Embed Size (px)
Citation preview

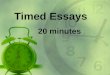
Carbohydrate…. rapid digestion, total absorption/conversion to glucose (100%)
Protein…………..…………slow digestion, partial conversion to glucose* (~40%)
Fat…………………………….slow digestion, little conversion to glucose** (<20%)
Meal 1 Hr 2 Hrs 3 Hrs 4 Hrs 5 Hrs 6 Hrs 7 Hrs 8 Hrs
CHO
Pro
Fat
BG
Timed Effect on Blood Sugar Levels
1

Types of Carbohydrate
The three main types of carbohydrate are: Starch (also known as complex carbohydrates)
Sugar
Fiber
Foods that contain carbohydrate are: Grains and starchy vegetables
Beans and legumes
Fruit
Dairy products like milk and yogurt
Sweets and snack foods like chips
2

Carbohydrate and diabetes
• Although low carbohydrate diets might seem to be a logical approach to loweringpostprandial glucose, the ADA specifically states that "low-carbohydrate diets (restrictingtotal carbohydrate to < 130 g/day) are not recommended in the management of diabetes"(ADA, 2006).
• The glycemic effect of carbohydrate foods cannot be predicted based on their structure(i.e., starch versus sugar) owing to the efficiency of the human digestive tract in reducingstarch polymers to glucose. Starches are rapidly metabolized into 100% glucose duringdigestion, in contrast to sucrose, which is metabolized into
. Fructose has a lower glycemic index (GI).
• The basic guidelines for the amount of carbohydrate to eat at meals and snacks, e.g., 3 to4 carbohydrate choices/meal (60 g/meal ± 15 g) and 1-2 carbohydrate choices (15-30 g)at snacks.
3

Glycemic Index and Glycemic load
The glycemic index (GI) measures the relative area under the postprandial glucose curve of 50 g of digestible carbohydrates compared with 50 g of a standard food, either glucose or white bread.
Low GI ( less than 55 )
Moderate GI ( 55 to 70 )
High GI (more than 70 )
Estimated glycemic load (GL) of foods , meals , and dietary patterns iscalculated by multiplying the GI by the amount of carbohydrates in each foodand then totaling the values for all foods in a meal or dietary pattern.
Low GL ( 10 or less )
Moderate GL ( 11 to 19 )
High GL (more than 20 )
4

GL GLGI
Krau
se’s
fo
od
an
d n
utr
itio
n t
her
apy,
20
12
GI
5

No ideal distribution of macronutrients (carbohydrate, protein, fat) for a diabetes nutrition prescription has been identified.
A healthy eating pattern is recommended.
6

Nutrition Recommendations
Total Daily Energy Intake
Carbohydrate : 45-65%
• (The recommended dietary allowance (RDA) for digestible carbohydrate is 130 g/day )
• Fiber : total 25-30 g/d (15-25 g/1000 kcal)
Protein : 15-20% or 12-16%
Fat : Total fat 25-35%
• Polyunsaturated fatty acids up to 10%
• Monounsaturated fatty acids up to 20%
• Saturated fats < 7% (Saturated and trans fatty acids< 10% )
• Cholesterol (mg/d) <200 mg/d7

• CHO = 55-65%
• Pro = 12-16%
• Fat < 30%
• CHO = 45-65%
• Pro = 20-35%
• Fat = 10-35%
Modern nutrition in health & disease Krauses food & nutrition therapy
• CHO = 50-60%
• Pro = 10-20%
• 25% < Fat < 35%
IOM
8

Certain high risk groups may benefit from an appropriate vitamin-mineral supplement
♣ Growing and developing children and youths
♣ Women during pregnancy and lactation
♣ Individuals eating < 1200 kcal / day
♣ Elderly individuals (especially people with low SES)
♣ Patients in ICU or long term nursing facilities
♣ Total vegetarians
♣ Patients with poor glycemic control
9

مرور فهرست جانشینیکالری چربی پروتئین کربوهیدرات گروه غذائی
80 1-0 3 15 نشاسته
60 - - 15 میوه
100120
160
3-05
8
88
8
1212
12
شیر
بدون چربی•کم چربی•کامل•
متغیر متغیر متغیر 15 سایر کربوهیدراتها
25 - 2 5 سبزیجات
5575
100
35
8
77
7
--
-
گوشت و جانشین های آن
(لخم)کم چرب•متوسطچربی•پر چرب•
45 5 - - گروه چربی


12
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,
Supplement 1, January 2015

13
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,Supplement 1, January 2015

14
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,Supplement 1, January 2015

15
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,Supplement 1, January 2015

16
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,Supplement 1, January 2015

17
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,Supplement 1, January 2015

18
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,Supplement 1, January 2015

19
Nutrition Therapy Recommendations
Topic Recommendations Evidence Rating
Diabetes Care Volume 38,Supplement 1, January 2015





موارد احتیاط عوارض بالینیکاربرد اثرات درمانی مکانیسم عمل نام دارو دسته دارویی

موارد احتیاط عوارض بالینیکاربرد اثرات درمانی مکانیسم عمل نام دارو دسته دارویی

Dr. Amiri, Nutritionist 26

27

Re
lati
ve In
sulin
Eff
ect
Time (Hours)
0 2 4 6 8 10 12 14 16
Long (Glargine)
18 20
Intermediate (NPH)
Short (Regular)
Rapid (Lispro, Aspart , Glulysine)
Insulin Time Action Curves
Dr. Amiri, Nutritionist 28

Injection sites
• It is usually recommended to be injected on these areas:
Abdomen
Outer top of the thighs
Outer arms
Buttocks

Dr. Amiri, Nutritionist 30

Dr. Amiri, Nutritionist 31

Dr. Amiri, Nutritionist 32

Dr. Amiri, Nutritionist 33

Diabetes Care Volume 38, Supplement 1, January 2015

توضیحات (mg/dl)قند قبل از ورزش
تا زمان رسیدن قند خون به مقادیر هدف ! ممنوع.نباید ورزش کرد 80کمتر از
نکات ذکر شده در مورد مصرف کربوهیدرات و کاهش انسولین مصرفی
250–80
بود نباید )+( اگر . باید کتون ادرار اندازه گیری شودبودن می توان ورزش کرد ( -)در صورت . ورزش کرد
.ولی نیازی به مصرف کربو هیدرات اضافی نیست 300–250
!ممنوع ورزش 300از بیشتر
خون قبل از ورزشقند

Effect of physical activity
Insulin Signaling Pathways That Regulate Glucose Metabolism in Muscle Cells and Adipocytes. Implications for Insulin Resistance and Diabetes Mellitus –nejm 1999.

Insulin dose reduction guidelines
for planned postprandial exercise

• Bolus insulin:
• ↓ Pre-exercise bolus insulin by 10-80% according to duration and intensity, when activity follows a meal
• Following prolonged exercise, subsequent meal boluses may need to be ↓‘d by 25-50%
• Basal insulin:
• Injected morning basal insulin may need to be ↓‘d by 10-50% for planned or continuing activity in the afternoon
• Injected bedtime basal insulin may need to be ↓‘d by 10-30% following prolonged endurance exercise
• Pump basal rates should be decreased by an appropriate amount prior to the start of activity (30 - 60 min.) and may need to be continued for several hours after
Exercise: General Recommendations
38

Important notes:
♣ The first priority for persons requiring insulin therapy is to integrate an insulin
regimen into the patient's lifestyle.
♣ After an initial food/meal plan is determined (with the patient's input), it should be
reviewed with the health professional who is planning the insulin regimen.
♣ With the many insulin options now available, an insulin regimen can usually be
developed that will conform to the patient's preferred meal times and food choices.
Flexible insulin regimens using basal (background) insulin and bolus (mealtime)
insulin or insulin pumps give the patient freedom in timing and composition of
meals and are the preferred mode of therapy to maximize blood glucose control and
minimize complications.
Dr. Amiri, Nutritionist 39

♣ The total amount of carbohydrate in the meal (and snacks, if desired) is
the major determinant of the bolus rapid-acting insulin dose and post-
prandial glucose response.
♣ After determining the amount of insulin required to cover the patient's
usual meal carbohydrate, patients can be taught how to adjust bolus
insulin doses based on the amount of carbohydrate they are planning to
eat (insulin-to-carbohydrate ratio).
♣ For persons receiving fixed insulin regimens and not adjusting mealtime
insulin doses, consistency of day-to-day carbohydrate amounts at meals
is important.
Important notes:
Dr. Amiri, Nutritionist 40

♣ All persons with type 1 diabetes and many persons with type 2 diabetes who
no longer produce adequate endogenous insulin need replacement of insulin
that mimics normal insulin action.
♣ After eating, plasma glucose and insulin concentrations increase rapidly,
peak in 30 to 60 minutes and return to basal concentrations within 2 to 3
hours in non-diabetics.
♣ To mimic this, rapid-acting insulin, such as lispro, aspart, or glulisine, is
given at mealtime; doses are adjusted based on the amount of carbohydrate in
the meal.
♣ Basal or background insulin, such as determir, glargine, or NPH, is required
in the post-absorptive state to restrain endogenous glucose output primarily
from the liver and to limit lipolysis and excess flux of free fatty acids to the
liver.
Important notes:
Dr. Amiri, Nutritionist 41

The type and timing of insulin regimens should be individualized
based on eating and exercise habits and blood glucose
concentrations.
Important notes:
Dr. Amiri, Nutritionist 42
In persons with type 1 or type 2 diabetes who adjust their mealtime
insulin or who are on insulin pump therapy, insulin doses should
be adjusted to match carbohydrate intake (insulin-to-carbohydrate
ratios).

Dr. Amiri, Nutritionist 43
What is Insulin to carbohydrate ratio (ICR)?

سبت و تعیین بهترین نفرم ثبت غذاهااستفاده از : روش اول
ممکن برای هر وعدۀ غذا
تعداد واحد انسولین برای= هر واحد کربوهیدرات
تعداد واحد انسولین رگوالر در هر وعده
تعداد واحد کربوهیدرات در آن وعده
محاسبه نسبت انسولین به کربوهیدراتروشهای
Dr. Amiri, Nutritionist 44

مقدار انسولین رگوالر روزانه استفاده از : روش دوم
تعداد واحد انسولین برای هر واحد= کربوهیدرات
کل واحدهای روزانه انسولین رگوالر
متوسط واحد کربوهیدرات مصرفی در طول روز
محاسبه نسبت انسولین به کربوهیدراتروشهای
Dr. Amiri, Nutritionist 45

30قانون استفاده از : روش سوم 30کل مقدار انسولین روزانه تقسیم بر
محاسبه نسبت انسولین به کربوهیدراتروشهای
Dr. Amiri, Nutritionist 46

Insulin Sensitivity Factor (ISF)
1800
Dr. Amiri, Nutritionist 47