Embed Size (px)
Citation preview

Early Human Development, 32 (1993) 197-206 0 1993 Elsevier Scientific Publishers Ireland Ltd. All rights reserved. 037%3782/93/%06.00
197
EHD 01389
The incidence of obstructive apneas in preterm infants with and without bronchopulmonary
dysplasia
Carlos Fajardo, Jorge Alvarez, Anita Wong, Kim Kwiatkowski and Henrique Rigatto
Department of Pediatrics, Department of Physiology and Department of Reproductive Medicine University of Manitoba, Manitoba (Canada)
(Received 18 June 1992; revision received 8 December 1992; accepted 28 December 1992)
summary
We tested the hypotheses that (1) pretetm infants with bronchopulmonary dysplasia (BPD) have an increased incidence of obstructive apneas as compared to those without BPD (control) and (2) the respiratory pattern during obstructive apneas may be associated with more pronounced hypoventilation. Ventilation was measured with a flow-through system. We examined 2929 total apneas in 12 infants with BPD and 4366 apneas in 12 control infants matched for study weight (1.51 f 0.11 kg in the BPD group and 1.62 f 0.12 kg in the control group, P = 0.6) and for postconceptional age (33.3 + 0.8 weeks in the BPD group compared with 33.4 f 0.7 weeks in the control group, P = 0.6). The incidence of central apneas predominated in the BPD group (2551/2929, 87%) and in the control group (4188/4366, 96%). Obstructive apneas were more frequent in the BPD group (37812929, 13%) than in the control group (178/4366, 4%, P = 0.004). The increased incidence of obstructive apneas in infants with BPD was observed in Quiet sleep (9.1 vs. 1.6%, P = 0.03) and in REM sleep (14.2 vs. 3.6%, P = 0.009). This increased in- cidence of obstructive apneas was applicable to short apneas (< 10 s, 10.9 vs. 2.7%, P = 0.003) and long apneas (> 10 s, 27.5 vs. 16.4%, P = 0.01). There were no signiti- cant changes in ventilatory pattern that could be uniquely attributed to one type of apnea. The findings suggest: (1) the great variability in the incidence of obstructive apneas reported in the literature relates, at least in part, to the clinical status of the infants and (2) ventilatory pattern is not a useful predictor of either type of apnea.
Correspondence to: Henrique Rigatto, Neonatal Research, Department of Pediatrics, WR125 -Women’s Hospital, 735 Notre Dame Avenue, Winnipeg, Manitoba, Canada R3E 0L8.

198
Key words: sleep state; newborn infant; control of breathing; respiratory pattern
Introduction
Apneas of various durations are common in preterm infants yet there is great con- troversy about the incidence of central and obstructive apneas [l-5]. Also the physiologic mechanism responsible for either type of apnea remains greatly unknown. Regarding incidence, one report showed the incidence of central apneas being as high as 93% [4] whereas another showed the incidence of obstructive apneas to be 58% [5]. We thought that some of these differences might be related to whether the population studied had or had not bronchopulmonary dysplasia (BPD) with its inherent borderline hypoxemia [7- 111. It might also depend on the length of apnea, the longer apneas having a greater chance of obstructing. Regarding mechanism, it would be interesting to know whether there are changes in ventilatory pattern either preceding or following apnea that would characterize central or obstructive apneas. Thus, we hypothesized that (1) differences in the incidence of central and obstructive apneas reported in the literature are dependent on the clinical status of the infants studied and (2) ventilatory pattern may changewith a more pronounced decrease in ventilation associated with obstructive apneas as compared with central apneas.
The purpose of this study was therefore to test these hypotheses by comparing apneas in infants with and without BPD.
Methods
Subjects We studied 24 preterm infants, 12 with BPD and 12 without BPD (control). In in-
fants with BPD mean birth weight was 1.1 f 0.05 kg (S.E.), gestational age 27.5 f 0.38 weeks, and postnatal age 41.6 f 4 days. In the control group birth weight was 1.5 f 0.14 kg, gestational age 30.9 f 0.8 weeks, and postnatal age 18.3 f 2.5 days. The two groups were matched for study weight (1.51 f 0.11 kg in the BPD group compared to 1.62 f 0.12 kg in the control group, P = 0.6) and for postconceptional age (33.3 f 0.8 weeks in the BPD group compared with 33.4 f 0.7 weeks in the control group, P = 0.6). Infants with BPD and controls were enrolled sequentially over a period of 21 months (October 1987 to July 1989). BPD was defined by: (1) the need for supplemental oxygen and (2) abnormal radiological findings indicative of residual lung disease at 28 days [12]. The duration of ven- tilatory support was 13 days (range l-42) in the BPD group and 2.5 days (range 0.42-12 days) in the control group. The duration of oxygen therapy was 53.6 days (range 28-87) in the BPD group and 5.4 days (range 0.42-19) in the control group. The mean inspiratory oxygen concentration at the time of the study was 30.5 (range 21-62) percent in the BPD group and 21.5 (range 21-27) percent in the control group. The corresponding saturations were 94.8 f 0.8 and 95.4 f 0.6% in the two groups, respectively. All BPD infants but one were on oxygen at the time of the study; conversely all control infants were on room air, except for one infant who was

199
receiving oxygen for treatment of apnea. The studies were done after 29.4 f 4.0 days (range 1 l-59) of extubation in the BPD group and 15.7 f 2.1 days (range 7-30) of extubation in the control group. The study was approved by the Faculty Committee on the Use of Human Subjects in Research, University of Manitoba and a written parental consent was obtained.
Methods Our system to measure breathing pattern and ventilation has been described
[4,7,8]. Briefly, breathing was measured using a nosepiece and a flow-through system. Alveolar PCO* (P*co~) and PO2 (PA02) were measured using Beckman oxy- gen and carbon dioxide analyzers (model OMl 1 and LB-2, Beckman Instruments Co., Fullerton, CA) Heart rate was measured using conventional leads and oxygen saturation was measured using a Nellcor Oximeter (model N-lOOC, Nellcor, Hayward, CA). The electroencephalogram (EEG) was recorded with electrodes plac- ed in the C-4/A-l positions. The electrooculogram (EOG) was recorded from the upper outer canthus of the left eye and the lower outer canthus of the right eye and referred to the right ear lobe. Respiratory efforts were determined using surface diaphragmatic electromyography (EMGdi) Diaphragmatic electromyography was measured using two surface electrodes placed above and below the costal margin at, or just lateral to, the right mid-clavicular line [13]. Chest and abdominal displace- ments were measured using mercury strain gauges [14]. These strain gauges were placed at the level of the fourth intercostal space and just above the umbilicus. All signals were recorded on a Nihon Kohden 21 channel recorder (Model 4221, Nihon Kohden, Tokyo, Japan) and were also taped for subsequent analysis.
Sleep states were classified into quiet, REM, transitional, and indeterminate. Quiet sleep state was defined by the absence of rapid eye movements coupled with trace altemans [ 15,161. REM sleep was defined by the presence of rapid eye movements on the EOG and continuous irregular low-voltage on the EEG. Transi- tional sleep with short epochs lasting 1-3 min which were usually observed during the transition from quiet to REM or vice-versa. Indeterminate sleep was defined as that which could not be described by other definitions.
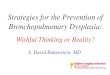
Apneas were classified into central and obstructive. Central apneas were those in which air flow and respiratory efforts (jEMGdi, chest and abdominal displace- ments) were absent. Obstructive apneas were those in which absent air flow was associated with some respiratory efforts. This obstructive group therefore includes apneas traditionally known as purely obstructive and mixed [4]. A typical tracing of relevant variables is shown in Fig. 1.
Procedure Infants were studied on the Ohio Neonatal Intensive Care Unit (Ohio Medical In-
struments, Madison, WI) in a neutral thermal environment (skin abdominal temper- ature 36.5 f 0.03’C). This unit is located in a research laboratory adjacent to the Intermediate Care Nursery. After appropriate placement of the electrodes, nosepiece and strain gauges, the infant was allowed to sleep. When the infant did not settle, a feeding was offered. Similarly, if infants woke during the study, they were fed and

200
Fig. 1. Representative tracing in infant J.K. (weight 1.93 kg, 42 days old) with bronchopulmonary dysplasia. Note that (A) represents central apnea with cessation of respiratory flow and no respiratory efforts and (B) represents an obstructive apnea with cessation of flow but some respiratory efforts as indicated by arrows.
the study was continued. During the study, the infants inhaled the same inspired oxygen concentration they were receiving in the nursery. In each study, at least one epoch in each sleep state was recorded.
Data collection and analysis The measurements were made by hand from the polygraph tracing. First the trac-
ing was divided into the various epochs corresponding to the different sleep states. Second all apneas longer than 3 s were measured. A duration of 3 s was chosen because it is not too short to be confused with a prolonged expiration, and we wanted to measure all apneas not only those longer than 20 s. In addition, to know whether changes in specific ventilatory variables could predict the appearance of obstructive or central apneas, we measured ventilation (V,), tidal volume (Vr), fre- quency (f), inspiratory time (T,), expiratory time (Ta), PAco2 and PAoZ in five breaths preceding and following the apnea. These measurements were made in 14 in- fants in whom obstructive and central apneas of similar duration were observed. All measurements were made by an observer blind to the assignment group and were entered into a computer program in order to do the appropriate statistical analysis. The significance of the differences in the incidence of apneas between the BPD and the control groups was measured using a non-parametric test (Mann Whitney) and that within the groups was measured using the Wilcoxon Signed Rank Test. Values

201
were expressed as mean * S.E. (or range). A probability value 10.05 was con- sidered significant.
Results
General observations The average duration of each study was 3.6 f 0.3 h (range 2.2-6.0 h) in the BPD
group and 3.3 f 0.3 h (range 1.2-4.8) in the control group. The overall duration of all the studies was 42.7 h in the BPD group and 40.6 in the control group. Infants in the BPD group spent 28.9% of the time in quiet sleep, 32.9% in REM, 7.4% in transitional sleep, and 30.8% in indeterminate sleep. Infants in the control group spent 36.8% in quiet sleep, 25.4% in REM sleep, 8.2% in transitional sleep, and 29.6% in indeterminate sleep. This sleep state distribution did not differ significantly between the two groups. The number of apneas was 2929 in the BPD group and 4366 in the control group. The duration of obstructive apneas was significantly greater than that of central apneas in both groups (9.0 f 1.2 s vs. 6.2 f 0.8 s in the BPD group and 8.3 * 0.8 s vs. 5.5 f 0.2 s. (P < 0.05)).
The incidence of apneas Central apneas predominated in the BPD group (2551/2929,87%) and in the con-
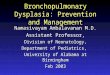
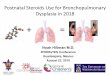
trol group (4188/4366, 96%). Obstructive apneas in the BPD group (378/2929, 13%) were more frequent than in the control group (178/4366,4%, P = 0.004) (Fig. 2). The increased incidence of obstructive apneas in BPD infants was observed in quiet sleep (9.1 vs. 1.6%, P = 0.03) and in REM sleep (14.2 vs. 3.6%, P = 0.009) (Fig. 3); dif- ferences were not significant in transitional and in indeterminate sleep states. The incidence of obstructive apneas was greater in BPD than in control groups for both short apneas (cl0 s, 10.9 vs. 2.7%, P=O.O03) and long apneas (>lO s, 27.5 vs. 16.4%, P = 0.01) (Fig. 4).
m CONTROL
* OBSTRUCTIVE CENTRAL TYPE OF APNEA
Fig. 2. The incidence of central apneas was significantly higher than that of obstructive apneas in both groups. The incidence of central apneas was lower and that of obstructive apneas was significantly higher in the BPD than in the control group. Values represent mean f SE. (tP ~0.05 between central and obstructive; *P <O.OS between BPD and control group).

m ??PD
m CONTROL
Fig. 3. The incidence of obstructive apneas increased in REM sleep in both groups (tP s 0.05 between sleep states). The incidence of obstructive apneas was higher in the BPD group than in the control group in quiet and REM sleep but this was of marginal significance only.
Fig. 4. The percentage of obstructive apneas was significantly higher in long apneas than in short apneas in both groups. Note that in the BPD group the percentage was higher than in the control group. (tP S 0.05 in relation to 2 10 s; *P 5 0.05 in relation to control).
Oxygen saturation, heart rate, and ventilatory measurements In the BPD group, 24 out of 378 (6.4%) obstructive apneas, and 56 out of 2551
(2.2%) central apneas were associated with oxygen desaturations less than 80% (P < 0.05). In the control group, 13 out of 178 (7.3%) obstructive apneas and 16 out of 4188 (0.4%) of the central apneas were associated with such desaturation (P < 0.05). Similarly, in the BPD group, five out of 378 (1.3%) obstructive apneas and one out of 2551 (0.04%) central apneas showed bradycardia defined as a heart rate of less than or equal to 80 beats/min (P < 0.05); in the control group, seven out of 178 (3.9%) obstructive apneas and eight out of 4188 (0.2%) central apneas showed bradycardia (P < 0.05). Although obstructive apneas were associated with more desaturations and bradycardias, the proportion of these remained statistically similar in both groups. Finally, there were no particular trends in ventilatory measurements made either before or after apnea which could characterize the presence of an obstructive versus a central apnea (Fig. 5).
Discussion
We found that the incidence of obstructive apneas was higher in infants with bron- chopulmonary dysplasia than in control infants. These differences applied to all sleep states. This incidence was also higher in apneas shorter than 10 s and in those equal or longer than 10 s. There was also a significant increase in the incidence of obstructive apneas in apneas longer than 10 s compared with those shorter than 10 s in both groups of infants. There was no particular ventilatory pattern associated with either central or obstructive apneas. These findings suggest that (1) the discrep- ancy in the incidence of obstructive apneas reported in the literature may be depen-

203
Fig. 5. Ventilatory variables in five breaths before and after apnea are summarized in this figure. No statistical significances were reached when comparing central vs. obstructive apneas.
dent, at least in part, on whether the infant had or did not have BPD and (2) ventilatory pattern is not predictive of either type of apnea.
Previously we found a predominance of central apneas in healthy infants but sick infants were not studied [4]. Similarly, publications from other investigators have primarily concentrated on populations recovering from RDS which suggest that they may have had some degree of residual lung disease or BPD [5,9]. Bentele et al. [l] however studied a group of infants recovering from RDS and compared them with

204
healthy infants. They found that at 40 weeks of postconceptional age obstructive apneas were less in the sick group than in the control group but obstructive apneas predominated at 54 and 62 weeks of postconceptional age. The differences were observed during non-rapid eye movemements (quiet sleep) only. In the present study, we noticed that infants with BPD had more obstructive apneas than control infants in the various sleep states, although this was significant only in quiet and REM sleep. The findings of Bentele et al., although at somewhat later postconcep- tional age, appear to support the present observations.
Recently, Sekar et al. [ 171 measured the incidence of obstructive apneas in a group of infants with BPD matched to a control group. They found that BPD infants without supplemental oxygen had more central apneas than non-BPD infants and there was no difference in the incidence of obstructive apneas. The exact reason for the differences in their study and ours is not entirely clear. However, when oxygen was given to their BPD infants, maintaining similar oxygen saturation to the control group, the non-BPD group had more central apneas, a finding similar to ours, although the incidence of obstructive apneas remained unchanged. Because our BPD infants were on supplemental oxygen and their saturations were similar to the con- trol group, our results should be compared with their BPD group on supplemental oxygen. Thus the only difference remaining is related to the incidence of obstructive apneas. This could be explained by the later postconceptional ages of their groups (37.1 and 38.0 weeks in the BPD and non-BPD groups) compared with ours (33.3 and 33.4 weeks), a fact that could imply that their BPD infants were as healthy as their control infants in which case a difference would not be expected.
Purely obstructive apneas are rare. Because mixed apneas, with some obstructive breaths occurring at the end of the respiratory pause, comprised the majority of obstructive apneas, we thought that obstruction might be more prevalent in the long rather than in the short apnea. Our results confirmed this prediction, the incidence of obstructive apneas being significantly greater in apneas longer than in those shorter than 10 s. The reason for this increase in obstruction with the length of apnea is not entirely clear. Studies done in anesthetized cats suggested that central inhibi- tion of breathing is associated with general loss of airway motor tone and possible collapse [18]. It is tempting to speculate that such mechanism is present in mixed apneas in which central inhibition of breathing would be followed by airway collapse and obstruction. This collapse would affect both upper and lower airways.
In the present study we have elected to consider all apneas greater than three seconds. The rationale for this choice was to determine whether obstructive apneas predominated when all ranges of apneas were considered. The more prolonged pathologic apneas - those equal or longer than 20 s -occur in infants who are also having short apneas. To understand better the overall profile of obstruction we thought it would be important to consider all apneas greater than three seconds, although it is understood that short apneas (< 5 s) are benign and in general, of no clinical significance. Fig. 2 shows that even in apneas less than 10 seconds, obstruc- tive apneas predominated in the BPD group. This finding suggests that obstruction is probably more likely to occur in infants with BPD, but the length of apnea may enhance this effect. It is conceivable that airway narrowing; hypoxemia, or both, present in infants with BPD may contribute to airway obstruction. Increased satura-

205
tion would tend to stabilize the respiratory control system and diminish the appearance of central apneas.
Because obstructive apneas were longer and associated with more desaturations and bradycardias than central apneas, we thought that breath-to-breath measure- ments of ventilatory variables preceding or following apnea could differ. Our results however showed that there were no specific changes in ventilation which would in- dicate an imminent obstruction. The findings are probably best explained by the fact that these two types of apneas appear to be predominantly central in origin; in the obstructive type, the obstruction generally occurs towards the end of the respiratory pause (mixed apneas).
In conclusion, we found that the incidence of obstructive apneas was increased in infants with bronchopulmonary dysplasia compared to controls. This appeared to occur in all sleep states although differences approaching significance were observed in quiet and REM sleep states only. These findings suggest that the incidence of obstructive apneas depends, at least in part, on whether the infant has or has not BPD and whether apneas are long or short. We further speculate that this obstruc- tion may, at least in part, be enhanced by hypoxic airway constriction present in these infants [l 11. Finally, there were not specific changes in ventilatory pattern associated with a given type of apnea.
Acknowledgements
This work was supported by the Medical Research Council of Canada, grant MT- 4980, the Manitoba Medical Services Foundation and the Children’s Hospital of Winnipeg Research Foundation. The authors wish to thank Debbie Bialek, Sheena Schiissler and Marie Meunier for typing and helping in the preparation of this manuscript.
References
1 Bentele, K.H.P., Albani, M., Budde, C. and Schulte, E.J. (1985): Sleep apnoea profile in preterm infants recovering from respiraiory distress syndrome. Arch. Dis. Child., 60, 547-554.
2 Butcher-Puech, M.C., Henderson-Smart, D.J., Halley, D., Lacey, J.L. and Edwards, D.A. (1985): Relation between apnoea duration and type and neurological status of preterm infants. Arch. Dis. Child., 60, 953-958.
3 Dranslield, D.A., Spitzer, A.R. and Fox, W.W. (1983): Episodic airway obstruction in premature infants. Am. J. Dis. Child., 137, 441-443.
4 Lee, D.S., Caces, R., Kwitatkowski, K., Cates, D. and Rigatto, H. (1987): A developmental study on types and frequency distribution of short apneas (3 to 15 sets) in term and preterm infants. Pediatr. Res., 22, 344-349.
5 Mathew, O.P., Roberts, J.L. and Thach, B.T. (1982): Pharyngeal airway obstruction in preterm in- fants during mixed and obstructive apnea. J. Pediatr., 100, 964-968.
6 Miller, M.J., Carlo, W.A., DiFiore, J.M. and Martin, R. (1988): Airway obstruction during periodic breathing in premature infants. J. Appl. Physiol. 64, 2496-2500.
7 Rigatto, H. and Brady, J.P. (1972): Periodic breathing and apnea in preterm infants. I. Evidence of hypoventilation possibly due to central respiratory depression. Pediatrics, 50, 202-218.
8 Rigatto, H. and Brady, J.P. (1972): Periodic breathing and apnea in preterm infants. II. Hypoxia as a primary event. Pediatrics, 50, 219-228.
9 Thach, B.T., Brouillette, R.T., Abu-Osba, Y.K., Wilson, S.L. and Mathew O.P. (1980): Prevalence of mixed and obstructive apneic spells in preterm infants (abstract). Pediatr. Res., 14, 637.

206
10
11
12
13
14
15
16
17
18
Davi, M., Sankaran, K., MacCallum, M., Cates, D. and Rigatto, H. (1979): The effect of sleep on chest distortion and on the ventilatory response to CO* in neonates. Pediatr. Res., 13, 982-986. Tay-Uyboco, J.S., Kwiatkowski, K., Cates, D.B., Kavanagh, L. and Rigatto, H. (1989): Hypoxic airway constriction in infants of very low birth weight recovering from moderate to severe bron- chopulmonary dysplasia. J. Pediatr., 115, 456-459. Bancalari, E. and Gerhardt, T. (1986): Bronchopulmonary dysplasia. Pediatr. Clin. N.Am., 33, l-23. Moriette, G., Van Reempts, P., Moore, M., Yorke, K. and Rigatto, H. (1985): The effect of rebreathing CO, on ventilation and diaphragmatic electromyography in newborn infants. Respir. Physiol., 62, 387-397. Luz, J., Winter, A., Cates, D., Moore, M. and Rigatto, H. (1982): Effect of chest and abdomen un- coupling on ventilation and work of breathing in the newborn infant during sleep. Pediatr. Res., 16, 297A. Dreyfus-Brisac, C. (1970): Ontogenesis of sleep in human prematures after 32 weeks of conceptional age. Dev. Psychobiol., 3, 91-121. Dreyfus-Brisac, C. (1979): Ontogenesis of brain bio&ctrical activity and sleep organization in neonates and infants. In: Human Growth, Vol. 3, p. 157. Editors: F. Falkner and J.M. Tanner. Plenum, London. Sekar, K.C. and Duke, J.C. (1991): Sleep apnea and hypoxemia in recently weaned premature in- fants with and without bronchopulmonary dysplasia. Pediatr. Pulmonol., 10, 112-l 16. Mitchell, R.A., Herbert, D.A. and Baker, D.G. (1985): Inspiratory rhythm in airway smooth muscle tone. J. Appl. Physiol., 58, 911-920.