Embed Size (px)
Citation preview
Document of The World Bank
Report No: ICR2042
IMPLEMENTATION COMPLETION AND RESULTS REPORT (IDA-H2290)
ON A
GRANT
IN THE AMOUNT OF SDR 21.6 MILLION (US$31 MILLION EQUIVALENT)
TO THE
REPUBLIC OF BENIN
FOR A
MALARIA CONTROL SUPPORT PROJECT
December 29, 2011
Africa Technical Health Country Department Africa Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
ii
CURRENCY EQUIVALENTS (Exchange Rate Effective: 11/18/2011)
Currency Unit = CFAF (XOF)
CFAF 1.00 = US$0.0021 US$1.00 = CFAF 485
FISCAL YEAR
January 1 – December 31
ABBREVIATIONS AND ACRONYMS
ACT Artemisinin-based combination therapy ANC Antenatal care BCC Behavior change communication CAME Centrale d’Achat des Medicaments Essentiels et Consommables Medicaux
CAS Country Assistance Strategy CDC United States Centres for Disease Control CPMP Cellule de Passation des Marches Publics
DDS Direction Departementale de la Sante
DGA Development Grant Agreement DHS Demographic and Health Survey DNPS Direction Nationale de la Protection Sanitaire
DPP Direction de la Programmation et de la Prospective
GFATM Global Fund for AIDS, TB and Malaria GoB Government of Benin ICR Implementation Completion Report IEC Information, education and communication IPTp Intermittent preventive treatment for pregnant women IRS Indoor residual spraying ISR Implementation Status Report ITN Insecticide-treated net LLIN Long-lasting insecticide-treated net LQAS Lot Quality Assurance Sampling Method M&E Monitoring and evaluation MDG Millennium Development Goal MERG RBM’s Monitoring and Evaluation Research Group MIRT World Bank’s Malaria Implementation Resource Team MIS Malaria Indicator Survey MoEF Ministry of Economy and Finance MoH Ministry of Health MSH Management Sciences for Health MTR Mid-term review NGO Non-governmental organization NSP National Strategic Plan NTB National Tender Board OPCS World Bank’s Operations Policy and Country Services Vice Presidency PAD Project Appraisal Document PADS Projet d’Appui au Developpement du Systeme Sanitaire
PITA Plan integer de travail annuel (Annual Integrated Work Plan) PIU Project Implementation Unit PMI President’s Malaria Initiative (USAID)
iii
PNDS GoB’s National Health Sector Development Plan (2009-2018) PNLP Programme National de Lutte contre le Paludisme
PRSC Poverty Reduction Strategy Credit QALP World Bank’s Quality Assessment of Lending Portfolio RBM Roll Back Malaria RDT Rapid diagnostic test SIGFiP Systeme Integre de Gestion des Finances Publiques
SIGL MoH’s Information System for Logistics Management SIRP Systeme d’Information de Routine du Paludisme
SNIGS Systeme National d’Information et de Gestion Sanitaires
SP Sulfadoxine/pyrimethamine TTL Task team leader UNICEF United Nations Children’s Fund USAID United States Agency for International Development WHO World Health Organization
Vice President: Obiageli K. Ezekwesili Country Director: Madani Tall Sector Manager: Jean-Jacques de St. Antoine
Project Team Leader: Ayite-Fily d’Almeida ICR Team Leader: Denise Vaillancourt
iv
BENIN
Malaria Control Support Project
CONTENTS
Data Sheet A. Basic Information i B. Key Dates i C. Ratings Summary…………………………………………………………………………..i D. Sector and Theme Codes…………………………………………………………………..ii E. Bank Staff………………………………………………………………………………….ii F. Results Framework Analysis……………………………………………………………….ii G. Ratings of Project Performance in ISRs v H. Restructuring v I. Disbursement Graph vi
1. Project Context, Development Objectives and Design ............................................... 1 2. Key Factors Affecting Implementation and Outcomes .............................................. 6 3. Assessment of Outcomes .......................................................................................... 13 4. Assessment of Risk to Development Outcome ......................................................... 26 5. Assessment of Bank and Borrower Performance ..................................................... 27 6. Lessons Learned ....................................................................................................... 29 7. Comments on Issues Raised by Borrower/Implementing Agencies/Partners .......... 30 Annex 1. Project Costs and Financing .......................................................................... 32 Annex 2. Outputs by Component ................................................................................. 35 Annex 3. Economic and Financial Analysis ................................................................. 41 Annex 4. Bank Lending and Implementation Support/Supervision Processes ............ 42 Annex 5. Beneficiary Survey Results ........................................................................... 43 Annex 6. Stakeholder Workshop Report and Results ................................................... 44 4Annex 7. Summary of Borrower's ICR and/or Comments on Draft ICR ................... 47 Annex 8. Comments of Cofinanciers and Other Partners/Stakeholders ....................... 49 Annex 9. Achievements against Project Targets 51 Annex 10. List of Persons Met 55 Annex 11. List of Supporting Documents .................................................................... 59
MAP
i
A. Basic Information
Country: Benin Project Name: BENIN: Malaria Control Booster Program
Project ID: P096482 L/C/TF Number(s): IDA-H2290 ICR Date: 12/29/2011 ICR Type: Core ICR Lending Instrument: SIL Borrower: REPUBLIC OF BENIN Original Total Commitment:
XDR 21.60M Disbursed Amount: XDR 21.08M
Revised Amount: XDR 21.60M Environmental Category: B Implementing Agencies: Ministry of Health Cofinanciers and Other External Partners: RBM Partners B. Key Dates
Process Date Process Original Date Revised / Actual
Date(s)
Concept Review: 06/03/2005 Effectiveness: 03/16/2007 03/16/2007
Appraisal: 03/16/2006 Restructuring(s): 04/28/2010 08/29/2010
Approval: 06/01/2006 Mid-term Review: 03/16/2009 05/19/2009 Closing: 02/28/2011 06/30/2011 C. Ratings Summary
C.1 Performance Rating by ICR
Outcomes: Satisfactory Risk to Development Outcome: Moderate Bank Performance: Satisfactory Borrower Performance: Moderately Satisfactory
C.2 Detailed Ratings of Bank and Borrower Performance (by ICR)
Bank Ratings Borrower Ratings
Quality at Entry: Satisfactory Government: Moderately Unsatisfactory
Quality of Supervision: Satisfactory Implementing Agency/Agencies: Satisfactory
Overall Bank
Performance: Satisfactory Overall Borrower
Performance: Moderately Satisfactory
ii
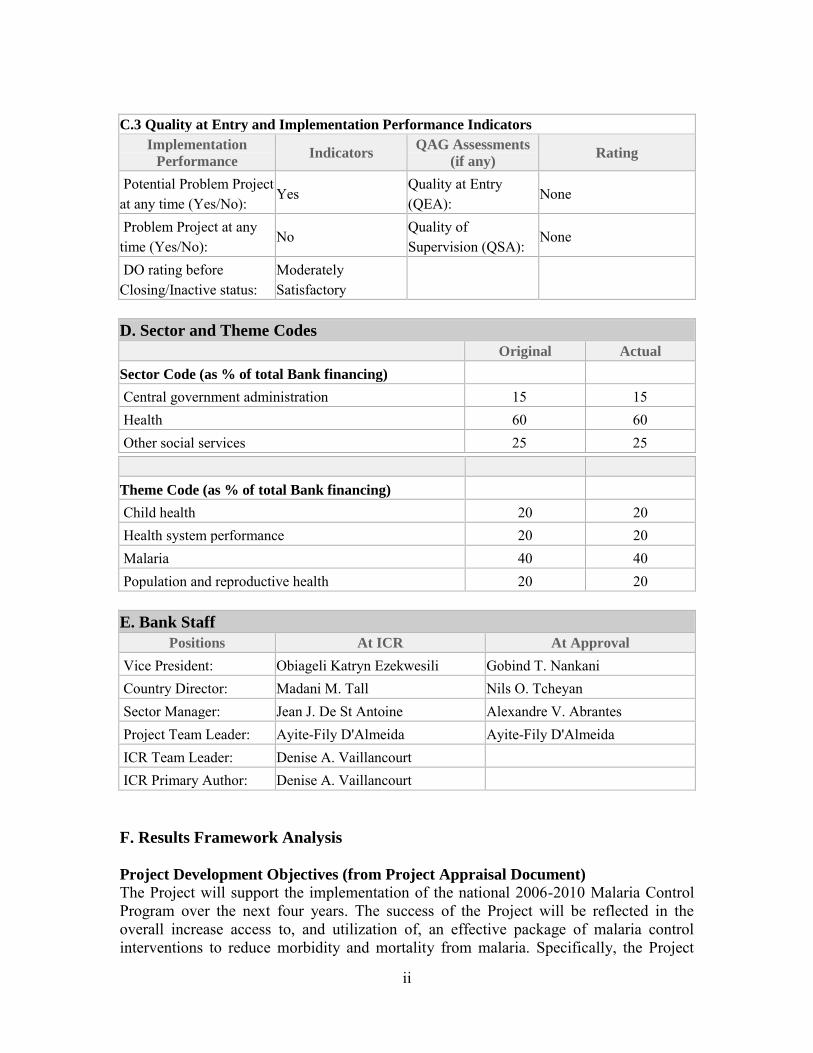
C.3 Quality at Entry and Implementation Performance Indicators
Implementation
Performance Indicators
QAG Assessments
(if any) Rating
Potential Problem Project at any time (Yes/No):
Yes Quality at Entry (QEA):
None
Problem Project at any time (Yes/No):
No Quality of Supervision (QSA):
None
DO rating before Closing/Inactive status:
Moderately Satisfactory
D. Sector and Theme Codes
Original Actual
Sector Code (as % of total Bank financing) Central government administration 15 15 Health 60 60 Other social services 25 25
Theme Code (as % of total Bank financing) Child health 20 20 Health system performance 20 20 Malaria 40 40 Population and reproductive health 20 20 E. Bank Staff
Positions At ICR At Approval
Vice President: Obiageli Katryn Ezekwesili Gobind T. Nankani Country Director: Madani M. Tall Nils O. Tcheyan Sector Manager: Jean J. De St Antoine Alexandre V. Abrantes Project Team Leader: Ayite-Fily D'Almeida Ayite-Fily D'Almeida ICR Team Leader: Denise A. Vaillancourt ICR Primary Author: Denise A. Vaillancourt F. Results Framework Analysis Project Development Objectives (from Project Appraisal Document) The Project will support the implementation of the national 2006-2010 Malaria Control Program over the next four years. The success of the Project will be reflected in the overall increase access to, and utilization of, an effective package of malaria control interventions to reduce morbidity and mortality from malaria. Specifically, the Project
iii
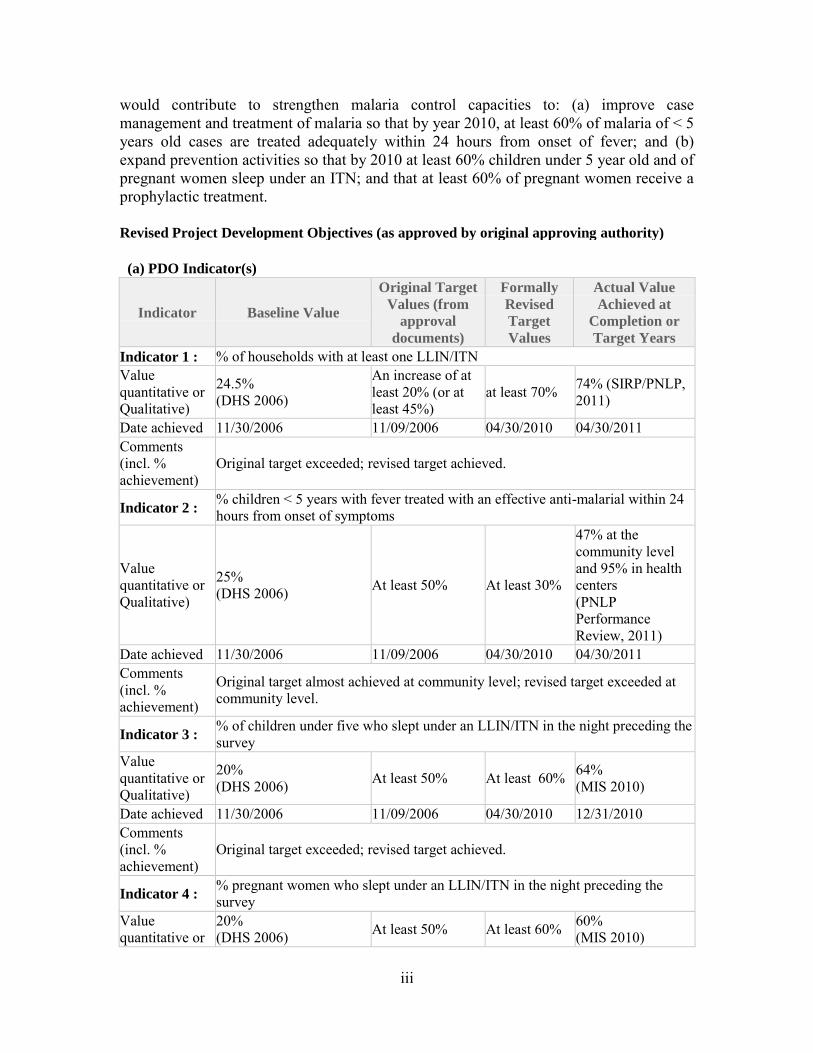
would contribute to strengthen malaria control capacities to: (a) improve case management and treatment of malaria so that by year 2010, at least 60% of malaria of < 5 years old cases are treated adequately within 24 hours from onset of fever; and (b) expand prevention activities so that by 2010 at least 60% children under 5 year old and of pregnant women sleep under an ITN; and that at least 60% of pregnant women receive a prophylactic treatment. Revised Project Development Objectives (as approved by original approving authority) (a) PDO Indicator(s)
Indicator Baseline Value
Original Target
Values (from
approval
documents)
Formally
Revised
Target
Values
Actual Value
Achieved at
Completion or
Target Years
Indicator 1 : % of households with at least one LLIN/ITN Value quantitative or Qualitative)
24.5% (DHS 2006)
An increase of at least 20% (or at least 45%)
at least 70% 74% (SIRP/PNLP, 2011)
Date achieved 11/30/2006 11/09/2006 04/30/2010 04/30/2011 Comments (incl. % achievement)
Original target exceeded; revised target achieved.
Indicator 2 : % children < 5 years with fever treated with an effective anti-malarial within 24 hours from onset of symptoms
Value quantitative or Qualitative)
25% (DHS 2006) At least 50% At least 30%
47% at the community level and 95% in health centers (PNLP Performance Review, 2011)
Date achieved 11/30/2006 11/09/2006 04/30/2010 04/30/2011 Comments (incl. % achievement)
Original target almost achieved at community level; revised target exceeded at community level.
Indicator 3 : % of children under five who slept under an LLIN/ITN in the night preceding the survey
Value quantitative or Qualitative)
20% (DHS 2006) At least 50% At least 60% 64%
(MIS 2010)
Date achieved 11/30/2006 11/09/2006 04/30/2010 12/31/2010 Comments (incl. % achievement)
Original target exceeded; revised target achieved.
Indicator 4 : % pregnant women who slept under an LLIN/ITN in the night preceding the survey
Value quantitative or
20% (DHS 2006) At least 50% At least 60% 60%
(MIS 2010)
iv
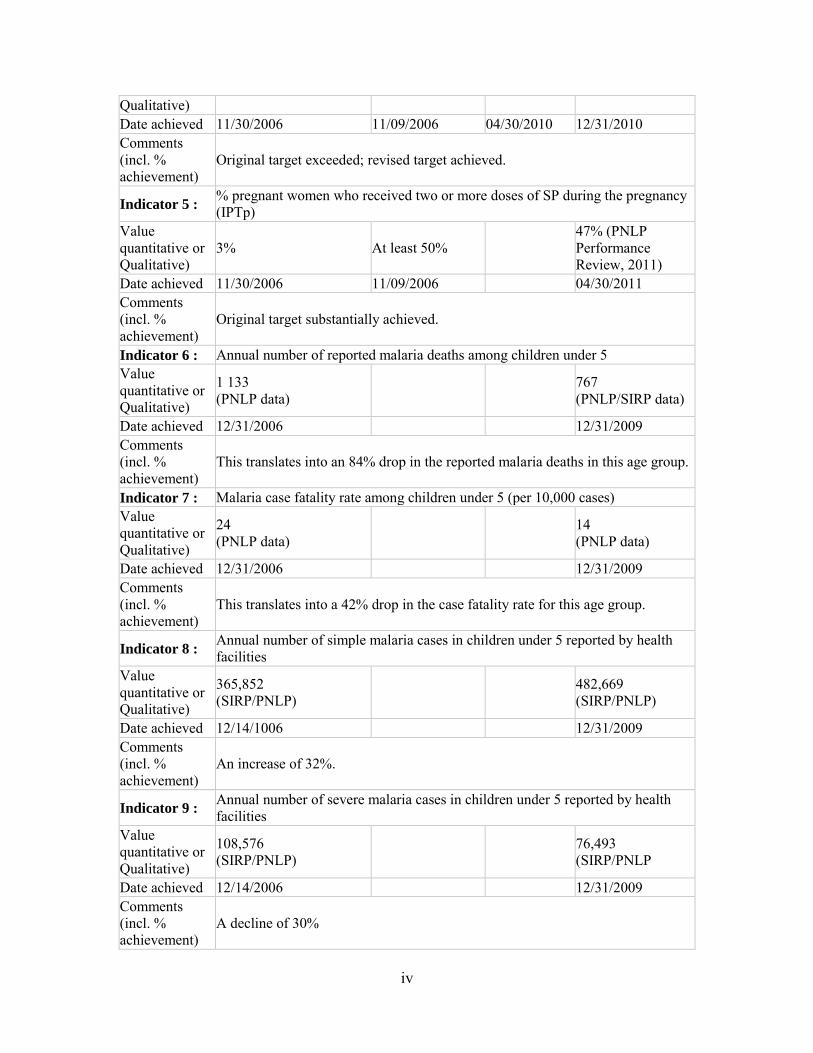
Qualitative) Date achieved 11/30/2006 11/09/2006 04/30/2010 12/31/2010 Comments (incl. % achievement)
Original target exceeded; revised target achieved.
Indicator 5 : % pregnant women who received two or more doses of SP during the pregnancy (IPTp)
Value quantitative or Qualitative)
3% At least 50% 47% (PNLP Performance Review, 2011)
Date achieved 11/30/2006 11/09/2006 04/30/2011 Comments (incl. % achievement)
Original target substantially achieved.
Indicator 6 : Annual number of reported malaria deaths among children under 5 Value quantitative or Qualitative)
1 133 (PNLP data) 767
(PNLP/SIRP data)
Date achieved 12/31/2006 12/31/2009 Comments (incl. % achievement)
This translates into an 84% drop in the reported malaria deaths in this age group.
Indicator 7 : Malaria case fatality rate among children under 5 (per 10,000 cases) Value quantitative or Qualitative)
24 (PNLP data) 14
(PNLP data)
Date achieved 12/31/2006 12/31/2009 Comments (incl. % achievement)
This translates into a 42% drop in the case fatality rate for this age group.
Indicator 8 : Annual number of simple malaria cases in children under 5 reported by health facilities
Value quantitative or Qualitative)
365,852 (SIRP/PNLP) 482,669
(SIRP/PNLP)
Date achieved 12/14/1006 12/31/2009 Comments (incl. % achievement)
An increase of 32%.
Indicator 9 : Annual number of severe malaria cases in children under 5 reported by health facilities
Value quantitative or Qualitative)
108,576 (SIRP/PNLP) 76,493
(SIRP/PNLP
Date achieved 12/14/2006 12/31/2009 Comments (incl. % achievement)
A decline of 30%
v
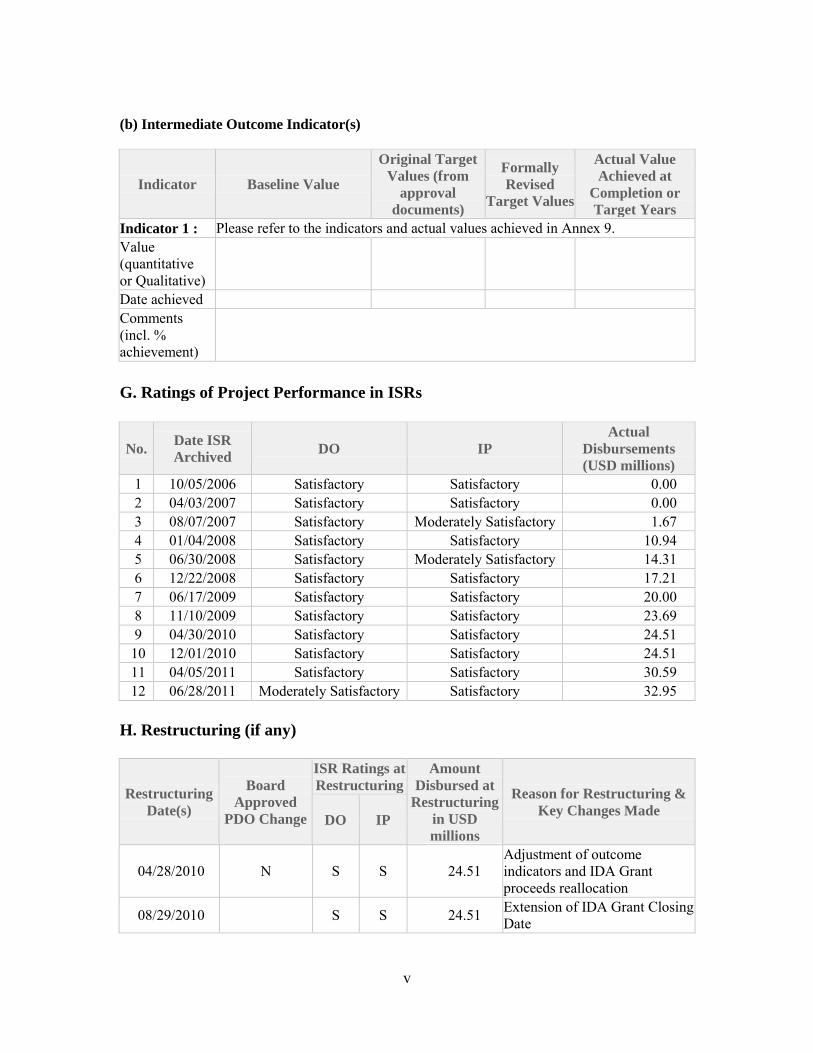
(b) Intermediate Outcome Indicator(s)
Indicator Baseline Value
Original Target
Values (from
approval
documents)
Formally
Revised
Target Values
Actual Value
Achieved at
Completion or
Target Years
Indicator 1 : Please refer to the indicators and actual values achieved in Annex 9. Value (quantitative or Qualitative)
Date achieved Comments (incl. % achievement)
G. Ratings of Project Performance in ISRs
No. Date ISR
Archived DO IP
Actual
Disbursements
(USD millions)
1 10/05/2006 Satisfactory Satisfactory 0.00 2 04/03/2007 Satisfactory Satisfactory 0.00 3 08/07/2007 Satisfactory Moderately Satisfactory 1.67 4 01/04/2008 Satisfactory Satisfactory 10.94 5 06/30/2008 Satisfactory Moderately Satisfactory 14.31 6 12/22/2008 Satisfactory Satisfactory 17.21 7 06/17/2009 Satisfactory Satisfactory 20.00 8 11/10/2009 Satisfactory Satisfactory 23.69 9 04/30/2010 Satisfactory Satisfactory 24.51
10 12/01/2010 Satisfactory Satisfactory 24.51 11 04/05/2011 Satisfactory Satisfactory 30.59 12 06/28/2011 Moderately Satisfactory Satisfactory 32.95
H. Restructuring (if any)
Restructuring
Date(s)
Board
Approved
PDO Change
ISR Ratings at
Restructuring
Amount
Disbursed at
Restructuring
in USD
millions
Reason for Restructuring &
Key Changes Made DO IP
04/28/2010 N S S 24.51 Adjustment of outcome indicators and IDA Grant proceeds reallocation
08/29/2010 S S 24.51 Extension of IDA Grant Closing Date
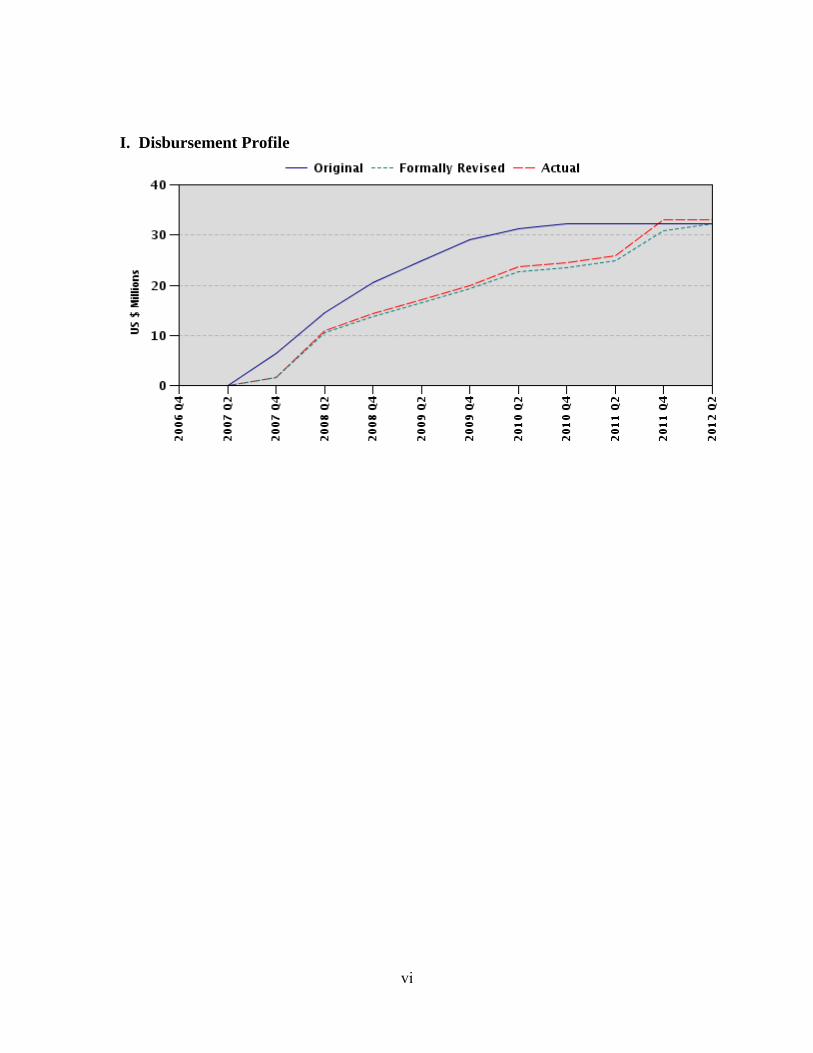
vi
I. Disbursement Profile
1
1. Project Context, Development Objectives and Design (descriptive, taken from
other docs, not evaluative)
Context at Appraisal (brief country/sector background, rationale for Bank assistance)
1. At the time of project design, malaria was the leading cause of mortality among children and morbidity among adults in Benin. Pregnant women and their unborn children were known to be particularly vulnerable to this disease, which was a major cause of perinatal mortality, low birth weight and anemia. Benin’s Poverty Reduction Strategy Paper and Joint Staff Assessment (February 21, 2003) cited incidences of simple malaria in 1999 of: 120 per 1,000 within the general population; 437 per 1,000 among infants (0-11 months); and 219 per 1,000 among children (1-5 years). Studies and estimates cited in the Project Appraisal Document (PAD) put direct malaria deaths of children under 5 between 10,000 and 20,000 annually, with an additional 5,000 to 6,000 of indirect malaria deaths in this age group. 2. In 2006 Benin’s health sector consisted of 3 tertiary hospitals, 6 general hospitals, 46 provincial hospitals (26 public and 20 private) and 784 primary health centers (481 public and 303 private). Health system issues included: weak sector management (including inadequate decentralization and results focus); insufficient resources; distortions in human resource distribution to the detriment of rural areas; disparities in service provision between geographic regions and economic groups; and poor quality and limited access to services by the poor. These were being addressed by a number of reforms, notably: the adoption of a human resource management strategy (2004); the transfer of funds to health district management teams for operating costs as of the 2004 budget; the launch of marginal budgeting for bottlenecks approach recommended in the 2004 Country Health Status Report; consideration of poverty and performance criteria starting with the 2005 budget exercise, which culminated in increased resources for health districts; and a pro-poor policy adopted in 2005 to provide free health services for those who could not afford the fees. In the early years of the new millennium, over one-third of health facility visits were estimated to be generated by malaria. 3. In 2000 the Government of Benin (GoB) adopted a national policy on malaria and developed the first National Strategic Plan (NSP) (2001-2005), with the technical support of the World Health Organization (WHO) and other partners, and in line with Roll Back Malaria (RBM) and Abuja objectives. In 2001 a Facilitators Group (Groupe des Facilitateurs), made up of RBM partners,1 under the overall coordination of WHO, served to support and coordinate RBM efforts. The first NSP sought to reduce morbidity and mortality from malaria generally in Benin by 50 percent by 2010, with the following specific goals: increase malaria control coordination capacities; provide adequate access and treatment to at least 80 percent of malaria patients; provide access to preventive measures such as long-lasting insecticide-treated nets (LLINs) to at least 80 percent of at-risk populations (pregnant women and children under 5); provide at least 80 percent of pregnant women with prophylactic treatment; and strengthen M&E for malaria control. 4. A new national Malaria Strategy for 2006-2010 (in final draft at the time of project design and subsequently adopted during the first year of implementation) supported essentially the same
1 This informal advisory group was comprised of technical agencies, multilateral and bilateral donors, NGOs, the private sector, and research institutes.
2
objectives as the first NSP, but with some updates. Recognizing growing resistance to chloroquine and on WHO’s recommendation, the new strategy aimed to phase out the use of chloroquine and scale up the use of Artemisinin-based combination therapy (ACT), from 50 percent in 2007 to 100 percent in 2009. It also: envisaged the more vigorous distribution and promotion of LLINs; introduced Pharmo-Vigilence; devoted attention to training of health providers to implement the new ACT protocols and intermittent preventive treatment for pregnant women (ITPp) implementation. The estimated cost of implementing this Strategy (US$70 million equivalent) far exceeded available resources ($1.9 million of GoB budget in 2006, or 2 percent of the total health allocation; US$4.4 million from the Global Fund for AIDS, TB and Malaria (GFATM); and modest resources from WHO and UNICEF). The GoB requested World Bank financing through its Africa Region Malaria Booster Program, which aims to amplify RBM’s impact in the world’s worst-hit region.2 Box 1: Benin’s Strategic Plan for Malaria Control, 2006-2010 Goal:
Contribute to the improvement of the health status of the population General Objective:
Between 2001 and 2010 reduce by 50 percent the levels of mortality and morbidity due to malaria between 2001 and 2010 Specific Objectives:
Between 2001 and 2010: Ensure the adequate treatment of 80 percent of simple malaria cases in children under five in the home and in the
community in less than 24 hours after the onset of symptoms Ensure the adequate treatment of 80 percent of simple malaria cases presented in health facilities Ensure the correct treatment of 80 percent of serious malaria cases in line with the national malaria control policy Achieve an 80 percent rate of ITN use by children under five Achieve an 80 percent rate of ITN use by pregnant women Ensure 80 percent coverage of pregnant women with the intermittent preventive treatment of Sulfadoxine-
Pyrimethamine Components:
Management of the Malaria Control Program and its partnerships in order to Roll Back Malaria Treatment of malaria cases in health facilities, at the community level and in households Prevention of malaria through the integrated control of vectors and intermittent prevention treatment of pregnant
women Integrated communication, including: behavior change communication, advocacy and social mobilization Epidemiological and entomological surveillance and surveillance of the therapeutic efficacy of anti-malaria
medicines; and monitoring and evaluation of the Malaria Control Program Research. Source: République du Benin, Ministére de la Santé, Direction Nationale de la Protection Sanitaire, PNLP, “Plan de
suivi et d’évaluation du plan stratégique de lutte contre le paludisme au Benin 2006-2010,” décembre 2006.
5. The Bank’s support was prompted by the recognition of both GoB and the Bank of its strategic importance, given malaria’s high incidence and negative impact on human and economic development (CAS Report No. 26054-BEN, July 6, 2003).
2 The Booster Program translates the World Bank’s Global Strategy and Booster Program into an outcome driven assault on malaria in Africa. It builds on a revitalized RBM Global Partnership, complementing the efforts of other partners both at national and regional level. It is planned to last 10 years, including an intensive phase (July 1, 2005 – June 30, 2008), during which the Bank would contribute to an aggressive effort to scale up and achieve impact. It aimed to increase rapidly the utilization of ITN and IPTp services to 60 percent among target groups. In the long-term, it aims to contribute to achieving the Abuja targets and the goals outlined in the RBM Partnership’s Global Strategy: halving malaria-associated mortality between 2001 and 2010 and halving it again by 2015.
3
Original Project Development Objectives (PDO) and Key Indicators (as approved)
6. The Project was to support the implementation of the national 2006-2010 Malaria Control Program over the next four years. The success of the Project was to be reflected in increased access to, and utilization of, an effective package of malaria control interventions to reduce morbidity and mortality from malaria. Specifically, the Project aimed to contribute to the strengthening of malaria control capacities to: (a) improve case management and treatment of malaria so that by year 2010 at least 50% of malaria of <5 years old cases would be treated adequately within 24 hours from onset of fever; and (b) expand prevention activities so that by 2010 at least 60% of children under five years old and of pregnant women would sleep under an ITN; and that at least 60% of pregnant women would receive a prophylactic treatment.3 Annex 1 (Results Framework and Monitoring) of the PAD also specifies other outcomes, which this ICR will assess: strengthened program M&E and upgraded institutional (PNLP management) capacities. Revised PDO (as approved by original approving authority) and Key Indicators (and
reasons/justification)
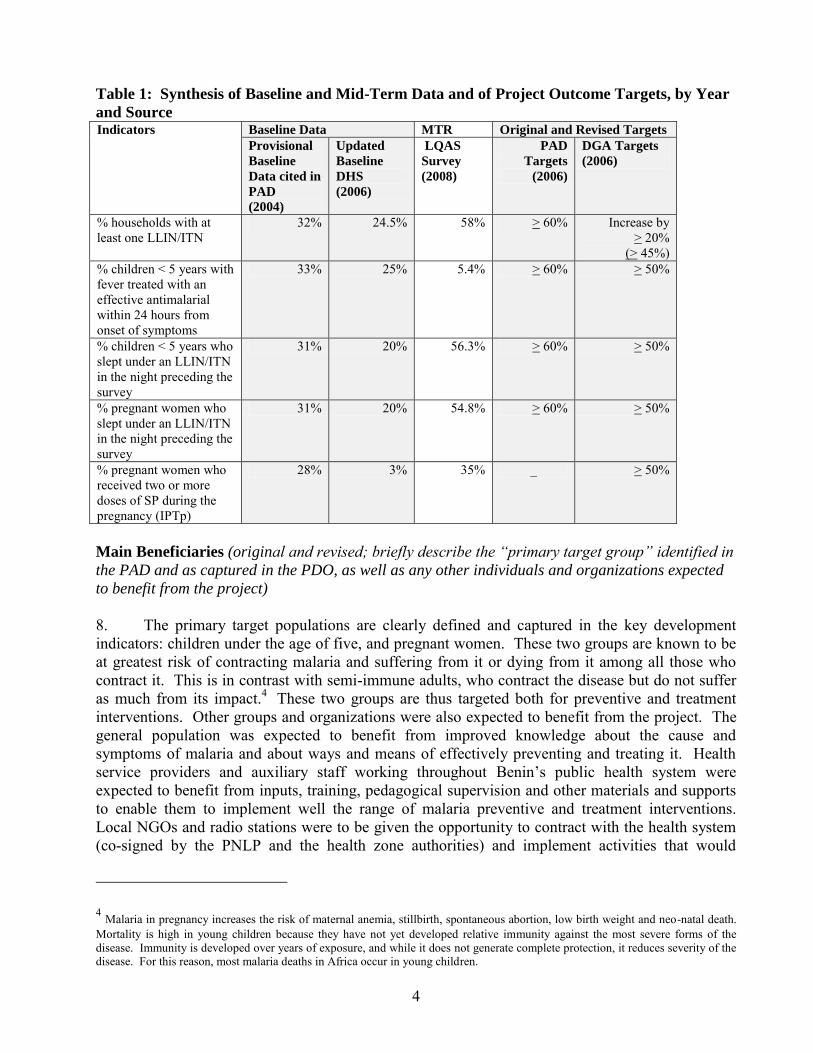
7. The project development objectives did not change during the life of the project. But several project targets were revised in April 2010 when the project was 70 percent disbursed. The revisions were made in light of updated baseline data and progress achieved as of the mid-term review in 2008. Three targets (on LLIN access and use) were amended to be more ambitious, while one target (on effective treatment) was revised to a more modest level. Table 1 below provides a synthesis of the project’s: baseline data (original and updated to reflect the 2006 DHS data); mid-term progress (2008); and project targets, both original and revised (the latter approved by the Bank in April 2010). In addition to the changes in baseline and target values, this table points out discrepancies between the original project targets articulated in the PAD, and those (more modest targets) articulated in the DGA (Schedule 6. Performance Indicators). The Bank’s documentation on the project restructuring (notably the changes to target values) acknowledges these discrepancies in retrospect, noting that the set in the Development Grant Agreement (DGA) were the binding ones. This evaluation thus bases itself on the targets set in the DGA.
3 These are the objectives articulated in the PAD (pp ii and 5). The objectives in the DGA are consistent with these objectives, but more succinctly stated. Above-stated project objectives are also consistent with Annex 1 of the PAD. There is some discrepancy between the project-specific targets articulated in the PAD and in the DGA, which is discussed/addressed in Section 3 (Assessment of Outcomes). Key performance indicators for the project are consistent with those for the program, but targets are more modest.
4
Table 1: Synthesis of Baseline and Mid-Term Data and of Project Outcome Targets, by Year
and Source Indicators Baseline Data MTR Original and Revised Targets
Provisional
Baseline
Data cited in
PAD
(2004)
Updated
Baseline
DHS
(2006)
LQAS
Survey
(2008)
PAD
Targets
(2006)
DGA Targets
(2006)
% households with at least one LLIN/ITN
32% 24.5% 58% > 60% Increase by > 20%
(> 45%) % children < 5 years with fever treated with an effective antimalarial within 24 hours from onset of symptoms
33% 25% 5.4% > 60% > 50%
% children < 5 years who slept under an LLIN/ITN in the night preceding the survey
31% 20% 56.3% > 60% > 50%
% pregnant women who slept under an LLIN/ITN in the night preceding the survey
31% 20% 54.8% > 60% > 50%
% pregnant women who received two or more doses of SP during the pregnancy (IPTp)
28% 3% 35% _ > 50%
Main Beneficiaries (original and revised; briefly describe the “primary target group” identified in
the PAD and as captured in the PDO, as well as any other individuals and organizations expected
to benefit from the project)
8. The primary target populations are clearly defined and captured in the key development indicators: children under the age of five, and pregnant women. These two groups are known to be at greatest risk of contracting malaria and suffering from it or dying from it among all those who contract it. This is in contrast with semi-immune adults, who contract the disease but do not suffer as much from its impact.4 These two groups are thus targeted both for preventive and treatment interventions. Other groups and organizations were also expected to benefit from the project. The general population was expected to benefit from improved knowledge about the cause and symptoms of malaria and about ways and means of effectively preventing and treating it. Health service providers and auxiliary staff working throughout Benin’s public health system were expected to benefit from inputs, training, pedagogical supervision and other materials and supports to enable them to implement well the range of malaria preventive and treatment interventions. Local NGOs and radio stations were to be given the opportunity to contract with the health system (co-signed by the PNLP and the health zone authorities) and implement activities that would
4 Malaria in pregnancy increases the risk of maternal anemia, stillbirth, spontaneous abortion, low birth weight and neo-natal death. Mortality is high in young children because they have not yet developed relative immunity against the most severe forms of the disease. Immunity is developed over years of exposure, and while it does not generate complete protection, it reduces severity of the disease. For this reason, most malaria deaths in Africa occur in young children.
5
expand outreach and promotion activities. Departmental-level (DDS) and health zone staff were slated to benefit from program management and capacity building support, including: training, systems strengthening, supervision supports, office furniture and equipment and other operating costs to enable them to better fulfill their respective coordination and oversight responsibilities. PNLP staff, as well, stood to benefit from the same types of support aimed at strengthening their systems and capacities for program coordination and management. Original Components (as approved)
9. The following presentation of components is drawn from Schedule 2 of the DGA, for its brevity and clarity. It is consistent with the more detailed component descriptions in the PAD, except for the absence of the Vector Management Plan subcomponent of Component 4, which has been added. Annex 2, which assesses component outputs against original plans, draws on the component detail in the PAD. Original component costs shown below include contingencies. Actual costs are derived from GoB final estimates and the Bank’s disbursement data (details in Annex 1).
10. Part A: Improving Case Management and Access to Treatment (original estimate:
US$14.7 million or 29 percent of original project cost; actual cost: US$8.1 million or 24 percent
of the final project cost). Improving malaria treatment capacity of the public and private health sectors and qualified NGOs, through the provision of goods, equipment, technical advisory services, training, and the provision of malarial drugs including ACT to the public sector health clinics at all levels and subsidized prepackaged ACT to the private sector and qualified NGOs. 11. Part B: Scaling Up Prevention Activities (original estimate: US$13.0 million or 45
percent of original project cost; actual cost: US$21.3 million or 65 percent of the final project
cost). Introduction of large-scale community efforts for malaria prevention, through the provision of training for public and non-public distributors and community mobilizers, the provision of LLINs to vulnerable target groups, IPTp and SP medication for pregnant women, and the organization of IEC/BCC campaigns. 12. Part C: Strengthening of Monitoring and Evaluation Activities (original estimate:
US$1.7 million or 8 percent of original project cost; actual cost: US$0.9 million or 3 percent of
the final project cost). Strengthening of the malaria-related monitoring and evaluation system and data management at both the central and operational level, through the provision of financial and technical assistance support, and training, equipment and operational research. 13. Part D: Program Management, Capacity Building and Promoting Regional
Cooperation (original estimate: US$1.6 million or 5 percent of original project cost; actual cost:
US$2.7 million or 8 percent of the final project cost).
1. Project Management. Strengthening of the management capacity of the PNLP, through the contracting of additional specialized staff and for operating costs of the PNLP Unit and the provision of equipment and rehabilitation works related to the execution of the program.
2. Capacity Strengthening. Strengthening of the capacity and expertise of the PNLP staff, MoH and qualified NGOs, through the provision of specified training.
3. Regional Cooperation and Knowledge Sharing. Promotion of regional cooperation and knowledge management regarding malaria prevention, monitoring and control activities through technical assistance, learning seminars and financial support to the MoH for inter-regional communication, including travel and communication expenses.
6
4. Implementation of the vector/pest management plan prepared by PNLP and disclosed in February 2006. Support to PNLP’s Vector Management & Social Marketing Unit efforts to integrate vector management into partnership agreements with health facilities, NGOs and the private sectors benefitting from Government financing.
Revised Components
14. Project components were not substantially revised.
Other Significant Changes (in design, scope and scale, implementation arrangements and
schedule, and funding allocations)
15. There were no other significant changes. 2. Key Factors Affecting Implementation and Outcomes
Project Preparation, Design and Quality at Entry (including whether lessons of earlier
operations were taken into account, risks and their mitigation identified, and adequacy of
participatory processes, as applicable)
16. A July 2010 QALP Assessment rated quality at entry as “satisfactory” on all points: strategic relevance; realism of design and risk assessment; and fiduciary, safeguards and GAC aspects. The following findings of this ICR corroborate the QALP assessment.
17. Soundness of Background Analysis. Background analysis undertaken during project preparation was sound. The project was grounded in extensive country analysis, undertaken by the GoB and its malaria partners, led by WHO. Analysis drew on information and studies examining operational, medical, institutional aspects as well as a review of Benin’s experience in implementing RBM over the previous several years. An evaluation of progress and constraints in delivering an effective anti-malarial package, undertaken in March 2003, was an important source. Analysis drew heavily on the knowledge and expertise of WHO and the RBM partnership, which undertook multiple missions to this end over the two years leading to project design. This work also drew on the Africa-wide analysis of the burden of malaria and the shortcomings of national programs and their partners’ support, undertaken in the context of preparing the Africa Region’s Malaria Booster program. Interventions were thus based on best available and respected scientific evidence of efficacy and technical advice. 18. Analysis of lessons was thorough, encompassing the global experience in malaria control, and the Bank’s experience in Benin, spanning its whole portfolio and its health sector-specific portfolio, including both health systems and disease-specific interventions. Most notable among the many lessons distilled and incorporated into project design are: the importance of decentralized efforts and community involvement; strong investment in M&E; the use and further strengthening of the health system in the context of fighting a single disease; and the importance of simplicity of partnership arrangements with NGOs and community-based organizations. 19. The rationale for the Bank’s involvement was to complement technical and financial support provided by other partners, in line with its comparative advantage. This included: building on health sector budget support and dialogue through PRSCs I and II; the ability to commit to a multi-year effort; program-specific capacity building experience and expertise in the context of a health
7
systems approach; and the ability to bring cross-disease, cross-sectoral experience and lessons to the approach.
20. Assessment of Project Design. The project was well designed, with appropriate objectives and indicators and a results framework that established clear links from activities (or components) to outcomes. (See Section 3 presenting relevance of design analysis for more detail.) Responsibility for project coordination and management was placed in the PNLP. Instead of establishing a separate PIU, the PNLP staff was to be supplemented by a procurement expert and a financial management expert to ensure respect of the Bank’s fiduciary exigencies. This encouraged the utilization and further strengthening of the PNLP staff at all levels of the health system, including those in the Departments and zones. PNLP was assessed and considered to have adequate staff capacity to undertake the managerial and technical aspects of project implementation, with the support and backstopping of the Bank. Terms of reference for fiduciary staff were submitted to IDA for non-objection prior to effectiveness, along with a procurement plan for the first 18 months of implementation. The contracting of NGOs to work at the community level was essential to the behavior change objectives and the expected uptake of prevention and treatment interventions. Draft contract agreements for NGOs were submitted to IDA prior to effectiveness, and about 30 health NGOs, pre-qualified under GFATM financing, were slated to scale-up their activities with project support. Working contracting processes and arrangements, employed by GFATM, were adopted by the project. While there were no co-financiers, the design and implementation enjoyed the inputs and excellent collaboration and coordination of all RBM partners, under the leadership of WHO.
21. Adequacy of Government Commitment. Government commitment was high at the time of project preparation and even before. Relevant policies and strategies were in place. Ownership and budget support of the malaria control program had been strong since 2000, with malaria prominently featured in the PRSP. The Head of State, himself, was interested in scaling up malaria efforts in Benin, with GoB ultimately deciding to utilize the remaining funds under Benin’s IDA allocation for the malaria project. Thanks to the participatory process used to develop the 2006-2010 Malaria Strategy, which the project was designed to support, ownership among a broad range of stakeholders was strong.
22. Risk Assessment and Mitigation. The overall risk rating was high, reflecting a very candid and realistic assessment of project risks, including: slow/stalled implementation due to capacity constraints and/or change in Government, unavailability of LLINs on the world market, failure to reach priority groups, inability to bring about behavior change, inadequate priority to M&E and use of data for decision-making, and issues of governance and corruption. Mitigation measures were appropriate, including: the (continued) mobilization of technical and financial support from the RBM partnership; the assessment and support of commodity procurement and distribution capacity; well-designed IEC/BCC activities delivered by NGOs; regular, rigorous, joint reviews of program performance, based on simple reporting requirements; and audits/spotchecks of the proper accounting of funds and goods acquired under the project. Implementation (including any project changes/restructuring, mid-term review, Project at Risk
status, and actions taken, as applicable)
23. The project became effective on March 16, 2007, after a slight delay due to the need for GoB to produce a legal opinion on the Grant Agreement acceptable to IDA. There were some delays in implementation, due to slow processing of priority bidding documents and weakness in the coordination and management of the project. But these were managed and mitigated with close
8
Bank guidance and supervision. By the time of the mid-term review, which took place in May 2009, two sets of data were available that warranted amendments to some of the project’s outcome targets: (a) final data from the DHS 2006 revealed lower baseline values than the best estimates available at the time of project approval; and (b) the 2008 LQAS survey showed that progress on three outcome indicators already exceeded end-of-project targets,5 progress on another6 was on track, and progress on the other7 was very modest. Targets were thus adjusted accordingly, the first three being adjusted upwards, and the last one being reduced. It is important to note that both the original and revised (DHS 2006) baselines for effective treatment of children under five included the use of chloroquine, which was considered as an effective treatment in these data sources, while the (mid-term) LQAS survey and the target excluded the use of chloroquine from their definitions of an effective treatment, as the project was supporting GoB policy, endorsed by RBM, to phase out the use of chloroquine and phase in the use of ACTs. 24. Overall implementation was satisfactory, although there were delays in some activities, such as training. In light of the new data and of the MTR conclusions that found the project to be in full compliance with all legal covenants, social and environmental safeguard requirements and financial management exigencies, the project was restructured in 2010, in response to a request of GoB submitted to the Bank on April 9, 2010. The main elements of the restructuring were: (1) the adjustments to the outcome targets, as itemized in Table 1; (2) the reallocation of the proceeds of the project to reflect actual disbursements and projections for the use of the balance of project funds; and (3) the extension of the original closing date (February 28, 2011) to June 30, 2011 to accommodate an action plan proposed by the PNLP. The action plan included: activities linked to (a) the national mass campaign distribution of LLINs; (b) household and health facilities surveys to document end-of-project results; (c) research to assess the use of LLINs and ACTs; and (iv) the audit of project accounts. This restructuring did not warrant Board approval and thus was approved by the Vice President of the Africa Region. 25. Major Factors Affecting Implementation. During two of the four years of project implementation (2009 and 2010), successive strikes of health staff (at all levels of the health pyramid) constituted an important impediment to project implementation at the level of the health zones. During these years, commodities for prevention and treatment interventions were in place, staff had been trained and communities had been informed and motivated to access preventive and treatment interventions. But when health staff were on strike, those seeking bednets through regular vaccination and ANC services and those seeking treatment could not access these services when staff were absent. Strikes were outside of Government or implementing agencies’ control. 26. Slow approvals of procurement documents submitted to the Direction Nationale des
Marches Publics caused serious delays in the acquisition of goods and in disbursements. Delays averaged two months, but in certain cases went up to three months, even though the GoB standards call for approval within 15 days. Likewise, delays in signatures of contracts by the Ministry of Economy and Finance (MoEF) averaged two months, and went up as high as five months, notwithstanding the 15-day turnaround requirement. There were also delays in the commitment of
5 % of households with at least 1 LLIN; % of children under 5 who slept under a LLIN/ITN during the night preceeding the survey; and % pregnant women who slept under a LLIN during the night preceding the survey.
6 % pregnant women who received two or more doses of SP during the pregnancy (IPTp)
7 % children with a fever treated with an effective antimalarial within 24 hour from the onset of symptoms
9
procurements in MoEF’s Systéme Intégré de Gestion des Finances Publiques (SIGFiP), caused by insufficient credit given to the project in the national budget, despite the estimates prepared and submitted to MoEF. Compliance with Government counterpart financing obligations under the project had a favorable impact on implementation. All of these factors were subject to Government
control.
27. Within the control of the Implementing Agency (Ministry of Health/PNLP) were the changes in Project Coordinators. There were four Coordinators during the four-year implementation period. In 2008 during a time of ministerial changes and inadequate project performance, the outgoing coordinator was duly replaced by the Ministry with a person who had the required skills and expertise, in response to the Bank’s demands. While delays in the training of health staff on the new policy and protocols for treatment and prevention interventions might initially be considered as being within MoH/PNLP’s control, these delays were linked to the availability of initial stocks of critical inputs, held up by above-noted procurement delays. Very favorable to good project implementation were the semi-annual reviews of program (and project) performance organized by PNLP and attended by MoH Cabinet, relevant Divisions in MoH, the Bank’s team and other RBM partners, and other national partners and institutions involved, which fostered a shared vision, good coordination and productive partnerships. Also favorable to project implementation were the strong links with communities, especially through NGOs and community-based malaria volunteers, which provided enhanced synergies between supply- and demand-side activities. As noted below, strong M&E also favorably influenced implementation. 28. During 2008 political changes (new minister) and turnover of project coordinator posed problems with lack of decisions and poor decisions. This has been the only period of serious concern during implementation. Monitoring and Evaluation (M&E) Design, Implementation and Utilization
29. Design. The design of M&E was strong. A full component was developed to ensure that it was given sufficient attention and support. (See the description of Component 3 for details of planned support.) Support emphasized: capacity building; the development of an M&E framework for the 2006-2010 Strategic Plan for Malaria; the refinement of the system and indicators and their integration into the sector-wide system for data collection and management (SNIGS); the use of data for priority setting, identification and resolution of implementation bottlenecks and strategic decision-making, by staff at all levels of the health system. Support also envisaged the collaboration, coordination and complementarity of the Bank’s Malaria Implementation Resource Team (MIRT), RBM’s Monitoring and Evaluation Research Group (MERG) and WHO in providing technical assistance and backstopping to PNLP to this end.
30. Implementation. M&E was implemented, as designed. An M&E framework was developed. Indicators were refined to better track program performance and outcome; and these were integrated into the SNIGS. A number of studies and surveys were implemented and capacity was built at all levels of the system. Section 3 (paragraphs 61-64) of this report and Annex 2 (on outputs) provide more detail on the implementation of M&E.
31. Utilization. There was interest in using results emanating from the different evaluations throughout the project’s life, at operational and strategic levels, alike. At the operational level, the 2008 LQAS results pointed to health zones that were not performing well on key project indicators, covering both prevention and treatment interventions. These health zones were targeted for corrective action. They prepared action plans targeted at improvements on
10
key indicators, which were supported by project financing for their implementation. Monitoring and support of all Departments and zones were especially meaningful in the context of performance-based contracts signed under the project and linked to targets and indicators. At the strategic level, the different evaluations proved to be very useful for strategic decision making. For example, the results of the evaluation of vector resistance to insecticides influenced the choice of insecticides for the treatment of bednets utilized in Benin. Moreover, tests on the sensitivity of parasites to anti-malarial drugs made possible the development of strategies aimed at slowing parasite resistance. Of note is the isbu forbidding the use of monotherapies in Benin. The DHS 2006 and LQAS also influenced the resetting of (mostly) more ambitious and better informed targets. Annual reviews of program performance and the health facilities survey pointed to weaknesses in service quality, which were subsequently targeted. Performance-based contracts with NGOs were seriously implemented and linked to project indicators, with a small number of contracts not being renewed, based on unsatisfactory performance. Safeguard and Fiduciary Compliance (focusing on issues and their resolution, as applicable)
32. Safeguards. The project was appropriately classified as Category B and triggered OP/BP/GP 4.01 (Environmental Assessment) and OP 4.09 (Pest Management) due to the large amount of pests and pesticides that would be handled as part of the project. A Medical Waste Management Plan and a Vector/Pest Management Plan were prepared and disseminated. During project implementation there were some delays in compliance, due to low institutional capacity and weak cooperation among involved institutions. These delays were reflected in ISRs, which downgraded safeguards compliance in two of 12 ISRs prepared on the project. Close supervision by the Bank supervision ultimately ensured satisfactory implementation of the medical waste and vector/pest management plans. Activities were undertaken to support the identification and destruction of larvae breeding areas through a participatory approach, involving MoH, the community and Cotonou’s municipality actors. A system was also developed and implemented to properly dispose of discarded plastic wrappings for the LLINs, which were potentially hazardous to the population. The ICR mission saw evidence of this system during its field visits. 33. Procurement. Capacity assessments during design pointed to the inexperience of the procurement unit of MoH (CPMP), and the long experience of the Centrale d’Achat des
Médicaments Essentiels et Consommables Médicaux (CAME) in the procurement of medicines and medical supplies. The design envisaged the hiring of a contractual procurement specialist to work with CPMP and the delegation of about 70 percent of the procurement to CAME. WHO was also envisaged to be heavily involved, especially for the procurement of the drug Coartem and the provision of technical advice and assistance. The Operational Manual was to clarify roles and responsibilities and procurement procedures. Also envisaged to mitigate procurement risks: (i) low thresholds of Bank prior review for all major packages under the project, (ii) at least two procurement missions (four in the first year) and (iii) one procurement audit per year. In addition, corruption clauses, including penalties, were included in all bid documents to be used by CPMP and CAME. Publishing of a procurement plan, bid evaluations and contract awards was made mandatory for all agencies. 34. Already noted slow and inefficient review and clearance procedures of the National Tender Board (NTB) and the delays in MoEF signature of contracts undermined the timely availability of critical project inputs, most notably, ACTs and LLINs. Even without the delays caused by the NTB and MoEF, procurement performance was not optimal in the early years of the project. There was some confusion about roles and responsibilities of CPMP, PNLP/procurement staff, and the CAME. The arrival of a new coordinator in mid-2008 marked the start of efforts to address procurement
11
issues and culminated in a substantial improvement in performance, thanks to a number of strengthening measures: procurement training for two staff of CPMP and one of CAME; extension of the contract of an additional procurement specialist; strengthening of CAME capacity for safe storage of pharmaceutical products; and a clarification of roles and responsibilities, especially between CAME and PNLP, and including a closer collaboration between PNLP and CPMP.
35. The initial recruitment of some 30 prequalified NGOs to work at the community level (one per zone) was delayed from early 2007 to December 2007. Two aspects of this particular procurement were improved in light of project experience. First, the initial process was modeled after the GFATM process, which was undertaken at the central level. This caused health zones to feel little ownership of NGOs’ activities. In certain cases NGOs were not readily accepted by the communities they were serving, as they were not involved in the selection process. And the NGOs did not have a strong sense of accountability to the health zone. The next round of contracting was undertaken with the full involvement of the local level (health authorities, local authorities, civil society) and the contracts were signed by the PNLP coordinator and the executive directors of these NGOs. But activity reporting of these structures was subject to the review of the health zones before their transmission to the DDS and PNLP. These measures served to incorporate the lessons of the first round. Second, selection criteria were revised to be more rigorous and more responsive to the need; and more rigor was applied in the selection of NGOs. Evidence of this rigor is demonstrated in the fact that contracts of a few low-performing NGOs in the first round of contracts were not renewed for the next round.
36. Financial Management. Fulfilled effectiveness conditions successfully set up financial management arrangements within PNLP. Financial management was well implemented initially, but gradually deteriorated by June 2008 (at which time the task team rated it MU), due to the under-utilization of accounting software and the failure to update accounting entries resulting in substantial delays in the submission of financial monitoring reports. Also at this point in time, control of operating expenditures was found to be weak, as evidenced in the anomalies in travel and training expenses, detected by financial management supervision missions. Vigorous intervention of the task team and effective implementation by PNLP of the team’s recommendations, including the recruitment of a second accountant, corrected these weaknesses. By the time of the 2009 MTR financial management performance was found to be fully satisfactory. There were no overdue audits, no qualified issues or accountability issues raised in audit reports. This satisfactory performance continued through the rest of the life of the project.
Post-completion Operation/Next Phase (including transition arrangement to post-completion
operation of investments financed by present operation, Operation & Maintenance arrangements,
sustaining reforms and institutional capacity, and next phase/follow-up operation, if applicable).
37. The project was designed to support GoB’s malaria NSP 2006-2010. During the ICR mission, a new NSP (2011-2015) was approved by GoB and strongly endorsed by the President of the Republic, who considers malaria a priority. The new strategy builds on the experience and lessons of the previous ones, and introduces a few refinements: to extend coverage of treatment and prevention interventions to all of Benin’s population; and to ensure more routine testing in health facilities to confirm malaria diagnosis before dispensing ACT. The adequacy of budget provision is in question, given that MoH’s overall budget allocation has declined. With the good coordination and substantial support of Benin’s malaria partners, there is likely to been continued support to the provision of essential inputs (nets, drugs, tests), and to other aspects of the program, including continued support to M&E and research. PNLP’s ongoing efforts to map needs and the interventions of all partners should be useful to this end. The staffing and management of PNLP
12
appears to be adequate to implement the new five-year strategy, although it will need to be accompanied and supported. This will be especially important (a) at the decentralized levels of MoH (Departments and health zones); and (b) in light of possible consolidation and streamlining of some PNLP functions into already existing MoH structures. All goods acquired under the project have been audited and are accounted for. Their adequate operation and maintenance will depend on overall capacity of the health system to this end. 38. In response to overwhelming interests (expressed by policy-makers, implementers, RBM partners, and beneficiaries) in continued Bank support, a supplemental grant for malaria in the amount of US$10 million is being processed under the ongoing Benin Health System Performance project. In addition, a follow-on Malaria Booster operation is being developed to continue critical support in the Bank’s area of comparative advantage (especially strategic program management capacity building, and health systems strengthening). (See also section on Risk to Development Outcome.)
13
3. Assessment of Outcomes
Relevance of Objectives, Design and Implementation (to current country and global priorities, and
Bank Assistance Strategy)
Relevance of Objectives and Design: High
39. The project is highly relevant to the country’s development objectives, global priorities and the Bank’s Assistance Strategy. With regard to the country’s development objectives, the GoB has recently articulated its development priorities and objectives in its new (March 2011) Poverty Reduction Strategy Paper. Two of the six pillars are of relevance to this project’s development objectives: Strengthening of Human Capital; and Improving the Quality of Governance. In the context of the first of these two pillars, GoB aims to improve the accessibility and quality of health services, highlighting the importance of making headway on three MDGs, all addressed in this project: under-five mortality rate; maternal mortality; and combating malaria, HIV/AIDS and tuberculosis. Malaria-specific interventions include: prevention, case management, behavior change communication, epidemiological and entomological surveillance and research. GoB’s 10-year National Health Sector Development Plan (PNDS 2009-2018) recognizes malaria as the main cause of child mortality and adult morbidity and calls for concerted action to combat this disease as a priority. The project was conceived to support the objectives of Benin’s second five-year malaria NSP (2006-2010), which, itself, supports the PNDS. The recently approved (September 2011) third five-year malaria NSP (2011-2015) supports the same objectives and is made up of the same components or interventions as the second plan, but with some refinements: (a) coverage will move beyond vulnerable target groups to cover the entire population; (b) private sector coverage and involvement will be more vigorously pursued; and (c) pharmaco-vigilence will also receive more attention.
40. Malaria is a global priority. RBM was formed to address malaria in recognition of (i) the high burden of disease it creates in Africa and in other regions of the world; and (ii) under-exploited opportunities to address it, given the proven technologies for its prevention and treatment.
41. The project is highly relevant to the Bank’s priorities and development objectives. Its Health, Nutrition and Population strategy aims to support to countries’ efforts to control priority diseases (malaria cited specifically) through health systems strengthening and a strong results focus. The Bank established the Malaria Booster Program to further stimulate its active involvement in RBM and to “boost” malaria efforts in Africa. Two of the three strategic objectives of the Bank’s current Country Assistance Strategy (January 30, 2009) are relevant to this project: Improving Access to Basic Services (with specific reference to malaria control); and Promoting Better Governance and Strengthening Institutional Capacities (including decentralization and community development). Key performance indicators and milestones for measuring CAS success are drawn directly from GoB’s malaria NSP (both the second and the current ones), which are also reflected in the project, focusing on access and coverage of key malaria interventions: LLIN utilization; case management/treatment; prophylactic treatment for pregnant women; essential malaria inputs; and capacity building. Relevance of Design
42. The design is highly relevant from a number of perspectives. First, the choice of interventions is highly appropriate, providing a sound, technically appropriate balance between case management/treatment and prevention. Case management/treatment interventions were designed to
14
reflect and support MoH’s new policy, grounded in WHO recommendations, to treat malaria cases with ACT (and to phase out chloroquine as a treatment option) and to test patients with malaria symptoms before treating them. Prevention interventions also support WHO recommendations and protocols, focusing on increasing the use of LLINs by two vulnerable groups (under fives and pregnant women) and on IPTp for pregnant women through mass distribution campaigns as well as routine services (vaccination and ANC). IEC, BCC and other ways and means of community outreach and involvement included in the project are also critical to the achievement of targets and objectives. The decision not to launch immediately under this project indoor residual spraying (IRS), larvae breeding control and other hygiene and sanitation initiatives, was a sound one. It shows appropriate selectivity of well-established results-oriented interventions that are already ambitious and within the mandate of MoH/PNLP to implement. Spraying, hygiene and sanitation activities were being piloted and supported by others and are known to be very complicated (involving multiple sectors and actors) and expensive (requiring frequent repeating of actions). 43. Second, the project (and the NSP it was supporting) was articulated around a well-established results chain (and appropriate indicators) that documented inputs (nets, drugs, tests, other critical supplies and equipment), outputs (persons trained, supervision protocols produced, radio messages diffused…), processes (regular planning, monitoring and evaluation, supervisions…), outcomes (access/use of preventive and treatment services) and impacts (trends in malaria mortality and morbidity) and the plausible links in the chain. These are well captured in the PAD’s results framework and in GoB’s M&E plan and strategy and are reflective of RBM and WHO logframes for malaria. Third, a strong M&E component helps maintain a results focus and builds capacity for strategic management of the program, including the finetuning of interventions and strategies as experience unfolds. (See also paras. 29-31 on M&E design, implementation, and use.) 44. Fourth, the institutional and implementation arrangements were based on two sound principles: (1) the placement of project management responsibility within the structure responsible for the program; and (2) the full use of the health system and its various actors for project implementation, rather than employing a more “vertical” approach. Instead of establishing a project management unit, PNLP was given overall responsibility for project management, supplemented only by a few specialized staff (procurement and financial management specialists and support staff). Component 4 supported PNLP capacity strengthening to this end, which extended to the DDS (which have malaria units) and to the health zones. The full use of health system actors emphasized that malaria control was to be acknowledged as the responsibility of the entire health system. In addition to PNLP, other MoH departments and entities were involved: DNSP, DPP, CAME and CPMP. Likewise the DDS were mobilized and made responsible beyond the specific technical responsibilities of their malaria units. At the operational and community levels, over and above the health zone actors, NGOs, local radio stations, community health workers and other community and local organizations and officials were also involved. Partnerships between the three levels of MoH (central level, six DDS, and 34 health zones), and between MoH and NGOs/radio stations, were established through performance-based contracts, which helped clarify roles and responsibilities, and kept a strong results focus, given that their bottom lines were about delivering on targets and indicators. (More detail on the contracts with NGOs in the procurement section). 45. Fifth, the project nurtured and supported strong partnerships with other development partners supporting Benin’s malaria efforts. This was particularly evident in the M&E efforts, which coordinated the technical and financial support of all partners, in an effort to ensure one M&E framework and system – the Government’s – that all partners would rely upon. It was also
15
reflected in a covenant in the legal agreement that called for joint annual malaria reviews conducted with donor partners and stakeholders along with an integrated budgeted plan for the following year, in light of accomplishments, challenges, and available technical and financial support.
Achievement of Project Development Objectives (including brief discussion of causal linkages
between outputs and outcomes, with details on outputs in Annex 4)
Rating: Substantial
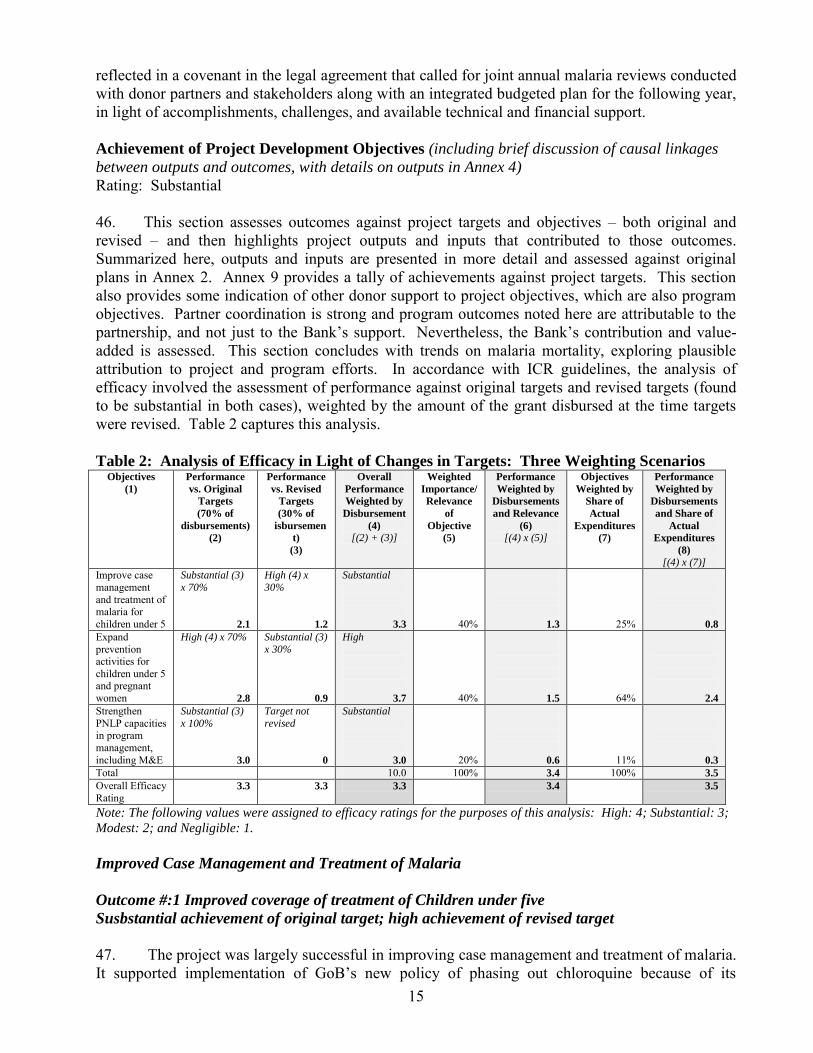
46. This section assesses outcomes against project targets and objectives – both original and revised – and then highlights project outputs and inputs that contributed to those outcomes. Summarized here, outputs and inputs are presented in more detail and assessed against original plans in Annex 2. Annex 9 provides a tally of achievements against project targets. This section also provides some indication of other donor support to project objectives, which are also program objectives. Partner coordination is strong and program outcomes noted here are attributable to the partnership, and not just to the Bank’s support. Nevertheless, the Bank’s contribution and value-added is assessed. This section concludes with trends on malaria mortality, exploring plausible attribution to project and program efforts. In accordance with ICR guidelines, the analysis of efficacy involved the assessment of performance against original targets and revised targets (found to be substantial in both cases), weighted by the amount of the grant disbursed at the time targets were revised. Table 2 captures this analysis.
Table 2: Analysis of Efficacy in Light of Changes in Targets: Three Weighting Scenarios Objectives
(1)
Performance
vs. Original
Targets
(70% of
disbursements)
(2)
Performance
vs. Revised
Targets
(30% of
isbursemen
t)
(3)
Overall
Performance
Weighted by
Disbursement
(4)
[(2) + (3)]
Weighted
Importance/
Relevance
of
Objective
(5)
Performance
Weighted by
Disbursements
and Relevance
(6)
[(4) x (5)]
Objectives
Weighted by
Share of
Actual
Expenditures
(7)
Performance
Weighted by
Disbursements
and Share of
Actual
Expenditures
(8)
[(4) x (7)]
Improve case management and treatment of malaria for children under 5
Substantial (3)
x 70%
2.1
High (4) x
30%
1.2
Substantial
3.3
40%
1.3
25%
0.8
Expand prevention activities for children under 5 and pregnant women
High (4) x 70%
2.8
Substantial (3)
x 30%
0.9
High
3.7
40%
1.5
64%
2.4
Strengthen PNLP capacities in program management, including M&E
Substantial (3)
x 100%
3.0
Target not
revised
0
Substantial
3.0
20%
0.6
11%
0.3
Total 10.0 100% 3.4 100% 3.5
Overall Efficacy Rating
3.3 3.3 3.3 3.4 3.5
Note: The following values were assigned to efficacy ratings for the purposes of this analysis: High: 4; Substantial: 3;
Modest: 2; and Negligible: 1.
Improved Case Management and Treatment of Malaria
Outcome #:1 Improved coverage of treatment of Children under five
Susbstantial achievement of original target; high achievement of revised target
47. The project was largely successful in improving case management and treatment of malaria. It supported implementation of GoB’s new policy of phasing out chloroquine because of its
16
increasing inefficacy and phasing in the use of ACTs for the treatment of malaria. The project achieved its objective of increasing the proportion of children under five with a fever that are treated with an effective anti-malarial within 24 hours from the onset of symptoms. By the project’s end, the proportion of children presenting themselves at the community level with fever and receiving effective treatment was 47 percent,8 exceeding the revised (April 2010) target of 30 percent, and almost achieving the original target of 50 percent. The proportion of children presenting themselves at health centers with fever and receiving effective treatment was 95 percent.9 It should be pointed out that the baseline provided in DHS 2006 (25%) is misleading for the purposes of this evaluation. In 2006 chloroquine was considered to be an effective treatment. But under MoH’s new policy and strategy, and as envisioned in the project, effective treatment is defined as ACT. It is more accurate then to define the baseline as 0, as ACT had not been introduced before the start of the project. A Health Facility Survey conducted in November/December 2009 raised some issues of service quality. While it was conducted only one year after inputs and training were provided, and a year and a half before the project’s end – and therefore cannot be taken as end-of-project status – it is worth noting, even though improvements may have been made in the meantime. Adherence to national policy on prescription of anti-malarials was 88 percent.10 This Survey also documented some shortcomings in testing. Less than half (41%) of health centers were able to perform malaria testing by microscopy or rapid diagnostics test (RDT), but all hospitals could perform testing. Adherence to the national policy on testing (confirming diagnosis before treating) was 53 percent (all patients), 25 percent (children under five) and 70 percent (over five). Policy and training on testing were found to be somewhat ambiguous, especially for children under five. Confirmation of diagnosis using RDTs at the community level is currently not required. 48. Project Outputs. Substantial numbers of public health workers were trained in improved case management, covering the new malaria policy, the proper and routine diagnosis, and the correct utilization of ACTs. In total, some 10,000 health workers received this training. Specifics included: 85 Level A lab technicians (vs. 90 planned); 90 Level B lab technicians (vs. 140 planned); 1,997 health providers (doctors, nurses, midwives) in referral hospitals (considerably more than the 275 planned); 166 doctors at the health zone level (less than 430 planned); 2,526 health workers (of a total of 3,373), exceeding the 2,363 target; and 3,581 (of a total of 3,682) non qualified health workers, exceeding the 1,781 target. Most of this training occurred in 2008 and 2009, and was followed up by regular, semi-annual supervision by central PNLP to the DDS level. Supervisions by the DDS to the health zones, by the health zones to the health centers, and by health centers to the community level were carried out less regularly than planned. Training guides, materials and supervision protocols were developed to support these activities. While the project (and other donor financing) provided substantial supplies of essential inputs, the Health Facility Survey (2009) documented that 33 percent of health centers had stockouts of ACTs for at least three days.
8 PNLP Performance Review, April 2011. The 2010 MIS documented a coverage of 25 percent. The difference between these two levels is due to two factors. First, the MIS exercise was carried out during a period of severe nationwide flooding at a time where many communities already benefiting from community-based treatment interventions were inaccessible (both to survey staff as well as to some community health workers). Second, after the MIS exercise, in December 2010, community-based treatment was extended to numerous other communities with the support of Africare.
9 Ibid.
10 Nearly all patients who tested positive were given an antimalarial. However, 22 percent of those testing negative were given an antimalarial.
17
According to the PNLP Performance Review Report (April 2011), 88 percent of health facilities reported no ruptures in ACTs of more than one week, during the previous three months, and 79 percent reported no ruptures in RDTs of more than one week, during the previous three months. Training of private sector was not carried out, as this sector was supported in part by other partners.
49. Project Inputs. Over the four-year implementation period the project acquired and distributed a total of 25.3 million ACT treatments. These drugs were first made available in mid-2008 to all public health facilities in all 34 health zones and all 12 departments in the country through CAME and its three regional depots. The project also procured rapid diagnosis tests (RDTs) for all health facilities and microscopes and related laboratory supplies and materials to 9 health facilities (National University Hospital, three zonal hospitals and five health centers) and to the PNLP. Additionally, the project provided in 2009 64,244 A Kits and 49,799 B kits for the management of serious malaria cases in children under the age of 5. 50. Other Donor Support. While the Bank was the first to supply Benin with ACTs, other donors also provided substantial amounts of ACTs, most notably: USAID/PMI, GFTAM, and (to a lesser extent) UNICEF. GoB also financed modest amounts. In addition, USAID/PMI provided substantial systems support and capacity building to CAME and to MoH/PNLP at all levels of the system to strengthen the management of inputs, stocking and distribution. Since the health facilities survey, several changes have been made to the drug supply chain management system. A commodity logistics system was designed and a computerized tool for commodities/logistics data management is used in 29/34 health zones (May 2011). The Central Medical stores (CAME) elected and trained a new board of directors and signed a new convention with PMI support. With PMI TA, software was installed and calibrated in central and regional warehouses. Still the availability of key commodities (antimalarials and diagnostic testing supplies) should be monitored and stock-outs should be eliminated. Some donors, especially GFATM, also supported the establishment, training and backstopping of community malaria workers (relais communautaires), who played a key role in treating malaria cases at the community level and promoting prevention knowledge and behavior change. Other partners, notably the Bank and UNICEF, supported relais
communautaires, but only on the prevention/promotion front. Outcome #2: Improved Protection of Pregnant Women against Malaria
Substantial achievement of original (unchanged) target
51. The project substantially achieved its objective of improving the protection of pregnant women against malaria. From a baseline of 3 percent (2006 DHS), 47 percent of pregnant women received two or more doses of IPTp (PNLP Performance Review, April 2011), closely approaching the target of 50 percent. The 2010 MIS (which records an overall level of 46 percent) documents important discrepancies across departments, however. Zou-Collines had the highest level of IPT coverage (61 percent) and Atacora and Donga had the lowest level (31 percent). Additionally, there is a gap of 10 percentage points between urban and rural areas (52 and 42 percent, respectively). But the gap between the richest and poorest quintiles is small (51 and 46, percent respectively). The Health Facility Survey (November/December 2009) documented that 54 percent of eligible pregnant women were given SP. Of the 94 pregnant women not eligible, 81 percent were not given the drug. This translates into an overall adherence to national policy on IPTp of 66 percent. 52. Project Outputs. Doctors, midwives and nurses (itemized in the previous outputs paragraph) were trained in the IPTp policy and how to implement it. As is noted previously, PNLP supervision of DDS was regular (and included this aspect of service delivery), but other supervisions (DDS to zones, zones to health centers, and health centers to community level) were
18
less regular. Ninety percent of health facilities reported no ruptures in SP stocks that exceeded one week, during the previous three months (PNLP Performance Review, April 2011). 53. Project Inputs. The Bank procured 593,400 doses of Sulfadoxine/Pyrimethamine (SP) in support of this activity, or 74 percent of the 800,000 doses initially planned. 54. Other Donors. PMI provided an additional 1.1 million units of SP during the period 2008-2010.
Outcome #3: Improved Bednet Access and Use by Target Groups
High achievement of original targets; substantial achievement of revised targets
55. The use of LLINs by the two target groups increased substantially during the life of the project, with targets fully achieved. The proportion of children under 5 who slept under a LLIN in the night preceding the survey increased from a baseline of 20 percent (2006 DHS) to a level of 64 percent in 2010 (MIS, 2010). This level exceeded the original target of 50 percent and fully achieved the adjusted target of 60 percent (adjusted in light of the MTR level of achievement: 56 percent). 56. Likewise, the proportion of pregnant women who slept under a LLIN in the night preceding the survey increased from a baseline of 20 percent (2006 DHS) to a level of 60 percent in 2010 (MIS 2010). This level also exceeded the original target of 50 percent and fully achieved the adjusted target of 60 percent (adjusted in light of the MTR level of achievement: 55 percent). However, the MIS does document disparities in achievements across departments. Zou-Collines achieved the highest levels of bednet use: 80 percent of children under five; and 70 percent of pregnant women, while Oueme/Plateau registered the lowest levels of 54 and 41 percent, respectively.11 Notwithstanding these variations across departments, urban rural differences in LLIN use (69 vs. 62 percent for children under five; and 64 vs. 57 for pregnant women) and differences between highest and lowest wealth quintiles (75 vs. 64 percent for children under five; and 68 vs. 57 percent for pregnant women) were smaller than those documented in the 2006 DHS, indicating improvements in equity.12 57. Project Outputs. The percentage of households possessing at least one LLIN was documented at 40 percent in 2010 (MIS, 2010), but increased to 74 percent when it was measured again, after the 2011 mass campaign. This represents a substantial increase over the baseline of 25 percent (DHS 2006), and demonstrates full achievement of the (revised) 70 percent target. The 2010 MIS also revealed that 87 percent of those households possessing LLINs reported that they were indeed hanging properly, an indication of the high utilization of existing nets. Rural households reported an even higher level of properly hung bednets (91 percent) than urban households (83 percent). Likewise, the poorest quintile reported a higher level (91 percent) than the
11 It is interesting to note, however, that the ranking of regions has changed from the time of the 2006 DHS to the 2010 MIS. In 2006 Zou-Collines was the fourth best performer for under-five LLIN use (at 25 percent), and rose to the number one position by 2010, while Oueme ranked first on this indicator in 2006 (at 31 percent) but did not increase at pace with other departments. Likewise, in 2006 Zou-Collines was a middle performer on use of LLINs by pregnant women (at 21 percent) and Oueme ranked first on this indicator (at 29 percent). But Zou-Colline’s improvements outpaced those of Oueme by 2010.
12 In 2006, LLIN use by children under five was 25 percent in urban areas and 17 percent in rural areas; and LLIN use by pregnant women was also 25 percent in urban areas and 17 percent in rural areas. The 2006 DHS documents large differentials in LLIN use by the highest and lowest wealth quintiles: 34 vs. 9 percent for children under five; and 29 vs. 9 percent for pregnant women.
19
richest (85 percent). There were discrepancies in levels across departments (95 percent in Atacora/Donga; and 73 percent in Atlantique/Littoral), but even the lowest level was substantial. Availability of bednets and their effective use by target groups are attributable to the large-scale promotion and distribution of LLINs supported by the project. Key outputs included the conduct of two mass distribution campaigns (one in 2007 to which the project provided 1.4 million LLINs or 84 percent of all nets distributed; and one in 2011 to which the project provided 1.7 million LLINs), including training of supervisors and distributors, logistics/transport of LLINs to villages, supervision, monitoring and evaluation of operations; the design and diffusion of sensitization (IEC) tools and audiovisual productions; design and diffusion of tailor-made radio productions through contracts with local radio stations. In the end, all 3,737 villages of Benin received LLINs. Another key output is the facility-based, routine distribution of LLINs to target populations: children under five at the time of measles vaccination; and pregnant women during ante-natal visits. The project prepared guidelines and supported the training of a range of actors to this end. 58. PNLP strengthened partnerships with communities, with NGOs covering each one of the country’s 34 health zones. Contracted NGOs worked to increase the knowledge of communities about how malaria is contracted and to encourage behaviors for its prevention. Thirty-three contracts were signed in 2007 between NGOs and each health zone, and most were renewed in 2009, on the basis of good performance. Two were not renewed, because of unsatisfactory performance and replaced by better performing ones. Contracts with local radio stations supported the design and dissemination of radio spots and shows aimed at information and behavior change, and radio call-in shows that assessed communities’ knowledge and understanding of the causes of malaria and ways to treat and prevent it. National Malaria Day events took place in Dassa (2008), Lokossa (2009) and Cotonou (2010). 59. Project Inputs. The project provided 1.4 million LLINs for the 2007 mass campaign, 86 percent of all nets distributed during that campaign. It supported the second (2011) campaign with 1.7 million LLINs. Total LLINs acquired under the project exceeded the initial target of 2.2 million. The project made LLINs available for routine distribution to pregnant women through ANC services, initially through the use of the stock left over from the 2007 mass campaign. The project subsequently procured 475,000 additional LLINs to ensure continued supply of nets for this service, but there were delays in their availability. PMI provided nets for ANC services, and the 475,000 nets purchased by the project were ultimately used to fill the gap in available LLINs for the 2011 mass campaign. 60. Other Donor Support. The PMI financed the LLINs needed to cover their routine distribution to children under five vaccinated for measles and, as noted above, provided nets for ANC services when project nets availability was delayed. In total PMI provided about 1.4 million LLINs between 2008 and 2010. PADS also provided about 0.2 million during this time period and UNICEF about 40,000 (PNLP Performance Review, April 2011). GFATM was also heavily involved in the 2011 mass campaign. Outcome #4: Strengthened M&E and Program Management Capacity
Sustantial achievement of original (unchanged) objective
61. The project achieved its objectives of strengthening M&E and strategic management capacity of Benin’s malaria program. These achievements, expressed in terms of outputs and outcomes, are noted below.
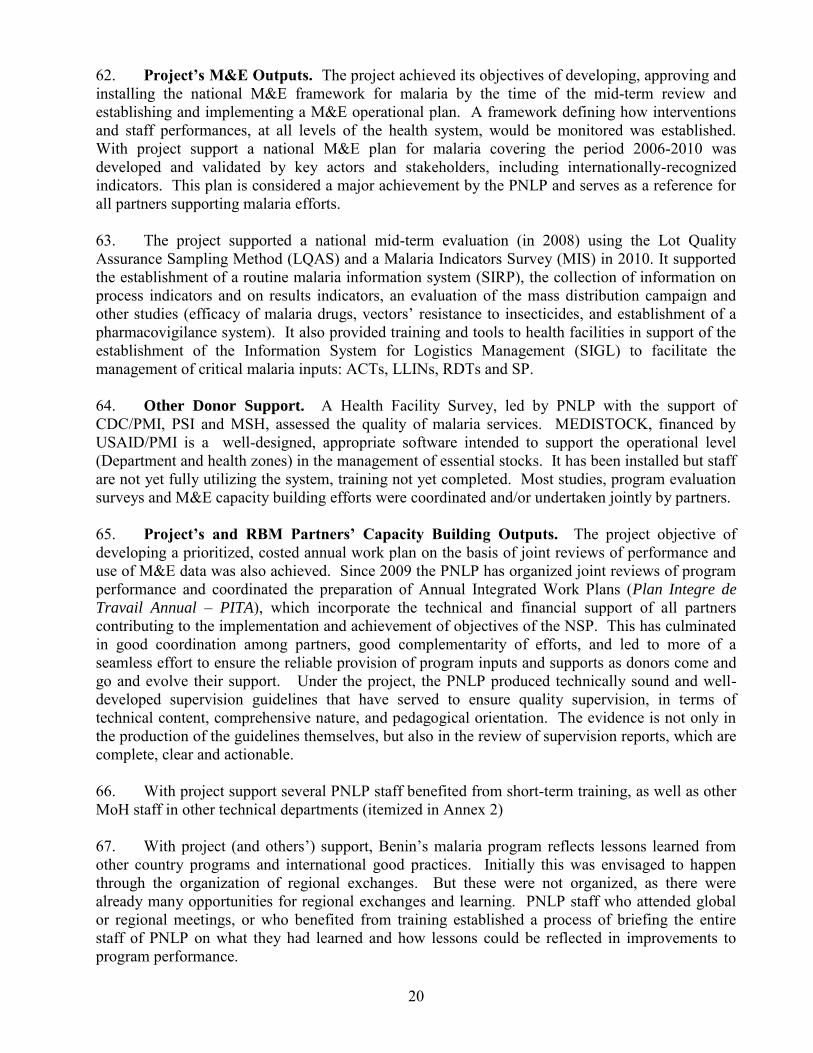
20
62. Project’s M&E Outputs. The project achieved its objectives of developing, approving and installing the national M&E framework for malaria by the time of the mid-term review and establishing and implementing a M&E operational plan. A framework defining how interventions and staff performances, at all levels of the health system, would be monitored was established. With project support a national M&E plan for malaria covering the period 2006-2010 was developed and validated by key actors and stakeholders, including internationally-recognized indicators. This plan is considered a major achievement by the PNLP and serves as a reference for all partners supporting malaria efforts.
63. The project supported a national mid-term evaluation (in 2008) using the Lot Quality Assurance Sampling Method (LQAS) and a Malaria Indicators Survey (MIS) in 2010. It supported the establishment of a routine malaria information system (SIRP), the collection of information on process indicators and on results indicators, an evaluation of the mass distribution campaign and other studies (efficacy of malaria drugs, vectors’ resistance to insecticides, and establishment of a pharmacovigilance system). It also provided training and tools to health facilities in support of the establishment of the Information System for Logistics Management (SIGL) to facilitate the management of critical malaria inputs: ACTs, LLINs, RDTs and SP.
64. Other Donor Support. A Health Facility Survey, led by PNLP with the support of CDC/PMI, PSI and MSH, assessed the quality of malaria services. MEDISTOCK, financed by USAID/PMI is a well-designed, appropriate software intended to support the operational level (Department and health zones) in the management of essential stocks. It has been installed but staff are not yet fully utilizing the system, training not yet completed. Most studies, program evaluation surveys and M&E capacity building efforts were coordinated and/or undertaken jointly by partners.
65. Project’s and RBM Partners’ Capacity Building Outputs. The project objective of developing a prioritized, costed annual work plan on the basis of joint reviews of performance and use of M&E data was also achieved. Since 2009 the PNLP has organized joint reviews of program performance and coordinated the preparation of Annual Integrated Work Plans (Plan Integre de
Travail Annual Ŕ PITA), which incorporate the technical and financial support of all partners contributing to the implementation and achievement of objectives of the NSP. This has culminated in good coordination among partners, good complementarity of efforts, and led to more of a seamless effort to ensure the reliable provision of program inputs and supports as donors come and go and evolve their support. Under the project, the PNLP produced technically sound and well-developed supervision guidelines that have served to ensure quality supervision, in terms of technical content, comprehensive nature, and pedagogical orientation. The evidence is not only in the production of the guidelines themselves, but also in the review of supervision reports, which are complete, clear and actionable.
66. With project support several PNLP staff benefited from short-term training, as well as other MoH staff in other technical departments (itemized in Annex 2)
67. With project (and others’) support, Benin’s malaria program reflects lessons learned from other country programs and international good practices. Initially this was envisaged to happen through the organization of regional exchanges. But these were not organized, as there were already many opportunities for regional exchanges and learning. PNLP staff who attended global or regional meetings, or who benefited from training established a process of briefing the entire staff of PNLP on what they had learned and how lessons could be reflected in improvements to program performance.
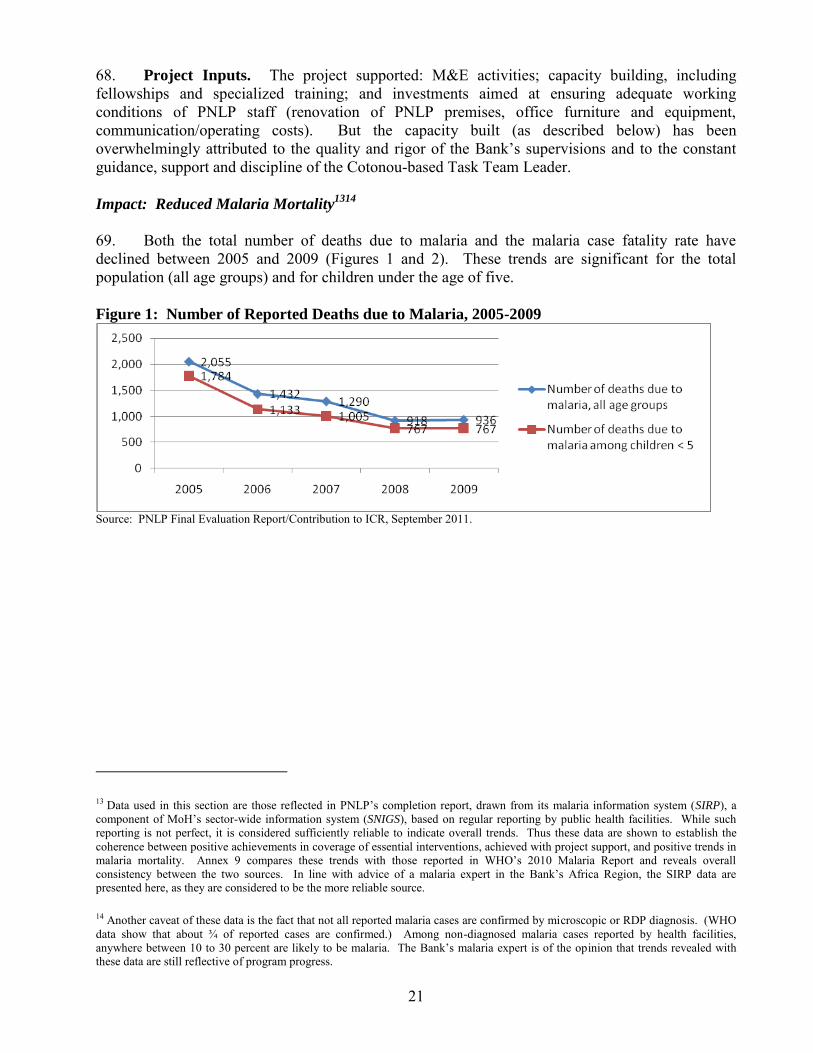
21
68. Project Inputs. The project supported: M&E activities; capacity building, including fellowships and specialized training; and investments aimed at ensuring adequate working conditions of PNLP staff (renovation of PNLP premises, office furniture and equipment, communication/operating costs). But the capacity built (as described below) has been overwhelmingly attributed to the quality and rigor of the Bank’s supervisions and to the constant guidance, support and discipline of the Cotonou-based Task Team Leader.
Impact: Reduced Malaria Mortality1314
69. Both the total number of deaths due to malaria and the malaria case fatality rate have declined between 2005 and 2009 (Figures 1 and 2). These trends are significant for the total population (all age groups) and for children under the age of five. Figure 1: Number of Reported Deaths due to Malaria, 2005-2009
Source: PNLP Final Evaluation Report/Contribution to ICR, September 2011.
13 Data used in this section are those reflected in PNLP’s completion report, drawn from its malaria information system (SIRP), a component of MoH’s sector-wide information system (SNIGS), based on regular reporting by public health facilities. While such reporting is not perfect, it is considered sufficiently reliable to indicate overall trends. Thus these data are shown to establish the coherence between positive achievements in coverage of essential interventions, achieved with project support, and positive trends in malaria mortality. Annex 9 compares these trends with those reported in WHO’s 2010 Malaria Report and reveals overall consistency between the two sources. In line with advice of a malaria expert in the Bank’s Africa Region, the SIRP data are presented here, as they are considered to be the more reliable source.
14 Another caveat of these data is the fact that not all reported malaria cases are confirmed by microscopic or RDP diagnosis. (WHO data show that about ¾ of reported cases are confirmed.) Among non-diagnosed malaria cases reported by health facilities, anywhere between 10 to 30 percent are likely to be malaria. The Bank’s malaria expert is of the opinion that trends revealed with these data are still reflective of program progress.
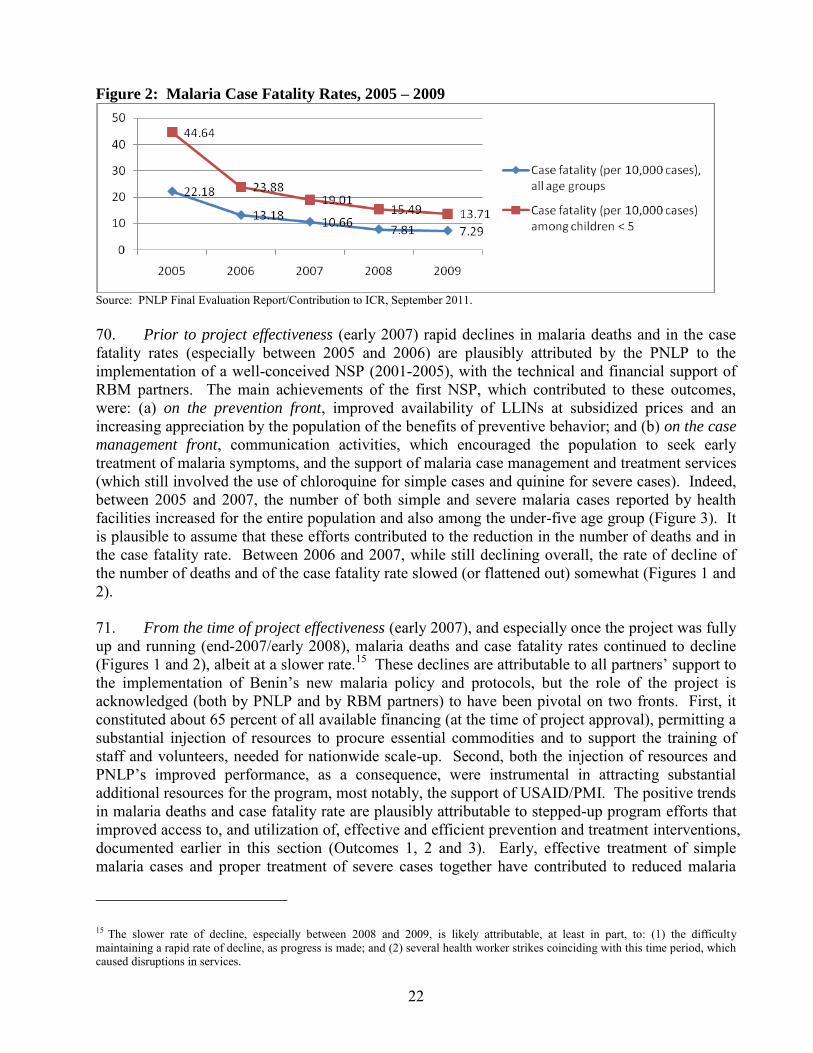
22
Figure 2: Malaria Case Fatality Rates, 2005 – 2009
Source: PNLP Final Evaluation Report/Contribution to ICR, September 2011. 70. Prior to project effectiveness (early 2007) rapid declines in malaria deaths and in the case fatality rates (especially between 2005 and 2006) are plausibly attributed by the PNLP to the implementation of a well-conceived NSP (2001-2005), with the technical and financial support of RBM partners. The main achievements of the first NSP, which contributed to these outcomes, were: (a) on the prevention front, improved availability of LLINs at subsidized prices and an increasing appreciation by the population of the benefits of preventive behavior; and (b) on the case
management front, communication activities, which encouraged the population to seek early treatment of malaria symptoms, and the support of malaria case management and treatment services (which still involved the use of chloroquine for simple cases and quinine for severe cases). Indeed, between 2005 and 2007, the number of both simple and severe malaria cases reported by health facilities increased for the entire population and also among the under-five age group (Figure 3). It is plausible to assume that these efforts contributed to the reduction in the number of deaths and in the case fatality rate. Between 2006 and 2007, while still declining overall, the rate of decline of the number of deaths and of the case fatality rate slowed (or flattened out) somewhat (Figures 1 and 2).
71. From the time of project effectiveness (early 2007), and especially once the project was fully up and running (end-2007/early 2008), malaria deaths and case fatality rates continued to decline (Figures 1 and 2), albeit at a slower rate.15 These declines are attributable to all partners’ support to the implementation of Benin’s new malaria policy and protocols, but the role of the project is acknowledged (both by PNLP and by RBM partners) to have been pivotal on two fronts. First, it constituted about 65 percent of all available financing (at the time of project approval), permitting a substantial injection of resources to procure essential commodities and to support the training of staff and volunteers, needed for nationwide scale-up. Second, both the injection of resources and PNLP’s improved performance, as a consequence, were instrumental in attracting substantial additional resources for the program, most notably, the support of USAID/PMI. The positive trends in malaria deaths and case fatality rate are plausibly attributable to stepped-up program efforts that improved access to, and utilization of, effective and efficient prevention and treatment interventions, documented earlier in this section (Outcomes 1, 2 and 3). Early, effective treatment of simple malaria cases and proper treatment of severe cases together have contributed to reduced malaria
15 The slower rate of decline, especially between 2008 and 2009, is likely attributable, at least in part, to: (1) the difficulty maintaining a rapid rate of decline, as progress is made; and (2) several health worker strikes coinciding with this time period, which caused disruptions in services.
23
mortality. From a pre-project (2006) baseline of 365,852, the annual number of simple malaria cases in children under 5 reported by public health facilities increased by 30 percent to 482,669 in 2009. Concurrently, the number of severe malaria cases among children under 5 reported by health facilities declined by 30 percent percent (from 108,576 in 2006 to 76,493 in 2009). These data corroborate patterns of observations from program staff, health workers and civil society/communities that increased, early treatment of malaria cases has reduced the number of severe cases.
Figure 3: Number of Simple and Severe Malaria Cases Reported by Health Facilities, 2005-
2009
Source: PNLP Final Evaluation Report/Contribution to ICR, September 2011. Efficiency (net present value/economic rate of return, cost effectiveness, e.g., unit rate norms, least
cost, and comparisons; and financial rate of return)
Rating: Substantial 72. The project was efficient on a number of fronts. It prioritizes and supports (as does Benin’s malaria strategy) the most cost-effective interventions for malaria control, identified by WHO, in a stable endemic malaria area, such as Benin: (a) prevention through (i) the use of LLINs by children under five and pregnant women; and (ii) the provision of IPTp to women during pregnancy; and (b) case management through effective treatment in a health facility and home management, where appropriate.16 The phasing out of chloroquine, documented to be no longer effective in Benin, and the use of ACTs also assures more effective treatment and more efficient employment of funds and efforts. WHO’s strategy also identifies indoor residual spraying as another intervention, in a stable endemic malaria area, “where appropriate.” GoB considers this strategy to be complementary to its core strategy of LLINs.17
16 In 2005 WHO’s definition of effective case management (noted in the 2006 PAD) was presumptive treatment for suspected cases. It has recently changed this definition to the treatment (in facilities) of cases confirmed by laboratory or rapid testing. Benin is also evolving its strategy and action in this sense.
17 The PAD notes that in 2006 GoB opted not to include this intervention nationwide because of its concerns about the harmful effects of pesticides..
24
73. The strong coordination among all Benin’s malaria partners permitted a more effective and efficient use of their technical and financial support, including: regular coordination meetings; joint reviews and joint planning on an annual basis; implementation of joint activities (2011 mass campaign and M&E/research support, being two cases in point). It was also efficient to integrate the malaria information system into MoH’s sector-wide SNIGS. The reliance on the health system to carry out malaria interventions avoided the creation of parallel efforts and structures, examples being the distribution of LLINs to target groups through regular health services (measles vaccination and ANC). The development and management of performance-based contracts with clear performance indicators between central-level PNLP and the Departments and health zones for the implementation of malaria interventions clarified roles and responsibilities and encouraged a strong results focus that stakeholders note has contributed to their productivity. The contracts between PNLP and health zones were also signed by Departments, thus strengthening their oversight and support functions, as well as their authority. The decentralization of malaria efforts ensured a stronger link with the community, whose knowledge and behaviors were crucial to the project’s success. The role of NGOs and community malaria workers were pivotal. 74. While reliance on the health system is a strong feature of this disease-specific project’s design and implementation, it also risks some inefficiencies in activities and approaches supporting project objectives, because the health system is in need of considerable strengthening. While improving, the distribution of commodities and the management of these stocks are in need of further strengthening. There are still some stockouts of commodities reported and some reported leakages. But it is significant to note that the project was more efficient than the overall program in terms of the management, availability and use of essential commodities. The Bank was the first RBM partner to provide ACTs to Benin in support of the implementation of its new treatment protocol. And the Bank financed almost all of the LLINs for the first (2007) mass campaign. Subsequent stockouts of malaria commodities are attributed to GoB and other donor-financed stocks that were delivered behind schedule. While there were leakages of drugs in the sector, an investigation commissioned by the Minister of Health and transmitted to the Bank by letter of July 2009 confirmed that the drugs that were being sold illicitly on the market were not those financed by the Bank. 75. The quality of basic health services is not yet adequate. Underlying this are issues associated with: irregular and uncoordinated supervisions of mixed quality; uncoordinated training and inadequate training follow-up; occasional staff strikes; inadequacies in staffing and human resources management; and inadequate operational budgets. These health system inefficiencies did have an effect on the efficiency of malaria project and program efforts. But the alternative of bypassing the health system and adopting a parallel approach would have been less efficient in the long run. Indeed, many informants (both GoB and RBM partners) observed that the project and program’s use of the health system had the effect of strengthening certain aspects of the health system. Indeed there was strong consensus that a continuation of this approach holds the potential for the malaria program to be the vehicle for health systems strengthening.
76. The size of the PNLP staff at central level and the special malaria cells at the Departmental level have been instrumental in the successful implementation of the intensified effort warranted under the malaria strategy. But some in MoH are questioning the efficiency of the size of these staffs and point to the opportunity for their consolidation and further integration. While successful malaria control requires the involvement and support of other departments and divisions in MoH, not all of them are reported to have provided adequate support or felt particularly accountable for
25
supporting malaria activities and outcomes. These shortcomings to efficiency are classified as minor.
Justification of Overall Outcome Rating (combining relevance, achievement of PDOs, and
efficiency)
77. High relevance, substantial efficacy18 and substantial efficiency culminate in an overall rating of satisfactory. On the advice of the World Bank’s Operations Policy and Country ServicesVice-Presidency (OPCS), a moderately satisfactory rating was assigned to the project’s development outcome rating on the final Implementation Status Report (ISR). Even though available trend data gave indication that the project targets and objectives were likely to be achieved, the end-of-project data were in the process of being collected and so the final evidence was not available for this ISR. Overarching Themes, Other Outcomes and Impacts (if any, where not previously covered or to
amplify discussion above)
78. Poverty Impacts, Gender Aspects, and Social Development. The PDOs were articulated around two groups known to be most vulnerable to malaria morbidity and mortality: children under the age of five and pregnant women. Prevention and treatment objectives aimed at these two target groups were achieved. Thanks to successful safeguard compliance, there were no negative effects on Benin’s population.
79. The malaria burden falls disproportionately on the poor population who are at increased risk of being infected more frequently and less likely to access care when confronting severe malaria episodes. PNLP analysis reveals that the gaps across income groups in access to both treatment and prevention have closed during the time of project and program implementation. (Data cited in Efficacy section.)
80. It is probable that benefits leaked beyond the project’s target group. There is strong demand for LLINs beyond these target groups. Indeed, Benin’s new malaria strategy (2011-2015) has broadened its prevention and treatment targets to encompass Benin’s entire population.
Institutional Change/Strengthening (particularly with reference to impacts on longer-term
capacity and institutional development).
81. Institutional strengthening was significant, and largely attributable to the Bank’s efforts. First, it was significant that the Bank’s project was placed under the overall responsibility of the PNLP. This design supported a learning-by-doing process that enabled the staff to take on its line management responsibilities of overall strategic management and oversight and improve along the way. Second, the Bank was noted to be very rigorous in its interactions with the PNLP, both through supervision missions and through regular contact and exchanges made possible by the task team leader’s Benin base. The task team leader had high expectations and insisted on rigor and excellent performance. While this proved difficult for PNLP staff at the project’s outset, it was reported by all, including those at decentralized levels, that this process built capacity as no other
18 Efficacy was rated substantial, both against original targets and against revised targets. See Table 2 for details.
26
had done before, on a number of fronts: M&E and use of data for decision-making; financial management; strategic management; and aid coordination.
82. Other Unintended Outcomes and Impacts (positive and negative). The utilization rates of two critical services – ANC and childhood vaccination – increased during the life of the project. These increases were attributable to the very strong demand for LLINs, generated by this project, and to their provision to clients as a part of these routine services.
Summary of Findings of Beneficiary Survey and/or Stakeholder Workshops (optional for Core
ICR, required for ILI, details in annexes)
83. A workshop of stakeholders and beneficiaries was held in Bohicon, Department of Zou-Collines on (September 28, 2011) during the ICR mission to allow these groups to share their views on the project’s performance. Three groups discussed and synthesized their opinions: beneficiaries/civil society; operational level service providers and managers; and central level MoH, including PNLP and other key MoH divisions involved. These findings are presented in Annex 6. In summary, there was remarkable consistency across the three groups on: the success of the project in achieving its objectives; the importance of its decentralized design and its ability to reach and affect communities; the appreciation of the World Bank’s rigor in supervising and guiding the project and in building capacity; and a concern about the sustainability of the achievements and activities supported under the project. This last point is taken up in the following section.
4. Assessment of Risk to Development Outcome Rating: Moderate 84. The maintenance and further improvement of this project’s (and program’s) development outcome will depend on a number of factors. On the technical front, the changes in Benin’s approach to malaria prevention (vigorous promotion of LLINs) and case management (replacement of chloroquine with ACTs) were not exclusive to this project. Rather they are encapsulated in Benin’s own malaria policy and strategy, and reflective of WHO recommendations. Thus they are likely to be sustained. On the financial front, there is concern that a declining national budget for health could undermine the implementation of activities essential to the continued coverage of high-risk groups with quality prevention and treatment interventions (not to mention the extended coverage of these interventions to all segments of the population, in line with Benin’s new strategy). This would include: continued prevention and treatment activities to influence the knowledge, behaviors and utilization of prevention and treatment interventions by new cohorts of vulnerable groups (involving the continued financing of inputs and activities of a range of implementers); and health systems strengthening to improve services quality, strengthen human resources management, development and supervision, improve commodities acquisition, distribution and management, and to ensure good operation and maintenance of buildings, vehicles and equipment. It would also include the support of essential operating costs for program management, including the costs of communications and of continued rigor and depth in M&E and research. While RBM partners are well equipped to cover some of these needs, especially commodities and some aspects of capacity building, others will need the adequate support of the national budget. 85. On the social front, there is strong awareness, support and appreciation of the efforts and results of this project on the part of civil society, including beneficiaries, local officials and community activists and groups (see stakeholders’ views presented in Annex 6), and a call for continued support. From an institutional perspective, considerable capacity for strategic program management has been built, with the Bank taking a lead role in coaching and supporting central-
27
and Departmental-level malaria staff and efforts, but informants and direct observation indicate that more of this type of effort is needed to consolidate gains and further strengthen institutions. Politically speaking, there is strong support at the highest levels of government for malaria efforts, a recent announcement of the Head of State that all malaria treatment services would be free to vulnerable groups, a case in point. This policy will need to be matched with the resources to enable its full implementation. On the environmental front, continued compliance with safeguards is likely, given GoB’s concern about the potential negative effects of insecticides. But this, too, will require light financing.
5. Assessment of Bank and Borrower Performance (relating to design, implementation and outcome issues) 5.1 Bank
(a) Bank Performance in Ensuring Quality at Entry (i.e., performance through lending phase)
Rating: Satisfactory 86. The above section (2) on “Project Preparation, Design and Quality at Entry” provides details demonstrating a strong quality at entry. They will be summarized here. The strategic relevance of the project was strong, as evidenced in the high relevance of both it objectives and design. A clear results framework and viable institutional arrangements enhanced the likelihood that project investments would culminate in the achievement of development objectives. Technical aspects of the project were grounded in WHO recommendations, endorsed and supported by other RBM partners, and reflected in Benin’s own malaria strategy. Fiduciary aspects were well prepared, based on thorough assessments of capacities in procurement and financial management; and capacity building arrangements and interventions were put into place to ensure readiness for implementation. Relevant safeguards were properly assessed and addressed in the project design. Institutional aspects were strong in that they: relied on the program line manager and staff; focused equally on the deconcentrated levels of the health system and clarified their own roles in project/program implementation; and understood the importance of community-based, demand-side interventions, appropriately assigning these to experienced NGOs that would work in the 34 health zones.
87. M&E design strengthened the results focus, emphasized the importance of its use for problem solving and decision-making, and envisaged the coordination and collaboration of all RBM partners on this front, as well as the integration of malaria M&E into the sector-wide M&E system. The risk assessment was candid, thorough and proposed risk mitigation appropriate. The Bank’s inputs and processes were solid, drawing on the expertise of a multi-disciplinary team and good collaboration with all RBM partners, including WHO as the technical leader.
88. This satisfactory rating is consistent with the QALP on this project, conducted in July 2010.
(b) Quality of Supervision (including of fiduciary and safeguards policies)
Rating: Satisfactory 89. The Bank’s supervision was strongly focused on the development impact. There was usually an M&E expert on the team. Much effort was placed on updating the baselines in light of new DHS data, and guiding/supporting a mid-term LQAS survey to provide indication of progress against outcome targets, and outcome targets were revised in light of both new data sets. Aide-
28
memoires and internal reporting kept the development outcomes in the forefront, and issues raised about delays or weaknesses in implementation were always addressed in light of their impact on achieving development outcomes. The Bank was candid and rigorous in assessing and addressing project management and coordination issues. In 2008 when project management suffered, a consequence of political changes and a change in the project coordinator, urgent actions brought resolution (the appointment of a capable project coordinator) quickly and effectively.
90. Supervision of fiduciary and safeguards aspects was also strong. Procurement missions and post reviews were carried out as scheduled and their findings reflected in the overall supervision reporting. The post procurement reviews reported various deficiencies in procurement handling by the PNLP/Unit and suggested appropriate mitigation measures such as recruitment of an additional procurement specialist and training. Supervision also reviewed the procurement plan and verified contract management by PNLP. Supervision of financial management focused on improving financial management capacity and performance. Mission reports were thorough and pro-active in identifying weaknesses (e.g., internal control) and agreeing action plans to address them. Proactive financial management supervision helped upgrade performance from Moderately Unsatisfactory to Satisfactory in the span of one year and maintain satisfactory performance throughout the rest of the project life. The Bank team closely supervised environmental safeguards aspects of the Project, provided detailed reports and recommendations in the Aide Memoires, and adjusted the ISR ratings to reflect compliance performance.
91. The task team leader’s performance was highly satisfactory. Informants (spanning central, departmental, and operational level staff) were consistent in recognizing the capacity building effects of: his close, pedagogical supervision, the candor and problem-solving orientation of the Aide-memoires, the rigor with which he assessed the performance and capacity of the PNLP and all implementing agencies, the high standards he set for them all, and the constant guidance he provided to them, which enabled them to improve. His success in strengthening capacity is also acknowledged in the Borrower’s ICR. He has also earned the high respect of all RBM partners, who recognize the comparative advantage he brought to the partnership, as well as the respectful, collaborative approach. There was also candor in internal reporting, which reflected a pro-activity in the oversight of this project. Both Government and partners noted their appreciation of the composition of Bank supervision teams, which were multi-disciplinary and responsive to current issues and constraints, as well as their reliance on (rather than duplication of) expertise available through the RBM partnership. WHO participation in every supervision mission undertaken during project implementation provides a good illustration. BB allocation ($80,000) was lower than for other projects because of the location of the TTL in the field. The allocation was supplemented with trust funds to provide additional expertise on missions, especially M&E.
92. This ICR’s assessment of supervision is consistent with the July 2010 QALP, which also rated it satisfactory. (c) Justification of Rating for Overall Bank Performance
Rating: Satisfactory 5.2 Borrower Performance
NOTE: When the government and implementing agency are indistinguishable, provide rating and
justification only for Overall Borrower Performance.
(a) Government Performance:
29
Rating: Moderately Unsatisfactory 93. Government ownership and commitment to this project were strong, given that (1) the social and economic toll of malaria on Benin’s population was well known and (2) a solid policy and multi-year strategy had been endorsed and adopted. Even the Head of State has spoken publicly about malaria as a priority and recently introduced a new policy of free malaria treatment for pregnant women and children. The Government consistently honored its counterpart obligations (annual provision of US$1.9 million equivalent to the PNLP). However, a significant shortcoming in Government performance was the failure to facilitate the efficient processing of procurements of essential commodities, critical to the launch of key project activities, both prevention- and treatment-related. The National Procurement Agency took months, instead of the 15-day turnaround standard, to approve procurements. MoEF also took months to sign key contracts, instead of the 15-day turnaround standard. These delays had important implications on implementation progress (See section on Major Factors Affecting Implementation.) (b) Implementing Agency or Agencies Performance:
Rating: Satisfactory 94. The PNLP was highly committed to the achievement of the project development objectives and this drove them to work hard and efficiently. The whole staff was devoted to the focus on, and involvement of, communities in project implementation; and the PNLP staff includes a sociologist, who devotes himself to ensuring that the project is centered on communities, that NGOs working with communities are performing in a satisfactory manner, that community malaria workers have what they need to perform their functions, that communities have inputs to the design of relevant IEC/BCC campaigns, and that benefits are indeed reaching the communities. The utilization of M&E data in decision-making by the PNLP has been robust. PNLP’s relationship with the development partners is solid. The Departmental-level malaria units appear to have implemented their responsibilities in line with the contractual obligations. Over and above joint annual reviews and joint planning events, PNLP and its partners meet on a monthly basis and coordinate and collaborate effectively, in line with comparative advantages of the various partners. Fiduciary performance was adequate, improving over time with close Bank supervision and guidance. 95. With regard to other implementing agencies, NGOs working at the zone levels performed well over all. A couple of NGOs that did not perform satisfactorily during the first two years of the project were not renewed. Their working relationships with the health zones improved in the second round of contracts when the local level was involved in their selection and health zones were responsible for validating NGO reports before their transmission to PNLP. CAME’s involvement in managing drug procurements, storage and distribution was satisfactory, and improved over time, especially once roles and responsibilities between PNLP, CAME and CPM were further clarified. Other MoH divisions, both technical and administrative, also collaborated with PNLP. But it has been noted that accountabilities for achieving malaria objectives are perceived to fall exclusively on the PNLP, which tempers other divisions’ support and involvement. Research institutions, contracted by PNLP to undertake studies, performed well. (c) Justification of Rating for Overall Borrower Performance
Rating: Moderately Satisfactory
6. Lessons Learned (both project-specific and of wide general application)
30
96. Rigor and candor in the Bank’s supervision can play a pivotal role in capacity building.
The task team leader’s presence in the field and his rigorous, pedagogical approach to accompanying and guiding the PNLP in strategic management and oversight of the project (and program) were consistently cited as being a critical factor of success in strengthening Benin’s capacity, and recognized as an important comparative advantage of the Bank. 97. Even within a single disease program, a sector-wide approach can achieve great synergies
and efficiencies in planning, financing, implementation, evaluation. The seamless coordination and collaboration among the RBM partners has culminated in a number of good practices and efficiencies. One example is the effort to undertake joint studies and evaluations. This has resulted in: efficiency in evaluation implementation (cost sharing); results that are accepted by all interested parties; and good data quality thanks to the use of international standards and protocols. Another example is the truly joint, collaborative nature of the second (2011) mass campaign, which involved the coordinated support of multiple partners, all working toward one set of objectives. Coordinated efforts to ensure a reliable supply of essential commodities is yet another example. Joint planning and reviews have helped underpin these synergies. 98. It is possible to support a single disease through a health systems approach. Disease control and health systems strengthening are not mutually exclusive. The malaria program has a clear, disease-specific set of inputs, activities, outputs and outcomes, but it relies on the health system for its implementation. This reliance on the health system (rather than opting for a more vertical, parallel approach) has caused inefficiencies and weaknesses in implementation. But all stakeholders agree that it has also provided – and continues to provide – a vehicle for health systems strengthening. This being said, failure to clarify that accountabilities for malaria
outcomes lie with the entire health system, and not just with the PNLP, can cause other MoH
departments to compromise the quality and quantity of their support to this end. 99. Quality of supervision depends in part on striking the right balance between depth and
breadth of supervision efforts. There is evidence and strong consensus that both the quantity and quality of supervision needs to be increased and that quality supervision requires the proper technical expertise. There is also ongoing debate about the need for integrated supervision. But a tension has emerged about how to reconcile a sufficiently in-depth, technically accurate disease focus with the philosophy of an integrated supervision. While integrated supervision makes sense from health systems and efficiency perspectives, it needs to be reconciled with the need to ensure (i) coverage of the breadth of malaria-specific activities and technical guidance (diagnosis, treatment, prevention..); and (ii) the involvement of malaria experts who are up to date on the latest protocols vs. generalists, who are not. 100. Community malaria workers were pivotal in the success of the malaria program. While not directly financed under the Bank’s project, these workers were the first point of contact of children under five suffering from malaria symptoms. Community-level treatment has enhanced the ability of the health system to treat children within 24 hours of the onset of symptoms and, according to health facility staff, contributed to a decline in severe cases. They have also been instrumental in encouraging LLIN use. Other donors and NGOs working on other diseases and health systems strengthening are depending increasingly on these same workers to deliver other services. MoH is challenged to establish a policy to manage this precious resource, both to ensure that the workload is manageable and to decide on fair and proper motivation of these workers. 7. Comments on Issues Raised by Borrower/Implementing Agencies/Partners
31
(a) Borrower/implementing agencies:
101. Annex 7 provides a summary of the Borrower’s ICR. The report was very well prepared, drawing on a strong evidence base. The overview of project design and assessment of its implementation and outcomes are fully consistent with the ICR. The Borrower’s evaluative comments are highlighted as follows. The project was found to have truly boosted the implementation of Benin’s national malaria policy. The role of the Bank was highly valued. The importance of maintaining and further strengthening gains made under this project is emphasized. The Bank’s continued technical and financial support is strongly solicited as GoB embarks on the implementation of its new NSP for 2011-2015. 102. PNLP has reviewed and endorsed the final draft of this ICR. (b) Cofinanciers:
103. The project was not formally cofinanced, but the PNLP and the project benefited from the close collaboration and coordination of the RBM partners. Annex 8 summarizes the views of the RBM partners on the project, who met as a group with the ICR mission in September 2011 to share their views. In short, they expressed strong consensus on three points: (1) the overall success of the project and, more broadly, of Benin’s national malaria program over the past five years; (2) concerns about the sustainability of achievements and the need for continued support, especially with regard to health systems strengthening; and (3) the value added of the strong coordination and collaboration among RBM partners and opportunities for continued and enhanced efforts to this end. (c) Other partners and stakeholders (e.g., NGOs/private sector/civil society):
104. A civil society subgroup, composed of elected officials, community representatives, community health workers, NGOs and local radio stations, synthesized their views on project achievements, remaining challenges and lessons. These views are captured in Annex 6 (Group A). In summary, this group has a strong (and accurate) appreciation of the project’s contribution and outcome and it points to the importance of continued efforts, both to consolidate and to extend gains. Challenges include: elimination of any stock-outs of essential commodities; remuneration of community malaria workers, perhaps through local initiatives/budgets; community mobilization to clean the environment; and strengthened supervision of community-level activities by health zones. It is noteworthy that this group appreciates the link between M&E and the achievement of results.
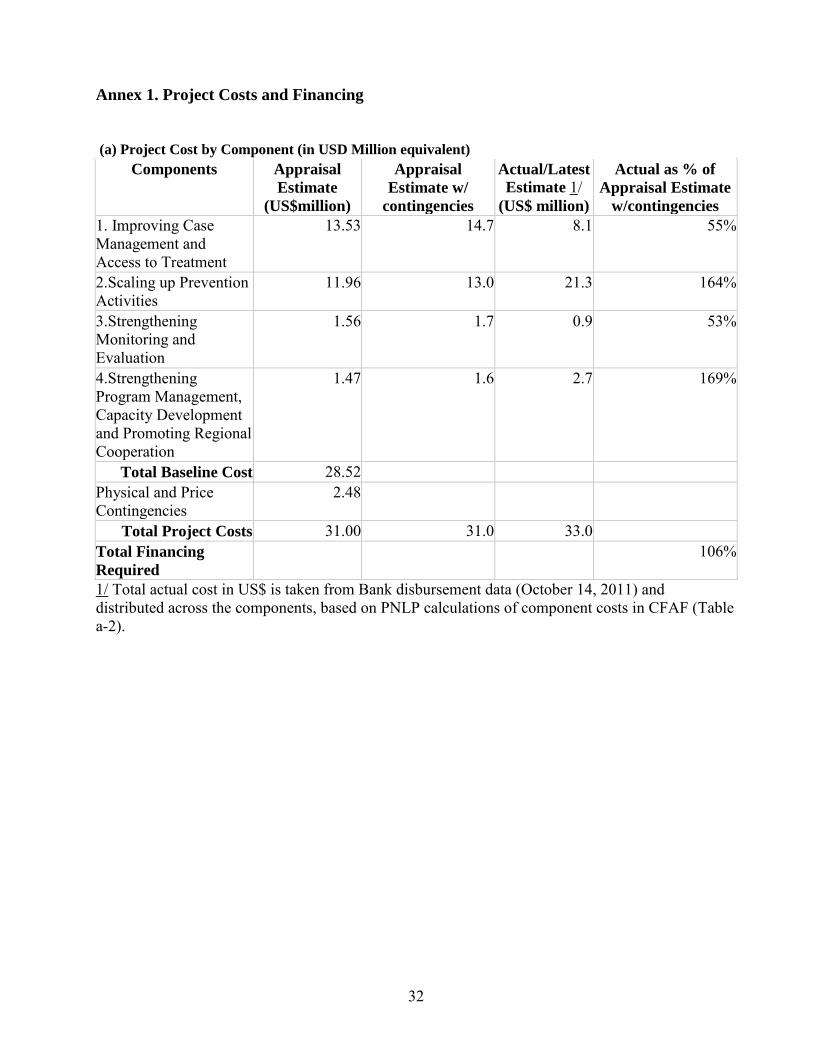
32
Annex 1. Project Costs and Financing
(a) Project Cost by Component (in USD Million equivalent)
Components Appraisal
Estimate
(US$million)
Appraisal
Estimate w/
contingencies
Actual/Latest
Estimate 1/ (US$ million)
Actual as % of
Appraisal Estimate
w/contingencies
1. Improving Case Management and Access to Treatment
13.53
14.7 8.1 55%
2.Scaling up Prevention Activities
11.96 13.0 21.3 164%
3.Strengthening Monitoring and Evaluation
1.56 1.7 0.9 53%
4.Strengthening Program Management, Capacity Development and Promoting Regional Cooperation
1.47 1.6 2.7 169%
Total Baseline Cost 28.52 Physical and Price Contingencies
2.48
Total Project Costs 31.00 31.0 33.0 Total Financing
Required 106%
1/ Total actual cost in US$ is taken from Bank disbursement data (October 14, 2011) and distributed across the components, based on PNLP calculations of component costs in CFAF (Table a-2).
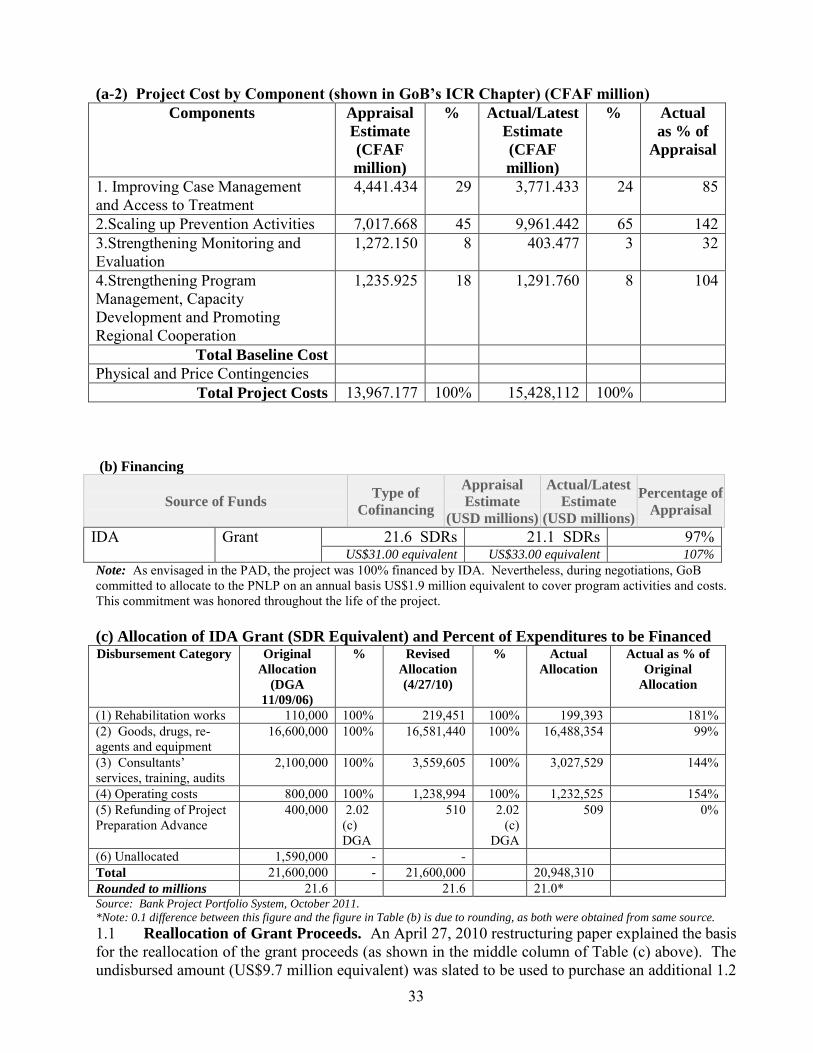
33
(a-2) Project Cost by Component (shown in GoB’s ICR Chapter) (CFAF million)
Components Appraisal
Estimate
(CFAF
million)
% Actual/Latest
Estimate
(CFAF
million)
% Actual
as % of
Appraisal
1. Improving Case Management and Access to Treatment
4,441.434 29 3,771.433 24 85
2.Scaling up Prevention Activities 7,017.668 45 9,961.442 65 142 3.Strengthening Monitoring and Evaluation
1,272.150 8 403.477 3 32
4.Strengthening Program Management, Capacity Development and Promoting Regional Cooperation
1,235.925 18 1,291.760 8 104
Total Baseline Cost Physical and Price Contingencies
Total Project Costs 13,967.177 100% 15,428,112 100%
(b) Financing
Source of Funds Type of
Cofinancing
Appraisal
Estimate
(USD millions)
Actual/Latest
Estimate
(USD millions)
Percentage of
Appraisal
IDA Grant 21.6 SDRs 21.1 SDRs 97% US$31.00 equivalent US$33.00 equivalent 107%
Note: As envisaged in the PAD, the project was 100% financed by IDA. Nevertheless, during negotiations, GoB committed to allocate to the PNLP on an annual basis US$1.9 million equivalent to cover program activities and costs. This commitment was honored throughout the life of the project. (c) Allocation of IDA Grant (SDR Equivalent) and Percent of Expenditures to be Financed Disbursement Category Original
Allocation
(DGA
11/09/06)
% Revised
Allocation
(4/27/10)
% Actual
Allocation
Actual as % of
Original
Allocation
(1) Rehabilitation works 110,000 100% 219,451 100% 199,393 181% (2) Goods, drugs, re-agents and equipment
16,600,000 100% 16,581,440 100% 16,488,354 99%
(3) Consultants’ services, training, audits
2,100,000 100% 3,559,605 100% 3,027,529 144%
(4) Operating costs 800,000 100% 1,238,994 100% 1,232,525 154% (5) Refunding of Project Preparation Advance
400,000 2.02 (c) DGA
510 2.02 (c)
DGA
509 0%
(6) Unallocated 1,590,000 - - Total 21,600,000 - 21,600,000 20,948,310 Rounded to millions 21.6 21.6 21.0* Source: Bank Project Portfolio System, October 2011.
*Note: 0.1 difference between this figure and the figure in Table (b) is due to rounding, as both were obtained from same source.
1.1 Reallocation of Grant Proceeds. An April 27, 2010 restructuring paper explained the basis for the reallocation of the grant proceeds (as shown in the middle column of Table (c) above). The undisbursed amount (US$9.7 million equivalent) was slated to be used to purchase an additional 1.2
34
million LLINs to increase the coverage of targeted groups in the context of the new mass campaign, provide new stocks of ACTs and RDTs to be rolled out into public health facilities, and finance household and health facilities surveys to document results achieved at the end of the Project. Reallocations across disbursement categories were made to rectify higher-than-planned spending on rehabilitation works, consultant services and operating costs, which became overdrawn. The reallocations did not entail changes in activities, nor did they affect total project costs. Moreover, there was no change to the 100 percent financing of all disbursement categories.
1.2 Extension of Closing Date. By letter of September 14, 2010, responding to GoB’s request to the Bank of July 14, 2010, the World Bank approved a four-month extension of the original closing date, from February 28, 2011 to June 30, 2011. This extension was granted to allow GoB to complete a few major activities, which would consolidate the results achieved to date. Activities included: The organization of a mass campaign distribution of LLINs involving major RBM donors
including the Bank. (The Bank procured on time 1.2 million LLINs but few major donors encountered delay in their provision process, forcing GoB to postpone the campaign from July 2010 to Nov 2010.); and
Completion of an action plan, included in GoB’s request, composed of: o Activities linked to the national mass campaign distribution of LLINs o Household and health facilities surveys to evidence results achieved at the end of the
Project o Research activity to assess the effects of the integrated malaria control through the use
of LLINs and of ACTs in malaria case management o Audit of the project account as required in the DGA.
35
Annex 2
Outputs by Component19
Component 1: Improving Case Management and Access to Treatment (original estimate:
US$14.7 million, or 29% of original project cost; actual cost: US$8.1 million, or 24% of the final
project cost). 2.1 Critical Inputs. Over the four-year implementation period the project acquired and distributed a total of 25,325,010 ACT treatments to improve case management and access to treatment of simple cases of malaria. These drugs were first made available in mid-2008 to all public health facilities in all 34 health zones and all 12 departments in the country through CAME and its 3 regional depots. That same year and under the responsibility of the DPMED, the project also supported the removal of chloroquine and other artemisinine-based monotherapies from public health facilities and private retailers throughout the country and their destruction and proper disposal. It also supported improved case diagnosis through the provision in September 2008 of 1,600,000 rapid diagnosis tests (RDTs), ordered in 2007. RDTs are in use now in all public health centers in the country. In addition, it supplied in 2008 “BX41” microscopes and (together with national budget support) related laboratory supplies and materials to nine health facilities (the National University Hospital, 3 zonal hospitals and five health centers) and to the PNLP. RDTs and lab equipment and supplies were assessed on the basis of a mapping exercise undertaken by PNLP in 2008. In addition, the project provided in 2009 64,244 A Kits and 49,799 B kits (ordered in 2007) for the management of serious malaria cases in children under the age of 5 years. 2.2 Training. Health service providers were trained with a view to improving their knowledge and skills necessary for proper case management. Such training covered essential elements, most notably: GoB’s new Malaria Control policy, the proper and routine diagnosis, including the utilization of RDTs, and the correct utilization of ACTs. In total, some 10,000 health workers received this training. Specifically: 85 Level A lab technicians (vs. 90 planned) and 139 Level B lab technicians (vs. 140 planned) were trained in the proper diagnosis of malaria, using both microscopic and RDT methods. Training was supported with manuals and training guides. A total of 1997 health providers (doctors, nurses and midwives) were trained in malaria case management in referral hospitals, considerably more than the 275 initially planned. This difference is due to an initial underestimate of the number of health providers working in these facilities. At the health zone level 166 doctors were trained in 2009 and 2010 to implement the new Malaria Control Policy. This essentially covered all doctors operating in health zones, but less than the initial estimate of 430. Underpinning this training and pedagogical follow-up were the preparation and printing in 2008 of training materials and of a malaria supervision protocol for guiding/overseeing proper implementation of the new treatment policy throughout the zones’ catchment areas. At the operational, front-line level, 2,526 (of a total of 3,373) doctors, nurses, midwives, lab technicians, pharmacists and other qualified health workers were trained in 2008 to implement the new case management and treatment protocols (exceeding the 2,363 target, as were 3,581 (of a total of 3,682) non-qualified health workers (exceeding the target of 1781). The original targets were found to be underestimates, following a micro-planning exercise undertaken by field-based actors. Orientation meetings planned for private facilities were not undertaken. Also not undertaken were: the organization of meetings with pre-service trainers and the preparation of curricula on the new
19 Original cost estimates are drawn from PAD estimates, inclusive of contingencies.
36
policy. The project did not organize, as planned, a workshop to prepare and validate an implementation plan for dispensing ACT at the community level, but Catholic Relief Services has been working on this front. The project also supported the supervision/oversight of proper implementation of the new policy. Semi-annual supervision by the central level to the departmental level was carried out quite regularly. Supervisions by the DDS to the health zones, by the health zones to the health centers, and by the health centers to the community level are reported to have been carried out less regularly than planned. But they did occur several times per year, as reported by PNLP, and directly observed by the evaluation team during field visits. 2.3 The establishment of a system for pharmacovigilance is in process. This is being undertaken under the leadership of the DPM, which has the mandate for this work. Elements include: the preparation and validation of a form for reporting side effects; the establishment of an ad hoc committee on pharmacovigilance; and the identification of pilot health facilities (sentinel sites) for monitoring side effects. 2.4 Communication/Advocacy. National-level communication and advocacy activities were organized to sensitize national opinion on the new Malaria Control policy and its importance in addressing the country’s high morbidity and mortality due to malaria.
Component 2: Scaling Up Prevention Activities (original estimate: US$13.0 million or 45
percent of original project cost; actual cost: US$21.3 million or 65 percent of the final project
cost).
2.5 This component supported essentially two types of prevention activities: (1) the large-scale promotion and distribution of LLINs to pregnant women and children under the age of five; and (2) improved coverage of intermittent preventive treatment (IPT) for pregnant women through the dispensing of Sulfadoxine Pyrimethamine (SP) as a part of ante-natal care (ANC). Essentially all activities planned under this component were carried out. 2.6 Mass distribution campaigns to households. The project was the principle financier of the first mass distribution campaign, which took place in 2007: nets, activities, financing. The project provided 1.4 million LLINs, 86 percent of all nets distributed during the campaign. The project supported a second mass distribution campaign in 2011, with 1,675,000 LLINs. Total LLINs acquired exceeded the initial target of 2.2 million. The project supported other activities associated with the successful mass campaigns. A workshop was held to design different sensitization tools (posters, health center signs, billboards, information brochures, etc.). Audiovisual productions (films, TV spots, radio spots in 12 local languages, documentaries) were designed and diffused. The project trained radio and newspaper journalists and briefed town criers (crieurs publics) – one per village – on the campaign objectives and targets. Under contract with the PNLP radios transmitted messages to the population before, during and after the campaigns and on the utilization and care of LLINs. The project also supported a number of planning and training activities associated with the organization, logistics and implementation of the campaign, including: validation of the LLIN distribution protocol, coupled with Vitamine A and Albendazole distribution; preparation and validation of commune, health zone and departmental microplans; training of 692 arrondissement supervisors and 198 commune supervisors, and of 28,581 net distributors; transport of LLINs from the port of Cotonou to communes; management of stocks; radio contracts; monitoring and evaluation activities. In the end, all 3737 villages of Benin received LLINs.
37
2.7 Routine distribution of LLINs through regular health services. The project prepared guidelines and supported the training of the range of actors involved in the facility-based, routine distribution of bed nets to target populations: children under five at the time of project made LLINs available for routine distribution to pregnant women through ANC services initially through the use of the stock left over from the 2007 mass campaign. The project subsequently procured some 475,000 additional LLINs to ensure continued supply of nets for this purpose, but there were delays in their availability. PMI provided nets for ANC services, and the 475,000 nets purchased by the project were ultimately used to fill the gap in available LLINs for the 2011 mass campaign.
2.8 Community Partnerships through NGO Contracts. PNLP strengthened partnerships with communities with NGOs covering each one of the country’s 34 health zones. Contracted NGOs worked to increase the knowledge of communities about how malaria is contracted and to encourage behaviors for its prevention. Thirty-three contracts were signed in 2007 between NGOs and each health zone, and most were renewed in 2009. Two were replaced by other NGOs in 2009, because of their unsatisfactory performance. National Malaria Day events took place in Dassa (2008), Lokossa (2009), and Cotonou (2010).
2.9 Intermittent Preventive Treatment involves the provision of two doses of Sulfadoxine-Pyrimethamine to pregnant women during the course of their antenatal visits. The project supported implementation of this aspect of Benin’s Malaria Strategy through the acquisition of 593,400 doses of SP, or 74 percent of the 800,000 doses initially planned. Other RBM partners provided additional doses.
Component 3: Strengthening of Monitoring and Evaluation (original estimate: US$1.7 million,
or 8 percent of the total original project cost; actual cost: US$0.9 million, or 3 percent of the
final project cost).
2.10 With project support a national Malaria Control M&E framework was developed and validated, covering the 2006-2010 period, its indicators responsive to international exigencies. This framework is relied upon by all partners contributing to the program and constitutes a major accomplishment. In an effort to harmonize the support and efforts of all partners, an annual integrated work plan incorporating the contributions of all is now routinely prepared, the first one produced in 2009.
2.11 Under this component several evaluations were undertaken to assess the extent to which goals and targets set under the 2006-2010 strategic plan were achieved. To this end, the project supported a national Lot Quality Assurance Sampling (LQAS) exercise in 2008 and a Malaria Indicators Survey (MIS) in 2010. Under the overall coordination of PNLP, the project also contributed to a Health Facility Survey, implemented jointly with CDC/PMI, PSI and MSH and to a study of malaria health indicators in health facilities in all 12 of Benin’s departments. The project also supported studies to assess on an annual basis the levels of resistance of plasmodium to antimalarial medicines and of the vector to LLINs and insecticides. These activities were contracted out to various research/scientific institutions in Benin, under the supervision of PNLP. 2.12. To ensure regular data on malaria from health facilities a routine malaria information system (SIRP) and a logistics management information system (SIGL) were established. The SIGL tracks information on essential malaria inputs (ACTs, LLINs, RDTs and SP). The process of establishing the SIRP included project support to the training of health facility staff and the provision of data collection tools.
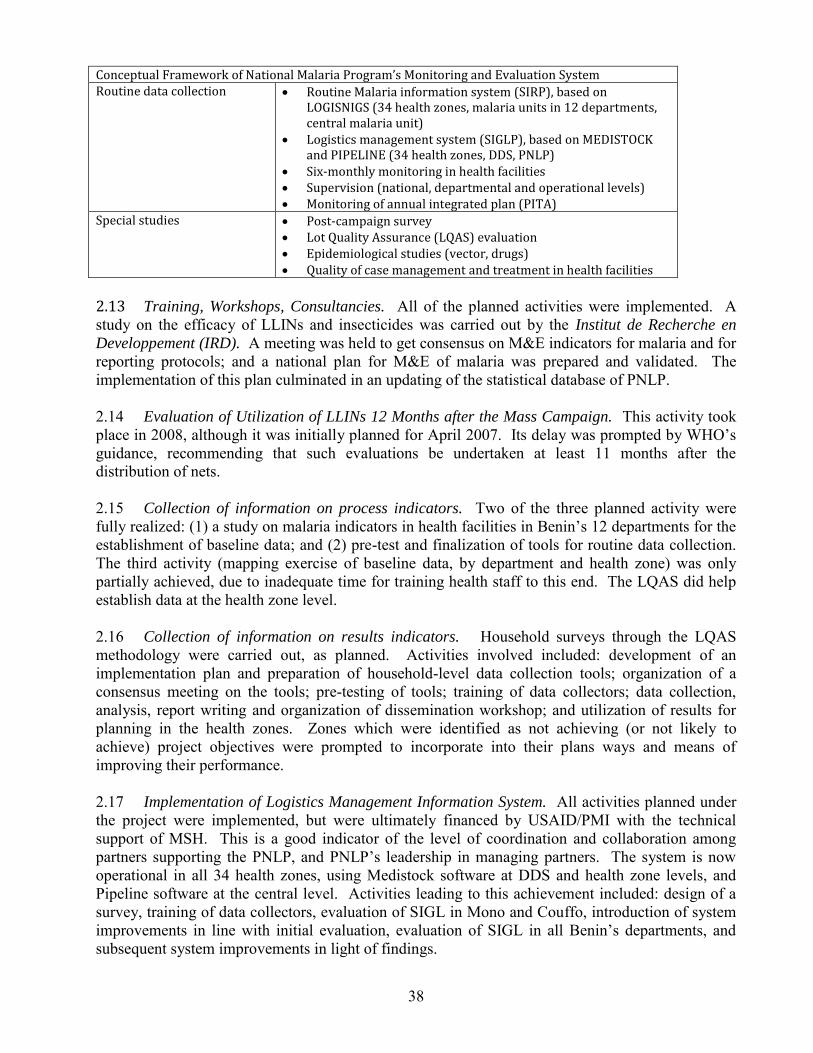
38
Conceptual Framework of National Malaria Program’s Monitoring and Evaluation System Routine data collection Routine Malaria information system (SIRP), based on
LOGISNIGS (34 health zones, malaria units in 12 departments, central malaria unit)
Logistics management system (SIGLP), based on MEDISTOCK and PIPELINE (34 health zones, DDS, PNLP)
Six-monthly monitoring in health facilities Supervision (national, departmental and operational levels) Monitoring of annual integrated plan (PITA)
Special studies Post-campaign survey Lot Quality Assurance (LQAS) evaluation Epidemiological studies (vector, drugs) Quality of case management and treatment in health facilities
2.13 Training, Workshops, Consultancies. All of the planned activities were implemented. A study on the efficacy of LLINs and insecticides was carried out by the Institut de Recherche en
Developpement (IRD). A meeting was held to get consensus on M&E indicators for malaria and for reporting protocols; and a national plan for M&E of malaria was prepared and validated. The implementation of this plan culminated in an updating of the statistical database of PNLP. 2.14 Evaluation of Utilization of LLINs 12 Months after the Mass Campaign. This activity took place in 2008, although it was initially planned for April 2007. Its delay was prompted by WHO’s guidance, recommending that such evaluations be undertaken at least 11 months after the distribution of nets. 2.15 Collection of information on process indicators. Two of the three planned activity were fully realized: (1) a study on malaria indicators in health facilities in Benin’s 12 departments for the establishment of baseline data; and (2) pre-test and finalization of tools for routine data collection. The third activity (mapping exercise of baseline data, by department and health zone) was only partially achieved, due to inadequate time for training health staff to this end. The LQAS did help establish data at the health zone level. 2.16 Collection of information on results indicators. Household surveys through the LQAS methodology were carried out, as planned. Activities involved included: development of an implementation plan and preparation of household-level data collection tools; organization of a consensus meeting on the tools; pre-testing of tools; training of data collectors; data collection, analysis, report writing and organization of dissemination workshop; and utilization of results for planning in the health zones. Zones which were identified as not achieving (or not likely to achieve) project objectives were prompted to incorporate into their plans ways and means of improving their performance. 2.17 Implementation of Logistics Management Information System. All activities planned under the project were implemented, but were ultimately financed by USAID/PMI with the technical support of MSH. This is a good indicator of the level of coordination and collaboration among partners supporting the PNLP, and PNLP’s leadership in managing partners. The system is now operational in all 34 health zones, using Medistock software at DDS and health zone levels, and Pipeline software at the central level. Activities leading to this achievement included: design of a survey, training of data collectors, evaluation of SIGL in Mono and Couffo, introduction of system improvements in line with initial evaluation, evaluation of SIGL in all Benin’s departments, and subsequent system improvements in light of findings.
39
2.18 Survey on the Quality of Services. This activity consisted of the design and implementation of a health facilities survey to assess the quality of services. Originally envisaged to be undertaken with project support, this activity was ultimately designed and undertaken with the participation of other development partners, notably MSH, PSI and the project. While this partnership took time to establish and to ensure that the activities/interests of all partners were incorporated into the study, the benefits of this coordination were worth the effort. Partners split the costs of the study and took ownership of its results. The technical supervision and oversight of CDC provided quality assurance of the study’s integrity and results. 2.19 Four other planned studies were implemented: (1) two studies on the efficacy of malaria drugs; (2) a study on vectors’ resistance to insecticides; (3) establishment of a pharmacovigilance system; and (4) a qualitative study on the effect of LLIN utilization by target groups on the demand for malaria care (study carried out, but never finalized). A study on the social and economic costs of malaria was not carried out. 2.20 M&E activities were strengthened at all levels of the health system with: (1) the provision of computer and office equipment; (2) capacity building through long and short-term training; and (3) the establishment of the malaria information system (SIRP) regularly updated and able to produce data on malaria morbidity and mortality. This was implemented through an approach which strengthened the SNIGS by integrating variables allowing the assessment of program performance against targets and objectives and the tracking of various inputs (LLINs, ACT, SP) for the country. The statisticians and heads of the Studies, Planning and Statistics service in the 34 health zones were trained in the utilization of LogiSNIGS. 2.21 Epidemiological surveillance is carried out with regularity, essentially composed of the regular collection of morbidity and mortality data in health facilities, malaria surveillance in sentinel sites, surveys on the coverage of LLINs, etc. Component 4: Strengthening Program Management, Capacity Development and Promoting
Regional Cooperation (original estimate: US$1.6 million, or 5 percent of total estimated cost;
actual cost: US$2.7 million or 8 percent of final project cost).
2.22 Program Management. The project purchased computers, printers and pick-ups for central level PNLP, the six DDS-level malaria units and 30 health zones. It also provided a motorcycle to each of the 34 health zones and one for PNLP, central. In addition it provided PNLP, central level, with office furniture and office and media equipment to carry out its functions. (These are itemized in a detailed note prepared by the PNLP, available on file; and all of these acquisitions have been audited and accounted for.) The project also rehabilitated the PNLP offices, adding a second floor to a one-story building, and constructing a small annex building to house the staff. It also constructed and equipped a storage facility for the Centrale d’Achat des Medicaments Essentiels (CAME) to increase its storage capacity to receive and manage drugs to be purchased with project proceeds. The project supported the running costs of PNLP including: office supplies, vehicle operation and maintenance, communications.
2.23 The project financed the audits of the PPF and of the project years 2007, 2008, 2009 and 2010, carried out by two independent auditing firms. In addition, the General Inspectorate of MoH carried out a control of funds allocated to health zones and to the DDS. The Project Coordination also carried out annual supervision missions to oversee the management and use of funds in health zones and DDS during the four-year implementation period.
40
2.24 The project also financed the mid-term evaluation of the project in May 2009 at a workshop with 97 participants representing all structures involved in implementation, including civil society organizations and financial and technical partners. A final evaluation workshop was held in Bohicon in June 2011, again with wide participation of actors and stakeholders.
2.25 Capacity Development. Four contractual staff were recruited to support PNLP in project implementation: a procurement specialist, a financial manager, an accountant and an administrative assistant. The project also provided substantial short-term training. Five DDS-level staff benefited from short-term training (epidemiology, malaria case management, and performance-based management); and one DDS-level staff completed a Master’s degree in epidemiology. Nineteen staff of PNLP benefitted from short-term training, covering such topics as: epidemiology, results-based management, procurement of medicines and medical supplies, pharmacovigilance, management, leadership training, project financial management, project management; and one PNLP staff received one year of training in public health. Other MoH staff in other technical departments also benefited from short-term training, notably in: procurement of medicines and medical supplies (public procurement unit/MoH and CAME); procurement for civil works, supplies and consultants services (public procurement unit/MoH); and project audit and control (Inspectorate/MoH).
2.26 Regional Cooperation and Knowledge Sharing. The project financed study tours for PNLP staff (of which one from the DDS-level) to observe malaria diagnosis and treatment practices in Brazil. PNLP delegations also participated in semi-annual exchanges organized by the West African RBM Network (WARN) and in annual meetings of the pharmaceutical groups SANOFI and NOVARTIS to review and discuss best practices.
2.27 Implementation of the Vector/Pest Management Plan. All three activities planned under this subcomponent were implemented: (1) the organization of a training workshop for socio-health actors on the management of pesticides; (2) the organization of a consensus-reaching workshop of all sectors using pesticides; and (3) the implementation of the management of pests and pesticides action plan. Implementation of these activities involved: preparation of an action plan; reaching agreement with all actors using pesticides coming from Health and Rural Development Ministries; establishment of a pilot committee, created by Ministry of Health arrête on September 14 2009 and holding of meetings since October 15, 2009; document review on utilization of larvicides; environmental audit on the treatment of gite larvaires with bio larvicide in Cotonou neighborhoods; printing of various manuals on management of pests and pesticides; training and launch of village committees responsible for pest and pesticide management in villages and city neighborhoods in Benin; surveillance study on the resistance of malaria vectors to pesticides; equipment and material support to the Mayor of Cotonou for pest and pesticide management; and collection of empty packaging for distributed LLINs and their placement at a designated site and their ultimate destruction/disposal by a specialized institution.
41
Annex 3 Economic and Financial Analysis
3.1 No new economic analysis was undertaken at the end of this project, but all of the findings of the economic analysis undertaken at the time of project design (and captured in Annex 9 of the PAD) still hold. 3.2 Project achievements notwithstanding, the socio-economic burden of malaria on Benin’s population is heavy. Malaria is the number one cause of adult morbidity, seriously undermining productivity and income earning capacity, both at the individual/family levels, and at the macro-economic level. It is the number one cause of under five mortality; and malaria in pregnant women contributes to low birth weight, perinatal mortality and maternal mortality. Malaria also causes indirect costs that affect vulnerable and poor groups most. 3.3 The new treatment drugs (ACTs) are more expensive than the (no longer effective) chloroquine they are replacing. Still, the package of high-impact prevention and treatment interventions recommended by WHO for stable endemic malaria20 (and adhered to under Benin’s malaria policy and strategy) are highly cost effective. They have the potential (demonstrated under this project) to have an enormous impact on the health of mothers and children, especially, and on adults, at low cost. 3.4 The analysis of bottlenecks undertaken during project design also still holds, focusing largely around health systems issues and the ability to reach communities. Over the ensuing five years, with the support of this project and many other interventions, some headway has been made on these bottlenecks. But they still constitute an agenda for action, mostly through intensified health system strengthening efforts, which are ongoing. 3.5 See also paragraphs 72-76 of the main text, which assesses project efficiency.
20 Such as what is found in Benin.
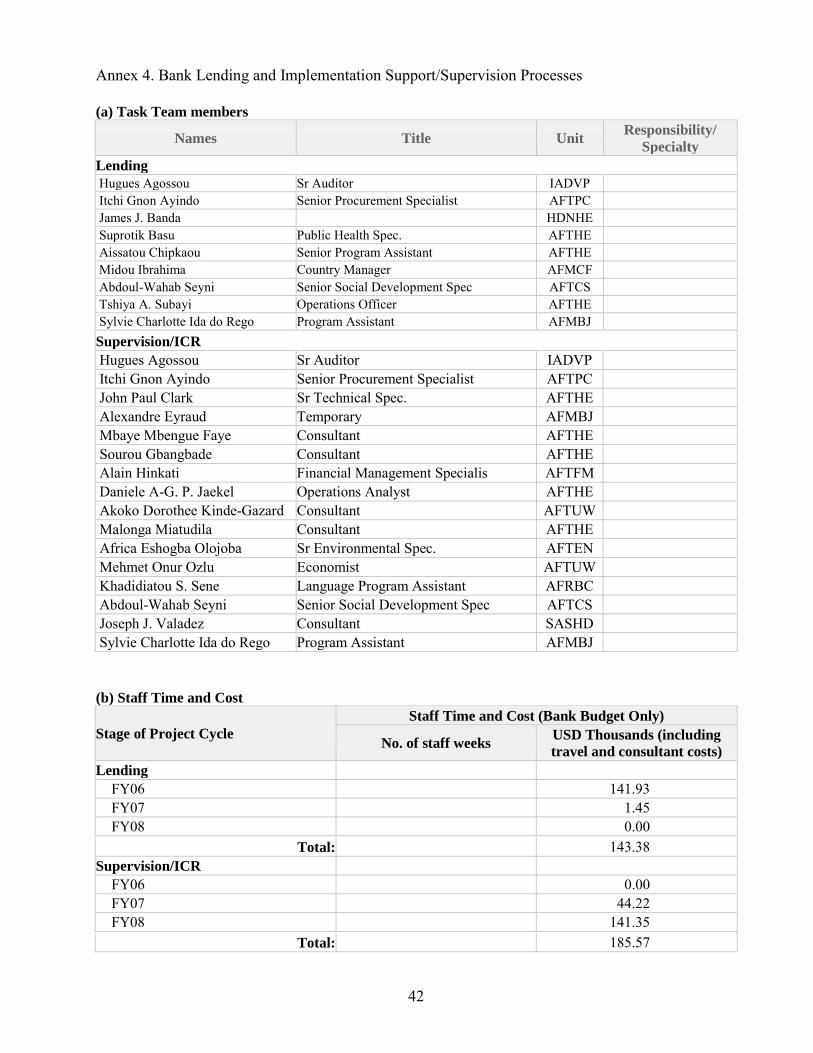
42
Annex 4. Bank Lending and Implementation Support/Supervision Processes
(a) Task Team members
Names Title Unit Responsibility/
Specialty
Lending Hugues Agossou Sr Auditor IADVP Itchi Gnon Ayindo Senior Procurement Specialist AFTPC James J. Banda HDNHE Suprotik Basu Public Health Spec. AFTHE Aissatou Chipkaou Senior Program Assistant AFTHE Midou Ibrahima Country Manager AFMCF Abdoul-Wahab Seyni Senior Social Development Spec AFTCS Tshiya A. Subayi Operations Officer AFTHE Sylvie Charlotte Ida do Rego Program Assistant AFMBJ
Supervision/ICR Hugues Agossou Sr Auditor IADVP Itchi Gnon Ayindo Senior Procurement Specialist AFTPC John Paul Clark Sr Technical Spec. AFTHE Alexandre Eyraud Temporary AFMBJ Mbaye Mbengue Faye Consultant AFTHE Sourou Gbangbade Consultant AFTHE Alain Hinkati Financial Management Specialis AFTFM Daniele A-G. P. Jaekel Operations Analyst AFTHE Akoko Dorothee Kinde-Gazard Consultant AFTUW Malonga Miatudila Consultant AFTHE Africa Eshogba Olojoba Sr Environmental Spec. AFTEN Mehmet Onur Ozlu Economist AFTUW Khadidiatou S. Sene Language Program Assistant AFRBC Abdoul-Wahab Seyni Senior Social Development Spec AFTCS Joseph J. Valadez Consultant SASHD Sylvie Charlotte Ida do Rego Program Assistant AFMBJ
(b) Staff Time and Cost
Stage of Project Cycle
Staff Time and Cost (Bank Budget Only)
No. of staff weeks USD Thousands (including
travel and consultant costs)
Lending
FY06 141.93 FY07 1.45 FY08 0.00
Total: 143.38 Supervision/ICR
FY06 0.00 FY07 44.22 FY08 141.35
Total: 185.57

43
Annex 5.
Beneficiary Survey Results No end-of-project beneficiary survey was carried out.
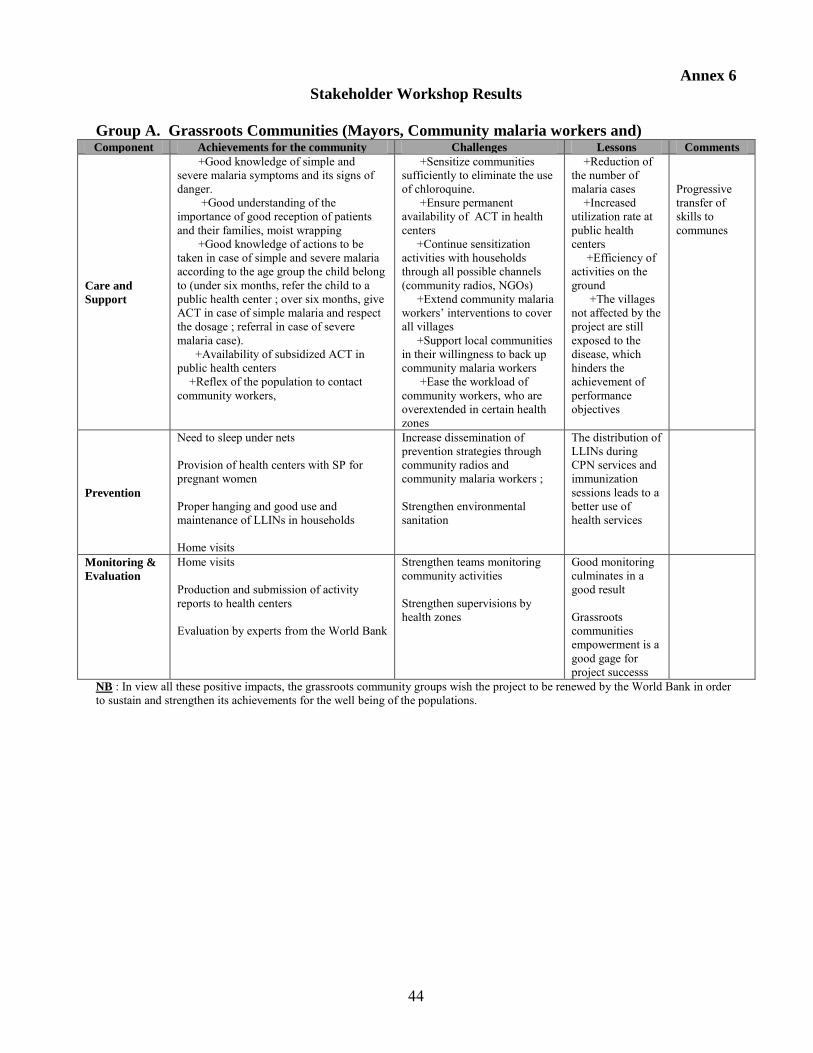
44
Annex 6
Stakeholder Workshop Results
Group A. Grassroots Communities (Mayors, Community malaria workers and) Component Achievements for the community Challenges Lessons Comments
Care and
Support
+Good knowledge of simple and severe malaria symptoms and its signs of danger. +Good understanding of the importance of good reception of patients and their families, moist wrapping +Good knowledge of actions to be taken in case of simple and severe malaria according to the age group the child belong to (under six months, refer the child to a public health center ; over six months, give ACT in case of simple malaria and respect the dosage ; referral in case of severe malaria case). +Availability of subsidized ACT in public health centers +Reflex of the population to contact community workers,
+Sensitize communities sufficiently to eliminate the use of chloroquine. +Ensure permanent availability of ACT in health centers +Continue sensitization activities with households through all possible channels (community radios, NGOs) +Extend community malaria workers’ interventions to cover all villages +Support local communities in their willingness to back up community malaria workers +Ease the workload of community workers, who are overextended in certain health zones
+Reduction of the number of malaria cases +Increased utilization rate at public health centers +Efficiency of activities on the ground +The villages not affected by the project are still exposed to the disease, which hinders the achievement of performance objectives
Progressive transfer of skills to communes
Prevention
Need to sleep under nets Provision of health centers with SP for pregnant women Proper hanging and good use and maintenance of LLINs in households Home visits
Increase dissemination of prevention strategies through community radios and community malaria workers ; Strengthen environmental sanitation
The distribution of LLINs during CPN services and immunization sessions leads to a better use of health services
Monitoring &
Evaluation
Home visits Production and submission of activity reports to health centers Evaluation by experts from the World Bank
Strengthen teams monitoring community activities Strengthen supervisions by health zones
Good monitoring culminates in a good result Grassroots communities empowerment is a good gage for project successs
NB : In view all these positive impacts, the grassroots community groups wish the project to be renewed by the World Bank in order to sustain and strengthen its achievements for the well being of the populations.
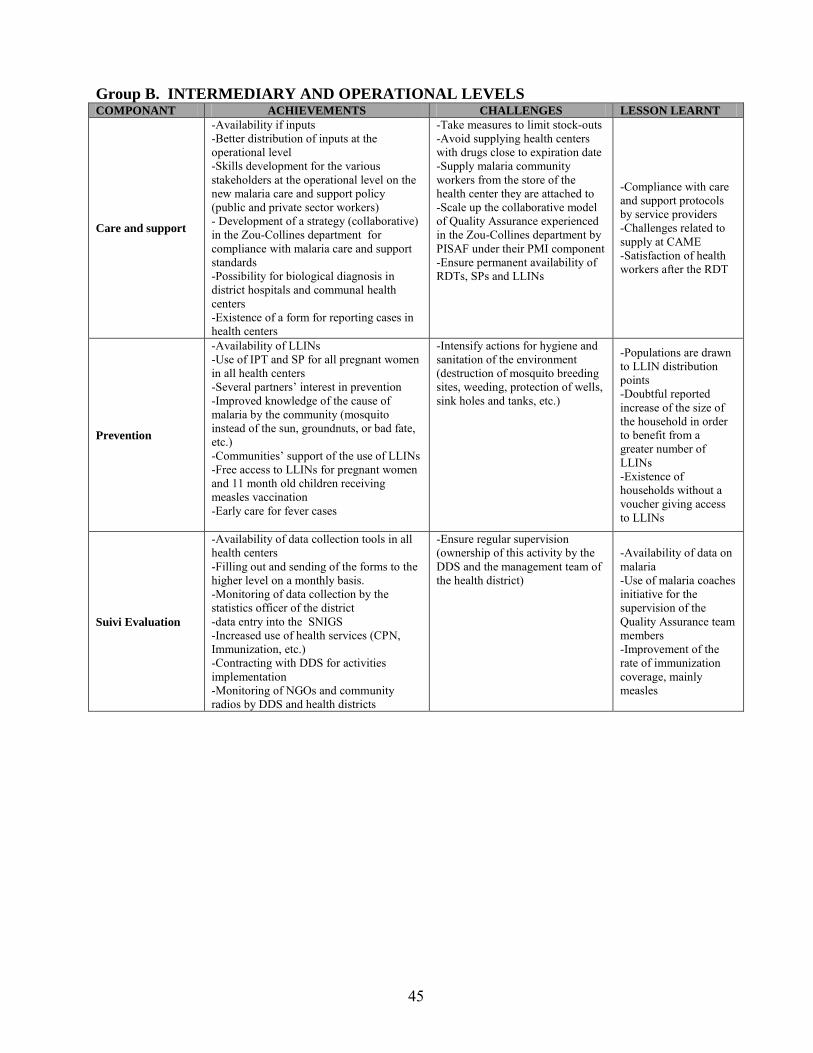
45
Group B. INTERMEDIARY AND OPERATIONAL LEVELS COMPONANT ACHIEVEMENTS CHALLENGES LESSON LEARNT
Care and support
-Availability if inputs -Better distribution of inputs at the operational level -Skills development for the various stakeholders at the operational level on the new malaria care and support policy (public and private sector workers) - Development of a strategy (collaborative) in the Zou-Collines department for compliance with malaria care and support standards -Possibility for biological diagnosis in district hospitals and communal health centers -Existence of a form for reporting cases in health centers
-Take measures to limit stock-outs -Avoid supplying health centers with drugs close to expiration date -Supply malaria community workers from the store of the health center they are attached to -Scale up the collaborative model of Quality Assurance experienced in the Zou-Collines department by PISAF under their PMI component -Ensure permanent availability of RDTs, SPs and LLINs
-Compliance with care and support protocols by service providers -Challenges related to supply at CAME -Satisfaction of health workers after the RDT
Prevention
-Availability of LLINs -Use of IPT and SP for all pregnant women in all health centers -Several partners’ interest in prevention -Improved knowledge of the cause of malaria by the community (mosquito instead of the sun, groundnuts, or bad fate, etc.) -Communities’ support of the use of LLINs -Free access to LLINs for pregnant women and 11 month old children receiving measles vaccination -Early care for fever cases
-Intensify actions for hygiene and sanitation of the environment (destruction of mosquito breeding sites, weeding, protection of wells, sink holes and tanks, etc.)
-Populations are drawn to LLIN distribution points -Doubtful reported increase of the size of the household in order to benefit from a greater number of LLINs -Existence of households without a voucher giving access to LLINs
Suivi Evaluation
-Availability of data collection tools in all health centers -Filling out and sending of the forms to the higher level on a monthly basis. -Monitoring of data collection by the statistics officer of the district -data entry into the SNIGS -Increased use of health services (CPN, Immunization, etc.) -Contracting with DDS for activities implementation -Monitoring of NGOs and community radios by DDS and health districts
-Ensure regular supervision (ownership of this activity by the DDS and the management team of the health district)
-Availability of data on malaria -Use of malaria coaches initiative for the supervision of the Quality Assurance team members -Improvement of the rate of immunization coverage, mainly measles
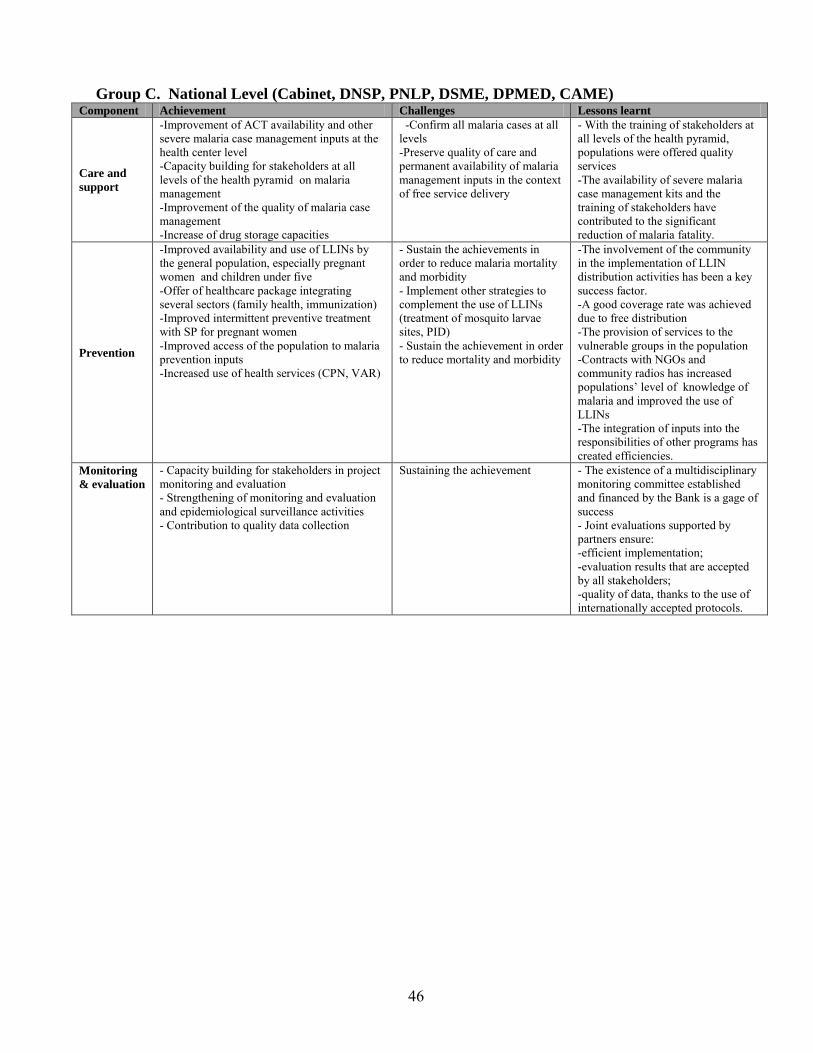
46
Group C. National Level (Cabinet, DNSP, PNLP, DSME, DPMED, CAME)
Component Achievement Challenges Lessons learnt
Care and
support
-Improvement of ACT availability and other severe malaria case management inputs at the health center level -Capacity building for stakeholders at all levels of the health pyramid on malaria management -Improvement of the quality of malaria case management -Increase of drug storage capacities
-Confirm all malaria cases at all levels -Preserve quality of care and permanent availability of malaria management inputs in the context of free service delivery
- With the training of stakeholders at all levels of the health pyramid, populations were offered quality services -The availability of severe malaria case management kits and the training of stakeholders have contributed to the significant reduction of malaria fatality.
Prevention
-Improved availability and use of LLINs by the general population, especially pregnant women and children under five -Offer of healthcare package integrating several sectors (family health, immunization) -Improved intermittent preventive treatment with SP for pregnant women -Improved access of the population to malaria prevention inputs -Increased use of health services (CPN, VAR)
- Sustain the achievements in order to reduce malaria mortality and morbidity - Implement other strategies to complement the use of LLINs (treatment of mosquito larvae sites, PID) - Sustain the achievement in order to reduce mortality and morbidity
-The involvement of the community in the implementation of LLIN distribution activities has been a key success factor. -A good coverage rate was achieved due to free distribution -The provision of services to the vulnerable groups in the population -Contracts with NGOs and community radios has increased populations’ level of knowledge of malaria and improved the use of LLINs -The integration of inputs into the responsibilities of other programs has created efficiencies.
Monitoring
& evaluation
- Capacity building for stakeholders in project monitoring and evaluation - Strengthening of monitoring and evaluation and epidemiological surveillance activities - Contribution to quality data collection
Sustaining the achievement - The existence of a multidisciplinary monitoring committee established and financed by the Bank is a gage of success - Joint evaluations supported by partners ensure: -efficient implementation; -evaluation results that are accepted by all stakeholders; -quality of data, thanks to the use of internationally accepted protocols.
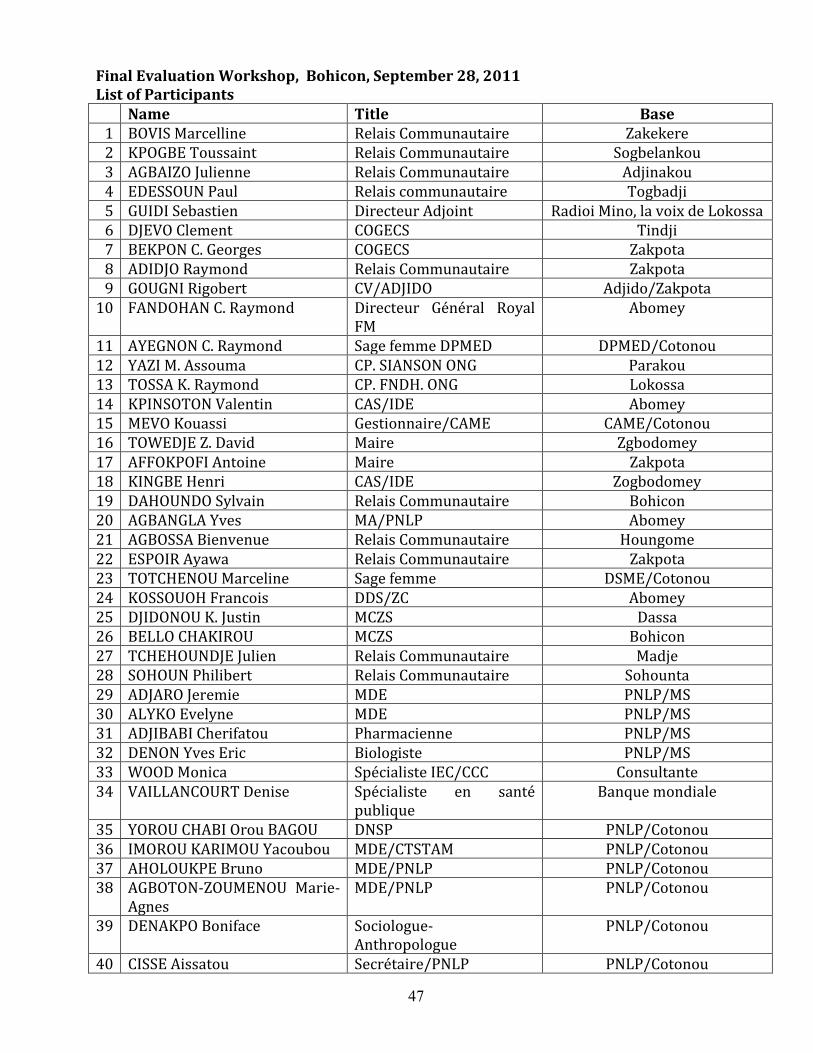
47
Final Evaluation Workshop, Bohicon, September 28, 2011 List of Participants Name Title Base
1 BOVIS Marcelline Relais Communautaire Zakekere 2 KPOGBE Toussaint Relais Communautaire Sogbelankou 3 AGBAIZO Julienne Relais Communautaire Adjinakou 4 EDESSOUN Paul Relais communautaire Togbadji 5 GUIDI Sebastien Directeur Adjoint Radioi Mino, la voix de Lokossa 6 DJEVO Clement COGECS Tindji 7 BEKPON C. Georges COGECS Zakpota 8 ADIDJO Raymond Relais Communautaire Zakpota 9 GOUGNI Rigobert CV/ADJIDO Adjido/Zakpota
10 FANDOHAN C. Raymond Directeur Général Royal FM
Abomey
11 AYEGNON C. Raymond Sage femme DPMED DPMED/Cotonou 12 YAZI M. Assouma CP. SIANSON ONG Parakou 13 TOSSA K. Raymond CP. FNDH. ONG Lokossa 14 KPINSOTON Valentin CAS/IDE Abomey 15 MEVO Kouassi Gestionnaire/CAME CAME/Cotonou 16 TOWEDJE Z. David Maire Zgbodomey 17 AFFOKPOFI Antoine Maire Zakpota 18 KINGBE Henri CAS/IDE Zogbodomey 19 DAHOUNDO Sylvain Relais Communautaire Bohicon 20 AGBANGLA Yves MA/PNLP Abomey 21 AGBOSSA Bienvenue Relais Communautaire Houngome 22 ESPOIR Ayawa Relais Communautaire Zakpota 23 TOTCHENOU Marceline Sage femme DSME/Cotonou 24 KOSSOUOH Francois DDS/ZC Abomey 25 DJIDONOU K. Justin MCZS Dassa 26 BELLO CHAKIROU MCZS Bohicon 27 TCHEHOUNDJE Julien Relais Communautaire Madje 28 SOHOUN Philibert Relais Communautaire Sohounta 29 ADJARO Jeremie MDE PNLP/MS 30 ALYKO Evelyne MDE PNLP/MS 31 ADJIBABI Cherifatou Pharmacienne PNLP/MS 32 DENON Yves Eric Biologiste PNLP/MS 33 WOOD Monica Spécialiste IEC/CCC Consultante 34 VAILLANCOURT Denise Spécialiste en santé
publique Banque mondiale
35 YOROU CHABI Orou BAGOU DNSP PNLP/Cotonou 36 IMOROU KARIMOU Yacoubou MDE/CTSTAM PNLP/Cotonou 37 AHOLOUKPE Bruno MDE/PNLP PNLP/Cotonou 38 AGBOTON-ZOUMENOU Marie-
Agnes MDE/PNLP PNLP/Cotonou
39 DENAKPO Boniface Sociologue-Anthropologue
PNLP/Cotonou
40 CISSE Aissatou Secrétaire/PNLP PNLP/Cotonou
48
Annex 7
Summary of Borrower’s ICR
7.1 The Borrower’s ICR (Rapport d’achevement du Projet d’Appui a la Lutte contre le
Paludisme Ŕ Don IDA H 229-BEN) was prepared in September 2011 (available for the September/October ICR Review Mission), and formally submitted to the Bank in early October. The report was very well prepared, drawing on a strong evidence base, thanks to the successful M&E activities and outputs, and benefiting from good analysis. 7.2 The report presents an accurate overview of project objectives and components, in sync with this ICR’s presentation. It notes its strong appreciation of the project design, which allowed the placement of project management and coordination in the agency responsible for the overall malaria program (PNLP). This is noted to have provided a unique opportunity for capacity building through an applied approach. 7.3 For each component the report itemizes: original and actual costs, the main elements of project support and outcomes. These highlights are not repeated here because they are fully in sync with the presentation of components in this ICR (Main Text and Annex 2). These data are based on detailed itemization and costs that were available at the level of the PNLP (and reviewed by the ICR mission). This report quickly reviews procurement and financial management implementation, and raises difficulties caused by delays in approvals and contract signatures attributable to the National Tender Board and MoEF. Based on project and program data generated by the strong M&E work, the Borrower’s report provides actual data against original and revised targets for each key performance indicator. Again, because outcome data were reviewed by the mission and reflected in the Main Text, outcomes will not be repeated here. 7.4 The following paragraphs provides some highlights of evaluative comments included in the Borrower’s ICR. First, the project was found to have truly boosted the implementation of Benin’s national malaria policy. With regard to prevention, it brought a dynamism to the decentralization of activities right to the community level, and with the active support and involvement of health zones and NGOs and local radio stations, with very encouraging, tangible results. Likewise, a new dynamism was also introduced to case management efforts, also with tangible results. The project also contributed to health systems strengthening. 7.5 Second, the role of the Bank was highly appreciated, especially for: its multi-disciplinary teams, its close collaboration with WHO and other RBM partners, the close and rigorous follow-up and support of the Cotonou-based TTL. Third, factors facilitating project implementation included: strong Government commitment; the integration of the project into the work/mandate of the PNLP; the personnel, logistical and material support to PNLP to help it do its job; and the good partnership within and beyond MoH to implement malaria policy and strategy. Fourth, factors constraining project implementation included: delays in non-objections from DNMP; delays in the signature of the LLINs contract; delays in launching the ACT activities; issues of stockage of inputs; occasional strikes of health workers; delays in procurements due to delays in approvals (by National Tender Board) and signatures (by MoEF); and delays in preparing Terms of Reference for studies and technical specifications. 7.6 Fifth, the quality of relations between the Bank and the Government were satisfactory, attributable to the commitment of both parties to the PDOs. Sixth, the quality of the various institutions, research/study bureaus and consultants, who contributed to the project, was found to be
49
good. Collaborators included: the University’s Faculty of Science (FCC), the Center for Entomological Research of Cotonou (CREC), the Regional Institute for Public Health (ISRP), among others. PNLP stated that it gained valuable knowledge and experience through these collaborations. 7.7 Seventh, the importance of maintaining and further strengthening gains made under this project is emphasized. This will require Government support as well as technical and financial support from partners. On the M&E front, there is need to continue efforts to strengthen the information system to ensure timely availability of quality data with a view to better program management, stronger oversight of program performance and adjustments to efforts in this light. Additional resources are necessary to this end. 7.8 The Borrower’s ICR concludes by stating that the project’s objectives have been achieved, which explains the declining trends in mortality, especially among children under five years of age. Momentum can only be assured with continued support both to maintain gains and to further extend the coverage of interventions. The Bank’s technical and financial support is strongly solicited as GoB embarks on the implementation of its new NSP (2011-2015).
50
Annex 8
Comments of Roll Back Malaria (RBM) Partners
8.1 On September 29, 2011, the ICR mission organized a meeting of RBM Partners to solicit their views on the performance of the Benin Malaria Control Support Project. The meeting was chaired by Dr. Marie-Agnes Agboton-Zoumenou, Coordinator, PNLP, and attended by key members of her staff and representatives of: AFRICARE, Catholic Relief Services, Belgian Cooperation, PSI, UNFPA, UNICEF, the United States Centers for Disease Control, USAID, and WHO. This note synthesizes strong consensus among the partners on a number of points: (1) the overall success of the project and, more broadly, of Benin’s national malaria control program over the past five years; (2) concerns about the sustainability of achievements and the need for continued support, especially with regard to health systems strengthening; and (3) the very strong coordination and collaboration among RBM partners and opportunities for continued and enhanced efforts to this end. A brief overview of each of these points is presented below.
8.2 Successful Outcome. All partners appreciated the PNLP’s presentation of performance against project targets, all of which were essentially achieved (with some targets exceeded). (See also Section 3 of this ICR.) These included increased coverage (to at least 60 percent) of target groups (children under 5 and pregnant women) with essential prevention and care interventions. Both technical and managerial capacities were developed with program/project assistance. The PNLP and all partners acknowledged that these achievements are not solely attributable to the Bank-financed project. Rather they are attributable to the collective efforts of all partners supporting Benin’s PNLP. This being said, the value added of the Bank’s support was easily distinguished. The Bank was the first to finance the provision of major commodities to enable the nationwide launch/implementation of Benin’s new malaria strategy: ACTs, RDTs, SP and LLINs. The Bank’s financial support and the PNLP’s good performance attracted other major sources of support, USAID/PMI an important example. The Bank’s role in building the capacity of the PNLP in the areas of program strategic management and oversight, coordination of aid, procurement, financial management, results-based M&E and technical rigor in supervision was duly acknowledged. This support was provided by the pro-activity of the Cotonou-based task team leader, complemented by the rigor and regularity of a multi-disciplinary team, which supervised the project, in close consultation with PNLP and its partners, and left instructive aide-memoires to guide the follow-up and improvement measures. It was also grounded in the design of the project which opted out of a PIU approach and, instead, made the PNLP responsible for project management.
8.3 Challenges of Sustainability and Health Systems Strengthening. There is great concern about the ability to sustain the gains achieved under the project and program during the last five years. This will depend on continued support to the PNLP, in terms of commodities, and in terms of activities, both preventive (behavior change promotion, mass campaigns for new cohorts) and treatment-related (quality assurance, including training, supervision). It will also involve continued support to strategic management and oversight, which are the regular, operational responsibilities of PNLP at all levels of the system, including: costs of program management, communications, coordination, monitoring and evaluation, and the use of these data for decision-making and overseeing accountability. As one speaker so aptly put it, sustainability does not mean just to continue what was done in the past, but, rather to build on what was done and to change to a second phase of improvement and health systems strengthening. Indeed, there was strong consensus that not only is health systems strengthening critical to the continued improvement and sustainable

51
success of the PNLP. Malaria control interventions can actually be an entry point to a more rigorous, more holistic health systems strengthening approach. While acknowledging that many RBM partners have the capacity and the opportunity to provide much of what is needed both in terms of program-specific and health systems strengthening support, the Bank’s already demonstrated value-added, especially in terms of capacity building, was considered to be essential to future success. One important challenge of health system strengthening, which was cited as needing attention, is the fuller utilization of data for decision-making at the operational level.
8.4 Strengthened Partnerships and Aid Coordination. Benin’s RBM partners are very well coordinated, with considerable evidence to substantiate this: excellent coordination/collaboration around M&E and research/evaluation studies; joint support to the 2011 mass campaign, drawing on comparative advantages; coordination and complementarity in the timing and provision of malaria commodities; monthly meetings between PNLP and RBM partners, with productive technical and strategic discussions; and joint annual planning and review meetings. It was also noted that there is room for improved coordination. One activity, considered to be critical to strengthened coordination and partnership, is the detailed mapping of all malaria support and interventions provided by each partner in each locality. Some work is underway to this end, but it needs to be both detailed and comprehensive in order to facilitate improved coordination and achieve greater efficiency of all support.
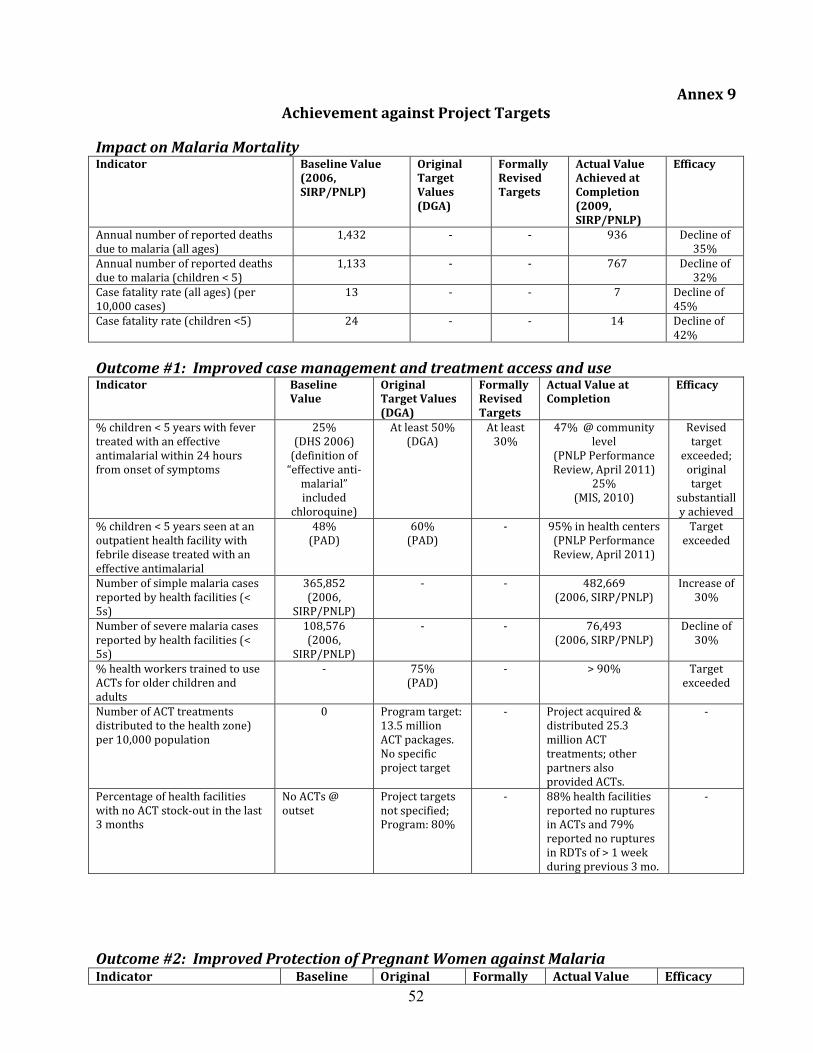
52
Annex 9
Achievement against Project Targets
Impact on Malaria Mortality Indicator Baseline Value
(2006, SIRP/PNLP)
Original Target Values (DGA)
Formally Revised Targets
Actual Value Achieved at Completion (2009, SIRP/PNLP)
Efficacy
Annual number of reported deaths due to malaria (all ages)
1,432 - - 936 Decline of 35%
Annual number of reported deaths due to malaria (children < 5)
1,133 - - 767 Decline of 32%
Case fatality rate (all ages) (per 10,000 cases)
13 - - 7 Decline of 45%
Case fatality rate (children <5) 24 - - 14 Decline of 42%
Outcome #1: Improved case management and treatment access and use Indicator Baseline
Value Original Target Values (DGA)
Formally Revised Targets
Actual Value at Completion
Efficacy
% children < 5 years with fever treated with an effective antimalarial within 24 hours from onset of symptoms
25% (DHS 2006)
(definition of “effective anti-
malarial” included
chloroquine)
At least 50% (DGA)
At least 30%
47% @ community level
(PNLP Performance Review, April 2011)
25% (MIS, 2010)
Revised target
exceeded; original target
substantially achieved
% children < 5 years seen at an outpatient health facility with febrile disease treated with an effective antimalarial
48% (PAD)
60% (PAD)
- 95% in health centers (PNLP Performance Review, April 2011)
Target exceeded
Number of simple malaria cases reported by health facilities (< 5s)
365,852 (2006,
SIRP/PNLP)
- - 482,669 (2006, SIRP/PNLP)
Increase of 30%
Number of severe malaria cases reported by health facilities (< 5s)
108,576 (2006,
SIRP/PNLP)
- - 76,493 (2006, SIRP/PNLP)
Decline of 30%
% health workers trained to use ACTs for older children and adults
- 75% (PAD)
- > 90% Target exceeded
Number of ACT treatments distributed to the health zone) per 10,000 population
0 Program target: 13.5 million ACT packages. No specific project target
- Project acquired & distributed 25.3 million ACT treatments; other partners also provided ACTs.
-
Percentage of health facilities with no ACT stock-out in the last 3 months
No ACTs @ outset
Project targets not specified; Program: 80%
- 88% health facilities reported no ruptures in ACTs and 79% reported no ruptures in RDTs of > 1 week during previous 3 mo.
-
Outcome #2: Improved Protection of Pregnant Women against Malaria Indicator Baseline Original Formally Actual Value Efficacy
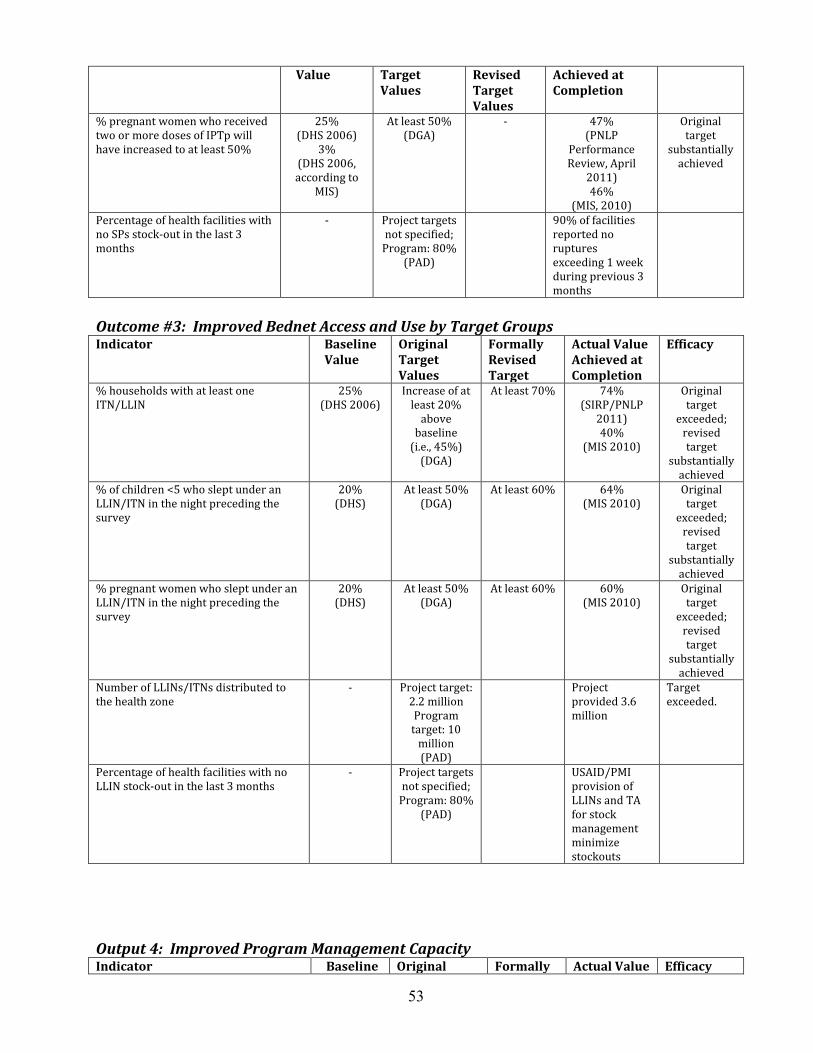
53
Value Target Values
Revised Target Values
Achieved at Completion
% pregnant women who received two or more doses of IPTp will have increased to at least 50%
25% (DHS 2006)
3% (DHS 2006, according to
MIS)
At least 50% (DGA)
- 47% (PNLP
Performance Review, April
2011) 46%
(MIS, 2010)
Original target
substantially achieved
Percentage of health facilities with no SPs stock-out in the last 3 months
- Project targets not specified;
Program: 80% (PAD)
90% of facilities reported no ruptures exceeding 1 week during previous 3 months
Outcome #3: Improved Bednet Access and Use by Target Groups Indicator Baseline
Value Original Target Values
Formally Revised Target
Actual Value Achieved at Completion
Efficacy
% households with at least one ITN/LLIN
25% (DHS 2006)
Increase of at least 20%
above baseline
(i.e., 45%) (DGA)
At least 70% 74% (SIRP/PNLP
2011) 40%
(MIS 2010)
Original target
exceeded; revised target
substantially achieved
% of children <5 who slept under an LLIN/ITN in the night preceding the survey
20% (DHS)
At least 50% (DGA)
At least 60%
64% (MIS 2010)
Original target
exceeded; revised target
substantially achieved
% pregnant women who slept under an LLIN/ITN in the night preceding the survey
20% (DHS)
At least 50% (DGA)
At least 60%
60% (MIS 2010)
Original target
exceeded; revised target
substantially achieved
Number of LLINs/ITNs distributed to the health zone
- Project target: 2.2 million Program target: 10
million (PAD)
Project provided 3.6 million
Target exceeded.
Percentage of health facilities with no LLIN stock-out in the last 3 months
- Project targets not specified;
Program: 80% (PAD)
USAID/PMI provision of LLINs and TA for stock management minimize stockouts
Output 4: Improved Program Management Capacity Indicator Baseline Original Formally Actual Value Efficacy
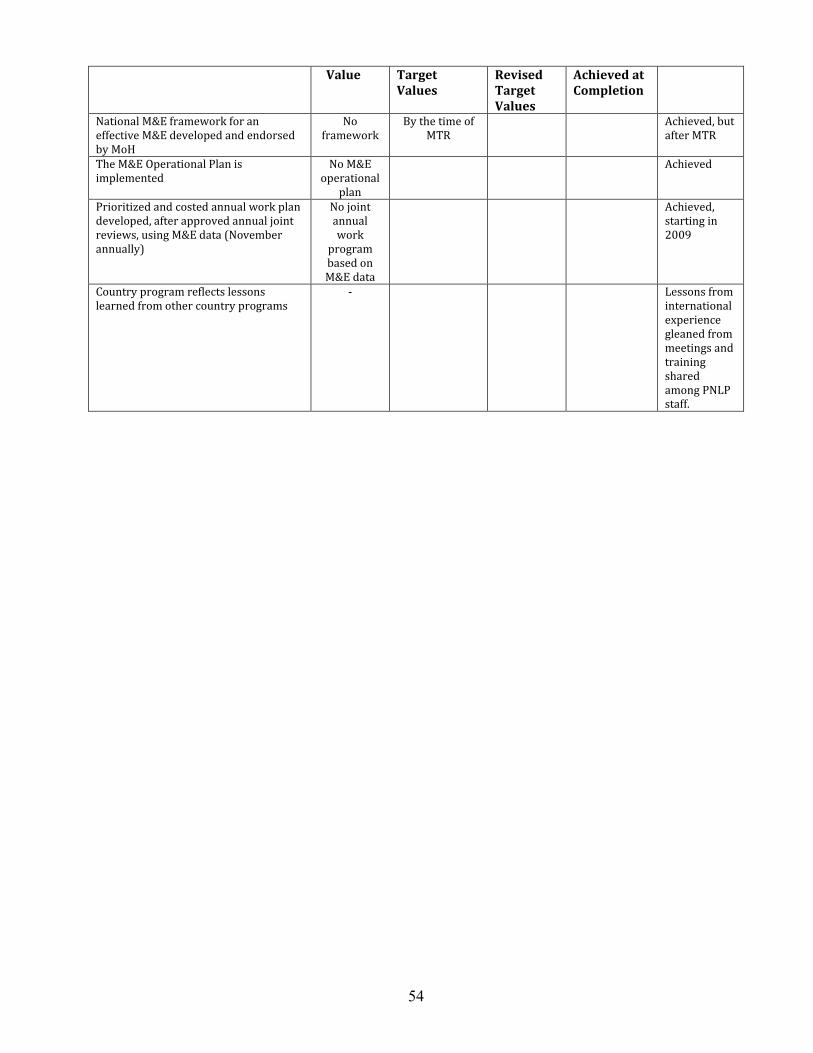
54
Value Target Values
Revised Target Values
Achieved at Completion
National M&E framework for an effective M&E developed and endorsed by MoH
No framework
By the time of MTR
Achieved, but after MTR
The M&E Operational Plan is implemented
No M&E operational
plan
Achieved
Prioritized and costed annual work plan developed, after approved annual joint reviews, using M&E data (November annually)
No joint annual work
program based on M&E data
Achieved, starting in 2009
Country program reflects lessons learned from other country programs
- Lessons from international experience gleaned from meetings and training shared among PNLP staff.
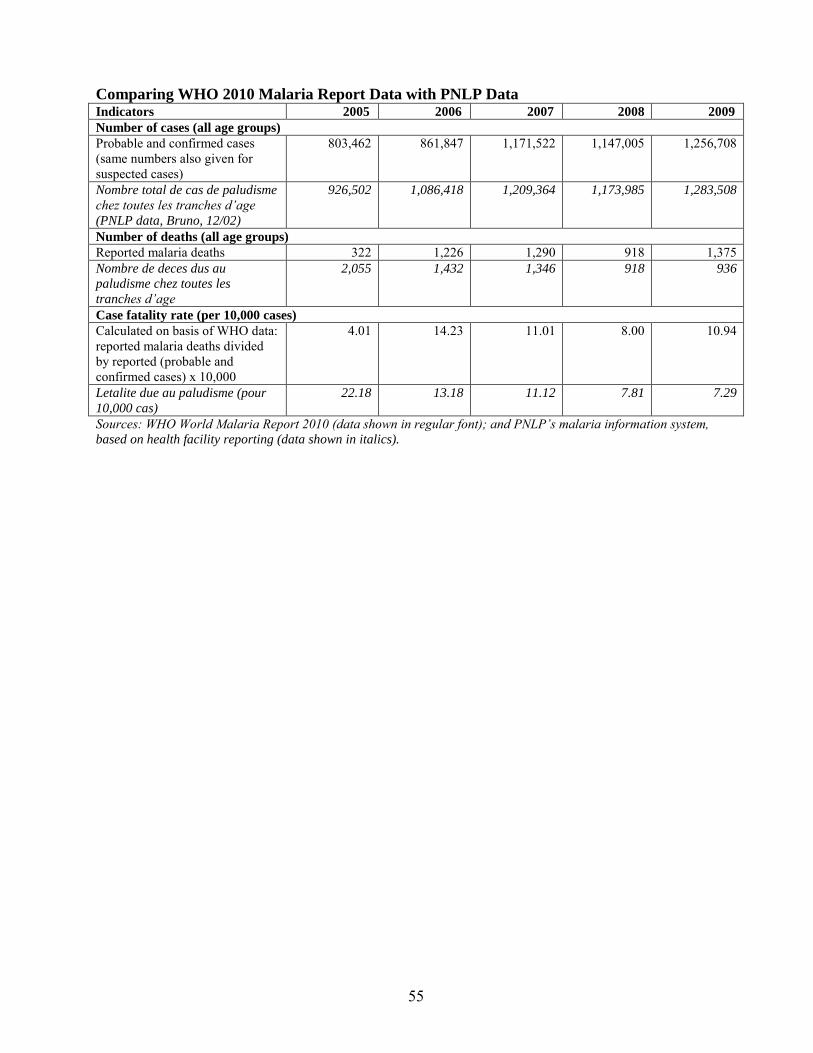
55
Comparing WHO 2010 Malaria Report Data with PNLP Data Indicators 2005 2006 2007 2008 2009
Number of cases (all age groups)
Probable and confirmed cases (same numbers also given for suspected cases)
803,462 861,847 1,171,522 1,147,005 1,256,708
Nombre total de cas de paludisme
chez toutes les tranches d’age
(PNLP data, Bruno, 12/02)
926,502 1,086,418 1,209,364 1,173,985 1,283,508
Number of deaths (all age groups) Reported malaria deaths 322 1,226 1,290 918 1,375 Nombre de deces dus au
paludisme chez toutes les
tranches d’age
2,055 1,432 1,346 918 936
Case fatality rate (per 10,000 cases) Calculated on basis of WHO data: reported malaria deaths divided by reported (probable and confirmed cases) x 10,000
4.01 14.23 11.01 8.00 10.94
Letalite due au paludisme (pour
10,000 cas)
22.18 13.18 11.12 7.81 7.29
Sources: WHO World Malaria Report 2010 (data shown in regular font); and PNLP’s malaria information system,
based on health facility reporting (data shown in italics).
56
Annex 10
List of Persons Met
Benin
Cotonou
Ministry of Health
Office of the Minister
Dorothée A. KINDE GAZARD, Ministre de la Santé Yacoubou IMOROU KARIMOU, Conseiller, Santé de Travail (ancien Coordonnateur PNLP pendant 3
ans Office of the Director of Cabinet
Docteur Marie Rose NAGO, Pédiatre, Directrice de Cabinet Secretariat General
DocteurValere Goyito, Secrétaire Général du Ministère Direction de la Programmation et de la Prospective
AKPAMOLI Alphonse D., DirecteurAdjoint de la Programmation et de la Prospective (jusqu’au 21 septembre 2011), Coordonnateur Programme Renforcement du système de la santé (RSS) (à partir du 22 septembre 2011)
Hoteyi A. Mathilde, SEP/DPP Alakpo A. Sanoussi, SGSI/DPP Kessou Daniel Abalo, SC, DPP Akpamagbo Clément, SP/DPP do Rego, Dominique, CSE, DPP Amoussou Raymond, DAPP/DBB Direction des Pharmacies, du Médicament et des Explorations Diagnostiques
Loko Frederic, Directeur DNSP
Dr Orou Bagou YOROU CHABI, Directeur National de la Santé Publique (DNSP) Direction de la Santé de la Mère et de l’Enfant (DSME)
Dr. Olga Agbohoui-Houinato, Pediatre, Directrice DSME Agence Nationale de Vacination –Soins de Santé Primaires [ancien Programme Elargi de
Vaccination (PEV)]
Dr N’Déye Marie BASSABI-ALLADJI, Directrice :
Programme National de Lutte contre le Paludisme (PNLP)
Marie-Agnès AGBOTON-ZOUMENOU, Médecin de Santé Publique, Paludologue, Coordonnatrice du PNLP
DENON Yves Eric Donan, Coordonnateur Adjoint ADJIBABI B. Cherifatou, Chef Service Pharmacie, Pharmacovigilance AHOLOUKPE N. Bruno, Chef Service Suivi Evaluation OKE Mariam, Chef Service Surveillance Epidémiologique
57
CHAFFA Evelyne, Chef Service Lutte Anti Vectorielle Intégrée ADJARO Boukari Jeremie, Chef Service Information, Education et Communication TOKPONON T. Filemon, Service Lutte Anti Vectorielle Intégrée TOHUNGODO Geoffroy Dominique, Chef Service Financier et Comptable DENAKPO Boni Y. Dessowu, Chef Service Interventions à Base Communautaire Partenariat-Plaidoyer ADOGNON C.A. Dede Larissa, Chef Service Secrétariat Administratif GNINTOUNGBE E. Eve, Service Prise en Charge des Cas et Traitement Préventif Intermittent ANANI Kouessi, Service Laboratoire et Chimiosensibilité AKAKPO Evelyne J. Cossiba, Service Lutte Antivectorielle Intégrée FASSINOU Hector, Service Lutte Antivectorielle Intégrée SIANOU Antoine, Service Laboratoire et Chimiosensibilité AKOUETE A. Julienne, Service Communication VIAKINNOU Coffi Alexandre Rodrigue, Magasin PNLP HABIBOU Florent, Chef Service Administratif et Logistique AGBAKOU Félix, Gestionnaire du PALP MEVO Valéry, Spécialiste en passation des marchés
Centrale d’Achat des Médicaments Essentiels et Consommables Médicaux (CAME)
Emmanuel Yaovi TOSSOU, Pharmacien, Responsable Unité de Gestion des Programmes Spécifiques
International Development Partners
Africare
Josette Vignon Makong, MD, MPH, Directrice Pays, Africare-Bénin/Côte d’Ivoire Dr. Rachade Zime NAKOU, Pharmacien, Spécialiste en Gestion des Achats et Stocks Ahmed Rachid Moustapha, Responsable Financier HOUNNANKAN Cossi Athanase, MD/MPH, Eco Santé, Chargé de projet Catholic Relief Services
Christophe Droeven, Représentant Résident, Programme du Bénin et du Togo Dr. Seraphin Yaovi VISSOH, MD, MPH, Socio-Anthropologue PSI
Megan Wilson, Directrice Adjoint-Programmes Njara RAKOTONIRINA, Responsable de Département Santé Maternelle et Infantile Bienvenu Wakpo, Coordonnateur Programme Paludisme
United Nations Children’s Fund (UNICEF)
Hortense Désirée KOSSOU, Spécialiste Santé (Développement des Politiques et Stratégies) et ancienne Coordonnatrice, PNLP de 2005 à 2008 (ans)
Gilbert VISSOH, Spécialiste Santé/PCIME
United Nations Fund for Population Activities (UNFPA)
Theodore Soudé, Représentant Assistant
United States Agency for International Development (USAID)
Milton B. Amayun, MD, MPH, Family Health Team Leader Abdou Salam Gueye, MD, MPH, PHD, President’s Malaria Initiative (PMI)/Centers for Disease Control
and Prevention (CDC), Resident Advisor, PMI/Benin Cheryl Combest, Technical Assistant to USAID
58
World Bank
Fily d’Almeida, Task Team Leader, Projet d’Appui à la Lutte contre le Paludisme World Health Organization
Akpa Raphael GBARY, Dr Med, PhD, Resident Representative Département de Borgou/Alibori
Direction Départementale de la Santé, Parakou
Dr. Fatioulaye ISSA DJIBRIL, Directeur Départemental de la Santé Dr GADO Kora : Chef du Service Protection et Promotion Sanitaires Gnimavo Dominique, Infirmier, Cellule, PNLP Ezin Raymond, Assistant Social, Cellule, PNLP Zone Sanitaire de Tchaourou
Dr AÏFA Joachim :Médecin coordonnateur de la Zone Sanitaire Dr FADONOUGBO Xavier Médecin chef de Tchaourou M. DJINAHIN Félicien : responsable de la statistique et technicien de laboratoire MAMA SOUMOU Fousséni : Charge de la mobilisation sociale ADOUNVO Gélase : Chargé de l’Administration et des Ressources Centre de Santé, Tchatchou
M. SRACE Lucien : Infirmier Major, responsable du dispensaire
Mme GOURMA Barakatou : Sage femme
Président/Comité de Développement de l’Arrondissement Président, Comité de Gestion (COGES) M. SOULE Tarouwèrè, Membre, COGECS
Aide soignant Animatrice
ONG contractuelle pour l’appui communautaire
Département de Zou-Collines
Direction Départementale de la Sante, Abomey
Dr KOSSOUHO François, Directeur Departemental de la Santé, Abomey Dr. Agbangbla, Yves, Cellule PNLP Centre de Santé, Commune de Zakpota
Dr Serge TOUDONOU: Médecin chef, Centre de Santé M. TCHANHOU Cosme : Infirmier, Centre de Santé Mme DEGBEGNI Adèle : Sage femme, Centre de Santé M. GNONLONFOUN junior et M. Denis AKOUTEY : Equipe de laboratoire, Centre de Santé Relais communautaire (3) : Mme BOVIS Marcelline, M. KPOGBE Toussaint et Mme AGBAÏZO
Julienne Membres du COGECS : M. DJEVO Clément, M. BEKPON Georges et M. ADODJO Raymond Workshop Participants, Hotel Nifur, Bohicon
There were forty participants to this workshop, including substantial representation from community-level, civil society, elected officials, operational-level service providers and managers,
59
as well as central-level MoH staff. List of participants is provided in the Stakeholder Workshop Results Annex.
Senegal, Dakar
Christophe Lemière, Task Team Leader, Benin Health Systems Performance Project
U.S.A., Washington
John Paul Clark, Senior Technical Specialist, World Bank, AFTHE
60
Annex 11
List of Supporting Documents
European Union
Conseil Sante Consortium. 2011. “Etude sur les Comptes Nationaux de la Sante 2008 Ŕ Benin,”
Rapport final. Janvier.
République du Bénin
Institut National de la Statistique et de l’Analyse Economique (INSAE) [Benin] et Macro International, Inc. 2007. “Enquête Démographique et de Sante, Benin 2006: Rapport de
Synthèse,” Calverton, Maryland, USA: INSAE et Macro International. Décembre. République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2011. “Transmission des
indicateurs de fin de projet.” 25 Aout.
République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2011. “Plan Stratégique National
de Lutte contre le Paludisme: 2011 Ŕ 2015.” (Draft 1) Juillet.
République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2011. “Plan Stratégique National
de Lutte contre le Paludisme au Benin 2006-2010 Ŕ Etude des stratégies de pérennisation des
acquis de la mise en œuvre du plan stratégique 2006-2010.” Par Dr. Nuons Assomption,
Consultant sous financement de la Banque Mondiale. Mai. République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2011. “Revue de Performance du
PNLP.” Aide-Memoire. Mars. République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2009. “Plan intègre des activités
de la lute contre le paludisme pour l’année 2009 au Benin.” (produit avec l’appui technique et
financier de PISAF Ŕ Projet Intègre de Sante Familiale, et exécuté par URC – University Research Corporation – avec Abt Associates, under USAID Cooperative Agreement). Mars. République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2006. “Plan de suivi et
d’évaluation du plan strategique de lute contre le paludisme au Benin 2006-2010.” Décembre. République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2006. “Budget du Projet d’Appui a
la Lutte contre le Paludisme (Booster Program for Malaria Control).” 20 Novembre.
61
République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2006. “Résumé du Projet de Plan
Stratégique de Lutte contre le Paludisme au Benin National 2006-2010.” Février.
République du Benin, Ministère de la Sante Publique, Direction Nationale de la Protection
Sanitaire, Programme National de Lutte Contre le Paludisme. 2005. “Politique Nationale de
Lutte contre le Paludisme et Cadre Stratégique de Mise en Œuvre.” Novembre.
République du Benin, Ministère de la Sante Publique, Secrétariat General du Ministère, Direction
de la Programmation et de la Prospective, Service de la Gestion du système d’Information. 2010.
“Plan Stratégique de Renforcement du Systeme National d’Information et de Gestion Sanitaires
2011-2015,” Décembre.
République du Benin, Ministère de la Sante Publique, Secrétariat General du Ministère, Direction
de la Programmation et de la Prospective. 2009 (?). “Plan National de Développement Sanitaire
(2009-2018).
République du Benin, Ministère de la Sante Publique, Secrétariat General du Ministre, Direction
de la Programmation et de la Prospective. 2009. “Rapport sur l’Etat de la Sante au Benin en
2008.” Appuyé par la Confédération Suisse. 1ère édition. Décembre.
République du Benin, Ministère de l’Economie et des Finances. 2010. “Réallocation des fonds du
Don IDA et réajustement de certains indicateurs de performance dans le cadre du Projet d’Appui à
la Lutte contre le Paludisme (PALP).” Avril.
UNICEF
Bureau d’études et de soutien aux technologies en santé et développement. 2010. “Etude sur la
cartographie des interventions et intervenants en Sante Maternelle Néonatal et Infantile (SMNI), y
compris la communication pour le développement au Benin.” Avec l’appui de l’UNICEF. Rapport
provisoire. Version 2. Décembre.
USAID
Plan International, Abibou Mamadou and Modeste Anato. 2009. “Collaborative Approach to Community-based Malaria Prevention in Benin.” National Conference/Final Evaluation Report. Financed by USAID/Health Care Improvement Project. August. USAID. (No date). “President’s Malaria Initiative Benin Malaria Operational Plan FY2011.” USAID. 2011. “Audit of USAID/Benin’s Implementation of the President’s Malaria Initiative,” Audit Report No. 7-680-11-004-P, February 14. Aide-Memoires (series) ISRs (series) World Bank
62
World Bank. 2011. “Annonce mission de préparation du rapport d’achèvement PALP.” Lettre. 8
Aout.
World Bank. 2011. “Projet d’Appui a la Lutte contre le Paludisme au Benin/PALP Ŕ (H229-BEN)
Préparation du Rapport d’Achèvement” Guidelines for Government to prepare ICR. January 10. World Bank. 2010. Letter to Ministre de l’Economie et des Finances. “Projet d’Appui a la Lutte
contre le Paludisme (Don H229-BEN) Prorogation de la Date de Clôture du Projet,” September 14. World Bank. 2010. “Restructuring Data Sheet,” July 23. World Bank. 2010. “Restructuring Paper for Benin: Malaria Control Support Project – P096482.” Memorandum. July 21. World Bank. 2010. “Restructuring Paper on a Proposed Project Restructuring of Benin Malaria Control Support Project Grant H229-BEN, Republic of Benin.” Health, Nutrition and Population (AFTHE), Africa Region, July 21. World Bank. 2010. “Quality Assessment of Lending Portfolio (QALP-2) Final Report,” July 19. World Bank. 2010. Letter to Minister of Economy and Finance. “Benin – Projet d’Appui a la Lutte contre le Paludisme (Don H229-BEN) Réallocation de fonds et amendements aux indicateurs-clés de performance du Projet,” 28 Avril. World Bank. 2010. “Restructuring Paper on a Proposed Project Restructuring of Benin Malaria Control Support Project Grant H229-BEN Republic of Benin,” April 27. World Bank. 2010. “Project Appraisal Document on a Proposed IDA Grant in the Amount of SDR 14.9 million (US$22.8 million equivalent) of which SDR 5.1 million originates from Pilot CRW Resources (US$7.8 million equivalent) to the Republic of Benin for a Health System Performance Project.” April 9. World Bank. 2009. “Republic of Benin Health, Nutrition and Population, Health & Poverty Analytical Report,” Carried out jointly with Ministry of Public Health, with the support of the Global Alliance for Vaccines and Immunization (GAVI), UNICEF and the French Ministry of Foreign and European Affairs (MAEE), May. World Bank. 2009. “Country Assistance Strategy for the Republic of Benin for the Period FY09-12,” Country Department for Benin, Africa Region. January 30. World Bank. 2006. Incoming letter from MS/PNLP. “Budget du Projet d’Appui a la Lutte contre
le Paludisme (Booster Program for Malaria Control). November. World Bank. 2006. “Development Grant Agreement (Malaria Control Support Project) between Republic of Benin and International Development Association,” November 9. World Bank. 2006. “Project Appraisal Document on a Proposed Grant in the Amount of SDR 21.60 million (US$31 million equivalent) to the Republic of Benin for a Malaria Control Support Project,” Human Development II, Africa Region, May 3.
63
World Bank/Banque Mondiale. 2005. “Projet Booster de Lutte contre le Paludisme au Benin,
Programme de gestion des dechets issus des soins de santé, Rapport final,” par Mbaye Mbengue
Faye et Andre Soton, Janvier.
WHO
World Health Organization. 2010. “Guidelines for the Treatment of Malaria,” Second Edition. Other
d’Almeida et al. 2011. Parasites & Vectors. “Field evaluation of the intermittent preventive treatment of malaria during pregnancy (IPTp) in Benin: evolution of the coverage rate since its implementation,” June 16. “Protocol d’Accord de Compact entre le Gouvernement de la Republique du Benin et les
Partenaires Technique et Financiers relative a la Mise en Oeuvre du PTD 2010-2012 en vue
d’Atteindre les Objectifs du Millenaire pour le Developpement,” signe par: le Ministre de la Sante,
le Ministre de l’Economie et des Finances, et les Representants de: l’OMS, l’UNICEF, l’UNFPA,
l’Ambassade de Belgique au Benin, et la Banque Mondiale. (IHP+), 2010. (Hard copy only)
“Vector/Pest Management Plan” , Executive Summary. Benin Malaria Control Support Project. (No date).
ZouZou
CouffoCouffo
Ouémé
OuéméM
onoM
ono
SotaSota
Tassi
néTa
ssiné
Okp
ara
Okp
ara
Alp
ouro
Alp
ouro
Mék
rou
Mék
rou
AliboriAlibori
Mékro
u
Mékro
u
Panja
riPa
njari
NIGER RIVER
NIGER RIVER
BIGHT OF BENINBIGHT OF BENIN
LakeLakeVoltaVolta
LakeLakeKainjiKainji
OOuuéémm
éé
M O N OM O N O
COUFFOCOUFFO
B O R G O UB O R G O U
A L I B O R IA L I B O R I
ATA K O R AATA K O R A
C O L L I N E SC O L L I N E S
D O N G AD O N G A
Z O UZ O U
ATLANTIQUEATLANTIQUE
LITTORALLITTORAL
OU
EME
OU
EME
PLATEAUPLATEAU
PobéPobé
BohiconBohicon
AplahouéAplahoué
CovéCové
MalanvilleMalanville
Dassa-Dassa-ZouméZoumé
BembérékéBembéréké
AbomeyAbomey
CotonouCotonou
SakétéSakété
LokossaLokossa
DogboDogbo
ParakouParakou
NatitingouNatitingou
KandiKandi
OuidahOuidah
SavalouSavalou
DjougouDjougou
PORTO NOVOPORTO NOVO
AAtt aa kk oo rr aa MM
oo uu nn tt aa ii nn ss
M O N O
COUFFO
B O R G O U
A L I B O R I
ATA K O R A
C O L L I N E S
D O N G A
Z O U
ATLANTIQUE
LITTORAL
OU
EME
PLATEAU
Pobé
Bohicon
Aplahoué
Cové
Malanville
Dassa-Zoumé
Bembéréké
Abomey
Cotonou
Sakété
Lokossa
Dogbo
Parakou
Natitingou
Kandi
Ouidah
Savalou
Djougou
PORTO NOVO
TOGO
GHANA
NIGERIA
NIGER
BURKINAFASO
Zou
CouffoOuémé
Mono
Sota
Tassi
né
Okp
ara
Alp
ouro
Pendjari
Mék
rou
Alibori
Mékro
u
Panja
ri
NIGER RIVER
BIGHT OF BENIN
LakeVolta
LakeKainji
Koumongou Oué
mé
Gulf of Guinea
At a k o r a M
o u n t a i n s
To Dapaong
To Sokoto
To Dosso
To Kaiama
To Kabou
To Lomé
To Notsé
To Ibadan
0
0
1E
1E
2E
2E
3E
1E
3E 4E
7N
8N 8N
7N
9N 9N
10N 10N
11N 11N
12N
BENIN
This map was produced by the Map Design Unit of The World Bank. The boundaries, colors, denominations and any other informationshown on this map do not imply, on the part of The World BankGroup, any judgment on the legal status of any territory, or anyendorsement or acceptance of such boundaries.
0 604020 80
0 20 40 60 Miles
100 Kilometers
IBRD 33372
DECEMBER 2005
BENINSELECTED CITIES AND TOWNS
DEPARTMENT CAPITALS
NATIONAL CAPITAL
RIVERS
MAIN ROADS
RAILROADS
DEPARTMENT BOUNDARIES
INTERNATIONAL BOUNDARIES