Embed Size (px)
Citation preview

Accepted Manuscript
Therapeutic outcomes and thromboembolic events after treatment of acute arterialthromboembolism of the upper extremity
Hyung-Kee Kim , Heekyung Jung , Jayun Cho , Seung Huh , Jong-Min Lee , Young-Wook Kim
PII: S0890-5096(14)00611-6
DOI: 10.1016/j.avsg.2014.08.022
Reference: AVSG 2169
To appear in: Annals of Vascular Surgery
Received Date: 9 March 2014
Revised Date: 4 June 2014
Accepted Date: 21 August 2014
Please cite this article as: Kim HK, Jung H, Cho J, Huh S, Lee JM, Kim YW, Therapeutic outcomes andthromboembolic events after treatment of acute arterial thromboembolism of the upper extremity, Annalsof Vascular Surgery (2014), doi: 10.1016/j.avsg.2014.08.022.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Therapeutic outcomes and thromboembolic events after treatment of acute arterial 1
thromboembolism of the upper extremity 2
3
Hyung-Kee Kima, Heekyung Junga, Jayun Choa, Seung Huha, Jong-Min Leeb, 4
Young-Wook Kimc 5
6
aDivision of Vascular Surgery, Department of Surgery, bDepartment of Radiology, 7
Kyungpook National University School of Medicine, Daegu, cDivision of Vascular Surgery, 8
Cardiac and Vascular Center, Samsung Medical Center, Sungkyunkwan University School of 9
Medicine, Seoul, South Korea. 10
11
12
*Corresponding author: 13
Seung Huh, M.D., Ph.D., Professor 14
Division of Vascular Surgery, Department of Surgery 15
Kyungpook National University School of Medicine 16
130, Dongduk-ro, Jung-gu, Daegu, 700-721, South Korea 17
Phone: +82-53-420-6520 18
Fax: +82-53-421-0510 19
E-mail address: [email protected] 20
21
Article type: Original Article 22
23
Running title: Therapeutic outcomes after thromboembolism of arm 24

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Abstract 25
26
Background: To investigate short- and long-term outcomes of patients with acute arterial 27
thromboembolism of upper extremity, focusing on postoperative thromboembolic events by 28
etiology. 29
Methods: Hospital records of 53 patients (average age, 70 years; males, 49%) with acute 30
arterial thromboembolism of upper extremity treated between June, 1993 and December, 31
2013 were retrospectively reviewed, evaluating patient characteristics and clinical outcomes, 32
both short- and long-term. Subjects were stratified as those with (group I, 34) and without 33
(group II, 19) atrial fibrillation as underlying cause. 34
Results: Two patients received anticoagulation alone as conservative treatment. The 35
remainder (n=51) underwent surgical revascularization. Symptoms resolved in 51 patients 36
(96%) except 2 patients with postoperative re-occlusion, and there was no need of amputation 37
in all patients. Overall inpatient mortality was 5.6% (3/53). Patients of group I suffered most 38
of the recurrent thromboembolic events (group I: 17 events, 14 patients; group II: 2 events, 2 39
patients) recorded during follow-up (mean duration, 56.8±62.2 months). Respective event-40
free survival rates at 1 year, 3 years, and 5 years differed significantly by group: 77%, 44%, 41
and 44% for group I; 100%, 100%, and 83% for group II (p=0.004). Among 14 patients with 42
recurrent embolic events in group I, half of patients were not receiving anticoagulants, 43
however, anticoagulant cessation was generally arbitrary. Overall survival rates at 1 year, 3 44
years, and 5 years were 82%, 69%, and 52% for group I and 84%, 78%, and 70% for group II 45
(p=0.21). 46
Conclusion: In this study, surgical treatment of acute arterial thromboembolism of upper 47
extremity was largely successful. Especially in patients with atrial fibrillation, adequate long-48

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
term anticoagulation is indicated as prophylaxis, given the high rates of recurrent 49
thromboembolic events. 50
51
Keywords: thromboembolism, upper extremity, atrial fibrillation, recurrence 52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
INTRODUCTION 73
74
Acute arterial thromboembolism of upper extremity (ATUE) is implicated in a low 75
percentage (15-25%) of patients with acute limb ischemia.1-3 Standard treatment of acute 76
ATUE includes administration of heparin and balloon catheter thromboembolectomy via 77
brachial approach. More recently, thrombolysis and thromboaspiration have been reported as 78
acceptable options, based on short-term results.4-6 However, extended follow-up is another 79
matter because these patients are in the risk of recurrent thromboembolism due to the 80
potential source. 81
Whereas many follow-up studies amply detail long-term outcomes of acute arterial 82
thromboembolism of lower extremity (ATLE) (i.e., higher mortality relative to general 83
population and benefits of post-thromboembolectomy anticoagulation),7-9 similar efforts 84
addressing the upper extremity are few, assessing short-term outcomes at best.10-12 Such 85
reports are focused primarily on determining acceptable and sustained durability of surgical 86
treatment with balloon catheter; and although they do indicate a rise in mortality following 87
discharge of patients with acute ATUE, rates of recurrent embolic events in this setting are 88
not well-documented long-term. 89
The purpose of this study was to investigate short- and long-term therapeutic outcomes of 90
patients with acute ATUE, focusing on postoperative thromboembolic events by etiology. 91
92
MATERIALS AND METHODS 93
94
Between June, 1993 and December, 2013, 53 consecutive patients undergoing treatment for 95
acute ATUE at Kyungpook National University Hospital, Daegu, Republic of Korea, were 96

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
eligible for study. The present study was initiated after obtaining approval from the 97
Institutional Review Board at our institution (IRB Number: KNUH 2013-12-036-001). 98
Informed consent for review of the medical records was exempted by the board because this 99
was a retrospective study. Patients suffering arterial trauma (including iatrogenic injury), 100
vascular access-related occlusion, and acute thrombosis of a chronic subclavian arterial 101
stenosis were excluded. 102
Fifty patients were admitted through the emergency department with acute-onset symptoms 103
such as loss of sensation, weakness, pain, paleness, lack of pulse, and remaining 3 patients 104
were consulted to our department during admission period caused by other disease. Prior to 105
December, 2002, conventional angiography was used for the diagnosis. Thereafter, computed 106
tomography angiography (CTA) or duplex ultrasonography was engaged. 107
General protocol called for intravenous heparin (3,000 to 5,000 IU as bolus injection) at time 108
of diagnosis and operative thromboembolectomy, using a Fogarty catheter. Lysis or 109
thromboaspiration were not permitted as initial interventions. Either S-shaped or longitudinal 110
skin incision was first made above the bifurcation of brachial artery. After harnessing of 111
brachial, radial, and ulnar arteries with vessel loops, transverse brachial arteriotomy was 112
performed, just proximal to the bifurcation. Bi-directional Fogarty thromboembolectomy of 113
the above three arteries then took place, and closure of the arteriotomy was achieved with 114
interrupted Prolene™ suture. The adequacy of thromboembolectomy was determined by 115
physical examination (i.e., palpation of radial artery) and hand-held Doppler device. 116
Completion angiography was not used if pulsation was restored, or if post-117
thromboembolectomy Doppler study was considered adequate. Unless contraindicated, all 118
patients subsequently were given low-molecular-weight or unfractionated heparin for 119
anticoagulation, which prior to discharge was replaced by warfarin for indefinite use as 120

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
tolerated. During the first 3 months, patients visited the outpatient clinic monthly for 121
international normalized ratio (INR) testing, monitoring of clinical symptoms, and physical 122
examination (including brachial and radial pulse assessment). This regimen was then 123
conducted at 3-month intervals, adjusting warfarin dosage as needed. If clinical symptoms 124
developed or physical status declined, duplex ultrasonography was performed to check for 125
embolic recurrence or stenosis. 126
Thromboembolic origins were explored via transthoracic/esophageal echocardiography and 127
enhanced cardiac CT scanning during the perioperative period, and the carotid artery was 128
evaluated for the presence of significant stenosis through additional duplex ultrasonography 129
or prior baseline diagnostic CTA that (carotid artery was included in the field of CT scan). In 130
patients with cardiac disorder detected by electrocardiography, echocardiography, and 131
enhanced cardiac CT scanning, ATUE was attributed to cardiac etiology. Holter monitoring to 132
exclude subclinical paroxysmal atrial fibrillation (AF) and thrombophilia test for the patients 133
without a definite mechanism were not generally performed in our series. 134
This was a retrospective analysis, based on a review of patient medical records. If the patients 135
were not able to reach the hospital, anticoagulation status, details of recurrent embolic events 136
and external survival data were obtained by calling patients themselves or their family. 137
Subsequently, we evaluated the demographics and clinical manifestations of the patients on 138
admission including CHA2DS2-VASc score13 in patients with AF, as well as their in-hospital 139
and long-term clinical outcomes post-treatment. Outcomes of interest were prior 140
thromboembolic events at any site, upper-limb amputation, death, and any recurrent 141
thromboembolic events during follow-up. Recurrent thromboembolic events was defined as 142
combined macroembolization in any site and cerebral infarction (possible thromboembolic in 143
nature) during the follow-up. Event-free survival time in acute ATUE was defined as the post-144

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
therapeutic interval during which objective signs of recurrent thromboembolic events were 145
absent. For evaluating basic characteristics and long-term outcomes, patients were stratified 146
as those with (group I) or without (group II) AF. 147
Student's independent t-test was applied for between-group age comparison. Given the 148
potential for skew, group comparison of symptom durations relied on the nonparametric 149
Mann-Whitney U test (also known as the Wilcoxon test for independent measures). The ten 150
categorical variables tested were subjected to chi-square analysis (if sample size was 151
adequate) or Fisher’s exact test (for smaller samplings). Overall and event-free survival rates 152
were estimated by Kaplan-Meier method, and the Log-rank test was used to compare groups. 153
The difference of recurrent embolic events according to CHA2DS2-VASc score in group I 154
was calculated by Cox regression analysis. All calculations relied on standard software (SPSS 155
v20.0; SPSS Inc, Chicago, IL, USA), with statistical significance set at p<0.05. 156
157
RESULTS 158
159
Patient characteristics and thromboembolic sources on admission 160
Average patient age was 70 years (range, 27-95 years), and 26 patients (49%) were male. 161
Group I patients were comparatively older. Among coexisting medical condition, congestive 162
heart failure was more common in group I and current smoker was more prevalent in group II. 163
Gender, duration of symptoms, and other coexisting medical conditions were similar for the 164
two groups (Table I). Median CHA2DS2-VASc score in group I was 5 (range, 2-8). Detailed 165
CHA2DS2-VASc score, median duration of symptoms and common associated comorbidities 166
are summarized in Table 1. 167
At the time of presentation, previous thromboembolic events were suspected by history in 24 168

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
patients (45%). Prior cerebral infarction was likely in 15 patients. A history of 169
thromboembolism in other site was also elicited in remaining nine patients (lower limb, 6; 170
upper limb, 2; superior mesenteric artery [SMA], 1) (Table 1), but prior thromboembolic 171
events in aggregate did not differ by group. 172
Right arm was affected in 39 patients (74%), with left arm affected in the remaining 14 173
patients. The most proximal site of occlusion was axillary artery (18 patients, 34%), followed 174
by brachial artery (33 patients, 62%). Two patients displayed radial artery occlusion (Table 1). 175
Thirty-eight (72%) patients had ATUE of probable cardiac etiology. Among them, emboli 176
were attributable to AF in 34 patients (group I), previous myocardial infarction in 2 patients, 177
and diseased mitral valves in 2 patients (vegetation on mitral valve, 1 patient; mitral valve 178
stenosis, 1 patient). In 15 patients (28%) without detection of cardiac disorders through 179
evaluation, proximal arterial source, between ascending aorta and lesion, was implicated in 180
six patients (thoracic outlet syndrome, 2 patients; previously occluded axillofemoral graft, 2 181
patients; floating thrombus of ascending aorta, 1 patient; subclavian artery aneurysm, 1 182
patient), and vasculitis was held responsible in two patients (both systemic sclerosis). No 183
basis of thromboembolism was identified in the seven remaining patients. Forty-eight 184
subjects underwent cardiac evaluation in search of cardiac thrombus, usually by transthoracic 185
echocardiography (n=40) and/or enhanced cardiac CT (n=18). Transesophageal 186
echocardiography was performed in two patients. Ten (8 cases through echocardiography; 2 187
through CT) of these 48 patients each harbored a thrombus of cardiac chamber (21%; 9 in 188
group I; 1 in group II). 189
190
Early post-therapeutic outcomes 191
Two patients (one in each group) received anticoagulants exclusively for mild symptoms. The 192

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
other 51 were treated initially by surgical thromboembolectomy (n=48) or arterial bypass 193
(n=3) under local (33/51, 65%) or general (35%) anesthesia. 194
Four (8%) of these 51 patients (1 in group I; 3 in group II) suffered re-occlusion of affected 195
arteries during in-hospital stays, necessitating repeat thromboembolectomy. One patient in 196
group I had patency restored after repeat thromboembolectomy at the time of discharge. 197
However, occlusions also recurred in three patients of group II, two of whom received an 198
anticoagulant as sole intervention. The third patient again underwent thromboembolectomy, 199
along with removal of an axillofemoral stump suspected as the thromboembolic source. None 200
of the patients required amputation. Otherwise, symptomatic relief was achieved in 51 201
patients (96%), with the exception of two post-thromboembolectomy re-occlusions after 202
treatment. 203
Within the postoperative period, three patients (5.8%) died. One in group I died from cerebral 204
infarction, and acute myocardial infarction and respiratory failure due to advanced pulmonary 205
tuberculosis was responsible in each patient in group II. 206
207
Long-term outcomes incorporating systemic embolic events 208
Mean follow-up duration was 56.8±62.2 months (median, 29.6 months; range, 1-248 months), 209
during which 19 recurrent thromboembolic events (group I, 17 (89%) in 14 patients; group II, 210
2 in 2 patients) were documented. Specifically, cerebral infarction (7 events), 211
thromboembolism of upper (4 events) and lower (3 events) extremities, and SMA embolism 212
(3 events) were recorded in group I, and each event of cerebral infarction and 213
thromboembolism of upper extremity was recorded in group II (Table 2). Of the eight 214
patients suffering cerebral infarction, seven had undergone carotid artery studies upon 215
admission for ATUE, but significant stenosis at carotid bifurcation was found in only one 216

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
patient of group I (>50% stenosis bilaterally). One patient experiencing recurrent ATUE 71 217
months after initial treatment in group II (previously occluded axillofemoral graft) finally 218
required amputation. There was no significant relationship between the recurrent embolic 219
event and CHA2DS2-VASc score in group I patients (hazard ratio 0.83; 95% confidence 220
interval, 0.54-1.29; p=0.41). 221
Among 14 patients with recurrent embolic events in group I, half of patients were not 222
receiving anticoagulants when first recurrent embolic events took place. Cessation of 223
prophylaxis was arbitrary in each instance, representing independent decisions (without 224
medical advice) in six and one non-restart after a bout of gastrointestinal bleeding. Two 225
patient was given low-molecular-weight heparin during admission and five patients were 226
taking warfarin at the time of recurrent embolic events. Mean INR of these five patients was 227
1.88 (four <2.0 each; maximum of 3.43). 228
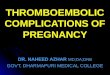
Event-free survival rates after initial therapy were 84% at 1 year, 65% at 3 years, and 58% at 229
5 years for patients overall. In subgroup analysis, respective rates were 77%, 44%, and 44% 230
for group I and 100%, 100%, and 83% for group II (p=0.004) (Fig. 1). 231
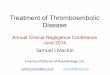
During the follow-up period, 23 patients died and 7 were lost to follow-up. Overall survival 232
rates after initial treatment were 83% at 1 year, 73% at 3 years, and 59% at 5 years (Fig. 2). 233
In subgroup analysis, respective rates were 82%, 69%, and 52% for group I and 84%, 78%, 234
and 70% for group II (p=0.21). Causes of death are indicated in Table 2. 235
236
DISCUSSION 237
Acute limb ischemia is the most common type of vascular emergency, accounting for 238
approximately 30% of such events.14 Acute ATLE is considered particularly serious, carrying 239
high rates of morbidity, amputation (10-15%), and mortality (~10%) by current reports.15-18 In 240

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
contrast, the outcomes of acute ATUE demonstrated lower rates of limb loss (0-3.1%)10,18,19 241
and mortality (~6%).10,14,18 The disparity in amputation rates for upper and lower limb 242
compromise may be explained by a better developed collateral circulation in the arms.20 243
Despite the fact that episodic ATUE is not always limb-threatening, and 244
thromboembolectomy is not an absolute requirement for limb salvage, investigators are still 245
troubled by functional arm deficits, with weakness and/or claudication that may persist after 246
conservative treatment (with or without long-term anticoagulation).21,22 Hence, most vascular 247
surgeons opt for thromboembolectomy as an aggressive measure to preserve function.3,10,23 In 248
our series, two patients received anticoagulants as the sole initial therapy for mild symptoms, 249
and another two patients received anticoagulants only for early occlusion after 250
thromboembolectomy. None of these four patients required amputation, possibly due to 251
sufficient collateral blood flow and lesser demands of upper (vs. lower) limb muscle mass. 252
The relatively lower mortality rate of acute ATUE may be influenced by several factors. 253
Compared with more muscular lower limbs, reperfusion injury of the upper extremities (after 254
revascularization) expectedly is less extreme. Furthermore, upper extremity occlusions are 255
more likely to be embolic in nature, rather than a consequence thrombosis at points of pre-256
existing arterial stenosis. Some researchers also note that atherosclerotic narrowing of the 257
brachial artery seldom occurs, and associated in situ thrombosis rarely presents 258
acutely.12,20,24,25 As such, acute ATUE is usually amenable to thromboembolectomy by 259
balloon catheter under local anesthesia, without the need for major vascular bypass surgery. 260
Ueberrueck et al.14 have also emphasized that in-hospital mortality is usually a function of 261
comorbidities and cerebral or visceral embolism, rather than procedure-related complications. 262
In our series, 94% of operated patients were treated initially by thromboembolectomy via 263
brachial approach, and 65% of these were done under local anesthesia. Our in-hospital 264

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
mortality rate of 5.8%, which we believe is comparable to other studies, was due to events 265
from underlying comorbidities rather than procedure-related complications. 266
Few reports have chronicled long-term outcomes of ATUE that encompass recurrent 267
thromboembolic events. However, a common finding in earlier efforts is that patients 268
undergoing upper limb thromboembolectomy were at increased risk of stroke and death, 269
compared with the population at-large.12,18,19,26 Andersen et al.19 studied a cohort (N=1377) 270
recruited nationwide over more than a decade (1990-2002), each subject status post-271
thromboembolectomy of upper extremity. By their account, 237 patients (19.1%) experienced 272
first-ever strokes after thromboembolectomy, and 20 of those patients were hospitalized for 273
the procedure when the stroke occurred. The relative risk of stroke was determined as 3.3-274
fold in males and 5-fold in females, compared with the general population. Unfortunately, no 275
other thromboembolic events were described and causes of death during the follow-up were 276
not specified. Magishi et al.18 reported event-free survival rates of 74% at 1 year and 27% at 277
3 years, with respective cumulative actuarial survival rates of 95% and 61%. In addition, 278
cerebrovascular disease was the primary comorbidity at admission and primary recurrent 279
thromboembolic pattern after operation in their series, although this study lacked 280
corroborating carotid arterial evaluations.18 281
In our patients, recurrent embolic events after ATUE were high, especially in patients with AF 282
where 1-year, 3-year, and 5-year event-free rates were 77%, 44%, 44%, respectively. Most 283
recurrent thromboembolic events involved cerebral infarction. There is no real evidence that 284
these strokes were embolic in nature and of cardiac origin, so one cannot assume a causal 285
relationship with index episodes of ATUE. However, in six of the seven affected, no 286
significant carotid arterial stenosis was detected at first presentation, which may have some 287
bearing in this context. 288

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
It is well-known that without anticoagulant treatment, the risk of ischemic stroke is far higher 289
than the risk of intracranial bleeding with treatment.27,28 Moreover, in our subset of high-risk 290
patients with a history of thromboembolism and atrial fibrillation, long-term anticoagulation 291
is sanctioned to prevent recurrent embolism.29 Despite a clear mandate for anticoagulation in 292
patients with AF, many such patients are not receiving appropriate treatment.18,19,30 In our 293
series, the median CHA2DS2-VASc score was 5 and all of the patients were comprised in 294
high risk group. However, half of our patients with AF were not taking anticoagulants at the 295
times thromboembolic recurrences took place, and in anticoagulated patients suffering 296
recurrences, recommended therapeutic levels were not reached. Unfortunately, many patients 297
arbitrarily discontinued anticoagulant therapy. Follow-up monitoring of long-term 298
anticoagulation admittedly is difficult, and elderly patients who are asymptomatic after 299
treatment are inclined to become noncompliant. 300
The reported 5-year survival rate after thromboembolectomy of upper extremity has been 301
ranged from 37% to 61% and the mechanism for high long-term mortaliry was speculated 302
that most of patients with ATUE were old and displayed with multiple comorbidities.10,12,18 303
Our cohort was comparable to other studies. Importantly, the cause of mortality in patients 304
with AF was primarily due to thromboembolic events, such as cerebral infarction and SMA 305
embolism. Although Licht et al.12 followed 148 patients with acute upper limb ischemia, 306
reporting no significant survival benefit from anticoagulant therapy beyond hospital stays, 307
they failed to address late outcomes in terms of embolic events and anticoagulation status. 308
Alternatively, Mills and Porter31 found that recurrent embolization may be preventable with 309
routine anticoagulation. Our data likewise underscore that regular follow-up with adequate 310
anticoagulation is critical, especially in instances of AF. Therefore, patients should be 311
educated on these principles and their potential to impact long-term outcomes. 312

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
The major limitation of this study is its retrospective nature and the small patient sampling 313
that was monitored over long a period of time. A significant number of subjects (total of 314
seven) progressively were lost to follow-up, and it was difficult to track INR values of 315
patients who were event-free, many of whom were seen at other facilities. This particular 316
limitation prohibits us from assessing the effect of adequate anticoagulation in 317
thromboembolic recurrences, and also there is a possibility to underestimate the actual 318
recurrent events due to the incomplete follow-up. In addition, although the majority of our 319
patients affected cerebral infarction during follow-up did not have significant carotid stenosis 320
at presentation, it may be difficult to have confidence that these events is mechanistically 321
related (from the same source/cause) to the index episodes of acute ATUE. 322
323
CONCLUSION 324
In this study, surgical treatment of acute ATUE was largely successful. However, the high 325
rates of thromboembolic recurrence and poor compliance we observed, especially in patients 326
with AF, indicate a need for patient education and adequate long-term anticoagulation as 327
prophylactic measure. 328
329
REFERENCES 330
1. Stonebridge PA, Clason AE, Duncan AJ, et al. Acute ischaemia of the upper limb 331
compared with acute lower limb ischaemia; a 5-year review. Br J Surg 1989;76:515-6. 332
2. Pemberton M, Varty K, Nydahl S, et al. The surgical management of acute limb 333
ischaemia due to native vessel occlusion. Eur J Vasc Endovasc Surg 1999;17:72-6. 334
3. Galbraith K, Collin J, Morris PJ, et al. Recent experience with arterial embolism of the 335
limbs in a vascular unit. Ann R Coll Surg Engl 1985;67:30-3. 336

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
4. Baguneid M, Dodd D, Fulford P, et al. Management of acute nontraumatic upper limb 337
ischemia. Angiology 1999;50:715-20. 338
5. Kim SK, Kwak HS, Chung GH, et al. Acute upper limb ischemia due to cardiac origin 339
thromboembolism: the usefulness of percutaneous aspiration thromboembolectomy via a 340
transbrachial approach. Korean J Radiol 2011;12:595-601. 341
6. Cejna M, Salomonowitz E, Wohlschlager H, et al. rt-PA thrombolysis in acute 342
thromboembolic upper-extremity arterial occlusion. Cardiovasc Intervent Radiol 343
2001;24:218-23. 344
7. Campbell WB, Ridler BM, Szymanska TH. Vascular surgical society of great britain and 345
ireland: two-year follow-up after acute thromboembolic lower limb ischaemia: the 346
importance of continuing warfarin treatment. Br J Surg 1999;86:707. 347
8. Aune S, Trippestad A. Operative mortality and long-term survival of patients operated on 348
for acute lower limb ischaemia. Eur J Vasc Endovasc Surg 1998;15:143-6. 349
9. Zaraca F, Ponzoni A, Sbraga P, et al. Factors affecting long-term outcomes after 350
thromboembolectomy for acute lower limb ischemia. Minerva Chir 2012;67:49-57. 351
10. Hernandez-Richter T, Angele MK, Helmberger T, et al. Acute ischemia of the upper 352
extremity: long-term results following thrombembolectomy with the Fogarty catheter. 353
Langenbecks Arch Surg 2001;386:261-6. 354
11. Pentti J, Salenius JP, Kuukasjarvi P, et al. Outcome of surgical treatment in acute upper 355
limb ischaemia. Ann Chir Gynaecol 1995;84:25-8. 356
12. Licht PB, Balezantis T, Wolff B, et al. Long-term outcome following 357
thrombembolectomy in the upper extremity. Eur J Vasc Endovasc Surg 2004;28:508-12. 358
13. Lip GY, Nieuwlaat R, Pisters R, et al. Refining clinical risk stratification for predicting 359
stroke and thromboembolism in atrial fibrillation using a novel risk factor-based 360

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
approach: the euro heart survey on atrial fibrillation. Chest 2010;137:263-72. 361
14. Ueberrueck T, Marusch F, Schmidt H, et al. Risk factors and management of arterial 362
emboli of the upper and lower extremities. J Cardiovasc Surg (Torino) 2007;48:181-6. 363
15. Henke PK. Contemporary management of acute limb ischemia: factors associated with 364
amputation and in-hospital mortality. Semin Vasc Surg 2009;22:34-40. 365
16. Ender Topal A, Nesimi Eren M, Celik Y. Management of non-traumatic acute limb 366
ischemia and predictors of outcome in 270 thrombembolectomy cases. Int Angiol 367
2011;30:172-80. 368
17. Eliason JL, Wainess RM, Proctor MC, et al. A national and single institutional experience 369
in the contemporary treatment of acute lower extremity ischemia. Ann Surg 370
2003;238:382-9. 371
18. Magishi K, Izumi Y, Shimizu N. Short- and long-term outcomes of acute upper extremity 372
arterial thromboembolism. Ann Thorac Cardiovasc Surg 2010;16:31-4. 373
19. Andersen LV, Mortensen LS, Lindholt JS, et al. Upper-limb thrombo-embolectomy: 374
national cohort study in Denmark. Eur J Vasc Endovasc Surg 2010;40:628-34. 375
20. Shindo S, Kojima A, Ishimoto T, et al. Arterial reconstruction in the upper extremities. 376
Vascular 2004;12:57-61. 377
21. Savelyev VS, Zatevakhin, II, Stepanov NV. Artery embolism of the upper limbs. Surgery 378
1977;81:367-75. 379
22. Ricotta JJ, Scudder PA, McAndrew JA, et al. Management of acute ischemia of the upper 380
extremity. Am J Surg 1983;145:661-6. 381
23. Eyers P, Earnshaw JJ. Acute non-traumatic arm ischaemia. Br J Surg 1998;85:1340-6. 382
24. Sorensen KE, Kristensen IB, Celermajer DS. Atherosclerosis in the human brachial 383
artery. J Am Coll Cardiol 1997;29:318-22. 384

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
17
25. Zeiher AM, Schachinger V, Minners J. Long-term cigarette smoking impairs 385
endothelium-dependent coronary arterial vasodilator function. Circulation 1995;92:1094-386
100. 387
26. Andersen LV, Lip GY, Lindholt JS, et al. Upper limb arterial thromboembolism: a 388
systematic review on incidence, risk factors, and prognosis, including a meta-analysis of 389
risk-modifying drugs. J Thromb Haemost 2013;11:836-44. 390
27. Friberg L, Rosenqvist M, Lip GY. Net clinical benefit of warfarin in patients with atrial 391
fibrillation: a report from the Swedish atrial fibrillation cohort study. Circulation 392
2012;125:2298-307. 393
28. Andersen LV, Mortensen LS, Lip GY, et al. Atrial fibrillation and upper limb 394
thromboembolectomy: a national cohort study. J Thromb Haemost 2011;9:1738-43. 395
29. Singer DE, Albers GW, Dalen JE, et al. Antithrombotic therapy in atrial fibrillation: 396
American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th 397
Edition). Chest 2008;133(6 Suppl):546S-92S. 398
30. Gossage JA, Ali T, Chambers J, et al. Peripheral arterial embolism: prevalence, outcome, 399
and the role of echocardiography in management. Vasc Endovascular Surg 2006;40:280-400
6. 401
31. Mills JL, Porter JM. Basic data related to clinical decision-making in acute limb 402
ischemia. Ann Vasc Surg 1991;5:96-8. 403
404
405
406
407
408

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
18
Table 1. Characteristics and potential sources of acute arterial thromboembolism of upper 409
extremity 410
Characteristics Group I (n=34) Group II (n=19) P value
Age, mean (range) 73.9 (58-95) 62.9 (27-85) 0.01
Male gender 14 (41%) 12 (63%) 0.13
Symptom duration, median hour (range) 7.5 (1-240) 16.0 (2-336) 0.09
Coexisting medical condition
Hypertension 25 (74%) 10 (53%) 0.12
Smoking (current smoker) 8 (24%) 11 (58%) 0.01
Diabetes mellitus 10 (29%) 2 (11%) 0.12
Congestive heart failure 12 (35%) 2 (11%) 0.05
Ischemic heart disease 5 (15%) 4 (21%) 0.56
Renal insufficiency (s-Cr>1.5mg/dL) 2 (6%) 0 0.28
Affected side 0.20
Right side 27 12
Left side 7 7
Proximal occlusion site 0.10
Axillary artery 9 9
Brachial artery 25 9
Radial or ulnar artery 2
Suspected causes of thromboembolism
Atrial fibrillation 34
Other cardiac causes 4
Proximal artery 6
Vasculitis 2
Unknown 7
Previous thromboembolic events 17 (50%) 7 (37%) 0.36
Cerebral infarction 11 4
Embolism of lower extremity 6 0
Embolism of upper extremity 0 2
Embolism of SMA 0 1
s-Cr, serum creatinine; SMA, superior mesenteric artery 411
412
413
414

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
19
Table 2. Thromboembolic events and causes of death in the aftermath of acute ATUE 415
Group I (n=34) Group II (n=19)
Recurrent embolic events 17* 2
Cerebral infarction 7 † 1
‡
Embolism of lower extremity 4 0
Embolism of upper extremity 3 1
Embolism of SMA 3 0
Under anticoagulation at recurrence 7 0
Causes of death
Cerebral infarction 4 1
Embolism of SMA 2 0
Myocardial infarction 2 1
Acute renal failure 1 0
Trauma 1 0
Pneumonia
Respiratory failure
1
0
1
1
Malignancy 2 1
Unknown 3 2
ATUE, arterial thromboembolism of upper extremity; SMA, superior mesenteric artery 416
* Three patients suffered multiple recurrent arterial embolizations. 417
† One of six patients showed >50% stenosis of carotid bifurcation bilaterally upon admission 418
for acute ATUE. 419
‡ One patient showed no significant carotid stenosis upon admission for acute ATUE. 420
421
422
423
424
425
426

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
20
FIGURE LEGENDS 427
428
Figure 1. Event-free rates after initial therapy by group. Respective rates in patient subset 429
with atrial fibrillation (AF) marked by significant increases relative to patients without AF 430
(p=0.004). 431
432
Figure 2. Overall survival rates after treatment by group. Kaplan-Meier estimates in patient 433
subset with atrial fibrillation (AF) and without AF were similar (p=0.21). 434

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT