Embed Size (px)
Citation preview

The PARTNER Stroke Substudy Writing Group*
On behalf of The PARTNER Trial Investigators and Patients
Transcatheter (TAVR) versus Surgical (AVR) Aortic Valve Replacement: Incidence, hazard,
determinants, and consequences of neurological events in the PARTNER Trial
* Miller DC, Mack MJ, Svensson LG, Kodali SK, Kapadia S, Anderson WN, Rajeswaran J, Blackstone EH

Presenter Disclosure Information
for PARTNER Trial, AATS May, 2011
D. Craig Miller , M.D.
Affiliation/Financial Relationship Company
Grant/ Research Support: NHLBI research grant RO1 HL67025
Consulting Fees/Honoraria:•The PARTNER U.S. Pivotal Trial Executive Committee, Edwards Lifesciences (uncompensated)•Stanford PI – The PARTNER Trial, Edwards Lifesciences (uncompensated)•Consultant, Abbott Vascular (MitraClip)•Consultant, Medtronic CardioVascular Division•Consultant, St. Jude Medical
Major Stock Shareholder/Equity Interest:Royalty Income:Ownership/Founder:Salary:Intellectual Property Rights:Other Financial Benefit:

Background Surgical AVR is the standard of care for
symptomatic aortic stenosis
Survival after TAVR is superior compared to medical therapy in inoperable patients, and is non-inferior to that after AVR in high-risk operative candidates, but neurological complications occur more frequently after TAVR
No randomized trial comparing TAVR and AVR focusing on neurological events has been performed

N = 699 N = 358
High RiskHigh Risk
InoperableInoperable
The PARTNER TrialThe PARTNER TrialStudy DesignStudy Design
Symptomatic Severe Aortic StenosisSymptomatic Severe Aortic Stenosis
ASSESSMENT: High-Risk AVR Candidate3,105 Total Patients Screened
ASSESSMENT: High-Risk AVR Candidate3,105 Total Patients Screened
Total = 1,057 patients
2 Parallel Trials: Individually Powered
StandardTherapyStandardTherapy
ASSESSMENT: Transfemoral
Access
ASSESSMENT: Transfemoral
Access
Not In StudyNot In Study
TF TAVRTF TAVR
Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority)
Co-Primary Endpoint: Composite of All-Cause Mortalityand Repeat Hospitalization (Superiority)
Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority)
Co-Primary Endpoint: Composite of All-Cause Mortalityand Repeat Hospitalization (Superiority)
1:1 Randomization1:1 Randomization
VS
YesYes NoNo
N = 179 N = 179

Numbers at RiskNumbers at Risk
TAVRTAVR 179179 138138 122122 6767 2626 Standard RxStandard Rx 179179 121121 8383 4141 1212
Standard Rx
TAVI
All
-cau
se m
ort
alit
y (%
)
Months
∆ at 1 yr = 20.0%NNT = 5.0 pts
50.7%
30.7%
HR [95% CI] =0.54 [0.38, 0.78]
P (log rank) < 0.0001
PARTNER cohort B (inoperable)All-Cause Mortality at 1 Year

Neuro events at 30 days and 1 year- Inoperable cohort B
Major Stroke
P = 0.06P = 0.18
All Stroke or TIA
P = 0.03P = 0.04
TAVR (n=179) Standard Rx (n=179)
per
cen
t

N = 179
N = 358InoperableInoperable
StandardTherapyStandardTherapy
ASSESSMENT: Transfemoral
Access
ASSESSMENT: Transfemoral
Access
Not In StudyNot In Study
TF TAVRTF TAVR
Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority)
Co-Primary Endpoint: Composite of All-Cause Mortalityand Repeat Hospitalization (Superiority)
Primary Endpoint: All-Cause Mortality Over Length of Trial (Superiority)
Co-Primary Endpoint: Composite of All-Cause Mortalityand Repeat Hospitalization (Superiority)
1:1 Randomization1:1 Randomization
VS
YesYes NoNo
N = 179
TF TAVRTF TAVR AVRAVR
Primary Endpoint: All-Cause Mortality at 1 yr(Non-inferiority)
Primary Endpoint: All-Cause Mortality at 1 yr(Non-inferiority)
TA TAVRTA TAVR AVRAVR VS
VS
N = 248 N = 104 N = 103N = 244
The PARTNER Study DesignThe PARTNER Study Design
Symptomatic Severe Aortic StenosisSymptomatic Severe Aortic Stenosis
ASSESSMENT: High-Risk AVR Candidate3,105 Total Patients Screened
ASSESSMENT: High-Risk AVR Candidate3,105 Total Patients Screened
Total = 1,057 patients
2 Parallel Trials: Individually Powered
N = 699 High RiskHigh Risk
ASSESSMENT: Transfemoral
Access
ASSESSMENT: Transfemoral
Access
Transapical (TA)Transapical (TA)Transfemoral (TF)Transfemoral (TF)
1:1 Randomization1:1 Randomization1:1 Randomization1:1 Randomization
YesYes NoNo

TransfemoralTransfemoral TransapicalTransapical
TAVRTransfemoral (TF) and Transapical (TA)

0
0.1
0.2
0.3
0.4
0.5
0 6 12 18 24
TAVR
AVR
Months
348 298 260 147 67
351 252 236 139 65
No. at Risk
TAVR
AVR
26.8
24.2
PARTNER cohort AAll-Cause Mortality at 1 Year
HR [95% CI] =0.93 [0.71, 1.22]
P (log rank) = 0.62

All neurological eventsat 30 days and 1 yearPARTNER Cohort A Trial (ITT)
5.5
8.3
2.44.3
0
10
20
30 Days 1 Year
All
neur
o ev
ents
(%
) TAVR AVR
Smith CR, ACC 2011, NEJM in press
P=0.04P=0.04P=0.04P=0.04

Purpose• Analyze stroke and TIA after TAVR and surgical AVR in high-risk (≈15%, floor= STS 8-9%), operable patients with symptomatic, severe aortic stenosis in the PARTNER Trial
• “As Treated” (AT) patients n= 657 (vs. ITT)
• Captured all neurological events at all times
• Prospective, independent, blinded adjudication of adverse neurological events by CEC, supplemented by CEC retrospective assessment of stroke severity
• Unblinded re-review of all CEC summaries and source documents by 2 investigators (DCM, MJM)

Patient characteristics (AT)Transapical Stratum Transfemoral Stratum
Variable
AVR(n = 92)
TA-TAVR(n = 104)
AVR(n = 221)
TF-TAVR(n = 240)
Age (years) (± 1 SD) 83 ± 6 83 ± 7 85 ± 7 84 ± 7
STS risk Score (± 1 SD) 12.1 ± 3.5 11.7 ± 3.6 11.5 ± 3.3 11.9 ± 3.2
Logistic EuroSCORE (± 1 SD) 30 ± 15 30 ± 16 29 ± 15 29 ± 17
NYHA class III-IV 96% 92% 95% 95%
Carotid endarterectomy / stent 17% 24% 6% 10%
Stroke or TIA within last 6-12 mo 7% 1% 1% 4%
Previous CABG 56% 50% 40% 40%
Coronary artery disease 84% 75% 75% 75%
Previous MI 38% 28% 26% 27%
Cerebrovascular disease 31% 43% 26% 24%
Peripheral vascular disease 62% 63% 35% 35%
COPD 64% 64% 65% 63%
Pulmonary hypertension 42% 53% 55% 54%
Atrial fibrillation 21% 32% 26% 23%
Mean aortic valve gradient (mmHg)
41 ± 13 42 ± 14 45 ± 15 43 ± 15
Aortic Valve Area Index (cm2/m2) 0.4 ± 0.1 0.4 ± 0.1 0.3 ± 0.1 0.4 ± 0.1
LV ejection fraction (%) 54 ± 11 54 ± 12 54 ± 13 52 ± 14

One year results (AT, n= 657)
Transapical Stratum
Transfemoral Stratum
Outcome at 1 year
AVR(n = 92)
TA-TAVR(n = 104)
AVR(n = 221)
TF-TAVR(n = 240) P-value
All-cause mortality 25% 29% 25% 21% .33
All neurological events
9.7% 14.1% 1.9% 6.1% 0.03
Major stroke 5.9% 9.4% 1.4% 3.5% .15Minor stroke 1.1% 1.0% 0% 0.8% .16TIA 3.9% 3.7% 0.6% 1.8% .25

47 patients, 49 neuro eventsIschemic- 72%, hemorrhagic- 0%,
ischemic evolving to hemorrhagic- 4%, unknown- 24%
Distribution of types of neurological events

0
2
4
6
8
10
12
14
TIA
Minor Stroke
Major Stroke
Timing of neurological eventsAVR
AV
AV
RRT
AV
TA
VRR
AV
AV
RRT
AV
TA
VRR
AV
AV
RRT
AV
TA
VRR
AV
AV
RRT
AV
TA
VRR
AV
AV
RRT
AV
TA
VRR
AV
AV
RRT
AV
TA
VRR
AV
AV
RRT
AV
TA
VRR
0-20-2daysdays
3-53-5daysdays
31-36431-364daysdays
11-3011-30daysdays
6-106-10daysdays
2-32-3yearsyears
1-21-2yearsyears

Risk Factors forNeurologic Events
Multiphase, multivariable non-proportional hazard analysis
Early high peaking hazard phase Later constant hazard phase

Risk FactorCoefficient ±
SD PR
(%)
Early hazard phase
TAVR 2.21±0.68 .001 59
Smaller AVA index in TAVR group
-11.8±5.1 .02 57
Incremental risk factors for neurologic events
R(%) = bagging reliability
Early high peaking hazard phase
Atrial fibrillation not significant in multivariable analysis

Early hazard of neurologic event
%/mo
0
20
40
60
80
.25 .50 .75 1.0
TAVR
AVR
Months after Procedure

Neurologic event- TF candidate
%%
0
5
10
15
20
25
30
6 12 18 24
AVR TAVR
MosMos5451
10699
179159
203170
242221
TAVRAVR
3.4
6.0
2.4
7.4
TF Candidate

Neurologic event- TA candidate
%%
0
5
10
15
20
25
30
6 12 18 24
TAVR
AVR
MosMos2627
6460
7667
10292
TAVRAVR
12
10
TA Candidate

Neurologic event by 1 moInfluence of smaller AVA index
%%
AVAI (cmAVAI (cm22/m/m22))
TF
TA
CandidateCandidate
TAVR
5
10
15
20
0.2 0.3 0.4 0.5 0.6

Risk Factor Coefficient ± SD P R (%)
Constant hazard phase
TAVR 0.40±0.43 0.4 22
(Higher) NYHA 0.95±0.40 .02 75
Stroke or TIA within 6-12 mo 1.93±0.64 .002 60
Non-TF TAVR candidate 2.3±0.45 <.0001 96
History of PCI (less risk) -1.60±0.63 .01 77
COPD (less risk) -1.06±0.47 .03 79
Incremental risk factors for neurologic events
R(%) = bagging reliability
Late constant hazard phase

Non-TF candidate differentiation
Female
PVD
CEA
CABG
100200 40 8060
%
TF stratumTA stratum

Later hazard- assigned stratum(TAVR and AVR combined)
%/m%/m
0
1
2
3
4
6 12 18 24
TF
TA
Candidate
Months after ProcedureMonths after Procedure

TAVR neurologic event by stratum
%%
TAVR
TF
TA
MosMos
Candidate
7.4
12
6.0
5410626
17964
20376
242102
TAVR-TFTAVR-TA
0
5
10
15
20
25
30
6 12 18 24

%%
0
5
10
15
20
25
30
6 12 18 24MosMos
AVR
TF
TA
3.4
10
2.4
519927
15960
17067
22192
TFTA
Candidate
AVR neurologic event by stratum

Major Stroke
Small number of events n= 29Conservative definition (modified Rankin score ≥2)
If stroke severity unclear, categorized as major

Major stroke (18 TAVR, 11 AVR)
%%
0
2
4
6
8
10
6 12 18 24
TAVR
AVR
MosMos6359
137128
252222
284239
344313
TAVRAVR
4.5
4.8
2.6
6.1

Competing Risks ofDeath and Neurologic Events

Competing risks
%%
0
20
40
60
80
100
6 12 18 24
Neuro event
Alive w/o neuro event
Months after ProcedureMonths after Procedure
Death before neuro event
AVR

Neurologic event
0
5
10
15
20
25
6 12 18 24
%%
AVR-TA
Consideringcompeting risks
TAVR-TA
67
59
11432
10618
17964
16062
20277
17067
240104221 92
TAVR-TFTAVR-TAAVR-TFAVR-TA
AVR-TF
12
5.59.1
2.2 2.6
6.5TAVR-TF

“Mortality Cost” of a Neurologic Event

“Mortality Cost” of neuro event
0
2
4
6
8
3 6 9 12
Observed/Expected
AVR
HazardRatio
Months after Neurologic EventMonths after Neurologic Event

0
2
4
6
8
3 6 9 12
Observed/Expected
HazardRatio
Months after Neurologic EventMonths after Neurologic Event
TAVR-TF
“Mortality Cost” of neuro event

0
2
4
6
8
3 6 9 12
Observed/Expected
HazardRatio
Months after Neurologic EventMonths after Neurologic Event
TAVR-TA
“Mortality Cost” of neuro event

• Prospective, independently adjudicated 30 day neurological event rates (stroke and TIA) were low
AVR= 2.6% TAVR= 5.6% p= .05
TF- AVR= 1.4% TAVR= 4.6% p= .04
Conclusions
• Remarkably low 30 day mortality rates in these elderly, very high-risk AS patients in both arms of study
AVR= 8% (O:E= 0.68) TAVR= 5.2% (O:E= 0.42) p= .15
TF- AVR= 8.2% TAVR= 3.7% p= 0.05
• Major stroke rates at 30 days were even lower
AVR= 2.3% TAVR= 3.8% p= .25
TF- AVR= 1.4% TAVR= 2.5% p= .37

Incremental risk factors for neurological events
• Early peaking high hazard phase:TAVRSmaller AVA index (TAVR group only)
• Later constant hazard phase:
Generalized heavy arteriosclerotic burden (“non-TF TAVR candidate”)
Stroke/TIA within 6-12 monthsHigher NYHA class
Conclusions

• Higher observed incidence of neurological events in the “non-TF candidate” stratum reflected the patient substrate, and was not related to the TA-TAVR or AVR procedures per se
Conclusions

• Taking competing hazard of death into consideration, the likelihood of a neurologic event was lowest in AVR patients and highest in TA-TAVR group
• A neurologic event raised the risk of mortality
• In AVR group: High peak, quickly returning to baseline hazard
• In TAVR groups: After initial peak, risk remained elevated throughout the 24 months of follow-up, particularly in TA stratum
Conclusions

• These results can only be interpreted within the constraints of the PARTNER Trial protocol:
• Carefully controlled patient selection
• Regimented training and proctoring
• Critical case monitoring and review
• Dedicated multi-disciplinary “Heart Valve Team” in these 26 centers
• “TF first” protocol philosophy and TAVR sheath sizes available
• Learning curve, first generation TAVR device
• Not adequately powered for TF vs. TA comparison
Limitations

Thank You

BACK-UP

EARLY HIGH HAZARD PHASE
• Peri-procedural anticoagulation management• Clopidogrel load, + dual antiplatelet Rx• Warfarin or dabigatran Rx• No protamine reversal (TF)• Bridge AF patients with heparin
• Cerebral embolic prevention devices
• Newer low profile THV deployment systems
• Carotid compression during BAV, THV deployment
LATE CONSTANT HAZARD PHASE
• More rigorous patient selection (TA)
InferencesCan TAVR stroke rate be lowered?

Brain DWMRI after TAVR
J Am Coll Cardiol 2010;55:1427–32

Brain DWMRI after TAVR
Valve New MRI lesions
Stroke
Ghanem CoreValve 73% 10%
Knipp SAPIEN 58% 4%
Kahlert Both 84% 0%
Astarci Both 91% 0%
Rodés-Cabau, Webb
SAPIEN 68% 3.3%

Embrella® Embolic Deflector
Initial Vancouver experience in 4 patients, 3 with TAVI and 1 with BAV
Effectiveness?
Safety?
Nietlispach et al., J Am Coll Cardiol Intv 2010;3:1133– 8

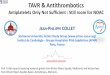
The PARTNER Trial Cohort A Death and Stroke (As Treated) n= 657
30 Days 1 Year
TF AVR
(n=221)TF TAVR (n=240) P value
TF AVR (n=103)
TF TAVR n=104
P value
Death 18 (8.2) 9 (3.7) 0.05 55 (25.2) 51 (21.3) 0.33
Stroke or TIA
All 3 (1.4) 11 (4.6) 0.04 4 (1.9) 14 (6.1) 0.03 TIA 0 (0.0) 3 (1.3) 0.08 1 (0.6) 4 (1.8) 0.25
Stroke Minor 0 (0.0) 2 (0.8) 0.16 0 (0.0) 2 (0.8) 0.16 Major 3 (1.4) 6 (2.5) 0.37 3 (1.4) 8 (3.5) 0.15
Transfemoral (TF) Substrate

The PARTNER Trial Cohort A Death and Stroke (As Treated) n= 657
30 Days 1 Year
TA AVR (n=92)
TA TAVR (n=104) P value
TA AVR (n=92)
TA TAVR n=104 P value
Death 7 (7.6) 9 (8.7) 0.79 23 (25.3) 30 (29.1) 0.55
Stroke or TIA
All 5 (5.5) 8 (7.9) 0.50 8 (9.7) 13 (14.1) 0.37
TIA 1 (1.1) 0 (0.0) 0.31 3 (3.9) 3 (3.7) 0.97
Stroke
Minor 1 (1.1) 1 (1.0) 0.95 1 (1.1) 1 (1.0) 0.95
Major 4 (4.4) 7 (7.0) 0.45 5 (5.9) 9 (9.4) 0.37
Transapical (TA) Substrate

Stroke Definition- The Modified Stroke Definition- The Modified Rankin ScaleRankin Scale
Minor• 0- No Symptoms• 1- No significant disability. Able to carry out all
usual activities, despite some symptomsMajor
• 2- Slight disability. Able to look after own affairs without assistance, but unable to carry out all previous activities.
• 3- Moderate disability. Requires some help, but able to walk unassisted.
• 4- Moderately severe disability. Unable to attend to own bodily needs without assistance, and unable to walk unassisted.
• 5- Severe disability. Requires constant nursing care and attention, bedridden, incontinent.
• 6- Dead.

Neurologic event
%%
0
5
10
15
6 12 18 24
TAVR
AVR
MosMos5858
130125
243218
278251
344313
TAVRAVR
11
6.78.0
4.5

30 Days 1 Year
OutcomeOutcome TAVRTAVR(N = 348)(N = 348)
AVRAVR(N = 351)(N = 351)
TAVRTAVR(N = 348)(N = 348)
AVRAVR(N = 351)(N = 351)
All Stroke or TIA – no. (%)All Stroke or TIA – no. (%) 19 (5.5)19 (5.5) 8 (2.4)8 (2.4) 0.040.04 27 (8.3)27 (8.3) 13 (4.3)13 (4.3) 0.040.04
TIA – no. (%) 3 (0.9) 1 (0.3) 0.33 7 (2.3) 4 (1.5) 0.47
All Stroke – no. (%) 16 (4.6) 8 (2.4) 0.12 20 (6.0) 10 (3.2) 0.08
Major Stroke – no. (%)Major Stroke – no. (%) 13 (3.8)13 (3.8) 7 (2.1)7 (2.1) 0.200.20 17 (5.1)17 (5.1) 8 (2.4)8 (2.4) 0.070.07
Minor Stroke – no. (%) 3 (0.9) 1 (0.3) 0.34 3 (0.9) 2 (0.7) 0.84
Death/maj stroke – no. (%)Death/maj stroke – no. (%) 24 (6.9)24 (6.9) 28 (8.2)28 (8.2) 0.520.52 92 (26.5)92 (26.5) 93 (28.0)93 (28.0) 0.680.68
Neurological Events at 30 Days and 1 Year All Cohort A PatientsN=699, ITT (not AT)
p-valuep-value p-valuep-value
Smith CR, ACC 2011, NEJM in press