View
225
Download
0
Embed Size (px)
Citation preview
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
1/28
September 1996 Volume 21) Npmber 3Tinnitus TodayTHE JOURNAL OF THE AMERICAN TINNITUS ASSOCIATION
"To carry on and support research and educ1ational activities relating to the treatment oftinnitus and other defects or diseases of the ear."
In This Issue:What You Should Know AboutOtotoxic MedicationsNew ATA-Funded ResearchSilent Dental Wo rk - At Last!Rising Above the Cacophony
Since 1971Research - Referrals- Resources
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
2/28
Sounds Of SilenceControl your aud ible ambience withsounds caused by Tinnitus with the
Ma rsona Tinnitus Masker from AmbientShapes. The frequency and intensity of thesimulated sounds match the tones heard bymany tinnit us sufferers. These maskingdevices are proven effective in ass istingmany patientS in adapting to their tinnitus.We cannot predict whether or not theMarsona is approp riate for you, bu t theprobability of successfu l masking is we llworth TAKING ADVANTAGE OF OUR 30DAY MONEY BACK GUARANTEE.The Ma rsona Tinnitus Masker weighsless than rwo pounds to make transportingeasy and offers over 3000 specific frequency selections to achieve high defin itionmasking. The Marsona Tinnitus Maskeruses less than 5 warts of power, or aboutas much electricity as a small night light.
Simple To Use sea rch the frequency range settingto determine the specific "Centerfrequency" of tinnitus sound(s) LO provideprecise masking.ORDER TOLL FREE NOWr: --- ....or credit card holders please call toll free. IOrder proclucr #1550 for the MarsonaI innitus .Masker. Or send a check for $249.00I(FREE shipping & handling). NC residents add6% sales tax. One (I ) year warranty-ThirtyI 30) d ~ ; ; ~ : ~ : ~ : : N I800-438-22441 704/324-5222 1~ Ambient Shapes, Inc.
widen 1he frequency range aroundspecific "cemer frequency" to add ambientsound to enjoy the most pleasing personalsound selec tion.Marsona Features
The Ma rsona fearures over 3000 settingsad justable cemer frequency, frequencyrange, and volume control. Privacy headphones can be used but are not included.The Tinnitus Masker has an ultra-highfrequency speaker, LED readout for easylegibility, a frequency comparison chan,and a built-in optional shut-off timer.The bedside Tinnitus Masker can bepurchased rhrough Ambient Shapes forhundreds less than purchasing anotherbrand .Size: L8.75" W5.85" H3. 121'. Uses 110-120V AC(220-240V available). ULand CSA approvedpower supply.I P.O. Box 5069 Hickory, NC 28603 I
------------------------.... - - .... __J - - - - - - - - - - - - - - - - - - - - - -
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
3/28
Tinnitus T o d ~ y Editorial and advertising offices:American Tinnitus Association,P.O. Box 5 Portland, OR 97207Executive Director & Editor:Gloria E. Reich, Ph.D.Associate Editor: Barbara Thbachn ickEditorial Advisor: 'Trudy Drucker, Ph.D.Advertising sales: ATA-AD, P.O. Box 5,Portland, OR 97207, 800/634-8978Tinnitus 7bday is published quarterly inMarch, June, September and December. It ismailed to members of American TinnitusAssociation and a selected list of tinnitus sufferers an d professionals who treat tinnitus.Circulation is rotated to 75,000 annually.The Publisher reserves the right to reject oredit any manuscript received for publicationand to reject any advertising deemed unsuitable for Tinnitus Today. Acceptance of advertising by TinnihtS 7i>day does not constituteendorsement of the advertiser, its productsor services. nor does Tinnitus TOday makeany claims or guarantees as to the accuracyor validity of the advertiser's offer. Theopinions expressed by contributors toTinnittt.$ 7bday are not necessarily those ofthe Publisher, editors, staff, or advertisers.American Tinnitus Association is a nonprofit human health and welfare agencyunder 26 USC 501 (c)(3)Copyright 1996 by American T innitusAssociation. No pa n of this publication maybe reproduced, stored in
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
4/28
From the Editorby Gloria E. Reich, Ph.D.,Executive Director"We'll talk about that" ..and talkthey did, for two and a halfdays. Pawel Jastreboff, Ph.D.,Susan Gold, M.A., and WilliamGray, M.D. hosted a trainingworkshop for twenty hearinghealth professionals from theU.S., Canada, and Germanywho absorbed, listened, and learned how tinni-tus retraining therapy (TRT), also called auditoryhabituation or habituation-based treatment, can
help people with tinnitus and hyperacusis. Thetreatment is designed to induce and facilitate thehabituation of tinnitus perception, resulting in adecreased awareness of tinnitus.TRT is not a "quick-fix," nor is it a cure, buti f a person is willing to follow the protocol andbe patient about results, it can be very beneficial. The theory is quite simple and uses thenaturally occurring mechanisms of the auditorysystem to reduce the annoyance and perceptionof tinnitus.Almost everyone attending the course spokeof how they had espoused components of thetreatment but had not put it all together in theway the group in Maryland was demonstrating.We talked about hearing aids, maskers, drugs,biofeedback, counseling, relaxation therapy. Allof these can be helpful as stand-alone treatmen t,
(1 . to r.) William C. Gray, M.D., Susan Gold, M.A ., CCC SPIA,and Pawel Jastreboff. Ph.D. - faculty for workshop.
4 Tinnitus Today/September 1996
but the revelation was in understanding howinstrumentation plus counseling can achievemuch more dramatic results.
Here's what happens . There are three deter-mining factors for selecting a treatment protocolI f hyperacusis or sound-sensitivity is presen
If the patient considers hi s or her hearingloss significant enough to create a communication problemIfbe ing in loud noise impacts hearing, tinnitus, or hyperacusis for more than just a fewhoursBased on these factors, five categories of
treatments are employed for patients at theMaryland Tinnitus and Hyperacusis Center.Some attendees were concerned that these fivecategories might no t be sufficient to describe thpatient population seen in their own practices.Protocols may involve the use of noise generators, hearing-aids, both, or neither, and alwaysinvolve directive counseling to help the patientneutralize any negative associations they mighthave formed about their tinnitus. The patient'ssound environment is enriched through thewearing of noise generators or with other techniques if necessary. After a period of time theauditory system begins to ignore the sounds ofboth the noise generator and the tinnitus. Yes , itsounds simple, and in theory it is, but as with altreatments, not everyone is a candidate. If youand your health professional believe this is thecorrect approach for your tinnitus, then be prepared to fully comply with the protocol for up totwo years before achieving habituation. rt is reasonable to expect some change in the first fewmonths of treatment but the habituation processtakes time. (Remember, if you're Uke most of usyour tinnitus has been training the system tonotice it for some timenow. Learning not tonotice it won't happen overnight.)A number of theclinicians who attended this training arealready seeing tinnitus patients and will be
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
5/28
NewATA-Funded ResearchPOSITRON EMISSIONTOMOGRAPHYSTUDY OF TINNITUSAND ITS RELATIONSHIP TO AUDITORYPLASTICITY. PrincipalInvestigators: AlanLockwood, M.D. andRichard Salvi, Ph.D.,State University of
Richard Salvi, Ph.D. New York at BuffaloAmount ofAward: $46,145Purpose: Th investigate the neural basis ofsubjective tinnitus by measuring changes incerebral blood flow in the cerebral cortex using
positron emission tomography (PET).Dr. Salvi writes: Tinnitus symptoms are currently assessed through patients' self reports,questionnaires, and pitch and loudness matching techniques. However, these techniques donot provide any information about the neuralmechanisms that are responsible for subjectivetinnitus. To overcome this problem, we will usea powerful, new brain imaging technique,positron emission tomography (PET) to measurethe regional blood flow in the cerebral cortex ofpatients with unilateral tinnitus. On the basis ofour preliminary data, we hypothesize that thephantom tinnitus sensation will be associatedwith a high level ofblood flow in the auditorycortex. Thus, PET imaging may provide anobjective method for assessing tinnitus and aidin identifying the region of the brain that is
From the Editor (continued)identified on our referral list as soon as theyinform us that they are ready to receive newreferrals for TRTDr. Jastreboffhas indicated that there will bemore of these workshops in the future. If youare a professional treating tinnitus patients, Iurge you to avail yourself of this information.Contact the Tinnitus and Hyperacusis Center atthe University of Maryland, Baltimore. MSTFBuilding, Room 434F, 10 S. Pine St., Baltimore,MD 21201. Phone: (410) 706-4339. Patients wish-
involved in producing these abnormal and sometimes debilitating phantom sensations. (Dr. Salviis seeking subjects for this study. See "ResearchSubjects Sought," p. 10)
TINNITUSASSOCIATED WITHSOUND-INDUCEDHEARING LOSS, PARTII, MAPPING THEMODIFICATIONS OFTHE METABOLICACTIVITY RELATEDTO TINNITUS ANDHEARING LOSS.
Pawel J. Jastreboff, Ph.D. Principal Investigator:Pawel J. Jastreboff, Ph.D., Sc.D., University ofMaryland a t Baltimore
Amount ofAward: $111,536Dr. Jastreboff writes: Hearing loss-related tin
nitus is the most frequent type observed in clinical practice. Until now there was no animalmodel for studying this type of tinnitus. Workperformed under the first part of this grant created such a model, which furthermore providesassurance that our results express tinnitus andno t reflect accompanying hearing loss. Theinvestigations of changes of metabolic activityrelated to tinnitus will point out the centers inthe brain involved in processing the tinnitus signal, and will be of fundamental significance forfurther works aimed at proposing mechanismbased methods of tinnitus alleviation.
ing more information may attend one of ATA'sregional meetings where the procedures usedat the Maryland clinic as well as proceduresused elsewhere will be discussed. Our nextmeeting will be in College Park, Marylandthis month (registration form on p. 22)followed by one in California in the springof 1997. Watch for information about theCalifornia meeting in the December issue ofTinnitus Tbday.
T innitus 'Jbday/ September 1996 5
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
6/28
Letters to the EditorFrom lime to lime, we include letters from our members about their experiences with non-traditionaltreatments. We do so in the hope that the information offered might be helpful. Please read these anecdotal reports carefully, consult with your physicianor medical advisor, and decide for yourself i fa giventreatment is right for you. As always, the opinionsexpressed are strictly those of the letter writers anddo not reflect an opinion or endorsement by ATA.
I m writing to tell you about my victory overchronic tinnitus. About l 1/ 2 years ago aftertarget shooting with a .22 revolver, I startedhaving mild dizziness and tinnitus in both ears.After waiting about nine months for my tinnitusand dizziness to go away, i t became obvious thatit wasn't going to, without intervention.1 consulted anENT specialist who, afterdoing a few tests, told me that l would have tolive with the chronic tinnitus. He also told methat I had a mild case of Meniere's disease andto restrict my salt intake. 1 was determined tofind a more effective remedy. 1 consulted Dr.Hansel De Bartolo, a nutritionally-oriented ENTspecialist in Sugar Grove, Illinois. Dr. De Bartoloput me on 90 mg. of zinc picol inate daily. Inaddition, he prescribed niacin, manganese, magnesium, rutin, and iodine. The zinc was by farthe most important nutrient in my case and inmost other cases of tinnitus that are precipitatedby acoustical or physical trauma, according toDr. De Bartolo. Because there aren't any satisfactory blood or hair tests that indicate the body'szinc levels, 1 use the "Zinc Status Thst" (EthicalNutrients, 800/ 877-1704) which indicates whenmy body stores of zinc are saturated. (Level 1 isprofound zinc deficiency; level 4 is the desirablezinc level.) I was also restrained temporar ilyfrom having foods and medications that are highin salicylates (raisins, apricots, apples, tomatoes,almonds, vinegar, soft drinks, beer, aspirin, allartificially flavored foods, and others). I was toldto use protective ear plugs when exposed to loudnoises such as a power lawn mower or whengoing to the movies. After nine months of treatment, I am 75% better and I'm improving everymonth. 1 still take zinc in fairly high doses.I also found that grape seed extract was helpful in controlling my dizziness. A few of my
6 Tinnitus 'Thday /September 1996
patients with dizziness who tried 50 mg. a daygrape seed extract found that it worked equallywell for them. (Ginkgo was ineffective in controlling my tinnitus and temporarily made mydizziness worse while I was taking it).Dr. fohn L. Mohney, Physician andSurgeon - Osteopathic, Houston, TX
I was having quite a problem with tinni tus fa while and not having medical insurance(or money) I wasn't sure what I would do.I learned that tinnitus had been associated witB-6 deficiency, and I knew that I'd been showinother deficiency signs of this vitamin. When Iexperienced the tinnitus, I increased my consumption of B-6 and the tinnitus went away.After a time, the tinnitus stayed away.If B-6 is taken for any period of time, equaldoses of B-1 and B-2 must be taken. Ideally, allthe B vitamins would be taken at once. Sincethere seems to be many causes of tinnitus, thisprobably won't work for everyone but I'm certain it could help some.
R. Hoefs, Los Gatos, CAA s a relatively new tinnitus sufferer uustover one year of severe ea r and headnoises) I found your publication to be thgreatest support! Until I received that first issuI felt so alone with this new affliction. I read thmagazine from cover to cover and found suchcomfort from the articles and from letters fromother people who were sharing their experiences.I highlighted suggestions from that issue thcould possibly help me. Muscle relaxants, vitamins, minerals and herbs, earmuffs, maskers,walkman usage, ideas for de-stressing were alltreatments to consider. I did buy earmuff stylesound protection, I started using a walkmanwhen in noisy outdoor environments, I tried todecrease the stressful situations in my life. Andvisited my local health food store to inquireabout any suggestions to help tinnitus."Ginkgo!" responded the store owner. Sheshowed me publications about this extract fromginkgo tree leaves, which stated that increasingcerebral blood flow might decrease symptoms otinnitus. Reluctantly, 1 purchased a two-monthsupply, with very little confidence that it wouldhelp.
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
7/28
Letters to the Editor (continued)About six weeks later, I was amazed to realize
that I hadn't heard any loud noises for two days.Then four days, then a week. Now, it's beenseven weeks! I no longer have the loud, ringing,banging head noises. You can imagine how wonderful it is for me to know the silence we allpray for. I sleep at night without the terribleintrusions. I'm not totally without symptoms.I still experience muffled noises at times, and Iknow that some sounds that used to trigger loudnoises still trigger some noises for me. Butthey're so much softer, no loud ringing a t all, andthey only happen occasionally. I'm becoming abeliever! Perhaps others might find some relieffrom this simple treatment.
Janet R. Lull, Los Altos Hills, CAI would like to add a helpful hint. When usingear plugs to reduce noise, I find that when Iadd a little hand lotion to my ear canal first- applied with the tip of a finger - the earplugs slip in better and give a much tighter fit.Bill Stanley, Bloomfield, NJ
ru:he "Letters to the Editor" column inhe June issue of Tinnitus 'Ibday, Kimroshan describes having palatalmyoclonus, a clicking of the palate due to muscle spasm. This is a condition that respondsrapidly to electromyographic biofeedback. Thesensors are placed on the frontalis muscle andthe patient is instructed to learn relaxation of thefrontalis muscle which helps all muscles associated with the seventh nerve. In my practice, thishas been extremely rapid and effective. I wouldrecommend a trial of EMG biofeedback for thiscondition.
Murray Grossan, M.D., Los Angeles, CA
I eveloped tinnitus in March of 1995 after ahead injury complicated by a severe infection in my left ear. I also developed recruitment and pulsating sounds with dizziness. Allounds were magnified so greatly that I wasunable to be in public places, listen to music, orwatch TV I had the most difficult time trying toleep at night without taking sleeping pills.After trying many different drugs includingXanax and Klonopin without relief and findingnothing medically wrong I was referred to a psyhiatrist, Dr. Thnnenbaum, in Fremont. I was
then put on an anti-depressant drug calledAnafranil, 75 mg. before bedtime.The tinnitus has now subsided enough for
me to completely forget about it during the day.I sleep very well at night without sleeping pillsand only notice the tinnitus when I am sittingand relaxing in the evening. The recruitment isgone along with the pulsating and dizziness.Anafranil has very little side effects and hasbrought me back to my old self. I do believe itsaved my life!Sally Darmitzel, Fremont, CAW hen I first wrote to you in September1995, I thought tinnitus would be relatively easy to cure if one "doctorshopped," used common sense with respect tolifestyle, diet, etc. 1 was wrong. I t has been avery complicated journey, full of anguish andsuicidal ideation more than once. But I see thelight at the end of the tunnel, and would like toshare what I have learned.My condition - intermittent, atypical tinnitus - manifests with buzzing sounds mostmornings when I wake up. I t is also there in thenight if I should wake up, but no t there when Igo to sleep. Sometimes the buzzing will start inmy left ear and, as the day progresses, create aband of sound across my brain that moves intothe right ear. By bedtime, it is extremely loud,and the roof of my mouth and my lower brainvibrate. Once this starts, it usually lasts 48 hoursthen abruptly stops on the third day. On otherdays, the buzzing fades shortly after awakening.I've learned to discern which way the day willgo by the quality of the morning sounds.
I have been able to diminish the number ofdays per month where the buzzing increases bydoggedly sticking with regularacupuncture/M.D. appointments despitenumerous times thinking it wasn'treally helping and by following the 1advice to slow down, decrease stress, fjincrease sleep (10 mg. of Elavil in theevening helps), practice meditationdaily, pray, and seriously rethinkpriorities. In the year of doing this,I have diminished the days of my48-hour episodes from 11 days inone month to four days this past
Tinnitus Today/ September 1996 7
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
8/28
Letters to the Editor (continued)month. I t took me almost a year and a half ofregular acupuncture treatments before I wentinto partial remission.I have also taken the alternative route ofTibetan herbs, vitamins, and skeletal manipula-tions with an excellent chiropractor. (I knowthat putting oneself in the bands of non-medicalpersons is not for everyone.)On my first appointment with the acupuncturist I learned that my kidney "chi" was out ofbalance. At that time l thought the connectionto my kidneys and ears might be esoteric buthave since been told by an audiologist that kidneys and ears are closely connected during theembryonic stage. I've learned to drink muchmore water and to stay away from anything coldsuch as ice water and ice cream. I have evenlearned to like drinking ho t water!Daphne S. Crocker-White, Ph.D.,Hillsborough, CAMy congratulations on your recent issue(June 1996) which is a candidate for"classic" back issue. From the poeticprose of Leon Morgenstern to Michael Cohen'splea ("We Need Each Other"), it made such wonderful reading for this sufferer of that mysterious condition we call tinnitus. Indeed, I was somoved as to wonder whether we as human
ATXs NEW BROCHURE"IfYou Have Tinnitus -The First Steps To Take"ATA's newest brochure is now available and
included on our Information You Can Order formin the center of this issue. The brochure offersnew tinnitus patients a step-by-step approach tomanaging the onset of tinnitus; defines thescope of services offered by ENT's, audiologists,and hearing aid specialists; includes a list of23 crucial questions to ask one's health careprovider; and suggests practical self-help mea-sures to take.You will receive a free copy of this brochurewhen you renew your membership during thenext year.8 Tinnitus 1bday/ September 1996
beings need some sort of pain to have a meaningful dialogue of any sort.Ruknet Cezzar, Ph.D., Hampton, VA
T hank you Dr. Morgenstern for your "MyPets, the Spider and the Cricket." Th methis was medical and psychological poetry. I want you to know that I have walked, andcontinue to walk, your road.You mention several times something thatcall the "etiology agony." I suspect that for peo
ple like us, whose vocational art involves diagnosing, not knowing what caused the tinnitushas got to be agonizing and you write about thiIn my case, I suffered a concussion when I wathrown through th e windshield of my automobile years ago, and I feel certain that that's theepisode that gave rise to the tinnitus.But other than satisfying the appetite of myintellect "to know," our experience is the same.
One treatment I have found that helps isyoga, and especially the asana (posture) calledthe Headstand. This, with diaphragmatic breathing concurrent, appears to quiet the whistling.Perhaps it is a result of the power of meditationand the rich delivery of oxygenated blood to thbrain. Again thanks for the beautifully crafted"slice of your life."
Arnold Thaw, Ph.D., Phoenix, AZ
Tinnitus and Hyperacusis: A"Multi-Therapies" TreatmenKenneth Greenspan, M.D., of the Centerfor Stress and Pain Related Disorders and theColumbia Presbyterian Medica] Center, is stillseeking patients for a study using a multi
therapy approach to treating tinnitus and hypeacusis. (See the June 1996 Tinnitus Tbday fordetails.)Due to an extended interruption in phoneservice, Dr. Greenspan expects that many people tried to reach the Center but couldn't. Heinvites them to call again.
Center for Stress and Pain Related Disorder348 E. 51st St., New York, NY 10022,(212) 888-5140, (212) 888-5162
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
9/28
What You Should KnowAbout Ototoxic Medicationsby Stephen Epstein, M.D.
Ototoxic medications are those drugs thathave the potential to cause damage to the innerear structures which may result in temporary orpermanent loss of hearing or an aggravation ofan existing sensorineural hearing loss.If you have an existing sensorineural hearing loss, regardless of the cause, when using ototoxic medications, you are more vulnerable toaggravation of that hearing loss.As a result of using ototoxic medicat ions, thedegree of hearing loss that occurs and theamount of recovery that follows depends uponthe amount and duration of the use of that particular medication. If you are consuming morethan one ototoxic medication, you are evenmore vulnerable to developing a sensorineuralhearing loss or aggravation of your existing sensorineural hearing loss.Some ototoxic medications such as aspirinand aspirin-containing drugs - regardless of theamount and duration of usage - when discontinued, result in complete recovery of hearingand cessation of associated symptoms such astinnitus. (Ed. note: A few patients have reportedto us that their tinnitus continued after aspirinuse was stopped.)Guidelines to FollowIn regard to the use of ototoxic medications,whether they are over-the-counter or prescription, there are several important facts youshould know and several important rules youshould follow:+ Always inform your doctor that you have asensorineural hearing loss or nerve-typehearing loss.+ Always ask your doctor, when he or she isprescribing new medications for you, toinform you of any potential side effects,
especially if the medication is ototoxic.+ Always read the labels or ask your pharmacist about the potential ototoxic effects ofover-the-counter medications.+ Always be aware of the early warning signsof ototoxicity.Signs of Ototoxicity, Listed in Order ofFrequency
1. The development of tinnitus (noises in theears) in one or both ears.2. The intensification of existing t innitus or theappearance of another sound that didn't
exist before.
3. Fullness or pressure in your ears - otherthan being secondary to an upper respiratory infection.4. The awareness of a hearing loss in an unaf
fected ear or the progression or fluctuationof an existing loss.5. The development of vertigo or spinning sensation usually aggravated by motion whichmay or may not be accompanied by nausea.
Should any of these symptoms developwhile taking any medication, stop the medication immediately and call your doctor.Ototoxic MedicationsFinally, you should be aware of the commonototoxic medications, how they are prescribed,and for what conditions they are given.The following is a simplified list of ototoxicmedications and represents the most commondrugs. (There are many other medications thathave been listed as poten tial ly ototoxic; however, the incidence is insignificant. Consult yourphysician to be sure.) Keep this list for readyreference.1. SALICYLATES -Aspirin and aspirin-containing products+ 'Ibxic effects usually appear after consuming an average of 6-8 pills per day.
+ Toxic effects are always reversible oncemedications are discontinued.2. NONSTEROIDAL ANTI-INFLAMMATORY
DRUGS (NSAIDS) - Advil, Aleve, Anaprox,Clinoril, Feldene, Indocin, Lodine, Motrin,Nalfon, Naprosyn, Nuprin, Poradol, Voltarin+ Thxic effects usually appear after consum-ing an average of 6-8 pills per day.+ Toxic effects are usually reversible oncemedications are discontinued.3. ANTIBIOTICS- Aminoglycosides,Erythromycin, Vancomycina. Aminoglycosides - Streptomycin, Kanamycin,Neomycin, Gentamycin, Tobramysin, Amikacin,Netilmicin. These medications are ototoxic whenused intravenously in serious life-threatening situations. The blood levels ofthese medications are usually monitored to preventototoxicity. ThpicaJ prepa-
Tinnitus Thday/ September 1996 9
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
10/28
What You Should KnowAbout Ototoxic Medications (continued)rations an d ear drops containing Neomycin andGentamycin have not been demonstrated to beototoxic in humans.b. Erythromycin - EES, Eryc, E-mycin, Ilosone,Pediazole, and new derivatives of Erythromycin- Biaxin, ZithromaxErythromycin is usually ototoxic when givenintravenously in dosages of 2-4 grams per 24hours, especially if there is underlying kidneyinsufficiency. The usual oral dosage ofErythromycin averaging one gram per 24 hoursis not ototoxic. There are no significant reportsof ototoxicity with the new Erythromycin derivatives since they are given orally and in lowerdosages.c. Vancomycin - Vancocin
This antibiotic is used in a similar manneras the aminoglycosides; when given intravenously in serious life-threatening infections, itis potentially ototoxic. I t is usually used in conjunction with the aminoglycosides whichenhances th e possibility of ototoxicity.
Research Subjects Soughtfor Brain Imaging StudyofTinnitus
Subjects are needed to participate in astudy whose purpose is to identify regions ofthe brain that are activated or involved withtinnitus. We are seeking individuals who canalter th e loudness (intensity) or pitch (frequency) of their tinnitus by: (1) moving orpressing on their jaw, tongue, teeth, face,neck or head or (2) moving their eyes (gazeevoked tinnitus) . Brain regions activated bytinnitus will be identified by PositronEmission Thmography (PET).For details, contact: Richard Salvi, Ph.D.,Hearing Research Lab, SUNY University ofBuffalo, Buffalo, NY 14214,Ph: (716) 829-2001, FAX (716) 829-2980,e-mail: [email protected]: Alan Lockwood, M.D., PET Center, VAHospital, Buffalo, NY 14215,Ph: (716) 862-3450; FAX (716) 862-3462,e-mail: [email protected]
10 Tinnitus Today/ September 1996
4. LOOP DIURETICS - Lasix, Edecrin, BumThese medications are usually ototoxic whgiven intravenously for acute kidney failure oacute hypertension. Rare cases of ototoxicityhave been reported when these medicationsare taken orally in high doses in people withchronic kidney disease.5. CHEMOTHERAPEUTIC AGENTS -Cisplatin, Nitrogen Mustard, Vincri stine
These medications are ototoxic when givefor treatment of cancer. Their ototoxic effectscan be minimized by maintaining blood levelsthe medications and performing serial audiograms. The ototoxic effects of these medicatioare enhanced in patients who are already takiother ototoxic medications such as the aminoglycoside antibiotics and th e loop diuretics.6. QUININE- Aralen, Atabrine (for treatme
ofmalaria), Legatrin, QVel Muscle Relaxa(for treatment of night cramps)The ototoxic effects of quinine are very simla r to aspirin and the toxic effects are usuallyreversible once medication is discontinued.If you must take ototoxic medications, youshould have your hearing monitored with perodic audiological evaluations.Just as you are responsible for your overahealth, you can take responsibility for thepreservation of your hearing or your existinghearing reserve. Being aware of ototoxic medictions and their potential warnings is a good saguard to protect your hearing - and a soundinvestment!Stephen Epstein, M.D, FA .C.S, is an otologist and a fellowtl1e American Academy of Otolaryngology- Head and NecSurgery, Inc., and the American College of Surgeons. He isdirector of The Ear Center in Wheaton, Maryland.Reprinted with permission from the SHHH Journal.Copyright 1996 Self Help for Hard ofHearing People, Inc.,7910 Woodmont Ave, #1200, Bethesda, MD 20814
CORRECTIONfrom Tinnitus - In the Eyes ofThe Law, Marc1996, Corrected spelling: Alan Spielman, Esq
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
11/28
1996 PDR Guide to Drug Interactions, Side Effects,and Indications: Tinnitus
The following is a list of prescription andover-the-counter drugs that when tested produced tinnitus. These tests were either "controlled" studies conducted by the manufacturerbefore the drugs were released, or "post-marketing" studies conducted with a larger populationafter the drugs were released . The incidence oftinnitus as a side effect from these drugs variesbut is generally quite small. The percentages arebased on drug use at recommended dosages.Accutane Capsules(Less than I%) .... ..... 2076Achromycin v Capsules .. ........ 1367Actifed with Codeine CoughSyrup ......................................1067Adalat CC (Less than 1.0%) ........589Children's Advil Suspension(Less than 3%) .... ................... 2692Alka-Selrzer EffervescentAntacid and Pain Reliever ....e 70IAlka-Seltzer Extra StrengthEffervescent Antacidand Pain Reliever .................. 703Alka-Seltzer Lemon LimeEffervescent Antacid
and Pain Reliever ....... ......... 703Altace Capsules(Less than 1%) ........ .. ........... ..1232Ambien 'Pdblets ( Infrequent) .... 2416Amicar S ~ ' I ' u p , Thblets, and Injection(Occasional) ........................ ...1267A.Anafranil Capsules (4% to 6%)803A.Anaprox/ Naprosyn(3% to 9%) ..............................21171\nsaid Thblets (1 -3%) ...............2579Atalen Hydrochloride IJ1jection(1 patiem) ..............................2301Aralen Phosphate Thblets(1 patiem) ..............................230lArthritis Foundation Safety CoatedAspirin Thblets .......... ............e 675Asacol Delayed-Release Thblets 1979Arthritis Pain Ascriptin ............. 631Maximum Strength Ascriptin ..e 630Regular Strength Ascriptin'Pdblets .................................... 629Asendin Thblets (Less than I %)1369Atretol Thblets .............................573Atrohist Plus Thblets .................. 454
A z a c ~ a m for JJ1jection(Less than 1%) .........................734Azo Gamanol Thblets ................ 2080Azo Gantrisin Thblets ................2081Azulfidine (Rare) ......................J949Arthritis Strength BC Pow'der ..e 609BC Powder ...............................e 609Backache Caplets . ....................e 613Bactrim DS Thblets .... ................2084Bactrim I.V: lnfusion ................. 2082Bactrim ............................. ......... 2084Bayer Children's ChewableAspirin .................................... 711Genuine Bayer Aspirin Thblets& Caplets....... .. ..713Extra Strength Bayer AnhritisPain Regimen Fonnula ..........e mExtra Strength Bayer AspirinCaplets & Thblets .....................712Extended-Release Bayer 8-HourAspirin ......................................712Extra Strength Bayer PMAspirin ......................................713
Aspirin Regimen Bayer RegularStrength 325 mg Caplets .... .. .. 709Bayer Select Backache PainReliefFormula ...... ................e 715Bcnadryl Capsules ... .................1898Benadryl Injection .... .. , ............ 1898Biocadren Thblets(Less than 1%) .......................1614Arthritis Strength BufferinAnalgesic Caplets ...... ............e 6J4Buprenex Injectable(Less than I%) .......... .............2006BuSpar (f'requent) ..................... . 737Cama Arthritis Pain Reliever ...e 785Capastat Sulfate Vials ............... 2868Carbocaine HydrochlorideInjection ................................. 2303Carde ne Capsules (Rare) .......... 2095Cardene I.v. (Rare) .... ......... .......2709Cardizem CD Capsules(Less than 1%) ...................... 1506Cardizcm SR Capsules(Less than 1%} .......................1510Card izem Injectable .............. .... 1508Cardizem Thblets(Less than 1%) .......................1512Cardura Thblets (1 %) ....... ....... ... 2186Cartrol Thblets (Less common) ...410C a ~ a f l a m (1% to 3%) .... ...............816Cipro l.V. (1% or less) ................. 595Cipro I.V. Pharmacy Bulk Package(Less than 1%) .........................597Cipro 'Pdblets (Less than 1%) ......592Claritin (2% or fewer patients ) .2349Claritin-D (Less frequem) ......... 2350Clinoril Tablets(Greater than I%) ..................1618Clomid . .................... .................1514Cognex Capsules (Infre quent) ..1901CozaarThblets (Less than 1%).. 1628Cuprimine Capsules(Greater than 1%) ..................1630Cytotec (Infrequent) .................2424Cytovene (1% or less) .. .............2103Dalgan Injection(Less than 1%) ......................... 538Dapsone Thblets USP ................1284Daranidc Thblets ....... ................1633Daypro Caplets (Greate r than 1%but less than 3%) ................... 2426Dcconamine ................ .............. 1320Demadcx Thblets an d Injection ..686Depakote Thblers (Greate r than 1%bu t no t more than 5%) .. ......... 415Depen Tirratable Thblets ........... 2662Desferal Vials ............................ ..820Desyt-el and Desyrel Dividose(1.4%) ....... " ........."""" ...........503Diamox lmravenous .. .. ........ .....1372Diamox Sequels(Sustained Release) ...............1373Diamox Thblets.......... . ..1372
Drugs that report an incidence of tinnitus at3% or more are marked with a triangle.Drugs that include no percentage of incidence can be further investigated by contactingthe drug manufacturers or a pharmacist. Moreinformation abou t all of these drugs can befound in the 1996 Physicians Desk Reference(PDR). The corresponding PDR page numberfollows each drug name.Always consult with your physician beforemaking any changes in medication.
Dilacor XR Extended-releaseCapsules (1.0%)................ .. .... 2018Dipentum Capsules (Rare) .......1951Diprivan Injection(Less than 1%) .......................2833Doan's Extra-StrengthAnalgesic ..............................e 633Extra Strength Dean's P.M ........e 633Dean's Regular StrengthAnalgesic ................... ............e 634Dolobid 'Pdblets(Greater than I in 100) ..........1654Duranest Injections ............ ........542Dyclone 0.5% and 1% TopicalSolutions, USP .. ........................544Easprin .................. ............. .......1914A EC-Naprosyn Delayed-Release'Pdblets (3% to 9%) ............. .... .2117Ecotrin ............................ .... .......2455Edccrin ....... .. ........1657Effexor (2%) ..............................2719Elavil ........................: ............... 2838Eldepryl Tablets ........................ 2550Emcyt Capsules ...... .................. l953Emla Cream ...... .. .................... ....545Empirin with Codeine Thblets .. 1093Endep Thblets ............................ 2174Engcrix-B Unit-Dose Vials . .......2482Esgic-plus 1'dblets (Infrequent) .1013Eskalith ...................................... 2485Ethmozine Thblets(Less than 2%) ...... ....... ...... .. ..2041Etrafon ......................................2355Fansidar Thblets .... ............ .........2114Feldene Capsules(Greater than 1%) .. .. ..............1965Fioricet Thblets (Infrequent) ..... 2258Fioricet with Codeine Capsules(lnfrequem) ... ......................... 2260Fiorinal with Codeine Capsules
(lnfrequem) ........................... 2262Flexeril Thblets (Less than I%) .1661Floxin I.V. (Less than 1%) .........1571Floxin 'Tllblets (200 mg, 300 mg, 400mg) (Less than l% ) ............. ..1567Flumadine Thblets & Syrup(0.3% to 1%) ........................... 1015Foscavir I J1jection(Less than 1%) .........................547Fungizone Intravenous ...............506Gantanol Thblets .......................2119Gamrisin ..... ..................... ........2120Garamycin lnjectabl e ................2360Glauclabs .. ...............................0 208Halcion Thblets (Rare) ...............2611Healthprin Aspirin ....................2455Hivid 1ablets (Less than I% toless than 3%) .................... .. ....2121Hyperstat I.V. lnjecti on .............2363Hytrin Capsules (At least 1%) .... 430Hyzaar Thblets .......................... 1677IBU Thblets (Greater than l %) ..1342Tlosone (Isolated reports) ............911
lmdur (Less than or equalto 5%) .....................................1323lnclocin (Greater than J%) ........1680lntron A (Less than 5%) ........... 2364Kerlone Thblets (Less than 2%) 2436Lan1ictal Thblets (1.1 %) .............1112A.Lariam Thblets (Among mostfrequent) ................ .................2128Lasix Injection, Oral Solutionand Thblcts .............................1240Lincocin (Occasional) ............ ...2617Lioresal 'Tllblets ...........................829Lithium Carbonate Capsules& Thblets ................................2230Lithonate/ Lithotabs!Lithobid ...2543Lodine Capsules and Thblets (Morethan I CJ6 but less than 3%) .... 2743Loprcssor Ampuls .......................830Lopressor HCT Thb1ets(1 in 100 patients) ....................832Lopressor Thblets ........................830Lore eo Thblets .......................... 1517Lotensin HCI' (0.3% to 1.0%) ....837Lotrel Capsules (Infre quent) ......840Ludiomil Tablets (Rare) ..............843Luvox Thblets ............................2544
A.MZM (Among reactions occurringmost oftcn) ..............................267Marcaine Hydrochloride withEpinephrine 1:200,000 ...........2316Marcaine HydrochlorideIJ1jection....................... .........2316Marca ine Spina1 .........................2319Marino! (Dronabinol) Capsules(Less than I%) .......................2231Maxaquin Thblets(Less than I%) .......................2440Methergine (Rare) .....................2272Methotrexate Sodium Thblets.Injection, for Injection andLPFIJ1jection (Less common) ......! 275Mexitil Capsul es (1.9% to 2.4%) .678Miacalcin Nasal Spray(Less than 1%) .............. .. ......2275Midamo r Thblets(Less than or equal to 1%).... .1703Minipress Capsules(Less than 1%) ....................... 1937Minizide Capsules (Rare) .......... l93 8Mintezol ....................................1704Mobigesic Thblers ........................602Moduretic Thblets ......... ............1705Mono-Gesic Thblets ..................... 792Monopril 'Tablets (0.2% to 1.0%) 757Children's Motrin Ibuprofen OralSuspension (Greater than 1%bu t less than 3%) ...................1546Motrin Thblets (Less than 3%) . 2625Motrin Ibuprofen Suspension, OralDrops, Chewable Tablets, Caplets(1% to less than 3%) ..............1546continued on page 12
Tinnitus Today/ September 1996 11
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
12/28
1996 PDR Guide to Drug Interactions, Side Effects,and Indications: Tinnitus (continued)Mustargen (lnfrequent) ......... ...1709Mykrox Thblets (Less than 2%) ..993&Nalfon 200 Pulvules & NalfonThblets (4.5%)..... . . ........917AAnaprox/Naprosyn(3% to 9%) ..............................2117Nehcin Vials, Hyporets & ADDVantage...... . . ... 1464Neoral (2% or less) ... ................2276Neptazane Thblcts .....................1388Nescaine/Nescaine MPF . .. ........ .554Netromycin Injection100 mg/mL.... ........ . ...2373Neurontin Capsules(Infrequent)..... .. ..... . ...l 922Nicorette .................... ............... 2458Noroxin Thblets ............ ......... ....1715Noroxin Thblets ........... .............. 2048Norpramin Thblets ....................1526Norvasc Thblets (More than 0.1%to 1%) ........................ ............ 1940Ornade Spansule Capsules ....... 2502Onhoclone OKT3 SterileSol ution ..................................1837Orudis Capsules(Greater than I%) ...... ............ 2766Oruvail Capsules(Greater than 1%) ....... .......... .2766PBZ Thblets ............................ ..... 845PBZ.SR Thblets ............... .............844Pamelor ........................... .......... 2280Parnate Thblcrs................ .......... 2503Paxil Thblets (Inf reque nt) .........2505Penctrex Thblets(Less than 1% bu t more than
or equal to 0.1%) ............ ........2031Pepcid 11'\.iection (Infrequent) .. 1722Pepcid (1nfrequent) . .. ............... l720Pepto-13ismol Original Liquid,Original and Cherry Tablets andEasy-To-Swallow Caplet s ........ 1976Pepto-13ismol Maximum StrengthLiquid ..................................... 1976Periactin ....... .............................1724Pcnnax Thblets (lnfrequem) ... ...575Phenergan lrl,jection ................. 2773Phenergan Thblets ....................2775Phrenilin (Infrequent) ... .... ......... 785
Plaquenil Sulfate Thblets .... .... ..2328Platinol.. ............................. ......708Platinol-AQlnjection ......... ..........710Pontocaine Hydrochloride forSpinal Anesthesia... . ...2330PREVACID Delayed-ReleaseCapsules (Less than I%) .... ....2562Prilosec Delayed-Release Capsules(Less than 1%) . .. . .. .......529Primaxin I.M ............. .. .............. 1727Primaxin LV. (Less than 0.2%) .1729Prinivil Thblets (0.3% to 1.0%) .1733Prinzide Thblets (0.3 to 1%) .... ..1737Procardia XL Extended Release'Thblets (1 % or less) . ............ .. 1972
.APrograf(Greater than 3%) ..... 1042ProSom Thblets (lnfrequent) ..... 449Proven il (2%) .... ............ ........ .. .2386Prozac Pulvules & Liquid, OralSolution (2%) ..................... ......919Questran Light ............................ 769Qucstran Powder . .... ...... .... .........770Quinaglute Dura-Thbs Tablets ....649Quinidex Extentabs ................... 2067Rccombivax HB (Less than 1%)1744.ARelafen Thblets (3% to 9%) ....2510ReVia Tablets (Less than 1%) .... .940Rifater ............................... ........1532Risperdal (Rare)...... . .....1301Romazicon (Less than 1%) ...... .. 2147Rythmol T'.tblets 150 mg,225 mg, 300 mg (Less than 1%to 1.9%) ....... .. ........ ......... ........ 1352Salflex Tablets (Common) ......... 786Sandimmune (2% or less) . .... ... 2286Sedapap Thblets 50 mg/ 650 mg
(Infrequem) ...........................l543Sensorcaine .... .... ....................... ..559Septra ........ .... ...... . . .......... 1174Septra t.V. lnfusion .................... ll69Septra t.V. Infusion ADD-VantageVials ........ 1171Septra .......... ......... ........... ......... ..1174Serzone 'Thblets (Up to 3%) .........771Sincquan (Occasional) .. ............ 2205Soma Compound w/ CQdeineTablets .................................... 2676Soma Compound Thblets ... ....... 2675
Tinnitus Poetry Book PlannedDaphne Crocker-White, Ph.D., clinical psychologist, poet, and ATA member will ed it an d
publish a small book of tinnitus poetry. Thepoems you have previously sent will be forwarded to her for possible inclusion. We areexcited about this project an d Daphne eagerlyawaits your poetry that describes your tinnitusexperiences.
12 Tinnitus 'Ibday/September 1996
Sporanox Capsules(Less than 1%) .......................1305&Stadol (3% to 9%) .................... 775Streptomycin Su lfate Tnjection2208Surmontil Capsules..... . ...2811Talacen (Rare) ........................... 2333Thlwin 11'\.iection (Rare) ............ . 2334Talwin Compound ....... .............2335Thlwin Injection ........................ 2334Talwin Nx .................................. 2336Tambocor Thblets(1% to less than 3%) ...... ........ 1497'Thvist Syrup ........... ......... ..........2297'Thvist Thblets ............................ 2298Tegretol Chewable Uiblets ...... ....852Thgretol Suspension .... ................852Thgretol Thblets ...........................852Ternaril Thblets, Syrup and SpansuleE..xtended-Release Capsules .... .483Tenex Thblets (3% or less) ........ 2074Thera-Gesic ...............................1781Ticlid 'Thblets (0.5% to 1.0%) .... 2156Timolide Thblets ....................... l748Timoptic in Ocudose . ...............l753Timoptic Sterile OphthalmicSolution ..................................1751Timoptio-XE .............................. 17551bbramycin Sulfate ll'\iection .. ...968Tofranil Ampuis .. .. ....................8541bfran il Tablets ...........................8561bfrru1il-PM Capsul es ........ ......... .8571blectin (200,400 and 600 mg)(1 to 3%) .......... .......... ......... .... 15811bnocard Thblets (0.4 -1.5%) .......5311bproi-XL 'Thblets .... ........ 5651bradol (I% or less) .................. 21591brecau ... ............................. .....2245Thiavil T < ~ b l e t s ... ......................... L 571riJisate (Less than 20% )2000Thinalin Repetabs Tabletsl3301bssend1783Tympagesic Ear Drops2342
llltram Tablets (50 mg)(Infrequent) ............................ 1585Univasc Thblets (Less than 1 %) 2410Ursinus lnlay-'Thbs ... .. ...............794Vancocin HCI, Oral Solution &Pulvules (Rare) .. .................... l483
Vancocin HCI, Vials & ADD-Van(Rare) .................. ...................Vannn for Oral Suspension andVantin Thblets(Less than 1%) ....................... 2AVascor (200, 300 and 400 mg)Thblets (Up to 6.52%) .............1Vaseretic Thblets
(0.5% tO 2.0%) .......................1Vasotec LV ...............................1Vasotec Thblets (0.5% to 1.0%) .1Videx Thblets, Powder for OralSolution, & Pediatric Powder fOral Solution (Less than 1%) .VivacrU Tablets ..........................1Voltaren Thblets (I% to 3%) ......Wellbutrin 'Thblets ...... . .....1.AXanax Thblets (6.6%) ............2.AXylocaine Injections(Among most common ..........Zebeta Thblets ........... ........ .. .......1Zesto retic (0.3% to 1 %) ........... .. 2Zestril Thblets (0.3% to l.0%) ...2Ziac......... . . .. .. .... .... ..1Zolofl Tablets (1.4%) .... .. .. .. .......2Zosyn (1.0% or less) .................1Zosyn Pharmacy Bulk Package(1.0% or less).... .... . ...1Zyloprim Thblers(Less than I%) ............ ...........1 Page numbers listed refer to1996 50th edition of the PDR.e De.scribed in PDR ForNonprescription Drugs1ncidence data in parentheses: A3% or more0 Described in PDR ForOphthalmologyCopyright PDR* Guide to DmgInteractions, Side Effects, andIndications"' keyed to PDR'* 50thEdilion, published by MedicalEconomics, Montvale, NJ 07645.Reprinted with permission. Allrights reserved.
As far as seeing one's poems in print,Daphne says, "Being published feels great - fthe first 30 minutes. In the end, it's the writinof it that really counts."We believe that thereading of it will also really count! The book ischeduled to be available by early December. profits from the book will be donated to ATA.
Deadline for submission: October 15, 1996All poems must be typed with name andaddress clearly visible.
Maximum lines per poem: 25Please submit to :TINNITUS c/oDSCW1840 Brookvale Rd.Hillsborough, CA 94010
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
13/28
Book ReviewBill Habets: The Tinnitus Handbook - ASelf-Help Guide. Encinitas, CA: United ResearchPublishers, 1996., reviewed by TI'udy DruckerThe modest claims for this book for laymenare fully justified. Although none of the information is new, it's good to have a commonsense, well-written, and intelligently organized
summary of most of what is generally knownabout tinnitus. The Handbook will be especiallyu ~ e f u l . to ?aticnts who are just beginning to copew1th tmmtus, and wonder what might lie ahead.
The book begins with three comprehensive~ n d accurate chapters on the anatomy and physwlogy of hearing, on the nature of sound and itseffects, and on the various processes that mightproduce tinnitus. A distinction is made betweenpeople with "normal" tinnitus who are not bothered by it, and those who are more or lessseverely troubled. Attempts to determine theloudness or type of tinnitus do no t correlatewith the degree of distress experienced by thepatients. Obviously, psychological factors are atvork. The chapter on psychological therapiesemphasizes the role of stress and the vicious circle of stress-induced-tinnitus and tinnitusinduced-stress.
Habets is explicit about the role of noise incausing or worsening tinnitus and hearing loss.Various types of protection on the job and elsewhere are described. Habets reminds everyonethat legal action can sometimes be taken by people who are inadvertently subjected to otherpeople's recreational mega-decibels.I especially liked a chapter about what thepatient can expect from examination and treatment by a primary-care physician, a physicianspecializing in diseases of the ear, and an audiologist. Habets urges all new patients to have athorough physical examination to rule out intercurrent disease, such as hypertension. The possibility that drugs can mitigate tinnitus(tranquilizers, antidepressants) or worsen it(aspirin, antibiotics) must be discussed with thephysician. Some patients find their tinnitusimproves if caffeine and/ or alcohol is eliminated or strictly limited. Smoking, even secondhand smoke, is a known exacerbant. If thetinnitus results from a food allergy, this must betraced down. There isn't much evidence that
particular foods will be of benefit, although theauthor's advice to follow a diet relatively low insalt, sugar, and saturated fat is generally accepted for most people.The Handbook has a good index and a list oforganizations in America and England that canprovide additional information about many of
the topics discussed. The latter is rather heavilyweighted in favor of groups that advocate various kinds of unconventional treatment. A fewwell-known sources of excellent informationnotably the Deafness Research Foundation a ~ d the Better Hearing Institute, were not included.A bibliography for further reading and sometext-keyed references would have made a goodbook better."Alternative" (complementary) therapy is thecurrent darling of many desperate people whosesuffering does no t yield to the resources ofmainstream medicine. Habets presents us with averitable smorgasbord of options, ranging fromsuch accepted and possibly useful modalities ashypnosis and biofeedback to the simply sillysuch as "aroma herapy" and other types of "NewAge" gimmickry. To his credit, the author steersclear of the exaggerated claims of too manypractitioners, claims that are not supported bythe well-designed and carefully control led studies we have come to expect from good modernmedicine. I t is not unusual that some peoplewil1 feel better, or even get well, for no discernible physiological reason; the placebo effectis w i ~ h us always. Anything will help somebody;nothmg will help everybody.Habets makes the important point that theoften heard claim, "well, it can't hurt" is not necessarily true. No type of nonstandard treatmentwill benefit the patient whose tinnitus is causedby an acoustic-nerve tumor, and such "treatment" is likely to keep him away from a realcure. A recent front-page article in The NewYork Times reported that, fore x ~ m p l e . ' some instances ofm1sapphed chelationtherapy have resulted indeaths. A fair-minded butvigilant skepticism is apowerful and vital weaponin the war against tinnitus.
Tinnitus 1bday/ September 1996 13
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
14/28
Lester Lemke, Cape Coral, FL
Nelly Nigro, Los Angeles, CA
Dwne Bootz, Jacksonville, FL
Bob Lewicki, Las Vegas, NV
Arlene Jewell, Pensacola, FL
Ann Andruchiw, Parma, OH14 Tinnitus Today/ September 1996
Ma lvina Levy,San Francisco, CA
Cheryl Ann. Raisanen,Woodridge, IL
Kindness Begets Kindnesby Barbara Thbachnick, Client Services Manager
Oh, the comfortThe inexpressible comfortOf eeling safe with a person
Having neither to weigh thoughtsNor measure wordsBut pouring themAll right out, just as they areChaffand grain together,Certain that a faithful hand willThke and sift them.
And with the breath ofkindnessBlow the rest awayby Dinah Craik (Reprinted with permission from the Hyperacusis Network Newsletter. June 1996.)
When we give a pint of blood, a shoulder of solace, or a moment oundivided attention, we are - as our species goes - really at our besI t is a grand experience to extend handfuls of hope to people who onparticular day are not able to do it for themselves.
We helper-types have all been on the receiving end of it too, whicis how we know that what we give can mean so much.We asked our Tinnitus Support Network people to tell us just wha
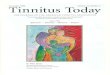
it is they get from giving their time and energy to others in this way.They answered, "A chance to give back the precious help that wasgiven to me when I needed it most." "A place to go where peopleunderstand my struggles." "Friendships I wouldn't part with." A kindness, given in earnest, will always find its way back to the giver.ATA's Self-Help Network changes weekly, shrinking with the natural order of things and growing when people, who are helped by othercaring people, choose to be of service themselves. It's a randomgrowth. For example, some cities like Chicago have two active tinnitusupport groups with six additional telephone contacts. Other cities likSan Diego and entire states (see map) have no support contacts at all.We're working to fill in these "support gaps." Do you live there? Andcan you help?
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
15/28
Elaine Sauer; Saskatoon, SK,Canada
Myrtha Castellvi,Bolingbrook, IL
SelfHelp NetworkIf you are interested in joining ATA's network, write for our SelfHelp Packet. To assist you in getting a support group started, we'llmail meeting announcements to 200-300 people with tinnitus in
your area, plus help you place press releases in your local papers toannounce the group. These efforts should help draw a good core ofpeople together. Or, if you prefer, we could list you as a telephone/support person in our network - still a vital point of contact forothers with tinnitus. (There is no cost to you either way.)Ours is an easily accessed network of telephone helpers and support groups. Current lists are sent to our members when they firstjoin ATA and then every year when they renew their memberships.When you become part of our network, your name definitely getsaround!
If you see yourself in these words, do write to us and let us knowhow you can help. If you are now or have ever been part of our network, or if you see yourself in these pictures, we send you deepestthanks from the bottom of our hearts.
Highlighted states are those without ATA support groups and/or telephone contacts.
Megan Vidis, Chicago, IL
Mike Cohen, Chicago, IL
Lillian Markowitz, Melrose, MA:-;-___ ... , ..:.. _ : ! f ~ ~ - - ~ ~ " . '. . . . .- ,I.. :I OiI ., i , '
Gail Brenner; M.A. C.C.C.A.,Philadelphia, PA
Thomas D'Aiuto, Thmpa, FL
Tinnitus Today/September 1996 15
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
16/28
ATA Research Report-An Interview with James A. Kaltenbach, Ph.D.by Barbara Th.bachnick, Client Services ManagerJames A. Kaltenbach, Ph.D., Associate Professor, Wayne StateUniversity School ofMedicine, discusses his recently-fundedATA research project, 'Changes in Spontaneous Activity andNeurochemistry of the Cochlear Nucleus Following Exposure toHigh Intensity Sound'
B'n Dr. Kaltenbach, please explain thetheory behind your research project.
JK: When a normal-hearing person goesfrom an environment of silence to one that isfilled with acoustic stimulation (or sound), theelectrical activity in the auditory system goesfrom a low-level spontaneous (orresting) activity to a higher level ofstimulus-driven activity. Since tinnitus is the sensation of sound inthe absence of acoustic stimulation,we would expect that the auditorystructures of the brain of someonewith tinnitus might show anincrease in spontaneous activitythat resembles stimulus-drivenactivity.
B'n How are you testing yourhypothesis?JK: We have been studying the
B'n Why is the dorsal cochlear nucleus inparticular being studied?JK: There are a couple of reasons. One is
that the dorsal cochlear nucleus receives inpdirectly from the auditory nerve, then procesit, and passes its output to higher levels of thauditory system. To understand what leads toincreases in spontaneous activity, we have tostudy the dorsal cochlear nucleus where thosincreases are like ly to originate.Also, in a recent study, tinnitus in somepatients was reduced or eliminated by electrily stimulating the surface of thedorsal cochlear nucleus. (These
patients had had acoustic neuromremoved and auditory brainstemimplants surgically implanted torestore their hearing.) I t appearsthat the dorsal cochlear nucleusinvolved in both the productionthe suppression of tinnitus.
B'n What led you to study thebrain's involvement in tinnitus geration instead of studying the est ructure itself?
spontaneous activity in the audita- fames A. Kaltenbach, Ph.D.JK: It's true that central disor
ders like tinnitus usually begin wan injury to the ear. However, it'known that more than half of tinnitus casesry systems of hamsters, specificallyin a structure in the auditory brainstem called
the "dorsal cochlear nucleus." The animals wereexposed to an intense tone for a period of fourhours, allowed to recover, and were then examined after one month. The spontaneous activityin their dorsal cochlear nuclei was compared tothat in non-exposed animals.
B'n What did you find?JK: We found that the animals exposed to
the intense tone one month earlier had abnormally high levels of spontaneous activity.Indeed, the increase was rather dramaticbetween five and 10 times higher than in normal-hearing animals.
There is another interesting aspect of thisfinding that makes it very attractive as a modelof tinnitus. Specifically, one month after exposure to an intense sound, the dorsal cochlearnucleus behaved like a normal-hearing animal'sdorsal cochlear nucleus in the presence of ahigh-pitch sound.16 Tinnitus 1bday/ September 1996
appear to involve changes in the auditory port ion of the brain. The notion is upheld by twoimportant findings. First, surgical removal ofcochlea or severing of the auditory nerve doeno t "cure" or relieve the symptoms of tinnitusInstead, following these surgeries, more thanhalf of such patients continue to have tinnituand in many cases, the tinnitus is worsened.Second, in patients with tinnitus on one side(unilateral tinnitus), the tinnitus can be maskby presenting a masking noise to the oppositear. This implies that the masking effect musbe mediated by structures between the earsin other words, by the brain itself.
Bn What do you expect to learn from thisresearch?JK: We expect to learn precisely why
intense sound exposure leads to increases inspontaneous activity and to tinnitus. ThanksATA's support, we're beginning to obtain somimportant clues.
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
17/28
An Interview with James A. Kaltenbach, Ph.D. (con tinued)My collaborator, Dr. Donald Godfrey at theMedical College of Ohio, found evidence of significant chemical changes present in animals
with abnormal spontaneous activity levels onemonth after they'd been exposed to sound. Onesuch chemical change was an increase in theamount of glutamate, a neurotransmitter whichacts to increase the activity of many cells in theauditory system.
BT: How will this information be translatedinto treatments for tinnitus?
JK: Once the sites of the tinnitus generatorshave been firmly established, and the mechanisms that trigger them have been identifiedchemically, we can use our animal model tobegin a search for drugs that will block increasesin spontaneous activity. The development ofeffective drug therapies for people with tinnitusdepends ultimately on gaining an understandingof the chemical pathways that underlie changesin spontaneous activity.
Highlights from Illinois - ATA's First Regional MeetingATA's Regional Meeting in Arlington Heights,
IL this past May closely resembled a tinnitus"town meeting" - an aU-day forum for a mixedaudience, balanced evenly between lay and professional attendees. During the morning's opensession, patients and professionals alike heardDr. Reich present an overview of ATA's researchgoals and mission, and Robert Sandlin, Ph.D.,Director of the California Tinnitus AssessmentCenter in San Diego, offer a thorough overviewofknown tinnitus causes. James Kaltenbach,Ph.D. explained his ATA-funded research project(see "ATA Research Report- An Interview withJames A. Kaltenbach, Ph.D.", p. 16) in whichcochlear cell changes were examined before andafter exposure to high intensity noise. SamHopmeier, BC-HIS, President of HopmeierHearing Services and Dr. Sandlin together discussed the benefits of hearing aids, maskers, andauditory habituation as relief-giving therapies fortinnitus.
In the afternoon, two concurrent sessionswere offered: one for health professionals andone focusing on self-help. For the professionals,Drs. Sandlin, Kaltenbach, and Reich as well asSam Hopmeier elaborated on auditory habituatorand masker fittings plus the scope of tinnitusresearch in the U.S. During the workshop-styleself-help session, Barbara Thbachnick demonstrated listening and communication techniquesto help anyone become an able one-on-one support giver. She encouraged the attendees to tapinto their rich resources of support - family,friends, and, of course, ATA. Jo Hazelby, a certified tinnitus counselor in the U.K. spoke of theenormous benefits realized by tinnitus patients
Nancy Good and Reg Thomaswho receive focused counseling. (Jo also spokeat the professional session to explain the linkbetween the medical and emotional needs oftinnitus patients.) Dr. Reich explained the principles of cognitive therapy, a crucial self-help aidthat treats the patient's reaction to tinnitusrather than the tinnitus itself. Nancy Good,LCSW, discussed and demonstrated the principles ofbiofeedback as a stress reduct ion tool.Good believes that the aim of stress management is not to reduce the stress, bu t to changethe body's reaction to it. In her hands-on (and"electrode-on") demonstration, Good's volunteerwas able to lower his heart rate by watching thedevice to which he was attached, relaxing hisface, and adjusting his breathing. BothThbachnick and Good will reprise their presentations at the Maryland meeting in September.
Tinnitus 1bday/ September 1996 17
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
18/28
Silent DentalWork At Last!by Barbara Tabachnick, Client Services Manager
Micro-air abrasion dentistry is exceptionallyquiet, so quiet in fact that one has to listen hardto hear it at all. This new star of dental technology was actually developed more than 40 yearsago at a time when its cost was 10 times greaterthan that of the also new high-speed (and highnoise) rotary drill. The drill became the dentalindustry's standard despite its high-pitchedwhine (above 4000Hz), associated pain, and theneed for local anesthetics with its use. Over theyears, patients grew more vocal in their demandfor less trauma in the dentist' s chair, and aninterest in air abrasion was resurrected. Its widespread acceptance throughout the U.S. began just18 months ago.In air abrasion cavity preparation, a smalldevice is held very near the cavity. From its tip,a concentrated stream of pressurized air - from45 pounds per square inch (psi) to 150 psi,depending on the manufacturer - mixes with afine powder of aluminum oxide particles and isaimed directly at the cavity. Excess powder issucked away by the in-the-mouth suctioningtube, common to all dental work. Any airborneparticles can be removed by an intake ai r filtration device (like Kreativ's KleanAir) placed nearby. These two devices produce the only audiblesounds during the procedure. The air filtrationmotor makes a mild hum. The intermittentin-the-mouth suctioning makes the loudestsound of all.
In addition to being quiet, air abrasion isessentially pain-free. Local anesthesia is usuallynot required.Micro-air abrasion technology has beenimproved over the years though no t yet to whereit can fully replace standard rotary metal drills.Rotary drills are still the tool of preference forextensive dental work: crown preparation, verylarge or deep cavities that require root canal, andremoving old s ilver (amalgam) fillings. But notin every case. Some dentists use air abrasiononly for the smallest pits and fissures, while others will work it into deeper cavities. Apparently,both the limitations of the equipment and thevariances among dentists play a part in determining the extent to which ai r abrasion is used.
18 Tinnitus 'Ibday/ September 1996
ATA member Craig Dennis needed serioudental work. But because he couldn't bear ththought of subjecting himself to the noise ofdrill, he put i t off for more than five years. TWof his teeth were close to needing root canalwork when he learned about air abrasion dentistry, then found a dentist who used it. RobeWindsor, D.D.S. in Thwson, Maryland, was abto save Dennis' teeth using only the AmericaTechnology's KCP air abrasion device. Dennisneeded no anesthesia for most of the procedu"I hate to applaud it as universally quiet," sayDennis, "but I have extreme sound sensitivityand tinnitus, and it worked for me!" The onlyinconvenience he notes was that he had to clhis eyes to avoid the dust particles.
James Frohnmeyer, D.M.D., has hadKreativ's MicroAir Abrasion unit less than twweeks and already uses it for 20% of his practice. "It works marvelously, it's faster, and noanesthesia is required," says Frohnmeyer, whalso notes that the time it takes for dentists tolearn the new technique is minimal.
Jerry Aso, D.D.S. uses Kreativ's devices tokeep the dental arena quiet for his patients. Ahe uses something else - a philosophy of cocern for the physical and psychological needseach patient. When a sound-sensitive patientdue to arrive, he will, for example, not run thultrasonic cleaner or other office machines thgenerate noise. Says Aso, "When you know ypatients' needs, you can find the rhythm to thdental work that works for them. Thking breaevery 20 seconds is not a problem. It's possibto do very complex work at that pace, at thosintervals."
Dr. Aso acknowledges the limitations of thnew technology. Air abrasion is not the precision tool he needs for cleaning out a deep cavty, so it loses ou t to the standard drill. But hewill use the air abrasion to the end point of itusefulness so that some of the drilling time isquiet. Aso notes that some rotary drills makeless noise than others, and he always opts forthe quietest one.
In the 1980s, hopes ran high that the surgeon's laser scalpel would make a successfulcrossover into the world of cavity repairs. It tolittle time, however, to uncover the problemswith that idea: 1) The heat from the laser was
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
19/28
Silent DentalWork At Last! (continued)found to literally "cook" th e nerve and consequently kill the tooth. 2) The precision neededfor decay removal is not yet possible with lasers.3) The price of the equipment is still out ofreach for most.A new water-cooled laser is being tested, butso far it's tooth cutting efficiency is "unimpressive," according to Stewart Rosenberg, D.D.S.,founder of the Academy of Laser Dentistry.Lasers do have their place in the- , - . . dental office, says Rosenberg.Argon lasers are used to harden the
composite tooth-colored fillingmaterial, and they make the com-posite filling twice as strong.Carbon dioxide lasers are used insoft-tissue surgeries in the mouth
because they eliminate bleeding andthe need for stitches. But the laser's usefulnessin the mouth ends there for now.
James Rademacher D.D.S., Ph.D., believesthat decay prevention awareness (fluoride treatments, dietary changes, proper flossing, etc.) isimpacting dentistry as a whole. Statistically, cavities are fewer in number and smaller in sizethan ever before. He speculates that in th e nearfuture, ai r abrasion dentistry will be all that isneeded. Until then, it is logical for patients tohave cavities attended to early, when ai r abrasion stands its best chance at being th e soletreatment.Dr. Rosenberg feels that the future of ai rabrasion dentistry looks brighter yet. New powders are being developed to improve ai r abrasion's capabilities. Professionals who use airabrasion equipment agree that, despite its limitations, it's a great start. For people who haveshied away from th e dentist's noisy drill for fearof worsened tinnitus, it should come as atremendous relief.
Call or write to th e manufacturers fbr th e names oflocal dentists who use these products.+ American Dental Technologies, KCP "Whisper Jet"1000 PAC - Air Abrasive Cavity Preparation System,
922 Harmony Hill Rd, West Chester , PA 19380,800/ 359-1959+ f
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
20/28
Questions and Answersby Jack A. Vernon, Ph.D., Oregon HearingResearch CenterDear Readers.As many ofyou know, I am retiring as ofAugust 15,1996. However, I will still be available to answer yourquestions. Questions can be sent to me c/o ATA. Ifyouneed to talk with me directly, I will take calls onWednesdays from 9:30am - noon and 1:30 - 4.30 pm(5031494-3675) starting September 4th.
[Q] Ms. D. from New Jersey writes that hertinnitus fluctuates . Some days she canhardly hear it; other days it is very loud.When it is quiet, the only thing that turns itback on is sleep. Even a very brief nap will produce very loud tinnitus. She asks, "Why?"
There is a group of tinnitus patients forwhom sleep is the trigger that turnstheir tinnitus from good to bad, or from
bad to good. One has to guess that there is somebrain mechanism involved with sleep controlwhich affects the brain center involved with tinnitus but, unfortunately, we do not know theidentity of these centers. There is one suggestion I would make to you and it is to use masking while you sleep. Marpac makes a tabletoptinnitus masker advertised in this journal, and Iwould suggest that you use it, or one like it, forsleeping to see if it is possible to disrupt thesleep effect without disrupting the sleep. Will itwork? I don't know, but try it and let's see.
[Q] Ms. B. in California writes that she hashyperacusis and that her attendingdoctor instructed her to wear ear plugsall the time. He said if you wear them aU thetime the hyperacusis will gradually go away. Shesaid she did just that and the hyperacusis gotworse. Why was that?
The sure way to make hyperacusisworse is to over protect the ears. Whenexposed to normal environmental
sounds it is important to wear no ea r protection.1b do so will make the hyperacusis worse. Thatis exactly what happened to you - but all is notlost. In the future, do no t over protect your ears.You can also desensitize your ears with a pinknoise audio tape. (For a copy, write to: TinnitusClinic c/ o Oregon Hearing Research CenterNRC04, 3181 SW Sam Jackson Park Rd.,20 Tinnitus Today/ September 1996
Portland, OR 97201.) For about two hours eacday, listen to pink noise at the maximum comfort level, and very gradually your tolerance loudness will return.
[Q] Mr. M. in Missouri is concerned abouthe possible damage from sounds henot hear, specifically the noise of powtools such as routers.Ear protection should be worn wheneyou are exposed to loud sounds, wheor not you can hear them. It is possibto exacerbate your tinnitus with loud sounds
you are unable to hear. I would encourage yocontinue to use those tools (I am well awarehow much fun it is to use them!) but to alwayprotect your ears when you do so. In my shohave five pairs of Thunder 29 ear muffs - onpair for each tool that makes loud noise.
[Q] Ms. P. from Pennsylvania writes a mointeresting account of her pulsatiletinnitus. I would like to present it herand ask our medical colleagues to give theiropinions of her treatment.
Ms. P. was diagnosed as having hydrocephalies, that is, an increase in theintracranial pressure causing the pulsatile sounds she heard. The corrective proce
dure that she'd had drained off some of thecerebral fluid via a craniotomy and shunting,which resulted in the disappearance of her pusatile tinnitus. The question remains whethenot it is a permanent solution.
Increased intracranial pressure is only onthe ways that pulsatile tinnitus can be producbut it is an unusual one that requires the attetion of a neurologist and a neurosurgeon.fRl Ms. H. from Colorado asks if Thnocara recommended treatment for tinnitu
Some years ago, five centers across thU.S. (Oregon Hearing Research Centerwas one) were se]ected to evaluate theeffectiveness ofThnocard, an ora] analog oflidcaine, on tinnitus. Each center was instructed
test 20 patients in an open study. I t was not adouble-blind, placebo-controlled study. Wefound we needed to introduce Tonocard to 60patients before we found 20 who could tolera
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
21/28
Questions and Answers (continued)the drug. (The side effects were so great.) Of the20 who took the full course of the Thnocard medication, only one patient had his tinnitusrelieved. The other four centers got about thesame results as we did, that is, a 5% success rate.The study of Thnocard was motivated by thesuccesses with IV lidocaine. In an IV injection,lidocaine will eliminate tinnitus in 23 of 26patients but only for about 30 minutes. It's longbeen thought that an oral form of lidocaine couldbe an effective tinnitus therapy. As you can seefrom the above results, Tbnocard is not theanswer.
[Q]Ms. S. from North Dakota asks, "I needto have some dental work which willinvolve drilling. Is the dental drill noiseloud enough to raise my tinnitus? Should I wear
ea r plugs?"The high-speed dental drill is very loud.Some den tists have acquired hearingloss and tinnitus themselves as a result
of using the high-speed dental drill. One dentist,who was a tinnitus patient in our clinic, did asurvey of dentists in the Northwest and NorthernCalifornia and found that every dentist who hadpurchased the high speed dental drill now had ahearing loss. Over half of them had moderate tosevere tinnitus. Those dentists were exposed tothat noise for a very long time (years) whereasyou will be exposed for a relatively short time(minutes). Nevertheless I think that the noisefrom a dental drill may, for some people, produce an increase in tinnitus. Remember, it iseasier to exacerbate tinnitus than to acquire it.
The fact that the dental drill is in contactwith the teeth means that its sound is transmitted to the ear by bone conduction as well as byair conduction. Because bone conduction is theprimary route of dental drill noise to the ear,wearing ea r plugs will not help much but it willhelp some. I would suggest that you explainabout vour tinnitus to your dentist and requestthat the drilling be done in short spurts withmany brief intervals of no drilling. (See SilentDental Work- At Last!, p. 18)
[Q]Mr. A. from Thxas writes that he is areformed alcohol and drug addict andwonders if it would be safe for him to tryXanax for his tinnitus. He goes on to say he is
desperate and is struggling with a very severebilateral noise-induced tinnitus.
Since there is a history of substanceabuse, I think it would not be ~ a f e tryXana-'< which for some people 1S habitforming. I further suggest that you question the
use of all drugs that have any habit-forming oraddictive characteristics.I would also recommend a very thoroughexploration of masking (hearing aids, or combination units of hearing aids and in-the-earmaskers called tinnitus instruments) as a possible relief procedure.
[Q]Mr. B. from Pennsylvania is an attorneywith a client who has head trauma
induced tinnitus . He asks if there are anyobjective tests of tinnitus which might be ofvalue to his client? Would the tinnitus be displayed on X-ray, CT scan, or MRI scan?
There are no completely objecti:e t ~ s t s of tinnitus. And unfortunately, tmmtusis not revealed on X- Ray, CT scan, or
MRI scan. You will find a discussion of"Litigation and Tinnitus" in the Proceedings ofthe Fifth International Tinnitus Seminar whichcan be ordered from the American TinnitusAssociation.For your information, courts of inquiry usually ask four questions regarding tinnHus:1. Does the plaintiff really have the tinnitus he
claims to have?2. Was the tinnitus caused by that indicated bythe plain iff?3. Is the tinnitus as severe as the plaintiffclaims?4. Is the tinnitus temporary or permanent?
Of these four questions, there is a test forthe first question which is somewhat objectiveand which has been accepted by other courts inthe past. The test is the reliability of repeatedloudness of tinnitus tests. If the plaintiff canrepeatedly match the loudness of his or her tinnitus within 2 dB, that performance is acceptedas evidence that the plaintiff has the tinnitus heor she claims to have. There are no objectivetests for the other three questions.
Send your questions to:Dr. Vernon c/o ATA, Tinnitus Thday/Q&A,PO Box 5, Portland, OR 97207-0005
Tinnitus Today/September 1996 21
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
22/28
Profile: NewATA BoardMember Paul J. Meade
Paul Meade
Paul Meade, a CertifiedPublic Accountant andChief Financial Officer forGaylord Industries inOregon, joined ATA's Boardof Directors on June 11,1996. Paul's connection totinnitus is not professionalbut it is personal. Both Pauland Phil Morton, ATA's
board chairman, work for the same company.His proximity to Phil on a daily basis has givenPaul the opportunity to see a person's strugglewith tinnitus first hand . Paul writes, "Witnessingthe difficulties Phil Morton has in conductinghis job has helped me to understand the magnitude of the problem and how challenging it canbe. l also have a desire to give back to the community, to help the millions of people affectedwith tinnitus."
We gratefully thank Paul for his willingnessto serve on ATA's Board of Directors.
WANTED!HEARING-AIDS AND/ OR
MASKERS IN ANY CONDITIONIf you have ever wondered what to do ~ " l i t h thosaids that are just sitting in the drawer, think nofurther. ATA will be happy to receive them.Donations to ATA are tax deductible, and we'llprovide an acknowledgement. Simply packagethem up carefully (a small padded mailing bagfine) and send to :
ATA, PO Box 5, Portland, OR 97207.If you are using UPS or another shipper, ship toour street address:
ATA, 1618 SW 1st Ave., #417, Portland, OR 97201What happens to the aids that you turn in? Insome cases they can be repaired and given toneedy people or used in charitable missions tounderdeveloped countries. Even i f they can't bereused as is, the parts are needed for repairingother aids. (And the plastic is recycled.) Your olaid could give someone the gift of hearing'
SPACE STILL AVAILABLE- CALL OR FAX TODAY!Targeting
1111.- 1111.- 1111 TinnitusATA REGIONAL MEETING
FOR PATIENTS AND PROFESSIONALSSEPTEMBER 26 , I 9 9 6COLLEGE PARK, MD
YES! I WILL AlTEND THE ATA REGIONAL MEETlNG SEPTI:MBER 2 6 , 1996A T THE IN N AND CONF ERENCE CE NT E R UNIVERSITY O F MARYLAND UNIVERSITY C O L L E G E , C O L L E G E PARK M D
NAME:_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _TEL :_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __ _
BUSINESS NAME:_______________________ AX:___________ADDRESS:_________________ rTY _ _ _ _ _ _ _ _ _ _ _ TATE ZIP
ENCLOSED IS A CHECK FOR MY $ 7 5 REGISTRATION FE ECHARGE MY $75 REGISTRATION FE E TO MY VISA/MASTERCARD
ACCOUNT # - - - - - - - - - - - - - - - - - - - - ~ ~ - - - - - - - - - - - - -ExPIRATION DATE TELEPHONE #--------- --------------SIGNATURE__________________ _I AM ATTENDING BECAUSE:
I HAVE TINNITUSA FAMILY MEMBER HAS TINNITUSI TREAT TINNITUS PATIENTSOTHER.________
TH E INN AND CONFERENCE CENTER HAS A UMITED NUMBER OF GUEST ROOMS AVAILABLE AT $74 SINGLE, $89 DOUBLECALL ( 8 0 0 ) 7 2 7 - 8 6 2 2 TO MAKE ROOM RESERVATIONS DIRECT LY WITH TH E CENTER
PROFESSIONALS PLEASE INDICATE CONTINUING EDUCATION CREDITS ( C E U s ) DESIRED: ASHA NIH S STATE
FAX THIS F ORM TODAY T O : (503) 2 4 8 - 0 0 2 4 O R C A L L (503) 2 4 8 - 9 9 8 5 E XT I 822 Tinnitus 1'bday/September 1996
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
23/28
Rising Above the Cacophonyby Mary Holmes Dague
Cupping your hands over your ears, youconfront the most feared question: can tinnitusget worse? Indeed it can. In the forty-threeyears I've lived with the malady, the sounds inmy head have developed from mere whispers tosirens, now approximately as loud as a lawnmower with pitch double the highest piano key.Tinnitus became my companion when I wasfour years old, the result of taking antibiotics. Inthe history of medicine, the development ofantibiotics ranks as one of the highest accomplishments, comparable to today's elusive searchfor a cure for AIDS. But in the early 1950s, thefull risks of antibiotics were not knownalthough the benef its were. Who could fault apediatrician for prescribing Aureomycin for ea rinfections at doses known now- but not then- to be too high?I knew a year before starting kindergartenthat I didn't hear as well as others and I knewalso that little sounds scurried about my ears.Neither frightening nor annoying, the tonesswayed through me, often taking shapes ofmusic in my in1agination. Since I was alreadystudying modern dance, the constant flow ofnotes seemed almost a gift to inspire newmovement.Never once did I consider telling the doctor,my parents, or my best friend that my perceptions of the world differed a bi t from theirs. Thehearing problem was minor and the tinnitus, aword I was no t to understand for many yearsyet, seemed insignificant.My elementary school career began brilliantly. A natural lip-reader; I found little impediment to hearing in the classroom. The annualhearing test was performed en masse, at cardtables. But in third grade, the school purchasedmy nemesis: a huge, gray, Beltone audiometer.The school nurse began testing students individually, and I was caught. Before informing myparents, the nurse tested me at least fifteentimes, challenging me each time "to do better"an impossibility. Now my imagination was racing not dancing: I could see myself admitted tosome school for the deaf, ostracized from myfriends. Suddenly I'd become, to my own mind,something of a freak.
Nightmares began to become true as thelocal otolaryngologist to whom I was referredquickly prescribed a tonsillectomy. So disappointed was the doctor when post-operativehearing tests showed no improvement, thathe recommended further surgery - amastoidectomy.
The pediatrician stepped forward, sendingme for a second opinion to Edmund P Fowler,Jr., M.D., Chief of Otology at ColumbiaPresbyterian Medical Center in New York City.Dr. Fowler, internationally famous as an otologist and researcher, dismissed the specter ofmastoidectomy within a moment of our meeting. My hearing loss was clearly caused bynerve deafness, and he was certain theAureomycin prescribed earlier was the cause.Dr. Fowler's mind ran at the speed of light; Isometimes marveled that even he could keep upwith his thought processes. Yet, his compassioninvoked the finest qualities of a healer. The doctor ran me through several weeks of testing atthe Speech and Hearing Clinic (which is nownamed for him) before the audiologist discovered my lip-reading. Dr. Fowler greeted thatinformation with a characteristic hearty laugh,congratulated me on my good work, andordered the evaluation re-done.On the very last day, after the very last test,the audiologist asked me one question: "Do youhave ringing in your ears?" At last. Someone hadasked the forbidden question. For seven years,I'd kept this secret. I responded with my ownquestion: "Is there any surgery for it?"
The answer of course was no, and for thefirst time I acknowledged the condition.Tinnitus. By withholding information about tinnitus, which is often the first sign of nerve deafness, I'd managed to push away the diagnosisfor years, caused myself one unnecessarysurgery, and came close upon another!My hearing loss then wasabout 25%, and the tinnitus noninvasive. Luckily, Dr. Fowler wasa tinnitus researcher, and hetalked with great enthusiasmabout the subject, always trying tolearn something new from me,sharing his knowledge in return; his positive attitude infused me. Asking questions
Tinnitus TOday / September 1996 23
7/30/2019 Tinnitus Today September 1996 Vol 21, No 3
24/28
Rising Above the Cacophony continued)about my dancing, the novel in my hand, plansfor college, Dr. Fowler wanted to know how mylife was progressing; my healing and tinnitus hecould evaluate himself. Never would he say, asotolaryngologists often do, "Just live with it!"This otologist's message was simple andhumane: "Live!''Before his sudden death when I was 16 yearsold, Dr. Fowler admonished me never to take upcigarettes, and suggested I may no t experiencefurther development of tinnitus. I had lost agreat friend and ally, and tried to memorizeevery moment we had shared as doctor-patient.I had never met anyone who had tinnitus or ajuvenile with hearing loss; this great physicianhad understood my journey and made me feel Iwas not alone.Although I never smoked a cigarette, tinnitusdid increase as my hearing declined. In additionto severe tinnitus, my hearing loss is now about90%. There's no cause for sadness, though : Iwear two programmable ReSound hearing aids,
Developed by SpeechPathologist. Mary Kleeman,the I See What You Sayprogram provides aninteresting. new approach toacquiring speechreadingskills for the hard ofhearing.
"Instruction andpractice areimaginative,easy to follow andenjoyable."Journal SelfHelp for
Hard of Hearing People
Learn Lip Readingwith this Fun,
Self-Help,Easy to Use,
Lipreading CourseVideo & Manual
Compensate for Noise & Tinnitus Aid Speech Discrimination En hance Communication Stop Feeling IsolatedThis clearly presented format ofinst.ruction includes practice activitiesfor single words to stories. Sixteenspeakers arc presented.
****mericanUniversityWa$ltlngton , D.C.
24 Tinnitus Thday/ September 1996
1ip-read well, conduct business by TTY and cputer, and boast a sensitive family and selfappointed hearing-ea