Embed Size (px)
Citation preview

By: Hanaa Adnan Rasheed6th stage Group B1
Supervised by: Prof.Dr. Ayla K. Ghalib

Points to Discuss:
1) Physiology of hemostasis.
2) Coagulation during pregnancy.
3) Thromboembolism in pregnancy:
• Superficial thrombophlebitis.
• Deep vein thrombosis.
• Pulmonary embolism.
• Thrombophilias.
4) Thromboprophylaxis.

Physiology of Hemostasis:
The term hemostasis means prevention of blood loss.
Whenever a vessel is severed or ruptured, hemostasis is achieved by several mechanisms:
(1) vascular constriction,
(2) formation of a platelet plug,
(3) formation of a blood clot as a result of blood coagulation, and
(4) eventual growth of fibrous tissue into the blood clot to close the hole in the vessel permanently. (1)


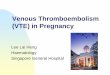
The extrinsic pathway
begins with a traumatized
vascular wall.
The intrinsic pathway
begins with trauma to the
blood itself or exposure of
the blood to collagen from
a traumatized blood vessel
wall. (1)


Coagulation During Pregnancy:
Plasma Fibrinogen concentration by ~
50%.
Factors: V, VII, VIII, IX, X and XII.
Platelet reactivity in 2nd and 3rd TMs till
12wk post partum.
Fibrinolytic activity.
Protein S (an inhibitor of coagulation). (2)

Pregnancy is a hypercoagulable state that
return to normal 4 weeks after delivery. (3)
WHY???

This hypercoagulability is particularly relevant at delivery, with placental separation…
At term, around 500ml blood flows through the placental bed every minute…
Without effective and rapid hemostasis, a woman could rapidly die from blood loss…
Myometrial contraction FIRST compress BV supplying placental bed…
Then FIBRIN deposition on pl. bed.(10% of blood fibrinogen is used for this process!). (3)

Thromboembolism in Pregnancy:
1. Superficial Thrombophlebitis
2. Deep Vein Thrombosis.
3. Pulmonary Embolism.
4. Thrombophilias.

Venous Thromboembolism (VTE)
Venous thromboembolism (VTE) is the leading
direct cause of maternal death throughout
pregnancy.
The incidence of thromboembolic complications,
pulmonary TE and DVT presented during
pregnancy is around 1/1000, with a further
2/1000 women presented in puerperium.
VTE is up to 10 times more common in
pregnancy than in comparable non-pregnant
subject. (2)

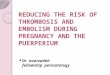
Hyper-
coagulability
Vascular Damage
Venous Stasis
Pathogenesis of VTE in Pregnancy


Risk Factors for VTE in Pregnancy (4)
Risk FactorsTimeframe
Previous venous thromboembolism
Thrombophilia
Medical comorbidities (e.g. heart or lung disease, SLE,
cancer, inflammatory conditions , nephrotic syndrome ,
sickle cell disease,
Age > 35 years
Obesity (BMI > 30 kg/m2)
Parity ≥ 3
Smoking
Gross varicose veins
Paraplegia
Pre-existing
Multiple pregnancy, assisted reproductive therapy
Pre-eclampsia
Caesarean section
Prolonged labour, mid-cavity rotational operative delivery
PPH (> 1 litre) requiring transfusion
Obstetric
Surgical procedure in pregnancy or puerperium
Hyperemesis, dehydration
Ovarian hyperstimulation syndrome
Potentially
Reversible

1* Superficial Thrombophlebitis
Clinical Features:
Swelling and tenderness of the involved extremity.
On physical examination, there is erythema, tenderness, warmth, and a palpable cord over the course of the involved superficial veins.
Treatment:
Bed rest, pain medications, and local application of heat are often sufficient treatment.
There is no need for anticoagulants, but anti-inflammatory agents may be considered. (5)


2* Deep Vein Thrombosis:
Clinical Features:
50% of cases are
asymptomatic.
DVT is much more common in
the left than the right leg.
Pain in the calf in association
with dorsiflexion of the foot
(positive Homans’ sign) .
Dull ache, tingling, tightness,
especially when walking. (5)


Investigations (6) :

3* Pulmonary Embolism:
Clinical Features:
Symptoms: - Pleuritic chest pain,
- Shortness of breath,
- Air hunger,
- Palpitations,
- Hemoptysis
Signs: º Tachypnea,
º Tachycardia,
º Pleural friction rub,
º Pulmonary rales,
º Signs of right ventricular failure. (5)

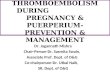
Investigations (6)
Other
investigations:
ECG
Arterial blood
gases
*CUS=
Compression
Ultrasound.
*CTPA=CT
pulmonary
Angiography.
*V/Q=
Ventilation
Perfusion Scan


Perfusion Ventilation

Treatment of VTE in Pregnancy:
Acute Phase Treatment:
• Thrombolytic Therapy:
• Streptokinase and TPA.
• Cannot be recommended in pregnancy except in life saving procedures:
• Skocked patient with massive PE.
• Iliofemoral venous thrombosis.
• Anticoagulants:
• Unfractionated Heparin:
• 40.000 IU/day
• IV infusion
• For (3-7) days
• Monitor by APTT (1.5-2.5)x normal.
• Fractionated or LMWH:
• Surgery.


Chronic Phase Treatment:
• Warfarin:
• Cross placenta
• If given in pregnancy it must be stopped at 36 wk.
• Monitor by PT and INR (target 2.0 – 3.0).
• Duration of action: 3 days
• S.E: bleeding tendency & teratogenecity.
Teratogenic Effects of Warfarin:
• Embryopathy.
• CNS abnormalities.
• ↑abortion and premature labour.
• Chondroplasia punctata.
• Nasal hypoplasia.


4* Thrombophilias
Congenital
• Anti-thrombin III deficiency
• Protein C deficiency
• Protein S deficiency
• Factor V Leiden
• Prothrombin gene variant
Acquired
• Antiphospholipid syndrome (2)

Antiphospholipid syndrome (APS)
Antiphospholipid antibodies are circulating
antibodies to negatively charged phospholipids.
They include lupus anticoagulant and
anticardiolipin antibodies.
Antiphospholipid antibody syndrome is defined
as the presence of at least one antibody in
association with arterial or venous thrombosis with
or without one or more obstetric complication
(unexplained fetal demise after 10 weeks’
gestation or severe preeclampsia or fetal growth
restriction before 34 weeks’ gestation).
Treatment: LMWH and Aspirin. If Hx of
thrombosis, require full anticoagulation. (5)



References:
1. Arthur C. Guyton. Guyton Textbook of Medical
Physiology. Elsevier Saunders. 11th edition.
2006. pages (419-468).
2. Edmonds D. Keith. Dewhurst’s Textbook of
Obstetrics and Gynecology. Blackwell
publishing. 7th edition. 2007. pages (270-281).
3. Philip N. Baker. Obstetrics by Ten Teachers.
Hodder Arnold. 18th edition. 2006. Pages (286-
299).

4. Reducing the Risk of Thrombosis and
Embolism During Pregnancy and Puerperium.
RCOG green top guideline. American College
of Obstetricians and gynecologists. No.37a.
November 2009. pages (1-35).
5. Neville F. Hacker, Josephe C. Gambone and
Calvin J. Hobel. Hacker and Moore’s
Essentials of Obstetrics and Gynecology.
Elseviers Saunders. 5th edition. 2010. pages
(191-218).

6. Cunningham F. Gary, Kenneth J. Levendo,
Steven L. Bloom et al. Williams Obstetrics.
Mc Graw Hill. 24th edition. 2014. Pages
(1028-1047).