Embed Size (px)
Citation preview
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 1/27
September 1998 Volume 23, Number 3
Tinnitus TodayTHE JOURNAL OF TH E AMERICAN T INNITUS ASSOCIATION
In This Issue:
"To promote relief, prevention, and the eventual cure of tinnitus forthe benefitof present and future generations"
Since 1971
Education - Advocacy - Research - Support
Sound Sensitivity- Hyperacusis and Recruitment
Pulsatile Tinnitus
Can You Feel What I Hear?
New ATA-Funded Research
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 2/27
ASound Pollution Solution~ i l l l l l l l ~ Sound lherapy - this is a relatively
untapped lifesty le enhancer. You're
providing yourself with a much healthi
er environment-a break from "sound pollution." It's a
whole new way to relax and soothe your senses. Thesounds of nature have away of bringing you to a different
place - a place where you II revel in agreat night's sleep; a
place where your concentration can be heightened and a
place where lhe stress of the dayvanishes almost instant
ly. Simply turning on a Marsona Sound Cond itioner from
Ambient Shapes can bring these pleasing sounds and
serenity to your life.
You see, sound conditioning makes
your surroundings as tranquil as a ight
spring rain or night time at a mounta in
lake. The lim its arestrictlywhere your
mind can take you. Sound Conditioners from Ambient
Shapes provide the stimulus, your body relaxes and your
mind goes where it wants to be. Let yourse lf be taken
away and let tranquility finally be a par t of your life
whether you're having difficulty sleeping, keeping on
track while working at home or the office, surviving the
unpleasantness of Tinnitus or trying to make it through
your stressful day. This cou ld be the simplest answer to
your toughest problems.
~ ~ ~ Three popular units offer you theH
.. . .. sounds that mother nature intended
for us to hear. One is perfect for the
home or office while the others are small and portable
enough to be taken with you when travelling.
ORDER TOLL FREE NOW
Major credit card holders please call toll free . Order
Item# MA1280 for theHome/Office Sound
Conditioner - $149.00 • Item # TSC350 CombinationSound Conditionerffravel Alarm Clock - $99.00 •
Item # TSC330 Model Sound Conditioner - $79.00
(FRE Eshipping & handling in USA). NC residents
add sales tax. One (1) year warranty
- Thirty (30) day money back guarantee.
800-438-2244Toll Pree Pax :800!872-2005•www.arnbientshapes.com
Local: 828/324-5222 • Pax: 828/327-4634~ ~ f . mb ient Shapes, Inc.
P.O . Box 5069 Hickory, NC28603-5069 U.S.A.
1280 for Office or Home:Create apersonalydes ignedsound environmentwith the ultimate inhigh quality s
avariety of soundselectionsand
ease of operation. The 1280 features "user friendly" push
buttoncontrols, LE Ds to
hghlight selections, and
slidecontrols ortoneand vo lume.
ITEM # MA1..... ......$1
SOUND SELECTIONS: Surf I • Su rf II • Brook • Rain • Waterfall • Train • Forest • Wind • C
eve • Lake shore • OVERLAYS: Sea gull • Buoy • Loons • Dove • Cricket • Hawk • R
Crossing • Owl • Frogs • Songbirds • FEATURES: Programmable "overlay sounds" • Dist
styl ing • Optional60 minute shut-off timer • Integ rated circuitry • Simple push button ope
• Digitized & synthesized effects • Color LED selection indicators
TSC-350 & TSC-330 for Travel:Compact and lightweight, these are ideal for the person on the move while still offering tile
masking capabilities of many full sized sound conditioners. Help create a familiar sound env
ment while away from home by emu lating Rain, Waterfall and Surf to mask unwanted sound
and noise.
-TS C-330 FEATURES: TSCC-330 camper model
comes with AC adapter &a DC auto connector •
TS CI-330 international model has adual voltage
power supply for overseas travelling • Distinctive
styling • Travel pouch included • Solid state
electronics • Quality construction
ITEM # TSC330 ..... .. ...$79oo
220/240 Volt Models add $1 o.oo
TSC- 350 FEATURES: Combination sound
tioner and travel alarm clock • Buill-in digita
alarm clock with LCD display • Gentle A
Travel Aarm • Available in a110 volt USA v
• TSCI-350 has international dual voltage •
350 Camper model has a 12 volt DC auto
Controllable LCD display light • Push button
tion • Side controls or tone and v
ITEM # TSC350 .. .... ...$
ALL MODELS: 30-day unconditiona l guarantee • One Year limited warranty • Made in he U

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 3/27
Tinnitus T o d ~ y Editorial and Advertising ofices:American Tinnitus Association, P.O. Box 5, Portland, OR 97207 • 503/248-9985, 800/634-8978 • [email protected], http:fjwww.ata.org
Execmive Director f.- Ediwr:Gloria E. Reich, Ph.D.
Associate Editor: Barbara ThbachnickT'mnuus 'Tbday is published quarterly in
March, June, September; and December. li ismailed to American Tinnitus Associationdonors and a selected list of tinnitus sufferers and professionals who treat tinnitus.Circulation is rotated 10 80,000 annually.
The Publisher reserves the right co reject oredit any manuscript received for publicationand to reject any advertising deemed unsuitable for Tinnitus 'Tbday. Acceptance of advertising by Trnnuus 'Ibday does nor constituteendorsement of the advertiser, its productsor services, nor does Trnnttt<s Tbday makeany claims or guarantees as 10 the accuracyor validity of the advertiser's offer. The opinions expressed by comributors to Trnmtus
'Ibday are not necessarily those of the
Publisher, editors, staff, or advertisers.American Tinnitus Association is a nonprofit human health and welfare agencyunder 26 USC 501 (c)(3).
Copyright 1998 by American Tin nitusAssociation. No part of this publication may
be reproduced, stored in a retrieval system,or transmitted in any form, or by any means,without t.he prior written permission of thePublisher. ISSN: 0897-6368
Executi.ve DirectorGloria E. Reich, Ph.D. , Portland, OR
Board of Directors
James 0. Chinnis, Jr., Ph.D., Manassas, VA
W. F S. Hopmeier, St. Louis, MOGary P. Jacobson, Ph.D. , Detroit, MISidney Kleinman, Chicago, IL
Paul Meade, Tigard, OR. Chmn.
Philip 0 . Monon, Portland, ORStephen Nagler, M.D., F.A.C .S. , Atlanta, GADan Purjes, New York, NY
Aaron I. Osherow, Clayton, MOSusan Seidel, M.A. , CCC-A, Towson, MDJack. A. Vernon , Ph.D . Portland, ORMegan Vidis, Chicago, IL
Honorary DirectorsThe Honorable Mark 0. Hatfield,
U.S . Senate, RetiredThny Randall, New York, NY
William Shatner, Los Angeles, CA
Scientific Advisor yCommitteeRonald G. Amedee, M.D., New Orleans, LARobert E. Brummett, Ph.D., Portland, ORJack D. Clemis, M.D ., Chicago, ILRobert A. Dobie, M.D., San Antonio, TXJohn R. Emmett, M.D., Memphis, TN
Chris B. Foster; M.D., La Jolla, CABarbara Go ldstein, Ph.D., New York, NYJohn W, House, M.D., Los Angeles, CAGary P. Jacobson, Ph.D., Detroit, MlPawel J. Jastreboff, Ph.D., Baltimore, MDRobert M. Johnson, Ph.D., Portland, ORWilliam H. Martin, Ph .D. , Portland, OR
Gale w. Miller, M.D., Cincinnati, OHJ. Gail Neely, M.D., St. Louis, MORobert E. Sandlin, Ph.D., El Cajon, CAAlexander J. Schleuning, n, M.D.,
Portland, ORAbraham Shulman, M.D., .Brooklyn, NYMansfield Smith, M.D., San Jose, CARobert Sweetow, Ph .D. , San Francisco, CA
Legal CounselHenry C. BreithauptSteel Rives Boley Jones &- Grey,
Portland, OR
The Journal of the American Tinnitus Association
Volume 23 Number 3, September 1998
Tinnitus, ringing in the ears or head noises, is experienced by as manyas 50 million Americans. Medical help is often sought by those whohave it in a severe, stressful, or life-disrupting form.
Table of Contents
7 ATA's New Board Members
9 Pulsatile Tinnitus
by John Risey, M.C.D., and Ronald G. Amedee, M.D.
11 A Tribute to the Chairman of the Boardby Cliff Collins
11 Introducing ATA's Board Chairman Paul Meade
13 New ATA-Funded Research
14 Sound Sensitivity
by Barbara Tabachnick
17 Can You Feel What I Hear? An Audiological Perspective
by Norma Rivera Mraz
19 A Self-Help Journey
by Carrol Jude
20 ATA Support Givers - Welcome!21 Collectible Commemorates Quest for Silence
and Benefits ATA Cause
by Corky Stewart
Regular Features
4 From the Editor
by Gloria E. Reich, Ph.D.
5 Letters to the Editor
22 Questions and Answers
by Jack A. Vernon, Ph.D.25 Special Donors and Tributes
Cover: 'Exquisite• (28"x 36" oi l on canvas) by Arletha Mueller Ryan, 15 Touchstone,
Lake Oswego, OR 97035, 503/636-8838

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 4/27
FROM THE EDITOR
by Gloria E. Reich Ph.D.,
Executive Director
National Health Council which promotes thehealth of all people by advancing the voluntahealth movement.
As summer draws to a close, A very interes ting item came on our e-maATA's
activitiesgather momen
- recently. Ithad
to do withgenetic
research antum. Many hearing-related was entitled "What's Blond and Blue-Eyed and
societies have their annual Read All over?" Have you guessed? The answ
meetings in the fall and tradi- is Iceland DNA (deoxyribonucleic acid, thetionally ATA attends these to basic genet ic material of human life). In this
provide information about tin- example, Icelandic DNA data was said to be
nitus and tinnitus research to much sought after by pharmaceutical compa-the attendees. This year will nies who have found that they are able to loc
be no different. We look forward to seeing many genes responsible for disease about four t i m ~of you at the International Hearing Society, the faster than from DNA in the general populat1American Academy of Otolaryngology Head and Furthermore, geneology is a national pastimeNeck Surgery, the Academy of Dispensing Iceland with most families being able to traceAudiologists, and the American Academy of their roots back to about 900 A.D. Now, all we
Family Physicians meetings. have to do is to encourageThis year I will again be a research about hearing defects
guest speaker at the Sixth Annual using this fantastic database anConference on Tinnitus perhaps we'll get some of theManagement in Iowa City, IA, on breakthroughs we're all hoping
September 18-19. This year's guest for. Anyone in Iceland haveof honor will be Dr. Peter H. tinnitus?
Wilson, a psychologist from South We recently heard from Judy
Australia, who will be speaking Brivchik, our tinnitus support
about attention control and cogni- group leader in Lancaster, PA,tive restructuring therapies for that July was, in Pennsylvaniatinnitus. The conference is open least Tinnitus Awareness Mon
I
to professionals and patients. For _ What a great idea! You can conmore information contact Richard ,2"_ tact your local city or state'Jyler (319/ 384-9757). Tony Randall new son, officials about having tinnitus
The National Institute on Jefferson Salvmt Randall recognized for a special week o
Deafness and Other Communication Disorders month where you live.
(NIDCD) held a principal investigators meeting Honorary ATA board member Tbny Randaabout tinnitus in May. As an invited guest, I was is pictured here with his second child, Jeffersvery happy to hear these investigators discuss Salvini. Jefferson was born June 15 , 1998 and
the latest tinnitus research findings and their also welcomed by his mother Heather and sisideas for future studies. In general the National Julia, who was born Aprilll, 1997. Our conglnstitutes of Health (NIH), of which the NIDCD ulat ions to the entire family.
is a part, is attempting to engage the public to Lastly, I regret to report the deaths this su
help set research priorities. Right now your con- mer of two valued colleagues and friends,gressional representative is the best person to le t Donna Dickman, Ph.D., Executive Director o
know how you think the government the Alexander Graham Bell Association for thagencies should be spending Deaf, and Aram Glorig, M.D., a leading authoresearch dollars. In the futurethe NIH hopes to create an ty on the ear and its disorders. Dr . Dickman w
a strong voice for oral deaf education. Dr. Glooffice of public liaison to review first observed cases of severe hearing impair-~ ~ ~ 4 ~ i } ~ G ~ ~ ~ ...... .. and respond directly to public ment and tinnitus caused from bomb and she
input. ATA not only talks blasts while he was stationed in England duridirectly with officers of the Second World War. Dr. Glorig addressed th
. .~ ~ ~ ~ ( l t h e NIDCD but also Fifth International Tinnitus Seminar in 1995participates in the about noise-induced hearing loss. B
4 T inn i tus Thday/ Septe mber 1998

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 5/27
Letters to the Editor
From tirne to tirne, we include letters
from our members about their
experiences with "non-traditional"
treatments. We do so in the hope that
the information offered might be helpful.
Please read these anecdotal reports
carefully, consult with your physician or
medical advisor, and decide for yourself
if a given treatment might be right for
you. As always, the opinions expressed
are strictly those of the letter writers and
do not reflect an opinion or endorsementbyATA .
Iave been a long time member of your orga
nization and an avid reader of your journal,Tinnitus 7bday. A common theme I see in
your journal is a distinct frustration on the part
of your members with the medical profession. Ialso believe that this frustration leads to considerable disappointment and anger and potentialanimosity towards our profession.
As you know, tinnitus is a very difficult,
challenging complaint. Unfortunately, themajority of causes of tinnitus are idiopathic(of unknown origin), despite very expensiveworkups and evaluations.
What you need to know, though, is that it isextremely frustrating for us as health careproviders also. Despite attending many seminars and reading many journals and textbooks,I still do not have an answer for many of the
causes of tinnitus I see daily in my practice.Certainly I am not satisfied with this and hope-
fully in the future this will be resolved.
It is encouraging to me that such concepts asTinnitus Retraining Therapy bring hope to aU of
us. In addition, the recent identification of aregion of the brain that seems to register the
tinnitus is also encouraging. We in the profession do not have all of the answers nor do wemaintain that we do. We do, however, workhand-in-hand with our patients, with mutual
respect and empathy. Please do not take our
inability to provide immediate resolution of the
tinnitus complaint as evidence of indifferenceand arrogance. This is certainly not the case. We
all look forward to the day when we can provideour tinnitus patients with a distinct and absolutecure for their tinnitus.
Stuart A. Morgenstein, MD , 231 S. Ga1y, Suite#110, Bloomingdale, TL 60108, 6301307-0088
M wife, who has had tinnitus for a number
of years, was getting very depressed
because of it. I took her to an otolaryngologist who said there was no cure for tinnitus and
to go home and learn to live with it. I then tookher to a TMJ dental surgeon. After $566 worthof x-rays, he recommended treatment at a costof $1500 with no guarantees. Our insurance
wouldn't help.
I have been studying herbal medicines and
decided to have my wife try St. John's Wort forher depression rather than the Zoloft our familydoctor prescribed. After a month of taking St.John's Wort, her depression was much better
and the pounding has stopped. She is the best
she has been since the tinnitus first started.Even the ringing is better. Perhaps this mighthelp someone else. Keep up your good work.
Donald G. Haynes, 1040 Greenwood Dr. #JA,Hendersonville, NC 28791 -1912, 7041698-8686
Snce the early '70s, I have suffered from a
neural damage/high tinnitus whine compounded by a blood pulse that I hear every
waking moment. I haven't found a cure foreither of these conditions, but my reaction tothem could be useful to others, namely to lookfor a positive side (believe it or not!) to this
condition.
I am a professional scientist and also, 1 am
told, a creative person. And fortunately so. Ineed to keep my attention occupied so I don'thave to focus on the fun and games going on in
my head. Perhaps in keeping my mind active,often to the point of exhaustion, I have also kept
myself sane.
There are two things Twould like to share.In 'Transcendental Meditation (TM), which Istudied in the 1970s, they teach each student aspecial sanskrit word, the repeating of which
leads to a meditative state. From studying my
reaction to meditation, I found that with time, Ino longer need a magic word. Instead I focus onmy blood pulse and neural whine and after a
Tinnitus ibday/ Scptember 1998 5

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 6/27
Letters to the Editor (continued)
while, pass into a progressively deeper meditational state. My tinnitus then gives me an infallible clue as to my level of meditation and mental
state: as I get deeper in, the tinnitus initially getslouder, and then at a certain point drops away.After 20 minutes or so, I return refreshed without the tension I accumulate after a day of
listening to myself. I use my "defect" as a tool todetermine if I am entering calmer meditationalstates.
I have also found a way of listening to music
that provides me with a tool to help me ignoremy own "music." I play my favorite tapes (especially percussion) many times until I know them
by heart. By listening carefully, I noticed that
my mind anticipates each coming note, as if itwere grasping it, or checking it with its memory
of the musical piece. Then I need only try and
dislodge my attention from the music . If 1 am
successful, the music essentially fades out leaving me in a meditation. This is also what I dowith tinnitus: I focus on it intently for a number
of minutes, and it tends to fade as my mind getstired ofbeing forced to grasp the noises. The
interesting thing is that the internal noises of
tinnitus are only unbearable when I allow an
invisible mental hand to grasp at the noiseinstead of allowing the sound to pass through
my mind like the noise pollution it is.
I hope this can help. In any case, it will giveyou some internal games to play with your
favorite record! I would be curious to hear
written reactions from others who tr y this.
John F Caddy, Via Cervialto 3, Aprilia 04011,
Latina, Italy
Im beginning with carefully selected patients
to offer Tinnitus Retraining Therapy (TRT) in
my clinic. No, I have not taken one of the
courses at the University of Maryland and I disagree with the implications that physicians and
audiologists who have no t been formally trainedcannot adequately provide TRT. I do understand
the need to avoid the impression among practitioners that TRT is as easy as placing devices in
people's ears. I have encountered some patients
wearing these devices (dispensed at other clinics) who have no understanding of their tinnitus,the use of the devices, or even of the ultimate
goal of the therapy. I believe that physicianswho have a sincere interest in treating tinnitus
patients, who are compassionate enough and
patient enough to hear their worries and who
6 Tinnitus ll:lday/ September 1998
take the time to educate their patients and thfamilies, can provide TRT effectively.
I will be attending one of the courses inBaltimore in the near future but this is in the
spirit of thoroughness and sincere interest inthis topic. Perhaps the message to ENT physicians should be, if you don't have 80% or gresuccess, learn from those with experience wh
this might be.
Michael T Thixido, M.D., Family Ear;Nose & Throat Physicians, Limestone MedicCenter, 1941 Limestone Rd., Suite #103,Wilmington, DE 19808, 302/998-0300
I
n July 1995, I overpressurized my left midear while trying to equalize underwater.Immediately thereafter an d ever since I
have had a high-frequency ringing in my ear.Consultation with physicians at the time resuin a prognosis of one of two things happeningeither the ringing would go away, or I wouldhave to live with it. After three years of livingwith it I obtained some literature from theAmerican Tinnitus Association and decided tseek out a specialist.
The masker I now wear gives me a degreof control that I never had before. The "shhh"sound made by the device is certainly easier live with than the "eeee" that my ear produceon its own. The ability to increase or decreasthe volume of the masker allows me to adjusthe contrast between the two sounds. I can
choose to hear a blend of the two sounds or Ican completely drown out my tinnitus sound
and bear only "shhh." Bedtime used to be thetime that my tinnitus annoyed me the most,now I can decide what sound I want to hear
when falling asleep. There is already a residusoothing effect from the masker that makes tringing less noticeable even when I'm not weing it.
I hope you will relate my experience to otpatients so that they might be encouraged in
their struggle with this condition.
Neil A. Best, 1400 S. Joyce St., ffl511,
Arlington, VA 22202, 703/979-0169
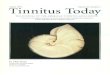
In his "Questions and Answers" column in tJune 1998 Tinnitus Tbday, Dr. Vernon mentions that 25 dB is the loudest tinnitus he h
ever measured. I hope that readers will not
misinterpret this finding, which refers to the nitus decibel level over the threshold of heari
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 7/27
ATA's New Board Members
Gary P Jacobson, Ph.D.,Director, Division ofAudiology,Henry Ford Hospital & Medical
Center, 2799 W: Grand Blvd.,Detroit, MI 48202-2689,313/876-3280
Dr. Jacobson writes:
I became interested in t innitus during th e development
of a grant eight years ago. ItGary P. Jacobson, Ph.D. became clear to me then that
there were few clinical centers that existed
solely to manage the millions of patients withsevere and disabling tinnitus. I am still dismayed that although hearing loss, dizziness, ear
pain, and tinnitus are symptoms of ear disease,
all but tinnitus are discussed in detail in mos tgraduate programs in audiology . Because of this,I have spent much time over the past seven
years lecturing in the area of tinnitus.
Due largely to the combined efforts of the
ATA and contemporary research scientists, there
has been significant progress made over the past
10 years in the understanding of physiologicalmechanisms underlying tinnitus and in the
management of this disorder. My goals are forthe ATA to continue to support these endeavors,to continue to lobby Congress to fund tinnitus
research, and to continue their superb effortsinforming the pa tient community of the fru its of
this research.
I accept this appointment in an attempt tobetter represent to the Board the views of clini-
cians who are engaged in the management of
the tinnitus patient and of researchers who areinvolved in the study of this disorder.
Dr. Jacobson is also a member ofATA's Scientific
Advisory Committee.
Susan Seidel, M.A., CCC-A,Greater Baltimore MedicalCenter, 6701 N. Charles St.,Baltimore, MD 21204,410/828-2142
Ms . Seidel writes:
I have been an audiologist for39 years, the last 24 with theGreater Baltimore MedicalCenter. For 15 years running,
Susan Seide" M.A.
,CCC·A
I have also facilitated theBaltimore Area Tinnitus Self-Help Group with arolling membership of 200. (I have had severeleft-ear tinnitus for 30 years following a jet
engine exposure.)
As a newly-elected member to ATA's board,I would like to help with two goals of focus forthe ATA. One, I would like to see tinnitus and
no ise exposure preventive efforts included inelementary school curricula throughout the
country. And two, I would like to see tinnitustherapy approaches incorporated in all audio
logy graduate school curricula.I am very excited to help ATA reach its
goals - our goals - for th e future. B
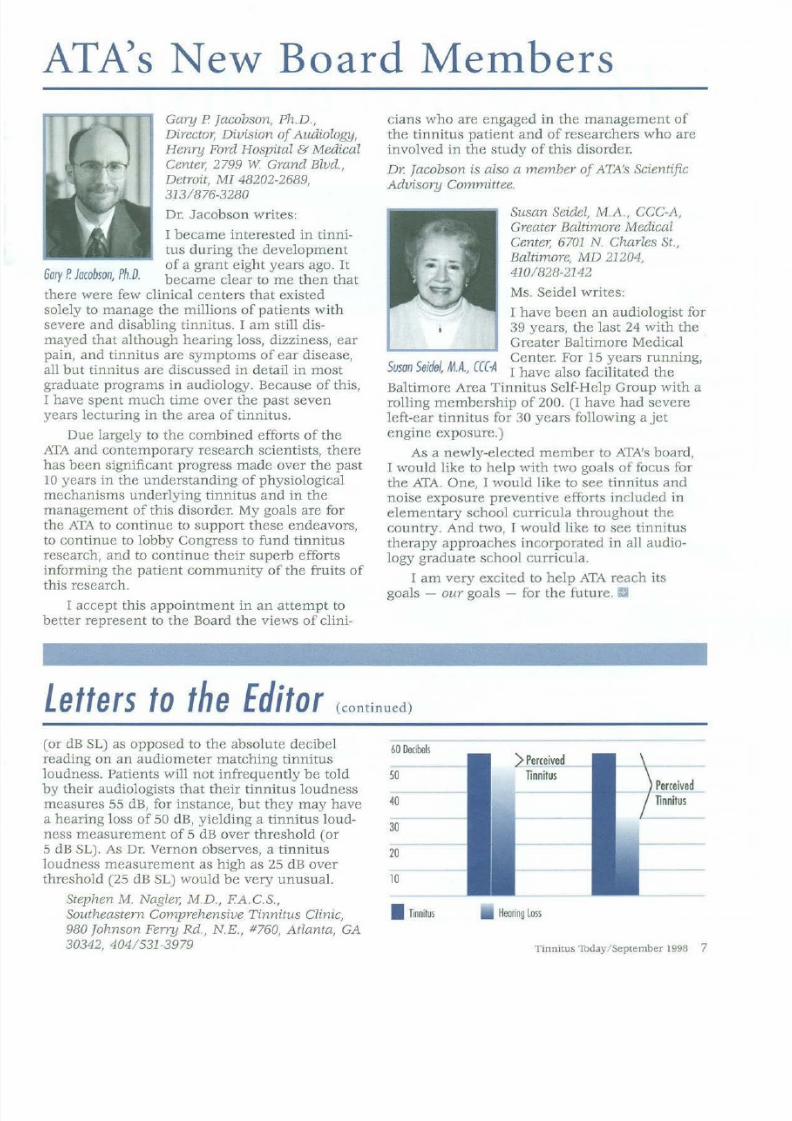
Letters to the Editor (continued)
(or dB SL) as opposed to the absolute decibelreading on an audiometer matching tinnitus
loudness. Patients will not infrequently be toldby their audiologists that their tinnitus loudness
measures 55 dB, for instance, but they may have
a hearing loss of 50 dB, yielding a tinnitus loudness measurement of 5 dB over threshold (or5 dB SL). As Dr. Vernon observes, a tinnitusloudness measurement as high as 25 dB over
threshold (25 dB SL) would be very unusual.
Stephen M. Nagler, M.D., F.A.C.S.,Southeastern Comprehensive Tinnitus Clinic,
980 Johnson Ferry Rd., N.E., #760, Atlanta, GA30342, 404/531-3979
60Dcibes
50
40
30
20
10
I Tinnitus
) Perceived
Tinnitus
Haring oss
)PerceivedTinntus
Tinnitus 1bday/ Septentber 1998 7
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 8/27
Advertisment
The Search is Over!Digital Tinnitus Mitigation ™
The FDA-approved Digital
Tinnitus Mitigation DTM-4
is the first multi-faceted cost
effective tinnitus alleviation
program ever developed.
The DTM-4 system includes
two CDs with unique digital
sounds that gently distract
hearing attention away from
tinnitus; one CD that provides
proprietary auditory training
sound patterns and verbal
instructions to train the user
to focus on sounds other than
the tinnitus; one CD that pro
vides methods and techniques
relating to stress-reduction,
coping skills and other factors
essential to successful tinnitus
alleviation; precision Sony
"ear bud" headphones for
optional private listening;
and a complete User
Guidebook. The Petroff
Audio Technologies DTM-4
system sells for $145+ $4 S/H
with a 30-day unconditional
money back guarantee.
8 Tinnitus Today/ September 1998
TESTIMONIALS ON DTM EFFECTIVENESS
The DTM technology effectively eliminates unwanted sound
produced below the tinnitus region, which to date has beethe major fault with conventional masking technology.- Dr. Jack Vernon (one of the world's foremost experts on tinnitus)
lam writing you to voice my unrestrained enthusiasm foryour DTM technology. I have to say I was completely over
whelmed by the sample you sent me. For years I have tried vaous devices in my practice. Personally, I suffer from tinnitus inboth ears. Your system alerted me to the potential that existswith well-thought-out solutions to this perplexing problem.- Dr. Steven M. Rouse (ENT)
I
have been a three-year sufferer of high-pitched tinnitus in
both ears. The condition reached a climax about six monthsago; at this time I could no longer achieve a good night's sleep(despite the use of a 1Sound soother' from the Sharper Image),and would always awake feeling slightly nauseated and dizzywith the condition continuing throughout the day. Throughout
this progression I have consulted among the best doctors in thefield. With failed treatments ranging from ginkgo biloba to having tubes surgically implanted, these fine physicians have com
up empty with respect to tinnitus. My initial reaction once Iturned on the first CD was one of utter amazement; I simply
could not believe how low the volume level was while maskingI can vividly remember having to turn the CD player on and oagain several times to make sure I still had tinnitus! With the
DTM process, I no longer hear the ringing (unless I concentrate). For the first time I have been able to get through a daywithout Advil and I have even been known to attend a fewmovies (with earplugs, of course). Thanks again."- Paul Pedrazzi
For information or to order at $145 +$4 S/H (Calif. res. add 81/2%)
with a 30-day unconditional money back guarantee, contact
Petroff Audio Technologies, 6520 Platt Ave. #813, West Hills, CA 91307
Ph: 81 8/ 883-1918 • Fax: 818/ 704-9976 E-mail: [email protected] site: wv.rw.tinnitushelp.com

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 9/27
Pulsatile Tinnitus
by John Rise'ft M.C.D., and Ronald G. Amedee, M.D.
Most people describe their tinnitus as being
constant or steady-state. A small percentage
(8-10%) of people, however, experience tinnitus
which they describe as rhythmic, beating,pounding, throbbing, or ''swooshing" in nature.Usually we are unable to hear the sounds causedby the heart forcefully pumping blood through
the arteries and veins. Attimes, however, these pulsations occur in or around
the middle ear or inner
ear, or near the hearing
nerve and become audibleto us. The perception of
the rhythmic flow of
blood through the head or
neck region is referred toas pulsatile tinnitus.These sounds become
audible as a result ofJohn Risey, M.C.D. uncontrolled high blood
pressure, erosion of bone
over an artery, certain benign vascular tumors,or crimped or constr icted blood vessels.
Pulsatile tinnitus can be classified as either
"objective tinnitus" if it can be heard by theexamining physician, or as "subjective" i f the tinnitus can only be heard by the patient. Pulsatiletinnitus usually occurs in one ear only and it isan important variant among tinnitus patients.One-sided tinnitus often indicates an underlyingmedical condition which can be quite serious but
which is usually correctable through medicine orsurgery.
Pulsatile tinnitus might occur as the person'sonly complaint or it might occur in conjunction
with other problems. The onset of pulsatile tinnitus is typically gradual and is often initially overlooked. The loudness of the pulsations might
grow somewhat over time. But most patients
report pulsatile tinnitus to be more of an annoyance than a severely intrusive experience.Possibly because pulsatile tinnitus does not
progress to a point where it is perceived as being
severe, only a small percentage of patients withthis complaint seek a medical evaluation withthis as their only problem. Patients are more
likely to seek medical attention when other complaints coincide with the pulsatile tinnitus.
Complaints of hearing loss, a sensation of
fullness in the ear, ear pain, drainage from theear in the form of pus or blood, and/or vertigo
might be experienced in addition to pulsatiletinnitus and require thorough medical and audiologic examinations. These additional symptoms
are associated with damage or disease affecting
either the middle ear,inner ear, and on occasion the hearing and balance nerves. A thoroughphysical examination by
an otolaryngologist can
reveal evidence of the
underlying cause in these
cases. The medical examination typically involvesvisual inspection of the
Ronald G. Amedee, M.D. eardrum and ear canal,
listening for pulsatilesounds through a stethoscope in various locations around the ear and head and neck, as wellas checking the blood pressure. In addition to
a medical examination, patients will undergo acomplete audiological examination. Hearingtesting is performed to determine what type(e.g. middle ear, inner ear, hearing nerve) of
hearing loss, if any, exists. In addition, tympanometry might be performed in an attempt to
record objective evidence of the pulsatile tinnitu s from the patient's ear canal. (Some typesof pulsatile tinnitus cause the eardrum to pulseevery time the tinnitus is heard by the patient.JYmpanometry tests how well the eardrumand bones behind the eardrum vibrate tosound.) Additional testing might be ordered if
the outcome of the physician's history-takingand physical examination or the audiologist'sexamination indicates a need for it.
These additional symptoms often indicatethe need for further workup: weakness or
numbness in the face, headache, double vision,or hoarseness. These complaints indicate that
the underlying cause of the problem could be
affecting more than just the hearing system.The specific combination of symptoms, and the
medical and audiologic exam results will help
the physician determine the need for further
evaluation(s).
More extensive diagnostic testing might be
ordered, including aCT scan, MRI, lumbar
puncture, and possibly an angiography. CTscans are computerized x-rays of the bony structures within the head and neck and are oftenuseful in cases of pulsatile tinnitus. These x-rays
Tinnitus lbday/ September 1998 9
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 10/27
Pulsatile Tinnitus (continued)
are ordered to establish if the problem is associated with erosion of bony structures within the
ea r and/or head. MRI is magnetic resonanceimaging, another computerized procedure whichis used to look at ''soft" (e.g. non-bony) tissue in
the same area and is especially helpful indetecting the presence of brain tumors. Lumbar
puncture is a procedure designed to detect the
presence of increased intracranial pressure. Aneedle is inserted at the base of the spinal column and a small amount of spinal fluid is
removed. Angiography is sometimes recommended to obtain a view of the blood vesselsin the head and neck looking for abnormalitiesin the arteries and veins which may be the
underlying cause of pulsatile tinnitus. Any or
all of these procedures might be required in
order to determine the underlying cause for the
complaint and to help establish a diagnosis.
Pulsatile tinnitus can be caused by many
medical conditions (see Thble 1). Some, such as
previously undiagnosed and untreated highblood pressure (hypertension), might be relatively easy to diagnose and treat. Other conditions might require surgery or the use of
radiation and chemotherapy. Conditions such ashardening of the arteries (atherosclerosis),benign intracranial hypertension1 and heart
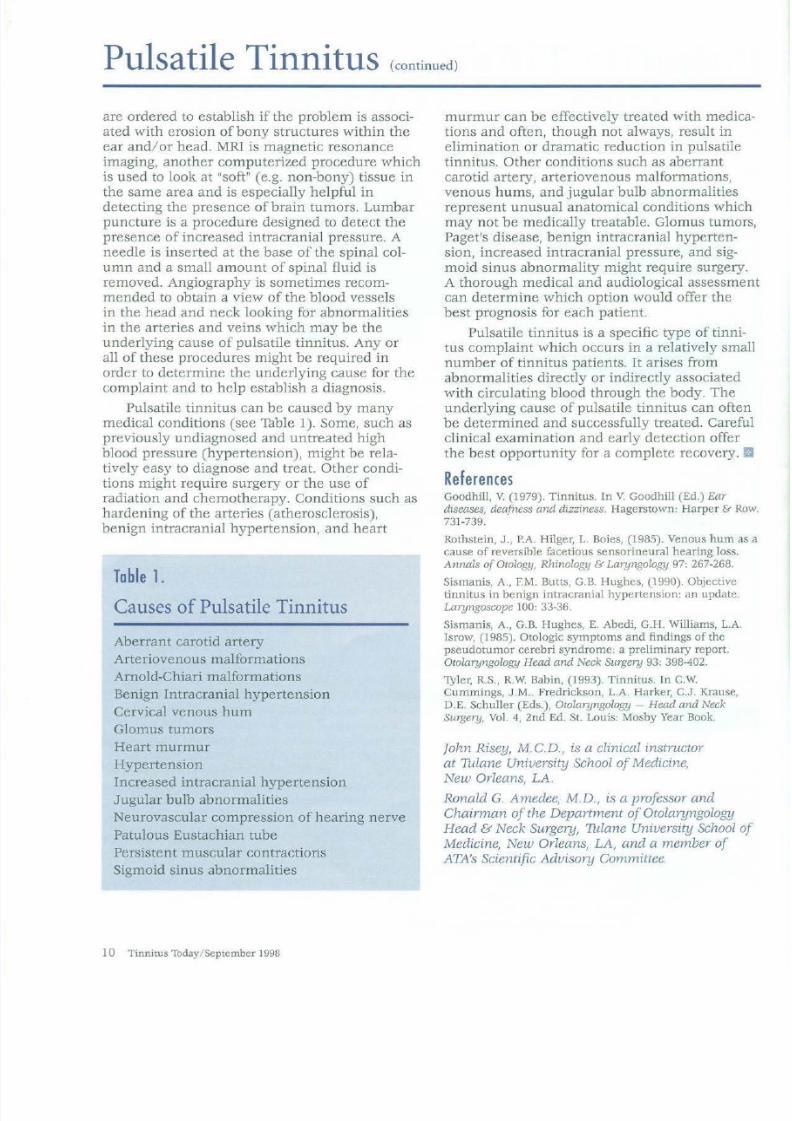
Table 1.Causes of Pulsatile Tinnitus
Aberrant carotid artery
Arteriovenous malformations
Arnold-Chiari malformations
Benign Intracranial hypertension
Cervical venous hum
Glomus tumors
Heart murmur
Hypertension
Increased intracranial hypertension
Jugular bulb abnormalities
Neurovascular compression of hearing nerve
Patulous Eustachian tube
Persistent muscular contractions
Sigmoid sinus abnormalities
1 0 Tinnitus 1bday September 1998
murmur can be effectively treated with medictions and often, though not always, result in
elimination or dramatic reduction in pulsatiletinnitus. Other conditions such as aberrant
carotid artery, arteriovenous malformations,
venous hums, and jugular bulb abnormalitiesrepresent unusual anatomical conditions whicmay not be medically treatable. Glomus tumoPaget's disease, benign intracranial hypertension, increased intracranial pressure, and sigmoid sinus abnormality might require surgeryA thorough medical and audiological assessmcan determine which option would offer thebest prognosis for each patient.
Pulsatile tinnitus is a specific type of tinnitus complaint which occurs in a relatively smnumber of tinnitus patients. I t arises from
abnormalities directly or indirectly associatedwith circulating blood through the body. The
underlying cause of pulsatile tinnitus can oftebe determined and successfully treated. Carefclinical examination and early detection offerthe best opportunity for a complete recovery.
References
Goodhill, V. (1979). Tinnitus. In V. Goodhill (Ed.) Ear
diseases, deafness and dizziness. Hagerstown: Harper & R
731-739.
Rothstein, J., P.A. Hilger, L. Boies, (1985). Venous hum acause of reversible facetious sensorineural hearing loss.Annals ofOtology, Rhinology & Laryngology 97: 267-268.
Sismanis, A. , F.M. Butts, G.B. Hughes, (1990). Objectivetinnitus in benign intracranial hypertension: an update.Laryngoscope 100: 33-36.
Sismanjs, A., G.B Hughes, E. Abedi, G.H. Williams, L.A
Isrow, (1985). Otologic symptoms and findings of thepseudotumor cerebri syndrome: a preliminary report.Otolaryngology Head and Neck Surgery 93: 398-402.
'!yler, R.S., R.W. Babin, (1993). Tinnitus. In c.w.
Cummings, J.M . Fredrickson, L.A. Harker, C.J. Krause,D.E. Schuller (Eds.), Otolaryngology -Head and NeckSurgery, Vol. 4, 2n d Ed. St. Louis: Mosby Year Book.
John Risey, M.C.D., is a clinical instructor
at Thlane University School ofMedicine,New Orleans, LA.
Ronald G. Amedee, M.D., is a professor andChairman of the Department ofOtolaryngologyHead & Neck Surgery, Thlane University SchoolMedicine, New Orleans, LA, and a member ofATA's Scientific Advisory Committee.

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 11/27
ATribute to the Chairman of the Board
by Cliff Collins
In June 1998, Philip 0. Morton stepped asideas Chairman of ATA's Board of Directors after
four years of service. Phil has served on the
board for ten years. I believe ATA members andsupporters should know
something about the levelof dedication Phil has
shown to the organization.
As noted in the June
1998 issue of TinnitusTbday, Phil was solelyresponsible for persuading
a national publisher of
high school textbooksto include mention of
tinnitus in their books. I t
.. is a prime example of thePhthp 0. Morton issue that is closest to his
heart: preventing young people from acquiringthe ear damage he himself did earlier in life.
Phil is in his mid-50s now, bu t he is still paying for the many years he spent as a guitarist in
a local rock band. In 1980, Phil came down withsevere tinnitus and hyperacusis, an oversensitivity to sound. He contacted the ATA to try to findhelp. Within a short time, he had taken it on as
his personal mission to warn young people about
the dangers of loud noise and loud music.In the service of that goal, he has gone to
schools to speak in classrooms, taking alongmemorabilia such as his old electric guitar and alarge photograph of his band taken the nightthey opened for the Beach Boys in Portland in
the 1960s. Phil knew if he could speak to kids on
their level, they would be more inclined to hear
his message.
He's also submitted to the public spotlightand appeared on talk shows, speaking openly of
his condition. He has encouraged others who
experience tinnitus to do likewise.
Undoubtedly Phil's most enduring legacyat ATA will be his creation of the Mission 2000plan, a carefully thought-out timetable for ATA's
growth and development. Mission 2000 ultimately was incorporated into what is now
called ATA's Strategic Plan, which encompasses
the organization's specific priorHies and reasonsfor being.
Fortunately, Phil will remain on the ATA
board for one more year, which gives the board
the benefit of his experience and also gives the
rest of us time to thank him for his years of service. Despite his tinnitus, Phil decided that the
best way to survive it was to take action. We canall gain inspiration from his example. a
Cliff Collins, of Aloha, Oregon, is a freelance writer.
INTRODUCING
ATA's Board Chairman
Paul Meade
Generally voluntary board
members have a vestedpersonal or professionalinterest in the non-profitorganization they're serving.Paul Meade doesn't havetinnitus; nor is he a hearing
heal thcare professional, but
he is the newly-electedChairman for the American
Tinnitus Association.
"I've seen the impact tinnitus has had on the
lives of friends. I never want to experience it
and I want to do all I can to further publicawareness and hearing protection activities,especially for youngsters," explains the 34-yearold father oftwo.
Phil Morton, retiring chairman, says of Paul,"He's a bright individual. And even though he
doesn't have tinnitus - maybe especiallybecause he doesn't have tinnitus - he looks atthings with a better and broader perspective."
As Chief Financial Officer for Oregon-basedGaylord Industries, Meade looks forward tohelping ATA "capitalize on the momentum
developed over the past few years through EARS
(the association's strategic action plan), research
funding, and recent publicity." Ill
Tinnitus Thday / September 1998 11
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 12/27
Advertisment
Free For 30 Days!
The Quick Reliet™Audio cassette orr CD Prrogram
Clinically tested and proven to be effective. Now available direct to you- free!
The Tinnitus Relief System (TRS) audio
programs were developed over several
years to make full use of an amazing
recording technology, 3-D Virtual Reality
Sound by Visual Sound. This technology
enhances the effectiveness of the TRS
products by combining entertaining,
soothing music and natural
recordings with digitally mixed,
sophisticated sound wave
composites (not static white noise).
This produces an exceptionally effective,
phase-canceling and masking effect.
This dual attack on tinnitus symptoms
provides a level of relief previously
unavailable to tinnitus sufferers.
Ask your ENT or audiologist about the
TRS programs.
"Personal Growth Technologies'Tinnitus ReliefSystem is the most effectiveand enjoyable clinically-proven tinnitusreliefproduct on the market today. "
-As Presented ByMichael LaRouere, M.D.1 Michigan Ear Institute
at the1997 AAQ-HNS Convention
Quick R e l i e f ' " users are finding their
two (2) CD or audio cassette programs
to be especially effective at reducing
their tinnitus and the stress often
associated with it.
All for just a one-time investment
o f $49.00 plus $3.95 SIH after
the 30 days. I 00% Guaranteed!
CALL NOW FOR QUICK RELIEFM!
Easy
Contact PGT's customer service departmentbetween 8:30 a.m. - 5:00 p.m. EST
1-800-511-0364Visit our website at: tinnitus-relief.com
1OOo/o GUARANTEED!404 East 10 Mile Road, Pleasant Ridge, MI 48069
Relaxing Effective Anytime Anywhere
12 Tinnitus Thday September 1998
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 13/27
NEW ATA-FUNDED RESEARCH
We are pleased to announce the
American Tinnitus Association's
support of the following tinnitus
research projects:Principal Invesigator: Kejian Chen , Ph.D.
Medical College of Ohio , Toledo , Ohio$33 ,000 for the study of spontaneous activity in
the dorsal cochlear nucleus following exposureto high intensity sound.
This study is expected to offer insight intothe mechanisms ofloud sound-induced tinnitus .The proposal aims to elucidate the cellular and
pharmacological mechanisms for the observedincreases in spontaneous firing rate in the dor
sal cochlear nucleus (part of the auditory pathway to the brain) after exposure to loud sound.The results will be useful for further experimental studies aimed to treat tinnitus with more specific drugs.
Principal Investigator: George M. Gerken , Ph.D.
Un iversity of Texas at Dallas, Callier Center for
Communication Disorders , Dallas, Texas
$30,000 for the study of auditory evoked potentials in tinnitus, hyperacusis, and hearing loss.
The experiments involve the auditory brain
responses that are evoked by brief sounds. In
problem-tinnitus patients, in hyperacusispatients, and in certain hearing-loss patients, it
is predicted that larger evoked potentials will be
obtained from some brain regions related tohearing. This research proposes to show that
some types of tinnitus and hyperacusis may be
caused by what are essentially mis-adjustmentswithin brain mechanisms. Previous research has
provided a handle which may permit some evaluation or even manipulation of the central auditory mechanism. If so, it may be possible to
alter or relieve tinnitus of central origin.
Principal Investigator: Mary B. Meikle, Ph.D .
Oregon Hearing Research Center, Oregon Health
Sciences University and Portland VA Medical
Center, Portland, Oregon$22,500 for the ATA National Tinnitus Data
Registry Project (NTDR).
The present registry contains detailed medical and audiological data from over 2600patients of the Oregon Hearing Research Center.
Over the next few years the registry willbecome national as it is expanded to include
information from other sites. The NTDR willprovide a systematic, well-documented, wellorganized basis for planning curriculum in med
ical and audiological training environments,increase public access to tinnitus informationfor their own health care needs, offer documentation concerning the relation between tinnitus
and disability, and provide data needed by
researchers in planning investigations about
tinnitus. This information will be useful to
major health care providers as well as the U.S.
government for public health care planning.
For a grant application and instructions,please send a request to ATA, P.O Box 5.
Portland, OR 97207-0005, call 800/634-8978, or
view the material on our website: www.ata.org.Click on "Tinnitus Research" for an on-lineapplication. Ill
WANTEDHEARING AIDS AND/OR
MASKERS IN ANY CONDITIONIf you have ever wondered what to do
with those aids that are just sitting in the
drawer, think no further. ATA will be happy
to receive them. Donations to ATA are taxdeductible, and we'll provide a receipt.Package them carefully (a small padded mailing bag is fine) and send to:
ATA, PO Box 5, Portland, OR 97207.If you are using UPS or another shipper,ship to our street address:
1618 SW 1st Ave., #417
Portland, OR 97201
What happens to the aids that you turn
in? In some cases they can be repaired and
given to needy people or used in charitablemissions to underdeveloped countries. Evenif they can't be re-used as is, the parts areneeded for repairing other aids. (And the
plastic is recycled.) Your old aid could givesomeone the gift of hearing!
Tinnitus 'Tbday/ September 1998 13

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 14/27
Sound Sensitivityby Barbaro Tabachnick,
Client Services Manager
Sound sensitivity has twoaccepted medical names -
hyperacusis and recruitment.However, people who havesound sensitivity describe the
experience with wide variation. Some sound-sensitivepatients are intolerant of a
particular appliance hum or the tone of a certainvoice. Some are devastated by any external sound
above a whisper. Some believe that they reallyhear too well (e.g., very quiet sounds in distantrooms) even when their measurable hearing losslogically negates the possibility. Some sound sensitive patients have no hearing loss; others have
significant hearing loss. Some have tinnitus -mild or incapacitating, with or without hearing
loss. Some have no tinnitus. Clinicians who treat
these patients define sound sensitivity with an
equal lack of consensus. Like tinnitus, sound sensitivity is a subjective experience an d is studiedbased primarily on the stories and observed reactions of the patients who have it.
Recruitm entRecruitment is a fairly common form of
sound sensitivity which can occur as a consequence of sensorineural hearing loss, ear surgery,
or ear-related illness,and which
occasionallyresolves on its own. A person with recruitment
finds that sounds at specific frequencies areuncomfortably loud, and that the sounds at thosefrequencies seem to increase in loudness quiterapidly. The loudness growth appears to occur in
the frequency range of that person's hearing loss.
Th e condition of recruitment - which generally co-exists with hearing loss - can be uncomfortable and unnerving. I t is often labeled
erroneously as hyperacusis, a more intrusivedisorder.
HyperacusisHyperacusis is an abnormal intolerance to
ordinary sounds. For the person with a severeform of this condition, an everyday noise - likethat from a dish being placed on a table - can be
far too loud, even excruciatingly loud. Hearing
loss and hyperacusis seldom occur simultaneously. Statistically, though, 90% of those who havehyperacusis also experience tinnitus - a constant
ringing or other distressing noise in the ears or
head. A few researchers regard hyperacusis as a"pre-tinnitus state" since tinnitus frequently
enough follows its onset.
14 Tinnitus Thday September 1998
Patients who are troubled by everyday envronmental sounds predictably have LoudnessDiscomfort Levels (LDLs) that measure below100 dB - often well below. Patients with sevehyperacusis can have LDLs in the 40-60 dB ra
The exact number of patients with hyperais unknown, perhaps because the definition o
hyperacusis and the ability to diagnose it varygreatly. The probability is also high that somepatients with concurrent disorders (like headadepression, or chronic pain) fail to report it.
What Causes Hyperacusis?Excessive noise appears to be a bonafide c
prit of this disorder. Some people report that thyperacusis began immediately following a siexposure to intense noise, like that from a gu
shot blast or an air bag deployment. Others
became sound-sensitive from long-term noiseexposure. Head injury, Bell's Palsy, chronic fasyndrome, epilepsy, Lyme disease, and drug seffects have all been associated with hyperacu
Josephine Marriage, Ph.D., audiological sctist in Cambridge, England, makes a distinctiobetween "central" and "peripheral" hyperacusiShe states that peripheral hyperacusis, seen foexample in Bell's Palsy patients, results from age to a mechanism (the acoustic reflex) in thitself. Central hyperacusis results from an abnmality in the mechanism in the brain that conthe amount of sound coming in. Marriage's 19
research examined the brain chemistry of patwith various neurological disorders (depressiomigraine, chronic fatigue, vitamin B-6 deficiensome forms of epilepsy, and others) - disordall known to co-occur with hyperacusis - in
search of a common feature in brain chemistrHer research indicates that a "disturbance," lika deficiency, in serotonin function in the braicommon to all of these disorders.
Although the exact point of injury and themechanism responsible for hyperacusis are nodefinitively known, most researchers believethe brain - not the ear - is the site of the prlem and that sound sensitivity is the result ofdysfunction in the brain's sound regulatory manism. Dr. Jonathan Hazell, tinnitus and hypecusis specialist in London, states that the cochof hyperacusis patients are of ten completely nmal. From the patient's point of view, howeveparticularly patients whose hyperacusis beganimmediately after a sudden exposure to very noise - the ears have it! These patients comm
ly experience ear fullness, ear pain, and muffhearing immediately preceding the onset of thhyperacusis.

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 15/27
Marriage offers another view on noiseinduced hyperacusis: excessive noise could damage the hearing mechanism "at the point where
the brain's 'efferent system' - the huge bundle ofnerve fibers that brings information from the
brain to the cochlea - joins up with the cochlea."She acknowledges that this is speculation, that
current research can neither refute nor confirmit. Elliot Rosenberg, M.D., summed it up: 11Theprecise nature or location of this sound adjustment mechanism is not yet known, but the
hyperacusis patient has clearly lost it."
What Makes Hyperacusis Worse?I t is a maddening enigma for hyperacusis
patients who find that their condition is worsened not only when they are exposed to noise,but also when they go too far to protect their ears
from it.11
Silence is the major factor enhancingboth hyperacusis and tinnitus," says PawelJastreboff, Ph.D., Director of the University ofMaryland Tinnitus and Hyperacusis Center.
Our sense of sight affords us an analogy.When we wake in the middle of the night, our
eyes are sensitive to all but very low-level light. Ifwe stay awake, we find that we can graduallyadjust to a slightly brighter light, then in time to
normal-level ambient light. Sensory organs that
are under-stimulated (like the eyes when wesleep) experience normal stimuli as excessivestimuli. When hyperacusic ears (or healthy ears
for that matter) are habitually protected withearplugs or earmuffs, they will experience normal sound as excessive sound when the muffs orplugs are removed.
Some hyperacusis patients have found that
caffeine, and a few antidepressant medicationslike Zoloft and Paxil, will make hyperacusisworse. (Fortunately, there are other medicationsthat can alleviate depression and not aggravatehyperacusis.)
Which Sounds Really Are Too loud?Many people with hyperacusis experience
palpable, legitimate pain from noise exposure -any noise exposure. So how can a person forwhom all sounds seem too loud determine whichsounds will actually cause damage? The debatelingers. Some doctors define excessive sound to
be sound at a level known to damage healthy
ears (100 dB and above). Hyperacusis patients say
excessive sound is any sound that hurts, even i f t
is 60 dB (the sound level of normal conversation)and they cite their reason: they do not havehealthy ears. Many sound-sensitive patients wear
earplugs and/ or earmuffs 12 or more hours a
day.I t
is understandable though ill-advised.Dr. Hazell acknowledges the difficulty hyperacu-
sis patients have accepting that "sound which can
be uncomfortable or even painful to the hearing
can be quite harmless to the ear."
Day-in and Day -out with Hyperacusis
The toll taken by hyperacusis on one's dailylife is significant, and in some cases dramatic.Scores of people with this condition avoid conversations above a whisper, shun all outside enter
tainment, decline attending family events, and
quit their jobs as they struggle to quiet down
their lives.
Nighttime for many is marred with sleeplessness. Daytime is punctuated with avoidance of
and accidental encounters with loud noise. Autensil against a dish, one's head rustling againstthe pillowcase, voices - including one's own -can drive the new hyperacusis patient to distrac
tion. A desperate few have resorted to barricading themselves in their homes for fear of
accidental exposure to a dog's bark or a car'shorn. I f it has progressed to this level, thenphonophobia - a fear of sound - is added to the
hyperacusis patient's list of woes. I t is a difficultspiral to unwind.
Dan Malcore was overvv-helmed by the suddenness and intensity of his hyperacusis when it
first appeared in 1991. Eight months along hisarduous road towards getting better, Malcorefounded the Hyperacusis Network, and beganpublishing a newsletter filled with everything he
could find on the subject. He encouraged hisreaders to write and submit stories about their
experiences which they did, and the network
flourished. It is from this bank of collected stories, and from his own experience, that he speaksou t on the subject of hyperacusis.
Malcore believes strongly that when sound
tolerances collapse suddenly and severely, and
most especially when the trauma is fresh,patients should use ear protection and refrainfrom sounds they cannot tolerate - at least forthe first few months - even i f he sounds are at
"normal" levels. "People have to stabilize some,and realize that they aren't going to get worse,"says Malcore. When a 40 dB whisper causes physical pain, people experiencing it cannot be convinced that 70 dB won't hurt them. He advisespatience and that in time, "they will slowly wean
themselves back into sounds."
Can Hyperacusis be Treated?Hyperacusis is many things: abnormal,
inexplicable, and - with much forbearance -treatable. Some patients have anecdotallyreported hyperacusis relief with blood pressure
reducing drugs like metopropol and popranolol,Tinnitus 1bday /Septembe r 1998 15

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 16/27
Sound Sensitivity (continued)
and with the anti-anxiety medication, Xanax.(Before beginning Xanax or any drug therapy, itis wise to weigh the potential benefit against the
potential for unwanted side effects.) In Goldsteinand Shulman's 1996 study of patients with dis
abling tinnitus and hyperacusis, audiological testspoint to the probable existence of several types of
hyperacusis. They write, "This could explain why
some individuals respond to treatment and othersdo not."
Tinnitus clinicians Jack Vernon, Ph.D., and
Pawel Jastreboff, Ph .D., Sc.D., concurrently discovered other workable treatments for hyperacusis while they were pursuing clinical care fortheir tinnitus patients. Their desensitizing treatment techniques have helped many hyperacusispatients become more tolerant of sound. Vernon'slow frequency (200-6000 Hz) "pink noise" proto
col requires the hyperacusis patient to listen topink noise se t at a volume just below the individual's discomfort level for two hours per day. The
two hours need not be consecutive. (A pink noiseCD is available from the Oregon Hearing
Research Center.) Vernon informs patients that
the process of sound desensitization is a long
one, that improved loudness tolerance might not
be seen for many months. Jastreboffs tinnitusretraining therapy (TRT) necessitates a patient's
willingness to wear two hearing aid-like noisegenerators, set initially at a "barely audible" broad
band level, for 8-10 hours per day for up to 24
months. Patient counseling is part of the TRTprotocol.
Dan Malcore, who used a sound desensitization protocol himself with success, knows very
well why many patients with severe hyperacusisare reluctant to tr y the program, or - havingtried it - stay with it. He comments: "For peoplewith hyperacusis, 'sound desensitization' is a hard
sell. They can't imagine putting more sound even quiet sound - into their ears at all le t alone
for 8-10 hours a day. It's a marathon-long therapy.There's so much time to get discouraged." On the
other hand, the improvement is significant formany of those who persevere with the program."The principles of TRT helped stabilize my ears.I'm back in the mainstream of my life," saysMalcore. Jastreboff notes that for his patients
with both hyperacusis and tinnitus, the symptom
of hyperacusis improves more quickly - usuallywithin six months.
The Future for Sound -Sensitive Patients
Malcore recalls hi s own unhappy "self-talk"that immediately followed the onset of his severehyperacusis: I am in a corner. I can't work. I missmy family. I miss my life. His perspective is now
16 Tinnitus 1bday/September 1998
one of optimism. "Compared to 20 years ago,there is so much hope for people with hyperacsis. Back then, things were bleak, but no moreMost of us don't have the ability to come back100%. But we all have the ability to come back
Sound desensitization protocols have chanover their few years in use, apparently for thebetter: the percentage of improved patients isclimbing. Experience still cautions us that no
single treatment can offer relief to all soundsensitive patients. However, for the tens of
thousands who were previously considered no
treatable, sound desensitization success is the
new hope and a growing reality. B
ReferencesGoldstein, Barbara. and Abraham Shulman: Tinnitushyperacusis and the loudness discomfort level test - apreliminary report. International Tinnitus Journal 2: pp. 83·1996.
Hall, James A.: Hyperacusis ..it's real and it can hurr. HearJournal, vol. 51: no. 4, Apri11998.
Hazell , Jonathan: Hypersensitivity of Hearing, Internet
posting, ww w.ucl .ac.uk/ "'rmijg101 /h ypl.htm, Nov. 30, 199
Jastreboff, Pawel, and Jonathan Hazell: A neurophysiologiapproach to tinnitus: clinical implications. British Journal oAudiology, 27 : pp. 7-17, 1993.
Marriage, J., and N. Barnes: Is central hyperacusis a sympof 5-Hydroxytryptamine (5-HT) dysfunc tion? Journal ofLaryngology and Otology,vol. 109: pp. 915 -921, 1995.
Reich, Gloria, and Susan Griest: A survey of hyperacusispatients. Proceedings of he Fourth lntemational TinnitusSeminar, Aran and Dauman, (eds.), pp. 249-253, 1992.
Rosenberg, Elliot: The eye as a model for understanding thdisability of hyperacusis. Hyperacusi$ Network newsletter,June 1995.
Vernon, Jack: Recruitment - when noise spells pain. TheVoice, June/July: 12-13, 1991
Vernon, Jack: Tteatment for hyperacusis. Hyperacusis NerwNewsletter, March 1998.
ResourcesPawel J. Jastreboff, Ph.D., Sc.D., University of MarylandTinnitus and Hyperacusis Center, 419 W. Redwood St. #360Baltimore, MD 21201-1734, 410/706-4339
Da n Malcore, The Hyperacusis Network, 444 Edgewood DrGreen Bay, WI 54302, 414/468-4667, [email protected]
Stephen M. Nagler, M.D., F.A.C.S., Southeastern
Comprehensive Tinnitus Center, 980 Johnson Ferry Rd. NE#760, Atlanta, GA 30342, 404/531-3979, [email protected]
Oregon Hearing Research Center, 3181 SW Sam Jackson PaRd., NRC04, Portland, OR 97201-3098, 503/494-8032,http:/ ww w.ohsu.edu.ohrc /
Jack A. Vernon, Ph.D., Oregon Health Sciences University,Oregon Hearing Research Center, 503/494-2187 (availablephone on Wednesdays, 9:30 a.m.-noon and 1:30 p.m.-4:30p.m.), [email protected]
Thanks to a generous grant from James L. S c h i l lthis article is available as a reprint. Reprints avaable free while supply lasts. Send $1 slh for onereprint, $3 s/h for five reprints to: ATA, P.O. Box
Portland, OR 97207-0005.

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 17/27
Can You Feel What I Hear?
An Audiological Perspectiveby Norma Rivera Mraz, M.A./CC·A
The relationship between the healer and thepatient has a major impact on the healing. We
know this scientifically and intuitively. The
human touch, for example, and expressions ofunderstanding and compassion have been
shown in numerous studies to be effective toolsin the healing process.We need only to think
back on our own lives torecall how a soothingword has eased a pain or
lessened a fear. I t istherefore important that
hearing health professionals communicate
wisely, compassionately,and accurately with
patients from the very
first meeting, whether
Norma RiveraMraz, M.A., CCC-A that communication
occurs by phone or inperson. Because we all form our first impressions in a matter of seconds, we as audiologistsmust be acutely aware o f - and ready to use -our abilities and power to build a healing rela
tionship at the very first meeting.Many people who experience illness or a dis
order like tinnitus automatically feel that no one
- especially their health care providers who donot have or have never had tinnitus themselves- can comprehend the magnitude of their pain
and suffering. If this were the case (which fortunately it is not), many of us in the hearing
health community would not be able to cultivatethe relationships necessary for positive, effectiveresults ·with patients.
When a t innitus patient is on the receivingend of empathy , I often hear them say, 11You can
feel what I hear!" They are amazed to learn that
I do no t have tinnitus and that even so, I genuinely understand the abyss they are in and the
despair and loneliness they are feeling. Whentinnitus patients come to you, know that they
will notice your professionalism and the degreeto which you care - even through all of their
confusion and concerns, even before they begin
to tell their story. They can see it and keenly
sense it.
Expressions of empathy can be easily communicated through body language - relaxed
posture, uncrossed arms, leaning forward to thepatient, and eye contact - steady and wari?,all executed naturally and without mechamcal
effort. Most health professionals are no t prepared
to offer this focused attention to their tinnitus
patients at every encounter, perhaps because of
tight schedules or other factors (like a b a ~ hair
day). But it is crucial that.we do so e a c ~ tuneand every time we come mto contact w1th our
tinnitus patients.
Another vital role the audiologist must play
is as an "active listener." Active listening is
absolutely necessary when working with andcounseling tinnitus patients and their families.I t is not a matter of parroting what your patients
say to you then nodding your head in responseto their comments. I t is instead hearing what
your patient is saying to you, taking those statements in compassionately just as you would dofor a close friend or family member who was in
distress. Active listening is another step in the
healing process, and it creates hope for the
future.
Tinnitus patients appear to have a height
ened sense of awareness of everything aboutthemselves and any change that might occur
within their bodies. Every word uttered by their
audiologists or their doctors takes on heightened
significance as well. For many patients, just
being told, "There's nothing we can do foryour tinnitus" can greatlydistort their sense of reali-ty and tragically their
peace of mind.Consequently, it is imper-
ative that we choose our
words and the overallmessage we wish to convey with precision.Negative comments, such
as "Go home and learn tolive "rith it," can sound
just as loud and intrusiveas any tinnitus signal.And besides, they havealready tried to live 'i\riththeir tinnitus and have found
Tinnitus 1bday/September 1998 17
•/
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 18/27
Advertisment
Need relief from
Tinnitus?• Take control of your ringing and hissing
• Safe, Effective, & Easy to Use• 6 tape hypnosis and subliminal
messaging program combining masking ,sound habituation and relaxation
• Free 62 page Tinnitus Research Guide• 30 day money back guarantee
Robert A. Magedoff, President
"I developed this program to provide relieffor my own tinnitus condition. I t worked
for me and I know it can work for you:'For Further Information Write:
Therapeutic Research Group, Ramco Industries, Inc.20423 State Road 7 • Suite 295 • Boca Raton, Fl33498
Or call toll free
l-877-726-2644 www. tinnitusaway.com
Con You Fee/ What I Hear? (continued)
unfavorable results, hence their visit to your
clinic. Patients often feel like they are failures or
weak in character because they can't just "forgetit." I t is even more problematic when health
care providers fail to advise patients on how toaccomplish this daunting task.
What DO they need to hear from us i f we donot have the answer? How about, "There areoptions available elsewhere that can better
address your tinnitus issues. Unfortunatelythese options are not available at this clinic
today." Suggest other clinics, the ATA, theInternet. Tinnitus patients can easily accesstrue (and false) information, especially via the
Internet. But even true information can be
misinterpreted or misrepresented and can lead
individuals with tinnitus down a lonely and dismal road unnecessarily. Inform them that there
are viable treatments that work. Be a wealth of
good information. I t is not the audiologists' and
doctors' responsibili ty for tinnitus patients to ge t
better; but it is the audiologists' and doctors'responsibility to be a source of guidance forthese patients.
18 Ti nnitus 1bday/ September 1998
This paper is based on my professionalriences as an audiologist and the personal vsystem I bring to each of my patients. I am
gratified by the comments from my patient"You really do understand me and my tinniissues." "I thought no one could comprehenwhat was happening with me, especially i f
didn't experience tinnitus themselves." "Yospeak as if you've lived in my home." "Youdescribed me in great detail." "You are an oin the desert."
I have seen tinnitus patients begin to fereassured, educated, enlightened, and inviged because of the time and patience I've githem. Personally or professionally, it is onemy greatest achievements . IBl
Norma Rivera Mraz, M.A., CCC-A, is AssociaDirector of the Southeastern Comprehensive
Tinnitus Clinic, 980 Johnson Ferry Rd., N.E .,
Atlanta, GA 30342, 4041531-3979,norma@tinn. com, www. inn. com

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 19/27
A Self-Help Journey
by Carrol Jude
What does it take to start a Tinnitus Self-HelpGroup? Not as much as you might think. For me,i t was mainly the desire to help another human
being who might be walking in the shoes I'mweating.
December 10, 1995, 9:28a.m. I was going into arestaurant across from Wichita State University. I t
was cold that Sunday morning, but there was no
moisture on the ground or in the air. I went toreach for the door and the next thing I heard wasmy head cracking on the tile of the entrance.
Someone had mopped in front of the door and
with the temperature at 19 degrees, a thin sheet
of ice had formed on the tile. That was the
moment I became acquainted with tinnitus -severe tinnitus in both ears.
The story from here has been experienced bymany of you. I went to five doctors here in
Wichita an d was told "learn to hv e with it" by allof them. No testing was done because, they said,there was nothing that could be done about thetinnitus. Now, three years later, I have maskers in
both ears, an d I have rejoined society. For this Ithank God, the American Tinnitus Association,and Sam Hopmeier of the Hopmeier Hearing
Centers in St. Louis, Missouri.
I first contacted ATA in 1996 about starting aself-help group an d was sent a packet of helpful
information. I read through it, but my ears werestill screaming at me an d I was just not ready. In
1997, I got my maskers, then recontacted BarbaraThbachnick and she sent another packet. Still, Ihad no idea how to pull this off. I knew there
were other people in my community who had
tinnitus but I could not name anyone. I calledBarbara again and she said ATA would help me
get started by sending out information to approximately 300 other "tinnitus people" in my area.
Next I needed to find a place to have our
meetings. I had been working for Inter-FaithMinistries as a manager of the Emergency Over
flow Shel ter for the Homeless. I t was a temporaryjob for the winter. One day while I was in the
general office of Inter-Faith, I asked the
Executive Director, Sam Muyskens what I wouldhave to do to have an office for a tinnitus support
group in that building. Sam asked, "What is your
budget?" Budget, what budget? I knew I ha d tokeep looking.
In April, when taking my two-year-old granddaughter to the park, I passed by the Deaf an d
Hard of Hearing Center coincidentally across the
street from Inter-Faith Ministries. I went into the
hearing center and asked the secretary i f hey ha d
a space I could use for a tinnitus self-help group.The answer was yes, an d at no cost.
My next step was to call Barbara and give herthe location, date (May 7th) an d time. ATA and
Barbara did their jobs well. They made and
mailed the flyers an d sent me materials to hand
ou t to people who would attend the meetings. In
the meantime, I talked with other people in the
community who worked with hearing-impairedpeople.
May 7, 1998, 6:00p.m. I went to the Deaf and
Hard of Hearing Center an hour ahead of time to
get ready. When I arrived I was told there had
Carrol Jude
been a scheduling mix-upan d we would be sharing
the space with a group of
hearing-challengedchildren. Oh no! There
was only one thing to doan d that was to take my
group across the street to
Inter-Faith Ministries. Iwent over to IFM and
talked to Sam and KathyFreed, the Administrators,an d told them of my
predicament. Kathy said,"You're a staff member (I
had stayed on as a receptionist) so, yes, you can
use the building." I thought we might use thesmall staff room so I se t it up hoping I might have
ten people. I walked across the street an d there
waiting for me were 24 people who had been contacted by ATA. I was overwhelmed!! I asked them
to walk across the street with me to Inter-FaithMinistries just for that night. The staff room wastoo smal l so I marched them an down the hall tothe conference room and there we held ou r firsttinnitus self-help meeting.
From that evening on, my life changed againdue to my tinnitus. The most wonderful peopleare sharing in my life journey as I am sharing in
theirs. People had no hope coming into the firstmeeting for we had all gone to the same doctors.Everyone left with something that could help
them live a little better an d no one felt alone. It
was agreed that we would meet on the firstThursday of every month. Everyone wanted to
continue to meet at Inter-Faith Ministries, so thatwas that. I had the key.
In the days to follow I talked with Barbara,made plans for the next meeting and sent flyersout to everyone. Barbara saw to it that I was
Tinnitus 1bday/ September 1998 19
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 20/27
ASelf-Help Journey (continued)
named a contact person for ATA. People started
calling from other states. At this point the funding for flyers and materials was coming out of mypocket. I talked with a lo t of people on the phone
and sent literature to them.
At our next meeting, only five of us showedup . Oops! You know, we had a great meeting anyway - r ea l quality. And I realized what happened. I had not followed through. So, I got onthe phone and called everyone - even after the
fact! Most of them had just forgotten and the timehad slipped by. They said they would be at the
next meeting.
I called the local paper and asked if theywould be interested in doing a story on our tinnitus self-help group. The answer was yes. KarenSchideler came out from the Wichita Eagle with aphotographer. I was quite nervous about this but Igot through the interview easily because the photographer has tinnitus. Karen said they wouldprint the article close to our next meeting date.The Eagle came out with the article a week
before our meeting. In one week I had 68 phone
calls and the caUs have not let up. I also averageseveral visits a week from people who just walkinto the office.
For the next meeting, I sent out flyers, followed by post cards a week before and made
phone calls to everyone the day and eveningbefore the meeting. We had 30 attend.
July 9, 1998, 12:10 p.m. The newly-formedWichita Tinnitus Association became a member
of Inter-Faith Ministries, voted on by their Board
of Directors. We are now a non-profit 501 (c)(3organization with all the privileges (like photocopying and mailing services) of the Inter-FaMinistries. Now we are ready to move forward
If you think you want to start a group, sea
your soul. Then contact ATA and they will dothey can to help. Find yoursel f a place to meeand get on with it. 'Trust the process. Get the
word out any way you can. You will find a lothelp you didn't expect. Don't ge t discouragedthe group is small. Great things happen in smgroups! Make it interesting and make it fun. Iinvited a hypnotist to our last meeting and webecame the most relaxed people in Wichita. Fthe next meeting, Elmer Jennings, long-timesupport contact, will take over. This is not a owoman show. Delegate, delegate, and delegatsome more. I asked for donations last time an
the group was very glad to give.Silence is a problem for tinnitus victims, b
people's silence about their tinnitus is an evebigger problem. Thlk about your tinnitus becathe person you're talking to just might have titus too.
My personal motto in life is "Empower aner to move an inch." That's your job if you wa
to start a tinnitus self-help group. And when wempower others, we empower ourselves. Ia
Carrol Jude is an ATA support group leader and
founder of the new Wichita Tinnitus AssociatioShe can be contacted at 1030 N. Market #204,Wichita, KS 67214-2936, 316/ 264-8853.
New ATA Support Givers WELCOMThe volunteers listed here and hundreds of
others worldwide offer their time and talents as
telephone contacts and/or tinnitus support groupleaders. We couldn't do without them.
What would happen if you volunteered too?For starters, we would add your name, address,and telephone number to the Support ContactsList that we send to all ne w ATA members, then
marvel at our growing network. You would experience an increase in your knowledge base abouttinnitus. (People with the disorder are excellentteachers about it.) And you would receive gratitude from new acquaintances and, in some cases,
new friends - something you'd just have to l
to deal with!
If you are you interested, able, and ready
help, call 800/634-8978 or write to us for a freSupport Givers Packet. You can also access the
packet on our web site (www.ata.org) and appon-line. Click on "Tinnitus Self-Help/Support.
A huge thanks to our support networkpeople - veterans and current additions alike
When one is helping another, both are stro
- German proverb
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 21/27
Collectible Commemorates Quest for Silence
and Benefits ATA Cause
by Corky Stewart, Program Development Manager
Not thinking about the December holiday season yet? Well, we're not trying to rush you, but wedo want you to know about Silent Night 1998, avery special and highly collectible ornament that
is available - in limited quantity - right now.Designed to createawareness of the tinnitus
sufferer's quest forsilence, this exquisiteEuropean glass ornament was hand craftedin Poland and is the firstin a series of three limit
ed editions created entirely for the benefit ofATA
by Joy to The World Collectibles,." Inc.William Shatner, ATA Honorary Director, no t
only endorses the ornament, he participated in the
design. When told that the ATA staff wanted to useSilent Night as the theme, he immediately suggested an angel covering its ears and this year's pieceof art evolved. The 1999 and 2000 editions will be
variations on the concept, thereby increasing valueof the series to collectors.
Priced at $54 plus shipping and handling, each
boxed ornament includes an attractive card from
William Shatner. They can be ordered toll free by
calling 877-0RNAMENT 877 676-2636)and
are alsoavailable at Christmas shops, gift and collectiblesoutlets, catalogs, and other fine retailers nationwide. Th find a location near you, check the website: www.joyworldcollectibles.com
New Support Group Leaders
A very few of the ATA ornaments are "ultracollectible" because they have been autographedby Mr. Shatner to be used to raise further funds
for the fight agains t tinnitus . One of tbese "ultras"is offered through an on-line auction (www.joyworldcollectibles .com) . Another wilJ be the objectof spirited bidding at the November 21, J998 StarTrek Convention in Los Angeles ATA will alsoauction a signed ornament online; watch our website (www.ata.org) for details on that and other
special events .
Not a Web Surfer? Never mind- we've savedone of the autographed "ultras" for a mail-in,sealed-bid auction. The rules are simple: entries
must be postmarked no later than September 30,1998· all bids will remain sealed until the close of
I
the auction; highest offer above the minimumwins (earliest postmark will determine the winner
in case of duplicate bids); minimum bid is $1,000.Mail your name, address, daytime telephone number, and ATA ID number along with your taxdeductible bid (just the figure, not the money) toATA Ornament Auction, PO Box 5, Portland, OR97207-0005. The envelopes will be opened onOctober 5, and all participants will be immediately notified of the winning bid.
Remember that the number of ornaments
available is limited and that ATA will receive a
donation from every sale. Solve that search for aspecial gift or add to your own heirloom collection and help fund further tinnitus education andresearch by purchasing Silent Night 1998 today . B
New Telephone Contacts
Becky BlankenshipTouma Ear & Balance Center
1616 13th Ave. #100Huntington, WV 25701-1692304/522-8800
Susan V. Rezen, Ph.DWorcester State CollegeSpeech Language
Steven Mann23 Pequot Dr.Norwalk, CT 06855203/866-9405
Marl Quigley1161 Packers Cir.Thstin, CA 92780714/505-6861
Hearing Clinic486 Chandler St.Worcester, MA 01602508/929-8551
Linda Z. Gilk
1845 Palisades Dr.Carlsbad, CA 92008760/434-6688
Barry Whitesell
4410 Brookhaven Dr.Greensboro, NC 27406336/674-1885
H arry Larson
3015 18th St. SouthSt. Cloud1 MN 56301320/253-2160
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 22/27
Questions and Answers
by Jack A Vernon, Ph.D., Professor Emertus,
Oregon Health Sciences University
Before going to the questions, I would like tothank the tinnitus patients who have written to
us. I have said it many times in the past and willundoubtedly say i t many times in the future:everything we know about tinnitus has been
taught to us by tinnitus patients. Thus I am most
grateful to you all.
QMrs. H. from South Dakota informs us
that as a result of an air bag explosionshe has high-pitched tinnitus and high
frequency hearing loss. She has suffered loss of
concentration, loss of sleep, and loss of socialenjoyment. She asks if tinnitus produced by an
air bag explosion can be relieved with masking?
Andoubtedly you were exposed to a lot of
noise from the air bag, but you were alsoexposed to a violent pressure change. So
it's hard to know what is responsible for the tinnitus. We've found that tinnitus induced by noiseexposure is more readily relieved by masking
than is tinnitus induced by head trauma or medications. But it is never possible to predict in
advance i f masking will be successful. The only
way to find out is to actually try it and thatmeans to be fitted by a professional who is competent in fitting tinnitus maskers. You might getan idea of whether or not masking will work for
you by doing the "faucet test" (stand near afaucet of running water and listen for a reduc-tion in your tinnitus) . Since your tinnitus is bilateral i t is likely that masking devices will be
required in both ears.
Q
Mr. P from Kentucky indicate s that upon
ascent and descent in airplanes he is
temporarily deaf for a few moments .Would continuing to fly cause permanent hearing loss?
Aassume that what you experience is a
failure of the eustachian tubes to functionproperly and if that is so then it will no t
produce any permanent hearing loss . If it is amatter of pressure changes during take-off and
landing you can correct the problem by wearing
tightly fitted earplugs (foam plugs do nicely) forboth of these events.
QMs . W. from Ohio indicates that descin commercial flight produces pain in
ears. She asks if this result is due
to he r tinnitus? She also asks if the noise of a
turboprop plane could be a problem?
Ahe pain in the ears upon descent in
aircraft is most likely due to pressurechanges. During the majority of flight
aircraft are pressurized at a level of 6000 feetThus on descent if the pressure equalizationnot correctly controlled, one could experiencsome major pressure changes and that in tur
could cause pain in the ears. But no, it has n
ing to do with your tinnitus. See the answer
Mr. P from Kentucky for a corrective measur
As to the noise of the turboprop, earplugs mprovide sufficient protection but you may alswant to try active noise cancellation. Earplugprovide passive attenuation which is greater
high-pitched sounds than low-pitched soundsBut the active noise cancellation devices promore complete noise cancellation of low frequency sounds like those heard on planes. Flittle less than $200 you can obtain a ProActi3000 noise cancellation device. I t is sold by NCancellation Technologies, Inc., One Dock StSuite 300, Stamford, CT 06902, 203/961-0500.Write or call Ms. Donna McLevy, the salesmanager. The unit is sold with a two-week
money-back guarantee .
QMr. B. from New Hampshire has read
article abou t DMSO and tinnitus in thWorld Wide Encyclopedia ofNatural
Healing. The art icle claims that nine of 15patients treated with DMSO experienced tinnre lief. Mr. B. asks if he should try this treatm
Aou might have trouble obtaining DMS
That article was published in 1974 and
since then, the FDA has regulated tha
DMSO is only available to veterinary physicifor use with animals. (Somehow, though, sompatients are still able to acquire DMSO.) DMS
has the property of penetrating the skin with
imparting any damage to the skin and thus ioriginal use was to carry pain suppressors intaffected joints of arthritic patients. The 1974study cited could be faulted in that there was
mention of the tinnitus severity of the patien

7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 23/27
selected for treatment and that unfortunately
there was no placebo-control group. Mr. B., I
would recommend that you try other treatments
and will gladly discuss this with you i f you are
interested. (Formore on DMSO,
see also"Alternative Therapies - Another Look" in the
December 1994 Tinnitus 'Ibday.)
QMr. L. from Minnesota writes that he
has experienced depression an d has had
tinnitus in his deaf left ear for many
years. He is currently taking St. John's Wortwhich to date has not helped his depression or
his tinnitus.
Ahave seen several patients who were
told that they were deaf in one or the
other ear. But all that means is that the
hearing is so impaired that the ear cannot profitfrom a hearing aid. Being able to hear and under-
stand speech from a hearing aid is vastly different from being able to successfully mask that
ear. J would encourage you to do the "faucet test"with the left ear pointing toward and near to the
sink. If the water sound has any suppression
effect at all on your tinnitus it is likely that awearable tinnitus instrument can provide some
relief for you. You indicate that until you became
a member ofATA you had not considered an ypossible connection between your t innitus and
your depression. Yet such a connection is very
common an d it might be possible to relieve your
depression if we can relieve your tinnitus. I t isclearly worth a try.
Also, if your depression is severe, it is not
likely that St. John's Wort will relieve it. On theother hand, if your depression is mild to moderate, then you could try the herb. (Give it at least
four weeks.)
Qnd A. Mrs. H. in Michigan writes to say
that the use of Evening Primrose Oil
(EPO) has completely relieved her pul
satile tinnitus . (Unfortunately she did not specifYthe dosage.) In 1982, Mrs. H. consulted an oto
laryngologist who informed her that her mild
hearing loss would progress to deafness in five
years if she did not have an operation he recom
mended. (He ignored the tinnitus problem.)
Mrs. H. did not have the operation and 16 years
later she hears as well as ever. In the ensuing
years her pulsatile tinnitus has returned several
times but each time it does, treatment with EPOhas always relieved it. Have any of you readers
with pulsatile tinnitus tried Evening PrimroseOil? I f so, please le t us know the results. I rec
ommendthat
patients with unrelievedpulsatiletinnitus contact Aristides Sismanis, M.D., in
Richmond, VA 804/786-3965). Not only is he
knowledgeable about this condition but he is avery compassionate and caring individual.
QMs. F. of North Carolina asks i f it is possible to cancel tinnitus with active noise
canceling devices.
As. F., these devices cancel external
sounds such as the drone of an aircraft or
other low-pitched environmental noises.
They achieve this cancellation by a set of microphones in the earphones that listen to the exter
nal sounds. The external noise is then fed intoan electronic circuit that analyzes the sound
wave and reverses it producing a completely
opposite sound which is played back against theincoming sound. This produces a cancellation of
both sounds. Technically, the cancellation is aphase reversal. Currently these devices are only
effective for sounds below 1500Hz. (The BoseCo. indicates that they are working on noise
cancellation technology that will cancel soundsup to 10,000 Hz.)
Now, can active noise canceling devicescancel tinnitus? The simple answer is no they
cannot, and for this reason: there is no actualsound in tinnitus (tinnitus is merely a soundlike perception - like the phantom limb phenomenon) and thus there is nothing physical tobe detected or played back against itself to effectcancellation.
Qr. B. in Illinois indicates that they have
two small fans running all night in theirchildrens' bedroom, because the fan
noise masks outside noises thus preventing disturbances of sleep. Mr. B. asks i f the fan noise
going all night long will ultimately damage his
children's hearing.
Acompliment you, Mr. B., for being sensi
tive to the hearing health of your chil
dren. I hope that same concern carries
over to that future time when they will be
tempted to attend amplified rock concerts.
Unless your fans are louder than any with
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 24/27
Guidelines for Writers
Tinnitus Tbday, the Journal of the
American Tinnitus Association welcomes submission of original articles about tinnitus and
related subjects. The articles selected for publi
cation are those that speak to an audienceof people with tinnitus, and to audiologists,otolaryngologists, otologists, hearing aid specialists, and other medical, legal, and governmental specialists with an interest in tinnitus.
Submit typewritten, double-spaced manuscripts on plain 81/zxll" paper with one-inch
margins all around. Include title; author(s)name(s) and biographical information; and,when appropriate, footnotes, references,legends for tables, figures, and other illustrations and photo captions. Our readers like to
"see" you. Please include a reproducible photo.Articles not exceeding 1500 words are preferred. If possible, submit manuscripts on 3.5"disk in WordPerfect 5.1 or higher format (PCcompatible).
Please do not submit previously publishedarticles unless permission has been obtained in
writing for their use in Tinnitus Tbday. ( P l e a sattach a copy of the written release to the artcle submitted.)
Include and sign the following release: "I
consideration of Tinnitus Tbday taking actionreviewing and editing my (our) submission,the author(s) undersigned hereby transfer(s)or otherwise convey(s) all copyright ownershto Tinnitus 7bday in the event that such work
published by Tinnitus Tbday."
Tinnitus 7bday also welcomes news items
interest to those with tinnitus and to tinnitus
health care providers, and information or
review copies of new publications in the fieldInclude your name, street and e-mail addresses, telephone and fax numbers, and those of
any others the editors might want to contactfor further information.
Please address all submissions or inquirieto: Editor, Tinnitus Tbday, P. 0. Box 5, PortlanOR 97207-0005.
Thank you for your consideration.
Questions and Answers (continued)
which I am familiar I seriously doubt that they
could cause any hearing impairment. However,
let's not guess. I recommend that you purchase
a sound level meter and measure the actualsound intensity of the fan noise. Radio Shacksells a small sound meter for about $35 which isamazingly accurate. With such a sound levelmeter, measure the intensity of the sound at thechildrens' ea r level. If the sound level is 85 dB
or more, that would be reason to purchase quieter fans. Otherwise, all is well.
Q Dr. S. from Hawaii writes to explain his
use of masking. He points out that sometimes the masking sound can become an
irritant even when it is preferred over the tinnitus sound. When this happens, he adds in theenvironmental sounds from the Marpac TSC 350
sound generator in order to effect "masking the
masker." Why, he asks, doesn't Starkey produce
the same sounds in their wearable maskers?
24 Tinnitus Thday/ September 1998
An some cases, a very high-pitched
tinnitus requires a very high-pitched(and unacceptable) sound to mask it.
Your invention of "masking the masker" is agreat idea and clearly another way to enhanc
the masking effect for patients with high
pitched tinnitus. Keep in mind that the masksignal does not always have to be at the sam
high frequency as the tinnitus signal to bringrelief. Only with proper testing can this be
determined.
Notice: Many ofyou have left messages requestithat I phone you. I simply cannot afford to meethose requests. Please feel free to call me on any
Wednesday, 9:30a.m. - noon and 1:30- 4:30p.m. 503/494-2187). Or mail your questions to:
Dr. Vernonc/o Tinnitus TodayAmerican Tinnitus AssociationPO Box 5
Portland, OR 97207-0005
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 25/27
SPECIAL DONORS AND TRIBUTES
ATA's Champions of Silence are a remarkablegroup of donors who have demonstrated their
commitment in the fight against tinnitus by
making a contribution or research donation of
$500 or more. Sponsors and Professional
Sponsors have contributed at the $100-$499 level.Research Donors have made research-restrictedcontributions in any amount up to $499.
acknowledged with an appropriate card to thehonoree or family of the honoree. The giftamount is never disclosed.
Our heartfelt thanks to all of these specialdonors!
All contributions to the American TinnitusAssociation are tax-deductible.
ATA's 'Tribute Fund is designated 100% forresearch. 1tibute contributions are promptly
GIFTS FROM 4-16 -98 to 7-15-98.~ · ~ Champions of Silence So l Charen Roben B. Horn Bruce K. Powell Ju dith K. Horning, M.A.
(Contributions of$500 Michael D. Childs Andrew Hrivnak, lf l Marceline Powell CCC·A
and above) Jean Cinader Gilben Hudson Otis D. Rackley, Jr., D.D.S. Martin H. Kulick, D.M.D.
Julia R. Amaral C. Dennis Clardy William H. Hurt Daniel D. Retchin David T. Malicke, D.O.
Peter D. Bonanno Bob Cobe H. June Ivins Jeffrey A. Ristlne Frank M. Melvin, M.D.
Robert Alvin Bowler Emory w. Cook Ray Jahn Jeffery A. Rbc Ernest E. Mhoon, Jr., M.D.
Joseph Decker Jack S. Cooley Thm Johnston Robert W. Roper Frank A. Skinner
John J. Delucca Capt. Thomas C. Crane, George C. Ju ilfs Lynn Rosemurgy Martin Smith
Joseph J. Demty USN, Ret. Harold S. Karpe Jennie E. K. Rosenblum Steven Strong. M.D.
Joel Garris, M.D. Robert H. Crittenden Emma L. Kellahcr Jo n M. Rundle Bradley S. Thedinger, M.D.Irene M. Glancey Roy W. Cronacher Stephen J. Kennedy Barbara L. Sanders Joseph B. Touma, M.D.
Seymour Greenstein Esther Cronson Dennis S. Kohara Esther Schoenfeld Ralph R. 1Yner, M.D.
Edmund J. Grossberg, CLU Sean Culkin Marvin Kowit Bruce Schommer J. Dan Weathers, M.D.
Norman Hascoe Eddie Cusheenberry Ronald T. Krasnitz William T. Schreitmueller Edwin F. Weaver, D.D.S.
W. F. Samuel Hopmeier, Martin L. Davidson E. Joseph Kubat Cindy SchtenCorporationswith
BC-HIS Marvin N, Demchick Susan R. Lallak Evelyn J . Schwenl
Gary P. Jacobson, Ph.D. Mary Ann Desutter Henry G. Largey Richard S. Shapiro Matching GiftsJohn Malcom Richard S. Dirkes Donald J. Larivee Robert J. Shapiro Boston Foundation/Polaroid
Bruce Martin Kathryn M. Dobrinski Fred R. Lawson John v. Shepherd, Sr. Fund
Steve Martin Charles Dolnick Rose Lee F'orrest Shook CitiCorp Foundation
Ray Matheny Robert E. Doran Jacques Leviant Michael Shorts Eastern Enterprises
Philip 0. Morton Jerry Down Gary w. Lightner Dawn T. Smith F'oundation
RJR Nabisco Irene Duffield Virginia A. Lobsinger Douglas H. Steves Equitable Foundation
Louise Parmley Joseph H. Eagan Philip J. Longo Lloyd Stockel Fannie Mae Foundation
Kenneth A. Preston Mary D. Eggers Catherine M. Lynd Barbara F. Sturtevant Hoechst Celanese
Dan Purjes A T. Evans Don Macaborski Richard W. Sullivan Foundation
N. Schaefer Jo y A. Fogarty Constantine J. Malfese Robert L. Szabo Johnson & Johnson
Martin F. Schmidt Francine and Ray Foster Peter A. Marrinan June M. Thblak J.P. Morgan Charitable Trust
James W. Soudriette Char Fowler Andy Matthiesen Harrison Thomas Millipore Foundation
Elsebeth S. Stryker Carol Fredrick Wayne E. Maxon William J. Tillman NGM Charitable F'oundation
Donald v. Thompson Arlene Friedman Mr. and Mrs. M. Richard James C. Thtten Pfizer
Jack A. Vernon, Ph.D. Robert F. Fuller May Elizabeth VanPatten Reader's Digest F'oundation
Patricia A. Zapp Robin R. Fuller Krist in E. McAbier Gary Yoyten US West Fou ndation
SponsorsRandall Gardner Romulus E. McCoy, Jr. Linda A. Wainhouse BequestsGerald Otis Gates Carol McCurdy Bernard J . Weber
(Individual Contributions Larry L. Gentry Angus McLeod Sheldon WeinigEstate of Irene M. Glancey
from S/00-$499) Dorothy E. Gilman Paul J. Meade David P. Wl1istler, Ph.D.TRIBUTESev. Alvin A. Andrus Bob Goodman Juerg Meng Henry J. Williams
Calvin Artke Gordon R. Goody Robert J. Mermuys David Winn In Memory OfElizabeth Bailey Marlene Greenebaum John M. Meyer James G. Winn Ken Berman's fatherJoseph M. Baria Elizabeth Grisbaum Bruce F. Meyers Robert E. Wolons Claire and Jacques SimonT. Larry Barnes Philip J. Gutentag Mildred Miller Brax Wright Lattie May BlytheEric Bartl1ell Paul R. Haas R. G. Miller Carter Wu rts Elaine E. BlantonNed K. and Jane L. John E. Hall Malt Minninger Paul W. Zerbst Sandy Delucca
Bartheltnas Larry E. Hall Perry Mitchell Richard D. Zujko, M.D. William ApostolidesDavid M. Banlert Thomas P. Hall Edward A. Moos Professional Sponsors Nancy CuccurulloSusan Bently Stephen C. Harris Robert E. Naser Deloitte & Touche, LLPSam Berkman Dorothea E. Haskins Sara Beall Neal
(Professional C o n t r i b u t i o n . ~ John J. Delucca
Deborah an d Charles Bern Charles B. Hauser Rober t Odiefrom $100-$499)
Steven F. GoldstoneRobert B. Berry Dennis D. Heindl Lawrence Ohmer
Natan Bauman, Ed.D.Norman Hascoe
William D. Bethell Heindl Family Foundation Julian M. OlfMarcus Boehm
Kenneth J. LapiejkoMary B. Bolen Harold J. Henderson Curtis S. Olson Constance Brown Hearing
John w. MacMurrayRichard A. Bolt William F. Hendren Phyllis R. Ongert
CenterCarol J. Makovich
Richard Bouthiette Elizabeth B. Hill Mark O'vyangMark Brumback, ACA
RJR NabiscoArt Bragg PatTicia Hines Allan F. Pacela, Sc.D., P.E. Linda A. Burba, M.S.,
Joseph PalumboCharles T. Brown Loren G. Hinkleman Harry J. Papajohn CCC·A
Thomas J. Pierce, Jr.William A. Burgin Lorraine Hizami v.tilJiam R. Patterson Lois N. Cohen, CSW, ACSW,
Ed G. RobertieUoTimothy P. Caire James R. Hoffman Phil R. Pearcy BCD
Huntley an d Lynne WitacreM. Cappelletti Construction, Thd Hofmeister Dow V Perry Norman Frankel, Ph.D.
Jason H. WrightInc. David G. Holmes Ron Perry W. F. Sa muel Hopmeier,
Arthur H irshberg's sisterBarbara Young Camp Julian Hoogstra Ja y L. Pomrenze BC·HIS
Claire and Jacques SimonPamela D. Chandler Max Horn Rob ert L. Pope
T in nitus Thday/September 1998 25
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 26/27
SPECIAL DONORS AND TRIBUTES (continu
Danny Isakson
Arlo and Phyllis NashRobert JanusMr. an d Mrs. John H.
Schleter
Lee J . Rowe
Thelma P. Batchelder
Hilda Sanford
Arlo an d Phyllis Nash
Martin L. an d Grita N.Schmidt
Martin F. Schmitd/Kate
Schmidt Moninger Fund
Phyllis Sharp
Mr. an d Mrs. John H.
Schleter
Max Spickel
Lena Clapham
Alfredo ThtiSouth Jersey Tinnitus
Support Group
In Honor OfErnest Auer
(Happy Father's Day)
Patrice Auer
Marion carver(35th anniversary of
E A R Services)
Dorothy Muto-Coleman.
M.A.Ralph Dawson
(90th birthday of myfather-in-law)
Donald E. Nace
Sherman Devitt
(For being a thought·
fu l cousin)
Charles M. SelsbergDavid an d Pearl
Greenberg
(50th Wedding
Anniversary)
Judith Pilz
Alfred an d Doris SchwartzJack Harary
(Happy Father's Day)
Mike. Cindy, & Adrian
Harary
Dr. Jack A. Vernon
Jack Salerno
Barry Whitesell
(Our son)
Mr. an d Mrs. E.D.Whitesell, Jr.
Research DonorsJames AdamsJoel Alexander
Earl W. Alvord, Jr.Dennis B. Anderson
Sally A. Anderson
Georgina Arbing
Frank Amal
Mary ArnoldCalvin Artke
Adelle H. Ausburn
Mary AustinLorraine L. Bachmann
Claire U. Bagley
Christine B. BakerDoloris w. Baker
Eileen F. BarretteTheodore w. Sayler
Peter B. Baylinson
Ida J. Beebe
Susan BentlyHoward G. Bernett
Jeanne B. Betcher
Lorraine E. Bieber
Jerome V. Biodolillo
Jackie w. BishopJean A. BlackSusan Black
Mildred S. Bom.,.itLouis G. BougieSt Antoinette BoykinEleanor P. BoyleMildred L. Bramley
Carol J . Branscomb
Elaine F. BrodeyCorrine Bmoks
Harry A. Bruhn
Ernest J. BucklesLewis BullardPatricia L. Buntele
Michael W. Burnham
Joan K. Bynaglc
Kelyne Campbeli-
'TbvmsendThrry R. Canter
Faye Cartmell
Mark A. CashEllis CaudillEdwin R. Chapman
Howard C. Chase
David and Debra Chatfield
Mildred Cherry
Susan P. Chizeck
Charles F. Clark
Mary L. CollinsElizabeth A. Conyers
Marilyn G. Cooperman
Eileen T. Corcoran
Esther Cronson
Richard J. D'AmbrosioCarl D'AquinoTheodore A. Dahlstrom, J t
William Michael Daniels
Fabio Romeiro
DealbuquerqueBarbara S. Derick
Rubye M. Dewitt
Rosa an d William Dixon
Ed Dobrinski
Cynthia A. DodsT. James Donnelly
Shirley DorazioAnne M. Dranginis, Ph.D.Marlene Drescher
Dr. George M. Drew
Virginia M. Dublanc
Charles B. EfirdMiriam EidlitzAda Eisenberg
Wayne Engel
Lawrence R. England, Jr.Laura R. Enright
Charlotte EricksonRon an d Joyce Evans
John 0 . Felt
Kathleen A. FerelloVirginia K. Fish
Leonard M. Fisher
Johnston K. FiteDonald FlachHarry Floersheim
Susan E. FoilesDolores S. FoleyRichard Fowler
Thllervo Frankel
26 Tinnitus 'Ibday/September 1998
Rhea FriedViola L. FuchsJames H. Fulcher
Nancy E. GalezaStephen P. Gazzera
Dr. Arthur Gelb
Mark S. Geller
Jennifer Gerhard
James GiordanoHowell R. Gnau
Barry S. GoldbergLinda B. Goodwin
Donna M. Graves
Jeannette E. Green
Dr. Judith L. Green
Judy A. GriffinRalph Gugeler
John Haleston
Norma M. Hammerberg
Michael P. Hanson
Penny Harmening
Don Heinz
Jeff Hellman
Ida G. Hibbard
E. Alan Hildstrom
John L. Hilgers
Roland F. HirschThd Hofmeister
Kay Hoiby-GriepW.F. Samuel Hopmeier, BC-
HlS
Mary Kay Horner
Chet Hosac
Robert K. Hoy
Jack Huang
RDsa Huang
E. C. Huckabee
Rachel Hudock
Gilbert Hudson
Donald E. Huebl
Janet v. Hughes
Nathan V. lyer
Ann Jackson
Perry Jamieson
Roger JohnstonBarry Jordan
George Joseph
R. L. Kcheley
Donald J. KellenbergerJoseph Kel lnerFrank L. Kellogg, Jr.
Robert A. Kirkman
Waldemar Kissel, Jr.
Roberta KitzmillerFrank V. KoenigSteve M. Konneman
Egon Kot, BC-HIS, FNAOJeffrey Kot, M.A.Gloria J. Koz1oskyVirginia C. Kuehner
Joseph A. Kuhn
Gary J. Kutzler
Erna LadageJerry J. LaForgia
Susan R. LallakNeil Lambert
Judith LarsonJeannette Lawrence
Arthur LaxerMarjorie Lazarus
Marilyn LeggFrederick S. Leimer
Stanley D. LevinCharles B. Levitin
Harry Levitt, Ph.D.
David LongAgnes Longtin
lnna Lorents
Fay J. LouieErnest A. LucciNick Luis
Anthony C. Lunn
Robert G. Lyon
Don Macaborski
Dan R. Malcore
Grace P. Maresca
Carol A. Markey
Gregory P. Markowiec
Lillian P. Markowitz
Julianne Mattimore
Robert L. Mauer
Wayne E. Maxon
Helen l. May
Edward MazzaJohnathon R. McCartney
Harold Mechanic
Ruth L. Meier
Carol A. MeiseNick Mendoza
Annette Meskin
Gary Mitchell
Craig G. MoffatPatricia A. MooreVirginia C. MorettiJulie Morin
Mr. an d Mrs. James G.
Mulhern
Betty Murray
Emogene Myers
Mae Nachman
Ian L. Natkin
Shoshana Noily'furry 0. NorrisDonald G. O'Brien, Sr.
William D. Odbert
Sally M. Oldham
Robert OroszLeonard J. PacificoKathleen Pacini
Jeffrey PaukerReginald J. Pearce
Ronald G. Pearson
'Ibm Pechtel
Milton Pentzer
Sara J. Peters
Linda M. Peterson
Shirley PeytonJudith Phillips
Susan G. PhillipsDorothy D. PiersonMarjorie M. Piscopo
Elaine T. PlattMichael M. Platt
Robert D. PoetaPam Pratt
Norma Price
Raymond w. Pritzke
Muriel S. QuintalMichael ReindlDonald L. Reinking
Charles R. Renegar
Gerald B. Rcnyer
Vernon T. RichardsSteve Richardson
l.ollv Rieken
Kydeen RiddleLoretta M. RoseMatthew P. RossGemma M. Rozich
Ron Ruda
Ruby L. RutherfordMike RutlandJuanita A. RyanMaria K. Sadlowska
Grace Sanders
Rae L. Savett
Edward Saydeh
Edna Schachter
Carol A. ScheiderDawn Schoenholz, Ph.Gus Schwandt
William Schwartz
Arlan R. Schwoyer
Thacy J. Sciandra
Cary Setzer
Norma T. Sheld
Wendy Shenker
Brooksie SilvaKatherine L. Simmons
Raymond C. Simon
Thomas J. SimsThelma M. SjostromLinda M. Slater
Jerry M. Smalley
Regina P. Smith
Walter A. Snell
.John SouroumanisDavid D. SouzaLaura J. Spear
Elizabeth H. Spencer
Harvey Spivack
Ed and Annetta St. ClaJames L. Stewart
Janet M. Stramaglia
Ernest E. Strickland
Richard W. SullivanGwendolyn D. Theriot
David Thomas
Greg Thompson, M.D.Joyce A. Thompson
Beth Ann Thompson
Gregory Thrner
Jan Vanroessel
Melvin J. Veldhuizen
Michael VucelichCarol WalkerJi m Walker
Walter W. Walker
John M. WardellWilliam K. Warren, Jr.William Warren
Foundation
Manha E. WayteWilliam J. and Sally J.
WebbDeanne L. Weir
Charles A. WellsJeane K. Wheeler
Frank Whitelam
Lawrence S. WickBarry WilliamsLev D. Willis, Jr.
Wendi WilsonGloria W. Wingfield
Sh irley L. Wireman
Dorothy A. WiseWilliam A. Yost. Ph.D.Mary Zakarian
Doris D. ZerbyFrederick B. ZOokFlorence Zuchowski
7/23/2019 Tinnitus Today September 1998 Vol 23, No 3
http://slidepdf.com/reader/full/tinnitus-today-september-1998-vol-23-no-3 27/27
"Silent Night 1998"ce- European Glass Ornament to benefit ATA &>
Endorsed by William Shatner, ATA Honorary Director
Limited Edition(See page 20 inside)
AMERICAN TINNITUS ASSOCIATION
P.O. Box 5, Portland, OR 97207-0005Forward and Address Correction
Non-Profit Org.
U.S. Postage
PAID
American TinnitAssociation