Embed Size (px)
Citation preview

2/2/2011
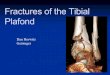
Tibial Plafond/Pilon Fractures

The Spectrum of Fracture

The Spectrum of Soft Tissue Injury

Relative Success
Dismal Failure
vs

The Soft Tissue Injury!!
Red Blisters
Clear Blisters
OpenFracture

Terrible Injuries
“Excellent Results” are rarely achieved
Fair-Good results are the norm
Outcomes are impossible to predict
Treatment complications must be avoided

Bone Soft Tissue

2 yrs.
Unusually good!

Tibial Plafond FracturesFair to Good Results Are the Norm
1991 - anterior B-3 fracture

6 months 3 years
Fair to Good Results Are the Norm

8 years
Fair to Good Results Are the Norm
Ankle score - 80Works as a laborer

5 years - no painankle score 95Case 1

6.5 yrs - miserable -
ankle score 45Case 2

Case 1 Case 2

� Avg. age 35-40
� Rare in children and elderly patients
� Males 3 x more common
� 3-9% of all tibia fractures
� Associated injuries 25-50%
� Increased incidence – Air Bags!!!
Save lives yes, but devastate the foot and ankle
Burgess et al JT 1995Lower extremity injuries in drivers
of air-bag equipped automobiles

Multiply injured patients with and without foot injuries ( 24 and 12 month follow ups)
Dramatic differences in pain, function and health related quality of life

Ankle Soft Tissues
Thin skin
Absent muscle
and adipose tissue
Lack of deep veins
Particularlyvulnerable!

The soft tissues over the anteromedial tibia are vulnerable

Dense trabecular structure of distal tibia

Bone is viscoelastic Axial load is rapid Shift in stress strain curve Tremendous energy release

Displacement
Load
Stress strain curves for rapid vs. slow rate of loading
Rapid axial load
Slow rotational load
Note the greater energy under
the curve!!

Rotational ankle fracturesare different - good prognosis and
few complicationswith standard techniques

Dense trabecular structure Thin soft tissues Axial Loading Typical fracture pattern Severe soft tissue injury

Reudi and Allgower - 1969


Is this a tibial plafond fracture? Does it belong in 43?

Plafond yes!!
C-2?
Or
C-3?

Four principles “stood the test of time”
Anatomical reduction
Stable internal fixation
Atraumatic technique
Early pain-free mobilization
“Precise reconstruction of articular surfaces is the goal, and is always preferred to tolerable malalignment”.

These Principals Illustrated for Fractures of the Tibial Plafond

Ill-Advised
Extensive surgical approaches
Fracture stripping
Prolonged tourniquet times
Bulky implants
Increased soft tissue injury
A recipe for disaster
}

Limb Threatening Complications

McFerran et al JOT 199221pts (40%) with major complications
require 77 additional operations Wyrsch et al JBJS 1996
3/18 amputations in closed fractures
Teeney and Wiss CORR 1993
37% infection and 26% fusion in Type 3’s
Cases Treated1980’sEarly 1990’s

Delays until surgery
Spanning ex fix part of most protocols
Percutaneous and limited approaches

Spanning ex fx Marsh et al JBJS 1995 – 43 cases 0% Wyrsch et al JBJS 1996 – 20 cases 5 %
External fixation same side Court Brown et al JOT 1999 – 24 cases 4% Tornetta et al JOT 1993– 26 cases 7%
Delayed plating Patterson and Cole JOT 2001 – 22 cases 0% Sands et al CORR 1998– 64 cases 6 % Sirkin et al JOT 1999 - 48 cases 6%
0-10%

1. Spanning articulated fixation with percutaneous or limited approaches to the articular surface and screw fixation
2. Percutaneous plating3. Standard plating through open approaches
after long delays for soft tissue recovery

Spanning fixator for three months A large monolateral frame fixed into the
talus and calcaneus Relatively earlier approaches to reduce the
articular surface percutaneously

Suited for all tibial plafond fractures Ideal for very comminuted cases Contraindicated with ipsilateral talus or
calcaneus fractures Beware diaphyseal extension or severe open
fractures which might delay healing

Span the zone of injury
Fixator applied first
Same technique all cases
One step surgery
Largely
percutaneous
AdvantagesArticulated

FIXATOR TECHNIQUE - Same for all cases!
Target the neck of the talus
posterioros calcis

Technical tips
Talar pinparallel to top of talus

Depth of insertion – Hindfoot pins must capture the entire talus and calcaneus
Harris viewCanale view

Position of pinsAssembled fixator
Keep the pins in the same plane!
Technical tips

Center the talus on two views
The articular surface can not be reduced if the talus Is not repositioned

Axial CT scan critical for pre op planning
The more you use limited approachesthe more planning that is required

Limited or percutaneous approachesand use of reduction aids

Reduction forceps based on anterolateral incision –
Watch out for SPN!

Open approaches when necessary based on major anterior fracture line
Direct approaches - no stripping

Percutaneous reduction sequencevisualized flouroscopically



2 year follow up

Never plated
Treat withfixator
Bone graft less
than 10%

ROM
Splinting
Wt. Bearing

~ 3 months after injury Outpatient clinic Calcaneal screw typically
loose Often use SLC for another
month

Uses medial sub cutaneous border Needs pre contoured plate Locking may offer advantages Ideal for a select group of fractures
Non articular distal tibia Limited articular involvement Build back articular block through limited
approaches

Distal tibia without articularDistal tibia without articularinvolvementinvolvement

External fixator Femoral distractor Manual traction Well placed clamps
Reduction: Ligamentotaxis

Femoral distractor
=

If Injured, Repair the Fibula

Pre-size and bend plate
Or use precountoured plate

• Rotation
• Curve
Anatomy:
Medial face

Incision

SubQ Tunnel

Insert plate

Confirm placement

Stab……Drill, Tap, & Screw

Post-op

4 months




Another example in a Another example in a more complex fracturemore complex fracture


5 months

Indicated to treat the range of tibial plafond fractures
Temporary spanning fixation and long delay to definitive surgery
Several different open approaches

1st Stage: Temporary Fixation application of spanning external fixator, ORIF of the fibula, as soon after presentation as possible, stabilize the fracture while allowing the
soft tissue swelling to resolve,
Interim: ice, elevation, pre-operative plan, TIME to allow swelling to resolve,
2nd Stage: Definitive Fixation ORIF tibia, removal of external fixator,

“Traveling Traction”Half Pins
TransfixationPin

Ice, elevation, CT scan, crutch training,
Pre-operative plan, TIME to allow
swelling to resolve,

Fibula posterolateral approach
when an anteromedial approach to the tibia is planned,
maximize the width of the skin bridge,

Fibula Implants:
Metaphyseal fracture 1/3 tubular plate, large screw,

Fibula Implants:
Metaphyseal fracture 1/3 tubular plate, large screw,

Fibula Implants:
diaphyseal fracture 3.5 LC – DCPlate
Rationale: cortical bone, highest energy fractures, slower healing,

Extensile Anteromedial Approach: “Workhorse”,
Anterolateral Approach: gaining in popularity,
Posterolateral Approach: recently proposed,

Anteromedial Approach Superficially:
minimum 7 cm skin bridge, begin ½ finger breath lateral to crest
over the anterior compartment, continue parallel to Anterior Tibialis
tendon, towards the talonavicular joint,
Post-operative soft tissue complications

Anteromedial Approach Superficially:
begin ½ finger breath lateral to crest over the anterior compartment,
continue parallel to Anterior Tibialis tendon,
towards the talonavicular joint, maintaining a 7 cm skin bridge,
Medial
talonavicular joint
medial

Anteromedial Approach Deep dissection:
carried out medial to Anterior Tibialis tendon,
longitudinal arthrotomy, gentle elevation of tendons and
neurovascular bundle,medial


Anteromedial Approach Deep dissection:
remain medial to Anterior Tibialis tendon,
longitudinal arthrotomy, gentle elevation of tendons and
neurovascular bundle,medial

Articular Reduction: largest and least displaced articular fragments
first, reduced fragments held with:
K-wires (1.2 or 1.6mm), pointed reduction forceps, lag screws,
reduce articular bloc to shaft, definitive fixation,

DON’T make medial a incision !!! the incision ends up directly over
the plate, difficult to close, increased wound complications,
deep infection, soft tissue loss, free flap only bailout,
burn bridges later reconstruction,
Not This Incision !!

Make This Incision !!

Anterolateral Approach Indications:
open medial wound, displaced Chaput fragment, lateral articular comminution,
Advantage: plate coverage, uninjured skin,
Caution Superficial peroneal nerve

Anterolateral Approach Deep Dissection:
through superior and inferior retinaculae, interval between toe extensors and fibula, elevate muscles off interosseous
membrane, Caution
Superficial peroneal nerve

Anterolateral Approach Deep Dissection:
through superior and inferior retinaculae,
interval between toe extensors and fibula,
elevate muscles off interosseous membrane,
Caution Superficial peroneal nerve

Advantages a single incision for ORIF
of the tibia and fibula, FHL is positioned
between the skin and the implants in case of post-op wound complication,
Disadvantages limited access to anterior
articular fracture fragments, prone position, sural nerve at risk,
Posterolateral Approach

Implants: Small Fragment Plates
cloverleaf shaped plate, distal radius “T” plates, 1/3 tubular plates, 3.5 LC-DCP,
Screws 3.5 cortical/4.0
cancellous, cannulated: 4.0/4.5

Implants: Small Fragment Plates
cloverleaf shaped plate, distal radius “T” plates, 1/3 tubular plates, 3.5 LC-DCP,
Screws 3.5 cortical/4.0
cancellous, cannulated: 4.0/4.5

Bone Graft support articular
fragments, augment healing, fill cancellous defects,
ICBG, Allograft, Synthetic
Calcium putties,

Meticulous Wound Closure meticulous closure, 1-0 vicryl for capsule, 2-0 vicryl for
subcutaneous tissue, 3-0 nylon for skin,
Allgower’s modification of the Donati stitch,
Allgöwer stitch modified by DonatiAllgöwer stitch modified by Donati

Summary: Tibial Plafond Fractures Represent both a bony and soft tissue injury, AO Principles:
Anatomic articular reduction, stable fixation, early mobilization of patient and limb.
several approaches to the tibia can be safely used, internal fixation is accomplished with small fragment
implants, meticulous soft tissue closure,

Results

Most have some pain
Most return to work
Detectable arthrosis - 50%
Arthrodesis rare

Pain Analysis
� 50% - no/minimal pain
� 35% - pain with weight bearing
� 15% - continuousMarsh et al. JBJS 1995

Sands et al CORR 1998 - 2-4 years after injury Delayed plating
Pollak et al JBJS 2003 – average 3.2 years after injury Plating and external fixation
Marsh et al JBJS Feb 2003 – 5-11 years after injury Spanning external fixation

0
20
40
60
80
100
PF* PR* BP* GH VT SF RE MH
Plafond
Norm
SF-36: Plafond vs Aged Matched Norms
5-11 years after injury (Marsh et al JBJS Feb 03)
Significantlydifferent

Ankle Osteoarthritis Scale: Plafond 5-11 Years after Injury
0
0.2
0.4
0.6
0.8
1
1.2
Pain Disability Mean
Plafond
Norm

0
2
46
8
10
12
1416
18
20
Grade 0 Grade 1 Grade 2 Grade 3
# of patients

25/33 rated their ankle good or excellent
Motion avg. 75% opposite
Only 2/37 late arthrodesis 5.4%

Sequential Ankle Score: 67 at 24 mo, 86 at 92 mo (p<.004)
Time to maximal healing: 2.4 yr (9 mo-5 yr)
Reasonable evidencethat patients improvefor a long time!
Do not be too quick to offerreconstruction!

1986 - 24 yo Male

1 year

7 years

14 years
Works light labor
Prefers high top boots
Occasional pain
Ankle score 80

Most have some ankle painCan not run or play sportsMeasurable effect on general health status70% with moderate or severe arthrosis
Excellent results are only rarely achieved

Most rate their outcome as good or excellent
Arthrodesis rate only ~ 5% Most feel they improve for years
Fair to Good Results Are the Norm

Summary and Conclusions

High energy fractures with severe associated soft tissue injury
Unpredictable outcomes Keep complications – 10% or less Results:
Generally not great But if you stay out of trouble not awful

Long lasting effect on patient health related quality of life and a greater effect on ankle pain and function
Arthrosis common by 2 years after injury and typical in the second five years. The clinical significance is variable.
The variation in outcome is unpredictable
The severity of injury/quality of reduction are important but better techniques to understand this critical interaction are needed

Do not be quick to suggest arthrodesis based on severity of injury or quality of reduction
Patients improve for a long time and most do not require arthrodesis
Complications must be avoided since they produce bad outcomes and the extent that we improve outcome with aggressive surgery is at least unclear