Embed Size (px)
Citation preview

They Are Paying US What?! Can
TAVR Ever be Financially Viable? Wilson Y. Szeto, MD
Associate Professor of Surgery
Surgical Director, Transcatheter Cardio-Aortic Therapies
Associate Director, Thoracic Aortic Surgery
Division of Cardiovascular Surgery
University of Pennsylvania Medical Center
Philadelphia, PA
TCT@AATS: New Technologies for A New Future
AATS 2013

Disclosure
Edwards Lifesciences
PARTNER trial Sub-Investigator
PARTNER II Steering Committee
Clinical Proctor
Micro Interventional Devices
Consultant

Can We Afford TAVR?

The Cost to Society

No Survival Benefit STS > 15
“Cohort C”

TAVR Drift Into Lower Risk Patients
Operable AS patients
90% 10%
Low-Intermediate Risk High Risk
Inoperable
Too Sick
II A A High
Risk
B Extreme
Risk
C
Courtesy M. Leon
New patients - increasing
50%?

Why grow TAVR as a Service Line?
Pro:
• Part of core mission of a multidisciplinary advanced valve program
• Strategic link to valve surgery – AVR is profitable
• “Upstream & downstream” activity – relatively minor
• ”Halo effect” – real but difficult to quantify
Con:
• Unprofitable on its own
• Resource intensive – opportunity cost to develop other services
• Few options to improve the financials – by hospitals or physicians

8
Contribution Margin of Various Cardiac Treatments
Surgery - Valve
PCI
EP - AICD / Pacemaker
Surgery - CABG
Medical - ArrhythmiaMedical - Heart Failure
Medical - ASC
Surgery - Other
Medical - ACS EPS
AAA
Surgery - Vascular Vascular - Interventional
Other
Medical - OtherMedical w Cath
TAA
Transplant / VAD
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
$80,000
- 100 200 300 400 500 600 700 800 900 1,000
Ave
rage
Con
trib
utio
n Pe
r Ca
se
Case Volume (Primary Cardiovascular Diagnosis )
Most Desirable
Least Desirable
Increase Volume
Increase Efficiency
Key:1) Bubble Size = Total Contribution2) Axes Cross at Averages (393, $12,075)
Valve procedures are highly profitable; generating a healthy average
contribution margin and per case gain

9
50% of growth in valves: “Partner Effect”
Accelerated slope
since initiation of TAVR
program
HUP – Valve primary procedure volume

10
Expired prior to decision
88
9.3%
Enrolled for TAVR trial
(Partner 1 & 2)
258
27.5%
Enrollment Failure
427
45.5%
Total TAVR Referrals 11/2007 – 10/27/2011
4 Year Total = 939
AVR +/- Concomitant
128
30.0%
Medically Managed
299
70.0%
Pending Workup / Decision
166
17.7%
To enroll 258 patients, 939 were evaluated
Of patients evaluated, approximately:
1 is 4 enrolled
1 in 8 is not enrolled but has open AVR


Results: 12-Month Follow-up Costs
D=($26,025)
D=$705 D=1,870 D=$79
Total F/U Costs (12 months)
TAVR $29,352
Control $52,724
D = $23,372
p<0.001

15,586
2,316 3,223
1,126
14,069
4,666
2,397
833 $0
$5,000
$10,000
$15,000
$20,000
Hospitalizations Rehab SNF Other Outpatient
TF-TAVR (n = 239) AVR (n = 217)
12-Month Follow-up Costs Transfemoral
D = $1,517
D = ($2,350)
D = 827
D = $293
Total F/U Costs (12 months)
TF-TAVR $22,251
AVR $21,965
D = $287
P = 0.97

Post FDA Approval
The Real World Financial Reality

PAYMENTS
Physician Pro fee payments are procedure-specific
Hospital payments aren’t

Pro Fee Coverage
FDA Approval
• TF & TA are FDA approved for all indications
• Covered by the CMS NCD for TAVR
As long as all other conditions of the NCD are met
Coverage
• Multi-discipline team approach between Cardiologist and Surgeon required
– Op notes must reflect co-surgery approach.
– “62” modifier recommended by CMS for both TF & TA
• Two face-to-face cardiac surgery evaluations prior to the procedure are required
• Private payers are creating coverage.
– Case-by-case approval often required for TA or High Risk indications for non-
Medicare patients
All patients need to be registered in the TVT Registry regardless of
payer

Pro Fee Coding 62.5%
to each
operator
PA Medicare Rates New CPT
Codes 2013Description Approach wRVUs
33361 - 62 TAVR with prosthetic valve; percutaneous femoral artery approach 25.13 $1,502.00 $938.75
33362 - 62 TAVR with prosthetic valve; open femoral artery approach 27.52 $1,643.00 $1,026.88
33363 - 62 TAVR with prosthetic valve; open axillary artery approachAxilliary
artery28.50 $1,701.00 $1,063.13
33364 - 62 TAVR with prosthetic valve; open iliac artery approach Iliac artery 30.00 $1,809.00 $1,130.63
33365TAVR with prosthetic valve; transaortic approach (eg, median sternotomy,
mediastinotomy)TAo 33.12
0318T - 62Implantation of catheter-delivered prosthetic aortic heart valve, open thoracic
approach, (eg, transapical, other than transaortic)TA
n/a ─ we
use 33.12
33367TAVR with prosthetic valve; cardiopulmonary bypass support with
percutaneous peripheral arterial and venous cannulation (eg, femoral vessels)
(List separately in addition to code for primary procedure)11.18
33368TAVR with prosthetic valve; cardiopulmonary bypass support with open
peripheral arterial and venous cannulation (eg, femoral, iliac, axillary vessels)
(List separately in addition to code for primary procedure)
14.39
33369TAVR with prosthetic valve; cardiopulmonary bypass support with central
arterial and venous cannulation (e.g., aorta, right atrium, pulmonary artery)
(List separately in addition to code for primary procedure)19.00
Effective January 1st, 2013
Deleted for 2013: 0258T, 0259T
Note: There are no RVUs for "T" codes. For internal purposes, we used 41/case.
TAVR Professional Charges
Femoral
artery
varies with carrier
Primarily
TA & TAo
PERFUSION
Add-on to Primary CPT:
33361, 33362, 33363,
33364, 33365, 0318T
Surgery Only
Replaces
0256T

Review of profitability measurement at UPHS
Revenue Payments, including IME & GME
─ Direct Cost Prices paid for billable services & supplies
Contribution to Overhead Earnings to apply to overhead
+ Indirect Revenue Funds not tied to specific patient stays, e.g., tobacco
settlement funds, emergency access grants
─ Indirect Cost Costs not tied to specific patient stays aka Overhead -
building, equipment, admin, malpractice, utilities, advertising
Gain/(Loss) Funds available for investment/
expansion/ replacement & upgrades
or losses to be subsidized
Bottom Line
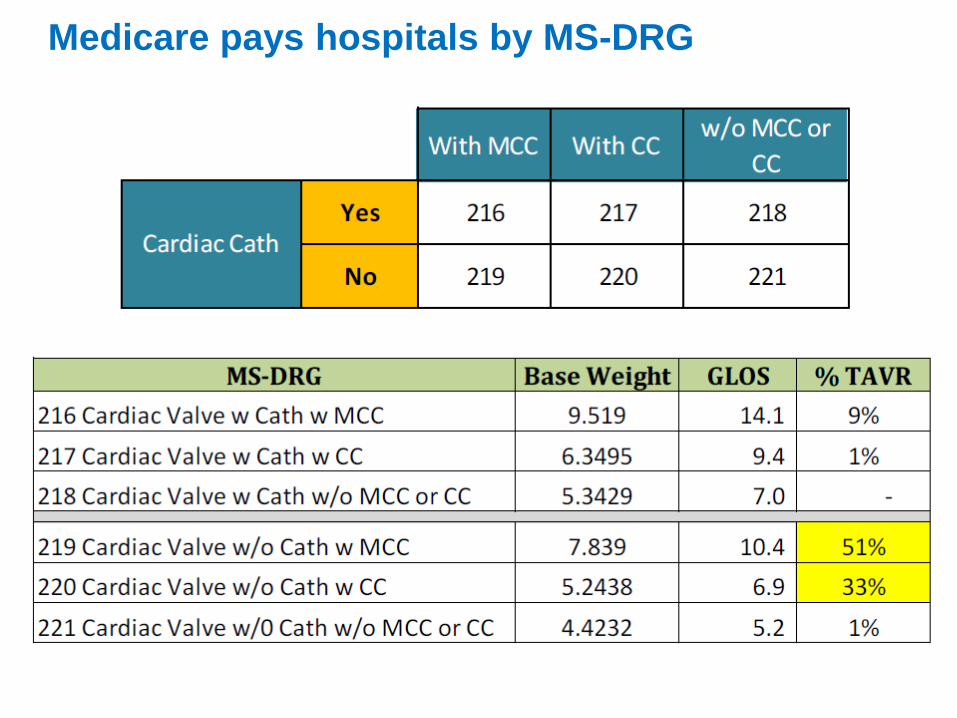
Medicare pays hospitals by MS-DRG

To Medicare these are all the same thing
MSDRGs 216 – 221
“Valve surgery”
• Endovascular / Transapical replacement of aortic valve
• Endovascular / Transapical replacement of pulmonary valve
• Endovascular replacement of unspecified heart valve
• Open heart valvuloplasty without replacement
• Open and other replacement of heart valve
• Annuloplasty
• Insertion of percutaneous external heart assist device
• Resection of other thoracic vessels with replacement
• Endovascular implantation of graft in thoracic aorta
TAAs
Root Hemi Arch
Ascending Hemi-arch
Ascending Hemi with
TEVAR
TEVAR
Thoracoabdominal


Medicare payment basics
$ Medicare payment
Hospital base determined
by several factors
$ Hospital-specific base rate
Indirect medical education
Disproportionate share
Regional wage rate adjustment
others
Determined by CMS x MS-DRG weight
As a result:
• HUP rates are 61% higher
• PPMC rates are 38% higher
• Medicare payments are 17% higher at HUP than PPMC for the same
procedure.
• HUP receives the 135th highest Medicare case rate in the country, PPMC
is 366th.
HUP - #8
PPMC - #185
University of Michigan - #24
New York-Presbyterian - #86
Massachusetts General - #97
Mayo St Mary - #150
Northwestern Memorial - #187

Medicare MS-DRG 219 payment 3 different hospital rates
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
$80,000
$90,000
$100,000
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Cu
mu
lati
ve $
Day Of Stay
HUP rate $72,959
Transfer penalty
“National” rate $45,409
PPMC rate $62,581

The cost of the valve is significant
Patient “PC” May 2012
4 hours of OR time includes perfusion, anesthesia, prep & recovery, intra-operative monitoring, additional cath & OR staff
Ancillary includes PT, RT, EKG
Department 1 2 3 4 5
OR Supplies 32,825
01305192 TAVIAORTIC VALVE 32,500 32,500
01304336 CATHETER ANGIOPLASTY NON LA 325 325
OR time 4,288 4,461 10%
Nursing - Med/Surg 802 802 802 2,405 5%
Nursing - SICU 1,606 1,606 4%
Lab 289 230 653 106 19 1,297 3%
Pharmacy 43 467 170 96 25 802 2%
Ancillary 176 110 144 69 87 413 1%
Imaging 36 26 143 26 62 293 1%
Total Direct 1,346 39,552 1,912 1,100 193 44,101 100%
Total Indirect 942 11,274 1,338 770 135 14,459
TOTAL COST 2,288 50,826 3,250 1,870 327 58,561
Day of Stay
74%
Total% Direct
Cost
OR Supplies, driven
by valve, are 74% of
direct cost


Medicare payment basics
$ Medicare payment
$ Hospital-specific base rate
Indirect medical education
Disproportionate share
Regional wage rate adjustment
others
x MS-DRG weight
Under certain conditions this
payment is reduced
For TAVR MS-DRGs, hospital payment is reduced when:
– LOS is at least one day less than the GLOS
– Patient is transferred to another hospital
or
– discharged to home health care when the patient receives clinically
related care within three days of discharge
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/AcutePaymtSysfctsht.pdf
Federal Register Pages 51,709-51-711
Determining the payment:
Transfer Rule
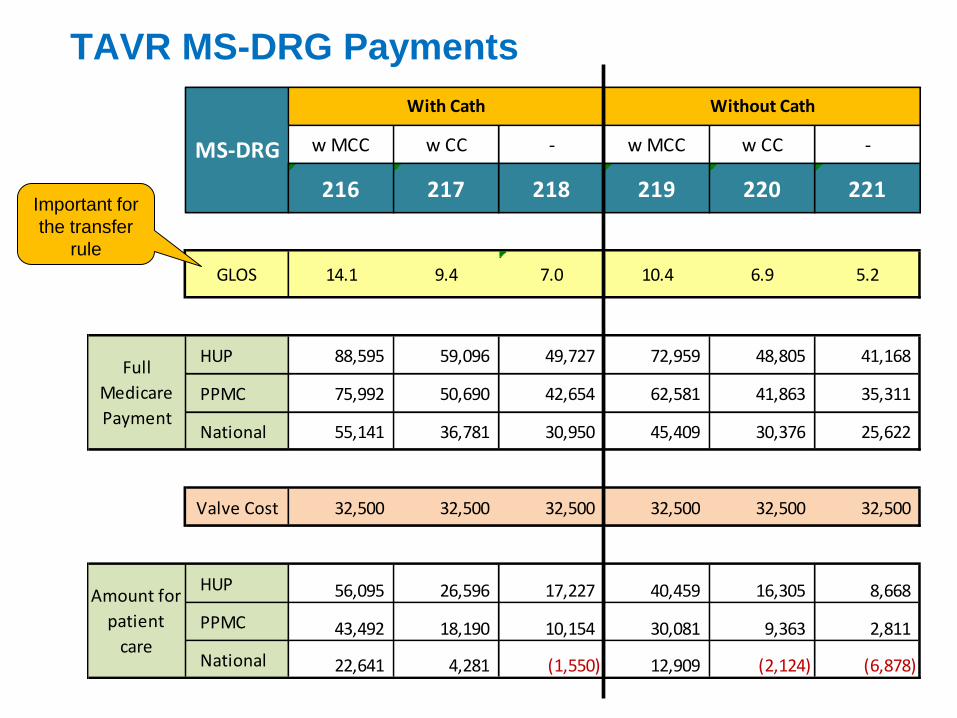
TAVR MS-DRG Payments
w MCC w CC - w MCC w CC -
216 217 218 219 220 221
GLOS 14.1 9.4 7.0 10.4 6.9 5.2
HUP 88,595 59,096 49,727 72,959 48,805 41,168
PPMC 75,992 50,690 42,654 62,581 41,863 35,311
National 55,141 36,781 30,950 45,409 30,376 25,622
Valve Cost 32,500 32,500 32,500 32,500 32,500 32,500
HUP 56,095 26,596 17,227 40,459 16,305 8,668
PPMC 43,492 18,190 10,154 30,081 9,363 2,811
National 22,641 4,281 (1,550) 12,909 (2,124) (6,878)
Without CathWith Cath
Full
Medicare
Payment
Amount for
patient
care
MS-DRG
Important for
the transfer
rule
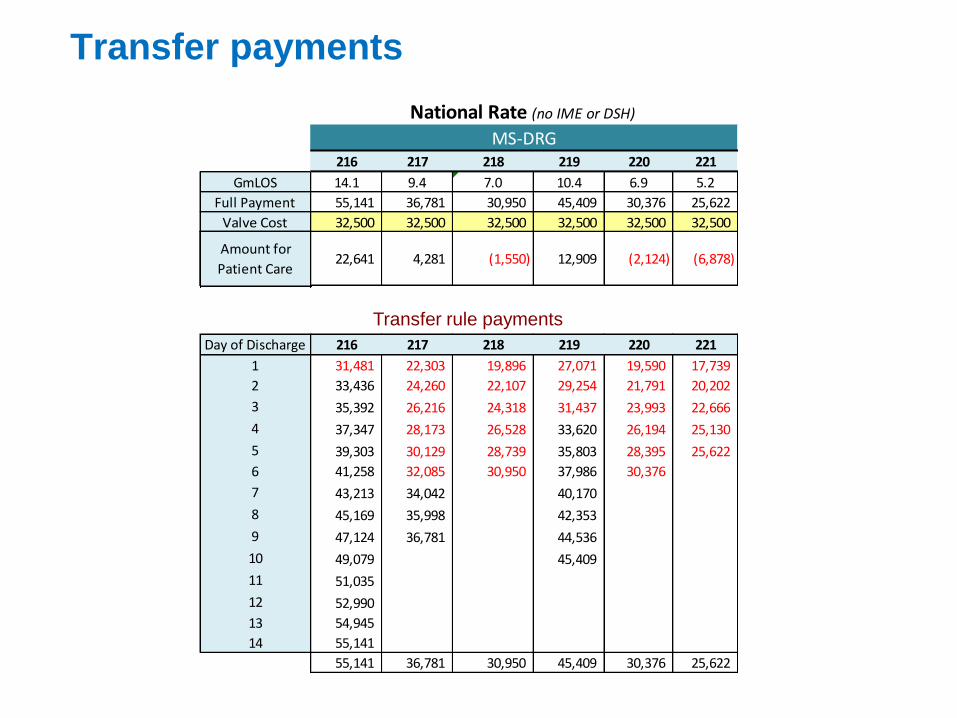
Transfer payments
Day of Discharge 216 217 218 219 220 221
1 31,481 22,303 19,896 27,071 19,590 17,739
2 33,436 24,260 22,107 29,254 21,791 20,202
3 35,392 26,216 24,318 31,437 23,993 22,666
4 37,347 28,173 26,528 33,620 26,194 25,130
5 39,303 30,129 28,739 35,803 28,395 25,622
6 41,258 32,085 30,950 37,986 30,376
7 43,213 34,042 40,170
8 45,169 35,998 42,353
9 47,124 36,781 44,536
10 49,079 45,409
11 51,035
12 52,990
13 54,945
14 55,141
55,141 36,781 30,950 45,409 30,376 25,622
Transfer rule payments
216 217 218 219 220 221
GmLOS 14.1 9.4 7.0 10.4 6.9 5.2
Full Payment 55,141 36,781 30,950 45,409 30,376 25,622
MS-DRG
PAYMENT BY LENGTH OF STAY UNDER THE TRANSFER RULE
National Rate (no IME or DSH)
Valve Cost 32,500 32,500 32,500 32,500 32,500 32,500
Amount for
Patient Care22,641 4,281 (1,550) 12,909 (2,124) (6,878)
Amount for
Patient Care

Conclusions
Fairway is narrow
• Short LOS often incurs transfer penalty
• Long LOS increase case cost
Only a few AMCs (hospitals with high IME payments) are
likely to cover their costs
Little room to improve the financial picture
TAVR (in isolation) is not profitable for most hospitals
Medicare rules change every year
Decreased valve cost could change it completely

Recommendations
Audit your program
Meet with your coders
Understand length of stay and site of stay
Understand the transfer penalty
Obtain the most appropriate reimbursement (DRG)
Photo By Thinkstock
Track patients
Analyze Cost
“Acute on Chronic diastolic heart failure”