Embed Size (px)
Citation preview

Arch Orthop Trauma Surg (1991) 110 : 216-219
A hi e °f Ort paedic a.dTrauma urgery © Springer-Verlag 1991
Tibia vaiga after fracture: Documentation of mechanism
D. Keret 1, H. T. Harcke 2, and J. R. Bowen 1
1 Department of Orthopaedics and 2 Department of Medical Imaging, Alfred I. duPont Institute, Wilmington, Delaware, USA
Summary. Tibia valga following fracture in the proximal metaphysis of the tibia in children was previously attri- buted to various mechanisms. This case report offers an additional explanation based on bone scintigraphy 10 months after injury. Decreased radionuclide uptake at the lateral proximal tibial physis without evidence of in- creased uptake on the medial side suggests that a Salter type V injury to the lateral growth plate can occur in conjunction with a medial metaphyseal fracture, result- ing in the development of tibia valga.
Tibia valga is known to occur as a consequence of a non- displaced fracture in the proximal metaphysis of the tibia in children. A number of theories have been proposed to explain the development of this deformity following a tibial fracture that does not directly involve epiphyseal plate. Although malreduction of the original fracture was often blamed for the deformity [3, 17-19], other mechanisms were invoked when tibia valga occurred in instances that clearly did not support this hypothesis. One suggestion was asymmetrical stimulation of the medial part of the tibia due to release of mechanical periosteal restraint [4, 6, 19]. Other authors believed that fracture callus caused an opening of the fracture gap, which led to the development of angulation because of the inhibition of interstitial growth [12, 13]. Early weight bearing [16] and discrepancy in growth between the tibia and fibula, with tethering of lateral tibial growth by the fibula [6, 21], also have been suggested.
Only a few reports have documented obvious mor- phological abnormalities [8, 22, 24, 251. Weber [22] showed an infolding and interposition of the pes an- serinus and a portion of the tibial periosteum in the medial opening of the fracture. Overgrowth of the medial part of the proximal tibia secondary to hyperemia introduced in the growth plate injury was proposed as a
Offprint requests to: David Keret, M.D., Editorial Services, Alfred I. duPont Institute, P. O. Box 269, Wilmington, DE 19899, USA
mechanism [9, 14]. In a recent case report from our in- stitution [24], this phenomenon was documented by using quantitative bone scintigraphy to demonstrate the pro- portionally greater uptake in the medial portion of the proximal tibial physis 5 months after fracture, when angular deformity was developing. Additional support for this phenomenon was given in 2 other reports [8, 25] that document asymmetrical growth recovery lines in the proximal tibia, suggesting overgrowth of the medial por- tion of the tibia compared with the lateral portion fol- lowing injury.
We have found only one report [7] that speculates that asymmetrical physeal growth can be due to retarda- tion of growth in the lateral portion of the proximal tibial physis. We present a case that supports this speculation using physiological evidence obtained from bone scintig- raphy. Our findings suggest that a Salter type V injury to the lateral portion of the growth plate can occur in con- junction with a medial metaphyseal fracture, resulting in the development of tibia valga.
Case report
A 2-year, 4-month-old girl sustained a mildly displaced transverse fracture in the left proximal tibial metaphysis and a greenstick frac- ture at the junction of the mid and proximal thirds of the fibula. She was treated for these closed fractures without reduction in a long-leg cast with the knee flexed 20 ° (Fig. 1). Radiographs taken 4 weeks later demonstrated healing, with periosteal new bone for- mation on the outer aspect of the tibial metaphysis. The tibial alignment was in a neutral position, and the casting was continued for a total of 9 weeks. At the time of case removal, healing had progressed, and the fracture gap was almost completely filled in. Tibial alignment showed 16 ° valgus deformity as measured using the metaphyseal-diaphyseal angle (Fig. 2). (The normal range for this patient's age is 0°-11°). The valgus deformity was noted to progress and was accompanied by development of genu recur- vatum. The tibia on the affected side was now 1.0 cm longer than the contralateral normal tibia.
Nine months after fracture, the child was referred for further investigation and possible surgical correction of the valgus defor- mity. Radiographs of the lower extremities in the standing position showed a metaphyseal angle of 27 ° in the injured left tibia and 8 ° in the normal right tibia (Fig. 3). There was a similar difference be-
D. Keret et al.: Tibia valga after fracture: Documentation of a mechanism 217
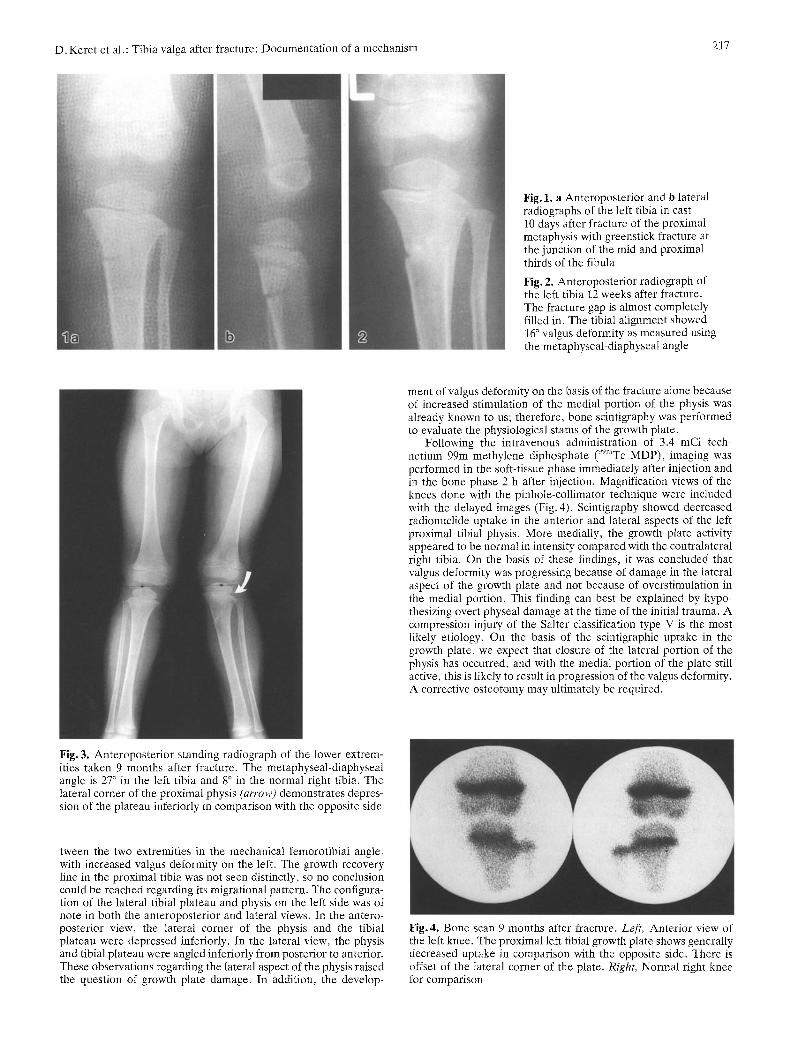
Fig. 1. a Anteroposterior and b lateral radiographs of the left tibia in cast 10 days after fracture of the proximaI metaphysis with greenstick fracture at the junction of the mid and proximal thirds of the fibula
Fig. 2. Anteroposterior radiograph of the left tibia 12 weeks after fracture. The fracture gap is almost completely filled in. The tibial alignment showed 16 ° valgus deformity as measured using the metaphyseal-diaphyseal angle
ment of valgus deformity on the basis of the fracture alone because of increased stimulation of the medial portion of the physis was already known to us; therefore, bone scintigraphy was performed to evaluate the physiological status of the growth plate.
Following the intravenous administration of 3.4 mCi tech- netium 99m methylene diphosphate (99mTc MDP), imaging was performed in the soft-tissue phase immediately after injection and in the bone phase 2 h after injection. Magnification views of the knees done with the pinhole-collimator technique were included with the delayed images (Fig. 4). Scintigraphy showed decreased radionuclide uptake in the anterior and lateral aspects of the left proximal tibial physis. More medially, the growth plate activity appeared to be normal in intensity compared with the contralateral right tibia. On the basis of these findings, it was concluded that valgus deformity was progressing because of damage in the lateral aspect of the growth plate and not because of overstimulation in the medial portion. This finding can best be explained by hypo- thesizing overt physeal damage at the time of the initial trauma. A compression injury of the Salter classification type V is the most likely etiology. On the basis of the scintigraphic uptake in the growth plate, we expect that closure of the lateral portion of the physis has occurred, and with the medial portion of the plate still active, this is likely to result in progression of the valgus deformity. A corrective osteotomy may ultimately be required.
Fig. 3. Anteroposterior standing radiograph of the lower extrem- ities taken 9 months after fracture. The metaphyseal-diaphyseal angle is 27 ° in the left tibia and 8 ° in the normal right tibia. The lateral corner of the proximal physis (arrow) demonstrates depres- sion of the plateau inferiorly in comparison with the opposite side
tween the two extremities in the mechanical femorotibial angle, with increased valgus deformity on the left. The growth recovery line in the proximal tibia was not seen distinctly, so no conclusion could be reached regarding its migrational pattern. The configura- tion of the lateral tibial plateau and physis on the left side was of note in both the anteroposterior and lateral views. In the antero- posterior view, the lateral corner of the physis and the tibial plateau were depressed inferiorly. In the lateral view, the physis and tibial plateau were angled inferiorly from posterior to anterior. These observations regarding the lateral aspect of the physis raised the question of growth plate damage. In addition, the develop-
Fig.4. Bone scan 9 months after fracture. Left, Anterior view of the left knee. The proximal left tibial growth plate shows generally decreased uptake in comparison with the opposite side. There is offset of the lateral corner of the plate. Right, Normal right knee for comparison

218 D. Keret et al.: Tibia valga after fracture: Documentation of a mechanism
Discussion
The progressive valgus deformity of the tibia in this pa- tient is not easily analyzed because in addition to a number of hypotheses that could be invoked, there is the possibility that a combination of mechanisms came into play.
Malreduction or inadequate reduction was suggested as the cause of deformity after the fracture in the proxi- mal tibial metaphysis. Immobilization of the knee in flexion prohibited the calculation of the true valgus deformity at the time of casting. The actual amount of valgus deformity became more obvious in the radio- graphs obtained following removal of the cast, when the knee was extended normally. In this situation, casting without an attempt at reduction could be a contributing factor to the amount of valgus deformity seen initially. This is not a sufficient explanation for the total defor- mity, however; the resulting progressive increase in the amount of valgus angulation requires additional ex- planation. Asymmetrical stimulation of the proximal tibial physis was documented as a valgus-producing mechanism in a previously published case report in which increased medial plate uptake caused more rapid growth in the medial portion of the metaphysis than in the lateral portion [24]. Although this mechanism may have been a factor during the healing process, it was shown to be self-limited. In that previously published case report [24], the deformity ceased when plate activ- ity returned to normal. Scintigraphy in our patient showed decreased activity in the lateral portion of the plate that is consistent with partial closure. This change laterally and anteriorly on the scintigraphic images can account not only for the valgus deformity but also for the genu recurvatum that has developed [1, 20].
The decreased lateral activity, which we postulate is due to primary injury of the physis at the time of initial fracture, answers two of the three criteria defined by Peterson and Burkhart [15], who challenged the exis- tence of type V injury in the Salter-Harris classification. The normal radiograph of the proximal tibial physis ob- tained initially favors the suggestion of an occult injury. Although the immobilization for the 9-week period may be considered, it does not explain the occurrence of a partial arrest. Another conceivable explanation for re- duced lateral physeal activity would be overloading of the physis because of the presence of angular deformity. This was not found to be true in another study [10] of an- gular deformity that showed that the loading of the plate does shift and, in fact, alters the activity by decreasing uptake in the portion of the plate receiving less stress. If this mechanism were true in our study, loading of the plate would increase in the lateral portion and decrease medially, so that one would expect reduced activity in the medial physis, which is the opposite of what we have demonstrated.
The increased length of the affected tibia needs to be discussed in view of the finding that the physeal uptake in that tibia is less than that of the tibia on the normal side. We believe that some overgrowth was likely to have occurred during the initial healing process, but we
think that this was only temporary in nature. It is prob- able that we performed scintigraphy at a time after medial plate activity had returned to its normal level. The filling in of the fracture gap during the remodeling process could also have contributed to some of the difference in length observed between the two tibias.
Asymmetrical tibial growth has been attributed to lat- eral tethering by an intact fibula. Other case reports [2, 25] have shown that valgus knee deformity can develop even when there is a completely displaced fibular frac- ture. A long-standing gap at the fracture site described in this report could have been filled with periosteum [11], superficial medial collateral ligament [5], or pes anserinus. We are unable to refute these points because there was no surgical intervention in this case. We believe that the progressive development after healing requires addi- tional explanation.
Conclusions
The case presented here supports the assumption of re- duced physeal activity in the lateral portion of the proxi- mal tibial growth plate as a mechanism for the develop- ment of valgus deformity following metaphyseal frac- ture. It also suggests that more than one of the many proposed mechanisms for the development of such de- formity may play a role in any particular case. The ob- servations in this case support the concept that Salter type V injury of the tibial physis does occur and may be entertained as a mechanism when progressive valgus deformity of the tibia occurs after a fracture has healed. We think it is extremely important to differentiate this mechanism from others, such as stimulation of the medial portion of the physis, because the deformity will progress in the presence of growth plate arrest, whereas it is apparently self-limited in the other circumstances. We believe that the patient described in this paper is likely to require surgical intervention by closure of the tibial epiphysis by medial epiphysiodesis and/or osteo- tomy at a later age.
References
1. Bahnson DH, Lovell WW (1980) Genu valgum following frac- ture of the proximal tibial metaphysis in children. Orthop Trans 4 : 306-307
2. Balthazar DA, Pappas AM (1984) Acquired valgus deformity of the tibia in children. J Pediatr Orthop 4: 538-541
3. Best TN (1973) Valgns deformity after fracture of the upper tibia in children. J Bone Joint Surg [Br] 55:222 (abstract)
4. Blount WP (1955) Fracture in children. Williams & Wilkins, Baltimore
5. Coates R (1977) Knock-knee deformity following upper tibial "greenstick" fractures. J Bone Joint Surg [Br] 59:516 (abstract)
6. Cozen L (1953) Fracture of the proximal portion of the tibia in children followed by valgus deformity. Surg Gynecol Obstet 97 : 183-188
7. Goff CW (1960) Surgical treatment of unequal extremities. Thomas, Springfield, Ii1
8. Green NE (1983) Tibia valga caused by asymmetrical over- growth following a nondisplaced fracture of the proximal tibial metaphysis. J Pediatr Orthop 3 : 235-237
D. Keret et al.: Tibia valga after fracture: Documentation of a mechanism
9. Griffin PP (1978) The lower limb. In: Lovell WW, Winter RB (eds) Pediatric Orthopedics, vol 2. Lippincott, Philadelphia, pp 884-886
10. Harcke HT, Zapf SE, Mandell GA, Sharkey CA, Cooley LA (1987) Quantitative bone scintigraphy in the evaluation of angular deformity of the lower extremity. Radiology 164: 437- 440
11. Houghton GR, Rooker GgD (1979) The role of the peri- osteum in the growth of long bones: an experimental study in the rabbit. J Bone Joint Surg [Br] 61 : 218-220
12. Jackson DW, Cozen L (1978) Genu valgum as a complication of proximal tibial metaphyseal fracture in children. J Bone Joint Surg [Am] 53 : 1571-1578
13. Lehner A, Dubas J (1954) Sekundfire Deformierungen nach Epiphysenl6sungen und epiphysenliniennahen Frakturen. Helv Chir Acta 21 : 388-410
14. Ogden JA (1982) Tibia and fibula. In: Skeletal injury in the child. Lea Febiger, Philadelphia, pp 587-591
15. Peterson HA, Burkhart SS (1981) Compression injury of the epiphyseal growth plate: fact or fiction? J Pediatr Orthop 1 : 377-384
16. Pollen AG (1973) Fractures and dislocations in children. Chur- chill Livingstone, Edinburgh
17. Rang M (1983) Tibia. In: Children's fractures, 2nd edn. Lip- pincott, Philadelphia, pp 229-300
18. Rooker GD, Salter RB (1980) Prevention of valgus deformity following fracture of the proximal metaphysis of the tibia in children. J Bone Joint Surg [Br] 62 : 527 (abstract)
219
19. Salter RB, Best T (1972) Pathogenesis and prevention of val- gus deformity following fractures of the proximal metaphyseal region of the tibia in children. J Bone Joint Surg [Br] 54 : 767 (abstract)
20. Skak SV (1982) Valgus deformity following proximal tibial metaphyseal fracture in children. Acta Orthop Scand 53 : 141- 147
21. Taylor SL (1963) Tibial overgrowth: a cause of genu valgum. J Bone Joint Surg [Am] 45 : 659 (abstract)
22. Weber BG (1977) Fibrous interposition causing valgus defor- mity after fracture of the upper tibiat metapbysis in children. J Bone Joint Surg [Br] 59 : 290-297
23. Weber BG (1980) Fractures of the proximal tibial metaphysis. In: Weber BG, Brunner C, Freuler F (eds) Treatment of frac- tures in children and adolescents. Springer, Berlin Heidelberg NewYork, pp 325-329
24. Zionts LE, Harcke HT, Brooks KM, MacEwen GD (1987) Post-traumatic tibia valga: a case demonstrating asymmetric activity at the proximal growth plate on technetium bone scan. J Pediatr Orthop 7 : 458-462
25. Zionts LE, MacEwen GD (1986) Spontaneous improvement of post-traumatic tibia valga. J Bone Joint Surg [Am] 68 : 680- 687
Received August 28, 1989






![Case Report of a Tibial Plateau Fracture Extending Through the … · describes tibia plateau fracture patterns and serves to guide operative treatment [5]. This fracture pattern](https://img.pdfslide.us/doc/110x75/5d1e74de88c99335368d6437/case-report-of-a-tibial-plateau-fracture-extending-through-the-describes-tibia.jpg)





















