Embed Size (px)
Citation preview

The Toronto Crown and Bridge Study ClubToronto, Ontario, Canada
September 25, 2020
“Management considerations for Temporomandibular Disorders Part 2”
byJeffrey P Okeson, DMD
Professor and DeanFounder, Orofacial Pain Program
Provost's Distinguished Service Professor University of Kentucky College of Dentistry
Lexington, Kentucky [email protected]
jeffokeson.net
1
I. Masticatory Muscle Disorders1. Protective Co-Contraction2. Local Muscle Soreness3. Myofascial Pain4. Myospasm5. Chronic Centrally Mediated Myalgia
II. Temporomandibular Joint Disorders1. Derangements of the Condyle-Disc Complex
a. Disc Displacement with Reductionb. Disc Displacement without Reduction
2. Structural Incompatibilities3. Inflammatory Disorders
Classification of Temporomandibular Disorders
2
Muscle PainMuscle pain is the most common type of pain
humans experience.
3
Muscle PainMuscle pain is the most common type of pain
humans experience.
Chronic muscle pain affects between11–24% of the world’s population
Cimmino et al. 2011
In the U.S. chronic pain are estimated to incur an economic burden of $500 billion dollars annually.
Miranda et al. 2010
4
We dentists have been trained to think of muscle pain as a consequence of an anatomic variation.
Muscle Pain
Malocclusion Incorrect joint position
5
Or ....we think about muscle pain as it relates to parafunction (bruxism, clenching, tooth wear).
Muscle Pain
Awake Time ClenchingSleep Related Bruxing
6

Or ....we think about muscle pain as it relates to parafunction (bruxism, clenching, tooth wear).
Muscle Pain
7
We dentists have developed many concepts regarding the etiology of muscle pain.
How valid are the data?
The data have been classically based on patient report and clinical observations.
8
We dentists have developed many concepts regarding the etiology of muscle pain.
How valid are the data?
The data have been classically based on patient report and clinical observations.
Current data is based on real time activity in a sleep lab.
9
1. TMD patients report more bruxing activity than controls.
Self-report of bruxism:55% of TMD patients report they bruxonly 15% of controls report they brux
Raphel et al. Sleep bruxism and myofascial pain TMD. JADA:143(11):1223-1231.2012
TRUE
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
10
1. TMD patients report more bruxing activity than controls.2. TMD patients actually brux more than controls.
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
Results of 2 nights in sleep studies:9.7 % of TMD patients showed bruxism10.9% of the controls showed bruxism (RMMA index of 1.7 events per 1.5 hours)
- no statically significant difference -
Raphel et al. Sleep bruxism and myofascial pain TMD. JADA:143(11):1223-1231.2012
TRUE
FALSE
11
1. TMD patients report more bruxing activity than controls.2. TMD patients actually brux more than controls.3. There is a correlation between the magnitude of tooth wear and
bruxing activity.
Lavigne, et al. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehab. 35:7: 476-495, 2008.
There is no difference in the magnitude of tooth wear and the amount of bruxing activity observed in a sleep lab.
TRUE
FALSE
FALSE
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
12

1. TMD patients report more bruxing activity than controls.2. TMD patients actually brux more than controls.3. There is a correlation between the magnitude of tooth wear and
bruxing activity.4. There is a strong correlation between tooth wear and RMMA
(rhythmic masticatory muscle activity).
Lavigne, et al. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehab. 35:7: 476-495, 2008.
There is no correlation between tooth wear and RMMA observed in a sleep lab.
TRUE
FALSE
FALSE
FALSE
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
13
1. TMD patients report more bruxing activity than controls.2. TMD patients actually brux more than controls.3. There is a correlation between the magnitude of tooth wear and
bruxing activity.4. There is a strong correlation between tooth wear and RMMA
(rhythmic masticatory muscle activity).5. There is a strong correlation between bruxing activity and pain.
Lavigne, et al. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehab. 35:7: 476-495, 2008.
There is no correlation between pain and RMMA observed in a sleep lab.
TRUE
FALSE
FALSE
FALSE
FALSE
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
14
1. TMD patients report more bruxing activity than controls.2. TMD patients actually brux more than controls.3. There is a correlation between the magnitude of tooth wear and
bruxing activity.4. There is a strong correlation between tooth wear and RMMA
(rhythmic masticatory muscle activity).5. There is a strong correlation between bruxing activity and pain.6. Patients who have pain have higher resting EGM activity.
Studies demonstrate that there are no differences in EMG activity between masticatory muscle pain patients and controls.
Yemm 1985Majewski 1984 Carlson, 1993Maillou, 1997Sevensson, 2004
TRUE
FALSE
FALSE
FALSE
FALSEFALSE
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
15
1. TMD patients report more bruxing activity than controls.2. TMD patients actually brux more than controls.3. There is a correlation between the magnitude of tooth wear and
bruxing activity.4. There is a strong correlation between tooth wear and RMMA
(rhythmic masticatory muscle activity).5. There is a strong correlation between bruxing activity and pain.6. Patients who have pain have higher resting EGM activity.7. Patients who brux more, have more pain.
Self-reported bruxers (cut off 4 episodes of RMMA an hour)Low frequency bruxers had more pain than the high frequency bruxers.
- Rompre et al, J of Dent Res, 2007
TRUE
FALSE
FALSE
FALSE
FALSEFALSEFALSE
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
16
1. TMD patients report more bruxing activity than controls.2. TMD patients actually brux more than controls.3. There is a correlation between the magnitude of tooth wear and
bruxing activity.4. There is a strong correlation between tooth wear and RMMA
(rhythmic masticatory muscle activity).5. There is a strong correlation between bruxing activity and pain.6. Patients who have pain have higher resting EGM activity.7. Patients who brux more, have more pain.
TRUE
FALSE
FALSE
FALSE
FALSEFALSEFALSE
Perhaps we need to begin to rethink muscle pain.
Common beliefs regarding bruxism, tooth wear, EMG and pain- Facts or Fiction ? -
17
In order to successfully treat muscle pain we need to understand normal muscle function and what factors lead to pain.
Muscle Pain
We need to think physiologically….….not dentally
18

Masticatory Muscle PainWhat is it?
What causes it?
SpasmAn involuntary, CNS induced tonic
contraction, often associated with local metabolic conditions.
Cramp
19
Masticatory Muscle Pain
Cramp
spasm in a calf muscle
20
Masticatory Muscle PainWhat is it?
What causes it?
Spasm
Yet studies demonstrate that there are no differences in EMG activity
between masticatory muscle pain patients and controls.
Yemm 1985Majewski 1984 Carlson, 1993Maillou, 1997Sevensson, 2004
21
A Clinical Masticatory Muscle Model
Okeson 2012
22
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Regional Myalgic Disorders
Myofascial PainCentrally Mediated Myalgia
Systemic MyalgicDisorder
Fibromyalgia
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction
23
NormalFunction
A Masticatory Muscle Model
Okeson, 2012
AnEvent
An event can alter normal masticatory muscle function.
The eventmay be local
or The eventmay be central
24

1. Sudden or unusual alteration in sensory input.2. Deep pain input.
a. associated with local structuresb. idiopathic pain input
3. Trauma.a. local injuryb. excessive or unaccustomed usec. muscle, tendon, or ligament strain
Local Factors:
An Event
25
NormalFunction
A Masticatory Muscle Model
Okeson, 2012
AnEvent
An event can alter normal masticatory muscle function.
The eventmay be local
or The eventmay be central
26
Central Factors:
An Event
1. Increased levels of emotional stress.(an up regulation of the autonomic nervous system)
2. A down regulation of the descending inhibitory system.(systemic disorders, illness, fatigue, diet, etc.)
27
NormalFunction
A Masticatory Muscle Model
Okeson, 2012
AnEvent
ProtectiveCo-
contraction
If the event does not resolve, or is of significant consequence, the muscles respond with protective co-contraction.
28
PainProtective muscle co-contraction(muscle splinting)
29
NormalFunction
Resolution
A Masticatory Muscle Model
Okeson, 2012
AnEvent
ProtectiveCo-
contraction
If the event is eliminated or isof little consequence,
the protective co-contraction resolves.
Normal humanexperiences.
30
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
AnEvent
ProtectiveCo-
contraction
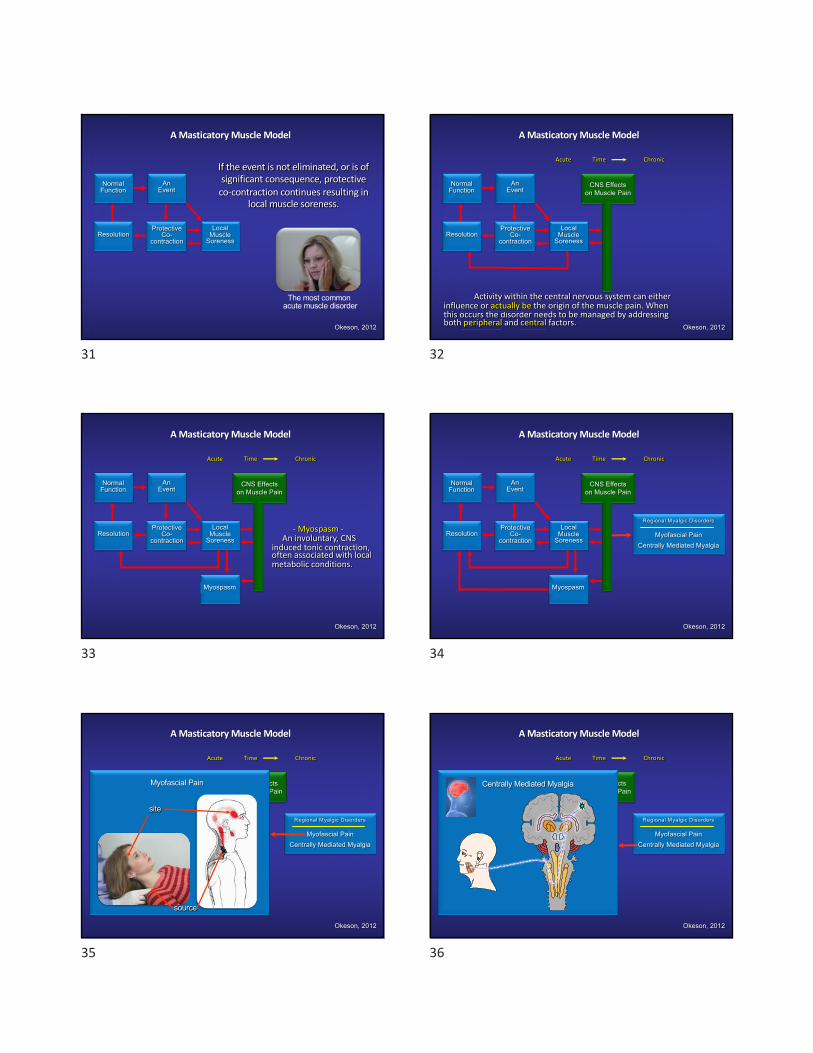
If the event is not eliminated, or is of significant consequence, protective
co-contraction continues resulting inlocal muscle soreness.
The most common acute muscle disorder
31
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Acute Time Chronic
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction
Activity within the central nervous system can either influence or actually be the origin of the muscle pain. When this occurs the disorder needs to be managed by addressing both peripheral and central factors.
32
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction- Myospasm -
An involuntary, CNS induced tonic contraction, often associated with local metabolic conditions.
33
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Regional Myalgic Disorders
Myofascial PainCentrally Mediated Myalgia
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction
34
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Regional Myalgic Disorders
Myofascial PainCentrally Mediated Myalgia
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction
Myofascial Pain
site
source
35
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Regional Myalgic Disorders
Myofascial PainCentrally Mediated Myalgia
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction
Centrally Mediated Myalgia
36

NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Regional Myalgic Disorders
Myofascial PainCentrally Mediated Myalgia
Systemic MyalgicDisorder
Fibromyalgia
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction
37
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Regional Myalgic Disorders
Myofascial PainCentrally Mediated Myalgia
Systemic MyalgicDisorder
Fibromyalgia
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
ProtectiveCo-
contraction
Fibromyalgia• Widespread muscular and joint pain.• The Wide Spread Pain Index (WPI).• The Symptom Severity Scale (SS).
• WPI of > 7 and SS of > 5• WPI of 3-6 and SS of > 9
• Lasting longer than three months.• There is no other explanation for the pain.
- Important Concept -This is not
a dental problem
38
NormalFunction
ResolutionLocal
MuscleSoreness
A Masticatory Muscle Model
Okeson, 2012
Regional Myalgic Disorders
Myofascial PainCentrally Mediated Myalgia
Systemic MyalgicDisorder
Fibromyalgia
Acute Time Chronic
Myospasm
CNS Effectson Muscle Pain
AnEvent
Managing Muscle Disorders takes some thinking.
ProtectiveCo-
contraction
ProtectiveCo-
contraction
1Local
MuscleSoreness
2
Myospasm
3
Myofascial Pain4
Fibromyalgia6
Important: They are all managed differently.
5 Centrally Mediated Myalgia
39
NormalFunction
Resolution
A Masticatory Muscle Model
Acute Time Chronic
AnEvent
ProtectiveCo-
contraction
Because of our limited time, we can only discuss the most common disorder.
Local Muscle Soreness1. Description2. Etiology3. History4. Examination findings5. Treatment
LocalMuscle
Soreness
40
A primary, non-inflammatory, myogenous pain condition.
- description -
Local Muscle Soreness
(muscle fatigue / over use)
41
1. Protracted co-contraction produces changes in the muscle tissue, such as fatigue, ischemia, resulting in the production of algogenic substances.
2. Deep pain input (may lead to “cyclic muscle pain”)3. Local tissue trauma
a. local injury (e.g. injections, strain)b. unaccustomed muscle use (e.g. bruxism, chewing
gum) (Delayed onset local muscle soreness)4. Increased levels of emotional stress
- etiology -
Local Muscle Soreness
42

1. The pain began several hours or days following an event associated with protective co-contraction. (e.g. altered sensory input, high crown)
2. Tissue injury (injections, opening wide, or unaccustomed muscle use - pain may be delayed).
3. Secondary to another source of the pain.4. Associated with an increased level of the emotional
stress.
- history -
Local Muscle Soreness
43
1. Structural dysfunction: a decrease in the velocity and range of mandibular movement. The full range of movement cannot be achieved by the patient. Passive stretching by the examiner can often achieve a more normal range of movement (soft end feel).
- clinical characteristics -
Local Muscle Soreness
2. Minimal pain at rest.3. Increased pain with function.4. Local tenderness to palpation.
44
The general goal of therapy is to reduce sensory input that can lead to cyclic muscle pain by:
1. Eliminate any ongoing altered sensory or proprioceptive input.2. Education patient and encourage physical self regulation.
a. decrease jaw use to within painless limits.b. stimulate proprioceptors with normal muscle use.c. promote emotional stress awareness / reduction.d. encourage reduction of non-functional tooth contacts
(cognitive awareness).3. Occlusal appliance therapy.4. Considered the use of mild analgesics. (ibuprofen 400mg tid)
- treatment -
Local Muscle Soreness
45
Expect results in 1-3 weeks.If the therapy is not successful, consider that either:
1. The etiologic factors are not being controlledor
- treatment -
Local Muscle Soreness
2. You have misdiagnosed the disorder.
MPD
46
Occlusal Appliance Therapy
TypeIndicationsFabricationClinical Protocol
47
The Stabilization Appliance
48

Occlusal Appliance Therapy
TypeIndicationsFabricationClinical Protocol
49
Local Muscle Soreness
Chronic Centrally Mediated Myalgia
Bruxism
The Stabilization Appliance
- Indications -
50
Occlusal Appliance Therapy
TypeIndicationsFabricationClinical Protocol
51
1. The appliance is stable and retentive.2. All the teeth contact evenly on flat surfaces in the
musculoskeletally stable position.3. Eccentric contacts are on the anterior teeth4. In the upright position, posterior teeth contact heavier
than the anterior teeth.5. The appliances smooth and polished.
Final Criteria for the Stabilization Appliance
52
Right lateral movement Left lateral movement
The Final Stabilization Appliance
53
The final mandibular stabilization appliance
Right lateral movement Left lateral movement
54
Occlusal Appliance Therapy
TypeIndicationsFabricationClinical Protocol
55
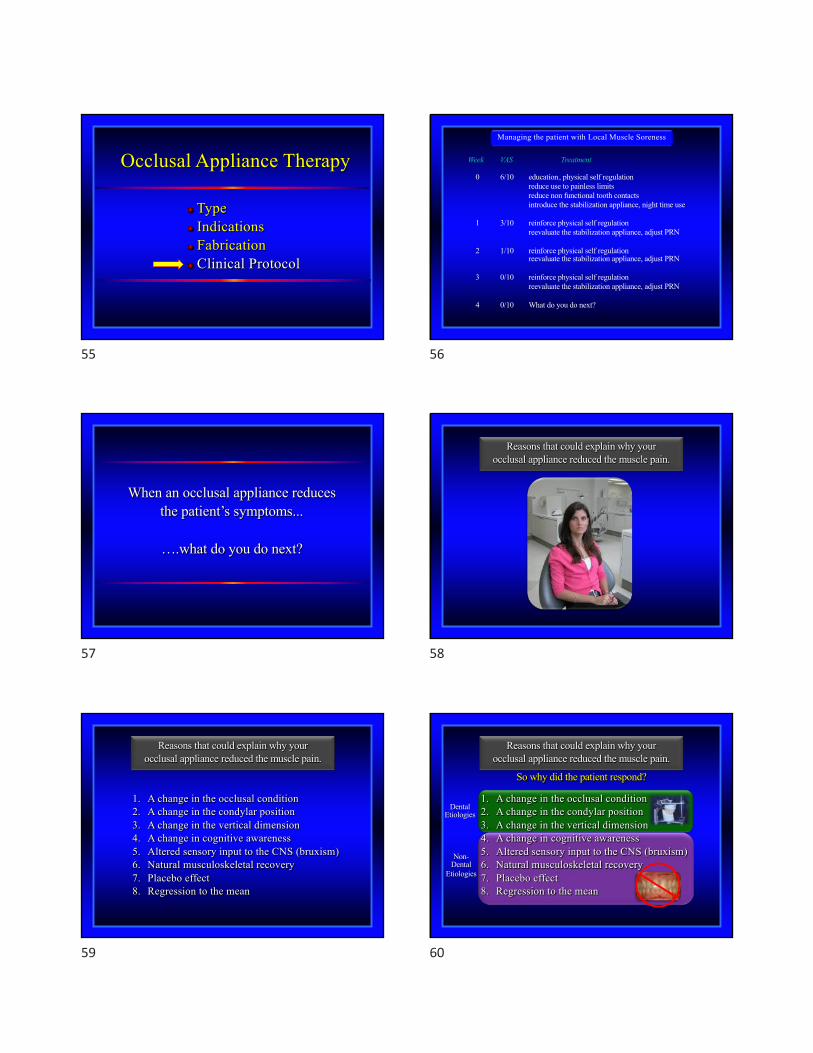
Managing the patient with Local Muscle Soreness
Week VAS Treatment
0 6/10 education, physical self regulation reduce use to painless limitsreduce non functional tooth contactsintroduce the stabilization appliance, night time use
1 3/10 reinforce physical self regulationreevaluate the stabilization appliance, adjust PRN
2 1/10 reinforce physical self regulationreevaluate the stabilization appliance, adjust PRN
3 0/10 reinforce physical self regulationreevaluate the stabilization appliance, adjust PRN
4 0/10 What do you do next?
Managing the patient with Local Muscle Soreness
56
When an occlusal appliance reducesthe patient’s symptoms...
….what do you do next?
57
Reasons that could explain why your occlusal appliance reduced the muscle pain.
58
1. A change in the occlusal condition2. A change in the condylar position3. A change in the vertical dimension4. A change in cognitive awareness5. Altered sensory input to the CNS (bruxism)6. Natural musculoskeletal recovery 7. Placebo effect8. Regression to the mean
Reasons that could explain why your occlusal appliance reduced the muscle pain.
59
DentalEtiologies
Non-Dental
Etiologies
So why did the patient respond?
1. A change in the occlusal condition2. A change in the condylar position3. A change in the vertical dimension4. A change in cognitive awareness5. Altered sensory input to the CNS (bruxism)6. Natural musculoskeletal recovery 7. Placebo effect8. Regression to the mean
Reasons that could explain why your occlusal appliance reduced the muscle pain.
60

Management of Temporomandibular Disorders
II. Temporomandibular Joint Disorders1. Derangements of the Condyle-Disc Complex
a. Disc Displacement with Reductionb. Disc Dislocation with Reductionc. Disc Displacement without Reduction
2. Structural Incompatibilities3. Inflammatory Disorders
I. Masticatory Muscle Disorders1. Protective Co-Contraction2. Local Muscle Soreness3. Myofascial Pain4. Myospasm5. Chronic Centrally Mediated Myalgia
61
Management of TM joint disorders
What about the use of an“Anterior Positioning Appliance” ?
62
A painful disc displacement
- Think orthopedically -
63
- Think orthopedically -
Anterior therapeutic position, pain reduction
64
The anteriorpositioning appliance
65
The anteriorpositioning appliance
66

- an interesting question -
When an “Anterior Positioning Appliance”reduces the patient symptoms…..
.....what do you do next ?
The problem was there were no data.
67
Which philosophy is correct?
The Re-builders
MS position
The Re-capturers
MS position
The Repairers
MS position
68
What is the short-term successof anterior positioning appliances?
69
Short-term Treatment of Disc Displacement With Reduction (phase I)
author # of pat type of tx duration reported success
Anderson et al 10 APA - 24 hrs/day 3 months sign. improvement1985 10 SA -24 hrs/day 3 months no change
Lundh et al 24 APA - 24 hrs/day 6 weeks much better1985 23 SA - 24 hrs/day 6 weeks slightly better
23 Control 6 weeks no change
Okeson 40 APA - 24 hrs/day 2 months 80%1986
Simmons et al 7 APA - 24 hrs/day 9 months 95%1995
Davies et al 40 APA - 24 hrs/day 2 months 88%1997 25 APA - only HS 2 months 65%
20 APA - only day 2 months 52%average 75-80%
70
What is the long-term successof anterior positioning appliances
for pain and dysfunction?
71
author # of pat type of tx duration success/pain & dysfunction
Moloney & 241 no occlusal changes 3 yrs 36%Howard,1986 APA & orthodontics 3 yrs 50%
APA & Cr / Bridge 3 yrs 43%
Okeson 40 no occlusal changes 2.5 yrs 25%1988
Butterworth 151 APA & orthodontics 1.75 yrs 51%et al, 1992
Davies et al 48 no occlusal changes 3 yrs 70%1997
Vichaichalerm- 17 no occlusal changes 4.2 yrs 35% vong et al,1993
Summers et al 75 APA & Cr / Bridge 1-6 yrs 52%1997
Tallents et al 68 APA & Cr / Bridge 1-3 yrs 44%1990
Long-term Treatment of Disc Displacement With Reduction (phase II)
average 45%
72

What is the long-term successof anterior positioning appliances
when pain and dysfunctionare evaluated separately?
73
author # of pat type of tx duration success/pain success/click
Moloney & 241 no occlusal changes 3 yrs not reported 36%Howard,1986 APA & orthodontics 3 yrs not reported 50%
APA & Cr / Bridge 3 yrs not reported 43%
Okeson 40 no occlusal changes 2.5 yrs 75% 33%1988
Butterworth 151 APA & orthodontics 1.75 yrs 86% 51%et al, 1992
Davies et al 48 no occlusal changes 3 yrs 87-92% 70%1997
Vichaichalerm- 17 no occlusal changes 4.2 yrs 77% 35% vong et al,1993
Summers et al 75 APA & Cr / Bridge 1-6 yrs 86% 52%1997
Tallents et al 68 APA & Cr / Bridge 1-3 yrs _ 44% 1990
Long-term Treatment of Disc Displacement with reduction (phase II)
average 83% average 45%
74
What is the long-term successfor Joint Sounds?
75
author # of pat type of tx duration success
Moloney & Howard 34 APA & orthodontics 3 yrs 50% click returned1986 14 APA & Cr / Bridge 3 yrs 43% click returned
Butterworth et al, 1992 151 APA & orthodontics 1.75 yrs 49% click returned
Summers et al, 1997 75 APA & Cr / Bridge 1-6 yrs 48% click returned
Tallents et al, 1990 68 APA & Cr / Bridge 1-3 yrs 56% click returned
Okeson, 1988 40 no occlusal changes 2.5 yrs 67 % click returned
Vichaichalermvong et al, 1993 17 no occlusal changes 4.2 yrs 65% click returned
Dolwick et al, 1987 33 TMJ surgery 4.2 yrs 58% click returned
de Leeuw , 1994 99 Nonsurgical 30 yrs 56% click returned
Long-term Success for Joint Sounds
average 55% return
76
Summary of Studies on Anterior Positioning Appliance Therapy
Long-term effects
Pain Clicking
Yes YesShort-term effects
Yes No
77
Treatment Considerations
Has the Disc been “recaptured” ?
78

MS position
Painful loading of the retrodiscal tissues.
79
Position the mandible forward off the retrodiscal tissues.(pain reduction)
MS position
The retrodiscal tissues adapt.
80
The condyle can now function in the musculoskeletally stable position painlessly.
(there may still be clicking)
MS position
81
Long-term Outcome of Disc Displacement with reduction
- conclusions from results of long-term studies -
Anterior positioning appliances may be helpful but only on a part time basis.
1. Educating the patient to the problem2. Reduce heavy chewing3. Reduce non-functional tooth contacts4. Appliance therapy
Our goal should be to help the patient adaptthe retrodiscal tissues by reducing loading forces.
82
Protrude the mandible
Contraction of the inferior lateral pterygoid.
83
With time the muscle develops
a myostatic contracture.
A painless shorteningof the functional length
of the muscle.
The result is a posterior open bite
84
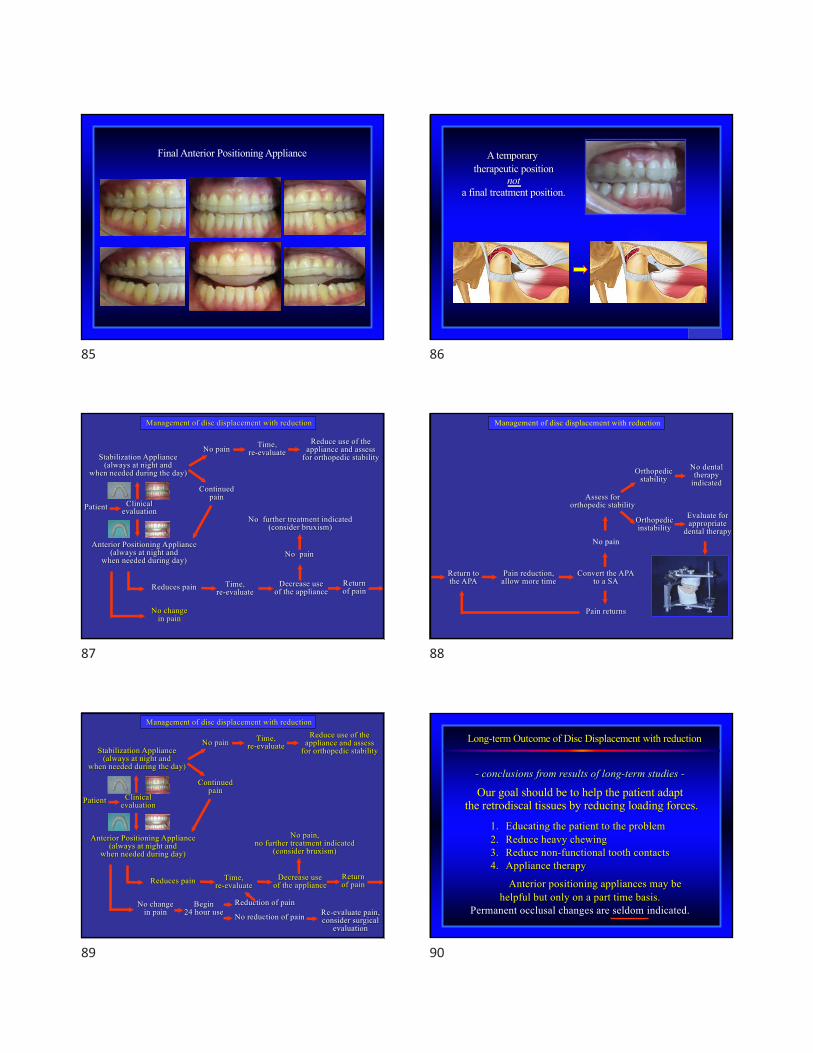
Final Anterior Positioning Appliance
85
A temporary therapeutic position
nota final treatment position.
86
Clinicalevaluation
Stabilization Appliance(always at night and
when needed during the day)
No pain
Continuedpain
Time,re-evaluate
Reduce use of theappliance and assess
for orthopedic stability
Anterior Positioning Appliance(always at night and
when needed during day)
Reduces pain Time,re-evaluate
Decrease useof the appliance
Returnof pain
Management of disc displacement with reduction
Patient
No changein pain
No pain
No further treatment indicated(consider bruxism)
87
Return tothe APA
Pain reduction, allow more time
Convert the APAto a SA
Orthopedic stability
Pain returns
No pain
Assess fororthopedic stability
Orthopedic instability
Evaluate for appropriate
dental therapy
No dental therapy
indicated
Management of disc displacement with reduction
88
Clinicalevaluation
Stabilization Appliance(always at night and
when needed during the day)
No pain
Continuedpain
Time,re-evaluate
Reduce use of theappliance and assess
for orthopedic stability
Anterior Positioning Appliance(always at night and
when needed during day)
Reduces pain
No changein pain
Time,re-evaluate
Decrease useof the appliance
No pain,no further treatment indicated
(consider bruxism)
Returnof pain
Patient
Begin24 hour use
Reduction of pain
No reduction of pain Re-evaluate pain, consider surgical
evaluation
Management of disc displacement with reduction
89
Long-term Outcome of Disc Displacement with reduction
- conclusions from results of long-term studies -
Anterior positioning appliances may be helpful but only on a part time basis.
Permanent occlusal changes are seldom indicated.
1. Educating the patient to the problem2. Reduce heavy chewing3. Reduce non-functional tooth contacts4. Appliance therapy
Our goal should be to help the patient adaptthe retrodiscal tissues by reducing loading forces.
90

- Some closing thoughts -
A few closing thoughts.
91
Remember the importance of establishing the proper diagnosis.
92
Some Important Questions
Who should you treat?
Success begins with selecting the patients you can help.
Cervical Pain
TMJ Pain
Neuropathic Pain
Muscle Pain
93
- Some closing thoughts -
Effective management of orofacial painis achieved more by thinking than doing.
Use your brain it isyour most powerful tool.
94
- Some closing thoughts -
Thinking provides the proper diagnosis,making treatment predictable and reliable.
95
- Some closing thoughts -
It’s what you think you know...
96

- Some closing thoughts -
It’s what you think you know...
...that keeps you from learning.
97
- Some closing thoughts -
“It’s not what you don’t know that gets you in trouble…..
...its what you do knowthat just ain’t so.”
Mark Twain
98
- Some closing thoughts -
“It’s what you learn after you know it allthat really counts.”
Coach John Wooden
99
- Some closing thoughts -
Confidence is what you feel…
100
- Some closing thoughts -
Confidence is what you feel…
...before you know all the details.
101
Don’t jump too soon.
- Some closing thoughts -
102

- Some closing thoughts -
This isn’t rocket science, but it does take some thinking.
103
- Some closing thoughts -
“The greatest problem in communicationis the illusion that
it has been accomplished.”
- George Bernard Shaw
104
Remember……next Monday morning, you are going to have a
28 year old female will come to your office.
Chief Complaint: facial pain with limited mouth opening
What will you do? How will youtreat her?
105
Do not ever lose sight of the fact that we are healthcare providers.We have been granted the privilege of treating our fellow men/women.
- A closing philosophical thought -
When you do this, you will have a happy and grateful patient.Treatment plan your patients as if they were family members.
106
Seventh EditionFebruary 2014
Quintessence Publishers1-800-621-0387
Eighth Edition488 pages
2019
Elsevier/Mosby Company1-800-325-4177
Newly Updated Lecture Series- DVDs or streaming -www.jeffokeson.net
Okeson Texts Okeson Home Page
University of KentuckyMini-Residency Program
June 7-11-2021 Shadowing Program
1 week (40 hr)
107