Embed Size (px)
Citation preview

VISUAL JOURNAL EMERGENCY
MEDICINE
the
of

The Visual Journal of Emergency Medicine publishes image-based case discussions representing the entire core curriculum and subspecialties of clinical emergency medicine. Images include clinical photos, EKGs, ultrasound images, plain radiographs, and representative CT and MR images.
Each image-based case will include a question and answer set.
Published in a mobile optimized online format, the journal provides a multidisciplinary clinical and educational publishing opportunity for emergency physicians, emergency medicine and other residents, fellows, emergency nurses, physician assistants, EMTs, paramedics, and clinicians in related fields. All submissions are peer-reviewed.
EDITOR-IN-CHIEFMichael Greenberg, MD, MPH Philadelphia, PA, USA
ASSOCIATE EDITOR-IN-CHIEFRita McKeever, MD Philadelphia, PA, USA
ASSOCIATE EDITORSViveta Lobo, MD Stanford, CA, USARalph Riviello, MD, MS Philadelphia, PA, USAMark Saks, MD, MPH Upland, PA, USADavid Vearrier, MD, MPH Philadelphia, PA, USA Laura Vearrier, MD Philadelphia, PA, USA
EDITORIAL ADVISORY BOARDJonathan Glauser, MD Cleveland, Ohio, USARobert Hendrickson, MD Portland, Oregon, USAMichael Holland, MD, MPH Syracuse, New York, USABohdan Minczak, MD Philadelphia, Pennsylvania, USA Donna Seger, MD Tennessee, USA Mark Silverberg, MD New York, New York, USA
RESIDENT-IN-TRAINING MEMBERSElisabeth Calhoun, MD, MPH Philadelphia, USAVirat Patel, MD Philadelphia, USA

Contents lists available at ScienceDirect
Visual Journal of Emergency Medicine
journal homepage: www.elsevier.com/locate/visj
Visual Case Discussion
Adolescent hand, foot, and mouth disease
Ciara J. Barclay-Buchanan
Assistant Professor (CHS), University of Wisconsin – Madison, Department of Emergency Medicine, Madison, WI, USA
A R T I C L E I N F O
Keywords:Hand, foot, and mouthRashPediatricAdolescent
A previously healthy 15-year-old boy developed a fever, sore throat,malaise, and fatigue. Within 48-h, he developed a vesicular andmaculopapular rash on the palms of his hands (Fig. 1), the soles ofhis feet (Fig. 2) and on his face (Fig. 3a). Painful intra-oral ulcerationsalso developed in his mouth (Fig. 3b). Several of his school classmatesand his 17-year-old brother also developed a similar constellation ofsymptoms within the same week.
Fig. 1. Maculopapular lesions on the palm of his hand. Fig. 2. Vesicular and maculopapular lesions on the sole of his foot.
http://dx.doi.org/10.1016/j.visj.2017.01.006Received 7 November 2016; Accepted 5 January 2017
Visual Journal of Emergency Medicine 7 (2017) 48–49
2405-4690/ © 2017 Elsevier Inc. All rights reserved.
MARK

Appendix A. Supplementary material
Supplementary data associated with this article can be found in theonline version at http://dx.doi.org/10.1016/j.visj.2017.01.006.
Further reading
1 Downing C, Romirez-Fort MK. Coxsackievirus A6 associated hand, foot and mouthdisease in adults: clinical presentation and review of literature. J Clin Virol.2014;4:381–386.
2 Irving S, Barclay-Buchanan CJ. Onychomadesis: a rare sequela of hand, foot, andmouth disease. J Emerg Med. 2015;49(4):e127–e128 [PMID:26113378].
3 Repass GL, Palmer WC, Stancampiano FF. Hand, foot, and mouth disease. identifyingand managing an acute viral syndrome. Cleve Clin J Med. 2014;81(9):537–543.
Fig. 3. a and b Maculopapular lesions around his mouth and intra-oral ulcerations onhis oral mucosa.
C.J. Barclay-Buchanan Visual Journal of Emergency Medicine 7 (2017) 48–49
49

Contents lists available at ScienceDirect
Visual Journal of Emergency Medicine
journal homepage: www.elsevier.com/locate/visj
Visual case discussion
Lens dislocation
Aliza Weinman, Jimmy Truong⁎, Cynthia Sanchez, Matt Abad
Department of Emergency Medicine, St Barnabas Health System, 4422 3rd Ave, Bronx, NY 10457, USA
A R T I C L E I N F O
Keywords:Lens dislocation
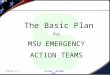
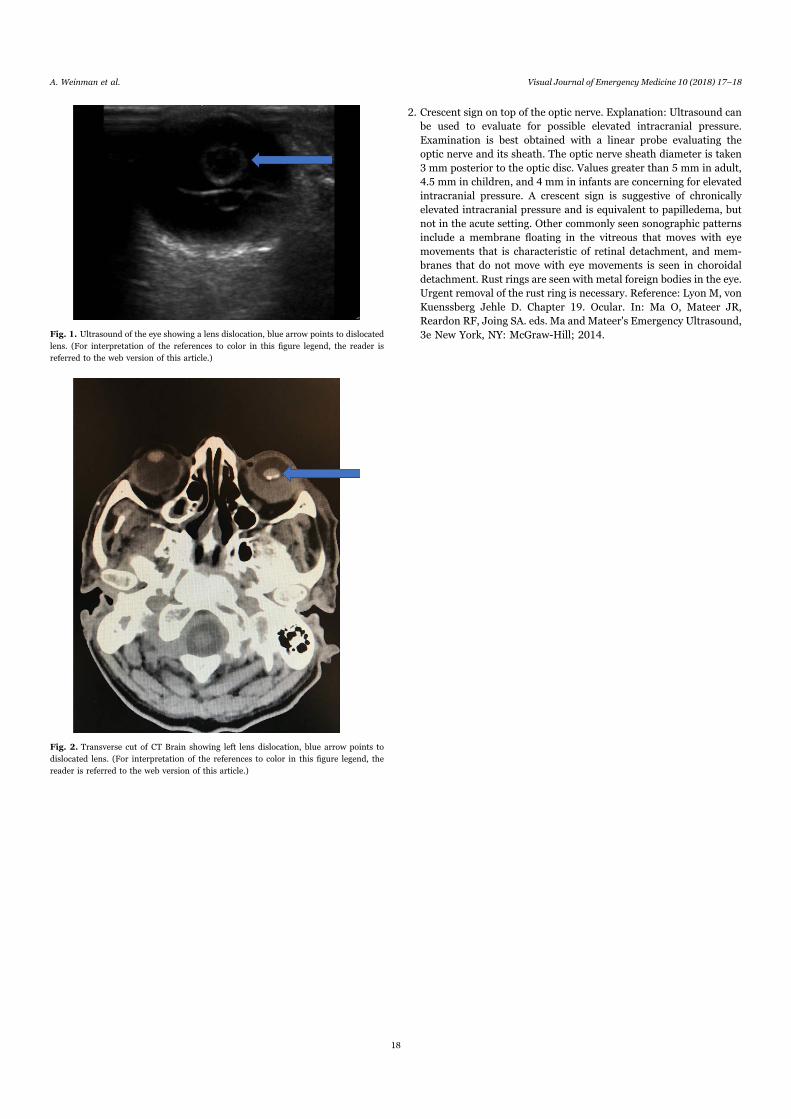
A 70 year old male presented to the Emergency Department after amechanical trip and fall onto his left side. He sustained a laceration to theleft periorbital area and an abrasion to his left hand. The patient deniedany usage of blood thinners or alcohol. He denied any other somaticcomplaints. His medical history was significant for left eye blindness ofunknown origin for the past year. Upon secondary survey, an evaluationof his left eye with point of care ultrasound was performed showing a lensdislocation shown in Fig. 1. The optic nerve sheath was measured to be0.4 cm and within normal range. A video of the dynamic ultrasound isshown in Video 1. The patient was taken for CT of the brain to evaluatefor intracranial pathology and shows a lens dislocation shown in Fig. 2.Upon discussion of the objective findings, his family arrived andconfirmed his optic pathology. After his laceration was repaired, he wasgiven close follow up and reminder to see his ophthalmologist.
Supplementary material related to this article can be found onlineat http://dx.doi.org/10.1016/j.visj.2017.07.007
Further reading
1 Weaver CS, Knoop KJ. Ophthalmic traumaKnoop KJ, Stack LB, Storrow AB, ThurmanR, eds. The Atlas of Emergency Medicine4e, New York, NY: McGraw-Hill; 2016.
2 Walker RA, Adhikari S, Walker RA, Walker Adhikari S, Richard A, Adhikari Srikar.Eye EmergenciesTintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM,eds. Tintinalli's Emergency Medicine: A Comprehensive Study Guide8e, New York,NY: McGraw-Hill; 2016.
3 Lyon M, von Kuenssberg Jehle D, Lyon M, von Kuenssberg Jehle D Lyon, Matthew ,Dietrich von Kuenssberg Jehle. OcularMa O, Mateer JR, Reardon RF, Joing SA, Ma O,Mateer JR, eds. Ma and Mateer's Emergency Ultrasound3e, New York, NY: McGraw-Hill; 2014.
Questions
1. Which of the following statements is correct regarding a lensdislocation?a. Secondary angle closure glaucoma may result when a displaced
lens causes pupillary blockage
b. A displaced lens appears as a crescent against a backdrop of thewhite reflex from the fundus
c. In dilating the pupil, the lens may sublux into the posteriorchambers
d. Surgery is required if the lens dislocates posteriourlye. Phacodonesis is the dislocation of the lens anteriorly
2. Which of the following is characteristic of increased intracranialpressure?a. Optic nerve sheath diameter < 3 mm in adultsb. Membrane floating in the vitreous, that moves with eye move-
mentsc. Membrane floating in the vitreous, that does not move with eye
movementsd. Crescent sign on top of the optic nervee. Rust ring
Answers
1. Secondary angle closure glaucoma may result when a displaced lenscauses pupillary blockage. Explanation: Lens dislocation occurs withblunt trauma to the globe. A complication that occurs is secondaryangle closure glaucoma from the lens causing pupillary blockage. Onexamination, the lens will appear as a crescent shape against a redreflex from the fundus. Dilatation of the pupil should be performedwith caution as it may cause the lens to sublux into the anteriorchamber. Phacodonesis can also occur, which is the tremulousness ofthe lens caused by a disruption of the zonule fibers. Coexisting diseasesthat are associated with lens dislocation include Marfan syndrome,homocystinuria, and tertiary syphilis. Surgery is required in caseswhere the lens dislocates anteriorly causing pupillary blockage andangle closure glaucoma. Reference: Weaver CS, Knoop KJ. OphthalmicTrauma. In: Knoop KJ, Stack LB, Storrow AB, Thurman R. eds. TheAtlas of Emergency Medicine, 4e New York, NY: McGraw-Hill.
http://dx.doi.org/10.1016/j.visj.2017.07.007Received 23 May 2017; Accepted 9 July 2017
⁎ Corresponding author.E-mail address: [email protected] (J. Truong).
Visual Journal of Emergency Medicine 10 (2018) 17–18
2405-4690/ © 2017 Elsevier Inc. All rights reserved.
MARK
2. Crescent sign on top of the optic nerve. Explanation: Ultrasound canbe used to evaluate for possible elevated intracranial pressure.Examination is best obtained with a linear probe evaluating theoptic nerve and its sheath. The optic nerve sheath diameter is taken3 mm posterior to the optic disc. Values greater than 5 mm in adult,4.5 mm in children, and 4 mm in infants are concerning for elevatedintracranial pressure. A crescent sign is suggestive of chronicallyelevated intracranial pressure and is equivalent to papilledema, butnot in the acute setting. Other commonly seen sonographic patternsinclude a membrane floating in the vitreous that moves with eyemovements that is characteristic of retinal detachment, and mem-branes that do not move with eye movements is seen in choroidaldetachment. Rust rings are seen with metal foreign bodies in the eye.Urgent removal of the rust ring is necessary. Reference: Lyon M, vonKuenssberg Jehle D. Chapter 19. Ocular. In: Ma O, Mateer JR,Reardon RF, Joing SA. eds. Ma and Mateer's Emergency Ultrasound,3e New York, NY: McGraw-Hill; 2014.Fig. 1. Ultrasound of the eye showing a lens dislocation, blue arrow points to dislocated
lens. (For interpretation of the references to color in this figure legend, the reader isreferred to the web version of this article.)
Fig. 2. Transverse cut of CT Brain showing left lens dislocation, blue arrow points todislocated lens. (For interpretation of the references to color in this figure legend, thereader is referred to the web version of this article.)
A. Weinman et al. Visual Journal of Emergency Medicine 10 (2018) 17–18
18

Contents lists available at ScienceDirect
Visual Journal of Emergency Medicine
journal homepage: www.elsevier.com/locate/visj
Visual Case Discussion
Submassive pulmonary embolus
Gayana Grigoryan⁎, Janeth Mantilla
St. Barnabas Hospital Health System, Bronx, NY, United States
A R T I C L E I N F O
Keywords:Submassive pulmonary embolism
30 year old male with no significant past medical history presentingto the emergency room for shortness of breath that started five monthsago when he had a cold. Patient remained in bed most of the time whilesick, has had shortness of breath that worsened with time and isassociated with decreased exercise tolerance. Patient describes notwanting to walk outside due to fear of becoming short of breath. Reviewof systems significant for progressive shortness of breath, lowerextremity swelling, decreased physical activity. Patient denied recenttravel, cough, hemoptysis, fever, calf pain, chest pain, history of cancer
or deep venous thrombosis. Patient appears comfortable, in no acutedistress, speaking in complete sentences, without accessory muscle use,lungs exam with decreased breath sounds at right base, lowerextremities with pitting edema. Vitals signs significant for tachycardiaat 112 beats per minute and tachypnea at 22 breaths per minute, bloodpressure 133/84. Pertinent labs BNP 539, troponin negative, WBC 6.3.EKG significant for sinus tachycardia and right heart strain, Fig. 1.Chest xray showed a right pleural effusion, Fig. 2. A bedside echoshowed evidence of right heart strain, Video 1. Computed tomography
Fig. 1. EKG showing sinus tachycardia and right heart strain (red arrows).
http://dx.doi.org/10.1016/j.visj.2017.07.019Received 23 May 2017; Received in revised form 10 July 2017; Accepted 16 July 2017
⁎ Corresponding author.E-mail addresses: [email protected] (G. Grigoryan), [email protected] (J. Mantilla).
Visual Journal of Emergency Medicine 9 (2017) 55–56
2405-4690/ © 2017 Elsevier Inc. All rights reserved.
MARK

angiography confirmed diagnosis of submassive pulmonary embolus,Fig. 3.
Supplementary material related to this article can be found onlineat http://dx.doi.org/10.1016/j.visj.2017.07.019.
Appendix A. Supporting information
Supplementary data associated with this article can be found in theonline version at doi:10.1016/j.visj.2017.07.019.
Questions
1. What is the most common electrocardiogram finding of pulmonaryembolism?a. S1Q3T3b. Right Bundle Branch Blockc. T wave inversions in V1-4d. Sinus tachycardiae. Supraventricular tachycardia
2. What is the gold standard for diagnosing pulmonary embolism?a. EKGb. CT chestc. Ultrasound (cardiac, DVT)d. CT Pulmonary Angiographye. V/Q scan
Answers
1. Sinus Tachycardia. Explanation: Although ECG findings are non-specific sinus tachycardia is the most common finding. S1Q3T3,right bundle branch block and T wave inversion in leads V1-4 allsuggest right heart strain and may strongly suggest pulmonaryembolus diagnosis. Reference: Ullman E, Brady WJ, Perron AD,Chan T, Mattu A. Electrocardiographic manifestations of pulmonaryembolism. Am J Emerg Med. 2001 Oct;19(6):514–9.
2. CT Pulmonary Angiography. Explanation: Pulmonary angiography isthe “gold” standard for confirming diagnosis of PE. V/Q scan hashigh sensitivity bur poor specificity. EKG findings are non specificand about 33% of patients with PE will have a normal EKG.Reference: Cohen R, Loarete P, Navarro V, Brooks, M.Echocardiographic findings in pulmonary embolism: An importantguide for the management of the patient. World Journal ofCardiovascular Diseases. 2012 July; (2) 161–164.
Fig. 2. A. PA chest xray B. Lateral Chest xray. Chest xray showing Airspace disease in theright middle and lower lobes, small right pleural effusion.
Fig. 3. Arrow pointing to filling defect in right pulmonary artery indicating pulmonaryembolism.
G. Grigoryan, J. Mantilla Visual Journal of Emergency Medicine 9 (2017) 55–56
56

Contents lists available at ScienceDirect
Visual Journal of Emergency Medicine
journal homepage: www.elsevier.com/locate/visj
Visual Case Discussion
Contained bowel perforation
Jean Dorcea, Jimmy Truonga, Maisah Shaikha,⁎, Brian Chiongb
a Department of Emergency Medicine, St. Barnabus Hospital, Bronx, NY, United Statesb Department of Radiology, St. Barnabus Hospital, Bronx, NY, United States
A R T I C L E I N F O
Keywords:DiverticulitisBowel perforationContained abscess
A 55 year old male presents to the ED with worsening abdominalpain since the morning. The patience has a history of two prior pelvicabscesses, both involving drainage via laparoscopy, and InterventionalRadiology placement of a pigtail catheter, respectively. The patient alsohas a pertinent history of diverticulitis, diagnosed one month prior, withradiologic evidence of a localized performation of the sigmoid colon.
On initial presentation, the patient appeared in acute distress secondaryto pain. His vitals were as follows: Temperature 36.3 °C, BP 147/
91 mmHg, HR 65 bpm, RR 16, SPO2 99 on RA. On abdominal exam, hehas audible bowel sounds by auscultation, generalized tenderness diffusely,and rebound tenderness. An immediate CT scan is performed which showsthickened sigmoid colon and diverticulae, consistent with diverticulitis(Fig. 1), and an abscess with air just above the sigmoid colon, consistentwith perforation and diverticular abscess (Fig. 2). The impression is acontained perforation of the sigmoid colon in an abscess.
The patient has an immediate surgical consult and is admitted for
Fig. 1. Thickened sigmoid and diverticulae consistent with diverticulitis (yellow arrow).
http://dx.doi.org/10.1016/j.visj.2017.08.013Received 28 June 2017; Received in revised form 9 August 2017; Accepted 19 August 2017
⁎ Corresponding author.E-mail address: [email protected] (M. Shaikh).
Visual Journal of Emergency Medicine 10 (2018) 51–53
2405-4690/ © 2017 Elsevier Inc. All rights reserved.
MARK

conservative management with antibiotics. However, the patient'sclinical course worsens, with worsening pain and increased leukocy-tosis. Repeat CT imaging of the abdomen demonstrates worseningappearance of the diverticular abscess and increased levels of inflam-mation (Fig. 3). The patient is eventually taken to surgery for anexploratory laparotomy and colonic diversion with end colostomy forrecurrent sigmoid diverticulitis perforation and abscess.
Appendix A. Supplementary material
Supplementary data associated with this article can be found in theonline version at doi:10.1016/j.visj.2017.08.013.
Further reading
1. Moore Frederick A, Catena F, Moore E, Leppaniemo A, Peitzmann A. Position paper:management of perforated sigmoid diverticulitis. World J Emerg Surg. 2013;8:55.
http://dx.doi.org/10.1186/1749-7922-8-55.2. Graham A. DiverticulitisTintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD,
Cline DM, eds. Tintinalli's Emergency Medicine: A Comprehensive Study Guide8 ed.,New York, NY: McGraw-Hill; 2016.
3. Strate LL, Modi R, Cohen E, Spiegel BM. Diverticular disease as a chronic illness:evolving epidemiologic and clinical insights. Am J Gastroenterol.2012;107(10):1486–1493 [Medline].
Questions
1. A patient presents with abdominal pain and found to have diverti-culitis with a Hinchey classification of Stage 3. Which of thefollowing is the best treatment?a. Discharge after PO challengeb. Discharge with PO antibioticsc. Admit for serial abdominal examd. Admit for IV antibiotics, onlye. Admit for IV antibiotics and emergent surgical intervention
Fig. 2. Abscess with air just above sigmoid consistent with perforation and diverticular abscess (yellow arrow). There is inflammed loop of small bowel more anteriorly (blue arrow).
Fig. 3. Progression of abscess (yellow arrow). Adjacent inflammed small bowel loops (blue arrow) and descending colon (red arrow).
J. Dorce et al. Visual Journal of Emergency Medicine 10 (2018) 51–53
52

2. Which of the following is true regarding diverticulitis?a. Younger patients with diverticulitis have higher rates of recurrence,
complicated presentation, and need for surgical interventionsb. Meckel's diverticulitis is treated medicallyc. Epiploic appendagitis occurs inside the colon and warrants a
surgical consultation for removald. Failed outpatient treatment of uncomplicated diverticulitis is
defined as symptoms or worsening imaging studies within 2weeks of initial episode
e. Hinchey 1 and 2 classifications involve perforated diverticulitis
Answers
1. Admit for IV antibiotics and emergent surgical intervention.Explanation: The Hinchey classification scheme is used for compli-cated diverticulitis. Stage 1 is defined as small, < 4 cm, confinedpericolic or mesenteric abscess and often are admitted for IVantibiotics and do not require percutaneous drainage. Stage 2involves a larger abscess that extends into the pelvis. Stage 3 showsperforated diverticulitis with purulent peritonitis and stage 4 isevidence of free perforation with fecal contamination into theperitoneal cavity. Evidence of complicated diverticulitis warrantsadmission. Evidence of perforation, holds a high mortality rate, andwill require volume resuscitation, IV antibiotics, and emergentexploratory surgery. Reference: Graham A. Diverticulitis. In:Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline
DM. eds. Tintinalli's Emergency Medicine: A Comprehensive StudyGuide, 8 ed. New York, NY: McGraw-Hill; 2016.
2. Younger patients with diverticulitis have higher rates of recurrence,complicated presentation, and need for surgical interventions.Explanation: Younger patients defined as < 40 years of age diag-nosed with diverticulitis have higher rates of recurrence, compli-cated presentations, and need for surgical interventions. Meckel'sdiverticulum is a true congenital diverticulum and Meckel's diver-ticulitis is often confused with acute appendicitis and warrantssurgical removal for treatment. Epiploic appendagitis is inflamma-tion of small fat-filled sacs in the lining of the colon that are due totorsion or venous thrombosis. Failed outpatient treatment ofuncomplicated diverticulitis is defined as symptoms or worseningimaging studies within 6 weeks of initial episode. In complicateddiverticulitis, the Hinchey classification scheme is used for com-plicated diverticulitis. Stage 1 is defined as small, < 4 cm, confinedpericolic or mesenteric abscess and often are admitted for IVantibiotics and do not require percutaneous drainage. Stage 2involves a larger abscess that extends into the pelvis. Stage 3 showsperforated diverticulitis with purulent peritonitis and stage 4 isevidence of free perforation with fecal contamination into theperitoneal cavity. Reference: Graham A. Diverticulitis. In:Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, ClineDM. eds. Tintinalli's Emergency Medicine: A Comprehensive StudyGuide, 8 ed. New York, NY: McGraw-Hill; 2016.
J. Dorce et al. Visual Journal of Emergency Medicine 10 (2018) 51–53
53

FREQUENTLY ASKED QUESTIONSWhy publish?• Opportunitytopublishyouruniqueimagesandvisualcasediscussionusingaquickandeasy
submissionprocess.• Experienceunsurpassedglobalreachvianumerouselectronicplatforms(ScienceDirect,
mobile-optimizedjournalwebsites)andsocialmedia.• Therearenofeesforsubmission.
How do I submit?• It’seasy!Visitjournals.elsevier.com/visual-journal-of-emergency-medicine• Asubmissiontemplateisprovidedtohelpsimplifythewritingprocess.
Do I need to use the submission template?• Yes.Thesubmissiontemplateisdesignedtomakesubmissioneasy.Simplydownloadandcomplete/
followtheinstructionsonthetemplate,anduploadthecompletedformsintotheEVISEsubmissionsystemalongwithyourimage(s)orvideo(s).YoucanaccessEVISEbyclickingthe,“Submityourpaper”tab.
What types of images are accepted?• Acceptableimagesincludehighqualityclinicalphotos,EKGs,ultrasoundimagesandvideo,plain
radiographs,andrepresentativeCTandMRimages.• Uptothreeimagesorvideoscanbesubmittedperarticle.• TheGuideforAuthors,locatedonthejournalhomepage,providesadditionalinformation.
Will my submission be peer reviewed?• Yes,allmanuscriptssubmittedarepeerreviewed.
Are samples available?• Yes!A sample issue can be seen athttps://www.sciencedirect.com/science/journal/sample/24054690.
ConnectwithourEmergencyMedicinecontentonTwitter@ELS_Emerg_Med