Embed Size (px)
Citation preview

J Clin Pathol 1983;36: 1256-1263
The exanthem of Ross River virus infection:histology, location of virus antigen and nature ofinflammatory infiltrateJ ROBERT E FRASER,* V MALA RATNAMOHAN,* JOHN PG DOWLING,t GAVIN JBECKER,t GEORGE A VARIGOS*
From the University ofMelbourne Department of *Medicine, and the Departments of tAnatomical Pathologyand tNephrology, The Royal Melbourne Hospital, Victoria, Australia
SUMMARY The exanthem of epidemic polyarthritis, a disease caused by Ross River (RR) virus,was examined three days after onset of the common erythematous and the rare purpuric forms ofthe eruption. The dermis showed a light perivascular infiltrate of mononuclear cells in both, withextravasation of erythrocytes in the latter. No immunoglobulins (IgM, IgG, IgA) or complementcomponents (Clq, C3) were detected. Most of the infiltrating cells were T lymphocytes of the Tsuppressor-cytotoxic class. Their perivascular location, the scarcity of other lymphocytes orphagocytes, and rapid resolution of the rash indicated that the T lymphocytes were responsiblefor cytotoxic destruction of virus-infected cells. A few monocyte-macrophage cells wereidentified in the perivascular infiltrate. RR virus antigen was found in the basal epidermal andeccrine duct epithelial cells of both types of lesion and in the perivascular zone of the erythemat-ous lesion, but appeared to have been eliminated from this region in the purpuric lesion. It issuggested that secondary effects of the T-cytotoxic reaction on nearby capillaries are responsiblefor erythema, oedema and purpura in the exanthem.
Many virus infections merely result in immunitywith trivial symptoms or none at all, and the levels ofspecific circulating antibody often show little rela-tion to the outcome. The nature of the cellularresponse to virus infection has therefore beenclosely scrutinised both for its part in elimination ofinfection and for its possible contribution to theoccurrence of disease. Much of this work has ofnecessity been limited to studies in vitro or toexperimental animal infections. With the develop-ment of monoclonal antibodies and otherimmunological techniques, the proportions of cir-culating T and B lymphocytes and T cell subsetshave been determined in some human virus dis-eases.'- The infiltrating cells in tissue lesions havebeen similarly examined in inflammatory diseases ofundetermined nature such as rheumatoid arthritis,4 5in skin disease,67 in leprosy8 and in chronic hepatitisassociated with hepatitis B antigenaemia9 but com-parable studies in acute human virus diseases havenot been reported at the time of writing.Epidemic polyarthritis is the major clinical syn-
drome arising from infection with RR virus, a
Accepted for publication 6 June 1983
mosquito-borne alphavirus. About two-thirds of thepatients develop a rash, which is usuallymaculopapular and resolves in 5-10 days. It some-times includes purpuric lesions and small vesicles,'0but these are rarely numerous. The rheumatic man-ifestations are both articular and extra-articular, andcan persist as long as three years. The virus isendemic in Australia and the South Pacific, and isclassified with rubella in the Togaviridae. Both vir-uses are of particular interest for their capacity toinduce rheumatic disease.The only cytopathology of the disease reported to
date is that of the synovial exudate, which is predo-minantly mononuclear in both the acute and chronicphases." 12 We describe here the pathological fea-tures of the rash in its usual form at the height of itsdevelopment, and in another example notable forthe exceptionally high proportion and extent of pur-puric lesions.
Material and methods
SOURCES OF TISSUECase IErythematous papular lesions were obtained from a
1256
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from

Exanthem of Ross River virus infection
man of 39 yr who had worked for ten months in anarea of endemic risk for RR virus infection but hadbeen well until the onset of polyarthritis with Achil-les tendonitis six days before skin biopsy. An irrit-able maculopapular rash, which faded on pressure,appeared three days before biopsy and spread toinvolve the whole of the trunk and limbs, includingpalms and soles, until it was nearly confluent at thetime of examination. Clinical findings were consis-tent with epidemic polyarthritis. Appropriate testsshowed no evidence of heterophile antibodies,recent /8-haemolytic streptococcal infection or ofrenal or hepatic dysfunction. Peripheral bloodshowed normal haemoglobin, erythrocyte sedimen-tation rate of 7 mm/h (Westergren), and aleucocyte count of 4.4 x 109/l with some atypicallymphocytes but an otherwise normal pattern.Diagnosis was confirmed by a rise in serumhaemagglutination-inhibition (HI) antibody titre toRR virus from 1/20 on the first day of illness to1/160 two weeks later. The rash resolved withinthree days. The patient's recovery was complete intwo weeks, and he had suffered no relapses whenreviewed 8 months later.
Case 2Purpuric papules were excised from a woman of 33yr who developed rash and polyarthritis with swel-ling of ankles and digital joints six days after leavingregions of high RR virus prevalence. The rash con-sisted of red macules and papules scantily distri-buted on the arms, wrists, palms, fingers, trunk, feetand soles, and much more numerous on the shinsand buttocks. Some in the latter site showed smallvesicles. The majority did not blanch on pressure,and were 1-2 mm in diameter, with a few to 5 mm.Face and oral mucosa were spared. There were noabdominal symptoms. Urine analysis including cellcounts was normal. Peripheral blood showed normalhaemoglobin, leucocytes (5.2 x 109/1) and plateletcount (204 x 1012/1). Erythrocyte sedimentationrate was 41 mm/h (Westergren). Other diagnos-tic tests cited in the first patient, together withserological tests for hepatitis A and B, IgMrheumatoid factors, tissue antinuclear factor andDNA antibodies were negative. Skin biopsies oflesions identified by the patient as recent were donethree days after onset. The last of the purpura hadfaded in two weeks. Rheumatic symptoms and signshad almost completely subsided three weeks afteronset, and the erythrocyte sedimentation rate hadreturned to normal (9 mm/h). Serum HI anti-body titres against RR virus were 1/40 on the thirdday of illness, and 1/20 after three weeks. Theselevels are significant but unusually low for the acutephase of the disease, but both samples were however
1257
shown by ELISA to contain specific IgM antibodies(courtesy of Dr J Aaskov).With local anaesthesia, lesions were removed
from the trunk in the first patient and from the palmand fingers in the second, by excision through thedeeper layers of the dermis with a trephine of 4 mmdiameter and a fine scalpel. Sections were immedi-ately frozen at - 70°C for immunochemical staining,fixed overnight in buffered formalin for routine his-tology, and fixed in 2-5% glutaraldehyde in 0-1 Mcacodylate buffer, pH 7.3, for electron microscopy.Cultures for virus were prepared from frozen andfresh tissue.
HISTOLOGYParaffin-embedded sections were stained withhaematoxylin and eosin, and with orcein-Giemsa.For electron microscopy, tissue was dehydrated inacetone and embedded in Spurr's resin after post-fixation in 2% OSO4 for 1 h. Sections of 800 nmwere stained with 2% uranyl nitrate and Reynold'snitrate.
ANTISERANormal rabbit serum and rabbit antiserum againstthe prototype strain of RR virus (T48; neutralisingtitre 1/250) were absorbed in two steps (2 h at 37°Cand 16 h at 4°C) with 6 mg of dried defatted humanskin powder per ml, and diluted 1/20. Sources anddilutions of fluorescein-conjugated sheep antiserawere as follows: antihuman IgM (1/15), IgA (1/15),IgG (1/30), C3 (1/15) Wellcome Aust Ltd,Melbourne and antirabbit IgG (1/20), fibrinogen(1/20) and Clq (1/15), Boehringer-Hoechst,Melbourne.
FLUORESCENT STAININGFrozen sections (6 ,um) were airdried, incubatedwith serum diluted in phosphate-buffered saline (pH7.4) for 30 min at 37°C and washed for 15 min inthree changes of buffer between successive steps andbefore mounting in buffered glycerol medium (pH8-6). Positive and negative controls for the specificantisera consisted of RR virus-infected and unin-fected human and insect cell cultures, and concur-rent biopsy specimens from various skin and renaldiseases (non-specific dermatitis, bullous pem-phigoid, pemphigus vulgaris, lupus erythematosus,IgA-, membranous and post-infectivenephropathies). Preparations were examinedwith a Zeiss Photomicroscope II fitted with exciterfilter BP450-490 and barrier filter LP520.
IDENTIFICATION OF CELLULAR INFILTRATESFrozen sections (6 ,um) were fixed inparaformaldehyde-lysine-periodate (PLP) and
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from

Fraser, Ratnamohan, Dowling, Becker, Varigos
Table 1 Immunofluorescent and immunoperoxidase staining in skin
Antibody Specifrity Site ofpositive reaction Ccm, arative numbers ofpositivecells
Case I Case 2
PHMI All leucocytes'3 Dermis: perivascular andscattered ++++ ND
OKT3 T lymphocytes5 Dermis: perivascular + + 0OKT4 T (inducer/helper)'6 Dermis: occasional cells in some
perivascular zones +/ 0OKT8 T (cytotoxic/suppressor)'' Dermis: perivascular +++ +++FMC32 Monocyte-macrophage"l Dennis: perivascular and
scattered + +/RRVt Ross River virus Basal epidermal cells ++ + +
Duct epithelial cells + +Dermis, penvascular +++ 0
OKT6 Langerhans cells Epidermis only + +FMC1O Granulocytes20 Dermis: probably mast cells Very few NDOKT10 Natural killer cells2' 0 NDVarioust IgM, IgG, IgA, C3, Clq, fibrin - 0 0
*The degree of cellular infiltration was varied and generally light.The grades compare the proportions of reactive cells.The smaller lesion in case 2 provided insufficient material for all reagents; ND = not done.
tPolyclonal antisera.
stained by a four-layer unlabelled peroxidase tech-nique'3 comprising sequential incubation withmouse monoclonal antibody, rabbit antimouse anti-body, excess sheep antirabbit antibody and pre-formed rabbit peroxidase-antiperoxidase com-plexes.
Tissue-bound peroxidase was then detected byincubation with diaminobenzidine (DAB) andH202. Endogenous peroxidase activity was blockedby the addition of NaN3 (0-3%) to the DAB solu-tion.'3 Monoclonal antibodies employed and theirspecificities are shown in Table 1.Macrophages were also identified histochemically
by staining for,8-glucuronidase.22
ATTEMPTED GROWTH OF VIRUSApproximately 6 mm3 of skin was mechanicallyhomogenised in 1 ml of Eagle's minimum essentialmedium. Confluent test tube cultures of Aedesalbopictus cells, C6/36 strain, were inoculated with0*1 ml of the homogenate and incubated at 30°C inappropriate growth medium. At three-day intervals,replicate cultures were frozen and thawed twicebefore passage into fresh C6/36 cultures. Supemat-ant was inoculated into Vero cell monolayers, whichwere incubated at 37°C and observed for cytopathiceffects. Cells from inoculated and control C6/36 cul-tures were also examined at each passage by theindirect immunofluorescence technique. In the sec-ond case, peripheral blood buffy coat cells and cul-ture medium from a primary culture of the skin werealso used to inoculate the insect cell cultures. Cul-tures inoculated with 0- 1 ml aliquots of the patient'sacute-phase serum, diluted 1/10, were treated simi-larly.
Results
LIGHT MICROSCOPYThe sole changes were slight perivascular oedemaand leucocytic infiltration in the erythematouslesions of case I with a light extravasation of ery-throcytes in the purpuric lesions of case 2 (Fig. 1).The intensity of the infiltrates varied in different reg-ions of the specimens, but the cells were consistentlymononuclear. The epidermis was normal except for,,clear" cells in the lower prickle cell layer, attri-buted to the anaesthetic. No platelet aggregation,thrombosis, fibrin deposition, or conspicuousendothelial damage was seen.
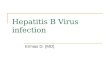
IMMUNOFLUORESCENT STAININGMinimal random punctate staining occurred withanti-albumin antiserum. No staining was seen withantisera against IgM, IgG, IgA, fibrinogen, C3 orClq. Specific staining for RR virus antigen (Fig. 2)was detected in the basal epidermal layer and ineccrine duct epithelial cells of both cases. Antigenwas also prominent in the penvascular regions in theerythematous but not in the purpuric lesionalthough the OKT8+ lymphocytes were mostnumerous in this region of both types of lesion.
ELECTRON MICROSCOPYIn case 1, the perivascular infiltrate included typicallymphocytes, moderately vacuolated cells ofhistiocyte-macrophage type and slightly more cellsof indeterminate class with short filipodia, and a lit-tle vacuolation (Fig. 3). The endothelial cells werenormal. In case 2, the infiltrating cells were mainlylymphocytes. Small vessels showed swelling of
1258
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from

Exanthem of Ross River virus infection 1259
V~~~~~~~~0~~~~~~~
J;~~~~~V
41Pb
Vs-
q N~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~q
iIh..:l,-C,..*\s-'.,_ #sJf A ,
;;;&' r iT. ! jpWb;-'VL)-^ m
* -'-AW -.
a wF.f tig b d
tz,- N Sf/,.At *
,.''o * *_','as,q>;
¢,,,..ii,
S- - 9 ne+/;S*S ".t t-
o~~~~ ~ ~ ~ ~~~~ ~Fg 2 Loaio ofviu antge byinirc
immunofikorescence. (a) Case 1. Antigen was detected inFig. 1 (a) Case 1. Light perivascular collections of cellular connective tissue surrounding superficial dermalmononuclear cells in superficial dermis. Elastin fibres stained' vessels, within the basal layers ofthe epidermis and eccrineblack. Orcein-Giernsa stain. Original magnification x 160. duct epithelium (E). Magnification x 250.(b) Case 2. Similar perivascular pattern ofmononuclear (b) Case 2. Antigen was detected in the basal layers of thecells, with extravasation oferythrocytes (arrow) into epidermnis and in eccrine duct-epithelium, but not in theoedematous dermis. Haematoxylin and eosin stain. Original perivascular tissue. Magnification x 250.magnifiation x 160.
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from

1260
i ,- -W*A.
..'
j~L.
qZ J
-. s
Fig. 3 Mixed collection oflymphocytes (L) and hisiiocytes(H) adjacent to vessel wall (V). Case 1. Electronmicroscopy. Magnifration x 3600.
endothelial cytoplasm and thickening of the base-ment membrane, but no deposition of fibrin. Novirus particles were found in either. TypicalLangerhans cells with Birbeck granules wereidentified in both cases, but only in the epidermis.
IDENTIFICATION OF CELLS WITH MONOCLONALREAGENTSIn the erythematous lesion (case 1), most of theinfiltrating cells reacted with the pan-T lymphocyteantibody, OKT3, and with the reagent for commonleucocyte antigen, PHM1. In the perivascularinfiltrates, small numbers of cells reacted with themonocyte-macrophage reagent, FMC32. The dis-tribution of f8-glucuronidase activity was similar.The most numerous cells in this region were
OKT8-positive. Very few were OKT4-positive (Fig.4). Only two granulocytes were identified in one sec-tion with FMC10 antibody. A normal density ofLangerhans cells was found in the lower and mid-spinous layers of epidermis with OKT6, but none
was detected in the dermis. No cells reacted withOKT10. Single dermal cells which stained withPHM1 and FMC32 outside the perivascular regionwere considered to be normal tissue histiocytes.
Examination of the smaller purpuric lesion was
limited to selected reagents. The cellular infiltrateswere almost entirely OKT8-positive, and concen-
Fraser, Ratnamohan, Dowling, Becker, Varigos
trated in the perivascular zones as in the first case.There were two conspicuous differences: mac-rophages were distinctly scarce, and the lympho-cytes did not react with OKT3.
In view of the irregular cell distribution and cleardistinctions observed, the results are summarised ingradeg rather than proportional counts (Table 1).
VIRUS CULTUREAll inoculated cultures were treated in a similarmanner. Growth medium from Aedes albopictus cellcultures at the first, second, fourth, and seventh pas-sages induced no cytopathic effects in Vero cell cul-tures. No virus antigen was detected in the Aedesalbopictus cells at the fifth, ninth and eleventh pas-sages.
Discussion
Opportunities for histological study of the skin innon-fatal exanthematous infections have beenunderstandably few. The normal epidermis, lightperivascular mononuclear cell infiltrate and slightoedema found in this study were identical with thechanges described in dengue fever,23 measles24 andinfectious mononucleosis.25 The cellular reactionwas remarkably slight in contrast with the erythema.It was nevertheless similar in nature to that observedin the synovial effusions of epidemic polyarthritis,where intracellular virus antigen is easily detected inthe first few days, no other elements of immunecomplex have been found, and the cells are almostentirely mononuclear."I 12 Monocytes and mac-rophages are, however, more numerous than lym-phocytes in the early effusions. Vasodilation, themajor clinical feature of this kind of rash, was obs-cured in the section by blanching after anaestheticinfiltration and retraction of the excised specimen.Despite the clinical similarity to Henoch-Schonleindisease in the second case, the characteristic his-tological features of this disease were entirely lack-ing.The participating cells were characterised by
monoclonal antibodies as T lymphocytes and cells ofthe monocyte-macrophage class, with few granulo-cytes and no B lymphocytes or other cells bearingsurface immunoglobulin. The most conspicuousfindings were the predominance of the OKT8 andthe scarcity of the OKT4 phenotypes. The formerhave been shown in vitro mainly to suppress activa-tion of B lymphocyte immunoglobulin synthesis,which requires OKT4 cell cooperation, and toexhibit alloantigen-specific lymphocytotoxic-ity.26 27 28 Cloning of alloantigen-activated T lym-phocytes has shown that OKT8+ cells can alterna-tively manifest the less specific "natural killer" (NK)
i Ar'
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from

Exanthem of Ross River virus infection
* ,,
/14se > Vt
'CI'v
..¢..~*4:>. 4
at
I-L
-
4.W
*
.
,'
Ap
S .1. f-,
* ,, s
b
.*
o. .* ;.1'.I . b.kII. -i.
4.i*3aa"i4
*'JF \~~~~~~~~~~1
a; ;_
._- '4Wita#b
~~ ~ ~ ~ ~ ~ ~ W
Fig. 4 Sections stained by monoclonal antibodies. Case 1. (a) Control preparation with unreactivemonoclonal cell culture medium. Brown pigment is seen only as melanin in the epidermis. Magnificationx 250. (b) FMC32 antibody against monocytes and macrophages. Brown peroxidase staining in dermalperivascular cells, and scattered through dermis. Magnification x 250. (c) OKT4 antibody against Thelperlinducer lymphocytes. Light background staining, but no positive staining in cellular perivasculararea. Clear area caused by separation artefact. Magnification x 400. (d) OKT8 antibody against Tcytotoxiclsuppressor cells. Strong peroxidase staining in dermal cells round small vessels. Larger clearareas are artefacts. Magnification x 400.
<'S..,
1261
fo a
-¼rA 1
S.I
e7i
. .) ..p *1 t
a
.. '..
-* 0_ r
I_
_e
Al
IL.
*0*%
.6
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from

1262
cell type of cytotoxicity,29 which is an early cellularresponse to alphavirus and flavivirus infection inmice.3031 No OKT10+ cells were found, but only62% of human NK cells identified as large granularlymphocytes in peripheral blood are OKT1O+,whereas another 20% are OKT8+, OKT3-.21 Thelatter pattern was seen in the second case, but itmight also be explained by technical factors8 or byloss of the pan-T lymphocyte marker in the courseof the tissue reaction. These patients recovered fromall aspects of their illness with unusual rapidity.Since the occurrence and intensity of symptomsafter RR virus infection show no relation to anti-body levels, it seems likely that the OKT8+ lympho-cytes were responsible for the cytotoxic eliminationof virus-infected cells, whether by antigen-specificor non-specific mechanisms.The pathogenesis of virus exanthems is varied and
still lacking direct evidence in many respects. T cellparticipation in measles is implied by the absence ofrash in patients with T cell deficiency.32 In rubella,cultivable virus has been found equally commonly inthe rash and in unaffected skin, and in the skin of apatient with no rash at all.33 The present evidenceindicates that, at least in RR virus disease, immunecomplexes seem to play little part and cytotoxic Tlymphocytes are paramount. The cell reaction wasessentially similar in both types of lesions. Throm-bocytopenia or disseminated intravascular coagula-tion can be discounted as a cause for the purpura.Virus antigen must have reached the epithelial cellsfrom the blood vessels, and was found in theperivascular zone of the erythematous lesion but notof the purpuric one although T cells had congre-gated in the corresponding region of both. It istherefore reasonable to conclude that virus-infectedperivascular cells had been eliminated from the pur-puric lesion. The erythema, oedema and purpura aremost likely to reflect the degree of vascular distur-bance induced by soluble products of the surround-ing cytotoxic reaction rather than lodgement of virusor immune complex in the vascular endothelium.
Virus was not located by electron microscopy, orgrown in culture. However, detection of virus byelectron microscopy requires high concentration,and failure to grow virus in an appropriate cell line34might have resulted from dilution of the inoculum (5x 10'), incomplete disruption of dermal fibres orprior damage in situ. The location of virus outsidethe vessels rather than on endothelium is bestexplained by secondary growth of virus in perivascu-lar dermal cells and spread to epithelium after theviraemic phase of infection. RR virus grows well inprimary human synovial cell cultures (Cunninghamand Fraser, unpublished observations 1980) and inearly-passage human synovial lines of fibroblast type
Fraser, Ratnamohan, Dowling, Becker, Varigos
(Ratnamohan and Fraser, personal observations1983) and could infect the analogous histiocytes andfibroblasts in the skin.Apart from the forms described, more persistent
nodular and plaque-like lesions, and macules lastingmore than 30 days have been observed in RR virusdisease and the rheumatic effects often persist orrelapse for months or years (personal observations).A variety of cellular reactions might therefore beexpected, including perhaps something akin to thepredominance of OKT4+ (inducer-helper) lympho-cytes in rheumatoid lesions.4 5 Preliminary studies ofthe synovial exudate suggest that this may be so(Fraser and Becker, unpublished observations1983). It remains to be seen whether lymphocytepatterns can be related to the tissues involved, orpredict or mark the onset of chronicity. It may bepossible, by correlation with the varied course of theillness, to infer the functional significance of the sev-eral monoclonal phenotypes in this disease, which isone of the most persistent forms of virus-inducedarthritis.
We are grateful to the patients for their cooperation.The monoclonal antibodies, FMC 10 and 32 werekindly provided by Dr H Zola, PHM1 by Dr RAtkins and RR virus antiserum by Dr J Aaskov.
Sources of support:The Rheumatism and Arthritis Association of Vic-toria. The Victor Hurley Medical Research Fund.
References
'Crawford DH, Brickell P, Tidman N, McConnell I, HoffbrandAV, Janossy G. Increased numbers of cells with suppressor Tcell phenotype in the peripheral blood of patients with infecti-ous mononucleosis. Clin Exp Immunol 1981;43:291-7.
2 De Waele M, Thielemans C, Van Camp BKG. Characterizationof immunoregulatory T cells in EBV-induced infectiousmononucleosis by monoclonal antibodies. N Engl J Med1981;304:460-2.
De Waele M, Thielemans C, Van Camp B. Immunoregulatory Tcells in mononucleosis and toxoplasmosis. N Engl J Med1981 ;305:228.
4 Janossy G, Duke 0, Poulter LW, Panayi G, Bofill M, GoldsteinG. Rheumatoid arthritis: A disease of T-lymphocyte/macrophage immunoregulation. Lancet 1981 ;ii:839-42.
Meijer CJLM, de Graaff-Reitsma CB, Lafeber GJM, Cats A. Insitu localization of lymphocyte subsets in synovial membranesof patients with rheumatoid arthritis with monoclonal anti-bodies. J Rheumatol 1982;9:359-65.
6 Bhan AK, Harrist TJ, Murphy GF, Mihm MC Jr. T cell subsetsand Langerhans cells in lichen planus: In situ characterizationusing monoclonal antibodies. Br J Dermatol 1981;105:617-22.
McMillan EM, Beeman K, Wasik R, Everett MA. Demonstra-tion of OKT6-reactive cells in mycosis fungoides. Am AcadDermatol 1982;6:880-7.
Van Voorhis WC, Kaplan G, Sarno EN, et al. The cutaneousinfiltrates of leprosy. N Engl J Med 1982;307:1593-7.
Janossy G, Montano L, Selby WS, et al. T cell subset
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from

Exanthem of Ross River virus infectionabnormalities in tissue lesions developing during autoimmunedisorders, viral infection and graft-versus-host disease. J ClinImmunol 11983;2, 3 July suppl: 42-55.
'0 Anderson SG, French EL. An epidemic exanthem associatedwith polyarthritis in the Murray Valley, 1956. Med J Aust1957;2: 113.
"Clarris BJ, Doherty RL, Fraser JRE, French EL, Muirden KD.Epidemic polyarthritis: A cytological virological andimmunochemical study. Aust NZ J Med 1975;5:450-7.
12 Fraser JRE, Cunningham AL, Clarris BJ, Aaskov JG, Leach R.Cytology of synovial effusions in epidemic polyarthritis. AustNZ J Med 1981;11:168-73.
Becker GJ, Hancock WW, Kraft N, Lanyon HC, Atkins RC.Monoclonal antibodies to human macrophage and leucocytecommon antigens. Pathology 1981 ;13:669-80.
4 Hancock WW, Becker GJ, Atkins RC. A comparison of fixativesand immunohistochemical techniques for use with monoclonalantibodies to cell surface antigens. Am J Clin Pathol1982;78:825-31.
'5 Kung PC, Goldstein G, Reinherz EL, Schlossman SF. Mono-clonal antibodies defining distinctive human T cell antigens.Science 1979;206:347-9.
6 Reinherz EL, Kung PC, Goldstein G, Schlossman SF. Separationof functional subsets of human T cells by a monoclonal anti-body. Proc Nad Acad Sci USA 1979;76:4061-5.
7 Reinherz EL, Kung PC, Goldstein G, Levey RH, Schlossman SF.Discrete stages of human intrathymic differentiation: analysisof normal thymocytes and leukemic lymphoblasts of T-celllineage. Proc Natl Acad Sci USA 1980;77: 1588-92.
1 Brooks DA, Zola H, McNamara PJ, Bradley J, Bradstock KF,Hancock WW, Atkins RC. Membrane antigens of human cellsof the monocyte/macrophage lineage studied with monoclonalantibodies. Pathology 1983;15:45-52.
'9 Fithian E, Kung P, Goldstein G, Rubenfeld M, Fenoglio C, Edel-son R. Reactivity of Langerhans cells with hybridoma anti-body. Proc Nad Acad Sci USA 1981;78:2541-4.
20 Zola H, McNamara P, Thomas M, Smart IJ, Bradley J. Thepreparation and properties of monoclonal antibodies againsthuman granulocyte membrane antigens. Br J Haematol1981 ;48:481-90.
21 Ortaldo JR, Sharrow SO, Timonen T, Herberman B. Determina-tion of surface antigens on highly purified human NK cells byflow cytometry with monoclonal antibodies. J Immunol1981;127:2401-7.
126322 Nayashi M, Nakajima Y, Fishman WH. The cytologic demonst-
ration of beta-glucuronidase employing naphthol AS-BIglucuronide and hexazonium pararosanilin: a preliminaryreport. J Histochem Cytochem 1964;12:293-7.
23 Sabin AB. Research on dengue during World War II.Am J TropMed Hyg 1952;1: 130-50.
24 Alien AC. The skin. A clinicopathologic treatise. 1954. St Louis:CV Mosby Co, 1954:307-8.
2 Ackerman AB. Histologic diagnosis of inflammatory skin dis-eases. Philadelphia: Lea and Febiger, 1978:198.
26 Thomas Y, Sosman J, Irigoyen 0, et al. Functional analysis ofhuman T cell subsets defined by monoclonal antibodies. 1.Collaborative T-T interactions in the immunoregulation of Bcell differentiation. J Immunol 1980;125:2402-8.
27 Reinherz EL, Kung PC, Goldstein G, Schlossman SF. A mono-clonal antibody reactive with the human cytotoxic/suppressorT cell subset previously defined by a heteroantiserum termedTH2. JImmunol 1980;124:1301-7.
28 Reinherz EL, Schlossman SF. The differentiation and function ofhuman T lymphocytes. Cell 1980;19:821-7.
29 Moretta L, Mingari MC, Sekaly PR, Moretta A, Chapuis B,Cerottini J-C. Surface markers of cloned human T cells withvarious cytolytic activities. J Exp Med 1981 ;154:569-74.
3 MacFarlan RI, Bums WH, White DO. Two cytotoxic cells inperitoneal cavity of virus-infected mice: Antibody-dependentmacrophages and nonspecific killer cells. J Immunol1977;199: 1569-74.
3' MacFarlan RK, White DO. Further characterization of naturalkiller cells induced by Kunjin virus. Aust J Exp Biol Med Sci1980;58:77-89.
32 Mims CA. The pathogenesis of infectious disease. London:Academic Press, 1977: 159.
33 Heggie AD. Pathogenesis of the rubella exanthem: Distributionof rubella virus in the skin during rubella with and withoutrash. I Infect Dis 1978; 137:74-7.
34 Rosen L, Gubler DJ, Bennett PH. Epidemic polyarthritis (RossRiver) virus infection in the Cook Islands. Am J Trop MedHyg 1981 ;30: 1294-302.
Requests for reprints to: Dr JRE Fraser, University ofMelbourne Department of Medicine, The Royal Mel-bourne Hospital PO, Victoria, 3050, Australia.
copyright. on M
arch 18, 2020 by guest. Protected by
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.36.11.1256 on 1 N
ovember 1983. D
ownloaded from