Embed Size (px)
Citation preview

The Status of Patient SafetyDonald M. Berwick, MD, President and CEO
Institute for Healthcare Improvement
10th Anniversary of To Err is Human
The Commonwealth Fund and Alliance for Health Reform
March 17, 2010: Washington, DC

Topics
1. Trends, Impact, and Gaps in Patient Safety
2. Priorities for Closing the Gaps
3. Constructive Roles for the Federal Government
4. A Vision for the 20th Anniversary of To Err Is Human
2

Trends since 1999• Firm documentation of widespread,
avoidable harm to patients.• Better understanding of the “safety
science.”• Better methods of detection and
measurement.• Better appreciation of a “culture of
safety.”• Breakthrough results in some
organizations.3

0
20
40
60
80
100
120
140
0 50 100 150 200 250
Ho
sp
ita
l Sta
nd
ard
ise
d M
ort
alit
y R
ati
o (
HS
MR
20
07
)
Hospital Standardised Reimbursement Ratio (HSRR 2007)
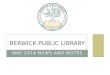
HSRR vs HSMR - Hospital Standardised Mortality Ratio vs Hospital Standardised Reimbursement Ratio (2007 Medicare Data)
Hospital Standardized Mortality vs. Hospital Reimbursement
Source: Sir Brian Jarman 2009

Institute for Healthcare Improvement Safety Campaigns
5
2004-2006
2006-2008

The Campaign “Planks” -- Twelve Changes for Safety
1. Rapid Response Teams
2. Evidence-Based Care for Heart Attacks
3. Medication Reconciliation
4. Prevent Central Line Infections
5. Prevent Surgical Site Infections
6. Prevent Ventilator-Associated Pneumonias
6

The Campaign “Planks” -- Twelve Changes for Safety
7.Prevent Pressure Ulcers
8.Reduce Methicillin-Resistant Staphylococcus Aureus (MRSA) Infections
9.Prevent Harm from High-Alert Medications
10.Reduce Surgical Complications (the Surgical Care Improvement Project (SCIP))
11.Evidence-Based Care for Congestive Heart Failure
12.Get Boards on Board
7

8

Sentara Williamsburg (Virginia)Zero Ventilator Pneumonias in Five Years!
9

10
Seton Family of Hospitals (Austin, TX)Birth Trauma Prevention
One Birth Injury in 10,000 Deliveries

Pressure Ulcer
11

Error Reduction at Ascension
Preventable Error Reduction in Rate
Pressure Ulcer
Neonatal Mortality
Birth Trauma
Ventilator-Acquired Pneumonia
Falls with Serious Injury
Bloodstream Infections
95%
79%
74%
56%
54%
32%

Palmetto Hospital Mortality Rates(South Carolina)
13

Does Improving Safety Save Money?
IMPROVEMENT COST SAVINGS NET
SURGICAL INFECTIONS
($110,000) $540,000 $430,000
BLOODSTREAM INFECTIONS
($22,500) $4,780,000 $4,757,500
VENTILATOR PNEUMONIAS
($1,268,500)(Reduced Revenue)
$1,166,400 ($102,100)
RAPID RESPONSE TEAMS
($390,000) ? ($390,000)
TOTAL ($1,791,000) $5,320,000 $4,695,400
14
HENRY FORD HEALTH SYSTEM

Closing Gaps – What Now?
• Governance – Boards – responsible for safety
• Better measurements of safety levels
• More transparency
• Science to devise standards that work
• “National learning systems” to spread the successes – Make “the best” become “the norm”
• National stewardship – a “public health” model
• Consequences for inaction
15

How Government Can Help:“Will, Ideas, and Execution”
GAP GOVERNMENT
Boards responsible for safety Map into accreditation standards
Better measurements of safety levels
Support prompt, active research on measurements of safety
More transparencyFurther develop Medicare data,
measurement, and reporting capacity
Science to devise standards that work
Support research on safety sciences and health care process designs
“National learning systems” to spread the successes
Develop public and private “extension” capacities for knowledge management
National stewardship – a “public health” model
Annual reports on quality and safety, with Congressional and Executive review
Consequences for inactionUnlink payment from volume; study “no
pay” for defects16

“20th Anniversary Report”
• Injury Rates in American Hospitals Measured and Tracked
• National and Regional “Learning Systems” Spread Good Practices
• Safety Education Routine in Health Professional Development
• Health Care Sets a Benchmark for High-Hazard Industries
• Patient Injuries Reduced by 90% from 1999• Health Worker Injuries Reduced by 90%
17

The “Triple Aim”
PopulationHealth
Experienceof Care
Per CapitaCost
18

How Do They Do That?High-Performing Communities in American Health Care
19
$10,250 to 17,184 (55)9,500 to < 10,250 (69)8,750 to < 9,500 (64)8,000 to < 8,750 (53)6,039 to < 8,000 (65)
Not Populated
Everett, WA
Sacramento,CA
Temple, TX
Tallahassee,FL
La Crosse,WI Cedar
Rapids, IA
Sayre,PA
Portland, ME
Richmond, VA
Asheville, NC

Price Adjusted Spending
2006
Increase in Spending
1992 – 2006
Annual growthrate
All Others (232) $9,695 $3,376 3.6%
Qualifying (74) $8,212 $2,645 3.4%
Participants (10) $7,924 $2,297 3.0%
Potential Annual Savings: 12.7% - 16.2%
What Are They Doing?
20
Per-Capita Spending – and Spending Growth – Are Lower.