Embed Size (px)
Citation preview

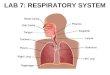
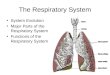
The Respiratory System
Airway Management
ALS & BLS

ObjectivesObjectives
• Review the anatomy and physiology of the
respiratory system.
• Demonstrate the use of basic and advanced • Demonstrate the use of basic and advanced
airway procedures and devices.

Upper AirwayUpper Airway
• Nasopharynx-Nares, Nasal Cartilage, Nasal
Bones, Maxilla
• Oropharynx-Lips, Cheeks, Tongue, Hard • Oropharynx-Lips, Cheeks, Tongue, Hard
and Soft Palates, Teeth, and Mandible.
• Pharynx-Muscular tube that extends from
the back of the soft palate to the upper end
of the Esophagus and Trachea.

Upper AirwayUpper Airway
• Epiglottis-Leaf shaped cartilage located at
the base of the tongue. Prevents food from
entering the respiratory tract during the act entering the respiratory tract during the act
of swallowing.
• Vallecula-Depression between the epiglottis
and base of the tongue.

Upper AirwayUpper Airway
• Larynx-Structure connecting the pharynx
and trachea. Consists of the thyroid
cartilage, cricoid cartilage, the upper end of cartilage, cricoid cartilage, the upper end of
the trachea, and the vocal cords.
• Trachea-Tube 10 to 12 centimeters long
connecting the larynx with the mainstem of
the bronchi. Trachea is somewhat rigid
consisting of C-shaped cartilaginous rings.

Upper AirwayUpper Airway
• Esophagus-Pliable tube running from the
Oropharynx to the digestive system.

Lower AirwayLower Airway
• Trachea extends to the Carina where it
divides into the Right and Left Mainstem of
the Bronchi.the Bronchi.
• Right Mainstem is almost straight whereas
the Left Mainstem acutely angles to the left.
• The Mainstems divide into Bronchioles
which lead to the Alveoli.

Lower AirwayLower Airway
• Alveoli are tiny sacs in the lungs where
most gas exchange takes place. Together
the Alveoli possess more than 40 square the Alveoli possess more than 40 square
meters of surface area.

LungsLungs
• Comprised of Bronchi, Bronchioles, and the
Alveoli
• Lungs are covered by connective tissue • Lungs are covered by connective tissue
called the Pleura. The Pleura is connected
to the lungs only at the Hilum.(point where
the bronchi enter the lungs)

LungsLungs
• Pleura consist of the visceral pleura, which
covers the lungs, and the parietal pleura,
which lines the thoracic cavity.which lines the thoracic cavity.
• Between the pleura is pleural fluid. Which
holds the two together and allows for
movement.

LungsLungs
• Right lung contains three lobes. Upper lobe,
Middle lobe, and Lower lobe.
• Left lung contains two lobes. Upper and • Left lung contains two lobes. Upper and
Lower lobes. Left lung has only two lobes
to allow room for the heart.

RespirationRespiration
• Defined as the exchange of gases between a
living organism and its enviroment

Respiratory Cycle Respiratory Cycle
• Requires coordinated interaction between
the respiratory system, central nervous
system, and the musculoskeletal system.system, and the musculoskeletal system.
• The lungs have no intrinsic capability to
contract or expand.

Respiratory CycleRespiratory Cycle
• Respiratory cycle begins when the lungs
have achieved a normal expiration. At this
point the pressure inside the thoracic cavity point the pressure inside the thoracic cavity
is equal to atmospheric pressure. The
contracting of the diaphragm and intercostal
muscles causes a downward movement and
outward expansion.

Respiratory CycleRespiratory Cycle
• This causes a lower pressure in the lungs
which pulls air in from the higher
atmospheric pressure.(Inspiration)atmospheric pressure.(Inspiration)
• When the pressure in the lungs once again
matches atmospheric pressure inspiration
stops.

Respiratory CycleRespiratory Cycle
• Once the diaphragm and intercostal muscles
relax the size of the chest cavity decreases
and air rushes out of the lungs.(Expiration)and air rushes out of the lungs.(Expiration)
• Inspiration is the active phase of respiration
and expiration is the passive phase.
• Tidal Volume is the volume of gas inhaled
or exhaled during a single respiratory cycle.
Usually 500 cc

Respiratory ProblemsRespiratory Problems

ObstructionsObstructions
• Tongue-Most common in infants and
children.
• Foreign Body-Food, loose teeth…..• Foreign Body-Food, loose teeth…..
• Trauma-Facial bones, teeth, nasal bones,
and clotted blood
• Laryngeal Spasm-Cord edema or Cord
spasm

ObstructionsObstructions
• Aspirations-Vomitus, blood, liquid drink

Inadequate Ventilation Inadequate Ventilation
• Hyperventilation or Hypoventilation
• Rates-Adult 12-20, Children 15-30, Infant
25-5025-50
• Disease such as Asthma or COPD

AssessmentAssessment

VisualVisual
• Adequate chest rise and fall.
• Color of skin.
• Flaring of the nares.• Flaring of the nares.
• Retraction of the intercostal muscles and
suprasternal notch.

AuscultationAuscultation
• Air movement at nose and mouth.
• Listening to bilateral lung fields. Six fields
in anterior thorax(upper, middle, and in anterior thorax(upper, middle, and
lower). Four fields in posterior thorax(upper
and lower).

PalpationPalpation
• Using the back of your hand or cheek.
• Feeling the chest for equal and adequate
chest rise and fall.chest rise and fall.

HistoryHistory
• Past medical history.
• History of present medical complication.
• Mechanism of injury.• Mechanism of injury.

BLS Methods For Maintaining
The Airway
BLS Methods For Maintaining
The Airway The Airway The Airway

Maintaining Airway Maintaining Airway
• Patient
• Head Tilt Chin Lift
• Modified Jaw Thrust• Modified Jaw Thrust
• Oropharyngeal Airway
• Nasopharyngeal Airway

Oropharyngeal AirwaysOropharyngeal Airways
• Allows air to pass around and through
device.
• Helps prevent obstruction by the teeth and • Helps prevent obstruction by the teeth and
lips.
• Helps manage unconscious patients who are
breathing spontaneously or need mechanical
ventilation.

Oropharyngeal Airways
• Makes suctioning of the pharynx easier
• Serves as an effective bite block in case of
seizures or to protect the endotracheal tube.seizures or to protect the endotracheal tube.

Oropharyngeal Airways
• Does not isolate the trachea.
• Cannot be inserted when teeth are clinched.
• May obstruct the airway if it is not inserted • May obstruct the airway if it is not inserted
properly.
• Can be dislodged easily.
• Should not be used on patient with gag
reflex.

Oropharyngeal Airways
• A properly sized Oropharyngeal airway
should measure form the flanged end at the
teeth to the angle of the jaw.teeth to the angle of the jaw.

Nasopharyngeal AirwayNasopharyngeal Airway
• Can be rapidly inserted.
• Bypasses the tongue.
• Can be used in the presence of a gag reflex.• Can be used in the presence of a gag reflex.
• Can be used when trauma has accrued to the
oral cavity.
• Can be used when the patient’s teeth are
clinched.

Nasopharyngeal Airway
• Does not isolate the trachea.
• It is smaller than the Oropharyngeal airway.
• Difficult to suction through.• Difficult to suction through.
• May cause severe nose bleeds if inserted to
forcefully.
• May kink and clog.
• Cannot be used if there is a basilar fracture.

Nasopharyngeal Airway
• Properly sized Nasopharyngeal airway will
be slightly smaller than the diameter of the
nostril and is equal to or slightly smaller nostril and is equal to or slightly smaller
than the distance from the nose to the
earlobe.

Esophageal Obturator Airway
• Insertion is easy and does not need the
visualization of the cords.
• Prevents gastric distention and • Prevents gastric distention and
regurgitation.
• Can be used on trauma patients who have
spinal injuries.

Esophageal Obturator Airway
• Adequate mask seal is difficult to maintain.
• Can cause esophageal trauma and rupture.
• May enter trachea if placed improperly.• May enter trachea if placed improperly.

VentilationVentilation
• Can be achieved utilizing the appropriate
bag valve mask I.e. adult, child, and infant.
• Mouth to mouth using a mask with a one • Mouth to mouth using a mask with a one
way valve.
• Oxygen delivery devices such as Non
Rebreather Mask or Nasal Cannula

ALS Airway ManagementALS Airway Management

ALS Airway ManagementALS Airway Management
• All Methods used in BLS management.
• Endotracheal Intubation

Endotracheal IntubationEndotracheal Intubation
• Inserting a Endotracheal tube into the
trachea.
• Tube Sizes-Adult 7.0 to 9.0, Child 4.0 to • Tube Sizes-Adult 7.0 to 9.0, Child 4.0 to
6.0, Infant 3.5 to 4.0
• General tube size is 7.5
• Adult and some child tubes have an
inflatable cuff to prevent distention.

Endotracheal Intubation
• Two Blade styles in this area Miller and
Macintosh.
• Macintosh is a curved blade which fits in • Macintosh is a curved blade which fits in
the Vallecula and raises the Epiglottis. Also
sweeps the tongue to the left when used
properly.

Endotracheal Intubation
• Miller blade is straight and fits over the
Epiglottis and raises the tongue and
Epiglottis up.Epiglottis up.
• Tube is formed into a “J” shape using a
stylet. Be sure not to insert the stylet past
the “eye of Murphy”, stylet should be one
half of an inch short of eye.

Endotracheal Intubation
• Using blade of choice and laryngoscope
open the airway until the cords are visible.
Insert the tube and visualize passing Insert the tube and visualize passing
through the cords. Once the cuff is no
longer visible inflate the cuff, remove the
stylet, and ventilate patient checking for
breath sounds. Check epigastrium, then left
chest, then right chest.

Endotracheal Intubation
• Make note of the tube depth and secure it
using an appropriate method.

Suctioning Suctioning

Suctioning The AirwaySuctioning The Airway
• Yankauer or “tonsil tip”suctioning devices
can be used to suction the upper airway.
• This device allows for larger volume and • This device allows for larger volume and
larger obstructions to be cleared. Measure
the device in the same method as an
Oropharyngeal airway. Suction only on the
way out and limit the suctioning time
around 10 seconds

Suctioning The Airway
• French catheters or “whistle tip” suctioning
devices can be used to suction upper and
lower airway.lower airway.
• French catheters can be used in stomas,
both Oropharyngeals and Nasopharyngeals,
and ET tubes.
• French catheters cannot remove large
volumes of secretions quickly or large
particles.

Suctioning The Airway
• Control suctioning by using the “on” and
“off” switch or the provided open port or
orifice.orifice.
• For large particles and volumes a thick
walled wide bore suctioning tube may be
used.

Suctioning The Airway
• Caution should be used when suctioning.
Forcibly using a Yankauer tip could cause
lacerations and other injuries. lacerations and other injuries.












![Respiratory system roadmap.pptx [Repaired] - Loginanatomical-sciences.health.wits.ac.za/roadmaps/Respiratory system... · DIVISION OF THE RESPIRATORY SYSTEM CONDUCTING PORTION Nasal](https://img.pdfslide.us/doc/110x75/5a78c3d87f8b9ae6228c9db0/respiratory-system-repaired-loginanatomical-scienceshealthwitsaczaroadmapsrespiratory.jpg)



![Anatomy and Physiology Respiratory System [Tab 2] Respiratory System](https://img.pdfslide.us/doc/110x75/56649ebd5503460f94bc631f/anatomy-and-physiology-respiratory-system-tab-2-respiratory-system.jpg)