Embed Size (px)
Citation preview
The Impact of Intermittent Preventive Treatmentwith Sulfamethoxazole Pyrimethamine on PregnantWomen and Newborns at Bon Samaritain Hospitalin N'Djamena, Chad.Ngaba Ngardig Neguemadji ( [email protected] )
Faculte de Medecine Bon Samaritain: Centre Hospitalier Universitaire Bon Samaritain Faculte deMedecine https://orcid.org/0000-0002-4510-7923Obélix Askemdet
Faculte de Medecine Bon Samaritain: Centre Hospitalier Universitaire Bon Samaritain Faculte deMedecineNamrata Hange
National University of SingaporeMaria Kezia Lourdes Ligsay Pormento
Ateneo de Manila University Ateneo School of Medicine and Public HealthZeryab Ghous Dogar
Larkin Community Hospital IncAmel Braham Chaouche
Benyoucef Benkhedda University Algiers: Universite d'AlgerManoj Kumar Reddy Somagutta
Avalon University School of Medicine
Research
Keywords: Malaria, intermittent Preventive Treatment, Sulfadoxine-Pyriméthamine, Pregnancy, newborn,developing nation, Chad.
Posted Date: April 20th, 2021
DOI: https://doi.org/10.21203/rs.3.rs-427486/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Title: The impact of intermittent preventive treatment with sulfamethoxazole pyrimethamine on
pregnant women andnewborns at Bon Samaritain hosp ital in Chad.
Authors:
Neguemadji Ngardig Ngaba*1; Obélix Askemdet1; Namrata Hange2; Maria Kezia Lourdes Ligsay Pormento3;
Zeryab Ghous Dogar4; AmelBraham Chaouche 5; Manoj Kumar Reddy Somagutta6.
Authorss i nformations
1.Department of Obstetrics and gynecology, Bon Samaritain hospital, quartier Walia, PoBox: 456, ND jamena,
Chad.
2.Eurasian Cancer Research Council, B - 1210, Golf Scappe, Diamond Garden, Basant Garden, Chembur,
Mumbai, Maharashtra 400071, India
4.Department of medicine, Ateneo de Manila University school of Medicine and Public Health, Katipunan
Avenue, LoyolaH eights, Quezon City 1108, Philippines.
4-Department of research, Larkin communityhos pital, 7031 SW 62nd Ave, South Miami,F L33143, U SA
5.Department of Dermatology, university of Algiers Benyoucef Ben Khedda, 2 Rue Didouche Mourad, Alger
Centre16000, A lgeria
6.Department of medicine, Avalon university school of medicine, 122 - 124 Santa Rosaweg, Willemstad,
Curaçao
Corresponding author:N eguemadji Ngardig Ngaba. Email: [email protected]
ABSTRACT
Background: The Chadian government established a program of free intermittent preventive treatment with
sulfadoxine-pyrimethamine (IPTp-SP) for pregnant women. This program estimated the impact of IPTp-SP on
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
the malarial prevalence among women and newborn children, a study was planned for pregnant women who
consulted in the Bon samaritain hospital in NDja mena, Chad.
Methods: This 14 month study was conducted on 149 pregnant women. They were followed until delivery for
outcomes such as malaria attacks, anemia and placental malaria, low birth weight and prematurity in newborns.
Data was collected with the help of a pretested questionnaire. Data was analysed with SPSS and R studio, Odds
risk was calculated.
Results: The mean age of the study participants was 25.8 s 6.2 years with 72.5% under the age of 20 years,
and half were housewives with a secondary school education. More than half of the pregnant women (84,
56.3%) never used insecticide-treated mosquito nets. Among the 149 study participants, (64, 42,95%) received
3 doses of IPTp-SP, while 31( 20.8%) did not receive any dose of IPTp-SP. Only 30% (45) of the total 149
participants reported to be malaria positive; while 28.9% (43) were diagnosed with placental malaria. Of the
43 placenta malaria cases, 21(48.83%) had not received SP. Most of the lower birth weight babies with weight
< 2500g (40,81.64%) were reported in pregnant mothers who have reported administration of one or no dose
of SP. Out of 31 pregnant women, 21 (67.7%) without IPTp-SP had reported at least one attack of malaria
during their pregnancy compared to 22 women out of 118(18.7%) of those who had at least one dose of
Sulfamethoxazole pyrimethamine (p = 0.001 ). Out of 31 pregnant women who have not received IPTp-SP,
26 women (83.9%) reported anaemiaw ith Hb <10.5g/dl while 17 (65.4%) with severeanemia Hb <8g/dl .
Conclusion: The maternal rate of attack of malaria, placenta infestation, maternal anemia,and low birth weight
babies decrease considerably with administration of three or more doses of s ulfadoxine-pyrimethamine.
Keywords: Malaria, intermittent Preventive Treatment, Sulfadoxine-Pyriméthamine, Pregnancy, newborn,
developing nation, Chad.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
BACKGROUND
In 2019, approximately 33 countries in the World Health Organization (WHO) African Region with moderate
to high transmission of malaria, estimated that 35% of pregnant women were exposed to malaria infection and
822,000 children had low birthweight (LBW). By WHO estimates, the subregion of Central Africa had the
highest exposure to malaria during pregnancy (40%) closely followed by West Africa (39%) and East- Southern
Africa (24%) [1]. In sub-Saharan Africa, Plasmodium falciparum is reported to be the main infecting parasite,
responsible for 99% of all malaria in pregnancy [2]. Malaria during pregnancy is characterized by the
sequestration of infected erythrocytes in placental intervillous spaces binding Chondroitin sulphate-A resulting
in placental malaria [3, 4].
Malaria infection during pregnancy has substantial risks for the pregnant woman and the fetus. For the pregnant
woman, malaria infection can lead to placental sequestration of the parasite which can lead to maternal anaemia
with subsequent consequences [5, 6]. Malaria infection also puts the mother at increased risk of death before
and after childbirth, and is an important contributor to stillbirth and preterm birth. Placental malarial infection
can lead to poor fetal growth and LBW [7-9], and is a major risk factor for perinatal, neonatal and infant
mortality [10]. Some recent studies have shown that placental malaria was associated with maternal anemia
and LBW newborns[11], while the use of insecticide-treated net (ITN) and IPTp-SP reduced the odds of malaria
in pregnancy [12].
To stop the consequences of malaria infections, WHO recommends in combination with vector control, and
prompt diagnosis and effective treatment of malaria the use of IPTp with SP as part of antenatal care (ANC)
in areas of moderate to high transmission [13]. According to the Demographic and Health Survey and Multiple
Indicators in Chad (EDS-MICS), malaria is the leading cause of morbidity and mortality in Chad as well as for
outpatient consultation [14].
Malaria was reported to be the first indirect cause of maternal mortality (84.6%) and second cause of infant
mortality (25.57%) in 2010 [15]. In May 2005, during the National Malaria Management Policy Change
Workshop in Chad, it was decided that IPTp-SP should replace Chloroquine chemoprophylaxis [16]. In
accordance with the recommendations of WHO, sulfadoxine-pyrimethamine (SP) is administered with a
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
minimum of three doses, starting during the second trimester, and spaced at least 1 month apart [17]. Three or
more doses compared to the two doses previously recommended by WHO guidelines were shown to be more
effective in several meta-analyses [16]. After the implementation of the new WHO strategy in February 2014,
this study was planned to evaluate the outcome of use of IPTp-SP and ITN through compliance to ANC of
pregnant women at Bon Samaritain hospital of Chad. To reach this objective, we determined the modalities for
SP prescription, then identified the different factors that may influence the prescription and adherence to IPTp-
SP, and assess the results of this prevent ion.
METHODS
Aim, Study design, setting, and participants
This study, conducted over 14 months, from June 01, 2014 to July 31, 2015. It included all pregnant women
enrolled in the antenatal consultation performed by the two primary health care facilities of the hospital. The
two primary health care facilities are administratively linked to the the department of Obstetrics &
Gynaecology of Bon Samaritan hospital in NDjamena . ND jamena is the capital and largest city in Chad;
malaria is endemic to the city especially during the rainy season when there is a reported rise in mosquito
habitats [18]. The Obstetrics & Gynecology department of the hospital consisted of 7 wards with 27 hospital
beds, and performed an average of 700 deliveries per year. During the study period, a total of 861 pregnant
women were admitted. Among them, 149 fulfilled the inclusion criteria and consented to participate in the
study. Our preliminary study consisted of providing information on intermittent preventive treatment to
pregnant women.
Characteristicsof parti cipants
Inclusion criteria
Women with singleton pregnancies in their first or second trimester were recruited. These pregnant women
who agreed to participate in the study and planned to give birth at the Obstetrics & Gynaecology Unit of the
university medicalhos pital Bon Samaritain regardle ss of theterms of IPTp-SP administrat ion.
Exclusion criteria
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
Pregnant women who had a (i) history of allergy to sulfonamides, (ii) multiple gestations and (iii) high risk
pregnancies or complications such as hypertension, diabetes mellitus, antepartum haemorrhage or postpartum
bleeding, eclampsiaand other compl ications were excluded from thes tudy.
Study variables
Independent variables
Independent variables include the number of IPTp-SP doses administered and sociodemographic
characteristics including age, education level, and occupation of patient as well as clinical parameters included
parity, use of insecticide-treated mosquito nets, number of antenatal consultations and reasons for not taking
IPTp-SP in previous pregnancy.
Outcome details
Outcome variables included malaria attacks-related positivity on the blood smear, hemoglobin level anemia
and placental malaria. While for newborns, LBW and prematurity were considered for analysis.
Data collection techniquesand tools
Data was collected through a pretested questionnaire composed of four main parts: (i) sociodemographic and
obstetric information. (ii) antimalarial prophylaxis, (iii) blood test results and (iv) newborn information. Data
regarding ITNs usage, including usage of ITNs in previous pregnancies, the reason for noncompliance, use and
frequency of ITN, specifically SP, were collected during antenatal consultation. Well trained healthcare
workers informed the pregnant women about the study protocol and blood collection procedure for the
diagnosis of placental malaria. Birth weight was measured by the attending midwife for all births within 30
minutes of delivery, using an electronic scale accurate to s10 grams and calibrated weekly. Newborns were
classified as normal birth weight (2.5 kg) or LBW (<2.5 kg) according to WHO guidelines [19]. Health care
workers collected data from the treating team through face to face interviews. A pretested questionnaire was
done a month before the survey on a sample of 30 pregnant women that allowed us to amend our survey sheet.
Laboratory testing and materials
Blood from finger prick for malaria microscopy and to measure hemoglobin (Hb) level, placental blood
samples for malaria microscopy were collected at delivery. Placenta blood smears were obtained from the
intervillous space of the maternal side of the placenta. Blood smear for malaria was using 10% Giemsa stain,
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
with pH 7.2 and examined under 1. 100X objective lens oil immersion of a light microscope. Microscopic
examination of thick films was used to detect the presence of parasites under high power magnification. This
was conducted employing WHO guidelines [20]. Maternal hemoglobin concentrations were estimated with a
portable HemoCue device (Angelhom, Sweden). Anemia is defined as Hb < 10.5 g/dL and severe anaemia
with Hb < 8 g/dL [21].
Ethical consideration
The author has received authorization and approval from the university medical hospital team, the Medical
Director and the administration of the Bon Samaritain hospital to conduct this study. The study protocol and
details were explained, and approval was obtained. The purpose, details of the study and blood taking for
malaria and placental malaria were explained to participants. Face to face interviews were conducted for
answering questionnaires. Verbal consent for study participation, intravenous and placenta blood taking was
explained and taken. The research team has respected the principle of anonymity throughout the investigation.
Verbal consentw asobt ained from all participants regarding theinterview and bl ood collection.
Data analysis
The collected data were analyzed using SPSS V.20.0 (SPSS Inc., Ch icago, IL, USA) and RStudio IDE
(integr ated development environment) version 3.6.3 of 2020-02-29. A comparison of the occurrence of
morbid even ts in the two groups receivin g IPTp-SP was made with the help of the odds ratio. Differences
in proportions were analyzed by the chi- square 2 - test. P < 0.05 was considered significant. Parity was
catego rized as primip ara, Pauci-Parous (wom en with 2-5 births) and grand-m ultiparous (women with>5
birth s). For research purposes, women were diagnosed as malaria positive if parasites were detected by
light micro scopy with Giemsa staining in peripheral blood. The diagnosis of placental malaria was made
if the placental samples collected from the placenta were positive. Data about SP dosage intake was
grouped into no IPT -SP doses, one or two (<3) IPTp-SP doses and greater than or equal to three (3 )
IPTp-SP.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
RESULTS
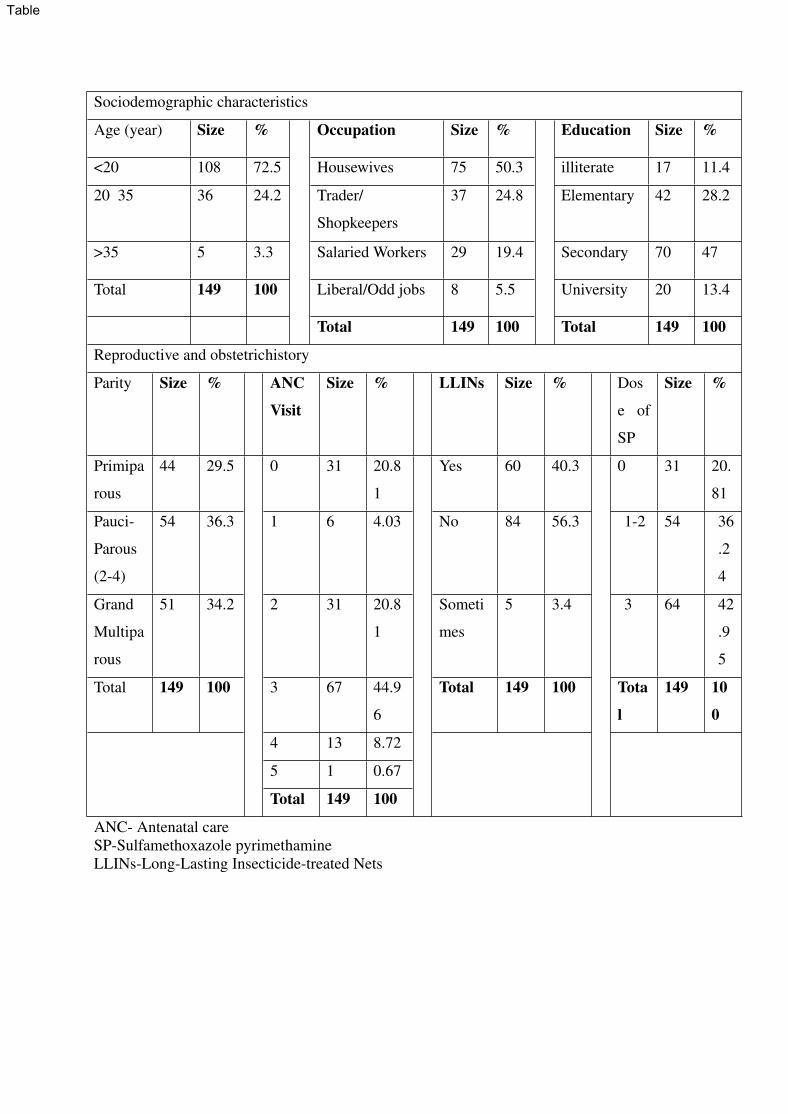
Sociodemographic Characteristics of Study Participants
Among 149 pregnant women, the average age was 25.8 s 6.2 years (table 1), with the majority under 20 years
(72.5%) followed by nearly one fourth (36, 24.2%) in the age group of 20-35 years. Furthermore, about half
(table 1) of the pregnant women had completed secondary school education (47.0%). Half (table 1) of study
participants reported to be housewives (75, 50.3%) followed by 24.8% (table 1) traders (37). Further
information about the sociodemographic characteristics is detailed in Table1.
Table 1: Sociodemographic characteristic and obstetric history
Reproductive and obstetric history of participants
Parity was divided into primiparous (women who are pregnant first time/have given birth to only one child),
pauci-parous (women with 2-5 birth/children) and grand-multiparous (women with >5 births/children). The
majority (table 1) of pregnant women in our study were pauci-parous (54, 36.3%) followed by grand
multiparous (51, 34.2%) (table 1). The majority of women attended three or more antenatal consultations
(81, 53.75%) (Table 1). However, 31(20.81%) (Table 1) pregnant women reported not attending any ANC
visit at all while remaining 188 (79.2%) (Table 1) reported at least one prenatal visit during their pregnancy.
Compliance to IPT-SP regimens
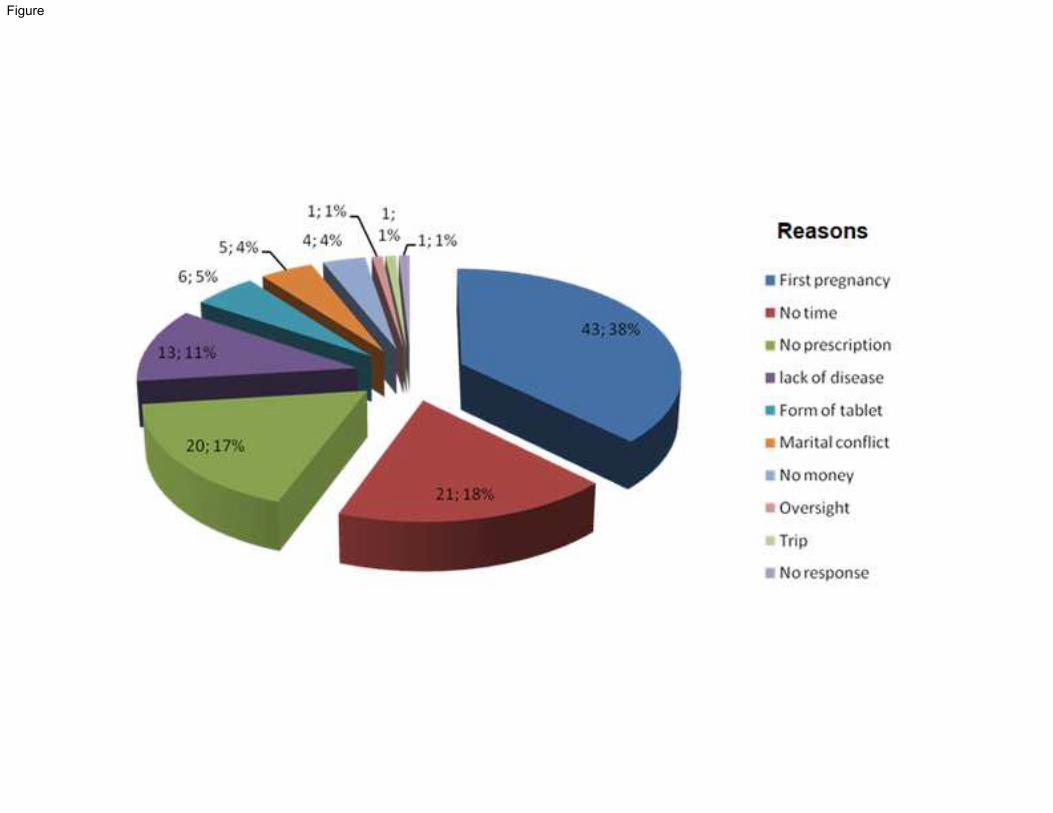
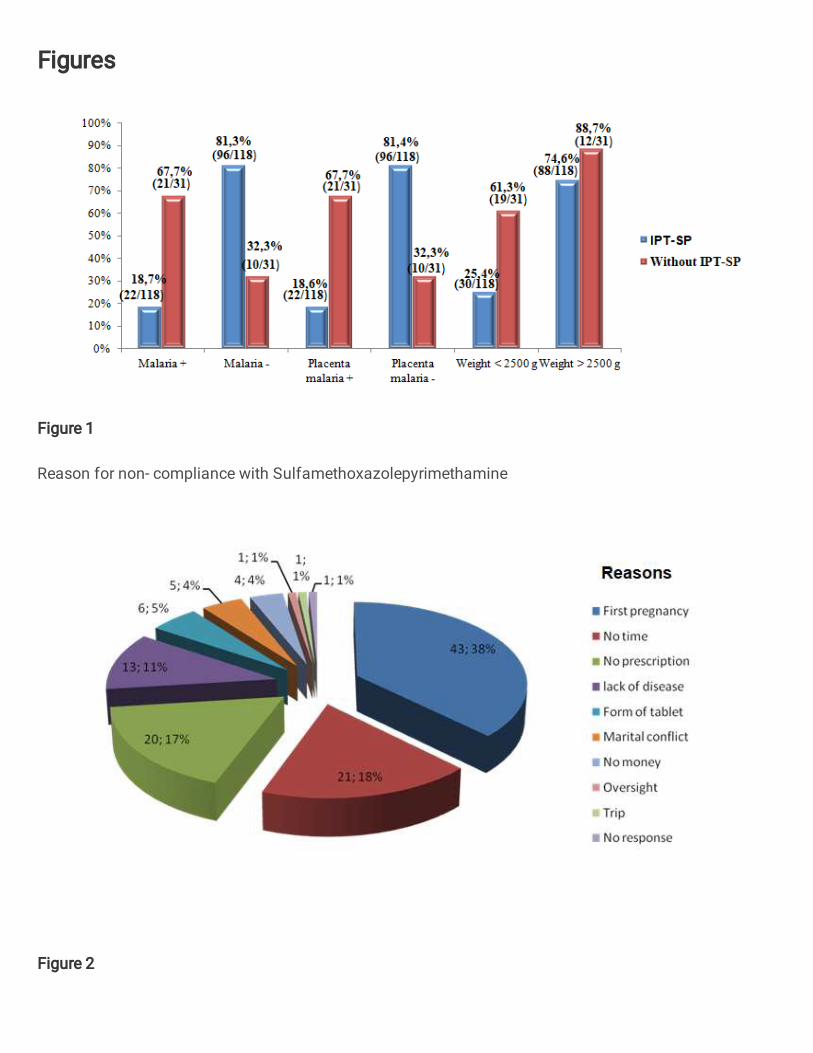
Three-fourth of pregnant women (115, 77.2%) (Figure 1) reported being non-compliant with IPTp-SP for
previous pregnancies. The most important reasons for the non-compliance to treatment quoted were (figure 1)
: the first pregnancy (43, 28.9%); no time(21,14%); no prescription (20,13.4%); lack of
disease(13,8.7%); form of tablet (6,5.2%); ma rital conflict (5,4.3%) and no money ( 4,2.3%). The rest
of the reasons (figure 1) were represented by oversight, tri p, and no response by each 1 participant
(0.9%).
Figure 1: Reason for non- compliance with Sulfamethoxazolepyrimethamine
Malaria Prevention regimens
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
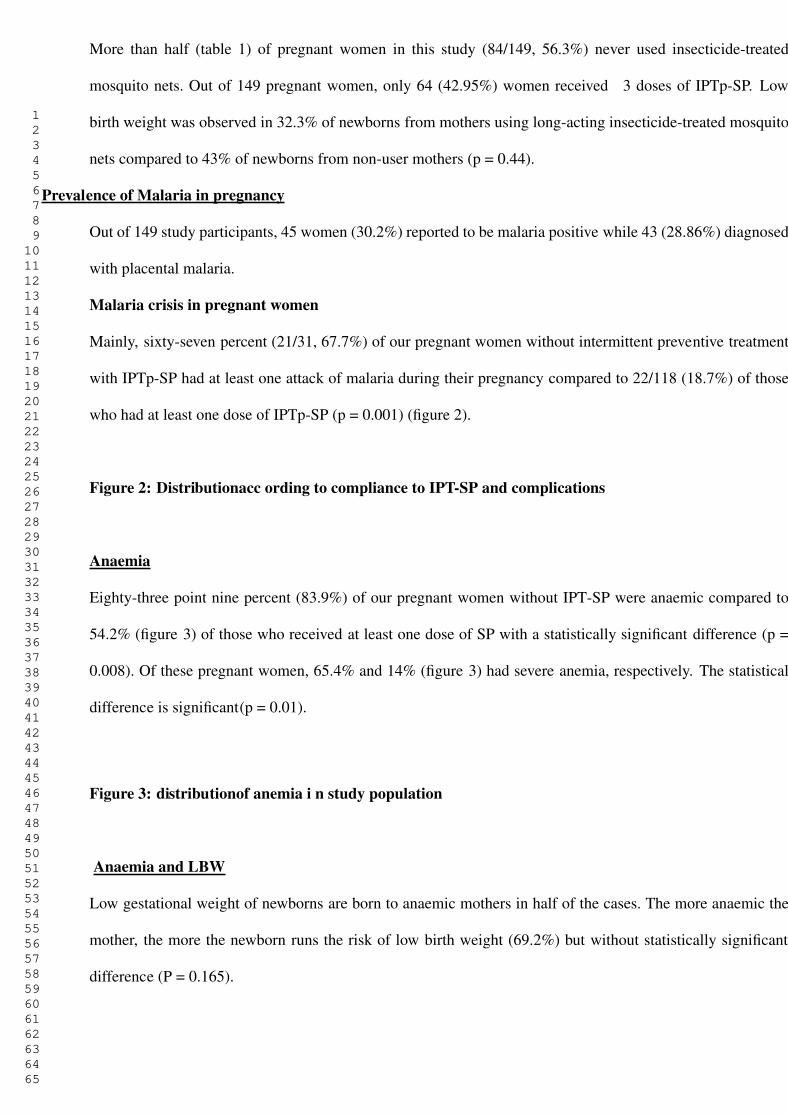
More than half (table 1) of pregnant women in this study (84/149, 56.3%) never used insecticide-treated
mosquito nets. Out of 149 pregnant women, only 64 (42.95%) women received 3 doses of IPTp-SP. Low
birth weight was observed in 32.3% of newborns from mothers using long-acting insecticide-treated mosquito
nets compared to 43% of newborns from non-user mothers (p = 0.44).
Prevalence of Malaria in pregnancy
Out of 149 study participants, 45 women (30.2%) reported to be malaria positive while 43 (28.86%) diagnosed
with placental malaria.
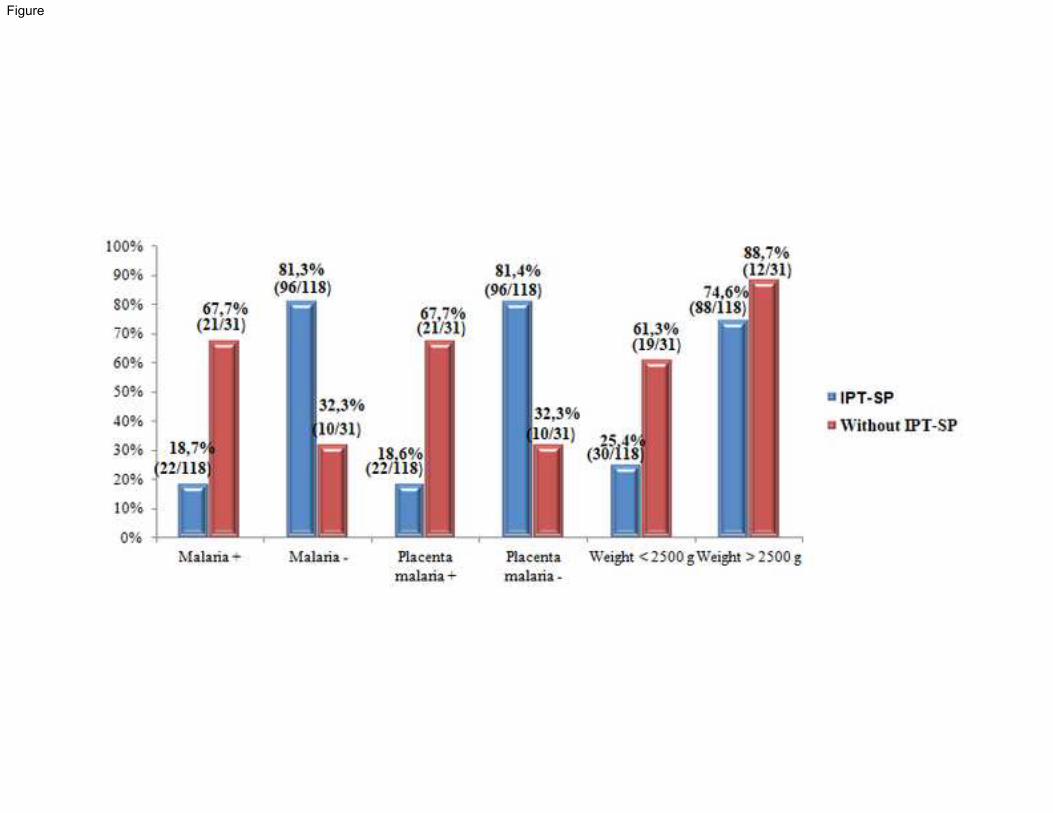
Malaria crisis in pregnant women
Mainly, sixty-seven percent (21/31, 67.7%) of our pregnant women without intermittent preventive treatment
with IPTp-SP had at least one attack of malaria during their pregnancy compared to 22/118 (18.7%) of those
who had at least one dose of IPTp-SP (p = 0.001) (figure 2).
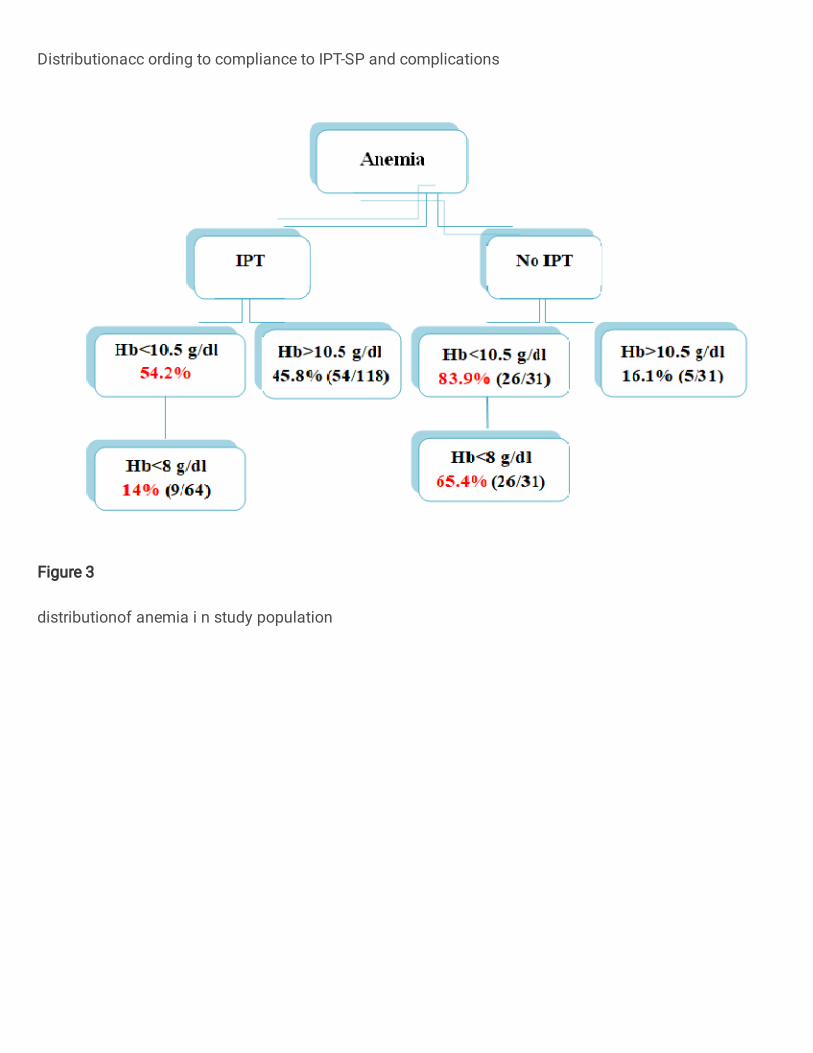
Figure 2: Distributionacc ording to compliance to IPT-SP and complications
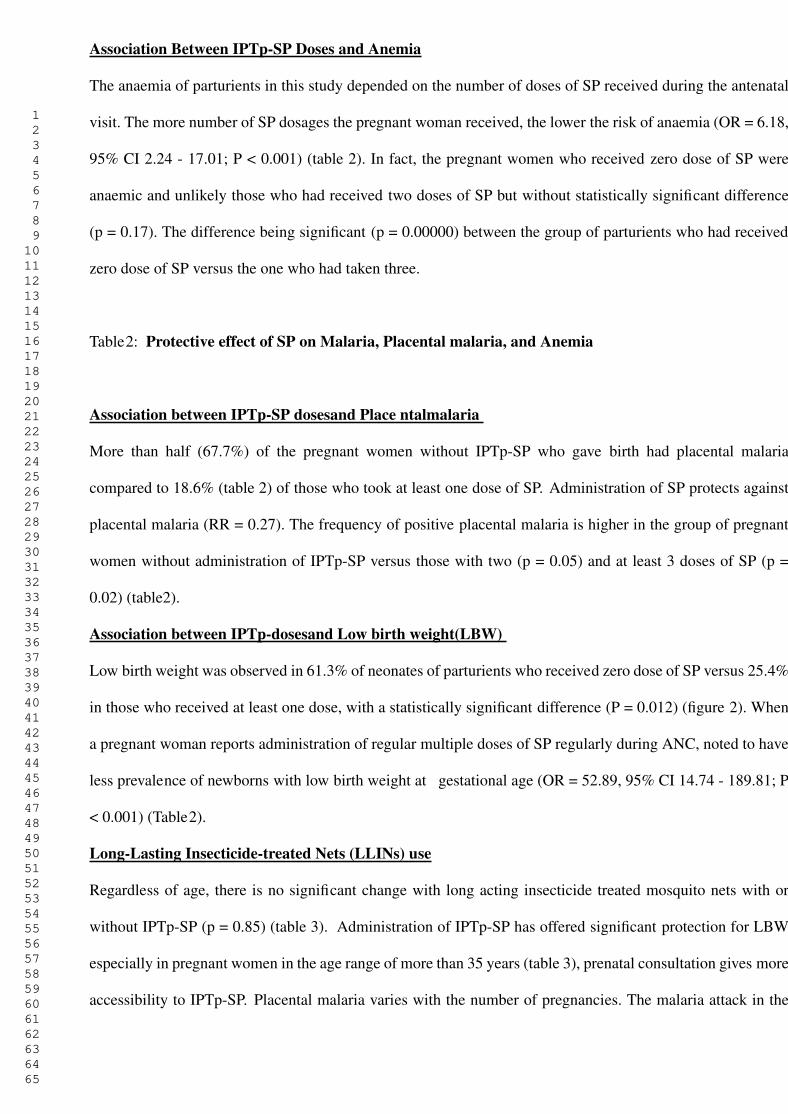
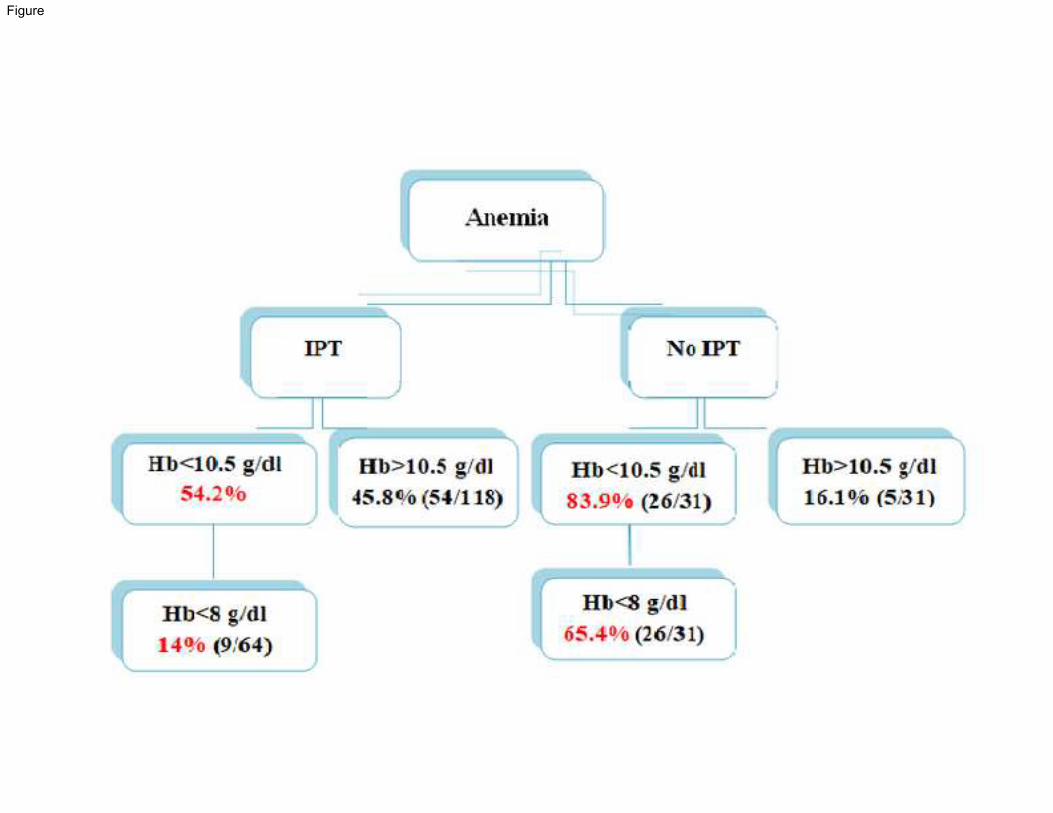
Anaemia
Eighty-three point nine percent (83.9%) of our pregnant women without IPT-SP were anaemic compared to
54.2% (figure 3) of those who received at least one dose of SP with a statistically significant difference (p =
0.008). Of these pregnant women, 65.4% and 14% (figure 3) had severe anemia, respectively. The statistical
difference is significant(p = 0.01).
Figure 3: distributionof anemia i n study population
Anaemia and LBW
Low gestational weight of newborns are born to anaemic mothers in half of the cases. The more anaemic the
mother, the more the newborn runs the risk of low birth weight (69.2%) but without statistically significant
difference (P = 0.165).
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
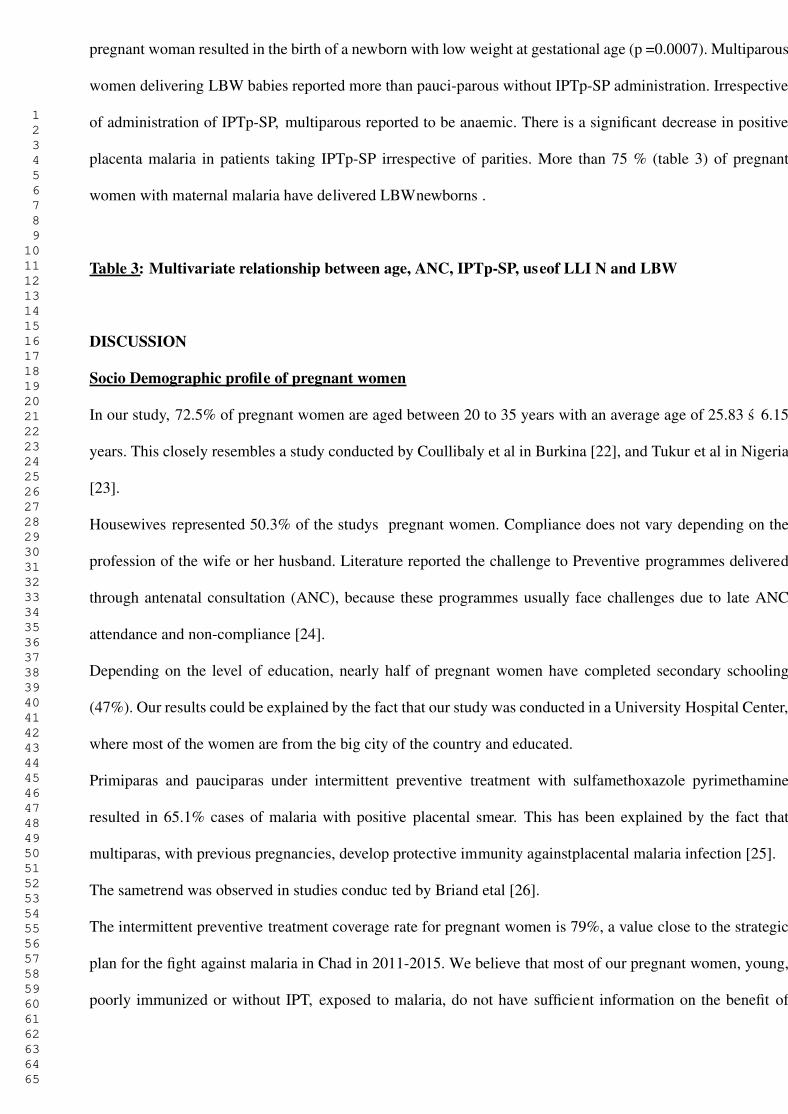
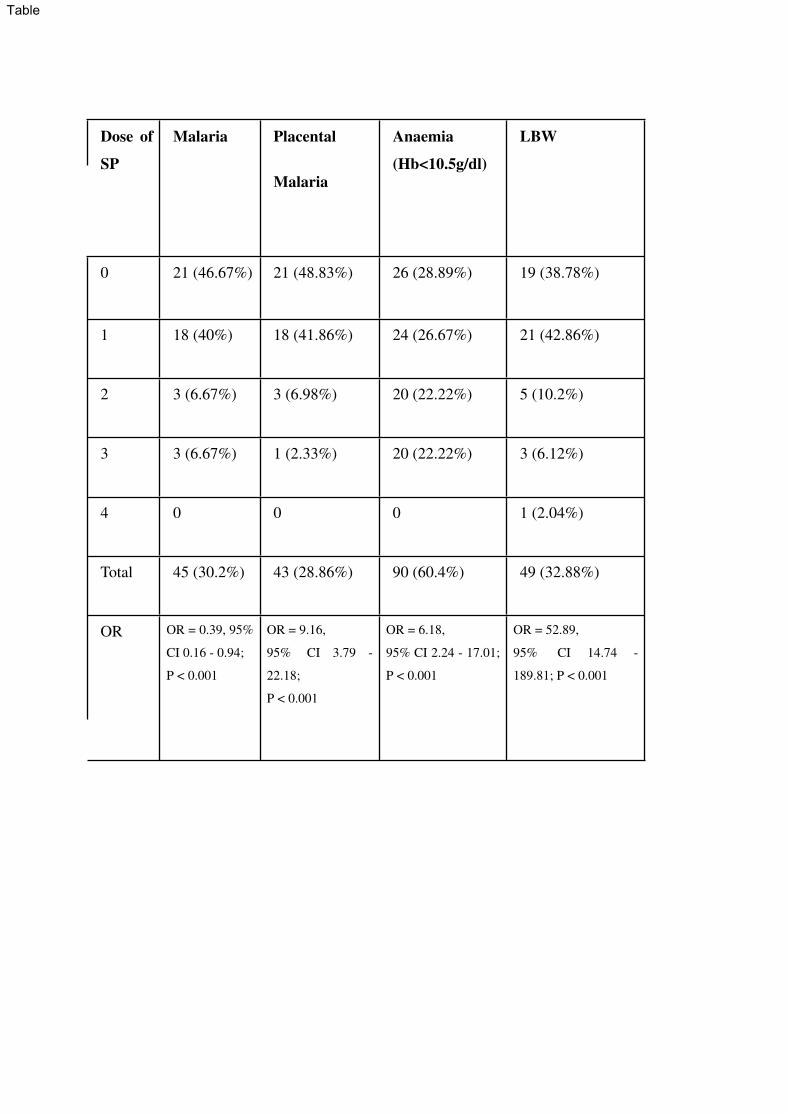
Association Between IPTp-SP Doses and Anemia
The anaemia of parturients in this study depended on the number of doses of SP received during the antenatal
visit. The more number of SP dosages the pregnant woman received, the lower the risk of anaemia (OR = 6.18,
95% CI 2.24 - 17.01; P < 0.001) (table 2). In fact, the pregnant women who received zero dose of SP were
anaemic and unlikely those who had received two doses of SP but without statistically significant difference
(p = 0.17). The difference being significant (p = 0.00000) between the group of parturients who had received
zero dose of SP versus the one who had taken three.
Table2: Protective effect of SP on Malaria, Placental malaria, and Anemia
Association between IPTp-SP dosesand Place ntalmalaria
More than half (67.7%) of the pregnant women without IPTp-SP who gave birth had placental malaria
compared to 18.6% (table 2) of those who took at least one dose of SP. Administration of SP protects against
placental malaria (RR = 0.27). The frequency of positive placental malaria is higher in the group of pregnant
women without administration of IPTp-SP versus those with two (p = 0.05) and at least 3 doses of SP (p =
0.02) (table2).
Association between IPTp-dosesand Low birth weight(LBW)
Low birth weight was observed in 61.3% of neonates of parturients who received zero dose of SP versus 25.4%
in those who received at least one dose, with a statistically significant difference (P = 0.012) (figure 2). When
a pregnant woman reports administration of regular multiple doses of SP regularly during ANC, noted to have
less prevalence of newborns with low birth weight at gestational age (OR = 52.89, 95% CI 14.74 - 189.81; P
< 0.001) (Table2).
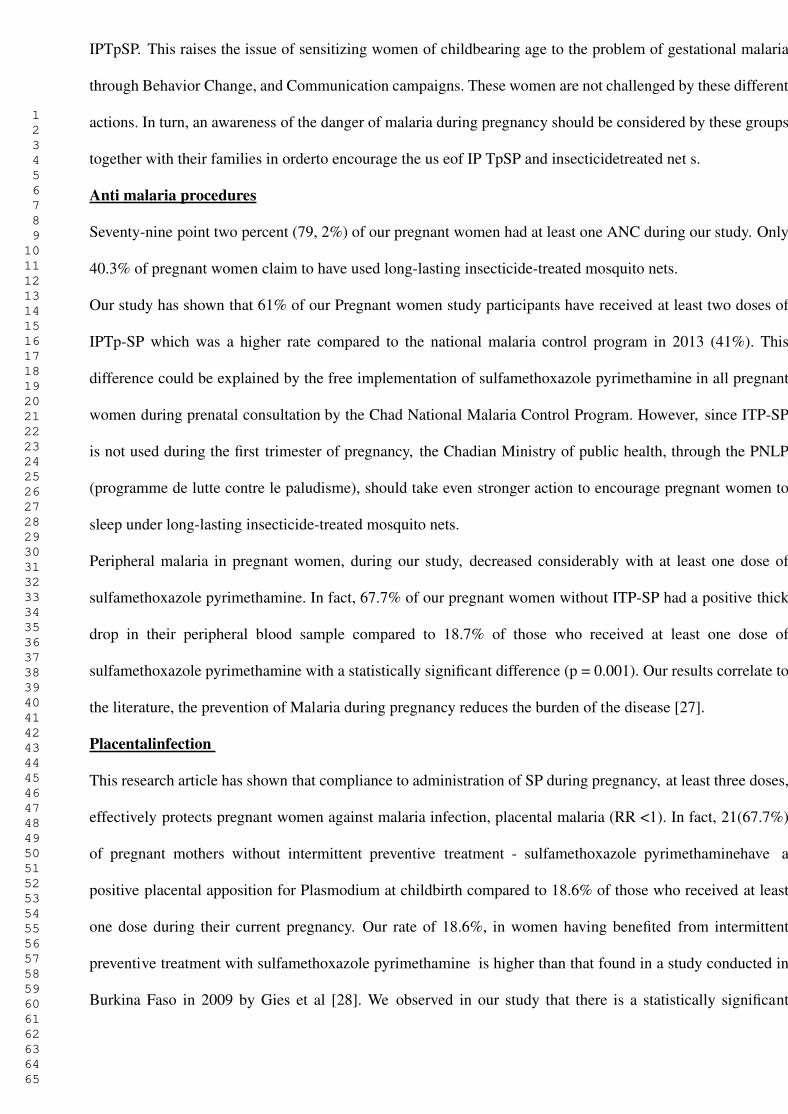
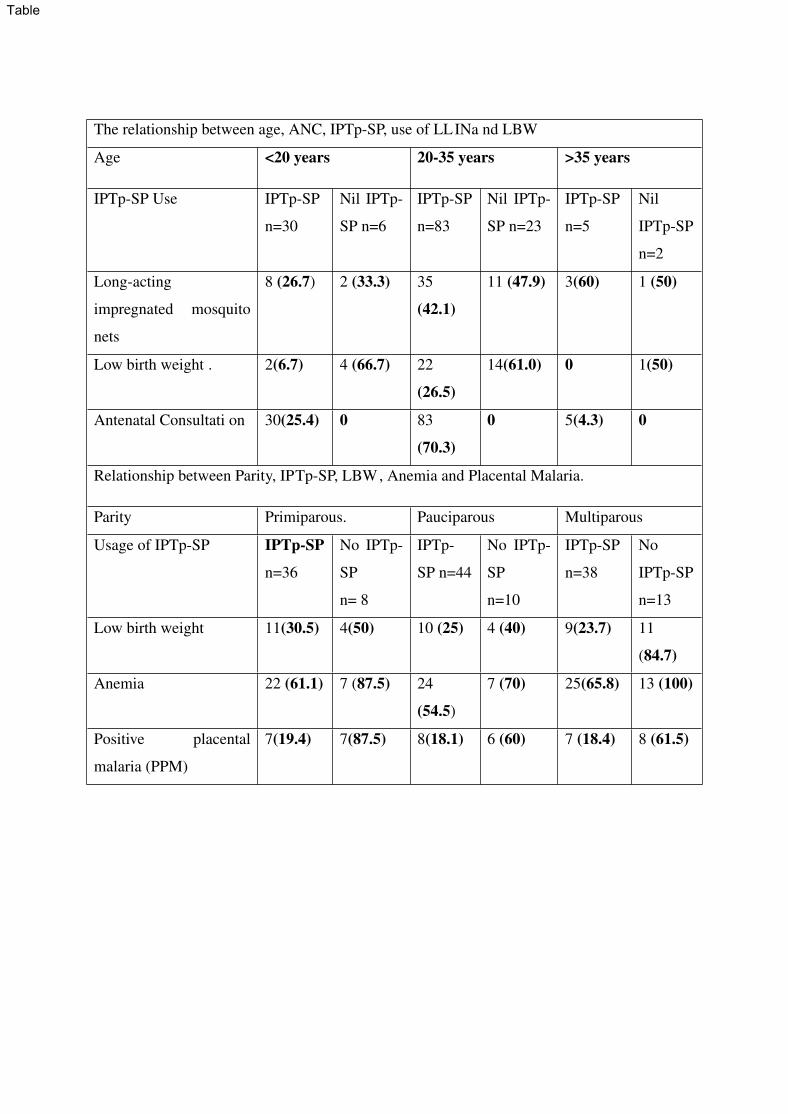
Long-Lasting Insecticide-treated Nets (LLINs) use
Regardless of age, there is no significant change with long acting insecticide treated mosquito nets with or
without IPTp-SP (p = 0.85) (table 3). Administration of IPTp-SP has offered significant protection for LBW
especially in pregnant women in the age range of more than 35 years (table 3), prenatal consultation gives more
accessibility to IPTp-SP. Placental malaria varies with the number of pregnancies. The malaria attack in the
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
pregnant woman resulted in the birth of a newborn with low weight at gestational age (p =0.0007). Multiparous
women delivering LBW babies reported more than pauci-parous without IPTp-SP administration. Irrespective
of administration of IPTp-SP, multiparous reported to be anaemic. There is a significant decrease in positive
placenta malaria in patients taking IPTp-SP irrespective of parities. More than 75 % (table 3) of pregnant
women with maternal malaria have delivered LBWnewborns .
Table 3: Multivariate relationship between age, ANC, IPTp-SP, useof LLI N and LBW
DISCUSSION
Socio Demographic profile of pregnant women
In our study, 72.5% of pregnant women are aged between 20 to 35 years with an average age of 25.83 s 6.15
years. This closely resembles a study conducted by Coullibaly et al in Burkina [22], and Tukur et al in Nigeria
[23].
Housewives represented 50.3% of the studys pregnant women. Compliance does not vary depending on the
profession of the wife or her husband. Literature reported the challenge to Preventive programmes delivered
through antenatal consultation (ANC), because these programmes usually face challenges due to late ANC
attendance and non-compliance [24].
Depending on the level of education, nearly half of pregnant women have completed secondary schooling
(47%). Our results could be explained by the fact that our study was conducted in a University Hospital Center,
where most of the women are from the big city of the country and educated.
Primiparas and pauciparas under intermittent preventive treatment with sulfamethoxazole pyrimethamine
resulted in 65.1% cases of malaria with positive placental smear. This has been explained by the fact that
multiparas, with previous pregnancies, develop protective immunity againstplacental malaria infection [25].
The sametrend was observed in studies conduc ted by Briand etal [26].
The intermittent preventive treatment coverage rate for pregnant women is 79%, a value close to the strategic
plan for the fight against malaria in Chad in 2011-2015. We believe that most of our pregnant women, young,
poorly immunized or without IPT, exposed to malaria, do not have sufficient information on the benefit of
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
IPTpSP. This raises the issue of sensitizing women of childbearing age to the problem of gestational malaria
through Behavior Change, and Communication campaigns. These women are not challenged by these different
actions. In turn, an awareness of the danger of malaria during pregnancy should be considered by these groups
together with their families in orderto encourage the us eof IP TpSP and insecticidetreated net s.
Anti malaria procedures
Seventy-nine point two percent (79, 2%) of our pregnant women had at least one ANC during our study. Only
40.3% of pregnant women claim to have used long-lasting insecticide-treated mosquito nets.
Our study has shown that 61% of our Pregnant women study participants have received at least two doses of
IPTp-SP which was a higher rate compared to the national malaria control program in 2013 (41%). This
difference could be explained by the free implementation of sulfamethoxazole pyrimethamine in all pregnant
women during prenatal consultation by the Chad National Malaria Control Program. However, since ITP-SP
is not used during the first trimester of pregnancy, the Chadian Ministry of public health, through the PNLP
(programme de lutte contre le paludisme), should take even stronger action to encourage pregnant women to
sleep under long-lasting insecticide-treated mosquito nets.
Peripheral malaria in pregnant women, during our study, decreased considerably with at least one dose of
sulfamethoxazole pyrimethamine. In fact, 67.7% of our pregnant women without ITP-SP had a positive thick
drop in their peripheral blood sample compared to 18.7% of those who received at least one dose of
sulfamethoxazole pyrimethamine with a statistically significant difference (p = 0.001). Our results correlate to
the literature, the prevention of Malaria during pregnancy reduces the burden of the disease [27].
Placentalinfection
This research article has shown that compliance to administration of SP during pregnancy, at least three doses,
effectively protects pregnant women against malaria infection, placental malaria (RR <1). In fact, 21(67.7%)
of pregnant mothers without intermittent preventive treatment - sulfamethoxazole pyrimethaminehave a
positive placental apposition for Plasmodium at childbirth compared to 18.6% of those who received at least
one dose during their current pregnancy. Our rate of 18.6%, in women having benefited from intermittent
preventive treatment with sulfamethoxazole pyrimethamine is higher than that found in a study conducted in
Burkina Faso in 2009 by Gies et al [28]. We observed in our study that there is a statistically significant
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
difference between pregnant women who received at least three doses of sulfamethoxazole pyrimethamine and
those who received no dose (p = 0.002). This shows that sulfamethoxazole pyrimethamine intermittent therapy
with three doses or more is effective. This therapy can be used as a practical strategy for reducing the risk of
placental infection with plasmodium in areas of endemic malaria.
Other preventive measures such as the use of long-lasting insecticide-treated mosquito nets and Environmental
control measures for control of mosquitoes might further help to reduce the burden of malaria in pregnant
women.
Moreover, in the present study, first-time mothers under intermittent preventive treatment with
sulfamethoxazole pyrimethamine remained the most vulnerable to malaria with 19.4% against 18.4% in
multipara. The difference is not statistically significant (P = 0.96). A relatively small sample size of the
population could explain this non-significant difference. In the literature, it has been shown that multiparous,
with previous pregnancies, develop protective immunity againstplacenta l malaria infection[ 25].
Appropriate evaluation of prevention strategies for malaria and placental infection during pregnancy is directly
linked to prevention of complication among newborns. Therefore, it would be necessary to develop strategies
for close monitoring for better adherence to intermittent preventive treatment with sulfadoxine- pyrimethamine
during the transmission season considering the high risk of transmission.
Low Birth weight
Low birth weight is a powerful predictor of children’s and maternal health, defined as less than 2500g [29].
Our study has reported a statistically significant protective effect of administration of IPTp-SP against LBW
(P=0.012) which is consistent with previously published literature [30]. This result reinforces current WHO
recommendations that the administration of sulfamethoxazole pyrimethamine with intermittent preventive
treatment shall beencouraged in Africa from two to three or m ore doses [13].
Our study has reported 32.8% (49/149) low birth weight newborns (P = 0.012). Specifically, this rate is 25.4%
in newborns whose mothers used IPT with SP during pregnancy versus 61.3% of mothers who did not use IPT.
Our study results are superior to those found by Borgella et al. in 2013 [31]. Literature has reported that
beneficial effect with three or more doses of sulfamethoxazole pyrimethamine during pregnancy protects
against the occurrenceof low birth weight [32].
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
Anaemia
Our study has reported 60.4% anemia cases in pregnant women. Our study has reported 83% of anemia in
pregnant women without ITP-SP compliance compared to 54.2% of anemia in pregnant women on ITP-SP (P=
0.008). Severe anaemia observed in pregnant women without administration of IPT (65.4%) while
administration of IPT reported to offer protection against anaemia (p=0.01). Our results are slightly inferior to
the study conducted by Omer et al in 2017 that found 67.7% in pregnant women and 22 of them (3%) had
severe anaemia (Hb < 7 g/dL) [11]. Although anemia in pregnant women is multi-factorial [33] malaria
infection has worsened anemiain pregnant women.
Limitations of the study
Our study has some limitations, the first one being small sample size. This study has considered outcome in
newborns, in future studies, we shall plan to evaluate long term effects on growth of children from mothers
with positive malariatests during pregnancy wit h and without IPTp-SP.
CONCLUSION
The study found that in pregnant women who took at least 3 doses of Sulphadoxine Pyrimethamine, there was
less placenta malaria and the women were more protected from malaria. Unfortunately a large number of
women didnt take the required dosage of Sulphadoxine Pyrimethamine. The malaria in pregnancy has resulted
in maternal anemia and low birth weight of newborn. Theefforts of sensibil isation need to be donein order t o
increase the compliance of pregnant women with the preventive programs through the antenatal consultation
for decreasing the maternal and newborn related malaria complication.
Ethics declarations
The author has received authorization and approval from the university medical hospital team, the Medical
Director and the administration of the Bon Samaritain hospital to conduct this study. The study protocol and
details were explained, and approval was obtained. The purpose, details of the study and blood taking for
malaria and placental malaria were explained to participants. Face to face interviews were conducted for
answering questionnaires. Verbal consent for study participation, intravenous and placenta blood taking was
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
explained and taken. The research team has respected the principle of anonymity throughout the investigation.
Verbal consentw asobt ained from all participants regarding theinterview and bl ood collection.
Consentfor pu blication
Not applicable
Competing interests
The authorsde clare that they have no competing interests.
Funding
Not applicable
Authors c ontributions
OA, and NNN designed the study and participated in the manuscript drafting. OA was responsible for patient
recruitment, clinical and laboratory examinations. OA, NNN, NH, MKRS, KMLP, ZD and ABC conducted
datainterpretat ion and statistical analyses. All authors read and approve d the final manuscript.
Acknowledgements
We are very grateful to the women who participated in the study. We also thank the midwives and health
administration staff at the study sites. Thanks are also extended to Betsaleel Gui-louvia who helped in Statistical
analysis.
Availabili tyof supporting data
All datarelated t o the present study areavailabl e.
Abbreviations
ANC : antenatal consultation
EDS-MICS: Demographic and Health Survey and Multiple Indicators in Chad
IPTp-SP: intermittent preventive treatment with sulfamethoxazole-pyrimethamine
ITN : Insecticide-treated net
LBW : Low birth weight
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
LLIN : Long-lasting insecticide-treated net
PNLP: Programme National de lutte contre le paludisme
SP: Sulfamethoxazole pyrime thamine
WHO : world health organization
REFERENCES
1. World malaria report 2020: 20 years of global progress and challenges [Internet]. Who.int. 2021 [cited 16
March 2021]. Available from: https://www.who.int/docs/default-source/malaria/world-malaria-
reports/9789240015791-eng.pdf?sfvrsn=d7a8ec53_3&download=true
2. World Malaria Report 2017 - World [Internet]. ReliefWeb. 2017 [cited 10 March 2021]. Available from:
https://reliefweb.int/report/world/world-malaria-report-2017
3. Beeson J, Amin N, Kanjala M, Rogerson S. Selective Accumulation of Mature Asexual Stages of
Plasmodium falciparum-Infected Erythrocytes in the Placenta. Infection and Immunity. 2002;70(10):5412-
5415.
4. Muthusamy A, Achur R, Bhavanandan V, Fouda G, Taylor D, Gowda D. Plasmodium falciparum-Infected
Erythrocytes Adhere Both in the Intervillous Space and on the Villous Surface of Human Placenta by Binding
to the Low-Sulfated Chondroitin Sulfate Proteoglycan Receptor. The American Journal of Pathology.
2004;164(6):2013-2025.
5. TAKO E, LOHOUE J, LEKE R, LEKE R, ZHOU A, TAYLOR D. RISK FACTORS FOR PLACENTAL
MALARIA AND ITS EFFECT ON PREGNANCY OUTCOME IN YAOU NDE, CAMEROON. The
American Journal of TropicalM edicine and Hygiene. 2005;72(3):236-242.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
6. Menendez C, Fleming A, Alonso P. Malaria-related Anaemia.P arasitology Today. 2000;16(11):469-476.
7. De Beaudrap P, Turyakira E, White L, Nabasumba C, Tumwebaze B, Muehlenbachs A et al. Impact of
malaria during pregnancy on pregnancy outcomes in a Ugandan prospective cohort with intensive malaria
screening and prompt treatment. MalariaJournal. 2013;12(1).
8. Guyatt H, Snow R. Impact of Malaria during Pregnancy on Low Birth Weight in Sub-Saharan Africa.
Clinical Microbiology Reviews. 2004;17(4):760-769.
9. Walker P, ter Kuile F, Garske T, Menendez C, Ghani A. Estimated risk of placental infection and low
birthweight attributable to Plasmodium falciparum malaria in Africa in 2010: a modelling study. The Lancet
Global Health. 2014;2(8):e460-e467.
10. VAN GEERTRUYDEN J, ERHART A, DALESSANDRO U, THOMAS F. THE CONTRIBUTION OF
MALARIA IN PREGNANCY TO PERINATAL MORTALITY. The American Journal of Tropical Medicine
and Hygiene. 2004;71(2_suppl):35-40.
11. Omer S, Idress H, Adam I, Abdelrahim M, Noureldein A, Abdelrazig A et al. Placental malaria and its
effecton pregnancy outcome s in Sudanese women from BlueN ile State. Malaria Journal. 2017;16(1).
12. Agyeman Y, Newton S, Annor R, Owusu-Dabo E. The Effectiveness of the Revised Intermittent Preventive
Treatment with Sulfadoxine Pyrimethamine (IPTp-SP) in the Prevention of Malaria among Pregnant Women
in Northern Ghana.J ournalof Tropical M edicine. 2020;2020:1-9.
13. WHO policy brief for the implementation of intermittent preventive treatment of malaria in pregnancy
using sulfadoxine-pyrimethamine (IPTp-SP) [Internet]. World Health Organization. 2014 [cited 10 March
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
2021]. Available from:
https://www.who.int/malaria/publications/atoz/policy_brief_iptp_sp_policy_recommendation/en/
14. Enquête Démographique et de Santé et à Indicateurs Multiples au Tchad (EDS-MICS) 2014-2015
[Internet]. Dhsprogram.com. 2015 [cited 10 March 2021]. Available from:
https://www.dhsprogram.com/pubs/pdf/FR317/FR317.pdf
15. Programme National de Lutte contre le Paludisme. Rapport annuel sur le paludisme 2010. NDjaména,
Tchad ; IDT: 2011.
16. A strategic framework for malaria prevention and control during pregnancy in the African region (archived)
[Internet]. World Health Organization. 2004 [cited 12 March 2021]. Available from:
https://www.who.int/malaria/publications/atoz/afr_mal_04_01/en/
17. WHO | Updated WHO policy recommendation: intermittent preventive treatment of malaria in pregnancy
using sulfadoxine-pyrimethamine (IPTp-SP) [Internet]. Who.int. 2012 [cited 20 March 2021]. Available from:
https://www.who.int/malaria/publications/atoz/who_iptp_sp_policy_recommendation/en/
18. WHO | World MalariaReport 2013 [Internet ]. Who.int. 2013 [cited 18 March 2021]. Available from:
https://www.who.int/malaria/publications/world_malaria_report_2013/en/
19. Yilgwan C, Abok I, Yinnang W, Vajime B. Prevalence and risk factors of low birth weight in Jos. Jos
Journal of Medicine. 2010;4(1).
20. Moody A. Rapid Diagnostic Tests for Malaria Parasites. Clinical Microbiology Reviews. 2002;15(1):66-
78.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
21. WHO | Basic malaria microscopy Part II: Tutor’s guide. Second edition [Internet]. Who.int. 2010 [cited
26 March 2021]. Available from: https://www.who.int/malaria/publications/atoz/924154791X/en/
22. Coulibaly S, Gies S, DAle ssandro U. Malaria Burden among Pregnant Women Living in the Rural District
of Boromo, Burkina Faso [Internet]. Ncbi.nlm.nih.gov. 2007 [cited 16 March 2021]. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK1709/
23. TUKUR I, MADAKI J, SAGAY A, THACHER T. A COMPARISON OF SULFADOXINE-
PYRIMETHAMINE WITH CHLOROQUINE AND PYRIMETHAMINE FOR PREVENTION OF
MALARIA IN PREGNANT NIGERIAN WOMEN. The American Journal of Tropical Medicine and Hygiene.
2007;76(6):1019-1023.
24. Crawley J, Hill J, Yartey J, Robalo M, Serufilira A, Ba-Nguz A et al. From evidence to action? Challenges
to policy change and programme delivery for malaria in pregnancy. The Lancet Infectious Diseases.
2007;7(2):145-155.
25. Fievet N, Tami G, Maubert B, Moussa M, Shaw I, Cot M et al. Journal search results - Cite This For Me.
MalariaJour nal. 2002;1(1):16.
26. Briand V, Denoeud L, Massougbodji A, Cot M. Efficacy of Intermittent Preventive Treatment versus
Chloroquine Prophylaxis to Prevent Malaria during Pregnancy in Benin. The Journal of Infectious Diseases.
2008;198(4):594-601.
27. Feng G, Simpson J, Chaluluka E, Molyneux M, Rogerson S. Decreasing Burden of Malaria in Pregnancy
in Malawian Women and Its Relationship to Use of Intermittent Preventive Therapy or Bed Nets. PLoS ONE.
2010;5(8):e12012.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
28. Gies S, Coulibaly S, Ouattara F, DA lessandro U. Individual efficacy of intermittent preventive treatment
with sulfadoxine-pyrimethamine in primi- and secundigravida in rural Burkina Faso: impact on parasitaemia,
anaemia and birth weight. TropicalM edicine & InternationalH ealth. 2009;14(2):174-182.
29. Hughes M, Black R, Katz J. 2500-g Low Birth Weight Cutoff: History and Implications for Future Research
and Policy.Mat ernal and Child Health Journal. 2016;21(2):283-289.
30. Eisele T, Larsen D, Anglewicz P, Keating J, Yukich J, Bennett A et al. Malaria prevention in pregnancy,
birthweight, and neonatal mortality: a meta-analysis of 32 national cross-sectional datasets in Africa. The
Lancet Infectious Diseases. 2012;12(12):942-949.
31. Huynh B, Fievet N, Briand V, Borgella S, Massougbodji A, Deloron P et al. Consequences of Gestational
Malaria on Birth Weight: Finding the Best Timeframe for Intermittent Preventive Treatment Administration.
PLoS ONE. 2012;7(4):e35342.
32. Kayentao K, Garner P, Maria van Eijk A, Naidoo I, Roper C, Mulokozi A et al. Intermittent Preventive
Therapy for Malaria During Pregnancy Using 2 vs 3 or More Doses of Sulfadoxine-Pyrimethamine and Risk
of Low Birth Weight in Africa. JAMA. 2013;309(6):594.
33. Antelman G, Msamanga G, Spiegelman D, Urassa E, Narh R, Hunter D et al. Nutritional Factors and
Infectious Disease Contribute to Anemia among Pregnant Women with Human Immunodeficiency Virus in
Tanzania. The Journal of Nutrition. 2000;130(8):1950-1957.
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
Sociodemographic characteristics
Age (year) Size % Occupation Size % Education Size %
<20 108 72.5 Housewives 75 50.3 illiterate 17 11.4
20 35 36 24.2 Trader/
Shopkeepers
37 24.8 Elementary 42 28.2
>35 5 3.3 Salaried Workers 29 19.4 Secondary 70 47
Total 149 100 Liberal/Odd jobs 8 5.5 University 20 13.4
Total 149 100 Total 149 100
Reproductive and obstetrichistory
Parity Size % ANC
Visit
Size % LLINs Size % Dos
e of
SP
Size %
Primipa
rous
44 29.5 0 31 20.8
1
Yes 60 40.3 0 31 20.
81
Pauci-
Parous
(2-4)
54 36.3 1 6 4.03 No 84 56.3 1-2 54 36
.2
4
Grand
Multipa
rous
51 34.2 2 31 20.8
1
Someti
mes
5 3.4 3 64 42
.9
5
Total 149 100 3 67 44.9
6
Total 149 100 Tota
l
149 10
0
4 13 8.72
5 1 0.67
Total 149 100
ANC- Antenatal care
SP-Sulfamethoxazole pyrimethamine
LLINs-Long-Lasting Insecticide-treated Nets
Table
Placental LBW
Malaria
Dose of
SP
Malaria Anaemia
(Hb<10.5g/dl)
0 21 (46.67%) 21 (48.83%) 26 (28.89%) 19 (38.78%)
1 18 (40%) 18 (41.86%) 24 (26.67%) 21 (42.86%)
2 3 (6.67%) 3 (6.98%) 20 (22.22%) 5 (10.2%)
3 3 (6.67%) 1 (2.33%) 20 (22.22%) 3 (6.12%)
4 0 0 0 1 (2.04%)
Total 45 (30.2%) 43 (28.86%) 90 (60.4%) 49 (32.88%)
OR = 0.39, 95%
CI 0.16 - 0.94;
P < 0.001
OR = 9.16,
95% CI 3.79 -
22.18;
P < 0.001
OR = 6.18,
95% CI 2.24 - 17.01;
P < 0.001
OR = 52.89,
95% CI 14.74 -
189.81; P < 0.001
OR
Table
The relationship between age, ANC, IPTp-SP, use of LLINa nd LBW
Age <20 years 20-35 years >35 years
IPTp-SP Use IPTp-SP
n=30
Nil IPTp-
SP n=6
IPTp-SP
n=83
Nil IPTp-
SP n=23
IPTp-SP
n=5
Nil
IPTp-SP
n=2
Long-acting
impregnated mosquito
nets
8 (26.7) 2 (33.3) 35
(42.1)
11 (47.9) 3(60) 1 (50)
Low birth weight . 2(6.7) 4 (66.7) 22
(26.5)
14(61.0) 0 1(50)
Antenatal Consultati on 30(25.4) 0 83
(70.3)
0 5(4.3) 0
Relationship between Parity, IPTp-SP, LBW, Anemia and Placental Malaria.
Parity Primiparous. Pauciparous Multiparous
Usage of IPTp-SP IPTp-SP
n=36
No IPTp-
SP
n= 8
IPTp-
SP n=44
No IPTp-
SP
n=10
IPTp-SP
n=38
No
IPTp-SP
n=13
Low birth weight 11(30.5) 4(50) 10 (25) 4 (40) 9(23.7) 11
(84.7)
Anemia 22 (61.1) 7 (87.5) 24
(54.5)
7 (70) 25(65.8) 13 (100)
Positive placental
malaria (PPM)
7(19.4) 7(87.5) 8(18.1) 6 (60) 7 (18.4) 8 (61.5)
Table
Figure
Figure
Figure
Figures
Figure 1
Reason for non- compliance with Sulfamethoxazolepyrimethamine
Figure 2
Distributionacc ording to compliance to IPT-SP and complications
Figure 3
distributionof anemia i n study population





























