Embed Size (px)
Citation preview

SUDANESE JOURNAL OF PAEDIATRICS AND CHILD HEALTH VallO: 2010
The Radiological Case of the month
Acute Disseminated Encephalomyelitis (ADEM) In A Four Year Sudanese Girl.SaW Abdulrahim SaW,
Associate Professor, Department of Paediatrics, The Academy Teaching hospital, University of Medical Sciences,Khartoum.
E-mail: [email protected]
A 4 year old girl brought to the hospital sufferingfrom fever, headache, convulsions & behavioralchanges. On examination she was febrile, pale, withchoreoathetoid movements & stupor that progressedrapidly to a state of coma. There were positive signsof meningeal irritation. GCS was 7 at the start. Therewas head lag & Rt. 6th cranial nerve palsy. Shewas spastic all over with exaggerated reflexes. Gotupgoing planter reflex. Later she developed typicalDecorticate position
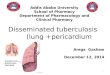
CBC, Blood grouping & BF for malaria randomblood sugar, renal profile & ABG. MRI was donefew days later, while on treatment, which is shownabove were alsodone.
Management was as follows: IVFs, NGtube, valium, IV antibiotics in form of ceftriaxone,Ampiclox & Gentamycin. Acyclovir, dexamethazone& metronidazole were also added.
She responded to our management, but withthe following sequelle: Aphasia, epilepsy & mentalretardation. So an antiepileptic drug and physiotherapywere started.
ADEM is an acute demyelinating disease, ofautoimmune etiology, most commonly affectschildren. It is a white matter inflammatory disease.'It usually follows a viral infection,' a nonspecificupper respiratory infection or vaccinations. ADEM ispredominantly a disease of children and in particularinfants.2 clinically there is fever, headache, stiffneck with multifocal deficits (Ataxia, hemiplegia &visual loss). The child may get fits, stupor or coma.
69

SUDANESE JOURNAL OF PAEDIATRICS AND CHILD HEALTH VallO: 2010
ADEM ultimately has a better prognosis.2 Mostcases have favourable outcome, but few are severeor fatal. Diagnosis carries important therapeutic andprognostic implications.3 CSF shows: An increase inWBC & protein level. Rarely there is what is calledADEM-like presentation A Multiple sclerosis is themain differential diagnosis.
MRI is the neuroimaging study of choice forestablishing the diagnosis and for following thecourse of the disease. The MRI shows: Multiplebilateral hyperintense lesions & perilesional edema.CT scan is relatively insensitive. The lesions regresswith successful treatment. Treatment starts with IVmethylprednisolone for three days followed by oralsteroids for few weeks. Infusions of immunoglobulinscan be given.
A study done in North Indian children stated that:
The presentation of paediatric ADEM in developingcountries is similar to that in developed countries.In spite of an aggressive presentation, most childrenrespond well to corticosteroids. MRI lesions disappearor are significantly reduced at six months in themajority of cases.5
References:(J) Horowitz MB. Comey C, Hirsch W, Marion D, Griffith B,
Martinez J. Acute disseminated encephalomyelitis(ADEM) orADEM-like inflammatory changes in a heart-lung transplantrecipient: a case report. Neuroradiology.1995; 37: 43437-.
(2) Bennetto L, Scolding N. Inflammatory ipost-infectiousencephalomyelitis. J Neurol Neurosurg Psychiatry. 2004; 75:2228-.
(3) Love S. Demyelinating diseases. J Clin Pathol. 2006; 59:115159-.
(4) Haghighi AB, Ashjazadeh N. Acute disseminatedencephalomyelitis-like manifestations in a patient withneuro-Behcet disease. Neurologist. 2009; J 5(5): 2824-.
(5) Singhi PD, Ray M, Singhi S, Khandelwal NK. Acutedisseminated encephalomyelitis in North Indian children:clinical profile and follow up. Journal of Child Neurology.2006; 21(10): 85157-.
70