Embed Size (px)
Citation preview

Tracy Minichiello, M.D.Associate Professor of Medicine
University of California, San FranciscoChief, SF VA Anticoagulation & Thrombosis Service
Thromboembolism Q&A: Cases and Controversies

CASE #1 A 55 year old woman being treated for osteomyelitis of the spine develops right upper extremity swelling. U/S reveals a DVT in the subclavian and axillary vein. She has a PICC line in that arm. How do you manage this?
a.Does she need anticoagulation?b.She will need another 3 weeks of IV
antibiotics. Do you remove the PICC Line?

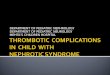
Venous thrombo
sis
Yes•Removal after fibrinolysis•Antibiotics•Anticoagulation if no contraindication•Elevate involved extremity
Septicthrombophlebitis?
Severelysymptomatic?
No
If SVCsyndrome or severesymptoms & lowbleeding risk
Considerthrombolysis
Yes
•Remove catheter•Anticoagulate
NoCatheterneeded?
No
•Remove catheter•Anticoagulate
Yes
•Keep catheter•Anticoagulate
Symptomsresolved?
No
Other accesssites available?
•Remove catheter•Place new catheter•Anticoagulate
•Keep catheter•Anticoagulate
Yes
No Considerthrombolysis
Yes
Management of catheter‐related venous thrombosisAnticoagulation generally recommended for 3 months after catheter removal

Upper Extremity DVT

CASE #2
A 45 year old man presents with complaints of moderate but persistent calf pain and swelling. He was kicked playing soccer a five days ago and symptoms have developed since then. Ultrasound shows DVT in the posterior tibeal vein. What do you recommend?

NEW CHEST GUIDELINESIn patients with acute isolated distal DVT of the leg and without severe symptoms or risk factors for extension, we suggest serial imaging of the deep veins for 2 weeks over initial anticoagulation (Grade 2C).CHEST 2012

ISOLATED DISTAL DVTant/post tibeal, peroneal
TREATMENTLOW RISKu/s 1-2 weeks and
treat only if extends proximally
HIGH RISKtreatment same as proximal DVT
HIGH RISK + d-dimer severe symptoms cancer VTE history no reversible provoking
factor hospitalized near proximal veins > 5 cm long, mult
veins, > 7 mm

CASE #3
A 55 year-old man presents with pleuritic chest pain. His BP is 120/70, HR 105, RR is 18, and his O2 sat is 97%. His physical exam is unremarkable. A chest CT shows multiple pulmonary emboli. ECG is normal.

CASE #3
What is this patient's risk of early mortality related to PE?
What anticoagulant regiman will you start and when?
Will he be admitted and if so for how long?

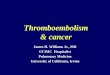
Pulmonary Embolism Severity Index
Risk Factor points Age age Male 10 Cancer 30 Heart failure 10 Chronic lung disease
10
HR > 110 20 SBP < 100 mmHG 20 RR >30 20 Temp < 36 20 Δ mental status 60 O2 sat <90% 20
Aujesky et al Eur Heart Journal 2006
class Points 30 day mortality
I 0-65 <1.7% II 66-85 <3.5% III 86-105 <7.1% IV 106-125 4-11% V >125 10-25%

Simplified Pulmonary Embolism Severity Index
Risk Factor points Age 1 if > 80 Cancer 1
Heart failure lung disease
1
SBP < 100 mmHG 1
O2 sat <90% 1
Severity class Points 30 day mortality LOW 0 1% HIGH 1 or more 10%
Jimenez, D. et al. Arch Intern Med 2010

Case #3a
His PESI score is 65, placing him in Class I, very low risk of PE related mortality. You decide to discharge him to home. He weighs 100 kg. He has CKD with CrCl of 39 ml/min. What dose of enoxaparin do you recommend?

Anticoagulation for VTEUse UFH preferentially
Immediate risk of bleeding
Renal Failure Extremes of weight Massive PE,submassive
PE when considering thrombolysis
CHEST 2012
LMWH preferred agent for acute treatment VTE

Enoxaparin Dosing in CKD
Treatment Doses Enoxaparin
1st 48hrs: 1mg/kg q12hrs* Maintenance: dose adjust based on renal function*:
Est CrCl(ml/min)
Fraction of usual daily dose
10‐19 0.320‐29 0.430‐39 0.540‐49 0.6≥ 50 1
Barras MA, Clin Pharmacol Ther. 2008; Barras MA, Ther Drug Monit. 2010

Enoxaparin Dosing in CKD
Barras MA, Clin Pharmacol Ther. 2008; Barras MA, Ther Drug Monit. 2010
Endpoints Individualized arm N=46
Conventional arm N= 54
Pvalue
Therapeutic Xa levels (0.5‐1)
69.9% 42.6% 0.02
SupratherapeuticXa (> 1)
9.3% 37.1% 0.02
Subthreapeutic Xa levels (<0.5)
12.9% 15.7% 0.97
Endpoints Individualized N=46
Conventional N= 54
P‐value
Any bleedig 1 (2%) 9 (15%) 0.03Composite bleed/bruise
6 (12%) 21 (40%) 0.003

CASE # 4
A 68 year old woman falls and fractures her hip. She is in CHF on admission so OR time is delayed. On HD #3 she becomes acutely short of breath and is found to have PE and DVT. How do you manage her anticoagulation perioperatively?

IVC Filter IndicationsIndication for IVC Filter Placement
ACCP( 1)
AHA (2)
British Committee for Standards in Hematology (3)
Thrombosis Interest Group of Canada (4)
Acute VTE and contraindication to anticoagulation
YES YES YES YES If proximal DVT present
VTE despite anticoagulation
NO YES MAYBE High intensity oral anticoagulation or LMWH should be considered prior to placement of filter
NO Anticoagulation should be intensified or alternative agent started. IVC filter will not prevent progression
Preoperatively in patients who have had recent VTE (within one month) and must have anticoagulation interrupted for surgery
____ ___ YES (VTE within 4 weeks prior to surgery)
YES (VTE within 2 weeks prior to major surgery)

IVC Filter Indications
Indication for IVC Filter Placement
ACCP( 1)
AHA (2)
British Committee for Standards in Hematology (3)
Thrombosis Interest Group of Canada (4)
Proximal DVT in patient with poor cardiopulmonary reserve
____ YES ___ There is no agreement on definition of poor reserve
Free-floating thrombus
____ ___ NO NO
Thrombolysis with proximal DVT
____ ___ NO NO
Primary prophylaxis in selected high risk patients (surgical, trauma etc)
NO ___ ____ NO

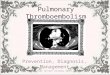
IVC Filters
PREPIC STUDY GROUP, Circulation 2005; Decousus NEJM 1998
Filter No Filter
PE@ 12 days
1% 5%
DVT @ 2 years
20% 11%
PE@ 2 years
3.4%(ns) 6.3%
PREPIC STUDY PREPIC 8 yr FOLLOW UP
DVTHR 1.52
PEHR 0.32
No survival benefit

NEW CHEST GUIDELINESIVC filters should only be placed in acute DVT who cannot tolerate blood thinners because of active bleeding or a high risk for bleeding. “We do not consider permanent IVC filter indication for extended anticoagulation”.CHEST 2012

How long will you recommend these patients stay on
anticoagulation? 55 yo man with
unprovoked PE?
3 months6 months12 monthsIndefinitely
68 yo woman with provoked PE?3 months6 months12 monthsIndefinitely

Risk of VTE Recurrence After Cessation of VTE
Risk factor 1st yr Next 5 yrs
Distal DVT 3% (6%) <10%
Major-transient
3% 10%
Minor-transient
5-6% 15%
Unprovoked At least 10% 30%
Recurrent > 10% > 30%
Kearon, Blood 2005

Diseases Associated with VTE
Systemic
disease
Clinical Features Diagnostic Data
IBD Bloody diarrhea, aphthous ulcers,
arthritis, rash
Histologic analysis of
intestinal biopsy
specimens
Nephrotic
syndrome
Periorbital edema, peripheral edema,
HTN, hypercholesterolemia
Urine protein analysis
Behcets Oral ulcers, genital ulcers,
ophthalmologic issues
--
(P. Vera/ ET Pruritis, plethora CBC, JAK-2 mutation

Systemic disease Clinical Features Diagnostic Data
Sickle cell disease Anemia, sickle crises Evaluation of the blood smear,
hemoglobin electrophoresis
Antiphospholipid
antibody
syndrome
Livedo, arthritis, rash Lupus anticoagulant, ELISA for
anticardiolipin antibody IgG and
IgM (assess 3 months after acute
event)
Cancer Weight loss, night
sweats
CBC, LFTS, PSA, pap smear,
routine cancer screening
Paroxysmal
nocturnal
hemoglobinuria
Hemolytic anemia CBC, Flow cytometry for CD55,
CD59
Pregnancy Amenorrhea Urine pregnancy test (all women of
childbearing age)

Copyright restrictions may apply.
Iorio, A. et al. Arch Intern Med 2010;170:1710-1716.
Recurrence Rate After Transient Risk Factor
3.3% in 1st yr
6.6% in 1st 2 yrs

Guidelines for Duration of Anticoagulation for VTE
Indication
8th ACCP guidelines
2012AHA 2010
ASH recommendations2008
First episode of VTE secondary to a transient risk factor
3 months (Grade 1B).
3 months (Class I Level A)
3 months
First episode of idiopathic (unprovoked) VTE
At least 3 months, prefer long-term treatment if risk/benefit ratio ok (Grade 2B).
At least 6 months, consider indefinite(Class I Level A)
6 months
Recurrent VTE Long term(Grade 1B).
IndefiniteClass I Level A).
Long term if APLS, AT deficiency or recurrence
Kearon et al CHEST suppl Feb 2012;Jaff et al Circulation 2011; Bounsameaux H et al Hematology 2009

Copyright ©2008 American Society of Hematology. Copyright restrictions may apply.
Siragusa, S. et al. Blood 2008
Residual Vein Thrombosis & VTE Recurrence
RVO+AC 19%
No RVO 1 %
RVO-AC 27 %
Recurrence rate

Palareti G et al. N Engl J Med 2006
Management Trial Using D-dimer Results to Determine Duration of Anticoagulation

Eichinger, Circulation 2010
Vienna Prediction Model for Recurrent VTE

Clinical Decision Rule Clinical predictors
Leg red or swollen or hyperpigment 5-7 mos after event
D-dimer >250 ug/L on ACBMI >30kg/m2Age> 65
Female patients with 0-1 risk factor had recurrence risk of 1.6%: ≥2 = 14%
Rodgers et al CMAJ August 2008

Risk Score For Predicting Recurrent VTE
DASHD-dimerAge > 50Sex-maleHormonal therapy
Score Annualized Risk≤1 3.1%2 6.4%≥3 12.3%
Tosetto A et al J Thromb Haemost. 2012

Risk Score For Predicting Recurrent VTE
DASH POINTSd-dimer elevated after completion of blood thinner
+2
age > 50 1male 1female with VTE on hormonal therapy
-2
SCORE ANNUALIZED RISK
≤1 3.1%2 6.4%≥3 12.3%
Tosetto A et al J Thromb Haemost. 2012

Clinical presentation predicts likelihood and type
of recurrence Distal (calf vein thrombosis)
Low risk of recurrence/PE Proximal- nearly 5 fold increased
recurrence risk over distal PE vs. DVT
Patients presenting with PE are 3x more likely to suffer recurrent PE than those presenting with DVT
Baglin T etJ Thromb Haemost. 2010

How long will you recommend these patients stay on
anticoagulation? 55 yo man with
unprovoked PE?
3 months6 months12 monthsIndefinitely
68 yo woman with provoked PE?3 months6 months12 monthsIndefinitely

Case 5c
Do either of these patients need a work up for laboratory thrombophilia?

Impact of Thrombophilia on Recurrence Risk
Patient group Recurrence of VTE per Yeartotal 2.6%1 thrombophilia defect 2.5%Iniitial VTE provoked 1.8%Initial VTE unprovoked 3.3%Unprovoked with thrombophilia 3.4%Unprovoked without thrombophilia
3.2%
Christiansen JAMA 2005
Shulman Amer j Med 1998

Impact of Acute Thrombosis & Anticoagulation on Thrombophilia Testing
increasedFactor VIII level
decreasedAntithrombinlevel
decreasedNo effectdecreasedProtein C, S
prolongedprolongedLupus anticoagulant
Anticardiolipinantibodies
WarfarinHeparinAcute VTEtest
no effectno effectincreasedFactor VIII level
increaseddecreaseddecreasedAntithrombinlevel
decreasedNo effectdecreasedProtein C, S
prolongedprolongedMay be prolonged
Lupusanticoagulant
no effectno effectMay beelevated
Anticardiolipinantibodies
WarfarinHeparinAcute VTEtest

Laboratory Thrombophilia
Women of childbearing years Patients with suspicion for APLS Strong family history of VTE Patients with recurrent VTE Results will influence therapy
(duration) Unprovoked PE < 50 yo

Individual Bleeding Risk on Anticoagulation
Bleeding Risk Factors Age > 75 Previous GI bleed
with no reversible cause
Previous bleed on warfarin
Renal/hepatic failure Antiplatelet therapy Cancer
Case fatality rate VTE Case fatality rate of
recurrent VTE highest in 1st 3-6 months-11%
Case fatality rate of recurrent VTE decreases after 3-6 months to 3.6%
Carrier Ann Intern Med 2010

Duration of AnticoagulationUnprovoked VTE
ng
riskConsider
indefinite
tx(PE,
male,
thrombophilia)Discuss
patient
preference
No
RVOClinical
prediction
rule:<1
stop
anticoagulation
Measure
D-dimer
at
30days,if
low
okIf
elevated
consider
Restarting
tx
ence
of
RVO
Continue
anticoagulation
and
repeat
U/S
IF DVT Get u/s and measure d-dimer . If d-dimer up continue AC

Aspirin for Prevention of Recurrent VTE.
Becattini C et al. N Engl J Med 2012
Recurrent VTE•ASA 6.6%•Placebo 11.2 %
•↓VTE 40% •No difference in major bleeding

CASE # 6
A 33 year old woman diagnosed with left lower extremity DVT 3 months ago maintained on warfarin present with complaints of pleuritic chest and shortness of breath. A CT angio of the chest reveals new bilateral subsegmental pulmonary emboli.

CASE #6
She reports compliance with her warfarin therapy and has an INR of 2.5 at the time of admission. She is admitted to your service for recurrent VTE. How do you manage this?

VTE Despite Anticoagulation
Medication adherence Antiphospholipid antibody syndrome Cancer DIC/Trousseaus Heparin-induced thrombocytopenia Myeloproliferative disorder Antithrombin deficiency Structural defect

VTE Despite Anticoagulation
Warfarin failureTransition to LMWH then transition to
warfarin with higher target OR continue LMWH
LMWH failureChange to BID dosingIncrease dosing by 20%Follow anti-Xa levels

Treatment of VTE Recurrence in Cancer
Patients
Lee, A ASH Education Book December 4, 2010

CASE #7
69 year old man with history of AFIB, diabetes, hypertension is having total hip arthroplasty. He is on warfarin as an outpatient for stroke prophylaxis. How do you mange his anticoagulation in perioperative period?

Perioperative Management of Anticoagulation
Spyropoulus et al Blood. 2012

Perioperative Management of Anticoagulation
Spyropoulus et al Blood. 2012

Case #8A 60 year old man with hyperlipidemia and hypertension on atenolol, a statin and ASA develops AFIB. His CHADS2 score is 1. You:A) start warfarin for stroke prophylaxisB) continue ASA for stroke prophylaxis

NEW CHEST GUIDELINES
AFIB CHADS2=0 no therapy (2B); CHADS ≥1 anticoagulant (1B);if unsuitable for AC use asa+clopidigrel rather than asa (1B)