inactive zymogens factors
which are converted to proteases activated factors that
eventually result in the conversion of
prothrombin into thrombin that will catalyzes fibrinogen into
fibrin and leads to the formation
of insoluble blood clotC and anticoagulant systemC which
involves antithrombin, protein 9,
and cofactor protein &. 3 balance in this system will make
our blood hemostasis normal,
whereas if there is any imbalance, it will lead to either
excessive blood clot formation
hypercoagulability state or lack of blood clot formation
bleeding problems.
3s we have discussed before, there
are three factors that caused venous
thrombosis, according to )irchow5*D+>,
they are' disruption of the blood flow
stasis, vascular damage, and
hypercoagulability state (ig#:+. 1n the
case of hormone replacement therapy
associated with venous thrombosis, the factor that plays role of
its development is factor
number three, that is hypercoagulability state. There has been
some studies that investigate
that the use hormone replacement therapy induces the state of
hypercoagulability which result
in the development of venous thrombosis. ne of the side effects
of using the hormone
replacement therapy is that the person5s hemostatic profile is
altered. There is a shift towards
(ig#:# Vircho*@s Triad
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
11/17
Page | 10
the production of inactive zymogens factors which are converted
to proteases activated
factors and there is a reduced synthesis of antithrombin which
is essential factor in
modulating the coagulation cascadeD. Therefore from this
imbalance hemostatic condition,
coagulation cascades is activated, through both intrinsic and
extrinsic pathway and meet the
common pathway where conversion of prothrombin into thrombin
catalyzes the formation of
fibrin.
The incidence of hormone replacement therapy6inducing63ein
thromboembolism#
The incidence of vein thromboembolism induced by the use of
hormone replacement
therapy has been increasing from the past few years. &ome
articles and even studies have been
investigating not just towards this incidence, but also how the
different route of administration
affecting vein thromboembolism differ.
Taken from the article of &cience %aily @ay 4>, 4D, it is
stated that hormone
replacement therapy given in skin patches, the trandermal route
of administration, may cause
fewer blood clots compared to when it is given orally, further
more for women who take the
oral route of administration more than double their risk of
developing a blood clot?.
&till from the same article, it is also mentioned that there
have been researchers who
conduct data review from eight observational studies and nine
randomised controlled trials.
0rom this data review, they found that women taking the oral
form of hormone replacement
therapy were two and three times more likely to develop a blood
clot, and that the risk was
higher during the first year of treatment?.
The @edscape @edical ournal about hormone replacement therapy
and venous
thromboembolism in postmenopausal women, had conducted a
research on the topic
discussed. This research studied about the recurrency of vein
thromboembolism on
postmenopausal women who were on a treatment of hormone
replacement therapy and had
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
12/17
Page | 11
had an episode of vein thromboembolism, and compared the result
when oral or trandermal
administration were used*. The result shows that transdermal
estrogen use after a first vein
thromboembolism event did not expose women to an excess risk of
recurrence. 1n contrast,
oral estrogens increased significantly the risk of recurrent
vein thromboembolism *.
)anagement#
)enous thromboembolism is one of the major causes of morbidity
and mortality, this is
due to one of its complication that is pulmonary embolism which
can be fatal. To prevent and
treat this disorder, certain therapy is needed, they are called
antithrombotic drug therapy. The
antithrombotic drug is classified into three catagories,
depending on how the drugs work, they
are' antiplatelet drugs, anticoagulants, and fibrinolytic
agents.
The example of antiplatelet
drugs are' aspirin, clopidogrel,
ticlopidine, abciximab, and
tirofiban. These drugs affect the
process of platelet aggregation on
different stages. 3spirin produces
its antithrombotic effect by
irreversibly acelating and inhibiting
platelet cyclooxygenase 9A-*,
an enzyme which play role in the
synthesis of thromboxane 34, which
is needed in platelet recruitment and
activation. 9lopidogrel and ticlopidine also work the same as
aspirin but they work onto
different enzyme, which is adenosine diphosphatase 3%8ase.
3bciximab and tirofiban
(ig#> -ite of Action of Antiplatelet
Brugs
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
13/17
Page | 12
(ig#? )echanism of Action of Heparin and 4o*6)olecular6
Weight Heparin
belongs to a class of 6811bF111a receptor antagonist. This class
works to prevent the activated
platelet to bind to adhesive molecules, such as fibrinogen and
von #illebrand factor and
therefore inhibit the process of platelet aggregation (ig#>*.
3spirin is usually administered
at doses of
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
14/17
Page | 13
intial bolus of + units or D unitsFkg, followed by an infusion
of *D unitsFkg per hour. The
dose of low-molecular-weight heparin used is given *+-4 unitsFkg
once daily. #arfarin, as
an oral anticoagulant, works by blocking vitamin ! epoxide
reductase which means that
vitamin ! epoxide cannot be reduced and therefore inhibiting the
role of vitamin !-dependent
factors, such as factor 11, )11, 1A, and
A, in the coagulation cascade (ig#7
*. The dosing used for warfarin is
usually started at a dose of +-* mg,
which is then titrated to correlate the
normal value of prothrombin time.
0ibrinolytic drugs that are used
to treat vein thromboembolism degrade the thrombi that has
formed on the wall of the blood
vessel. They are administered systemically or can also be
administered via catheters directly
into the substance of the thrombus. &treptokinase acts on
the fibrinolytic system by acting on
plasminogen, make a conformational
change and thus exposing its active
site which is able to degrade fibrin to
fibrin degradation products (ig#$ and
*. #hen given systemically, this
drug is given as an 1) infusion of *.+ million
units over ;-> minutes.
(ig#$ The (ibrinolytic -ystem
(ig# )echanism of Action of -treptokinase
(ig#7 )echanism of Action of Warfarin
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
15/17
Page | 14
.onclusion#
1n conclusion from what 1 get in my data review from several
text books, articles, and
medical journals, the results provide a contribution to an
epidemiological evidence that
transdermal hormone replacement therapy may be safe with respect
to vein thromboembolism
risk in general. This review can give an important consideration
and input for women at high
vein thromboembolism risk who re=uire hormone replacement
therapy for severe
postmenopausal symptoms. $educing vein thromboembolism risk by
using transdermal
hormone replacement therapy could improve the benefits-risks
profile of hormone therapy
among postmenopausal women.
References#
*. )alerie , 6enevieve 8:, ac=ueline 9, (elene (@, @arianne 9,
"ves &8. (ormone
Therapy and $ecurrence of )enous Thromboembolism 3mong
8ostmenopausal #omen. The
Gorth 3merican @enopause &ociety 4**C *D+' BDD-B?;.
4. &ymonds E@, &ymonds 1@. Essential bstetrics and
6ynaecology. 7ondon' 9hurchill
7ivingstoneC 4B. p. 4++-4+?.
;. Elder 3, @essinger :, Thacker (7. &pecial 1ssues in
#omen5s (ealth' (ormonal (ealth
1ssue of Early and 7ate 8ostmenopausal #omen. 1n' 7andefeld
9&, 8almer $@, ohnson @3,
ohnston 9:, 7yons #7, editors. 9urrent 6eriatric %iagnosis and
Treatment. Gew "ork'
@c6raw (illC 4B. p. ;+?-;>>.
B. 3nonymous. 3ge-3djusted 7ong-Term Estrogen Therapy'
9ardiovascular and %isease.
4>. 3vailable from'
http'FFwww.medscape.comFviewarticleF+4;D+*HB accessed @ay ;,
4**.
http://www.medscape.com/viewarticle/523851_4http://www.medscape.com/viewarticle/523851_4
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
16/17
Page | 15
+. 9reager @3, 7oscalzo . )ascular %isease of the Extremities.
1n' 0auci 3&, !asper %7,
7ongo %7, :raunwald E, (auser &7, ameson 7, 7oscalzo ,
editors. (arrison5s 8rinciples
of 1nternal @edicine. Gew "ork' @c6raw (illC 4D. p. *+
-
8/10/2019 Transdermal and Oral Hormonal Replacement Therapy and
the Incidence of Vein Thromboembolism Among Postm
17/17
Page | 16