Embed Size (px)
Citation preview

1
Diagnosing Interstitial Lung Disease Is No Longer “Business as Usual”: A Contemporary Diagnostic Approach to Fibrosing Interstitial Pneumonias
Brandon T. Larsen, MD, PhDSenior Associate ConsultantDepartment of Laboratory Medicine and PathologyMayo Clinic Arizona
Leeds Pathology 2019July 4, 2019
©2013 MFMER | slide-2
Case• 52-year-old woman with hypothyroidism, joint pain, and
ILD since 2009
• “Light” history of smoking (2 pack-years as teenager)
• School teacher, with no birds or mold exposure
• HRCT: “Indeterminate for UIP”
• ANA: 1:320
2
3
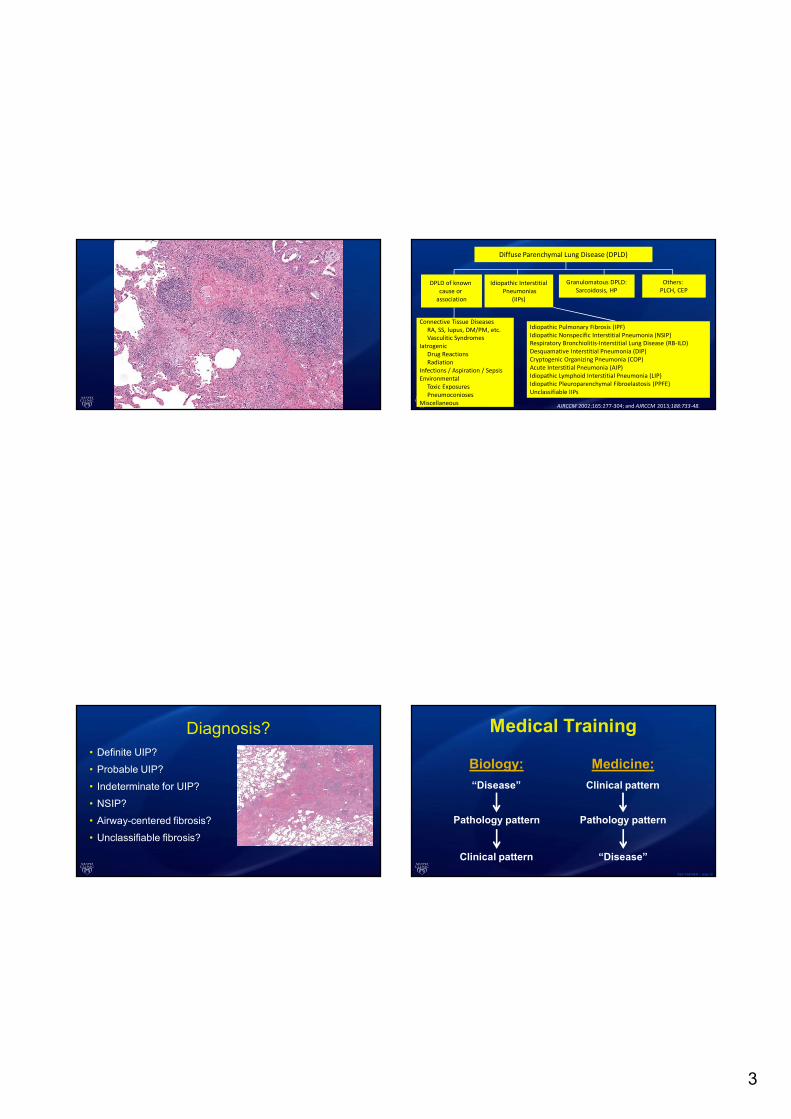
Diagnosis?• Definite UIP?
• Probable UIP?
• Indeterminate for UIP?
• NSIP?
• Airway-centered fibrosis?
• Unclassifiable fibrosis?
Diffuse Parenchymal Lung Disease (DPLD)
Idiopathic InterstitialPneumonias
(IIPs)
Granulomatous DPLD:Sarcoidosis, HP
Others: PLCH, CEP
DPLD of known cause or
association
Connective Tissue DiseasesRA, SS, lupus, DM/PM, etc.Vasculitic Syndromes
IatrogenicDrug ReactionsRadiation
Infections / Aspiration / SepsisEnvironmental
Toxic ExposuresPneumoconioses
Miscellaneous AJRCCM 2002;165:277-304; and AJRCCM 2013;188:733-48.
Idiopathic Pulmonary Fibrosis (IPF)Idiopathic Nonspecific Interstitial Pneumonia (NSIP)Respiratory Bronchiolitis-Interstitial Lung Disease (RB-ILD)Desquamative Interstitial Pneumonia (DIP)Cryptogenic Organizing Pneumonia (COP)Acute Interstitial Pneumonia (AIP)Idiopathic Lymphoid Interstitial Pneumonia (LIP)Idiopathic Pleuroparenchymal Fibroelastosis (PPFE)Unclassifiable IIPs
©2013 MFMER | slide-12
Medical Training
“Disease”
Pathology pattern
Clinical pattern
Biology:
“Disease”
Pathology pattern
Clinical pattern
Medicine:
4
©2013 MFMER | slide-13
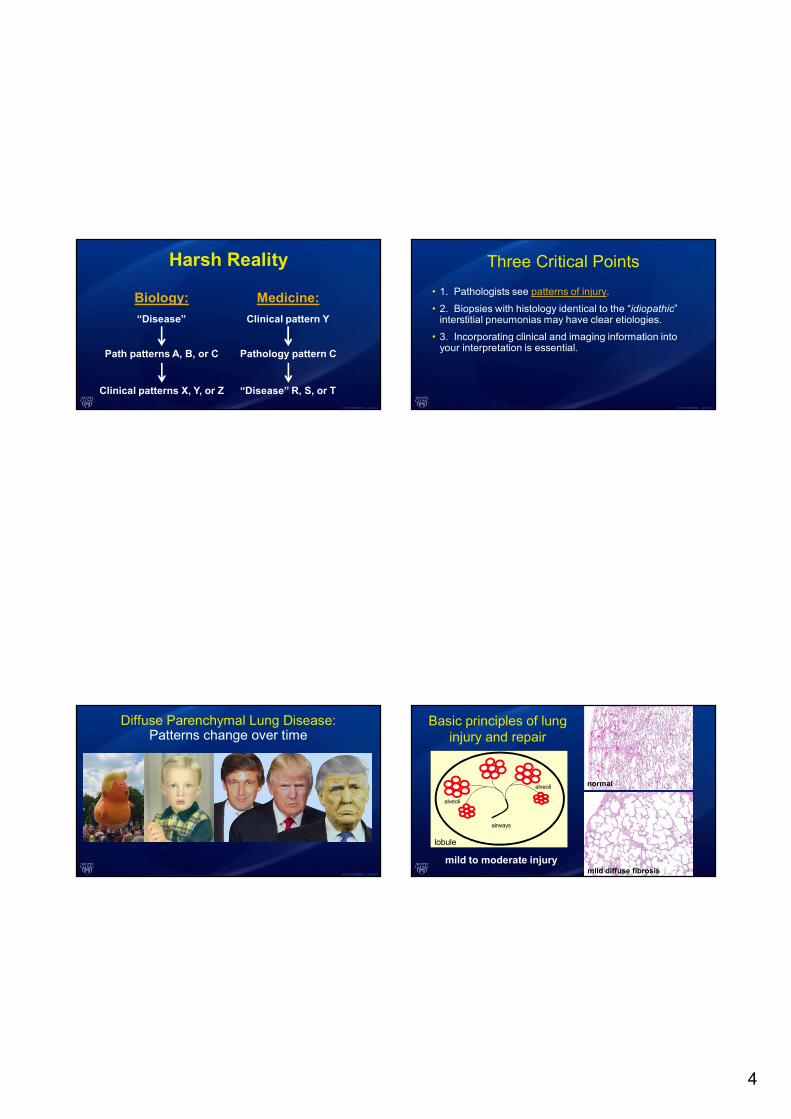
Harsh Reality
“Disease”
Path patterns A, B, or C
Clinical patterns X, Y, or Z
Biology:
“Disease” R, S, or T
Pathology pattern C
Clinical pattern Y
Medicine:
©2013 MFMER | slide-14
Diffuse Parenchymal Lung Disease:Patterns change over time
©2013 MFMER | slide-15
Three Critical Points
• 1. Pathologists see patterns of injury.
• 2. Biopsies with histology identical to the “idiopathic” interstitial pneumonias may have clear etiologies.
• 3. Incorporating clinical and imaging information into your interpretation is essential.
airways
lobule
alveoli
alveoli
mild diffuse fibrosis
normal
mild to moderate injury
Basic principles of lung injury and repair

5
airways
lobule
alveoli
alveoli
honeycombing
normal
severe injury
Basic principles of lung injury and repair
airways
lobule
alveoli
alveoli
airway-centered fibrosis
normal
inhalational injury
Basic principles of lung injury and repair
airways
lobule
alveoli
alveoli
peripheral, irregular, diffuse
normal
autoimmune injury
Basic principles of lung injury and repair
Bjoraker JA et al., Am J Respir Crit Care Med 1998 Jan;157(1):199-203
Idiopathic• IPF (CFA)
Non-idiopathic• Chr HP• CTD• Asbestosis• Chr drug rxn• Etc.
Prognostic significance of patterns
6
©2013 MFMER | slide-21
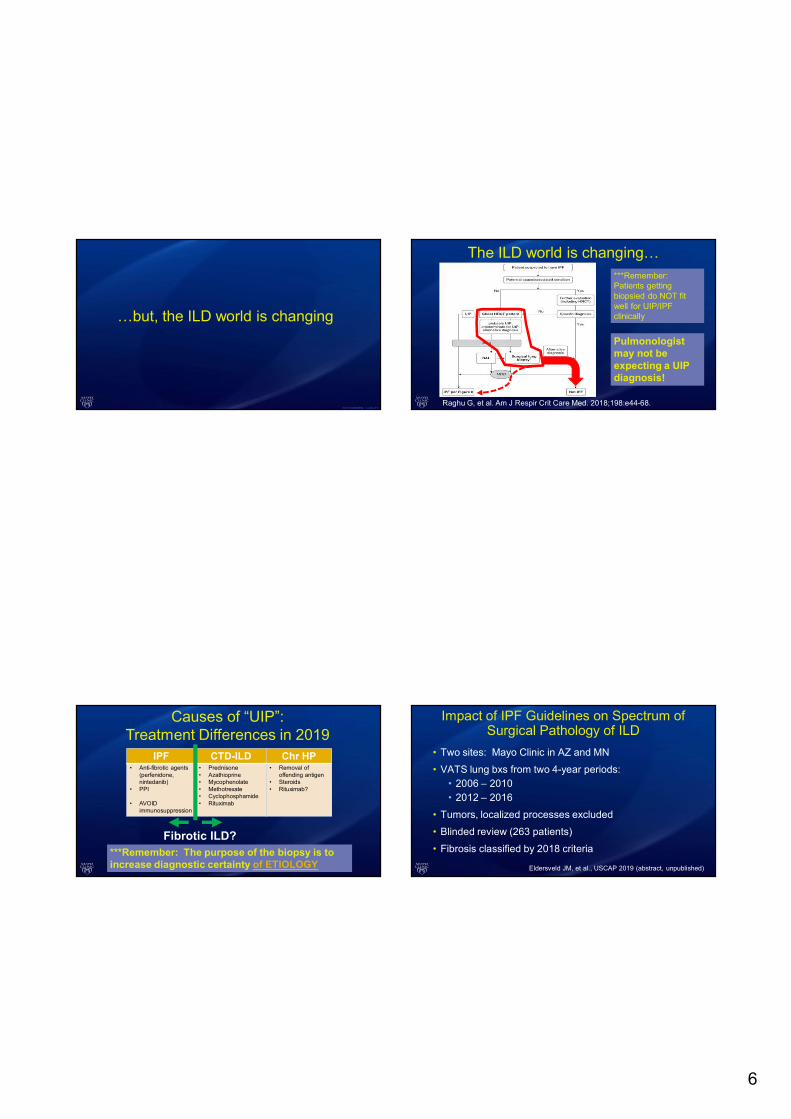
…but, the ILD world is changing
IPF CTD-ILD Chr HP• Anti-fibrotic agents
(perfenidone, nintedanib)
• PPI
• AVOID immunosuppression
• Prednisone• Azathioprine• Mycophenolate• Methotrexate• Cyclophosphamide• Rituximab
• Removal of offending antigen
• Steroids• Rituximab?
Causes of “UIP”:Treatment Differences in 2019
Fibrotic ILD?***Remember: The purpose of the biopsy is to increase diagnostic certainty of ETIOLOGY
Raghu G, et al. Am J Respir Crit Care Med. 2018;198:e44-68.
The ILD world is changing…
Pulmonologist may not be expecting a UIP diagnosis!
***Remember: Patients getting biopsied do NOT fit well for UIP/IPF clinically
Impact of IPF Guidelines on Spectrum of Surgical Pathology of ILD
• Two sites: Mayo Clinic in AZ and MN
• VATS lung bxs from two 4-year periods:• 2006 – 2010• 2012 – 2016
• Tumors, localized processes excluded
• Blinded review (263 patients)
• Fibrosis classified by 2018 criteria
Eldersveld JM, et al., USCAP 2019 (abstract, unpublished)

7
Eldersveld JM, et al., USCAP 2019 (abstract, unpublished)
Pre-2011
Post-2011
# o
f pa
tien
ts#
of p
atie
nts
Age
Age
Pretest probability of histology suggesting non-IPF diagnosis is now HIGH, even in elderly
The ILD world is evolving, too…
Relatively “old” pathology mantra:• Diagnose UIP when there is fibrosis with:
• Temporal heterogeneity• Old fibrosis (honeycombing)• Active fibroblast foci
• Geographic heterogeneity• Patchy
Photos: Public domain (www.canva.com)
Fire Extinguishers
Wood, Paper, Cloth, Etc.
Flammable Liquids
Flammable Gasses
Electrical Oils, Fats
Water
Foam
Dry Powder
CO2
8
Practice Your Skills!
Photos: Public domain (www.canva.com)
Practice Your Skills!
Photos: Public domain (www.canva.com)
Practice Your Skills!
Photos: Public domain (www.canva.com)
Alternative dx (not UIP) according to 2018 criteria
IPF CTD CrHP
Lymphoid Follicles - + +
Bridging Fibrosis - - +
Plasma Cells - + +
Chronic Bronchiolitis - + +
NSIP-like areas - + +
Multiple Patterns on the Same Biopsy - + +/-
IPF CTD CrHP
Hyaline Membranes +/- + -
Organizing Pneumonia +/- + +
Granulomas - - +
Marked Interstitial Infiltrate Away from Fibrosis
- + +
Prominant Airway Centered Changes - - +
Chronic Pleuritis - + -
Not listed in 2018 criteria
9
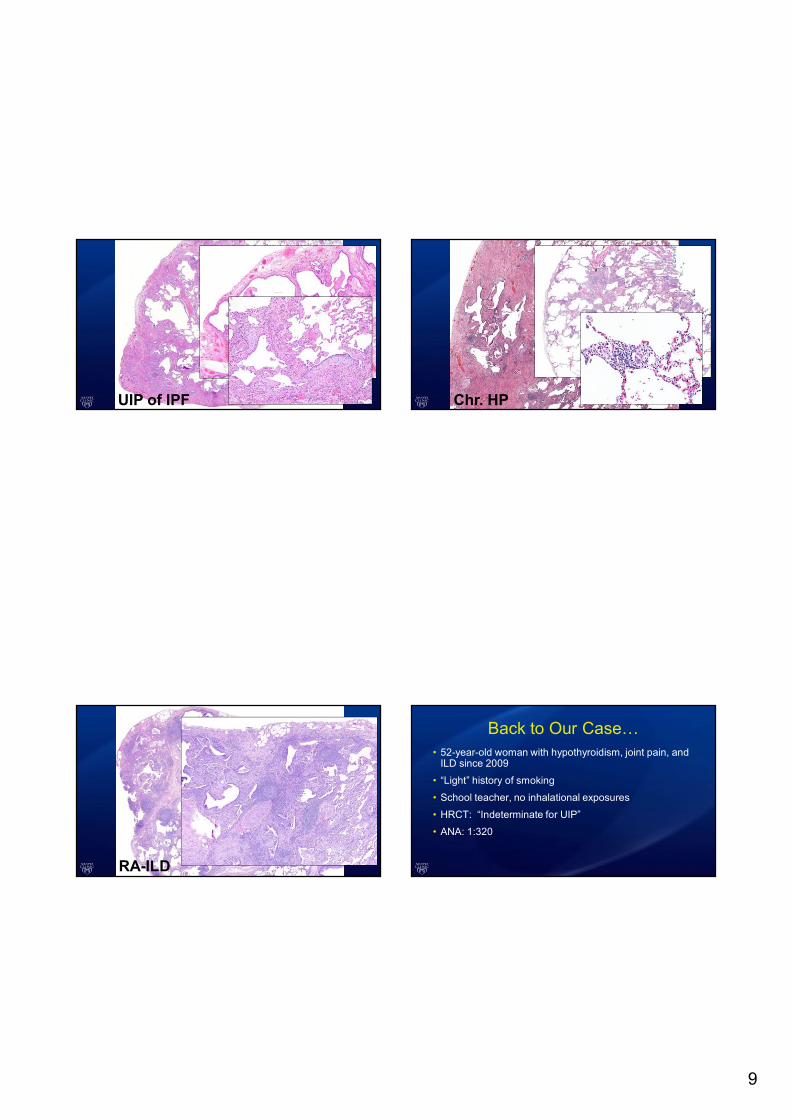
UIP of IPF
RA-ILD
Chr. HP
Back to Our Case…• 52-year-old woman with hypothyroidism, joint pain, and
ILD since 2009
• “Light” history of smoking
• School teacher, no inhalational exposures
• HRCT: “Indeterminate for UIP”
• ANA: 1:320
10
©2013 MFMER | slide-37
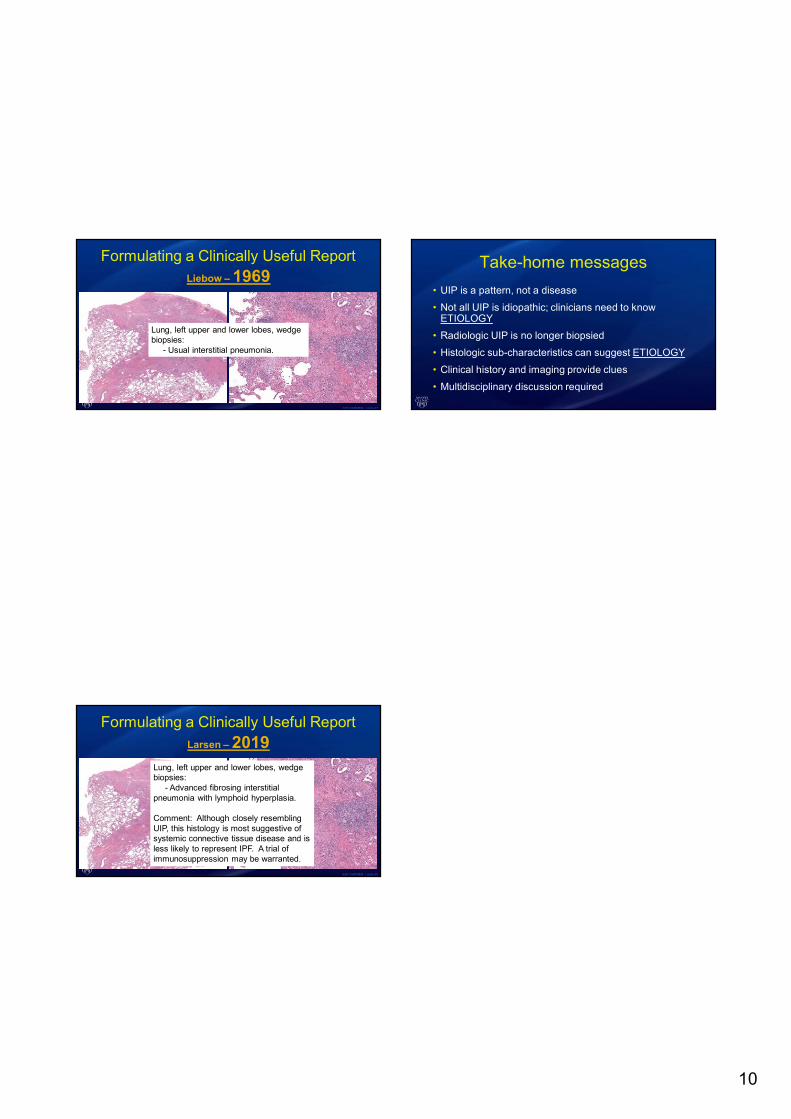
Formulating a Clinically Useful ReportLiebow – 1969
Lung, left upper and lower lobes, wedge biopsies:
- Usual interstitial pneumonia.
©2013 MFMER | slide-38
Formulating a Clinically Useful ReportLarsen – 2019
Lung, left upper and lower lobes, wedge biopsies:
- Advanced fibrosing interstitial pneumonia with lymphoid hyperplasia.
Comment: Although closely resembling UIP, this histology is most suggestive of systemic connective tissue disease and is less likely to represent IPF. A trial of immunosuppression may be warranted.
Take-home messages
• UIP is a pattern, not a disease
• Not all UIP is idiopathic; clinicians need to know ETIOLOGY
• Radiologic UIP is no longer biopsied
• Histologic sub-characteristics can suggest ETIOLOGY
• Clinical history and imaging provide clues
• Multidisciplinary discussion required





























