-
8/11/2019 To Plate or Not to Plate
1/64
Robert Southard, MDAssistant Professor of SurgeryBaylor College
of Medicine
-
8/11/2019 To Plate or Not to Plate
2/64
I have received speaking and consultation fees from Synthes and
BioMet
-
8/11/2019 To Plate or Not to Plate
3/64
30 yo man in MVC
Multiple rib fractures
-
8/11/2019 To Plate or Not to Plate
4/64
-
8/11/2019 To Plate or Not to Plate
5/64
30 yo man in MVC
Multiple rib fractures
Treated initially with epidural anesthesia
-
8/11/2019 To Plate or Not to Plate
6/64
30 yo man in MVC
Multiple rib fractures
Treated initially with epidural anesthesia
Pain limited ability to cough/use IS
Despite functioning epidural
Offered ORIF
-
8/11/2019 To Plate or Not to Plate
7/64
-
8/11/2019 To Plate or Not to Plate
8/64
-
8/11/2019 To Plate or Not to Plate
9/64
-
8/11/2019 To Plate or Not to Plate
10/64
-
8/11/2019 To Plate or Not to Plate
11/64
-
8/11/2019 To Plate or Not to Plate
12/64
-
8/11/2019 To Plate or Not to Plate
13/64
-
8/11/2019 To Plate or Not to Plate
14/64
100,000 patients admitted/year
Present in 10% of trauma admissions
Marker of significant blunt chest trauma
Associated with underlying injuries
Pulmonary contusion
Solid organ injury
-
8/11/2019 To Plate or Not to Plate
15/64
Recognized as an injury pattern afterinvention of automobile
Up to 80% mortality
-
8/11/2019 To Plate or Not to Plate
16/64
Fracture of 3 or more contiguous ribs in 2 ormore places
-
8/11/2019 To Plate or Not to Plate
17/64
Paradoxical movement of segment of chestwall
http://ps.cnis.ca/wiki/images/5/57/Chapter_65_Image_10_Web_Size.jpg
-
8/11/2019 To Plate or Not to Plate
18/64
Pulmonary Toilet
Pain control
Positive pressure ventilation
-
8/11/2019 To Plate or Not to Plate
19/64
Pulmonary Toilet
Pain control
Positive pressure ventilation
Anatomic correction unnecessary
-
8/11/2019 To Plate or Not to Plate
20/64
1990
-
8/11/2019 To Plate or Not to Plate
21/64
2001
-
8/11/2019 To Plate or Not to Plate
22/64
2014
-
8/11/2019 To Plate or Not to Plate
23/64
High mortality prompted attempts at therapy
Internal Pneumatic Support
Tried and True
Anatomic Fixation Technology Searching for an Indication
-
8/11/2019 To Plate or Not to Plate
24/64
High mortality prompted attempts at therapy
Internal Pneumatic Support Avery E, et al. Severe crushing
injuries of the chest; a new method
of treatment with continuous hyperventilation by means
ofintermittent positive endotracheal insufflation. Q Bull
Northwest
Univ Med Sch. 1955;29(4):3013
Anatomic Fixation Jones T, Richardson E. Traction on the sternum
in the treatment of
multiple fractured ribs. Surg Gynec Obstet. 1926;42:283.
-
8/11/2019 To Plate or Not to Plate
25/64
Jones 1926 Traction applied with bulletforceps
-
8/11/2019 To Plate or Not to Plate
26/64
Jaslow 1946 Clothes hangerpercutaneously fixed to
sternum
-
8/11/2019 To Plate or Not to Plate
27/64
Heroy 1951 Traction with clamp applied tosternum
-
8/11/2019 To Plate or Not to Plate
28/64
Schrire 1963 Cape Town Limpet
Plunger applied externally
Traction on metal cross-bar
-
8/11/2019 To Plate or Not to Plate
29/64
Constantinescu 1965 Easily placed T-hooksecured in chest
External fixation
-
8/11/2019 To Plate or Not to Plate
30/64
Advantages
Restores chest volume
Improves respiratory mechanics
Disadvantages
Danger of placement
Infection
Mechanical failure
-
8/11/2019 To Plate or Not to Plate
31/64
Suturing Fractures
Suture
K wires
Reported as part of other descriptionsLikely high rate of
failure, though not reported
-
8/11/2019 To Plate or Not to Plate
32/64
Intramedullary fixation
Klassen 1949 Medullary pegs
Crutcher and Nolen 1956 Pins Paris 1975 IM struts
-
8/11/2019 To Plate or Not to Plate
33/64
Plates
Labitzke 1980
Titanium
-
8/11/2019 To Plate or Not to Plate
34/64
Restoration of chest volume beneficial
Success of external fixation and ORIF
-
8/11/2019 To Plate or Not to Plate
35/64
Early fixation systems
Case reports showed they could be effective
Mechanical failures may not have been reported
Difficulties with fixation of ribs
-
8/11/2019 To Plate or Not to Plate
36/64
Difficulties with fixation of ribs
Thin walled
Bicortical screws necessary Neurovascular bundle
Plates wrapping around inferior border
Fear of devascularization
Possibility of nerve impingement
Constant motion of ribs
Failure using stiff plates
-
8/11/2019 To Plate or Not to Plate
37/64
Plates
Casali 2005
Judet plates Sanchez plates
-
8/11/2019 To Plate or Not to Plate
38/64
Acute Innovations
Inion OTPS
-
8/11/2019 To Plate or Not to Plate
39/64
STRATOS
Synthes MatrixRIB
BioMet
-
8/11/2019 To Plate or Not to Plate
40/64
Is this a technology looking for an indication?
Historically risk-benefit ratio favored internalpneumatic
stabilization
-
8/11/2019 To Plate or Not to Plate
41/64
Tanaka, et al Trauma 2002
37 Patients
Randomized on Day 5 Repaired Ribs 4-10
Pneumatic Stabilization Control
Surgical Stabilization of Internal Pneumatic Stabilization? A
Prospective Randomized Study of Management
of Severe Flail Chest Patients. H. Tanaka et al. J Trauma. 2002
Apr; 52(4):727-32
-
8/11/2019 To Plate or Not to Plate
42/64
Tanaka, et al Trauma 2002
-
8/11/2019 To Plate or Not to Plate
43/64
Tanaka, et al Trauma 2002
-
8/11/2019 To Plate or Not to Plate
44/64
Tanaka, et al Trauma 2002
-
8/11/2019 To Plate or Not to Plate
45/64
Granetzny et al ICVTS 2005
40 Patients
Fixation at 24 to 36 hours after injury Used Kirschner wires
Strapping and packing control
Surgical versus conservative treatment of flail chest.
Evaluation of the pulmonary status. A Granetzny et al.
Interact Cardiovasc Thorac Surg. 2005 Dec;4(6):583-7
-
8/11/2019 To Plate or Not to Plate
46/64
Granetzny et al ICVTS 2005
-
8/11/2019 To Plate or Not to Plate
47/64
Marasco et al JACS 2013
46 Patients
Vent dependent with flail chest Fixation at day 4 to 5
(mean)
Used Inion system biodegradable plates/screws
Only fixed 1 fracture in flail segment
Nonoperative management control
Protocolized extubation criteria in both arms
Prospective randomized controlled trial of operative rib
fixation in traumatic flail chest. SF Marasco et al. J
Am Coll Surg. 2013 May;216(5):924-32
-
8/11/2019 To Plate or Not to Plate
48/64
Marasco et al JACS 2013Outcomes Operative
group (n = 23)Nonoperative group(n = 23)
p Value
Duration of IMVpostrandomization,
h, mean SD
151.8 83.1 181.0 130.2 0.37
Total ICU stay, h,median (IQR)
324 (238380) 448 (323647) 0.03
Failed extubation,n (%)
3 (13) 1 (4) 0.61
Readmission toICU, n (%) 2/23 (9) 2/23 (9) 0.99
Pneumonia, n (%) 11/23 (48) 17/23 (74) 0.07
Duration ofhospital stay, d,median (IQR)
20 (1828) 25 (1838) 0.24
In hospital
mortality, n
0 1 0.87
-
8/11/2019 To Plate or Not to Plate
49/64
Marasco et al JACS 2013Outcomes Operative
group (n = 23)Nonoperative group(n = 23)
p Value
Duration of IMVpostrandomization,
h, mean SD
151.8 83.1 181.0 130.2 0.37
Total ICU stay, h,median (IQR)
324 (238380) 448 (323647) 0.03
Failed extubation,n (%)
3 (13) 1 (4) 0.61
Readmission toICU, n (%) 2/23 (9) 2/23 (9) 0.99
Pneumonia, n (%) 11/23 (48) 17/23 (74) 0.07
Duration ofhospital stay, d,median (IQR)
20 (1828) 25 (1838) 0.24
In hospital
mortality, n
0 1 0.87
-
8/11/2019 To Plate or Not to Plate
50/64
Marasco et al JACS 2013Outcomes Operative
group (n = 23)Nonoperative group(n = 23)
p Value
Duration of IMVpostrandomization,
h, mean SD
151.8 83.1 181.0 130.2 0.37
Total ICU stay, h,median (IQR)
324 (238380) 448 (323647) 0.03
Failed extubation,n (%)
3 (13) 1 (4) 0.61
Readmission toICU, n (%) 2/23 (9) 2/23 (9) 0.99
Pneumonia, n (%) 11/23 (48) 17/23 (74) 0.07
Duration ofhospital stay, d,median (IQR)
20 (1828) 25 (1838) 0.24
In hospital
mortality, n
0 1 0.87
-
8/11/2019 To Plate or Not to Plate
51/64
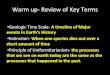
Marasco et al JACS 2013
Cost Analysis
Non-operative 5.17 more ICU days x $4,109/day
$21,243
Operative costs (OR time + Implants)
$6,800
Net savings
$14,443
-
8/11/2019 To Plate or Not to Plate
52/64
Leinicke et al Annals of Surgery 2013
Meta-analysis
Identified 9 comparative trials
Operative Management of Rib Fractures in the Setting of Flail
Chest: A Systematic Review and Meta-
Analysis. JA Leinicke et al. Ann Surg. 2013 Mar 18 (Epub)
-
8/11/2019 To Plate or Not to Plate
53/64
Leinicke et al Annals of Surgery 2013
-
8/11/2019 To Plate or Not to Plate
54/64
Leinicke et al Annals of Surgery 2013
-
8/11/2019 To Plate or Not to Plate
55/64
Leinicke et al Annals of Surgery 2013
-
8/11/2019 To Plate or Not to Plate
56/64
Leinicke et al Annals of Surgery 2013
-
8/11/2019 To Plate or Not to Plate
57/64
Not technology looking for an indication
Evolution of technology over time
Historically risk-benefit ratio favored internalpneumatic
stabilization
Recent advances may have shifted this balance
-
8/11/2019 To Plate or Not to Plate
58/64
Non-union
Severely displaced fractures
Failure of non-operative therapy
-
8/11/2019 To Plate or Not to Plate
59/64
Prospective study of 24 patients
3 months or more after injury
Resection of pseudoarthrosis, with plating ifdefect
-
8/11/2019 To Plate or Not to Plate
60/64
203 patients with rib fracture
7% had flail segments
Chronic pain in 22%
Decreased functional status in 53%
No identifiable injury characteristics predictive ofchronic
pain
The contribution of rib fractures to chronic pain and
disability. Gordy S, Fabricant L, Ham B, Mullins R,
Mayberry J. Am J Surg. 2014 May;207(5):659-62
-
8/11/2019 To Plate or Not to Plate
61/64
Nine case reports/series
Low complication rate
Many patients lost to follow up Patients reported decreased pain
postoperatively
-
8/11/2019 To Plate or Not to Plate
62/64
Little data
Delaying repair increases difficulty of case
Further trials needed to identify who is likelyto fail
non-operative therapy and benefit
from ORIF
-
8/11/2019 To Plate or Not to Plate
63/64
Flail chest
Yes
Severely displaced fractures
Not routinely, unless.
-
8/11/2019 To Plate or Not to Plate
64/64
Failure of non-operative therapy
Yes, but when????
Non-union
Maybe
![Home [] T6 decor plate ACC400 Universal wall plate Not only does the universal wall plate simplify the installation of the T6 wired thermostat, it offers](https://img.pdfslide.us/doc/110x75/5aaf9c307f8b9aa8438d82b6/home-t6-decor-plate-acc400-universal-wall-plate-not-only-does-the-universal.jpg)