Embed Size (px)
Citation preview

ThrombophiliasSharon Sams

Objectives
Overview of etiology of hypercoagulability Available tests Clinical correlation or “What do I do with
these results?” Inconclusive conclusions: To test or not to
test…

Risk Factors: Acquired
Age: largest gradient of risk Malignancy: prevalence ranges from 3-18% Surgery:
Orthopedic surgery:30 - 50% Abdominal surgery: 30% With anticoagulants: 18%
Major trauma: 50-60% Immobilization

Risk Factors: Acquired
Oral contraceptives: 4 X increase in risk Hormonal replacement therapy: 2-4 X
increase Pregnancy and post-partum: 10 X increase Antiphospholipid antibodies: 10 X increase

Genetic causes of Thrombosis
Deficiencies of natural coagulation inhibitors Antithrombin, protein C, and Protein S
deficiencies; < 1% of the population Quantitative (type I): normal protein but
reduced quality Qualitative (Type II): Normal amounts of a
defective protein Heterozygote: Increased risk 10 X Homozygote: purpura fulminans

Genetic Causes: Factor V Leiden
Most common genetic defect causing thrombosis among Caucasians
Prevalence of carriers: 5 % Found in 15 % of patients with venous
thrombosis Causes thrombosis via resistance to activated
Protein C Heterozygote: Increased risk 3-8 X Homozygote: Increased risk 50-80 X; Found
in 1 per 5000 people in general population

Genetic causes of Thrombosis
Prothrombin G20210A Mutation Prevalence: 3% of Caucasians Increased risk 3 X
ABO Blood Group Non-O blood groups: 2-4 X increased risk Higher von Willebrand factor levels and higher
factor VIII levels

Plasma Abnormalities
Hyperhomocysteinemia Homozygous deficiency of cystathionine beta-synthase
(CS): Homocystinuria→ atherosclerosis, arterial disease and venous thrombosis
Mildly elevated homocystine: 5-10% of the population; Increased risk 2 X; usually due to low intake of folate, B6 or B12
High levels of clotting factors Elevated levels (above 90th percentile) of prothrombin,
Factor VIII, Factor IX, and Factor XI: Increased risk: 2-4 x

Multi-Casual Model
The thrombotic event is the result of gene- gene interaction and/or gene-environment interaction.
Variable RR Annual Incidence%
Normal 1 0.008
Hyperhomocysteinemia 2.5 0.02
Prothrombin G20210A 2.8 0.02
Oral contraceptives 4 0.03
Factor Leiden heterozygote 7 0.06
OCT and Factor Leiden 35 0.3
Factor Leiden homozygote 80 0.5-1

Lab evaluation
Timing: Acute thrombotic event or anticoagulation
therapy will affect the parameters of functional assays.
Wait 6 months after acute event 10 days after the discontinuation of oral
anticoagulation therapy

Lab testing: APC Resistance
APC Resistance Factor Leiden V: DNA analysis via PCR is the
gold standard Acquired APC: Paired PTT’s performed in the
presence and absence of exogenous activated Prot C; →dilute patient plasma with Factor V deficient plasma: specificity and sensitivity approach 100%

Lab Testing: Protein C, Protein S and Antithrombin DNA testing not available Functional assay to measure protein activity is the
initial screen– low specificity Antigenic assays are immunoassays that measure
the quantity of the protein Conditions that affect assay:
Negative influence: Oral anticoagulants, Vitamin K deficiency, liver disease, recent thrombosis, surgical
procedures, DIC, L- Asparaginase therapy, oral contraceptives, estrogen replacement therapy, pregnancy, elevated acute phase reaction, heparin and nephrotic syndrome

Lab Testing:
Prothrombin (G20210A) Mutation DNA test via PCR
Homocysteine Immunoassay methods
Coagulation Factors

Lab testing: Antiphospholipid antibodies Low specificity: clinical correlation required Solid phase antiphospholipid antibodies
Anticardiolipin Antibeta2glycoprotien I
Lupus anticoagulants Clotting time based assays such as Russell
viper venom test, kaolin clotting time, or PTT Improved sensitivity by use of two screening
tests

Current Treatment
Acute events: Management of acute thrombosis is the same for patients with and without inherited thrombophilia Anticoagulation with warfarin for 3-6 months
Secondary prophylaxis: No controlled trials have evaluated the
duration of anticoagulation in pts with hereditary thrombophilias thus no standard protocols.

Treatment Proposal I
Risk Classification ManagementHigh Risk Indefinite Anticoagulation Two or more spontaneous events One spontaneous life-threatening event One spontaneous event is association with
the antiphospholipid syndrome, antithrombin def
or more than one genetic or allelic abnormality
Moderate Risk Vigorous prophylaxis in high- risk setting
One event with a known provocative stimulus Asymptomatic

Association Studies
In patients presenting with a first venous thrombosis (adults) 5% have a deficiency of a natural
anticoagulant by phenotypic testing 15% Factor Leiden V deficiency 3-5% Prothrombin G20210A Mutation >70% have no inheritable abnormality

Risk of Reoccurrence
Two year cumulative incidence of recurrent thrombosis ~ 15%
Five year cumulative incidence of recurrent thrombosis ~ 25%
Early studies: 2-4 X increase in risk in Factor V Leiden carriers However these studies were small in number
and retrospective

Cambridge Venous Thromboembolism Study (CVTE) (2003) Two year Prospective Study:
570 patients Recurrence rate was 11%
Lowest incidence after surgery related VTE (0%) Highest incidence with unprecipitated VTE (19.4%)
85% of patients were tested for heritable thrombophilic defects→ recurrence rates were not related to presence or absence of heritable thrombophilia.
CONCLUSION: Thrombophilia testing had no predictive value for reoccurrence (hazard ration 1.5 [95% CI 0.82-2.77]; p=0.187)
Baglin et al. Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: prospective cohort study. The Lancet 2003, (362):523-526.

Leiden Thrombophilia study (LETS) JAMA 2005 Prospective follow up study of LETS pts
447 patients followed for a mean of 7.3 years Incidence rate of recurrence was highest during the
first two years: annual rate of 3.2%; cumulative recurrence of 12.4% at 5 years
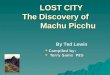
Risk of recurrence was 2.7 x higher in men than women (95% CI , 1.8-4.2)
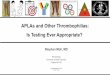
Higher risk of recurrence with idiopathic initial VTE Lower risk of recurrence with provoked initial VTE OCT use during follow up had a higher recurrence rate
(28 per 1000 pt-yrs vs 12.9 per 1000 pt-yrs)

Copyright restrictions may apply.
Christiansen, S. C. et al. JAMA 2005;293:2352-2361.
Recurrence Rates by Sex and Type of First Thrombotic Event

Copyright restrictions may apply.
Christiansen, S. C. et al. JAMA 2005;293:2352-2361.
Recurrence Rates by Oral Contraceptive Use in 215 Women Between 16 and 55 Years

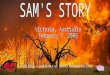
Copyright restrictions may apply.
Christiansen, S. C. et al. JAMA 2005;293:2352-2361.
Recurrence Rates for Prothrombotic Laboratory Abnormalities in 474 Patients

Leiden Thrombophilia study (LETS) JAMA 2005 Conclusion:
Hazard ratios calculated for reoccurrence according to individual defect → no defects were associated with a statistically significant hazard ratio
Clinical factors (male sex, use of OCT’s, idiopathic initial VTE) have a more significant role in risk of reoccurrence than lab abnormalities
Multi-causal disease. Combined defects at greater risk of reoccurrence?

Candidates for screening(Stefano et al 2002) All patients with venous thromboembolism,
independent of the age of onset, the circumstances and the severity
Cancer pts may be excluded Women with complications of a pregnancy All asymptomatic individuals who are a first degree
relative of a diagnosed carrier of a thrombophilic trait Asymptomatic women with a family history of venous
thromboembolism prior to use of oral contraceptives, HRT or pregnancy

Candidates for screening(Baglin 2004) Patient presents with first thromboembolism
Family history? If positive, testing is recommended Clinical circumstances- surgery or cancer? Testing not
indicated Clinical circumstance not associated with surgery or
cancer-acquired antiphospholipid activity is recommended
Screening asymptomatic relatives has no clinical utility Annual absolute incidence of venous
thromboembolism was very low

References:
1. Baglin T, Management of Thrombophilia: Who to Screen? Pathophysiol Haemost Thromb 2003/2004;33:401-404
2. Bauer KA, The Thrombophilias: Well defined risk factors with uncertain therapeutic implications. Ann Intern Med. 2001;135:367-373
3. Christiansen et al. Thrombophilia, Clinical Factors, and Recurrent Venous Thrombotic Events. JAMA 2005;293:2352-2361
4. Tripodi A, Laboratory diagnosis of thrombophilic states: where do we stand? Pathophysiol Haemost Thromb, 2002;32:245-248
5. Bauer et al. Hypercoagulability: Too many test, Too much conflicting data. Hematology 2002; 353-368
6. Stefanoe et al. Screeninf for inherited thrombophilia: indications and therapeutic implications. Haematologica 2002;87:1095-1108
7. Henry. Clinical Diagnosis and Management by Laboratory Methods. 20th ed. 2001 W.B. Saunders Co. Philadelphia
8. Baglin et al. Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: prospective cohort study. The Lancet 2003, (362):523-526.