Embed Size (px)
Citation preview
American Foundation for
Donation & Transplantation
Living Donation: Essential Donor Team Concepts
Clearwater, Florida
May 2013
Toolkit for the
Development of a KPD Program Policy & Procedure ~ Patient Education ~ Tracking Worksheets
Marie Morgievich APN.C, CNN, CCTC
Manager, Living Donor Institute
Transplant Nurse Practitioner
But a complex program with its own
Clinical
Administrative
…and Financial Implications.
Successful Exchange Programs have
strong clinical, administrative, and
financial management support.
Kidney Exchange: It‟s not just another living donor transplant…
Will Jane Succeed?…a short story:
LD coordinator is approached by her manager and
informed that in addition to her full caseload she will be
responsible for kidney exchange:
MANAGER: “Oh Jane…we feel you are the perfect
person to work on kidney exchange – it‟s going to be so
exciting! Dr. John is going to be the surgeon – can you
speak with him about it when you have a chance?…”
JANE: “Really?”
MANAGER: “Let me know how‟s its going and if you need anything.
JANE: „gulp‟
Consider › Clinical
RN, MDs (Nephrologists & Surgeons), SW
Identifying/Educating/Consenting/Match Reviews
Peri-operative support
› Administrative Manager/Director
Policy/Procedures & supporting resources for program: esp. staff time
› Finance Needs understanding of payment system
Communicates with other centers
› OPO / LAB Cross-matches
Packaging/Shipping
Registry data support
Transplant Team & Staffing
Key to success: Total Team Support
Exchange Coordinator: importance of nurse expert
Transplant Team needs to buy into Kidney Exchange
No eye rollers allowed
One coordinator needs to be kidney exchange expert
Need dedicated physician/surgeon to support that
nurse & work closely on program
Management needs to support
½ - 1 FTE RN time and ¼ FTE assistant time
Time may increase/decrease as exchanges increase
Exchange Coordinator: importance of nurse expert
Has to believe in exchange and want to become expert
Reaches out to other experienced coordinators for advice/help/develop rapport
Point person for all communication Physician/surgeons, registry, admin & financial managers, peri-operative
group, OPO, couriers, other centers
Coordinates all aspects of the exchange Available 24/7 during exchange
Has developed relationship with donor & recipient
STAFFING Saint Barnabas Living Donor Institute
Manager & Nurse Practitioner
Living Donor RN Coordinators Donna Walton Ethel Patino
LD Recipient RN Sol Acuna
Transplant Assistant (2) Alyson Thorward Elena Nieves
Social Worker (2)
Shared with department
Financial Coordinator (1) shared with department
Living Donor Advocate
Physicians Dr. Shamkant Mulgaonkar Dr. Anup Patel
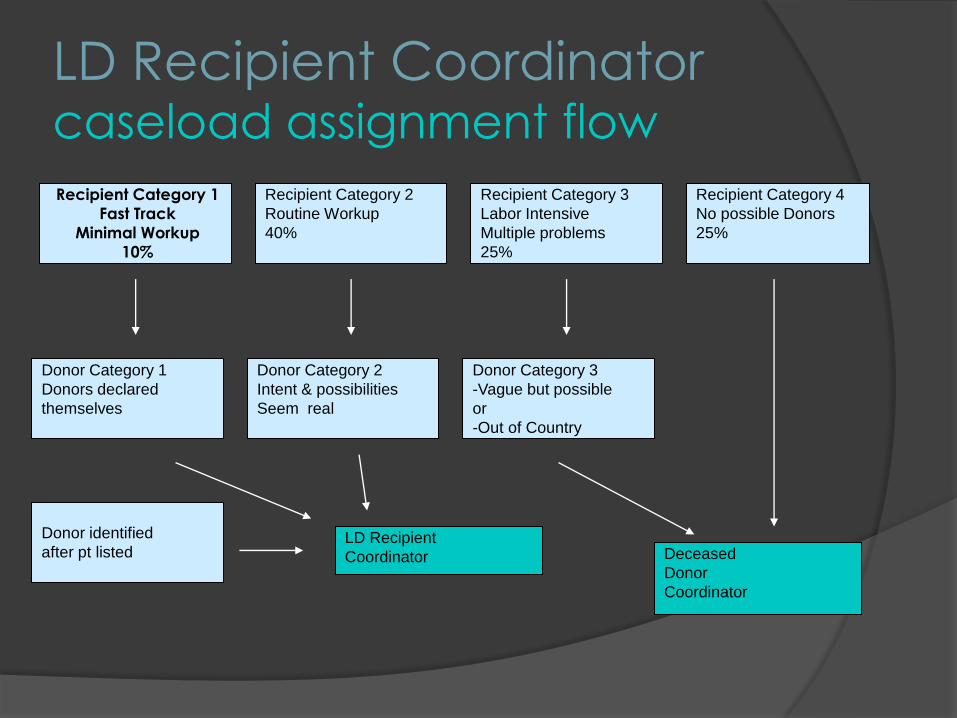
LD Recipient Coordinator caseload assignment flow
Recipient Category 1
Fast Track
Minimal Workup
10%
Recipient Category 2
Routine Workup
40%
Recipient Category 4
No possible Donors
25%
Recipient Category 3
Labor Intensive
Multiple problems
25%
Donor Category 1
Donors declared
themselves
Donor Category 2
Intent & possibilities
Seem real
Donor Category 3
-Vague but possible
or
-Out of Country
Donor identified
after pt listed Deceased
Donor
Coordinator
LD Recipient
Coordinator
Exchange Policy & Procedure
PURPOSE: To establish standards for the
evaluation, registration, and transplantation of
patients through the Living Donor Kidney
Exchange Program (LDKEP).
The goal: to increase the supply of kidneys
available for transplantation safely and
ethically.
NATCO website for attendees:
Find P&P from Barnabas Health, Cornell, UCLA,
University Wisconsin
Exchange Policy & Procedure Definitions
Living Donor Kidney Exchange Program: An exchange involving living
donors who are incompatible with their intended recipients so that
each donates to compatible recipients.
Intended Recipient: The recipient that the donor initially intended to
donate to but was found to be incompatible.
Intended Pair: The recipient/donor pair that was originally intended for
donation/transplantation.
Matched Pairs: The exchanged recipient donor pairs that are
compatible to each other.
Exchange Registry: A confidential data base that contains the names,
blood types, ages, medical profiles, and other significant information of
the recipient/donor pairs who have agreed to be listed in such a data
base awaiting compatibility matching with another incompatible
recipient/donor pair.
Exchange Policy & Procedure vital components:
Who/when/how patients are educated
Site tools used
Who is responsible for all aspects of exchange from identification pair to transplantation
Pairs satisfy the same medical, psychosocial & ethical selection criteria
Evaluation of donors
no out of state workups
Confidentiality & anonymity issues
Exchange Policy & Procedure vital components:
Registry, Match procedures, uses of Data
Shipping of living donor kidneys Risks
Logistics Simultaneous vs. bridge donation
What to do if a deceased donor becomes available for your recipient who has an exchange match …
Case Study: What would you do?
Your patient Bob Clifford – exchange wait time 3 years
55 y.o. male BG „O‟ , PRA 80%
In multi-center/state exchange txp date Mon Oct 4th
Exchange donor: 22 y.o. male in California, cxm negative
Est. CIT 12-14 hours
All final cxms pending
Deceased donor offer today Friday Sept 17th
48 y.o. local donor , cxm negative
Creatinine stable, died of asthma attack
Gestational DM 20 years ago
Case Study: What was done.
On-Call RN, Exchange RN & Transplant Physician discuss
situation
Exchange RN: “90% sure exchange will happen..but not 100%
Physician called pt and explained risks/benefits
Pt given choice
Conversation carefully documented
Pt chose to wait for exchange
Exchange Policy & Procedure vital components:
To avoid deceased donor offer from decimating an exchange:
Put pt. „on hold‟ in OTTR or your EMR within 3 weeks of exchange OR date
○ “Call Dr. ______ with any organ offers before notifying pt. “
In P&P & Education ○ Pt. will only be notified if offer is a 0 MM
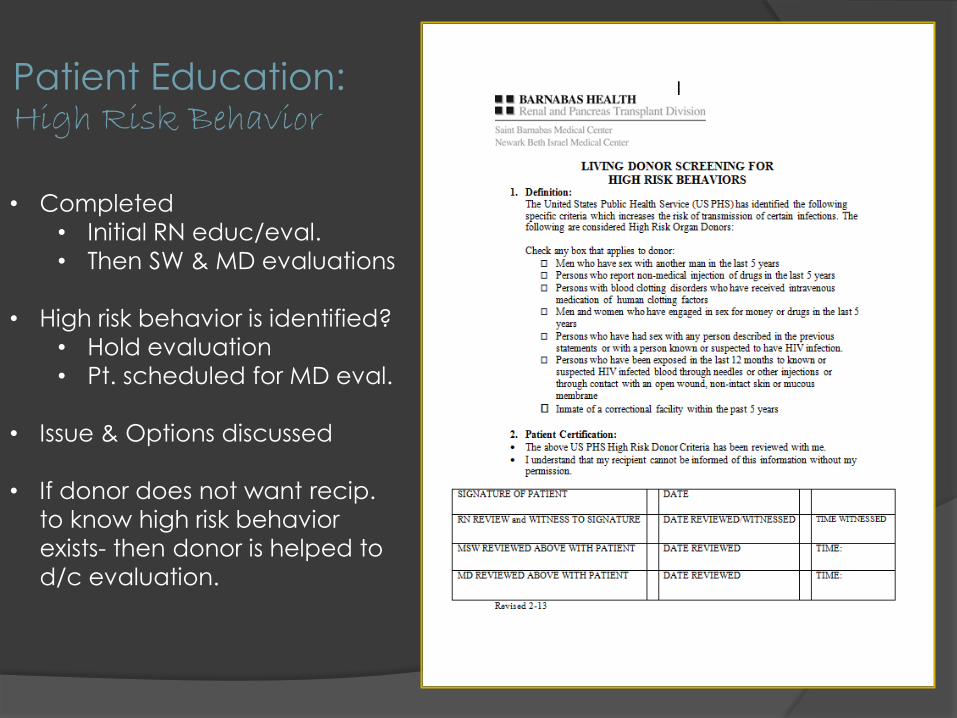
Patient Education: High Risk Behavior
• Completed
• Initial RN educ/eval.
• Then SW & MD evaluations
• High risk behavior is identified?
• Hold evaluation
• Pt. scheduled for MD eval.
• Issue & Options discussed
• If donor does not want recip.
to know high risk behavior
exists- then donor is helped to
d/c evaluation.
Summary of Steps to Exchange:
Identify Incompatible Pair
Educate
Consent
Verify & maintain recipient health status
Workup Donor
Registry Listing
Advanced Matching Strategies
Match offers & acceptance
Cross-matches
Finalize recipient & donor
preadmission testing
Surgical date &
logistic agreements
Donation/Transplant
Identify & Track Pairs Early & repetitive education of alternative programs
Incompatible does not mean „goodbye‟
Educate recipients to alternative programs at first evaluation visit
Educate donors to alternative programs before cxm
○ esp. when recip sensitized
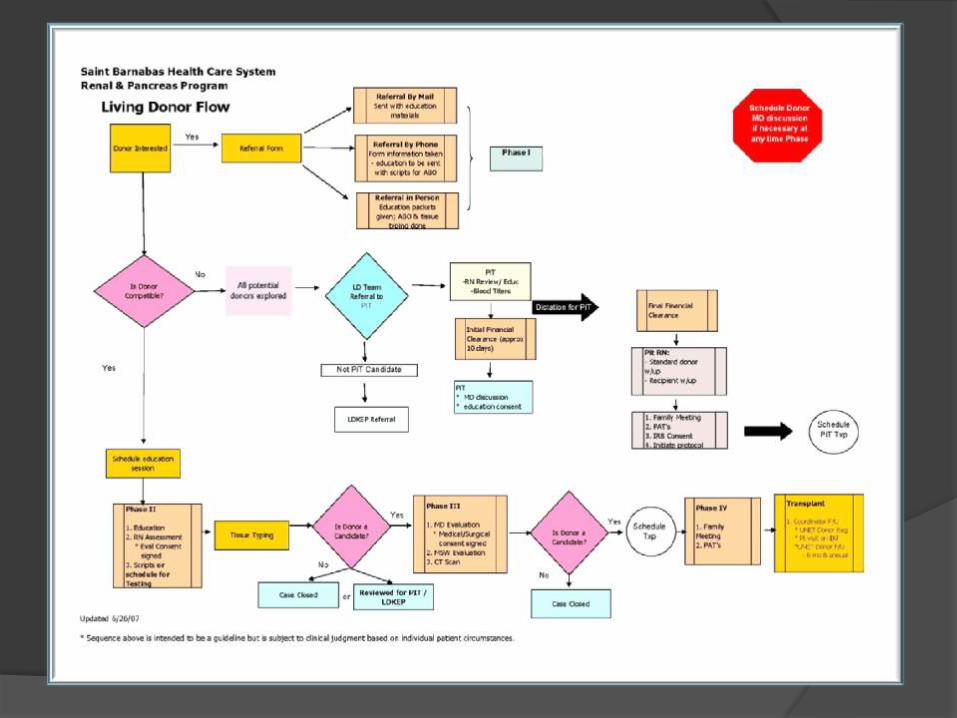
Flowchart to guide patient & decision pathway
Does everyone know what the next step is
Educate the LD Team with tools needed
give pairs basic info
System to communicate pair to exchange expert RN
Develop record keeping method
Regular meetings to review incompatible pairs
Identify & Track Pairs
Follow up with incompatible pairs immediately
Too much time – lose donor
Donor offered option of alternative program by exchange/incompatible expert RN
If donor agreeable to learn more, recip notified
If pair receives incompatibility info from confused staff member:
may lose pair and/or
pair is frightened of program/lose trust in process
Important to:
call all incompatible pairs to review incompatibly
meet with them for in-depth education session
inspire confidence/reasonable hope
Patient Educational Materials
KPD Educational Tools
UNOS Consents: 3 Forms
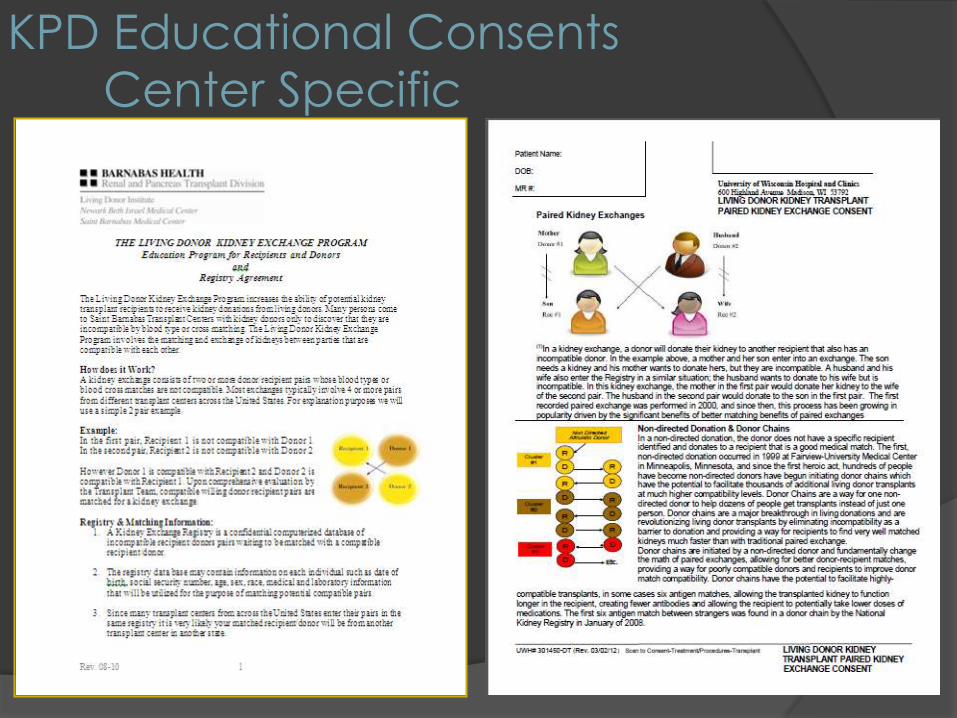
KPD Educational Consents
Center Specific
Education Tools: Fact Sheet
Pathways & Protocols
Education & Consenting Review your plan:
Standard education program for donors & recipients
Exchange Program Fact Sheet/Brochures
Center KPD Educational Consent
UNOS KPD Consents (if in UNOS registry)
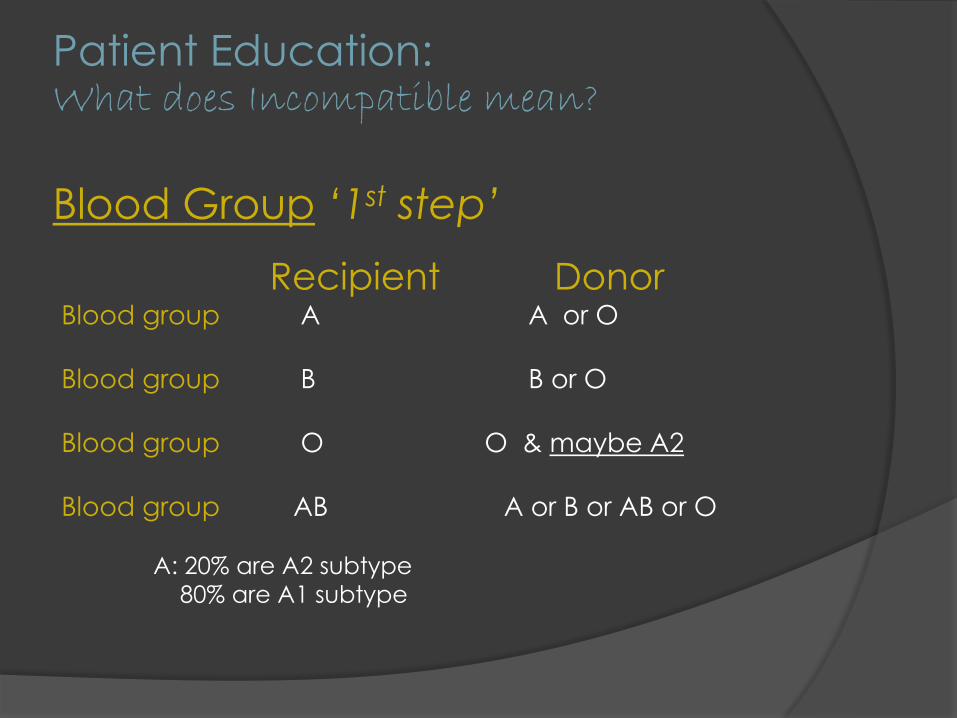
Patient Education: What does Incompatible mean?
Blood Group ‘1st step’
Recipient Donor Blood group A A or O
Blood group B B or O
Blood group O O & maybe A2
Blood group AB A or B or AB or O
A: 20% are A2 subtype
80% are A1 subtype
Patient Education: What does Incompatible mean?
Crossmatch ‘2nd step’
Basics of HLA: Human Leukocyte Antigens
Unique protein markers on almost all cells of our body
○ Make you who you are
○ That‟s how your body knows it not your kidney even
though same blood group
When kidney connected blood goes through and like a
credit card swipe immune system records the new proteins
○ Make antibodies
○ Will be incompatible with another human who has those proteins
you have been exposed to before
PRA %: „line up 100 people with same blood type…‟
Patient Education „basics‟ Blood Groups: New Science
We have antibodies against other blood groups
O‟s have Anti-A and Anti-B antibodies
A‟s have Anti B-antibodies & B‟s have Anti-A antibodies
Measured in titers
Titer 1:2, 1:4, 1:8, 1:16, 1:32 doubles each time…
1:32 stronger then 1:16
How many times does it take to wash out that stain?
Antibodies removed by plasmapheresis & IVIG
Typically 4 pre-op and 3 post-op
A2 blood group very similar to O blood group
Almost a compatible transplant in some cases
Patient Education Kidney Exchange or Incompatible Transplant ?
Blood group incompatible transplants
It is may be now possible to overcome in the blood group
barrier
○ Especially A2 donor to O recipient
Crossmatch incompatible transplants
some Positive crossmatches can be overcome
Kidney Exchange for Compatible transplant
What is the right treatment option?
Incompatible or Exchange?
A Painful Case Study A lesson in education & timing
Lori: 29 y.o. BG „O‟ PRA 47%
1st txp from Mom at age 15
Chronic allograph nephropathy
after 14 years with 1st txp – back on HD
Friend donor BG „O‟
+ crossmatch Needs full High Risk Incompatible Treatments
Formal incompatible education delayed –
donor started workup
A Case Study: A lesson in education & timing
In meeting – I realize Exchange is more
ideal -I call recipient to discuss ○ She‟s excited
Donor calls me the next day ○ She‟s furious
Formal incompatible education
scheduled ASAP with recipient & donor
A Case Study: A lesson in education & timing
Recipient realizes extent of desensitization &
wants exchange
Donor wants to directly donate via
incompatible transplant
Friendship in turmoil
Donor changes mind on donation
Transplant cancelled
Education:
Anonymity & Confidentiality
Pairs remain anonymous prior to kidney donation Avoid non medical based opinions
Anonymity cannot be guaranteed Safety over anonymity
Unidentifiable patient data compiled for future analysis
for purposes of understanding processes and improving
exchange transplantation.
Donor Workup in Kidney Exchange:
Donor medical record scrutinized by receiving ctr.
Variations exist on donor clearance
Nephrolithiasis – kidney stones
Microscopic hematuria
Hypertension
Hepatitis B core +
Renal anatomy
○ Multiple arteries
○ Right nephrectomy
Size of Txp Program
○ Low volume center more conservative
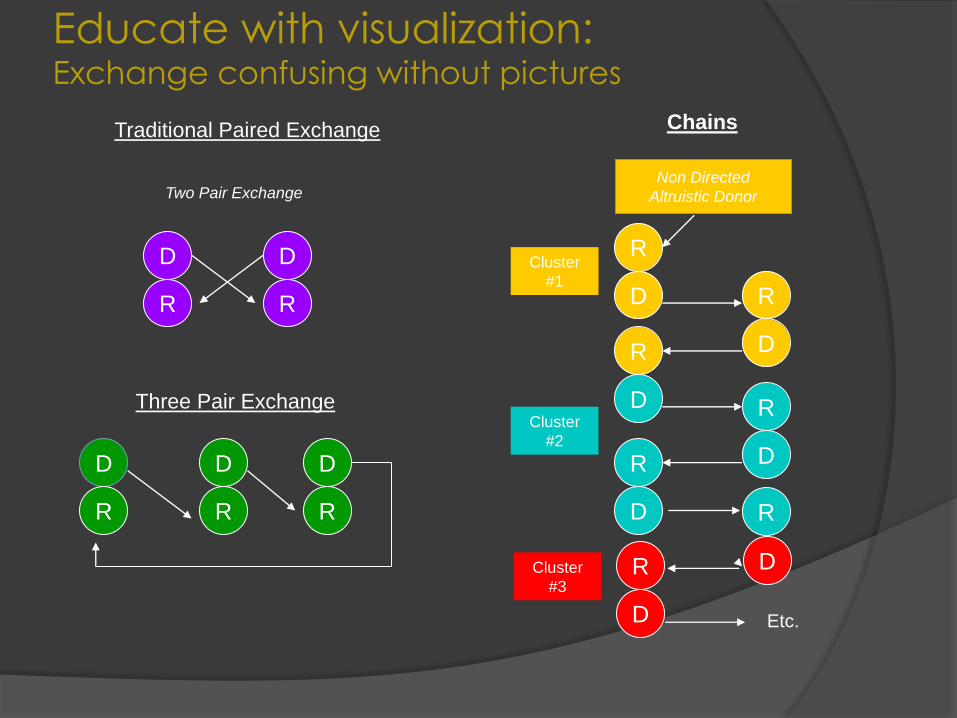
Educate with visualization: Exchange confusing without pictures
Traditional Paired Exchange Chains
Two Pair Exchange
Three Pair Exchange
Non Directed
Altruistic Donor
D D
R R
D D D
R R R
D R
D R
D R
D R
D
Cluster
#1
Cluster
#2
R
R
R
D
D
Etc.
Cluster
#3
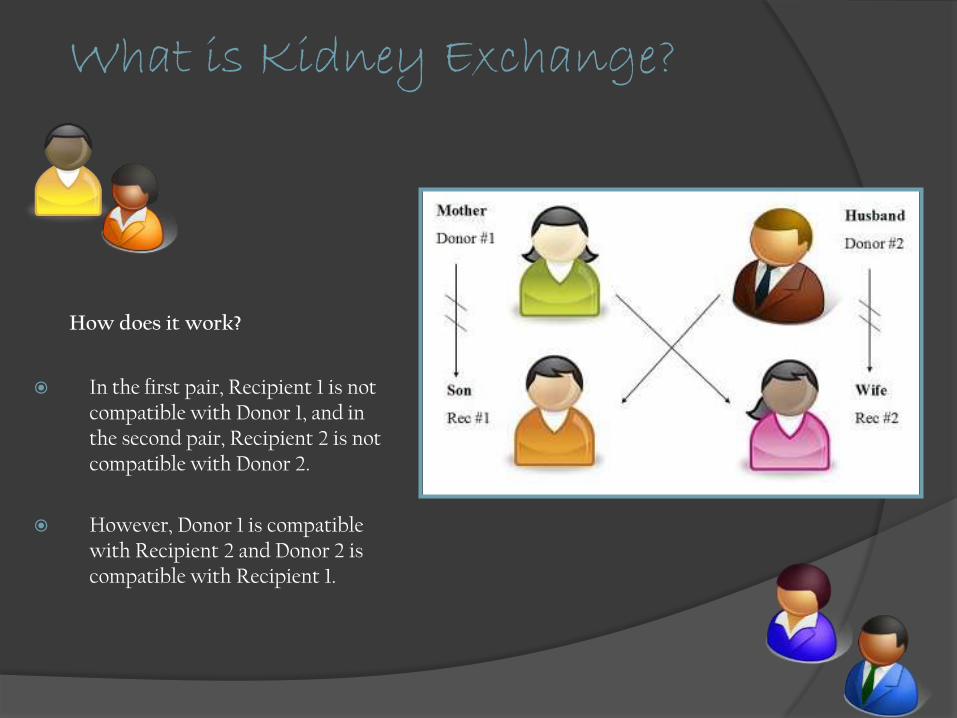
What is Kidney Exchange?
How does it work?
In the first pair, Recipient 1 is not compatible with Donor 1, and in the second pair, Recipient 2 is not compatible with Donor 2.
However, Donor 1 is compatible with Recipient 2 and Donor 2 is compatible with Recipient 1.
Education: Registry & Matching Info:
What is a Kidney Exchange Registry?
Which ones do we utilize
What info does it contain?
You will likely be matched with a donor/recipient
in another state
What will you be told about your match donor or
recipient
Your donor medical record – when is it sent to the
other center?
Education: Exchange and Incompatible Transplantation
Incompatible kidney exchange:
May be their best option
Unable to find a completely compatible exchange
For incompatible txp
An additional educational session & consent
Specific to treatments & risk of that incompatible txp
Has personalized protocol
Education: Surgery Schedule & Travel Information:
When possible kidney donations will occur
simultaneously or as close to the same time as possible
to ensure that no donor reneges.
There are some exceptions
Time zone changes
The donated kidneys are sent via ground or air
transportation.
Education: Risks of Shipped Kidney:
The following risks exist any time organs are
shipped for transplant:
Possible delay in function of organ caused by the extra
time it takes to transport a kidney between donor and
recipient institutions.
Accidental complete loss of organ due to transportation
accident between donor and recipient institutions.
It is the discretion of only the Transplant Surgeon and Team
to proceed with or stop surgical removal or
transplantation No recourse with UNOS
No Recourse with UNOS
Education: Transporting Kidneys What we do to keep them safe?
Specialized Courier: Arranges flights/backup flights
○ Charter flight in emergency
Transport kidney to/from airport
○ Communicates pickup/in transit/arrival ETA
Knows airport logistics –tendering kidney
Proprietary Hot Line to Airlines Control Centers & Management to:
○ pre-alert airlines, request lifeguard status and obtain real time information
GPS Kidney Tracking
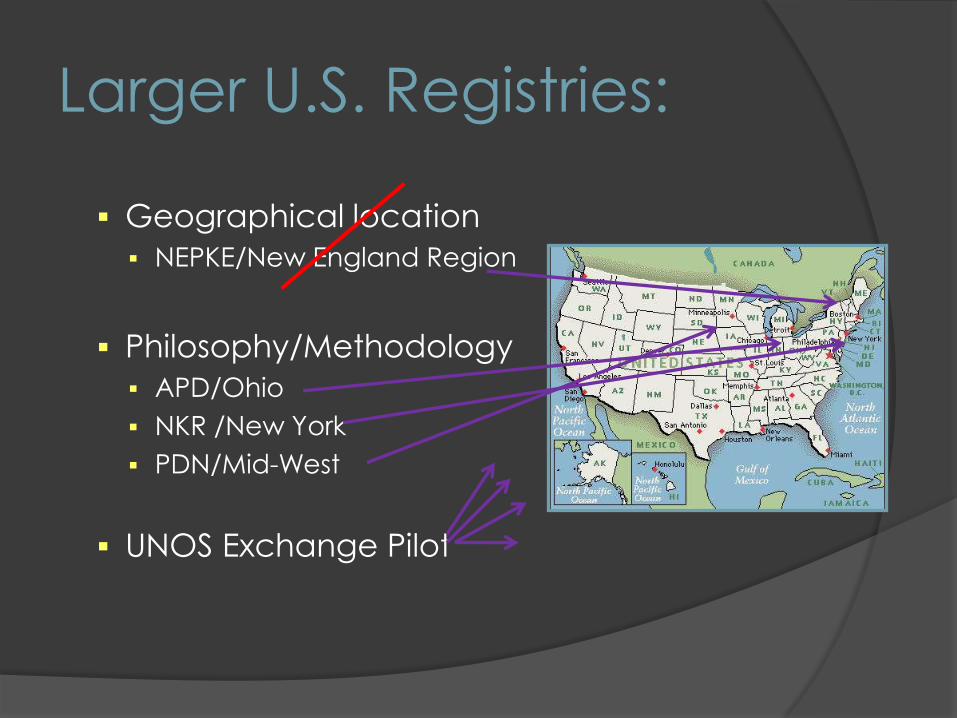
Larger U.S. Registries:
Geographical location
NEPKE/New England Region
Philosophy/Methodology
APD/Ohio
NKR /New York
PDN/Mid-West
UNOS Exchange Pilot
Utilizing Multiple Exchange Registries
Centers typically work with one registry
As gain experience – add another
registry
Matching is highly correlated with the
number of pairs within a matching
system/registry
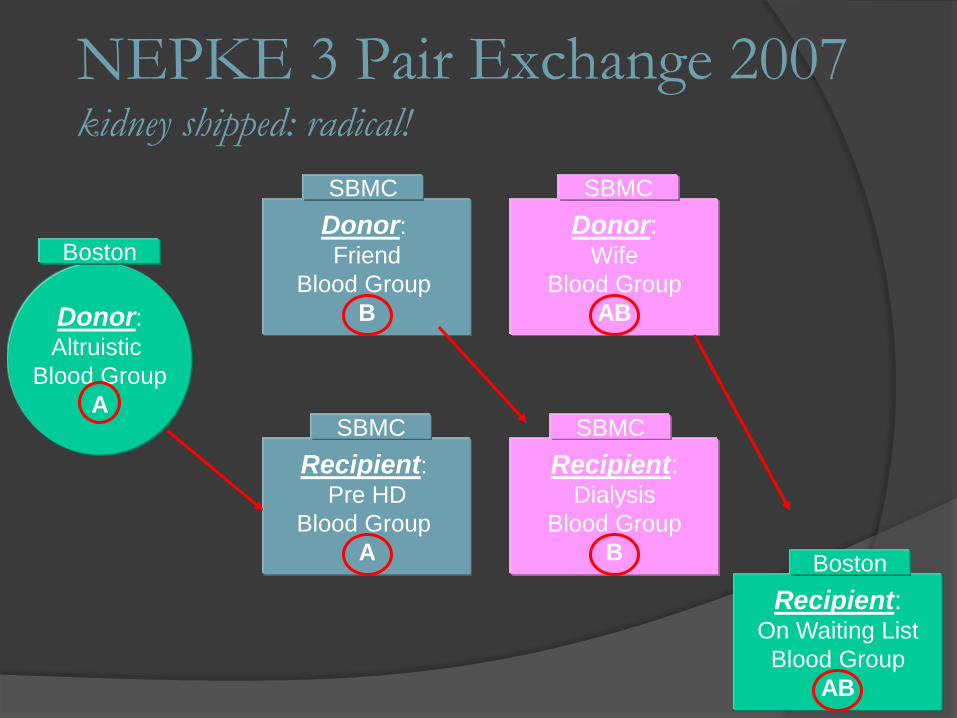
NEPKE 3 Pair Exchange 2007 kidney shipped: radical!
Donor:
Friend
Blood Group
B
Donor: Wife
Blood Group
AB
Recipient: Dialysis
Blood Group
B
Recipient: Pre HD
Blood Group
A
Donor:
Altruistic
Blood Group
A
Recipient: On Waiting List
Blood Group
AB
Boston
SBMC
Boston
SBMC
SBMC
SBMC

Donors & Recipients NDD
A
Waitlist
Recipient
AB
Exchange
Recipient
A
Exchange
Donor
AB
Exchange
Donor
B
Exchange
Recipient
B
Angela
Sung
Soon Robert Ben David
Practical Problems of Multi-Registry Participation
Data entry increased
Keeping organized Listing pair in multiple registries: how to choose?
Keeping track when activating/suspending pairs
Requirements of different registries Time consuming/Building new relationships
UNOS Pilot – new consents/additional diagnostics
Cost –some registries charge $$
Sustaining relationships: “you give the other registry all your „easy pairs‟ “
Multi-Registry Exchange:
Practical Approaches
If pair easy match
Choose registry with „local‟ txp centers
Limit data entry
Avoid matching in all registries simultaneously
List harder to match pairs in additional registries High PRA
O recipients

APD exchange April 2012
0 mm, 3rd Txp
November 2012
Compatible Pairs & Exchange
„Compatible Share‟
What compatible pairs are offered this program:
○ O donors with non-O recipients
○ No genetic advantage
Unless significant age mismatch
Why would you enter a compatible pair into the
exchange? ○ Age advantage – offer younger kidney
○ HLA advantage - improved match
○ Opportunity for Altruism to help incompatible pairs
We are still learning how to approach pairs
Very positive response
Internal matches
Why?
Non directed donor available
When have easier to match pairs
Registry „fatigue‟
Use of compatible pairs
○ Minimize risk to compatible pair
Still new concept for us
Takes time for full team buy-in
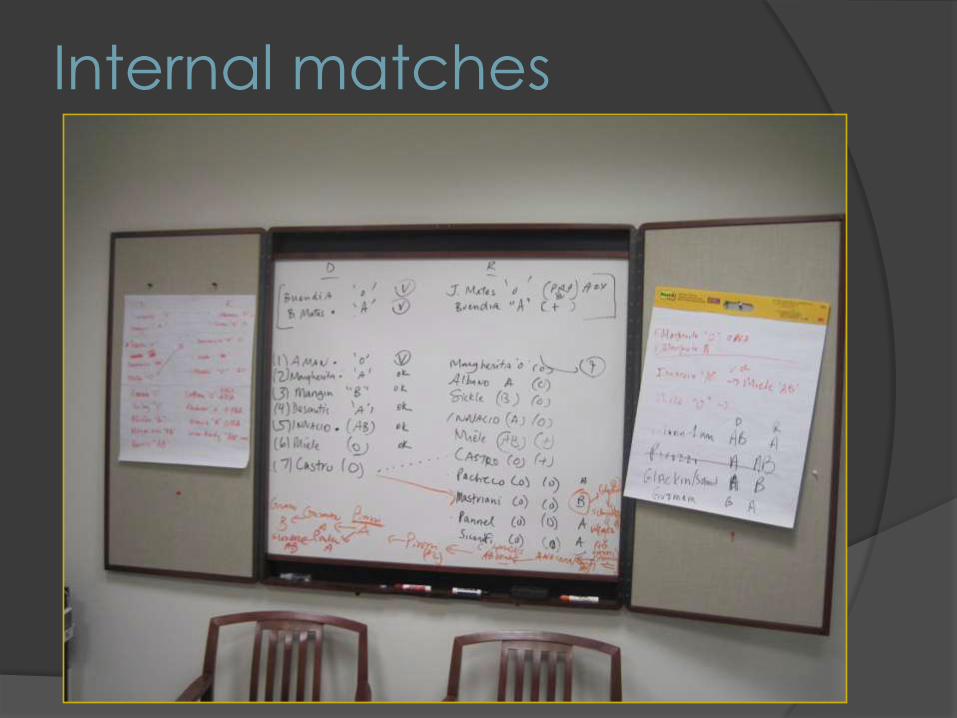
Internal matches
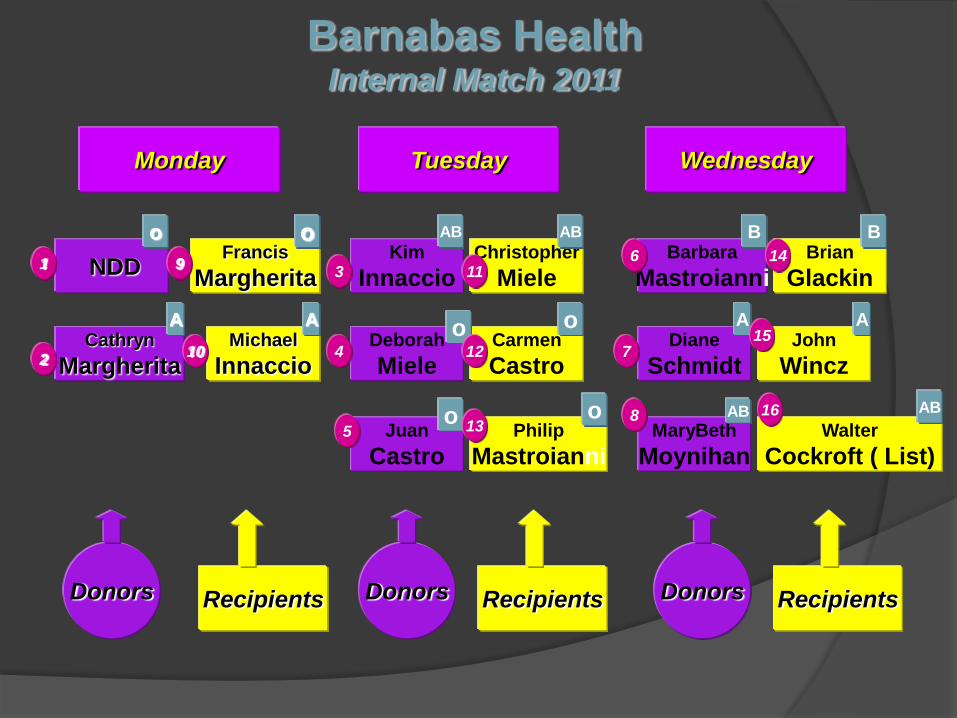
NDD Francis
Margherita
Cathryn
Margherita Michael
Innaccio
Kim
Innaccio Christopher
Miele
Deborah
Miele Carmen
Castro
Barbara
Mastroianni Brian
Glackin
Diane
Schmidt John
Wincz
MaryBeth
Moynihan Walter
Cockroft ( List) Juan
Castro Philip
Mastroianni
Monday Tuesday Wednesday
o
AB
B o
A A
AB
AB AB
A A
B
o o
o o
1
2
3
4
5
6
7
8
9
10
11
12
13
14
16
15
Donors Donors Donors Recipients Recipients Recipients
Barnabas Health Internal Match 2011

Internal Match December 2012
Internal matches
Response to:
More complicated national matches
Confines of registry rules
Cost of registry matches
○ $$$$ a txp – NKR & Sterling fees
Ease of internal
Minimal logistics/no shipping kidneys
No preservation/Minimal CIT
Should we do internal matches?
Facilitate more txp nationally?
Tracking Worksheets
Can be part of medical record
Barnabas Health
Chronological order of tasks
Johns Hopkins
Script of Events that need to occur
wih instructions
Johns Hopkins
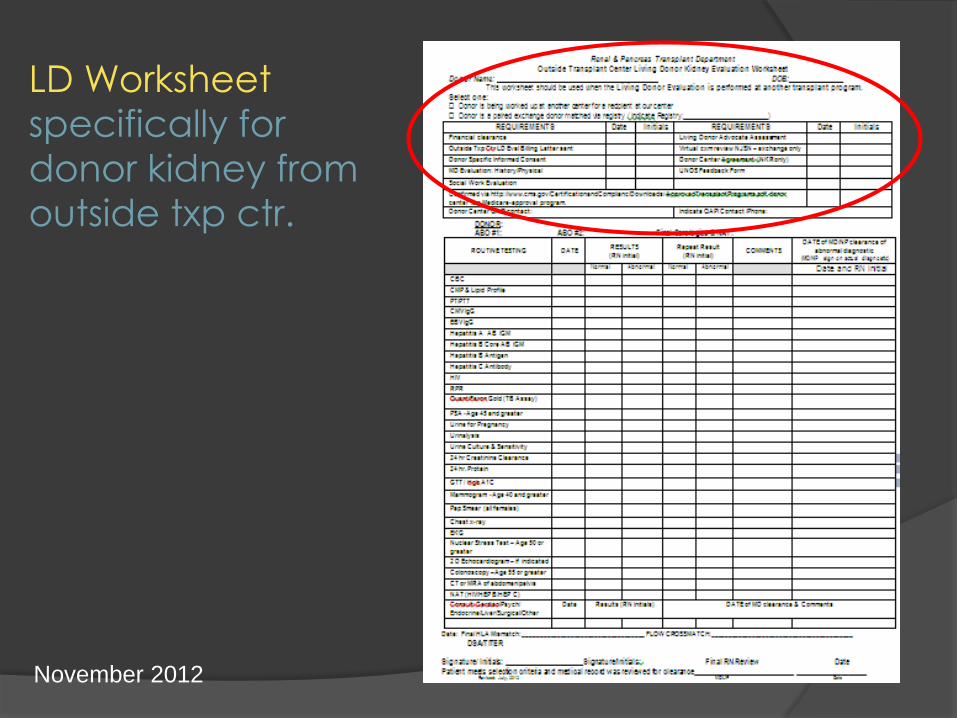
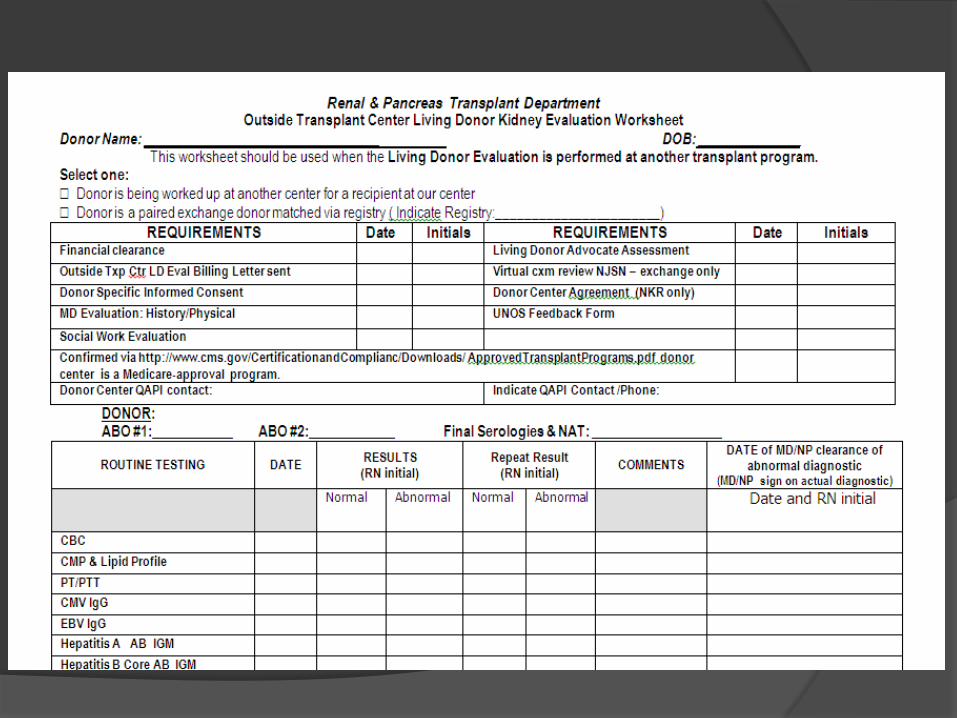
LD Worksheet
specifically for
donor kidney from
outside txp ctr.
November 2012
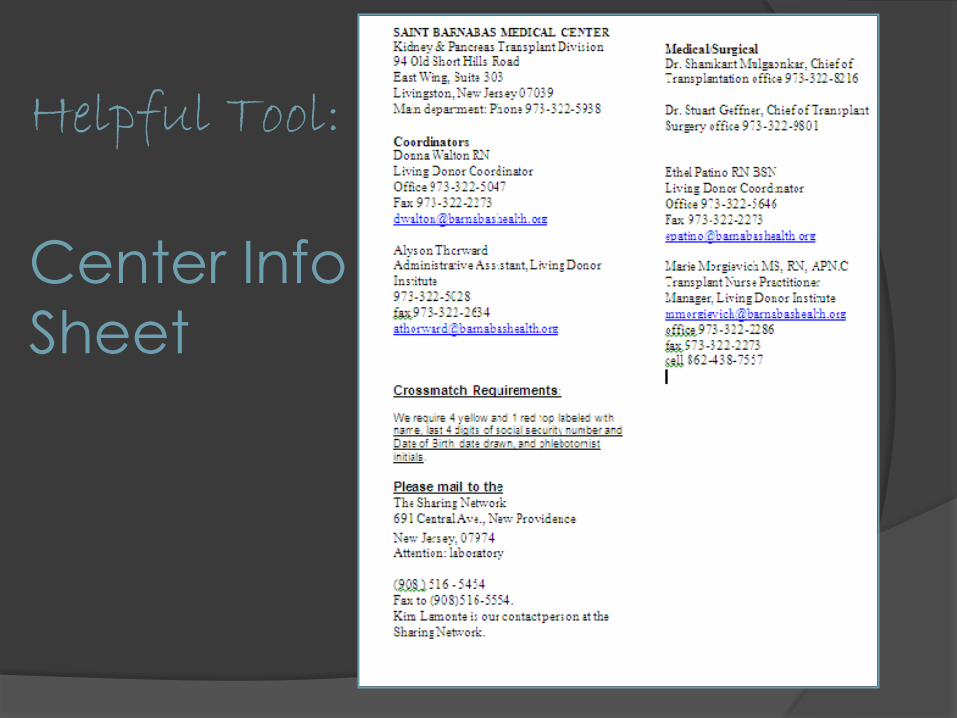
Helpful Tool:
Center Info
Sheet
Organizational Tool:
Create folder in INBOX
For each match: examples:
○ NKR chain 66 cluster 1
Keep all INBOX emails & important SENT emails in this folder
Scan donor records/other documents
Send via secure email to recipient center
Save this „sent‟ email in your INBOX exchange folder
Can remotely send record 24/7 to recipient center via blackberry or
other web access to your work email
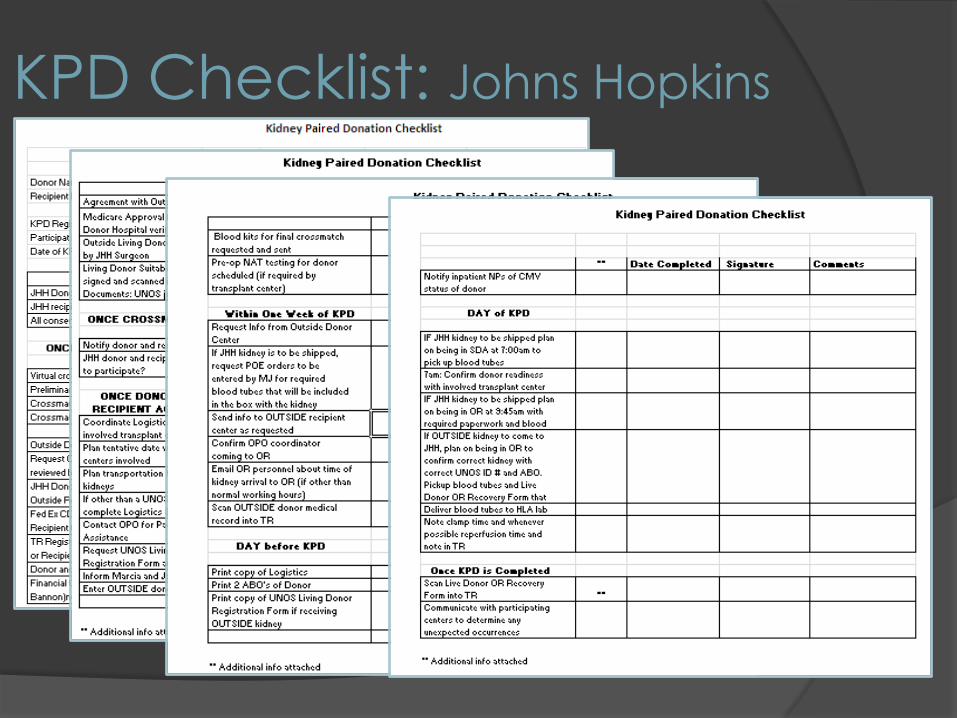
KPD Checklist: Johns Hopkins
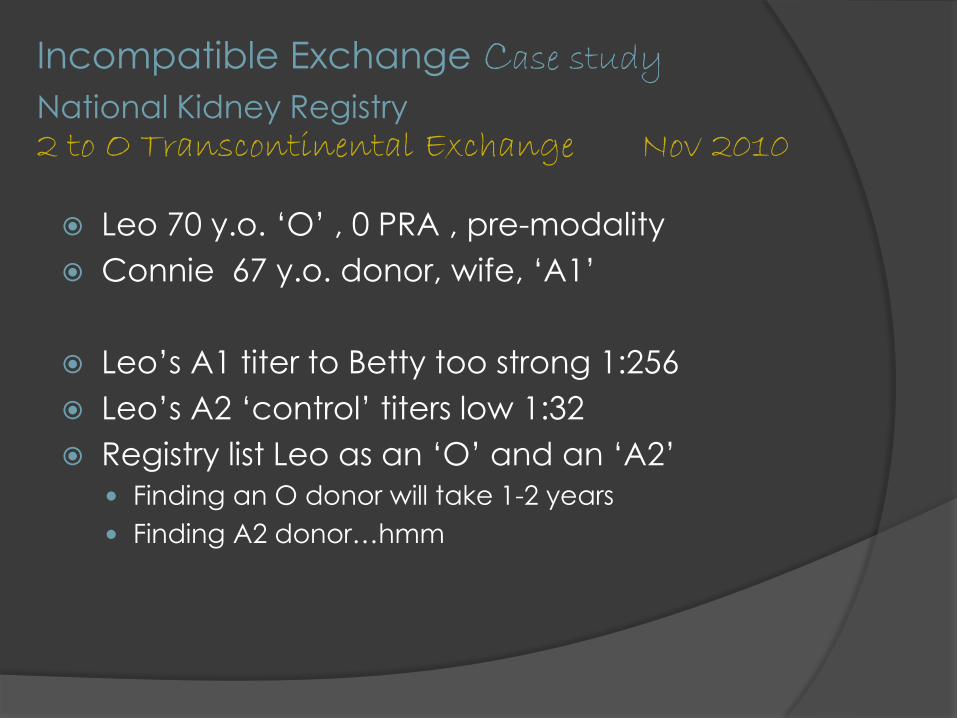
Incompatible Exchange Case study
National Kidney Registry 2 to O Transcontinental Exchange Nov 2010
Leo 70 y.o. „O‟ , 0 PRA , pre-modality
Connie 67 y.o. donor, wife, „A1‟
Leo‟s A1 titer to Betty too strong 1:256
Leo‟s A2 „control‟ titers low 1:32
Registry list Leo as an „O‟ and an „A2‟
Finding an O donor will take 1-2 years
Finding A2 donor…hmm
Incompatible Exchange Case study
A2 to O Transcontinental Exchange November 2010
Match offer 2 months
Jill 59 y.o. „A2‟
UCLA to Saint Barnabas: 12-14 hours cold ischemic time
Leo‟s A2 titers against Jill 1:32
Transplant scheduled
Plasmapheresis & IVIG: Mon, Tues, Wed & Thurs pre-op
○ Titers decreased to 1:2
○ Plasmapheresis & IVIG: Fri, Sat & Mon post-op
Leo‟s transplant functioned immediately: creatinine 1.3 & stable 3 years later
Was Leo happy?
Appreciative Patient: Leo
November 2012
Questions?
Please check NATCO website next
week for copies of all P&P, Patient
Education Materials and Worksheets
Contact Information
Marie Morgievich RN, APN.C, CCTC
Manager, Living Donor Institute
Transplant Nurse Practitioner
973-322-2286








![2020 PLUNGER TOOLKIT - Special Olympics€¦ · There are three easy ways to support my Plunge: 1. Online donation: Visit [insert personal donation page URL] 2. Offline donation:](https://img.pdfslide.us/doc/110x75/5f704b29e51e9a61aa28dcf1/2020-plunger-toolkit-special-olympics-there-are-three-easy-ways-to-support-my.jpg)



















