Embed Size (px)
DESCRIPTION
Articulo que habla sobre el manejo nutricional de los lactantes con broncodisplasia pulmonar.
Citation preview

Nutritional Management of the Infant WithSevere Bronchopulmonary DysplasiaJennifer Curtiss, RD,*
Huayan Zhang, MD,†
Pamela Griffiths, MD,‡
Edward G. Shepherd, MD,x
Susan Lynch, MDx
AUTHOR DISCLOSURE
Ms Curtiss and Drs
Zhang, Griffiths,
Shepherd, and Lynch
have disclosed no
financial relationships
relevant to this article.
This commentary does
not contain
a discussion of an
unapproved/
investigative use of
a commercial product/
device.
Education Gaps
1. Optimal growth and nutrition in infants with severe bronchopulmonary dysplasia
represent a complex interaction of the infant’s state and delivery of balanced
nutrition. Although this interaction is affected by level of respiratory support, the
infant’s environment, and caloric and protein intake, few high-quality studies are
available to guide nutritional management.
2. Most available studies have mainly addressed weight gain as a measure of growth,
whereas ongoing assessment requires incorporation of goals for linear growth in the
infant with severe bronchopulmonary dysplasia. More research is necessary to identify
ways to improve linear growth and promote balanced weight gain.
AbstractOptimal nutrition and growth in patients with severe, established bronchopulmonarydysplasia are complex and require an understanding of the factors and challenges thataffect this population. Most publications have reported weight gain as the primary out-come because of ease of measurement, accuracy, and repeatability. There is, however,increasing evidence that linear growth is better correlated with long-term developmentand pulmonary outcomes. In addition, factors such as stress, inflammation, respiratorysupport and stability, and medication exposures have a direct influence on achieving nu-tritional success in infants with severe bronchopulmonary dysplasia. This article reviewsconcepts related to these challenges and provides recommendations for achieving suc-cessful nutrition in this population.
Objectives After reading the article, readers should be able to:
1. Understand the complexity of the older preterm infant with severe bronchopulmonary
dysplasia (36 weeks’ corrected age and older) as it pertains to successful nutrition and
a progrowth state.
2. Understand the importance of linear growth as a goal in successful nutrition in the
patient with severe bronchopulmonary dysplasia.
3. Understand the importance of balanced weight for length proportions in this population.
4. Understand what factors may alter nutritional needs in the patient with severe
bronchopulmonary dysplasia.
IntroductionInfants with severe bronchopulmonary dysplasia (BPD) have complex and multifactorialnutritional challenges. These infants have periods of hypermetabolic states, often due toincreased work of breathing, and also have generalized growth suppression from chronicstress, inflammation, long-term hospitalization, infection, and medications. The primarygoal of nutritional support in this population is to deliver optimal constituents matchedto the specific needs of each patient at every critical period. This requires an understandingof the multiple factors that can affect the overall growth of the infant and how these are
*Department of Clinical Nutrition and Lactation, Nationwide Children’s Hospital, Columbus, OH.†Department of Pediatrics, Children’s Hospital of Philadelphia, University of Pennsylvania Perelman School of Medicine,
Philadelphia, PA.‡Pediatrix Medical Group, Phoenix Children’s Hospital, Phoenix, AZ.xDivision of Neonatology, Department of Pediatrics, Nationwide Children’s Hospital, Ohio State University, Columbus, OH.
Article pulmonology
e674 NeoReviews Vol.16 No.12 December 2015
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from

affected by disease progression. Long-term pulmonaryoutcome studies highlight the persistence of develop-mental lung abnormalities into young adulthood.
Unfortunately, few prospective nutritional data areavailable in patients with severe BPD, although there isstrong evidence that infants with severe BPD attain lowerrates of postnatal weight gain and growth than preterminfants without BPD. In addition, there is an inverse as-sociation between growth velocity and the proportion ofinfants who develop severe BPD. It is also clear that ad-equate nutrition is critical for lung growth, lung function,and tissue repair. Moreover, better nutritional measurescorrelate with better neurodevelopmental outcomes. Fi-nally, it is becoming increasingly evident that the growthstate of the infant is crucial and heavily affected by growthfactors that are often suppressed by stress and inflamma-tion. Therefore, balanced weight gain and linear growthrely on accomplishing both a progrowth state and deliv-ery of adequate constituents. We discuss these principlesand how they relate to the assessment of infants with se-vere BPD, how to determine the growth state, the opti-mal goals for constituents that are supplied to the infant,and factors that have negative nutritional effects.
Risk Factors for Suboptimal Nutrition in thePreterm Infant With BPDBPD is associated with numerous factors that negativelyaffect growth, including increased caloric expendituredue to increased work of breathing and sometimes irrita-bility, infection, inflammation, chronic stress, and medi-cation exposure.
Infection is common in preterm infants and causes in-creased energy expenditure in the short term and duringthe recovery phase. Protein catabolism ensues becauseadditional substrate is necessary for gluconeogenesisand production of acute-phase reactants. Fat use is im-paired, and fatty acid oxidation may be reduced. Theseeffects are mediated by cytokine response, endogenousglucocorticoids, and catecholamine release. Chronic in-flammatory states also affect growth through suppressionof insulin-like growth factor (IGF-1), a hormone criticalfor optimal growth. Markers of inflammation, includinginterleukin-6, C-reactive protein, and erythrocyte sedi-mentation rate, are associated with decreased IGF-1.Chronic stress is also associated with growth impairment,and elevated cortisol levels correlate with decreasedgrowth and suppression of IGF-1. The intensive care en-vironment causes chronic stress through noise, varying sleeppatterns, suboptimal developmental environment, and pain-ful procedures. The effect of these factors on growth in pre-term infants with BPD has not been determined, but there
is some evidence that mitigating these effects through infantmassage and increased parental presence is associated withimproved weight gain.
Some medications administered to infants with BPDresult in short-term clinical improvement but have a neg-ative effect on growth and nutrition. Systemic corticoste-roid administration in preterm infants leads to short-termgrowth failure, likely due to decreased IGF-1 and IGF-binding protein 3. Impaired glucose and fat use and pro-teolysis also play a role. In addition, calcium absorption isdecreased, and calcium and phosphorus retention is im-paired. The effects of systemic corticosteroids on growthmay extend into early childhood. Inhaled corticosteroidshave a dose-dependent growth suppressive effect in olderchildren, but there is no information on the effect of shortbursts of corticosteroids for management of acute airwayexacerbation in BPD.
The use of diuretics may cause electrolyte abnormalities,including hypochloremic metabolic alkalosis, hyponatre-mia, hypokalemia, hypomagnesemia, and hypocalcemia.Each of these, abnormalities may affect growth and bonemineralization. Hypochloremia leads to growth failure ininfants, whereas loop diuretics cause hypercalciuria, exacer-bate bone demineralization, and may lead to nephrocalci-nosis. Use of thiazide diuretics leads to increased distaltubular calcium uptake, but this effect may be lost if sodiumsupplementation is administered. Thiazide diuretics maylead to zinc insufficiency caused by an increase in urinaryzinc loss, which may negatively affect growth because zincplays an important role in growth and immune systemfunction.
Many important questions remain regarding the ef-fects of inflammation, stress, and medications on growthand nutritional requirements in preterm infants withBPD. These questions relate to the metabolism in respi-ratory and systemic infections, effect of stress related tothe neonatal intensive care unit (NICU) environment,utility of biomarkers of stress and growth factors, and ef-fect of short courses of oral corticosteroids for reactiveairway flare-ups. In addition, the long-term effects ofinhaled corticosteroids (patients receiving and not receiv-ing ventilator assistance) and outcomes of long-term di-uretic use in patients with severe BPD are unknown.
Prevention of these adverse effects includes measures toprevent infection (limiting use of central catheters, handhygiene), avoidance of inflammation, and reduction ofstressful stimuli (limit painful procedures, reduce noise).In addition, neuromodulation with kangaroo care andhand containment have produced encouraging results.
Diuretic use should be avoided if possible; however,when necessary, use should be brief and goal directed
pulmonology severe bronchopulmonary dysplasia
NeoReviews Vol.16 No.12 December 2015 e675
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from

(extubation, stabilization). Systemic corticosteroids shouldbe used judiciously to achieve an optimal balance of anti-inflammation and nutrition to promote growth. Few dataexist to guide initiation, dosage, and duration of inhaledcorticosteroid treatment.
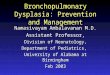
Assessment of Growth and Nutrition StatusNutritional assessments should include a review of prena-tal and past medical history, anthropometric data, medi-cation exposure, current therapies, and biochemical andclinical status. Anthropometric data typically consist ofmeasurements of weight, length, and head circumferenceand should be compared to reference data. These datashould be plotted and followed along an infant growthchart to better assess growth trajectories. Although weightcan be measured easily and accurately, it is influenced byfluid status and may not reflect changes in lean body mass.Linear growth is the best measure of assessing adequacy ofdietary intake and determining the presence of a progrowthstate in the infant. Linear growth is associated with leanbody mass accretion and organ growth and development.Lack of linear growth is common in this patient populationand is thought to be due to all the factors discussed above.Linear growth suppression is negatively associated withlong-term developmental outcomes (Fig 1).
Measuring length in a precise and reproducible manneris challenging in the NICU setting. Use of a recumbent-length board to measure crown-heel length is the mostaccurate and reliable means of assessing linear growth.Weight for length status should then be assessed for pro-portionality (weight/length at the 50th percentile) to avoid
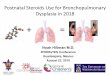
overweight status. Persistent weight gain at a rate thatcrosses growth chart percentiles without the same patternin linear growth warrants a reevaluation of energy intake,and is often associated with a change in the clinical status ofthe patient (change in energy expenditure, activity, expo-sure to corticosteroids) (Fig 2).
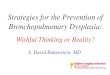
Premature infants with intrauterine growth restrictionand/or those who are small for gestational age have in-creased risk for abnormal growth patterns in the postnatalperiod and an increased risk for severe BPD with pulmo-nary hypertension (Fig 3).
Nutritional Constituents or SupplyPremature infants, especially those with established lungdisease, have high caloric demands because of increasedwork of breathing and to meet the metabolic requirementsfor growth and healing; indeed, energy intakes often ex-ceed 130 kcal/kg daily. These demands may necessitatethe use of highly fortified mothers’milk or calorically densepreterm formula. Older infants with stable respiratory statusmay require substantially fewer calories, depending on theirstability and level of activity. Individualized nutritional sup-port with close monitoring and titration is important toavoid overfeeding or underfeeding.
Adequate protein intake is critical to achieving ade-quate linear growth, lung growth, and tissue repair. Pro-tein needs for the preterm infant are high, ranging from3.5 to 4.2 g/kg daily, but needs decrease as correctedgestational age increases. There are currently no evidence-based protein recommendations for the infant with severeBPD. However, improved linear growth, lean tissue accre-tion, and bone mass have been found in patients with BPD
Figure 1. A former infant with severe bronchopulmonarydysplasia and long-term corticosteroid exposure born smallfor gestational age with linear growth suppression and highweight for length status.
Figure 2. The same infant several months later after lineargrowth accelerated with the weaning of corticosteroids, less fluid,and fewer calories, along with a higher protein nutrition plan.
pulmonology severe bronchopulmonary dysplasia
e676 NeoReviews Vol.16 No.12 December 2015
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from

with higher intake of protein and other nutrients, such aszinc. Providing adequate protein for corrected gestationalage and aiming toward the higher range may be beneficialto compensate for periods of catabolic, hypermetabolicstates when protein turnover is high. Medications, espe-cially corticosteroids, also negatively affect protein accretionand body composition; however, no studies are availablefor guidance in this population.
Nutritional supply is further affected because infantswith severe BPD are prone to interstitial pulmonary edema.Although it is well known that liberal fluid administrationearly in the postnatal course is associated with increased riskof BPD, no studies address optimal fluid administrationonce BPD is established. These patients require conserva-tive fluid administration to manage pulmonary edemawhile maintaining adequate delivery of nutrients and waterto meet nutritional and physiological needs. Fluid require-ments for patients with the most severe BPD are in therange of 110 to 140 mL/kg per day and decrease through-out the first year of life.
No studies have been performed in patients with se-vere BPD regarding carbohydrate supply; however, inadults, higher carbohydrate loads are associated with
increased carbon dioxide production. Therefore, it is ad-visable to avoid excess carbohydrate intake unless absolutelynecessary; unfortunately, infant cereals and thickening agentsmay add a significant amount of carbohydrates and calorieswhile displacing important proteins and micronutrients nor-mally received from breast milk or formula.
Zinc is an essential micronutrient that plays an impor-tant role in the function of growth-stimulating hormonesand potentially linear growth. In infants at risk for poorlinear growth, one should consider zinc supplementationbecause zinc content naturally decreases in breast milkthroughout the lactation. The demand for zinc is highestduring the most rapid phases of growth.
Mother’s own milk is preferred for enteral feeds. Forti-fication with human milk fortifier is recommended; up to30 kcal/oz along with other additives may be required.If human milk is not available, preterm infant formulashould be used for essential nutrients and protein to sup-port growth and bone health. Semielemental and elementalformulas are not routinely indicated for this population.
Metabolic Bone DiseaseMetabolic bone disease (MBD), also called osteopenia ofprematurity, is common in preterm infants. MBD incidenceand severity increase with decreasing gestation and birthweight, and MBD is more common in sick preterm infantsand those with BPD.
Most infants with BPD are extremely low-birth-weight(ELBW) infants who are born with inadequate mineral ac-cretion, which occurs during the third trimester when cal-cium and phosphorus are actively transported across theplacenta. After birth, many additional factors contributeto the development of MBD. First, parenteral and enteralsupplements of calcium and phosphorus do not match inutero accretion rates. Second, preterm infants in the NICUare often subject to restricted movement, which leads todecreased infant muscle activity and consequentially lessnew bone. Third, these infants are typically exposed tomul-tiple drugs, which affect overall bone health and density.Indeed, many of these treatments activate osteoclasts, de-crease calcium absorption, reduce osteoblast effectiveness,and increase renal calcium excretion, resulting in bone de-mineralization. Loop diuretics, such as furosemide, increaserenal calcium excretion and can cause calcium harvestingfrom bones. Caffeine is a long-standing treatment for apneaof prematurity but leads to urinary calcium losses contrib-uting to MBD. Corticosteroids have several adverse effectson bone metabolism, including inhibition of osteoblastfunction, enhancement of bone resorption, inhibition ofgastrointestinal calcium absorption, and increases in urinarycalcium loss.
Figure 3. Preterm growth chart of infant showing lineargrowth failure, particularly at 42 weeks’ gestational age, withincreasing rate of weight gain.
pulmonology severe bronchopulmonary dysplasia
NeoReviews Vol.16 No.12 December 2015 e677
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from

MBD leads to biochemical, hormonal, and radiographicchanges. The typical biochemical picture of MBD includesnormal serum calcium, low serum phosphorus, and highserum alkaline phosphatase (ALP) concentrations. Serumcalcium levels are typically normal because of the counter-regulatory mechanisms of bone formation and resorptionthat are modulated by parathyroid hormone, calcitriol,and vitamin D. In infants with MBD, the serum para-thyroid hormone level is normal to increased. Elevated25-hydroxyvitamin D concentrations may be indicative ofMBD. Bone radiography may reveal fractures in the mostsevere cases of MBD. However, plain radiography is an in-sensitive tool for diagnosing MBD because it will not revealsubtle decreases of bone mineralization. Dual-energy X-rayabsorptiometry (DEXA) accurately reflects most stages ofbone demineralization, but it involves radiation exposurefor the infant and is not portable. In addition, ELBWstandards for DEXA have not been established.
Although diagnosing MBD on the basis of abnormalbiochemical analysis findings is controversial and unproven,most clinicians agree that low serum phosphate and highALP concentrations indicate bone disease. Some recentdata indicate that ALP level increased more rapidly duringthe first 10 weeks after birth, and maximum ALP levelswere higher in infants who developed rickets or fracture,suggesting that trending early ALP levels may providegreater utility than a single measurement when evaluatingMBD risk. Although standard bone radiography does notallow an accurate assessment of bone demineralization, itdoes allow detection of fractures and remains a practical as-sessment of the presence of overt rickets.
MBD that results in undermineralization, softening,or fractures of the ribs can exacerbate already compro-mised lung function. Multiple long bone fractures, alongwith limited pulmonary reserve, also further limit the in-fants’ ability to acquire motor skills and in this way contrib-ute to their long-term developmental delay. Results fromDEXA and quantitative ultrasonography indicate that pre-term infants have a catch-up phase in their bone mineral-ization in their first year of life, but long-term stuntingeffects have been documented in these infants. Future re-search should focus on improving early detection of MBDin high-risk infants and developing novel strategies to bothoptimize nutrition and minimize potentially avoidableharmful exposures.
ConclusionIn summary, optimal nutrition in patients with severe BPDis complicated bymany factors, including lack of prospectivedata in this population, changing needs of the patient overtime, growth suppressive states of disease, comorbidities,
and high metabolic needs. Linear growth is critical andshould be measured accurately using a length board thenfollowed closely on appropriate growth curves.
Weight for length should also be followed closely andnutritional adjustments made at least weekly in concertwith a dietitian familiar with the infant population. Thesetitrations should take into account the state of the infantand exposure to negative metabolic factors. Weight forlength near the 50th percentile should be targeted.
The state of the infant is complex and includes factorssuch as chronic stress, medication exposure, comorbid-ities, and inflammation, and the goal should be to mini-mize any factors that impair growth.
Much attention should be given to the nonpharmaco-logic support and comfort of the infant. Decreasing stressof the intensive care unit environment, proactive encour-agement of parent involvement, skin-to-skin neuromod-ulation, and adequate respiratory support to allowdevelopmental activities are key factors to a progrowthstate. This is an especially important concept for the in-fant with severe BPD with a prolonged hospital stay.
Suggested ReadingArdran GM. Bone destruction not demonstrable by radiography.
Br J Radiol. 1951;24(278):107–109Backström MC, Kuusela AL, Mäki R. Metabolic bone disease of
prematurity. Ann Med. 1996;28(4):275–282Baveja R, Christou H. Pharmacological strategies in the prevention
and management of bronchopulmonary dysplasia. Semin Peri-natol. 2006;30(4):209–218
Bera A, Ghosh J, Singh AK, Hazra A, Mukherjee S, MukherjeeR. Effect of kangaroo mother care on growth and devel-opment of low birthweight babies up to 12 months of age:a controlled clinical trial. Acta Paediatr. 2014;103(6):643–650
Bozzetti V, Tagliabue P. Metabolic bone disease in pretermnewborn: an update on nutritional issues. Ital J Pediatr.2009;35(1):20
Brunton JA, Bayley HS, Atkinson SA. Validation and application ofdual-energy x-ray absorptiometry to measure bone mass and
American Board of Pediatrics Neonatal-PerinatalContent Specifications
• Recognize the clinical features ofbronchopulmonary dysplasia/chronic lungdisease.
• Know the caloric requirements for optimalpostnatal growth of preterm and terminfants, accounting for caloricexpenditures needed for physical activity and maintenance ofbodily temperature.
• Know the protein requirements of preterm and full-terminfants.
pulmonology severe bronchopulmonary dysplasia
e678 NeoReviews Vol.16 No.12 December 2015
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from

body composition in small infants. Am J Clin Nutr. 1993;58(6):839–845
Brunton JA, Saigal S, Atkinson SA. Growth and body compositionin infants with bronchopulmonary dysplasia up to 3 monthscorrected age: a randomized trial of a high-energy nutrient-enriched formula fed after hospital discharge. J Pediatr. 1998;133(3):340–345
Check J, Gotteiner N, Liu X, et al. Fetal growth restriction andpulmonary hypertension in premature infants with bronchopul-monary dysplasia. J Perinatol. 2013;33(7):553–557
Ehrenkranz RA, Younes N, Lemons JA, et al. Longitudinal growthof hospitalized very low birth weight infants. Pediatrics. 1999;104(2, pt 1):280–289
Ferrone M, Geraci M. A review of the relationship betweenparenteral nutrition and metabolic bone disease. Nutr ClinPract. 2007;22(3):329–339
Foote JM, Brady LH, Burke AL, et al. Development of anevidence-based clinical practice guideline on linear growthmeasurement of children. J Pediatr Nurs. 2011;26(4):312–324
Kovacs CS, Ho-Pao CL, Hunzelman JL, et al. Regulation ofmurine fetal-placental calcium metabolism by the calcium-sensing receptor. J Clin Invest. 1998;101(12):2812–2820
Kovacs CS, Kronenberg HM. Maternal-fetal calcium and bonemetabolism during pregnancy, puerperium, and lactation.Endocr Rev. 1997;18(6):832–872
Lee SM, Namgung R, Park MS, Eun HS, Park KI, Lee C. Highincidence of rickets in extremely low birth weight infants withsevere parenteral nutrition-associated cholestasis and bronchopul-monary dysplasia. J Korean Med Sci. 2012;27(12):1552–1555
Linshaw MA, Harrison HL, Gruskin AB, et al. Hypochloremicalkalosis in infants associated with soy protein formula. J Pediatr.1980;96(4):635–640
Lucas A, Brooke OG, Baker BA, et al. High alkaline phosphataseactivity and growth in preterm neonates. Arch Dis Child. 1989;64(7 Spec No):902-909
Lyon AJ, McIntosh N, Wheeler K, Williams JE. Radiological ricketsin extremely low birthweight infants. Pediatr Radiol. 1987;17(1):56–58
Madden J, Kobaly K, Minich NM, et al. Improved weightattainment of ELBW infants with bronchopulmonary dysplasia.J Perinatol. 2010;30(2):103–111
Masel JP, Tudehope D, Cartwright D, Cleghorn G. Osteopeniaand rickets in the extremely low birth weight infant–a survey of
the incidence and a radiological classification. Australas Radiol.1982;26(1):83–96
McIntosh N, Livesey A, Brooke OG. Plasma 25-hydroxyvitamin Dand rickets in infants of extremely low birthweight. Arch DisChild. 1982;57(11):848–850
Mitchell SM, Rogers SP, Hicks PD, Hawthorne KM, Parker BR,Abrams SA. High frequencies of elevated alkaline phosphataseactivity and rickets exist in extremely low birth weight infantsdespite current nutritional support. BMC Pediatr. 2009;9(1):47
Nyp M, Taylor J, Norberg M, Truog W. Impaired growth at birthand bronchopulmonary dysplasia classification: beyond small forgestational age. Am J Perinatol. 2015;32(1):75–82
Portale A. Blood calcium, phosphorus and magnesium. In: FavusM, ed. Primer on the Metabolic Bone Disease and Disorders ofMineral Metabolism. Philadelphia, PA: Lippincott William &Wilkins; 1999:115–118
Ramel SE, Demerath EW, Gray HL, Younge N, Boys C, GeorgieffMK. The relationship of poor linear growth velocity withneonatal illness and two-year neurodevelopment in preterminfants. Neonatology. 2012;102(1):19–24
Rigo J, Senterre J. Nutritional needs of premature infants: currentissues. J Pediatr. 2006;149(5 suppl):S80–S88
Ryan SW, Truscott J, Simpson M, James J. Phosphate, alkalinephosphatase and bone mineralization in preterm neonates. ActaPaediatr. 1993;82(6-7):518–521
Shaikhkhalil AK, Curtiss J, Puthoff TD, Valentine CJ. Enteral zincsupplementation and growth in extremely-low-birth-weightinfants with chronic lung disease. J Pediatr Gastroenterol Nutr.2014;58(2):183–187
Sharp M. Bone disease of prematurity. Early Hum Dev. 2007;83(10):653–658
Theile AR, Radmacher PG, Anschutz TW, et al. Nutritionalstrategies and growth in ELBW infants with bronchopulmonarydysplasia over the past 10 years. J Perinatol. 2012;32(2):117–122
Viswanathan S, Khasawneh W, McNelis K, et al. Metabolic bonedisease: a continued challenge in extremely low birth weightinfants. JPEN J Parenter Enteral Nutr. 2014;38(8):982–990
Wang D, Vandermeulen J, Atkinson SA. Early life factors predictabnormal growth and bone accretion at prepuberty in formerpremature infants with/without neonatal dexamethasone exposure.Pediatr Res. 2007;61(1):111–116
pulmonology severe bronchopulmonary dysplasia
NeoReviews Vol.16 No.12 December 2015 e679
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.16-12-e6742015;16;e674NeoReviews
LynchJennifer Curtiss, Huayan Zhang, Pamela Griffiths, Edward G. Shepherd and Susan
DysplasiaNutritional Management of the Infant With Severe Bronchopulmonary
ServicesUpdated Information &
http://neoreviews.aappublications.org/content/16/12/e674including high resolution figures, can be found at:
Referenceshttp://neoreviews.aappublications.org/content/16/12/e674#BIBLThis article cites 30 articles, 7 of which you can access for free at:
Subspecialty Collections
_drug_labeling_updatehttp://classic.neoreviews.aappublications.org/cgi/collection/pediatricPediatric Drug Labeling Updatefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
htmlhttp://classic.neoreviews.aappublications.org/site/misc/Permissions.xin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.neoreviews.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.16-12-e6742015;16;e674NeoReviews
LynchJennifer Curtiss, Huayan Zhang, Pamela Griffiths, Edward G. Shepherd and Susan
DysplasiaNutritional Management of the Infant With Severe Bronchopulmonary
http://neoreviews.aappublications.org/content/16/12/e674located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1526-9906. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Online the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,it has been published continuously since . Neoreviews is owned, published, and trademarked by Neoreviews is the official journal of the American Academy of Pediatrics. A monthly publication,
by guest on December 1, 2015http://neoreviews.aappublications.org/Downloaded from