Upload
others
View
0
Download
0
Embed Size (px)
Citation preview
EUROPEAN COMMISSION
The State of Mental Healthin the European Union
The State of Mental Health
in the European Union
EUROPEAN COMMISSION
Neither the European Commission nor any person acting on its behalf is responsible for any use that might be made of the following information. The information contained in this publication does not necessarily reflect the opinion or the position of the European Commission. Reproduction is authorised, except for commercial purposes, provided the source is acknowledged
Europe Direct is a service to help you find answers
to your questions about the European Union
New freephone number:
00 800 6 7 8 9 10 11
A great deal of additional information on the European Union is available on the Internet. It can be accessed through the Europa server (http://europa.eu.int). ISBN 92-894-8320-2 © European Communities, 2004 Photo cover page: © European Communities, reproduction authorised until 2012, provided the source is acknowledged. Printed by the services of the European Commission
ContentsList of contributors 5
Executive summary 6
1 Introduction 81.1 Mental health and mental illness 81.2 Burden of mental illness 91.3 Why publish a European report on mental health? 10
2 Comparing mental health in Europe 122.1 Context of mental health in Europe 122.2 Methodology for comparing mental health in Europe 15
3 Mental health status in Europe 203.1 Positive mental health 203.2 Negative mental health: psychological distress 20
and psychiatric disorders3.3 Suicide 253.4 Alcohol, tobacco and drug related problems 28
4 Protective and risk factors 344.1 Gender and mental health 344.2 Age and mental health 384.3 Marital status 434.4 Social factors - poverty, unemployment and deprivation 444.5 Rural-urban differences in mental health 484.6 Migration and mental health 51
5 Responses to mental health problems across Europe 545.1 General description 545.2 Psychiatric inpatient care 545.3 Community services, facilities and support 565.4 Mental health in primary health care 565.5 Staffing issues 575.6 Patient and family involvement 585.7 Use of psychotropic drugs 595.8 Survey results: Seeking help for mental health problems 61
6 Conclusions and recommendations 646.1 Summary of findings 646.2 Conclusions 666.3 Recommendations 66
Annex I Details of studies used in survey of surveysReferences
1
T H E S T A T E O F M E N T A L H E A L T H I N T H E E U R O P E A N U N I O N
2
T H E S T A T E O F M E N T A L H E A L T H I N T H E E U R O P E A N U N I O N
FiguresFigure 1 Determinants of mental health 11Figure 2 Population density in the EU and Norway 12Figure 3 Urban population in the EU and Norway 12Figure 4 Population aged over 65 in the EU and Norway 13Figure 5 Gross domestic product, unemployment and percentage of population at risk of poverty 14Figure 6 Health expenditure in EU countries and Norway 14Figure 7 Positive mental health in ten EU countries 20Figure 8 Psychological distress in ten EU countries 22Figure 9 Psychological Distress in seven EU countries (6 ESEMeD, plus UK) 22Figure 10 Any mental disorder in the last 12 months in six EU countries 23Figure 11 Any mood disorder in the last 12 months in six EU countries 23Figure 12 Anxiety disorders in the last 12 months in six EU countries 23Figure 13 Total suicide mortality rates across Europe, 1997 25Figure 14 Male deaths from suicide, events of undetermined intent and unknown and unspecified causes 25Figure 15 Female deaths from suicide, events of undetermined intent and unknown and
unspecified causes 25Figure 16 Trends in male suicide by country 26Figure 17 Trends in female suicide by country 26Figure 18 Suicide and old age in males across Europe 27Figure 19 Suicide and old age in females across Europe 27Figure 20 Suicides in young people across Europe 27Figure 21 Suicide, risk of poverty and unemployment 27Figure 22 Alcohol consumption across Europe 28Figure 23 Trend in alcohol consumption 1980–2001 29Figure 24 Trends in alcohol related death 1980–1997 29Figure 25 Occurrence of alcohol disorders in men and in women in the last 12 months
six European countries 25Figure 26 Effect of country on relative risk of lifetime alcohol disorders 26Figure 27 Cigarettes consumed per person per year in EU countries and Norway 27Figure 28 Deaths from smoking related causes in the EU and Norway 28Figure 29 Recent use of cannabis among young adults (15–34 years) in European Countries,
measured by national surveys 29Figure 30 Evolution of recent cannabis and cocaine use in some EU countries 32Figure 31 Trends in acute drug-deaths in some EU countries, 1985-99 33Figure 32 Positive mental health in men and women 34Figure 33 The effect of gender on the risk of poor mental health 35Figure 34 Relative risk of psychological distress for women compared to men in
some EU countries 35Figure 35 Psychological distress in males and females in some EU countries 35Figure 36 The effect of gender on the risk of depression 36Figure 37 Effect of gender for the risk of any disorders in ESEMeD 00Figure 38 Effect of gender for the risk of anxiety disorders in six EU countries 36Figure 39 Effect of gender for the risk of any disorders in six EU countries 37Figure 40 Ratio of male to female deaths from suicide in EU countries 37Figure 41 Ratio of male to female suicides across Europe, 1987 and 1997 38Figure 42 Relative risk of psychological distress for young people 38Figure 43 Psychological distress in seven EU countries 39Figure 44 Relative risk of any mental health disorders in young people in six EU countries 39Figure 45 Relative risk of anxiety disorders in young people in six EU countries 39Figure 46 Risk of psychological distress in older people 40Figure 47 Psychological distress in older people 40
3
T H E S T A T E O F M E N T A L H E A L T H I N T H E E U R O P E A N U N I O N
FiguresFigure 48 Relative risk of mood disorders in older people 41 Figure 49 Relative risk of anxiety disorders in older people 42Figure 50 Relative risk of psychological distress by marital status across Europe 43Figure 51 Mental health and living arrangements in six European countries 43Figure 52 Relative risk of mood disorders according to living arrangements 44Figure 53 Relative risk of psychological distress by employment status 47Figure 54 Psychological distress and unemployment in seven European countries 47Figure 55 Relative risk of any mood disorder in the last 12 months for unemployed people by country 47Figure 56 Relative risk of psychological distress by low income 48Figure 57 Psychological distress in rural and urban areas 50 Figure 58 Comparison of any mental disorders in the last 12 months for people living in
urban and rural areas 50Figure 59 Migration rates across Europe 51Figure 60 Psychological distress and migrants in five European countries 53Figure 61 Psychiatric hospital beds in European countries 55Figure 62 Numbers of psychiatrists in EU countries 57Figures 63 Numbers of GPs in EU countries 63Figure 64 Pharmaceutical expenditure across Europe 59Figure 65 People seeking help for a mental health problem 61 Figure 66 Relative risk of seeking help for a mental health problem among
cases of mental ill-health by country 61Figure 67 Probability of seeking help with a mental health problem 62Figure 68 People seeking help for mental health problems from any health provider 68 Figure 69 Types of providers consulted in case of mental health problems in the last year 69Figure 70 People seeking help from different providers in six ESEMeD countries 63Figure 71 Referrals from a family doctor to a mental health specialist 63Figure 72 Prescriptions of Drug for Individuals with any mental health disorder 63
4
T H E S T A T E O F M E N T A L H E A L T H I N T H E E U R O P E A N U N I O N
TablesTable 1 Prevalence rates of depressive disorders in selected major European studies 21Table 2 Prevalence of schizophrenia in the Nemesis study 24Table 3 Lifetime prevalence estimates of WMH-CIDI / DSM-IV mood disorders in
Europe for individuals aged 65+, ESEMeD project 41Table 4 Anxiety disorder in people aged over 65 in six European countries 42Table 5 Alcohol disorders in people aged over 65 in six European countries 43Table 6 Studies reporting associations with higher rates of the common
mental disorders, by indicators of less privileged social position 44Table 7 Impact of work on mental health 46Table 8 Depression in rural and urban areas in males and females 49Table 9 Consumption of antidepressants in 14 different
European Union countries 60Table 10 Consumption of anxiolytics and hypnotics in 14 different European Union countries 60
AcknowledgementsMany thanks to Frederic Capuano, Jocelyne Gagnon, Maria Carolina Hardoy, Trevor Hill, Zoe Morgan, Nick Taub, and Jane Smith for their help with this report.
5
T H E S T A T E O F M E N T A L H E A L T H I N T H E E U R O P E A N U N I O N
Participants and contributorsProject leaderViviane Kovess MGEN Foundation of Public Health, Paris 5 University, France
Co-ordinating boardTerry Brugha University of Leicester, UKMauro Giovanni Carta University of Cagliari, ItalyVille Lehtinen STAKES, National Research and Development Centre for
Welfare and Health, FinlandTopic expertsMatthias C Angermeyer (Older people) University of Leipzig, GermanyMariola Bernal (Immigrants) Sant Joan de Deu-SSM, SpainMiguel Xavier (Substances) Faculty Medical Sciences of Lisbon, PortugalFrance Kittel (Gender) ESP ULB Campus Erasme, BelgiumTom Fryers (Deprivation) University of Leicester, UK
National expertsBairbre Nic Aongusa Department of Health and Children, IrelandClaes-Goran Stefansson The National Board of Health and Welfare, SwedenHenrik Day Poulsen Copenhagen University Hospital, Rigshospitalet, DenmarkCharles Pull Centre Hospitalier de Luxembourg, LuxembourgJosep Maria Haro Abad Sant Joan de Deu-SSM, SpainHeinz Katschnig University of Vienna, AustriaMichael G Madianos University of Athens School of Nursing, GreeceOdd Steffen Dalgard University of Oslo, NorwayRob Bijl Ministry of Justice Research & Documentation, NetherlandsViviane Kovess MGEN Foundation of Public Health, Paris 5 University, FranceMauro Giovanni Carta University of Cagliari, ItalyVille Lehtinen STAKES,National Research and Development Centre for Welfare and Health, FinlandMatthias C Angermeyer University of Leipzig, GermanyMiguel Xavier Faculty Medical Sciences of Lisbon, PortugalFrance Kittel ESP ULB Campus Erasme, BelgiumTom Fryers University of Leicester, UK
Other expertsWolfgang Rutz WHO Regional Office for EuropeJohn H Henderson Mental Health EuropeGaetan Lafortune OECD
National refereesRaimundo Mateos Faculty of Medecine Santiago of Compostela, SpainPaul Bebbington University College London Medical School, UKJosé Miguel Caldas de Almeida Pan American Health Organization, PortugalAlv Dahl Aliv University Hospital, Norway Matti Joukaama University of Oulu, FinlandVenetsanos Mavrey University of Ionnina GreecePierluigi Morosini National Institute of Health, ItalyPer Nettelbladt Lund University, SwedenJohan Ormel University of Groningen, NetherlandsFrédéric Rouillon University Paris XII, FranceDermot Walsh Health Research Board Dublin, IrelandJohannes Wancata University of Vienna, AustriaSiegfried Weyerer Organisation Central Institute of Mental Health, GermanyKoen Demyttenaere KU Lueven, Belgium
Managing editorKaren McColl UK
This report aims to describe and compare the state ofmental health in the European Union and Norway, in thecontext of longstanding efforts of EU public healthprogrammes to promote good mental health and toprevent mental ill health.
A documented knowledge of the population’s mentalhealth status, and its determinants, is essential toestablish the basis for such programmes and to monitorand improve them.
In preparing this report, it has been assumed thatcollecting and comparing information on mental healthbetween countries will enable Member States to improvetheir understanding of mental health issues and to planappropriate policy responses. Mental health has to beconsidered as a public health priority due to the heavyburden it places on the EU and its Member States.
The report’s starting point is the acknowledgement thatMember States are different in terms of populationdensity, aging, poverty levels, cultural background andhabits. Furthermore, all of these factors have beenshown to have some links with mental health status andsome of them have been identified as risk factors.
This project has involved representatives from all EU countries plus Norway, WHO Europe, a representativeof a non-governmental organisation (Mental HealthEurope) and a representative of OECD Europe.
Each country representative was asked to summarise allthe surveys on mental health which had been carried outin their country. In addition, the experts each prepareda report on their country, its health system andparticular issues relating to the mental health domain.
Routinely collected statistics, such as cause of death orthe reasons for hospital discharge, do not fully reflectthe reality of the majority of mental health problems,which do not lead to death or hospitalisation. Thismeans that surveys among the general population arevery important for assessing the state of mental health.
Consequently this report has been prepared combiningtwo main kinds of data:
• routinely collected statistics on deaths from suicide,the use of drugs and alcohol and psychotropic drug consumption
• results from general population surveys.
The report is based on previous expert recommendationson mental health indicators, which propose that mentalhealth should be described in three dimensions. Positivemental health relates to well-being and the ability tocope with adversity. Negative mental health comprisesboth psychological distress, which refers to the presenceof symptoms (mainly depression or anxiety), anddiagnosis of psychiatric disorders. These are the threedimensions which have to be measured through surveys.
However, although many surveys which include mentalhealth measures were identified, the differences in surveytechniques and research methods make real comparisonsalmost impossible. This highlights the importance ofcollecting data in a comparable manner across the EU.
Two EU designed surveys – Eurobarometer and ESEMeD –provide important information for comparisons for mostof the countries. But even EU designed surveys facemethodological challenges when interpreting differences.
This report compiles the diverse indicators and describesthe major differences across countries in differentdimensions, with an attempt to set up individual countryprofiles where sufficient information was available.
Measures of positive mental health do differ significantlybetween European countries. Similarly, measurement ofpsychological distress in the two European surveysshows significant differences between Member States.After controlling for major socio-demographic variables,differences also appear for most of the psychiatricdisorders across the countries involved in the surveys.However, there are quite different patterns whenconsidering these three dimensions and this underlinesthe necessity of collecting information on diversedimensions (Section 3).
Suicide varies across Europe, ranging from 3 deaths per100,000 in Greece to 24 deaths per 100,000 in Finland.Although males have higher suicide rates, the ratio ofmale:female suicides differs across countries as well as therelative proportion of younger and older people whocommitted suicide.
6
T H E S T A T E O F M E N T A L H E A L T H I N T H E E U R O P E A N U N I O N
Executive Summary
Since methods for collecting suicide data are not totallyidentical, data on deaths whose suicidal intention isdoubtful (deaths from events of undetermined intent)have been compared as well.
In general, suicide rates have dropped across Europe in thelast 20 years. In all countries a decreased trend is observedfor suicide in males with the exception of Ireland and, toa lesser degree, of Spain and Luxembourg. This decreasingtrend is stronger for suicides among women.
Alcohol, tobacco and drug use all vary between MemberStates. Alcohol-related problems are responsible foraround nine per cent of Europe’s total burden of disease.Cigarette smoking is also relevant to mental healthbecause nicotine dependence has been defined as anaddictive disorder. Use of illicit drugs varies from countryto country and different usage patterns are also reflectedin national differences in acute drug-related deaths.
Since mental health surveys results have to beinterpreted with caution, a promising way to makecomparisons is to compare risk groups across countries.The main relevant factors are gender, age, marital status,employment, socio-economic status, rural-urban place ofliving and immigration status (See Section 4).
Important differences are reported concerning the relativerisk of women for psychological distress and depressiveand anxiety disorders across countries. Similarly, there aredifferences for young people in some countries. Data onthe older population were more difficult to compare fordepressive disorders, as well as for cognitive disorders,although they will represent a major challenge for eachcountry. To be divorced or to live alone is also a risk factorall around the EU, as are unemployment and poverty butthe magnitude of these risks varies. Data on urban/ruralcomparisons are more difficult to compare, partiallybecause socio-demographic compositions of the twopopulations are different and also because uniformdefinitions of what constitutes rural and what is urbanhave to be found. Very few data exist to allow comparisonson immigrant mental health status across countries.
The extent to which people seek help for any mentalhealth problems, who they seek help from and what helpis on offer also differ throughout the EU. Human andmaterial resources are different, quantitatively andqualitatively, across the EU. The reported use of care andhealth seeking behaviour, however, does not fit theavailability of resources and differs remarkably acrosscountries as does the type of help sought. Similarly, therelationships between the primary care system, which is themost frequent provider in all countries, and the specialisedmental health system are very different. Consequently, thetype of care provided varies too (Section 5).
Thanks to the ESEMeD and Eurobarometer surveys, it ispossible to present a complex picture of mental health insix countries, by putting together all available indicators.
This report demonstrates that comparisons of mentalhealth, and its socio-economic determinants, areessential and feasible. Yet such comparisons should beinterpreted with caution, at least until data is collectedin a more comparable manner across Europe.
Widespread, although not universal, improvements insome indicators, such as suicide or alcohol consumption,point to effective public health policies. The effectivenessof these interventions should encourage the remainingcountries, including the new Member States, to introducesimilar policies.
Comparisons of the different mental health provisionpatterns may also be fruitful for EU countries.
The report recommends that, at the EU level:
• information be collected about mental health acrossthe EU in an appropriate way to enable validcomparisons. EU level surveys have to be set upincluding longitudinal surveys and surveys on children,adolescents, immigrants and older populations. Datacollected in various surveys such as labour force surveysshould include a mental health component developed incollaboration with mental health surveys experts
• a report on mental health which collects and comparesdata from all sources, and which includes the enlargedEurope, should be produced on a regular basis in orderto stimulate common efforts across the Member States
Many of the above recommendations apply at thenational level as well as at the EU level. In addition,some further recommendations are made at MemberState level. These stress the importance of:
• implementing EU data collection guidelines andinstruments in each health-related survey and ofconducting mental health surveys accordingly atregular periods.
7
T H E S T A T E O F M E N T A L H E A L T H I N T H E E U R O P E A N U N I O N
It is increasingly evident that mental health problems area major public health burden. In the last few years, theworld has become more aware of this enormous burdenand the tremendous potential for mental health gains.
This project aimed to produce a report on the state ofmental health in the European Union and Norway and tostimulate the collection of further data on mental healthacross Europe.
This report describes and compares the state of mentalhealth in the various Member States and proposes abasis for relevant programmes for the promotion of goodmental health and the prevention of risk factors.Comparison of information on mental health betweencountries will enable Member States to improve theirunderstanding of mental health issues and to planappropriate policy responses.
1.1 Mental health and mental illness
Since mental health is a rather broad concept, abackground project was designed: the 'Key Concepts'project, was carried out in 1997 in order to ‘develop andevaluate the best options for the key concepts of mentalhealth promotion in Europe’.
This project considered that mental health has a positiveand a negative dimension. The positive dimension refersto the concepts of well-being and ability to cope in theface of adversity. This encompasses various dimensions
including: self-esteem, internal locus of control ormastery, optimism, and sense of coherence, to mentionthe most frequently measured.
The negative dimension relates to the presence ofsymptoms defined as psychological distress as well as to mental disorders. These mental disorders are defined through recognised classifications such as theInternational Classification of Disease (ICD10) or theDiagnostic Statistical Manual Version IV (DSM IV). In thisreport, all the disorders included in Chapter 5 of ICD10 areconsidered as mental disorders: organic mental disorders,deficiencies and dementias (whatever their cause),psychotic disorders, depressive and anxiety disorders,substance use disorders, personality and conduct disordersand eating disorders. Although disorders in children areincluded in Chapter 5, in this report only adult disorderswill be considered. Chapter 5 concerns psychiatricdisorders only and does not include any neurologicaldisorders from degenerative or traumatic origin.
It is important to clarify the relationship betweenpsychological distress and mental disorders. Psychologicaldistress refers to the presence of symptoms which aremainly types of depression or anxiety. These symptoms are usually measured by ‘checklists’ which produce a score by adding up the answers to the various questions.Psychological distress is, therefore, a continuousdimension. The symptoms are rather common and could betransient, for example, following a negative or stressfullife event. However, most of the time the person does notfit into a psychiatric diagnostic category and probably
8
1
I N T R O D U C T I O N
Introduction
The need for information on mental health in Europe has beenemphasised in the Public Health Policy, the Health MonitoringProgramme and the Public Health Programme (2003–2008) of theEuropean Commission.1 Problems relating to mental health are a public health priority: the social and economic costs of depression,for example, are of huge importance since depression will be, in a fewyears, the disease group with the second heaviest toll globally.2 Moreover,there is no good health without good mental health. Mental health isthus crucial to the well-being of individuals and societies.
1
never will. Those who are defined as having psychiatricdisorders, however, do usually also score highly on thepsychological distress checklist.
Psychiatric diagnoses on the other hand, are discreteentities described in classification through syndromes.These syndromes are a cluster of symptoms whoseduration, severity, and impairment on daily lifecorrespond to different diagnoses which usually relate toa need for care, either primary care or psychiatric care.
For each of these three dimensions, there are variousmeasurement instruments: positive mental health andpsychological distress are measured by checklists, while the categorical diagnoses are measured throughdiagnostic instruments which follow, as closely aspossible, the classifications which they aim to produce.
The report of the ‘Key Concepts’ project favoured amultidimensional approach where mental health wasconceived as an indivisible part of general health whichreflects the interaction between the individual and theenvironment.3 Mental health is influenced by a widerange of factors. These include individual biological and psychological factors, social interaction, societalstructures or resources and cultural values. This currentreport is based on the ‘functional model‘ of mentalhealth (Figure 1), which illustrates these interactions.
Crucial demographic factors which relate to mental healthare sex, age, marital status, ethnicity and socio-economicstatus. Socio-demographic factors can combine withpersonality characteristics to influence the onset, course,restitution and relapse of disorders in various ways.
Social networks and, especially, close confidingrelationships, can act protectively or as risk factors forthe onset and recurrence of mental ill health and mayaffect the course of an episode of illness. Perceivedsocial support, or a lack of it, has an effect on mentalhealth. Negative pressure from, or interaction with,social networks can also have an impact. Social supportshould not, however, be treated solely as anenvironmental factor as it is linked to other factors, suchas personality features.
Major occurrences in a person’s life that require somepsychological adjustment can be risk factors for mentalill health. These adverse ‘life events’, such as loss of apartner or of a job, can interact with other determinantsto have an effect on mental health. In addition, manylong lasting difficulties such as disability – either ofoneself or of someone close – or major financialproblems can result in chronic mental disorders.
The public health implications of the functional model ofmental health shown in Figure 1 are many. This modelstresses the importance of:
• prevention and health promotion in mental healthand the necessity of improving living conditions invarious areas: education, housing, employment,access to leisure and culture, human rights and healthcare organisation (especially the training of healthprofessionals to deal with psychological suffering),
• providing adequate care to those who need it and tocarefully allocate specialised and non-specialisedresources, according to the severity of disorders inorder to optimise resource use,
• providing adequate medical and social resources tothe severely mentally ill, and of minimisingdiscrimination, and of integrating people with severemental illness fully into society and helping theirfamily and friends to support them.
It is hoped that comparisons between the variousMember States may facilitate exchange of experiencesand of practices and that ultimately this will improve thesituation for the EU as a whole.
Figure 1. Determinants of mental health
Source: Korkelia et al, 20033
1.2 Burden of mental illness
Mental health is crucial to the overall well-being of individuals, societies and countries. The magnitude,suffering and burden in terms of disability and costs for individuals, families and societies are staggering.2Globally, it is estimated that as many as 450 millionpeople suffer from a mental or behavioural disorder andnearly one million people commit suicide each year.One in four families have at least one member with amental disorder.
PRECIPITATINGFACTORS
e.g.life events
MENTAL HEALTHIndividual resources
PRESENT SOCIALCONTEXT
e.g. social support
CONSEQUENCESPREDISPOSINGFACTORS• genetic factors• factors related
pregnancy and birth• early childhood
experiences• family environment• social circumstances• physical environment• education• employment• work conditions• housing
• level of wellbeing• physical health• psychiatric symptoms• knowledge & skills• quality of
relationships• sexual satisfaction• use of services• productivity• public • morbidity: substance
misuse • burden on family
and friends• social handicap
safety
SOCIETY & CULTURE
9
1
I N T R O D U C T I O N
According to the World Health Organization’s GlobalBurden of Disease project in 2001, one third of the years lived with disability are due to neuropsychiatricdisorders and a further 2.1% are associated withintentional injuries.2 Four of the six leading causes ofyears lived with disability are due to neuropsychiatricdisorders (depression, alcohol use disorders, schizophreniaand bipolar disorders).
Depression alone causes over 12% of the years lived withdisability globally, and ranks as the third leadingcontributor to the global burden of disease. More than150 million persons suffer from depression at any pointin time. About 25 million suffer from schizophrenia andmore than 90 million suffer from an alcohol or drugrelated problem. In 2000, more than 1.8 million deathswere attributed to alcohol related risks and 205,000deaths were attributed to illicit drug use.
Dementia presents another enormous challenge forEurope’s health and social care systems. There were anestimated 7.1 million cases of dementia in Europe in2000, and dementia is the principal cause of disabilityamong the elderly.
It is increasingly clear that mental health and physicalhealth are interconnected. A number of mentaldisorders, such as depression, anxiety or substanceabuse, are more common in people suffering fromcommunicable and non-communicable diseases. Andpeople suffering from chronic physical health problemsare more likely to develop mental disorders such asdepression. While in the general population theprevalence of major depression can range from three to10%, it is consistently higher in people affected by chronic disease. In people suffering from high blood pressure, for example, the prevalence of majordepression is up to 29%. In people living with HIV/AIDSthe prevalence is as high as 44%. Rates of suicide arealso higher among people with physical health problemsthan among other people. This co-morbidity – when aperson is suffering from two medical conditions at thesame time – has important consequences. People withco-morbid depression, for example, are less likely toadhere to medical treatment or recommendations, andare at increased risk of death or disability.
Given the prevalence of mental health and substancedependence problems, the emotional, but also thefinancial burden, on individuals, their families andsocieties is enormous. The economic impact of mentalillness includes the effects on personal income, onability to work (for individuals and for carers) and tomake productive contributions to the national economy,as well as the use of health and support services.
In the Member States of the European Union the cost ofmental health problems is estimated to be between 3%and 4% of gross national product. Of this, healthcarecosts account for an average of 2% of GNP. Studies have also shown that the relative and absolute costs oftreating chronic disease conditions, such as psychosisand neurosis, are comparatively high when contrastedwith a wide range of health disorders. The average annualcosts, including medical, pharmaceutical and disabilitycosts, for employees with depression are estimated as upto 4.2 times higher than costs for people with otherconditions. In the United Kingdom, for example, a studyinto the aggregate costs of all mental disordersestimated the total as 44.8 million euros.
An important characteristic of mental health is thatmental disorders often start at a relatively young ageand mortality from these disorders is relatively low. Thismeans that people can live for a long time with theeffects of mental ill-health and that the indirect costs,from lost or reduced productivity in the workplace, are high.
Similarly, it is known that the costs of mental healthproblems in childhood are large and largely hidden.Research from the UK shows the substantial additionalcosts generated by children with conduct disorders from ages 10 to 27 years in terms of education andcriminal justice.
1.3 Why publish a European report on mental health?
Health issues have belonged to the competence of theEuropean Community for a relatively short time. Healthwas mentioned in this sense for the first time in the1993 Maastricht Treaty in article 129:
‘The Community is to make a contribution towardsensuring a high level of health protection by 1) theencouragement of cooperation between the MemberStates and, if necessary, the provision of support to theiractions; 2) the promotion of policies and programmes ofthe Member States in the areas of disease prevention,research into causes and transmission of diseases, healthinformation and health education; and 3) fostering of co-operation with third countries and the competentinternational organisations in the sphere of public health.’
Further Treaties of the European Union have built on thisEuropean competence in public health. The 1997 Treatyof Amsterdam focused on health protection and diseaseprevention and identified the need for further actions to
10
1
I N T R O D U C T I O N
‘achieve improvements in public health’ as well asactivities to ‘prevent diseases and health problems’ andthe ‘reduction of risks to human health’.
Based on the mandate for public health established in Maastricht, the Commission of the EuropeanCommunities published in 1993 the Public HealthFramework Programme with its eight action programmes.This was adopted by the Parliament and Council inDecember 1995 and started in 1996.
Within the Public Health Framework Programme, anaction programme on health monitoring was launched inthe European Union and Norway. The main objectives ofthis Programme, which was adopted by the Parliament inJune 1997, were:
• to establish a set of Community (core andbackground) health indicators for monitoring healthin the Community that would facilitate the planning,monitoring and evaluation of Community programmesand actions, and that would provide added value toMember States’ own health information systems, thussupporting the development of national health policies;
• to specify the content of a network to be set up forthe collection and dissemination of health data andindicators, mainly with the aid of telematics; and
• to establish a capacity to undertake analyses, and tosupport the preparation and dissemination of reportson health status, trends and determinants and theimpact of policies.
Mental health was mentioned under the heading‘Functioning and Quality of Life’ as one area for whichhealth indicators might be established under a futureCommunity health monitoring system.
This, in turn, stimulated a number of projects in themental health field, financed by the EuropeanCommission, which have made an important contributionto this report. Specifically, this has included somecomparative community surveys, such as ODIN3, a largeEuropean survey (ESEMED)5, plus the addition of amental health part to the Eurobarometer survey in 2002.6
A project entitled Putting Mental Health on the EuropeanAgenda was carried out between 1998 and 2000. Thisproject outlined a public health approach for mentalhealth in Europe proposing a framework for mentalhealth policy in the European Union, published in thebook Public Health Approach on Mental Health in Europe.
The project strongly stressed the need to shift the focusof mental health. First, as a major contributor to healthand well-being, mental health needs to be brought out
from professional, organisational and political isolationinto the broader sphere of public health. Second, instead of concentrating on mental health at the level of individuals, it is important to strengthen thepopulation-level mental health approach. Third, there isa need to shift the understanding of mental health,which traditionally has focused on mental disorders.Instead of looking only at the negative side of mentalhealth, contemporary thinking and actions must drawattention to positive mental health.
In September 2002, a new public health programme wasadopted for the years 2003–2008.1 The generalobjectives of this programme are:
• to improve information and knowledge for thedevelopment of public health,
• to enhance the capability of responding rapidly andin a coordinated fashion to health threats, and
• to promote health and prevent disease throughaddressing health determinants across all policies.
Based on this new programme, the European Commissionhas identified its priority work areas. These include somecross-cutting themes such as health impact assessmentand tackling health inequalities. Other priorities relateto health information (including a working party formental health monitoring), to specific health threats andto health determinants, of which mental health is one.
The existing network of people concerned with mentalhealth in Europe, the European Network on MentalHealth Policy (ENMHPO), produced a framework andproposed key concepts and indicators relevant to goodmental health.3 The aim of this report is to build on thework of the ENMHPO and to expand the frameworkwithin the European Union.
The publication of this report on mental health isimportant in order to find out more about mental healthand its determinants. This report will enable overallcomparisons to be made and will enable people incharge of policies, analysts and researchers of theMember States to instigate their own preventionprogrammes. This report should also stimulate furtherprojects on mental health in Europe.
11
1
I N T R O D U C T I O N
2.1 Context of mental health in Europe
For many individuals within any one country of the EU,the diversity of European culture may seem the moststriking feature, and, indeed, there is incontrovertiblediversity. The differences of which most of us are aware(with the exception of language) are largely in rathersmall-scale traditional features of everyday life, whichimportantly define our identity and sense of belonging,and vary significantly within, as well as between, nation states.
Yet, looked at from outside, Europe may seemremarkably homogeneous. Profound changes have beentaking place across Europe as a whole, varying in paceand degree, but essentially similar in all countries.Changes in the nature of work increasingly emphasiseservices and communications rather than manufacturingand agriculture. The place of work in people’s lives haschanged, to provide a great deal more leisure time,which, together with the mechanisation of domestictasks, higher levels of disposable income and cheap andeasy travel, has provoked a huge tourist industry almosteverywhere. Communications – telephone, fax, e-mail,radio, television and internet – have opened up theworld, especially for younger people, even in remoterural areas.
Marriage, divorce and co-habitation, have changedthroughout the continent, apparently independent ofreligious traditions. First births are later and family sizeis smaller everywhere. In all countries, concurrent withthe reduction in children, there is a huge and growingincrease in elderly people, but they are fitter andhealthier for much longer. These changes in the make upof the population present serious challenges in relationto retirement and pensions right across Europe.
All of the features mentioned above, and many more, haveprofound implications for mental health – the experienceof ordinary people, the challenges of prevention, and theorganisation of treatment and care. These are importantissues where exchange of information and experience canbring significant benefits.
2.1.1 Population
In most countries there are very wide variations indensity of population, yet urbanisation continues itsapparently irresistible progress.
Figure 2.Population Density in the EU and NorwayAverage Population Density per square km, 2001
Source: WHO Health for All Database1
Figure 3. Urban Population in the EU and NorwayPercentage of Population Living in Urban Environment, 2001
Source: WHO Health for All Database
0
10
20
30
40
50
60
70
80
90
100
Austr
ia
Belgi
um
Denm
ark
Finla
ndFr
ance
Germ
any
Gree
ce
Irelan
dItaly
Luxe
mbo
urg
Neth
erlan
ds
Norw
ay
Portu
galSp
ainSwed
enUn
ited
King
dom
2001
0
100
200
300
400
500
Austr
ia
Belgi
um
Denm
ark
Finla
ndFr
ance
Germ
any
Gree
ce
Irelan
d
Italy
Luxe
mbo
urg
Neth
erlan
ds
Norw
ay
Portu
gal
Spain
Swed
en
Unite
d Ki
ngdo
m
2001
12
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
Comparing mental health in Europe
2
Immigration has also been a feature of most EUcountries in the last few decades and most migrantssettle also in towns.
Everywhere there are issues of multi-culturalism andassimilation, legal and illegal residents and citizenship,participation, discrimination and disadvantage. Thereare risks to both general health and mental healthattached to immigrant status, and to experience ofsocial exclusion, made more difficult by seriouscommunication problems related to alien languages andcultures (see Section 4.6).
In many countries of Europe there is concern about lowfertility, some failing to reach replacement level. OECDfigures for 2000 show Spain, Italy, Greece, Austria andGermany with very low rates (between 1.22 and 1.34births per women aged 15–49). The highest rates werefound in France and Ireland (1.89 births per woman).Alongside this, life expectancy has been increasing at allages. In most European countries 15-20% of thepopulation is aged 65 or more and about 4% aged 80 or more. The exceptions with lower proportions ofpopulation aged 65 or more in 1997 were Ireland,Netherlands and Luxembourg. Children under 15generally make up less than 20% of the population.
Figure 4. Population Aged over 65 in the EU and NorwayPercentage of population aged over 65, 1997
Source: WHO Health for All Database
This holds the prospect of increasing imbalance ofpopulations in favour of the elderly. As the proportion ofelderly people increases, high dependency levels aremaintained even where the proportion of childrendecreases. This probably means that people reachingtraditional retirement age will need to continue working– they are, in general much fitter and healthier thanprevious generations and face much longer retirement
prospects. It certainly means increasing numbers ofpeople with dementia and increasing numbers of carers,often themselves elderly and vulnerable (see Section4.2). It should also mean that children are more valued,but also that child deaths, now rare, are more tragic intheir effects on families.
The low birth and fertility rates are no doubt related toincreasingly late marriage, at least among middle-income groups. In all groups, and apparently in allcountries, marriage has become much less common, andco-habiting has become very common, whether short-term, anticipating marriage, or long-term. This hascreated havoc with marital status statistics, so that it is difficult to know what health associations there noware. Divorce has also become far more frequent, andliving alone consequently more common, needing moreindependent housing. This is often accompanied by alack of social support, especially of close confidingrelationships known to be protective in mental healthterms. Children increasingly have broken and multiplefamilies; it is not yet clear what mental healthconsequences there may be on a whole population scale.
In general, deaths from the main causes – heart disease,cerebro-vascular disease and malignancies – are falling.Virtually all European countries can point to year on yearincreases in life expectancy from birth (which deriveslargely from substantial improvements in peri-natal andinfant mortality), and in life expectancy from age 65 and80. Whatever the perceived problems, this represents ahuge success for both socio-economic improvement andhealth care systems. However, there are sub-groups thatdo not share these improvements to the full.
2.1.2 Economy
In a global context, all countries in the EU are relativelywealthy, with thriving economies and most aredesignated high income countries by the World Bank.Figures from the Organisation for Economic Co-operationand Development (OECD) showed only Greece, Portugaland Spain with significantly lower gross domesticproduct (GDP) in terms of dollars per capita aspurchasing power parity. This is confirmed by data fromWHO. The outstanding GDP of Luxembourg, which is thehighest in Europe, is presumably related to itsinternational status and the very high proportion of non-Luxembourgeois working there. It will be noted later theeffect this has on measures of health spending. Irelandhas the second highest GDP and this illustrates therelatively recent economic boom, and, perhaps, therelatively low proportion of elderly, non-productive people.
0
5
10
15
20
Austr
iaBe
lgium
Denm
ark
Finla
ndFran
ce
Germ
any
Gree
ce
Irelan
d
Italy
Luxe
mbo
urg
Neth
erlan
dsNo
rway
Portu
gal
Spain
Swed
en
Unite
d Ki
ngdo
m
1997
13
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
Yet, in almost all countries there are regions of pooreconomic performance, with relatively low familyincomes, high rates of unemployment, inadequateeducation, and limited opportunities. And there areethnic minorities or other distinct sub-groups in thepopulation who are also disadvantaged in these variousways. Since these features are linked at the populationlevel to higher prevalence rates of the common mentaldisorders, there are obvious implications for bothprevention and care.
Unemployment rates vary across Europe. But thesenational rates mask those regional and sub-groupvariations mentioned above. For example a rate of 10.4%in Germany masks 8.2% in the old ‘West’ and 18.6% inthe old ‘East’. In Italy, the overall rate hides the fact thatthere is a very high rate of unemployment in youngadults (age 15-24) nationwide, and particularly in youngadults in the South. Unemployment figures show onlypart of the picture of non-employment, and the rest ofthe picture will no doubt be very different in differentcountries. In Sweden, for example, alongside 4.7%unemployment among the workforce aged 16-64 years,we must also consider that there are 13.1% receivingsickness benefit, and therefore temporarily not working,and 8.0% receiving a disability pension, and thereforepermanently not working.
In many countries, as the economy has expanded, thereis concern about increasing gaps between rich and poor.The poor may increasingly include old people unless thepensions crisis currently experienced or anticipated bymost countries is resolved. Apart from social justice andequity, resolution of this issue is thus needed to avoidpotentially huge health and social care burdens oncommunities in the future with ageing populations.
Data on the proportion of population at risk of povertyare available from the EU’s New Cronos databank. Thepercentage of population below 60% of the medianequivalsed income after social transfers ranges from 10% in Sweden to over 20% in Ireland (Figure 5). These data must be interpreted cautiously, however, as theproportions given relate to each country's GDP. Being atrisk of poverty by this measure is, therefore, very differentin, for example, Luxembourg and Greece.
Figure 5. Gross Domestic Product, Unemployment andPopulation at Risk of Poverty Gross domestic product, purchasing power parity thousanddollars per capita, percentage unemployment andpercentage of population below 60% of the medianequivalised income after social transfers
Source: Eurostat New Cronos2 and OECD statistics3
2.1.3 Financing health care
There is great diversity in the health care systems ofdifferent countries within the EU, but there are somecommon themes. Total health spending varies; the highestcountries are Germany and France, the lowest Luxembourgand Ireland. However, if measured by per capita spendingper year as purchasing power parity (ppp), Luxembourg,with the lowest proportion of GDP, was the highest($2,613) in 1999 because of its very high GDP. By 2000,Germany had slightly exceeded Luxembourg (Figure 6). In2000, Spain, Portugal and Greece were the lowest, withexpenditure of around $1,400).
Figure 6. Health Expenditure in EU Countries and NorwayTotal health expenditure, purchasing power parity dollarsper capita, WHO estimates, 2000
Source: WHO Health for All Database
0
1000
2000
3000
4000
Austr
ia
Belgi
umDe
nmar
k
Finla
ndFr
anceG
erm
any
Gree
ceIrelan
dIta
ly
Luxe
mbo
urg
Neth
erlan
ds
Norw
ay
Portu
gal
Spain
Swed
en
Unite
d Ki
ngdo
m
2000
0
10
20
30
40
50
60
Luxe
mbou
rg
Irelan
d
Denm
ark
Nethe
rland
s
Austr
ia
Belgi
um
Germ
any
Italy
Finlan
d
Swed
en
Unite
d King
dom
Fran
ceSp
ain
Portu
gal
Gree
ce
GD
P P
PP
US
$ pe
r ca
pita
(th
ousa
nds)
0
5
10
15
20
25
Un
em
plo
yme
nt
Pe
rce
nta
ge
GDP Unemployment Risk of poverty
14
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
All countries appear to have been increasing their healthexpenditure over the last few years, but even large extrasums of money for health care as, for example, in the UK,take a very long time to work their way through thesystem to produce recognisable improvements. However,there is an overlap between 'health' and 'social'spending, especially in relation to long-term illness anddisability, not least in respect of mental illness. Fewcountries give the relevant social budget, but it is clear,for Germany and Sweden at least, that it is very large andmay be of a similar order to the overt 'health' budget. Nodoubt it is much less in some other countries.
The mixture of health care funding sources – fromtaxation, national or compulsory insurance, privateinsurance and direct patient payments – varies.Therefore, the proportions of total health expenditurethat are public and private also vary. High proportions ofpublic spending are now the norm in Europe, and theseare often very high proportions. The corollary is avariable private sector which, however, is mostcommonly an option for relatively affluent people, whocan afford it in a situation where they are alreadycovered by a national system of health care.
In every country there appear to be direct payments bypatients for some aspects of health care. This is probablymost common in respect of drugs, social care and dentalcare, but a few countries have charges for hospitalattendance or even GP consultations. In these casesthere are exemptions for poorer people. For example, inIreland where a fee is charged to see a GP, about onethird of the population have free medical cards. Ashealth budgets are under pressure everywhere, there is astrong impression that patient direct payments aretending to increase in many health care systems. This ismade explicit in a recent reform plan for health care inGermany. Although Sweden's comprehensive health andsocial care system is funded out of taxation, about 30%of the total health spend comes from direct patientpayments. Mental health is usually fully encompassed by national financial systems, whether insurance basedor tax based, but may not be covered by privateinsurance systems.
2.2 Methodology for comparing mentalhealth in Europe
This project has involved representatives from all EUcountries plus Norway, WHO Europe, a representative ofa non-governmental organisation (Mental Health Europe)and a representative of OECD Europe. See the list ofparticipants and contributors on page 5.
Each country representative was asked to prepare areport on all the surveys on mental health which hadbeen carried out in their country. In addition, theexperts were asked to prepare a report on the mainfeatures of their country, its health system andparticular issues relating to the mental health domain.
2.2.1 Methodology of this report
The aim of this report is to describe mental healthstatus, and its determinants, across Europe. As dataalready exist concerning psychiatric care systems, theemphasis is on epidemiological data.
Mental health and mental health needs can be measuredat both individual and population levels. These may beassessed using techniques such as surveys, analyses ofroutinely collected data, analyses of socio-economicindicators and combinations of these techniques. Healthand healthcare may be measured by various indicators.
This report has been prepared combining two main kindsof data:
• Routinely collected statistics• Results from general population surveys
2.2.1.1 Routinely collected statistics
This report followed the recommendations of the MentalHealth Indicators project.x This report presents ananalytical comparison of some macro indicatorscollected routinely from institutional sources in Europe.The objective is a general description of mental healthstatus, which includes well being, in the European Unionand Norway using officially available statistics.Monitoring a set of routine indicators could allow a goodgeneral framework and may provide a source ofhypotheses.
A review of macro indicators collected routinely frominstitutional sources such as World Health Organization(WHO), Organization for Economic Cooperation andDevelopment (OECD) and from EUROSTAT (particularlythe New Cronos databank) was carried out. Indicatorswhich could help illustrate mental health status, and theavailability of psychiatric care, for European countrieswere chosen.
Tables and figures are presented throughout the reportto enable internal comparisons within each country(trends over time) and between different Member States.Reliability of results may sometimes be doubtfulbetween countries but the measure of the temporaltrends in each nation allows methodologically safercomparisons.
15
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
SuicideSuicide mortality statistics were collected using theInternational Classification of Disease (ICD) 10 group‘Suicide and intentional self harm’. Suicide data areavailable from different sources: the OECD databank2,the WHO Health for All database1 and from Eurostat(New Cronos)3. The majority of data used in this reportare taken from the WHO Health for All Database.
Deaths due to events of undetermined intentThe Eurostat databank was used to provide rates for maleand female deaths due to events of undetermined intent.These figures are important because artefacts of deathregistration and disparities in the procedures fordetermining suicide may contribute to the internationaldiscrepancies in suicide rates. Rates of deaths due toevents of undetermined intent were therefore presentedas well as suicide rates.
Alcohol consumptionAt the population level the crude rate of the consumptionof alcohol and alcoholic beverages is measured per capita (litres of alcohol per person per year). The alcoholconsumption is calculated as the difference betweenproduction, alcohol imported and alcohol exported.
There are several reasons why these data should betreated with caution. On one hand, a country’s entirepopulation, irrespective of age, is sometimes used to calculate per capita consumption. This leads to areduction in the estimated average figures for the agegroups among which consumption is actually highest.On the other hand, consumption calculations are basedon statistics for the production and sale of differentalcoholic drinks, and this can lead to overvaluation(drinks that are produced but not consumed) and/orunder-valuation (undeclared or illegal production, drinksimported by tourists, countries with a high proportion of children and/or young people in general). Per capitadata thus provide us with what is, at best, an estimateof alcohol consumption, but not exact figures, howeverclose the approximation may be.
Data on alcohol consumption were taken from the WHOHealth for All Database for the sake of consistency, sincethe HFA database is a key source throughout this report.The WHO has also, however, been developing the GlobalAlcohol Database4 since 1997 and this contains a hugeamount of suitably treated and analysed information onthe most important indicators in this field.
When consumption trends from both sources are comparedit is interesting to note that, despite the fact that theGlobal Alcohol Database figures (weighted estimate forpeople over the age of 15 only) are higher than those fromthe Health for All database, both reveal the same trends.
Drug useData relating to drug use were taken from the 2002 and2003 reports of the European Monitoring Centre for Drugsand Drug Addiction (EMCDDA)5 which provides an annualoverview of the drug phenomenon in the European Unionand Norway. The data used in this report relate to trendsin drug use and trends in acute drug related deaths.
Mental health care resourcesThis project did not set out to describe the diversehealth systems across Europe. It was consideredrelevant, however, to bring in some data concerninghealth care resources; WHO data for general practitionersand psychiatric beds and Eurostat (New Cronos) forpsychiatrists.
Pharmaceutical drug useComparing psychotropic drug use across countries is notan easy task. Pharmaceutical companies provide data onthe spending in euros by country and by inhabitants and the data could be presented in categories (ATCclassification). In this way, antidepressants, sedative/anxiolytics and antipsychotics drugs can be identified.However the data are provided by a paid-for servicecompany (IMS) and are costly to obtain. In addition,this indicator reflects diverse prices so it does notreflect differences in consumption in countries.
The same company provides another indicator from arepresentative panel of physicians which is the numberof prescriptions by ATC. In this case, the data are basedon prescription analysis and one prescription couldconcern either a short or a long period of care, so theymay correspond to rather different number of units,Furthermore, hospital consumption is not taken into account.
To avoid all these biases the Defined Daily Dose system(DDD/1000 inhabitants) is supposed to be the standardas it uses total mg of product sold in a country by thestandard dosage for a day‘s treatment and reports it per1,000 inhabitants.
The EU has set up a website on this – Euromedicine –but unfortunately the DDD data are not available for allcountries. And some challenges remain with the DDDsystem. A standard dose for antidepressants, for example,is not easy to define since this may be different forindividual antidepressants.
This report presents data from all three approaches:
• Per capita euros expenditure• Number of prescriptions per inhabitant• Defined daily dose per 1,000 inhabitants
16
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
2.2.1.2 General population surveys
General population surveys are extremely importantwhen it comes to collecting mental health morbiditydata. This is because routinely collected statistics ondeaths related to mental health problems do not reflectthe reality of mental health. Nor do hospital dischargedata. These statistics contain no information on thelarge numbers of people who suffer from mental healthproblems but neither die nor are hospitalised as a result.
Comparison between surveys is difficult since thisrequires identical sampling design and use ofinstruments, including identical training for interviewersand diagnostic construction.
Instruments to measure mental healthAs previously described, mental health can be describedin three complementary dimensions. These are positivemental health (well-being) and negative mental health,which includes psychological distress and psychiatricdisorders.
Some instruments are actually designed to produceanswers which correspond to diagnoses of mentaldisorders. The Composite International DiagnosticInterview (CIDI), for example, is a diagnostic instrumentwhich is capable of uncovering a wide variety ofdiagnose. In general population surveys, however, it maybe limited to mood disorders, anxiety disorders and drug and alcohol disorders. These surveys will generateestimates of prevalence of particular disorders.
Other instruments measure more generic factors such as‘psychological distress’ by recording the presence orabsence of some symptoms, such as those of anxiety ordepression. This type of instrument produces a mentalhealth score, and for some of them cut-off points can beused to categorise people into groups such as ‘probablecases’ with mental health disorders. Instruments in thiscategory include the General Health Questionnaire (GHQ),the MHI-5 which is a sub-scale of a widely used genericinstrument, the Short-Form 36 (SF-36). The SF36 includessome positive mental health dimensions and somequestions on impairment due to mental health problems.The SF-12 has been derived from the SF-36 and includes ascore to evaluate mental health.
This report presents results derived using variousinstruments. Each instruments has been selectedbecause either the survey of surveys revealed that it wasone of the most commonly used instruments or becauseit was included in one of the two Europe-wide surveyswhose results are presented in the following chapters.The instruments presented are:
• Diagnoses of mood disorders, anxiety disorders andalcohol disorders derived using the CIDI interviewtool
• Positive mental health as assessed by the vitalitysubscale of the SF36 questionnaire
• Psychological distress as measured by the MHI-5 sub-scale of the SF-36 and as measured by the SF-12mental health sub-scale
• Risk of poor mental health as measured by the generalhealth questionnaire (GHQ-12) which identifiespeople with a ‘probable mental health problem’
There are difficulties when using mental health surveyinstruments across different countries and cultures.Some rules should be applied when translatinginstruments, such as those edited by WHO, and manyinstruments have validated versions in many languages.However, where there is careful translation, it has to bestressed that the interpretation of comparison results isdifficult. Differences could be either genuine mentalhealth differences, the expression of cultural differencesin the expression of symptoms or both. This is thedilemma of comparative psychiatry which is relevantthroughout this report.
Survey design issuesIn addition to the choice of instrument and classificationsystem, and the difficulties with translation ofinstruments, there are other important factors relating tosurvey design. These include:
• Source of sampling• Sampling design • Participation (response) rate• Weighting system• Translation of instruments • The setting of cut-off points
The issues outlined above have important consequenceson the reliability and applicability of survey results inthe population surveyed, and have implications for the comparability of results between surveys (see below). Even in multi-country surveys there aredifficulties in ensuring consistent survey design andexecution across all participating countries.
17
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
A survey of surveysFor this report, surveys done at national, regional andlocal levels were identified by national experts and frompublished and unpublished literature. A form collecteddetailed information about every survey using specifiedmental health instruments,a including the populationcovered, socio-demographics, sampling methods,instruments, analytical methods, main results, and ifdata were available for secondary analyses. To try toensure full coverage, additional National Referees wereasked to review the information.
Information was collected on about 200 surveys. Theintention was to use the results of these surveys togeneralise about prevalence and associations with knownrisk factors, and to pool data from many surveys wherepossible, for meta-analysis. However, many surveys weresmall-scale local surveys, no doubt locally useful butinappropriate for generalisation. And the diversity ofsampling approach, methods, instruments, analysis,diagnostic classification and presentation of resultsamong the others was so great as to preclude even simplecomparisons except in a few cases. Meta-analysis couldbe attempted on only 19 studies, using one of threestandard instruments (the General Health Questionnaire(GHQ), the Composite International Diagnostic Interview(CIDI) and the Short Form 36 (SF-36) and that withrespect only to gender differentials. Annex 1 gives theprincipal characteristics of the selected studies.
The results of the meta-analysis were limited. The resultsmostly lacked statistical confidence, although they didconfirm previous research findings that women generallysuffer worse mental health than men across manydifferent countries and regions (see Section 4.1).
There is huge potential for invaluable comparative meta-analyses where there are many surveys covering thesame ground in countries across the EU. This potentialcannot currently be realised, however, becauseresearchers have not used the same methods. If themany surveys carried out across Europe were morestandardised to enable their findings to be pooled intoa more powerful analysis, then the results of each studywould be much more valuable. This exercise highlightsthe importance of an agreement on standard researchpractice, which would guarantee comparable data, toenable the discovery of differences in mental healthbetween different communities across Europe.
2.2.1.3 European surveys
In addition to the 200 national surveys examined for thesurvey of surveys, data were collated and compared froma number of European level surveys. These included the
mental health questions which were included in theOctober 2002 Eurobarometer survey and theESEMeD/MHEDEA 2000 Project.
The Eurobarometer SurveyThe European Commission funds the Eurobarometersurvey on a wide range of topics twice a year in all EUMember States and two separate regions (East Germanyand Northern Ireland).b In October 2002 a set ofquestions relating to mental health was included.xThese questions were standardised survey measures thathad been proposed by the European project on theestablishment of indicators for mental health monitoringin Europe. These measures related to either negative orpositive dimensions of mental health. The questionsincluded were:
• two sub-scales of the SF-36: MHI-5 (psychologicaldistress measure) and EVA (energy and vitality whichare positive mental health measures). A score of 52 orless on the MHI-5 scale is taken to indicatepsychological distress
• a question about whether respondents had soughthelp from somebody for a mental health problemduring the last 12 months,
• a question on social support, the 3-item Oslo socialsupport scale.
Response rates for the Eurobarometer survey in October2002 ranged from 23% (Great Britain) to 84% (France).In eight of the countries/regions, the response rate wasless than 50%. Thus, for this report countries whoseresponse rates were below 45% were excluded. Thus,Denmark, Greece, Ireland, Northern Ireland, Finland andGreat Britain were excluded.
Despite the methodological issues outlined above, theEurobarometer survey provides interesting informationon mental health status in different European countriesand use of mental health services.
ESEMeDThe ESEMeD/MHEDEA 2000 Project6 (European Study ofthe Epidemiology of Mental Disorders/Mental HealthDisability: a European Assessment in year 2000)comprised six European national surveys in Belgium,France, Germany, Italy, the Netherlands and Spain.c Thesurvey, hereafter referred to as ESEMeD, was partiallysupported by the European Commission.
ESEMeD used the CIDI interview tool (see Section2.2.1.2) to diagnose current or previous mental disordersand also used the SF-12 scale to assess psychologicaldistress. The overall crude response rate of this study was61.2% and within countries the weighted response
18
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
rate ranged from 45.9% in France to 78.6% in Spain. The response rates for Belgium, Germany, Italy and theNetherlands were 50.6, 57.8, 71.3 and 43.4 percentrespectively.
For the SF-12 analysis, we also added the results of aGreat Britain wide national survey carried out in 2000that also used the SF-12.7
These mental health factors were compared with socio-demographic variables and the use of health services.The socio-demographic composition of the sample groupvaried significantly between countries, except for theratio of men to women.
For this report, analyses were carried out to compare therisk of different disorders between countries and tocompare the effect of certain risk factors. These analyseswere adjusted to take into account these differences insex, age, living arrangements (married or living withsomeone or not) and whether people live in a urban orrural setting.
2.2.1.4 Country reports
In addition to this survey of surveys, which led tospecific comparisons, national experts were asked towrite a report on the main features of their country andits mental health care system. To support this nationalreport indicator data tables (including available OECD,WHO and EUROSTAT data) for each country, werecirculated to each national expert.
All of these country reports included some backgroundinformation about the population and economy of thecountry, and the general health care system. Thisbackground information is important to supply contextfor the description of mental health status, care,problems and issues. A compilation of these countryreports will be published separately.
19
2
C O M P A R I N G M E N T A L H E A L T H I N E U R O P E
Notes
a This included any survey using GHQ, SF-36 or SF-12,any form of CIDI, BDI and CESD.
b The Eurobarometer surveys cover the population aged15 years or over, resident in each of the MemberStates. The basic sample design applied in all MemberStates is a multi-stage, random probability one. Ineach EU country, a number of sampling points is drawnwith probability proportional to population size (for atotal coverage of the country) and to populationdensity. The net sample sizes are about 1,000 percountry/region except Luxembourg (about 600) andNorthern Ireland (about 300), giving a total netsample of about 16,000. All interviews are face to facein the respondent’s home, conducted by a nationalsurvey agency.
c The survey is a cross-sectional face to face householdinterview with probability samples representative of adult population of the six countries. The targetpopulation were individuals aged 18 years or olderresiding in private households. A stratified multi-stagerandom sample without replacement was drawn ineach country. In most countries the sampling framewas either a register of residents or postal registries.In France, however, an adjusted commercially obtainedlist of telephone numbers was used. For moreinformation on ESEMeD results see Acta PsychiatrScandin 2004; 109 (Suppl 420): 1-64.
Despite the importance of mental health in public healthterms, we still have a great deal to learn about the stateof mental health in Europe. This chapter brings togetherroutinely collected statistics on suicide, alcohol anddrugs and survey results on positive mental health,psychological distress and diagnosis of mental healthproblems to help develop a picture of mental healthstatus throughout Europe and to understand thedifferences between EU Member States.
Although there have been many surveys at the national orregional level, this chapter, focused on inter-countrycomparisons, places special emphasis on the results of tworecent European level surveys: Eurobarometer and ESEMeD.
3.1 Positive mental health
As described previously, mental health has a positivedimension which can be evaluated in many ways which arevery useful indicators for monitoring mental healthpromotion programmes. Unfortunately, despite the factthat measures of positive mental health have been stronglyrecommended, very few data on positive mental health, orwell being, have been published in Europe.
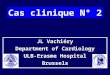
The few existing results come from the Eurobarometersurvey, which has used the vitality subscale of the SF36survey instrument (Figure 7).
Figure 7. Positive mental health in ten EU countriesScore on the vitality subscale of SF36 (0 to 100). The highest score has the highest positive mental health.Standardised against West German population.
Source: Eurobarometer1
Comparison of the different scores shows significantdifferences after some standardisation. Italy, Portugal,France and Sweden are in the lowest group and Belgium,Netherlands and Spain are in the highest. Germany,Austria and Luxembourg are in the middle.
It is interesting to note that positive mental healthscores, which are considered as reflecting a genuinedimension, do not correspond to the inverse of negativemental health as will be seen further on.
3.2 Negative mental health: psychologicaldistress and psychiatric disorders
Table 1 shows various survey results on mental healthdisorders and depressive disorders. The table illustratesthe fact that the surveys used different instruments,covered different time periods and that the populationssurveyed had different demographics. In addition, thesurveys differed in terms of design effect, participationrates, statistical analyses and weighting systems so theirresults can hardly be compared.
54
56
58
60
62
64
66
68
Italy
Portu
gal
Fran
ce
Swed
en
Luxe
mbo
urg
Germ
any (
New
Land
er)
Germ
any (
Old
Land
er)
Austr
ia
Belgi
um
Neth
erlan
ds
Spain
Tukey test
20
3
M E N T A L H E A L T H S T A T U S I N E U R O P E
Mental health status in Europe3
Fortunately, there are two European surveys usingidentical instruments and design and whose data can beanalysed together: Eurobarometer and ESEMeD.
However, even though much was done to ensurecomparability, care should be taken with comparisons sincethere are always unmeasured differences in estimates of therates of disorders. As a consequence, this report presentsonly a few overall comparisons and, instead, presents riskfactor comparisons for the major pertinent mental healthvariables (gender, age, marital status, employment,economic situation, rural/urban place of living andimmigration status) because it is safer to compare thesevarious risk factors within different countries.
The figures presented are mainly in the form of relativerisk, or odds ratio. The odds ratio is a number whichindicates how much the risk has to be multiplied for agiven country compared to another chosen as reference.Relative risk can also be presented in this way to
illustrate the size of a risk associated with one variable(such as being female) compared to another (such asbeing male). This format has the advantage that it canexpress, in a easy to understand manner, the risk. It alsoallows researchers to statistically ‘control’ for othervariables which might have an effect in order to ensurethat the risk is attributable to the country. Since thesurveys in question were done on samples, the oddsratios have a confidence interval which should notinclude one (which correspond to a risk at 0) - this willbe indicated in the figures. The odds ratios have beencalculated using stata and those presented have beenadjusted for the main demographic variables.
Two types of comparison are presented: psychologicaldistress, as evaluated by MHI5 (SF36) in Eurobarometerand the mental health scale of SF12 in ESEMeD, andcomparisons by psychiatric diagnoses according tomedical psychiatric classifications (major depressivedisorders and anxiety disorders).
21
3
M E N T A L H E A L T H S T A T U S I N E U R O P E
Table 1. Prevalence rates of depressive disorders in selected major European studies
Country Study Year Population Sample Instrument Taxonomy* Period Age Prevalencegroup All Male Female
Europe MHEDEA/ 2000-2002 Europe 21,425 WMH-CIDI DSM-IV 12-month 18+ 3.90% 2.60% 5%(6 National ESEMeD2 (Spain, Italy, samples) Germany
France, Belgium and Netherlands)
Finland Finland 20003 2000 national 8,028 CIDI ICD-10 12-month 30+ – 4 6
France (Basse Sante des BN4 1998 regional 1,445 CIDI-S DSM-IV 12-month 18+ 3.4 –Normandie)
Germany TACOS5 1998 regional 4,075 M-CIDI DSM-IV 12-month 18-64 2.1 1.1 3 (Lubeck & region)
Germany GHS6 1999 national 4,181 M-CIDI DSM-IV 12-month 18-65 8.30% 5.50% 11.20%
Netherlands NEMESIS7 1996 national 7,076 CIDI v 1.1 DSM-IIIR 12-month 18-64 5.80% 4.10% 7.50%
France (Paris) Paris/Sardinia8 1994-96 regional 2,260 CIDI-S 6-month 18+ 5.9 – –
France (Isle Sante des F9 1998 regional 1,183 CIDI-S DSM-IV 6-month 18+ 5.8 – –de France)
Italy Paris/Sardinia8 1994-96 3 different 1,040 CIDI-S ICD-10 6-month 18+ 6.5 – –(Sardinia) areas
Germany TACOS10 1998 regional 4,075 M-CIDI DSM-IV 4-week 18-64 0.8 0.3 1.2(Lubeck & region)
Netherlands NEMESIS7 1996 national 7,076 CIDI v 1.1 DSM-IIIR 4-week 18-64 2.70% 1.90% 3.40%
Great Britain 1st survey 1993 national CIS-R/SCAN ICD-10 2-week 16-64 2.30% 1.90% 2.80% psych morb11
Great Britain 2nd survey 2000 national CIS-R/SCAN ICD-10 2-week 16-64 2.80% 2.60% 3.00psych morb12
Source: E S Paykel MD FRCP FRCPsych FmedSci., T Brugha MD FRCPsych., T Fryers MD PhD FFPH. (2004) SIZE AND BURDEN OF DEPRESSIVEDISORDERS IN EUROPE. In: European Review on Size and Burden of Mental Disorders. To be published in European Neuropsychopharmacology.
3.2.1 Psychological distress
Psychological distress was measured by two near-identical instruments – MHI-5 and SF-12 – derived fromthe same source. These instruments aim to evaluatecommon symptoms, mostly concerning anxiety anddepression.
The Eurobarometer survey used the MHI-5 scale and arecommended cut-off point was used (Figure 8). Thismeans that those with a score at or below 52 have highpsychological distress. The differences betweencountries are significant.
Figure 8. Psychological distress in ten EU countriesPercentage with a score of 52 or less on MHI-5 scale ofSF36 – those who probably have mental health problems.Standardised against the West German population
Source: Eurobarometer
For SF-12 no standardised cut-off point is available buta low rate is associated with high psychological distressand a high rate with low psychological distress (Figure9). National UK survey data were added to the ESEMeDdata since they were collected using the sameinstrument.12 Data were weighted according to the UKpopulation distribution for age and sex.
Figure 9. Psychological Distress in Seven EU countries Mental health score on the SF-12 sub-scale in six ESEMedDcountries and the UK. A lower score indicates a higherlevel of psychological distress
Source: ESEMeD and UK psychiatric morbidity survey
When the two figures are compared the results arecoherent: France and Italy are those claiming thehighest psychological distress and Netherlands thelowest. Spain, Germany and Belgium are in-between.
When comparing results obtained with positive mentalhealth, one can see that some countries have strictinverse results such as the Netherlands, which has highpositive mental health and is low in psychologicaldistress. It is the reverse for Italy, Portugal and Francewhich have low levels of positive mental health and highlevels of psychological distress (Figures 8 and 9). Somecountries, however, such as Spain and Belgium are highfor positive mental health and relatively high as well forpsychological distress.
3.2.2 Psychiatric disorders
Data from the ESEMeD study enable presentation ofprevalence for major depressive disorders and anxietydisorders for the six countries involved.
2.65
3.11
4.454.514.64.61
3.69
2.50
3.00
3.50
4.00
4.50
5.00
FranceItalySpainGermanyBelgiumNetherlandsUnitedKingdom
Tukey Test
10.9
19.1
23.4
29.3 30.2
25.9
20.119.518.717.6
12.4
468
101214161820222426283032
Neth
erla
nds
Swed
en
Spai
n
Luxe
mbo
urg
Belgi
um
Aust
ria
Germ
any (
Old
Land
er)
Germ
any (
New
Land
er)
Fran
ce
Portu
gal
Italy
22
3
M E N T A L H E A L T H S T A T U S I N E U R O P E
Figure 10. Any mental disorder in the last 12 months in six EU countries Relative risk for any mental disorder in the last 12 months, using Italy as a base. Adjusted for sex, age, living arrangements and urban/rural
Source: ESEMeD
Five countries in the ESEMeD study had a higherprevalence of any mental disorder in the last 12 monthsthan Italy. Figure 10 shows the relative risk comparedto Italy for each of the other countries involved.
3.2.1.1 Depression
The six-country ESEMeD study included assessment oflifetime and current prevalence of mood disorders (whichincludes depression) and major depressive episodes.Figure 11 shows the relative risk for having had anymood disorder in the last 12 months compared to Italy.For all the following analyses, Italy was used as thereference for comparison because the rates for all theconditions were lower in Italy.
Figure 11. Any mood disorder in the last 12 months insix EU countries Relative risk for any mood disorder in the last 12 months, using Italy as a base. Adjusted for sex, age, living arrangements and urban/rural
Source: ESEMeD
Compared to Italy, there is a significantly increased riskof any mood disorder in Belgium, France and theNetherlands (Figure 11).
3.2.2 Anxiety
The ESEMeD survey assessed the lifetime and currentprevalence of anxiety disorders.
Figure 12. Anxiety disorders in the last 12 months insix EU countriesRelative risk adjusted for sex, age, living arrangementsand rural/urban. Italy as a Reference
Source: ESEMeD
The relative risk of anxiety disorders in the last 12months, compared to Italy, is shown in Figure 12. Foranxiety disorders, France, Germany and the Netherlandsare at risk compared to Italy. Spain and Belgium,however, do not have higher risk.
After controlling for major socio-demographic variables,differences do appear for most of the psychiatricdisorders across the participating countries. Italy has alower risk for any disorders in the last year than theother countries and Spain does not differ from Italy foranxiety and depressive disorders. On the other hand,France and the Netherlands are constantly higher thanItaly and Spain. Belgium is higher than Spain, Germanyand Italy for mood disorders but not for anxiety and itis the reverse for Germany.
Interestingly Italy, which has the lowest rate ofpsychiatric disorders, has one of the highestpsychological distress levels including within the samestudy where diagnosis as well as psychological distressquestions are asked to the same subjects. There arevarious ways that this might be explained. One of thesemight be that Italians are more prone to admit commonsymptoms than to report severe psychiatric symptoms.
Alternatively, there may be some social and culturalmechanisms which prevent those in psychological distressbecoming psychiatric diagnoses. This last hypothesis issupported by the fact that two macro-indicators: alcoholconsumption and suicide are at low levels for this country.Of course we cannot rule out the hypothesis that a rigidpsychiatric instrument such as the CIDI does not capture the
1.94
1.551.37 1.28
1.01.04
0,00
0,50
1,00
1,50
2,00
2,50
3,00
France TheNetherlands
Germany Belgium Spain Italy
1.48 1.411.25
0.94 1.0
2.11
0.00
0.50
1.00
1.50
2.00
2.50
3.00
France Belgium The Netherlands
Spain Germany Italy
2.23
1.721.6
1.321.2
1.0
0,00
0,50
1,00
1,50
2,00
2,50
3,00
France TheNetherlands
Belgium Germany Spain Italy
23
3
M E N T A L H E A L T H S T A T U S I N E U R O P E
diagnosis symptomatology. It worth noting that this lowrate for some of the diagnoses, more specifically depression,in Italy has been regularly reported in other surveys.
The analysis above illustrates that comparisons aredifficult to interpret, as well as demonstrating that dataare coherent between the two studies. This also showsthat psychological distress is a different dimension ofmental health to psychiatric disorders even though theydo overlap to a certain degree.
3.2.3 Psychosis
In addition to the mental health problems describedpreviously, it is important to consider other disorderssuch as schizophrenia.
Mental health literature suggests that the prevalence ofschizophrenia has varied enormously between studiesand countries. It is estimated that the average lifetimeprevalence of schizophrenia would be about 1% of thetotal population.
Large differences in the prevalence of schizophreniabetween different countries (from 0.3 per 1,000 to 13per 1,000) were found in one 1987 review. In addition,pockets with very high and very low prevalence havebeen detected.13
A review by Häfner and an der Heiden14 selected 30prevalence studies of schizophrenia published since1980. The lowest reported prevalence in these studieswas 0