Embed Size (px)
DESCRIPTION
International conference «Actual approaches to the extremely preterm babies: International experience and Ukrainian realities» (Kyiv, Ukraine, March 5-6, 2013)
Citation preview

Strategies for the Prevention of
Bronchopulmonary Dysplasia:
Wishful Thinking or Reality?
S. David Rubenstein, MD

Chronic Pulmonary Disorder which is
Consequence of Lung Injury that is
Abnormally Repaired
Bronchopulmonary
Dysplasia (BPD)

Old Definition of BPD
Need for supplemental oxygen at
> 28 days or > 36 wks gestation.

New Definition of BPD
• Mild BPD: need for supplemental oxygen > 28
days but not at 36 weeks gestation PMA
• Moderate BPD: need for supplemental oxygen >
28 days and < 30% at 36 weeks PMA
• Severe BPD: need for supplemental oxygen > 28
days, and > 30% at 36 weeks PMA and/or
positive pressure at 36 weeks PMA

Incidence of BPD at Columbia
BW(g) GA(wks) O2 (36 wks) Mild Mod. Severe
< 750 25.4±2.0 18.3% 31.6% 15.0% 3.3%
750-1000 26.9±1.8 1.4% 16.9% 1.4% 0
1001-1250 29.0±1.8 1.1% 0 1.1% 0
<1250 27.4±2.4 5.9% 14.1% 5.0% 0.9%
Sahni R., PAS 2003

“Old” BPD
• Disorder related to lung injury.
• Common in term & near term infants ventilated with
high pressures and O2 .
• Chest x-ray demonstrates areas of over-inflation, cystic
emphysema and fibrosis.
• Histopathology demonstrates interstitial and alveolar
edema, small airway disease, extensive inflammation and
fibrosis.

“Old” BPD

“New” BPD
• More of a disorder resulting from processes that
interfere with lung development, not injury.
• Common in VLBW infants with modest ventilatory
and oxygen needs.
• Chest x-ray: diffuse haziness which progresses to a
fine lacy pattern.
• Histopathology: decreased alveolarization, minimal
small airway disease and less inflammation/fibrosis.

“New” BPD

New BPD:
Diminished Alveolarization
• Normal alveolarization begins about 28 weeks
gestation: infants at term gestation have 20-50% of the adult
number of alveoli
• A variety of processes interfere with alveolarization
including: poor nutrition, hypoxia, hyperoxia, inflammation
and glucocorticoids

New BPD:
Diminished Alveolarization
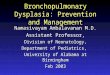
88 A.H. Jobe, M. Ikegami / Early Human Development 53 (1998) 81 –94
Fig. 4. Alveolar numbers for human infants at birth and for ventilated infants. The curve indicates the
normal increase in alveolar number with gestation age. Ventilation of the preterm lung results in decreased
alveolar numbers. Data from Hislop and co-workers [46,47].
7. Lung injury with the initiation of ventilation
Vyas et al. [48] measured lung expansion after term birth and observed high
negative esophageal pressures with inspiration and high positive esophageal pressures
with expiration. Adequate tidal volumes and functional residual capacities were
achieved most effectively in asphyxiated term infants when long inspiratory times (5
s) were used to initiate ventilation [49]. The long inspiratory times and relatively high
pressures overcome the resistance of fluid movement down the airways, a process
facilitated by high surfactant concentrations in fetal lung fluid at term. There have
been no systematic studies of the initiation of ventilation in VLBW infants. In animal
models, air opening pressures for fluid filled fetal lungs decrease as fetal lung fluid
volumes decrease and decrease as surfactant concentrations increase [50,51]. How-
ever, if fetal lung fluid volumes are very low, opening pressures increase because of
airway collapse [50], a situation that can occur after prolonged rupture of membranes.
Initiation of ventilation in VLBW infants often requires pressures greater than 30
cmH 0, probably because surfactant concentrations are low and fetal lung fluid2
volumes are high as a result of immature fluid clearance pathways. The generally
accepted goal for ventilation of the VLBW infant after delivery is to achieve a pink
infant with a P of about 40 mmHg as soon as possible, and this may not be easilyCO 2
achievable without risking lung injury. The VLBW infant destined to have RDS may
have a total lung capacity of only 20 ml /kg (Fig. 2). The lungs will inflate poorly and
nonuniformly because of surfactant deficiency despite the use of high pressures, and
ventilation in the midst of a resuscitation may not effectively limit tidal volumes to
volumes that will not enter the high volume injury zone. In practice this injury zone
Jobe et al, Early Human Development: 53 (1998) 81-94

Factors Contributing to Lung Injury
Jobe: Neoreviews 2006

Intrauterine Inflammation Increases the Risk of
Preterm Birth
• Histopathological evidence of chorioamnionitis is
present in 40-70% of preterm births (vs. 4-18% of
term deliveries)
• Incidence of infection (positive AF culture) is
32-35% with pPROM and 10-15% (spontaneous
onset of preterm labor with intact membranes)

Goldenberg et al NEJM 342: 1500-07, 2000
Incidence of positive chorioamniotic cultures in
women with intact membranes undergoing cesarean
section after spontaneous preterm labor

Percent of placentas harboring a microorganism
Biopsy of the chorion from 1,083 placentas (initiator of delivery: preterm
labor, preeclampsia) before the 28th week (Culture/PCR)
Week of pregnancy 23 24 25 26 27
Initiator of Delivery Route
Preterm labor: CS 56 62 42 46 34
vaginal 87 74 68 48 58
Preeclampsia: CS 33 24 21 28 22
Onderdonk and the ELGAN study group Am. J Obstet. Gynecol: July 2008

Intrauterine Infection and Preterm Labor
Goldenberg,
NEJM: May, 2000

There is a strong relationship between markers of
inflammation and BPD
• Amniotic fluid proinflammatory cytokine levels are
increased in infants who develop BPD
• Cord blood IL-6 concentration is an independent risk
factor for BPD and a better predictor than amniotic fluid
IL-6 levels.
Ghezzi 1998 & Yoon 1997, Yoon 1999

There is a strong relationship between markers of
inflammation in amniotic fluid and BPD
Yoon, Am J Ob Gyn; Oct 1997, 825-830

Intrauterine Infection, MMP-8 and CLD
Romero et. al., Am J Ob Gyn 2001, 185: (5)1149-1155
Halliday et. al., Arch Dis Child Fetal Neonatal ed 2004; 89: F61-64 2001; 84: F168-171

Intrauterine Inflammation & Risk of Chronic Lung
Disease
Chorioamnionitis No chorioamnionitis
RDS 33% 73%
BPD 63% 27%
Watterberg K. Ped. 1996 & 1997
* p< 0.003 * p<0.01
*
* *
*
*

Antenatal Administration of
Endotoxin in Fetal sheep
• Promotes lung maturation
• Increases proinflammatory cytokine expression (5 hrs)
• Increases influx of leucocytes
• Interferes with alveolar development
• Augments the inflammatory response when ventilated
Newnham 2001, Newnham 2002, Kramer 2001,
Kramer 2002, Moss 2002, Jobe 2001

Chorioamnionitis, Mechanical Ventilation &
Postnatal Sepsis: Modulators of Chronic Lung
Disease
• Chorioamnionitis 0.2 (0.0-0.5)
• Postnatal sepsis 1.3 (0.2-2.3)
• Ventilation> 7 d 1.6 (0.9-2.9)
• Ventilation > 7d and 3.2 (0.9-11)
chorioamnionitis
• Ventilation > 7d and 2.9 (1.1-7.4)
postnatal sepsis Van Marter J Ped. 2002

Mechanical Ventilation
Inflammation & Alveolarization
• Mechanical ventilation in experimental animals
with or without high O2 concentrations injures the
lung (and decreases alveolarization)
• Infants that progress to chronic lung disease have
persistence of leukocytes in alveolar lavages with
high concentrations of inflammatory mediators.

• Ventilation at low lung volumes (atelectrauma) also
causes release of cytokines and influx of white blood
cells.
Mechanical Ventilation
Inflammation & Alveolarization
• Over distention of the lung during mechanical
ventilation (volutrauma) disrupts structural elements
and leads to production of inflammatory mediators
(cytokines and chemokines).

Lung Injury Zones
Jobe and Ikegami 1998

Delivery Room Management
“Chronic Lung disease in preterm neonates may result
more from antepartum or delivery room events than
postnatal management.” (Jobe, J. Peds 1998)
“There is perhaps nothing more dangerous for the
preterm lung than an anxious physician with an
endotracheal tube and a bag” (Jobe, J Peds. 2005)

Delivery Room Management
• In infants with RDS, total lung capacity is
reduced by a widespread proteinaceous edema
• Mechanical ventilation aggravates the edema
(probably by epithelial disruption); surfactants
decrease the edema.

Delivery Room Management
• Surfactant instilled after mechanical ventilation
may be inactivated by leaking protein and may
fail to enter collapsed or fluid filled regions.
• This suggests that surfactant should be given as
early as possible. However, clinical trials have
not shown a consistent benefit to prophylaxis.

Delivery Room Management
Can lung damage occur immediately after
birth by giving a few large breaths?
If yes, will surfactant still be effective?

Neonatal Resuscitation
& Lung Injury
Bjorkland et al Ped. Res. 42: 348, 1997
Five pairs of lamb siblings were delivered at 127-128 d
gestation and one lamb in each pair was randomly
selected to receive 6 manual inflations at a volume
equal to inspiratory capacity (35-40 ml) before the start
of mechanical ventilation. All lambs then received
surfactant at 30 minutes of age.

Neonatal Resuscitation
& Lung Injury
Bjorkland et al Ped. Res. 42: 348, 1997
• Blood gases and pressure volume curves were
then recorded until the lambs were sacrificed at age
four hours.
• Lung histopathology was then examined

Neonatal Resuscitation
& Lung Injury
Bjorkland et al Ped. Res. 42: 348, 1997)
Pressure (cm H2O)
Control lambs Experimental group
15 15 30 30
Volu
me
(ml/
kg)
Volume (ml/kg
5 5
30
10 10 Before surfactant Before surfactant
45-135 min. 45 min.
75 min.
135 min.
20

Resuscitation & Lung Injury
Bjorkland et al Ped. Res. 42: 348, 1997

Neonatal Resuscitation
& Lung Injury • Ventilation with large breaths in an immature lung
may cause:
• Epithelial and microvascular injury
• Increased production of inflammatory mediators
• Flux of fluid into the air spaces
•Flux of fluid into the air spaces

Lung Overdistension Jobe
Am J Respir Crit Care Med 176: 575-581 (2007)
(PIP = 45-50 cm H2O)

Lung Overdistension Jobe
Am J Respir Crit Care Med 176: 575-581 (2007)
Bronchoalveolar lavage fluid: TP and cell count
Increased 5-fold, 11-fold, 14-fold
Increased 300-fold
* p < 0.01

Lung Overdistension Jobe
Am J Respir Crit Care Med 176: 575-581 (2007)
Cytokine mRNA in lung tissue

• All newborn infants exhibit an increase in urine
output postnatally (usually in the first day of life).
• In infants with RDS, the diuretic phase is delayed
and commonly occurs between 24 & 48 hours of life.
• A delay in the onset of diuresis until 5-7 days is
associated with an increased risk of BPD.
Fluid Therapy & BPD

Study Source Design N Outcome
Van Marter J Ped 1990 CCS 223 Infants with BPD
received amounts of
crystalloid & colloid
Van Marter J Ped 1992 MVA 223 Incidence of BPD
strongly correlated
with volume of
colloid received
Fluid Therapy & BPD

Randomized Trials of Postnatal
Na+ Supplementation
• Costarino et al: (N=17) Na+ restriction during the first
3-5 days of life significantly decreased the incidence of
BPD (J Pediatr 1992)
• Hartnoll et al: (N=46) Delaying Na+ supplementation
until 6% of the body weight was lost had a beneficial
effect on the risk for continuing O2 requirement (Arch Dis Child F19 1999)

Antenatal Steroids & BPD (True or False?)
• Antenatal steroids decrease the incidence
of bronchopulmonary dysplasia.

Antenatal Glucocorticoid Treatment
Does Not Reduce Chronic Lung Disease
Among Surviving Preterm Infants
Study Design: Case-referent study of 1454 LBW infants
born between 1991-93 at four university hospitals
Outcome: In multivariate logistic regression analyses
antenatal steroid Rx did not significantly decrease the rate
of CLD. OR .98 (.66-1.5)
Van Marter J Ped. 2001

Surfactant & BPD
True or False?
• The use of surfactant has decreased the likelihood
of chronic lung disease.
• Surfactants work best when given before the first
breath.

Surfactant Delivery room prophylaxis
Mortality
BPD
Pneumothorax
Treatment of RDS
Mortality
BPD
Pneumothorax
Natural Synthetic
•
•
•
•
•
•
• •
•
•
•
1.0 1.0

Continuous Positive
Airway Pressure

If you do not ventilate neonates
it’s hard to cause BPD!

The Significance of Grunting in
Hyaline Membrane Disease
• In infants with HMD, grunting is a protective
maneuver resulting from contraction of the
abdominal muscles and closure of the glottis
• Grunting can be prevented by intubation
• Intubation (and elimination of grunting) resulted
in a fall in oxygenation
Harrison et al Ped. 1968

Gregory et al. N Engl J Med 284: 1333, 1971
Treatment of idiopathic respiratory distress
syndrome with continuous positive airway pressure

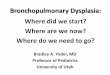
Weight N PaO2 (pre) PaO2 (post)
930-1500 10 37.1 116.4
1501-2000 5 38.1 114.8
2001-3830 5 48.6 96.0
Treatment of idiopathic respiratory distress
syndrome with continuous positive airway pressure
Gregory et al. N Engl J Med 284: 1333, 1971




Nasal CPAP

Survey of Infants Admitted to 8
Neonatal ICU’s
• No significant differences in survival
• Columbia had the lowest incidence of O2 use at
28 days and 3 months of age in survivors
• Observations: early use of CPAP, permissive
hypercapnia, no muscle relaxants, “J Wung”
Avery et al Pediatrics 79: 77, 1987

Do clinical markers of
barotrauma and oxygen
toxicity explain interhospital
variation in rates of chronic
lung disease?
Van Marter et al Pediatrics: 105, 1194, 2000

• Case-cohort study to evaluate the relationship between
NICU practices and the occurrence of BPD
• Birth weight 500-1500g (1991-93)
• Three NICUs: Babies, Beth Israel Hospital & Brigham
and Women’s Hospital
• Outcome: O2 at 36 weeks PMA
Columbia vs. Boston

Babies Boston
BPD 4% 22%*
CPAP 63% 11%*
Ventilation 29% 75%*
# days MV 13 d 27 d *
Surfactant 10% 45%*
Indomethacin 2% 28%*
Sedation 0% 46%*
Mortality 9% 10%
Postnatal Steroids 3% 4%
No significant differences in IVH, PVL, NEC or ROP

Long-Term Neurocognitive
Development

vLong-Term Neurocognitive
Development
Sanocka et al PAS 2002

Long-Term Neurocognitive
Development
Hypocarbia on day one was associated with a two-
fold increase in CP [odds ratio of 2.2 (1.0-4.0)]
Hypercarbia (PaCO2 > 55, < 65) had no effect on the
prevalence of CP, IQ or behavioral scores
Sanocka et al PAS 2002

Permissive Hypercapnia
• Intentional hypoventilation to avoid volutrauma
and diminish lung injury.
• Limited controlled data in infants to support its
efficacy & safety.

Lung Inflammatory Markers:
Effect of FiCO2
• Premature lambs studied at 132 days Exogenous surfactant to all (n=14) High TV and PIP for 30 minutes (10.8ml/kg, 40cm H2O)
• Group I IPPV (TV 6-8ml/kg): pCO2 of 40mm Hg for 5.5 hours
• Group II Same TV, PIP and F as group I; IPPV for 5.5 hours FiCO2 increased to maintain pCO2 of 95mm Hg.
• Alveolar wash after IPPV
Strand et al., Peds Research 2003

Lung Inflammatory Markers:
Effect of FiCO2
0
0.5
1
1.5
Protein Total WBC PMN H2O2
nl PCO2
hi PCO2
Strand et al., Peds Research 2003

Protective Effects: Hypercapnia
• Hypercapnic acidosis protects the heart and brain
against ischemic injury and protects the lung against
ischemic-reperfusion injury in experimental animals.
• Hypercapnia increases cardiac output and oxygen
delivery, decreases oxygen consumption, increases
mesenteric blood flow, attenuates oxygen induced
retinal neovascularization.

Protective Effects: Hypercapnia
• Hypercapnia upregulates pulmonary nitric oxide,
decreases inflammatory processes, and attenuates
production of free radicals.
• Human beings can tolerate exceptionally high
concentrations of CO2 and recover completely.
• Hypothesis: Hypercapnia may be protective in the
setting of acute organ injury.

CPAP started infants in 2 epochs, BW<1000g
1999-2002
(n=138)
2008-11
(n=235)
CPAP failure (%) 35 36
Surfactant given on failure (%) 52 63
Pneumothorax (%) 7.2 9.8
Mortality (%) 14.5 13.6
BPD (O2 at 36wk) (%) 10.9 8.1

Infants ≤1000g with RDS requiring
intubation after a trial of CPAP
Time of intubation pH PaCO2 PaO2/FiO2
(hrs)
CPAP-failure 29.7±18 7.19±.09 63±16
133±86
Blood gases at time of failure

Why is Columbia Successful with CPAP?
• Early use of NPCPAP
• Use of permissive hypercapnia
• Acceptance by nursing staff
• Bubble CPAP
• Meticulous attention to CPAP circuit
• Frequent suctioning; check prong position frequently
• Jen T. Wung, MD (be patient; give the baby a chance)

Lung Inflammatory Markers:
Effect of CPAP
• Premature lambs studied at 134 days labor induced with epostane and betamethasone vaginal delivery allows spontaneous breathing
• Lambs divided into 3 groups no IPPV IPPV at F = 40, PIP (maintain pCO2 at 40), PEEP 4 bubble CPAP, 5 cm H2O
• Evaluate lungs at 2 hours Jobe et al., Peds Research 2002

Lung Inflammatory Markers:
Effect of CPAP
7.1
7.2
7.3
7.4
7.5
0 15 30 60 120
time (minutes)
pH IPPV
CPAP
*
Jobe et al., Peds Research 2002

Lung Inflammatory Markers:
Effect of CPAP
30
40
50
60
70
80
0 15 30 60 120
time (minutes)
pC
O2
(m
m H
g)
IPPV
CPAP
Jobe et al., Peds Research 2002

Lung Inflammatory Markers:
Effect of CPAP
0
20
40
60
80
0 5 10 15 20 25 30 35 40
pressure (cm H2O)
volu
me (
ml/
kg)
IPPV
CPAP
Jobe et al., Peds Research 2002

Lung Inflammatory Markers:
Effect of CPAP
0
10
20
30
40
cell
s x
10
5/k
g
No IPPV IPPV CPAP
lymphs
mono
Jobe et al., Peds Research 2002

Lung Inflammatory Markers:
Effect of CPAP
0
2
4
6
8
neu
tro
ph
ils
x 1
05/k
g
No IPPV IPPV CPAP
PMN
Jobe et al., Peds Research 2002

Lung Inflammatory Markers:
Effect of CPAP
0
25
50
75
100
125
H2
O2
(m
icro
mo
les/
kg)
No IPPV IPPV CPAP
H2O2
Jobe et al., Peds Research 2002

The BPD Scorecard Intervention Relative Evidence
Importance
Antenatal steroids - strong
Surfactant + strong
DR management ++++ animal data
Fluid restriction ++ moderate
Early use of CPAP +++ minimal
Permissive CO2 +++ minimal







Nasal CPAP Set up ( 1 )
1. Oxygen blender
2. Flowmeter(5-10 LPM)
3. Heated humidifier
4. Thermometer
5. Inspiratory tubing
6. Nasal cannulae
7. Velcro

Nasal CPAP Set up ( 2 )
8. Manometer (optional)
9. Expiratory tubing
10. A bottle containing a
solution of 0.25% acetic
acid filled up to a depth of
7 cm. Distal tubing
immersed to a depth of 5
cm to create +5 cmH2O



Nasal CPAP Application (2)
4. Choose FiO2 to keep
PaO2 at 50’s or
O2 saturation at
83 – 93%

Nasal CPAP Application (3)
5. Adjust a flow rate 5-10 lpm to:
a) provide adequate flow to prevent rebreathings CO2
b) compensate leakage from tubing connectors and around CPAP prongs
c) generate desired CPAP pressure (usually 5 cmH2O)


Nasal CPAP Application (5)
7. Insert the lightweight corrugated tubing (preferrably with heating wire inside) in a bottle of 0.25% acetic acid solution or sterile water filled up to a height of 7 cm. The tube is immersed to a depth of 5 cm to create 5 cmH2O CPAP as long as air bubbling out of solution

Neonatal Resuscitation
& Lung Injury
Neonatal resuscitation bags can deliver
high volumes at very high pressures.
ComplianceLung = Δ Volume/Δ Pressure

Factors Contributing to Lung Injury
Jobe and Ikegami 1998

Effects of High TV Ventilation
Wada et al., J Appl Phys 1997

• Recovery from RDS is heralded by the onset of
diuresis.
• A delay in the onset of diuresis until 5-7 days is
associated with an increased risk of BPD.
• Diuretics may facilitate extubation in infants with
RDS who are not exhibiting a spontaneous diuresis.
Fluid Therapy & BPD

Study Design N BW Outcome
Bell et al* RCT 170 ~1430g No difference
Lorenz et al** RCT 88 ~1180g No difference
Tammela@ RCT 100 ~1300g BPD (4 wks)
Kavvadia # RCT 168 ~ 900g No difference
Fluid Therapy & BPD
*NEJM 1980, **J Ped 1982, @ Eur J Ped 1992, # Arch. Dis Child 2000

Permissive Hypercapnia
•VLBW infants with RDS (n= 49) randomized to a
hypercapnia group (PHC) (PCO2 45-55) or normo-
capnia group (NC) (PCO2 35-45).
• The total number of days on assisted ventilation was
2.5 in the PHC group and 9.5 in the NC group (P=.17).
• No difference in BPD, IVH, PVL or air leak
Mariani et al Pediatrics 1999