Embed Size (px)
Citation preview

The image of the children's nurse: a study of the qualities
required by families of children's nurses' uniform
STEVESTEVE CAMPBELLCAMPBELL BNurs, PhD, RGN, RSCN, NDN Cert , RHV, FRSH
Principal Lecturer and Head of Division of Children's Nursing and Learning Disabilities Nursing,
Faculty of Health, Social Work and Education, University of Northumbria at Newcastle,
NE7 7X41
CHRISTINECHRISTINE O'O'MALLEYMALLEY Dip HE, BSc, Adv Dip Health Sciences ,
RN(Chi ld)
Staff Nurse, PICU, The Newcastle Upon Tyne Hospitals NHS Trust, Newcastle General
Hospital, Westgate Road, Newcastle Upon Tyne, NE4 6BE
DONDON WATSONWATSON BA, MPhil , PhD, C Psychol , AFBPsS
Emeritus Professor in Applied Psychology, Faculty of Health, Social Work and Education,
University of Northumbria at Newcastle NE7 7XA
JANJAN CHARLWOODCHARLWOOD BA, RGN
Staff Development Manager, The Brendon Care Foundation, The Old Malthouse, Victoria Road,
Winchester S023 7DU
SUSANSUSAN MM. LOWSONLOWSON DMS, MA (Qual Mgt) , RGN, RSCN
Quality Development Manager, Southampton University Hospitals NHS Trust Tremona Road,
Southampton, S019 4XY
Accepted for publication 7 May 1999
Summary
· Traditional views of the nurse see `her' in a nurse's uniform, whether she be a
`sex symbol', `angel of mercy' or `battle axe'. Children's nursing has, over recent
years, moved away from the idea of the uniform into more child friendly clothes,
though the traditional uniform is still presented to the public by the media.
· The staff members of a Children's Outpatients Department (COPD) of a large
acute hospital requested knowledge of the qualities families required from the
uniform of nurses caring for them, prior to any change in uniform. This study
aimed to develop an understanding of these qualities via the use of a survey
presented to those attending the COPD.
· The ®ndings indicate that there is a complex relationship between the qualities
that families wish the uniform to present. A balance is needed between
presenting a professional authority ®gure, providing security for families and
suggesting an approachable ®gure, to allow effective communication between
staff and families.
Journal of Clinical Nursing 2000; 9: 71±82
Ó 2000 Blackwell Science Ltd 71

Keywords: atmosphere, children's nurse, communication, identi®cation, patient
con®dence, uniform.
Introduction
In the UK there has been a recent trend for children's
nurses to dispense with traditional uniforms. Glasper &
Miller (1992) have suggested that this re¯ects a desire to
make hospital environments more child friendly and
family centred. However, there has been little research
about the impact this has on families and about their views
on traditional uniform. Consequently, when a change in
uniform was proposed in the Children's Outpatients
Department (COPD) of an acute NHS trust, a study was
conducted to investigate the families' perspective on this
issue.
The nature of uniform in society
In order to set this study in context it is important to
consider some historical and fundamental issues about the
nature and role of uniform.
PURPOSE OF UNIFORMPURPOSE OF UNIFORM
Both uniformed organizations and the public view
the uniform as ideology, the former to proffer a
desired image to outsiders, the latter to retain
cherished emotive symbols. (Joseph, 1986; p. 116)
The essence of this statement is the belief that uniform
projects information about the identity of its wearers. It
informs about what they do and the qualities and attitudes
that can be expected of them. Thus uniform is used
explicitly as a form of communication and is interpreted
implicitly by individuals. Such communication takes place
among three participants: the wearer, the organization and
members of the public, individually and en masse.
Besides its role in transmitting information, uniform
also has an obvious, though perhaps secondary function, of
practical expediency. Smith (1990) suggests that uniform
can be viewed from these two perspectives, the intellectual
and the practical. Coombes & Heilman (1993) refer to
uniform in general as a non-verbal method of communi-
cation that denotes status, occupation, authority and
power, while Joseph (1986) also ®nds that uniform is a
method of communicating relationships both within and
without an organization. This involves the communication
of control implied by the `cluster of values and norms
which support these relationships' (Joseph, 1986; p.2) and
which affect the manner of communication between the
uniform wearer and the public. Uniform has a powerful
effect on the public, often bestowing on the wearer status
and a `certi®cate of legitimacy' (Joseph & Alex, 1972) to
invade physical and personal space. Nurses in particular
are endowed with this licence of safety, and children and
their families still tend to recognize a nurse by identi®-
cation with a uniform (Livingstone, 1995).
Brennan et al. (19952 ) recognizes the practical role of
uniform in nursing, in terms of maintaining cleanliness,
promoting freedom of movement and identifying the
wearer as a member of the nursing profession. However,
the role of the uniform in hygiene and infection control is
dubious, and nurses have been found to pay more
attention to infection control whilst wearing their own
clothes (Sparrow, 1991). Moreover, the promotion of free
movement has been limited by traditional uniforms
(Castledine, 1987). Its role in identifying nurses may be
questioned in the light of the ease of access to nurses'
uniforms and possibility of abuse of this status.
THE HISTORICAL DEVELOPMENT OF NURSES'THE HISTORICAL DEVELOPMENT OF NURSES'
UNIFORMSUNIFORMS
Three different vocations had a strong in¯uence on the
evolution of the role of the nurse: the church, the military
and the servant (Tiffany & Sparrow, 1987; Davies, 1995).
Each of these affected the way traditional nurses' uniforms
developed. Religious orders throughout history have cared
for the sick and dying, and nurses adopted the discreet
attire of the nun including a headdress similar to a wimple.
The military history of nursing dates from the period of
Nightingale during the Crimean war. She presented
nurses with a militaristic uniform of buckles, badges and
stripes, because they were working with soldiers who were
socialized into respecting the emblems of rank and
uniform. The servant-like uniform of nurses in cap and
apron also developed during the mid 19th century to
distinguish between trained nurses from religious and
military training institutions and the morally questionable
untrained nurses who offended the Victorian propriety of
the day (Tiffany & Sparrow, 1987; Davies, 1995).
PERCEPTIONS OF UNIFORMSPERCEPTIONS OF UNIFORMS
There are con¯icting views about perceptions of nurses'
uniforms. The symbolic role of representing care, com-
passion and authority can be seen as advantageous, and
many nurses claim to wear it with pride. At the same time
72 S. Campbell et al.
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82

it carries with it the confused stereotyping of nurses as sex
symbols, battle axes or angels of mercy (Nightingale,
1983), images which tend to be exploited and exaggerated
by the media.
An alternative view refers to the intellectual perception
of uniform as an outdated mode of dress for independent
professionals. It relates to a history of subservience no
longer appropriate for contemporary nursing, which has
already been abandoned in some ®elds such as mental
health and learning disabilities. MacFarlane (1990) adds to
the debate by questioning the legitimacy of formally
prescribing uniform for a set of professionals. This view
also regards uniform as counterproductive to the devel-
opment of a therapeutic relationship in which nurse,
patient and family are partners in care (Casey, 1988).
Uniform: a conceptual framework
An analysis of the meaning of uniform in general and of
nurses' uniform in particular identi®es the recurrent
themes of communication and stereotyping. A framework
may be constructed around these issues to allow some
theoretical consideration of the importance of nurses'
uniform, and to indicate what implications there may be
for nurses.
The literature indicates that uniform is seen as the
embodiment of social expectations of the nurse: it
visualizes the stereotype, and in so doing provides the
public with an obvious source of communication about the
healthcare system (Livingstone, 1995). It helps in com-
munication between the public and healthcare profession-
als by acting as a passport in initiating personal and
physically intimate relationships. Such communication is
generated by public expectations of what the uniform
symbolizes, irrespective of the quali®cation of the wearer
(Sparrow, 1991).
Stewart et al. (1979) point out that stereotyping ®rst
became a prevalent issue in psychology in the 1920s, but
since that time corruption of the concept has made it an
almost derogatory term. They analysed the work of
Cauthen et al. (19713 ) examining the traditional view of
stereotyping and concluded that as a method of grouping
behaviour it is a concept
¼ in which a single characteristic or label serves to
elicit a set of expectations or attributions which are:
1 too simple to describe accurately the class of
person (or any of its members) and, at the same time,
are
2 too broadly generalized to individuals to have
more than occasional validity. Additionally, it is
sometimes assumed that stereotypes are
3 particularly rigid and resistant to change.
(Stewart et al., 1979, p. 2)
They viewed previous de®nitions of a stereotype as too
simple and suggested that a contemporary conceptualiza-
tion of the process of stereotyping could be found within
the psychology of cognition, development of a stereotype
being equivalent to development of a schema. A schema is
characterized, within the cognition process, as a mental
operation, cultivated through experience, that is used to
understand new factors in the environment of the subject
by comparison with previous knowledge. Stereotypes arise
because information about new factors in the environment
is too complex, incomplete or ambiguous to rationalize
into individual perceptions. Because of this, stereotypes
are used as a means of categorizing such information.
Stewart et al. (1979) also refuted the notion that stereo-
types present rigid parameters for the perceptions that
could be contained within them, arguing that, like
schemata, stereotypes alter with experience.
The principal stereotype of the nurse and its visual
presentation by uniform has developed as the culmination
of three branches of the profession's origins, the servant,
religious and military backgrounds (Davies, 1995). The
notion of the nurse as a kindly handmaiden following
doctors' orders is wrapped up, quite literally, in nurses'
uniforms. This schema is maintained and supported by the
media, which usually portray nurses in traditional uniforms,
thus maintaining the stereotypical perception. This view of
the nurse seems to be one with which society is comfortable,
as most research indicates a preference for traditional
uniforms. Research ®ndings also indicate that traditional
uniforms present the expected image of the nurse and
increase the con®dence of those experiencing physical
treatment (Hawkey & Clark, 1990; Meyer, 1992; Marr &
Matthews, 1993; Rowland, 1994; Livingstone, 1995).
However, according to Stewart et al. (1979), stereotypes
can be altered and updated. Consequently, the outdated
view of the modern professional nurse as `handmaiden'
may be changed by the development of a schema
incorporating directly observed information about nurses
and their uniforms, thus producing an updated stereotype.
Such an acceptance has direct implications for the
representation and practice of nurses. It suggests that
acceptance of the public's perceptions and preferences
merely prolong the traditional stereotype and do nothing
to alter it.
The study
Children attending outpatients departments bring with
them a variety of experiences. They may be acutely or
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
Users' experiences of care Children's nurses and uniform 73

chronically ill, they may have already experienced hospi-
talization, and they will have almost certainly been
exposed to representations of hospital by the media.
In the Child Health Directorate of a busy, acute NHS
trust, nurses on the wards wore an alternative uniform
(polo shirts, colour coded to the practice area, with the
choice of trousers, skirts or shorts in navy blue). However,
nurses in COPD still wore traditional uniforms. Although
they were considering change, they were reluctant to do so
without good reason, and they felt suspicious that the
decision had already been made for them to adopt the
alternative style. The aim of the research was to establish
the perceptions of families, nurses and other healthcare
professionals in relation to nurses' uniforms. The results
of the research were to be the basis on which nursing staff
made a collective decision on whether to change uniform.
Methods
A method was designed using interview and questionnaire
techniques to explore families', nurses' and other health
care professionals' perceptions of nurses' uniform in
COPD. Ethical consent was gained prior to the com-
mencement of the interviews.
Stage one: the interviews
An inductive approach was taken initially, to develop a
tool that would identify factors which families considered
important about uniforms. This took the form of open-
ended, in-depth interviews with a group of families and
with a group of staff from a variety of professions
including nursing. Using a grounded theory approach
(Glaser & Strauss, 1967), the interviews were expected to
identify key categories that could be used for further
quantitative analysis of the views of families in the COPD.
In order to reassure the COPD nurses that their
involvement was valued, all were interviewed (n� 12). A
sample of paediatricians (n� 3) and a single representative
from the other professions (i.e. physiotherapist, dietician,
administrative assistants) were also involved (n� 5). In all
20 families were interviewed, two from each half-day
session in COPD. These COPD sessions are mainly
organized according to paediatric speciality, with general
paediatric problems included on most days. Families were
largely represented by mothers, and also by some older
children. Interviews of the professional and family groups
went on in parallel; it was concluded data had reached
saturation when constant comparison ceased to highlight
new areas of interest (Glaser & Strauss, 1967).
Interview ®ndings
The ®rst and clearest category to emerge from the constant
comparison of data was that of identi®cation by uniform.
Families expressed a need to know whom to approach
about issues that they wanted resolved in the COPD. This
was also an issue for other health care professionals, who
wanted to be able to identify nurses correctly.
Both groups, families and healthcare professionals, felt
that nurses' clothing should distinguish them from parents,
although the latter group was less concerned about this.
Family members felt embarrassed about approaching the
wrong person, and also did not want to confuse other
parents by being mistaken for nurses themselves.
Besides anxieties about distinguishing nurses from parents,
concern was expressed about identifying quali®ed staff.
Families wanted to differentiate between nurses and care
assistants, and care assistants did not like being mistaken
for quali®ed nurses. This issue was also raised by health
care professionals who were new to the COPD (a
physiotherapist and a paediatric registrar).
It was also seen as important to be able to identify the
sister-in-charge; this was an issue for a large number of
family members and for health care professionals. Families
wanted to know who was in authority to deal with their
concerns and problems. Healthcare professionals expres-
sed a need to identify the person in charge as a matter of
recognition of seniority.
The second major category found in interviews con-
cerned the type of `atmosphere' uniform was expected to
generate, and the personal attributes that the nurse
wearing it was expected to hold. There was debate
relating to the type of atmosphere the uniform was
expected to foster: a relaxed approachable environment or
a clinical, authoritative, con®dent one.
Communication was the third category and related to
issues such as perceptions of the formality and friendliness
of the nurse in uniform.
It was accepted that the categories were inextricably
linked but that they were de®nitive issues for further
investigation. The categories identi®ed in the interviews
were referred back to the nurses involved, to con®rm their
validity. The nature of these categories was discussed, and
there was acceptance that they represented areas that were
important to both families and nurses. (One category that
had been identi®ed by nurses, the ease of laundering
uniform, was recognized as of little interest to families.) It
was also useful to involve nurses in validating categories
because it helped them to perceive the research process as
`transparent' and not hidden from them. They were
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
74 S. Campbell et al.

therefore less likely to misconstrue the process as a
conspiracy to force them to change uniform.
A similar process of validation was undertaken with six
individual families, again to identify whether their views
about uniform could be encompassed within these cate-
gories. Families found this process dif®cult, because they
needed to develop some understanding of the concept of
content validity. Nine statements were developed for use
in the questionnaire and there were no issues discussed
during interviews that could not be accommodated within
these statements. The ®ndings were therefore accepted as
valid by both the nurses and the families (other profes-
sional groups were not included in this process).
Second phase of the study
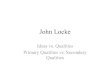
The nine statements were used as the framework for the
subsequent questionnaire (see Fig. 1). Because of the
Figure 1 The children's outpatient department questionnaire.
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
Users' experiences of care Children's nurses and uniform 75

diversity of children and families using COPD it was
decided to use as large a sample size as possible. A self-
report tool was required because of the large sample size
required. This also needed to assess the importance of
each of the statements to the families, and so it was
decided to use a tool based on a Likert-type scale.
Copies of the questionnaire were handed out to families
on registration at COPD by administrative staff and they
had the option to refuse to participate in the study. They
were then asked to return the form to the same place when
they came back to make their next appointment. Alto-
gether 500 copies of the questionnaire were distributed
and 430 (86%) were returned. No family refused to
participate.
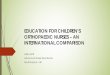
Findings
Findings are presented in three groups derived from the
themes identi®ed in the interviews: identi®cation, atmo-
sphere and communication (Fig. 2).
IDENTIFICATIONIDENTIFICATION
Statement 1: `It should be easy to identify nurses as nurses'
The results of Statement 1 illustrate that families
wanted nurses' clothing to allow them to be easily
identi®able as nurses (95% of the sample felt or
strongly felt that nurses should be clearly identi®able).
The inference is that people wish nurses to look like
nurses. However the statement does not ask in what
way nurses should be identi®able (there was a prefer-
ence for polo shirts rather than traditional uniform in
response to the ®nal question of the questionnaire). The
implication is that the role of the nurse is still associated
with a uniform that has been prevalent in the profession
throughout history and that the public wants nurses to
conform to their stereotypical schema. The preference
for polo shirts suggests, however, that this stereotype
may be changing.
Parents and children identify nurses by their uni-
forms. This identi®cation is based on historical stereo-
types and acceptance of the message given by uniform
and may provide the family with a false sense of
security. Livingstone (1995) found that children pre-
ferred the traditional style of uniform, perhaps because
it made them feel safer and reduced their confusion due
to their stereotypical, media-in¯uenced expectations of
nurses. Changing the way nurses present themselves
may have an impact on children's sense of security,
although it has been noted that children's preferences
can change when they experience more nurses dressed
less formally (Glasper et al., 1991). This seems to
indicate that there is potential for changing children's
stereotypes.
Statement 2: `It does not matter if nurses wear the same
kind of clothing as other staff or parents'
The purpose of Statement 2 was to identify whether
families were concerned about whether nurses wore
everyday clothing. In response to this, 67% disagreed or
strongly disagreed with the statement that `It does not
matter if nurses wear the same clothing as other staff or
parents'. The implication is that families want nurses to
appear physically different from other professionals and
the public.
The security provided by uniform may not only be
inappropriate but potentially hazardous. The assumption
that a person in uniform is a genuine nurse may have
serious child safety implications, and yet research shows
that people do make such assumptions. Franzoi (1988)
found that respondents identi®ed a nurse in traditional
uniform because such presentation met with expecta-
tions and yet failed to identify nurses in other clothing
such as `scrubs'. The implied security issue is that
uniform acts as a passport to patients and environments
without the need for validated identi®cation (Sparrow,
1991). The use of an informal uniform may, however,
stimulate patients, children and their families to ques-
tion the status of healthcare professionals, and to
recognize differences within the generic term `nurse',
thus developing different and more appropriate rela-
tionships with nursing staff. Consequently, there is an
implied need for education of patients and families on
appropriate identi®cation of staff.
Parents seem to want to be able to identify nurses easily
by their similar and distinctive clothes. It is important that
this need is met, whilst also taking into consideration
issues of security and other requirements of nurses'
uniform as put forward by families. The study did not ask
why families wanted to be able to identify nurses easily. It
would be interesting to pursue this question to give a
better insight into families' feelings about nurses and their
perceptions of the role.
Statement 3: `Nurses should wear the same kind of clothing'
The purpose of Statement 3 was to assess whether
different grades of nurses should wear the same kind of
clothing. The overall judgement on the statement at face
value was that they should (74%). However, re¯ection on
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
76 S. Campbell et al.

Statement 3 produced ambiguity of interpretation. This
ambiguity rests on whom the sample used as comparison
in deciding whether nurses should wear the same type of
clothing, i.e. does it matter, or should nurses wear the
same type of clothing as other nurses, other grades of
nurses, other health care professionals or the public? If one
assumes that the sample interpreted the statement as
intended then the results indicate that nurses should wear
the same type of clothing, irrespective of grade. It would
have been interesting to see whether the results would
have been consistent if Statement 3 had been presented
prior to Statement 2. It is possible that the group has
interpreted the statement accurately as they have already
indicated a preference relating to nurses' clothing in
respect to other professionals and the public.
Statement 4: `It is not important to be able to recognize
the Sister in Charge by the clothes that she wears'
Over 60% of the sample disagreed with this statement. The
need to identify the sister indicates that families still see the
sister as having responsibility for the care of the patient and
the nurse as carrying out sister's instructions. The
implication is that families are operating on a hierarchical
responsibility structure, in which the sister has responsi-
bility for the care of their child rather than a named nurse
under the auspices of the `Patient's Charter: Services for
Children and Young People' (Department of Health,
1996). Uniform may serve to perpetuate this outdated
mode of nursing, but parents want to be able to make this
distinction. It may be possible that those still seeking to be
able to identify the sister have not understood the concept
of the named nurse in family-centred care. The concept
may not have been conveyed clearly to parents, or they may
not have con®dence in the named nurse concept because of
the history of stereotyping of the nurse/sister relationship.
The implication therefore is that the public has a limited
understanding of the professional role, autonomy and
responsibility of the individual nurse: the stereotype of
handmaiden continues.
ATMOSPHEREATMOSPHERE
Statement 5: `The clothing that nurses wear should
promote a relaxed, clinical atmosphere'
The results of Statement 5 indicate that families wish
nurses to promote a relaxed atmosphere by the clothing
that they wear. Altogether, 90% of respondents agreed or
strongly agreed with the statement that clothing should
promote a relaxed clinical atmosphere.
The context of the term `atmosphere' relates to an
environment in which therapeutic relationships can be
promoted. In the past, the stereotypical hospital has been a
clinical, hierarchical, authoritarian institution run by
doctors and administered by servile ranks of nurses
(Davies, 1995). Such a culture may have contributed to
the fear of hospitals that appears commonplace in society.
The nursing profession has been attempting to alter this
perception, particularly where children are cared for, by
promoting models of care involving partnerships with
children and families (Casey, 1988). The aim is to create a
relaxed atmosphere in which families feel able to play an
equal role with nursing staff in caring for children in
hospital. This can only be achieved by developing
complementary relationships between staff and families,
which will be in¯uenced by the presentation of health care
professionals.
Rowland (1994) also supports the view that uniform can
affect the atmosphere of a relationship, and found that
traditional uniform was favoured for clinical tasks but that
the development of a therapeutic relationship was en-
hanced by a more casual uniform. Similar studies with
children have produced a variety of results. Meyer (1992)
found that children preferred to be cared for by nurses
wearing smock tops, and that they were frightened by
traditional uniform. Barrett & Booth (19444 ) assessed
children's preferences for doctors' uniforms, and found
that formal dress represented competence and was reas-
suring, whilst casual dress was seen as denoting friend-
liness and gentleness.
It can be seen from the literature that different styles
of dress meet different needs. Healthcare professionals
are perceived as more friendly when wearing casual
clothes, and this seems to contribute to the development
of a relaxed environment. However, more formal dress
carries with it an aura of competence and can instil
con®dence.
The results from Statement 5 raise the issue of whether
nurses aiming to produce a relaxed atmosphere can also be
assessed by their patients as being ef®cient. This has been
considered in previous papers; Kucera & Nieswiadomy
(1991) found that patients preferred traditional uniform
when a nurse was performing nursing care, but that when
ful®lling a counselling role a less clinical uniform was
considered appropriate. Rowland (1994) concurred with
these ®ndings in a general practice environment. It
appears therefore that traditional uniform is expected
during clinical procedures yet may act as a barrier in
developing nurse±patient relationships. Marr & Matthews
(1993) found that uniform was preferred because it created
an atmosphere that was military, organized, respected and
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
Users' experiences of care Children's nurses and uniform 77

Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
78 S. Campbell et al.

Figure 2 Questionnaire ®ndings.10
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
Users' experiences of care Children's nurses and uniform 79

promoted con®dence in the wearer. Franzoi (1988)
showed that uniforms were expected to promote an
atmosphere of competency, order and organization rather
than to enhance personal relationships. The sample
population was not children orientated, but similar views
were found within such an environment. Livingstone
(1995) found that children and parents preferred tradi-
tional nurses' uniforms; they may allow children to feel
more comfortable because they recognize the stereotypical
presentation of the nurse. Glasper & Miller (1992) found
that parents may have greater con®dence in uniformed
nurses, because of historical socialization, despite uniform
creating barriers in the development of the family±nurse
relationship.
Statement 6: `The clothing that nurses wear should
re¯ect that of an authority ®gure'
This statement deals with the issue of presenting a
clinically ef®cient nurse as opposed to an approachable
nurse with whom the families can develop a therapeutic
relationship. A signi®cant minority wished for an author-
ity ®gure (39% of the sample agreed or strongly agreed
with the statement that clothing should re¯ect an author-
ity ®gure). Extending the statement to which type of
atmosphere was required for clinical procedures as
opposed to discussion may have produced further data
that developed the ®ndings of Rowland's (1994) study.
A large minority (39%) did look to the nurse to present
an authority ®gure, which again may re¯ect stereotyping
of the nurse to instil con®dence. The development of
family participation in care seeks to promote the nurse as
an approachable ®gure, and expansion in understanding of
participation for consumers of health care will hopefully
see a greater acceptance of the nurse as a partner in care
rather than provider of care to passive recipients.
Another characteristic of uniform is the authority and
power it gives regardless of the actual role of the wearer.
Bamford & Sparrow (1990) found that uniforms did not
immediately create an awareness of grade of staff but
rather produced in patients a sometimes inappropriate
level of con®dence and competence in the wearer. Glasper
et al. (1991) reiterated this from the viewpoint of the
nurse, stating that uniform is used to gain authority and
increase the con®dence of nurses and particularly stu-
dents. Bischof (1995) suggests that uniform can aid
compliance by conferring legitimacy. Thus children may
permit activities which are uncomfortable or normally
taboo if performed by a doctor wearing a white coat, since
this is the uniform they expect to see. This argument may
be extended to justify the use of nurses' uniforms.
Con®dence in the professional, assessed by uniform,
may be inappropriate. Leventon (1989), reporting anec-
dotally from the view of the lay carer, found that uniform
produced a false sense of nurses' abilities, because
although nurses were differentiated by the colour of their
dress their rank was not. It was only by experience,
through long-term support by `nurses' in the generic
sense, that the carer was able to distinguish the compe-
tencies associated with the various coloured uniforms.
Dring (1987) states that nurses should be aware that it is
unacceptable to assume authority through wearing a
uniform in an environment in which nurse and patient
should be working in partnership. However, it is certainly
possible that uniform is used as a tacit method of control;
removal of traditional uniform may reduce this acceptance
of misplaced authority and enhance the therapeutic
relationship (Rowland, 1994). In conclusion, it could be
proposed that lay people see uniforms as enabling
differentiation of rank and profession; however, there is
inappropriate understanding about roles and this may lead
to conferring legitimacy that may not be justi®ed.
COMMUNICATIONCOMMUNICATION
Statement 7: `The choice of nurses' clothing should
create an informal situation'
The sample wanted an informal situation: 71% agreed/
strongly agreed with the statement.
Statement 8: `A casual style of uniform makes people
feel insecure'
A total of 59% disagreed/strongly disagreed with the
comment that uniform makes people insecure.
Statement 9: `The clothing that nurses wear should
help them to seem friendly'
Of these respondents, 93% agreed/strongly agreed with
clothing helping the nurse to seem friendly.
Comparing the results from Statements 7±9 with those
of Statements 5 and 6 suggests that although patients
require an atmosphere that instils con®dence in the
effectiveness of the practitioner, parents and children are
also looking for an informal, friendly environment in
which they feel secure and con®dent. Families require an
environment in which barriers to communication are
reduced and a successful partnership can be developed for
the bene®t of the child and family.
An atmosphere of equality and approachability is
espoused by children's nurses, with the aim of providing
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
80 S. Campbell et al.

an appropriate environment in which to develop a
therapeutic relationship with families. This therapeutic
relationship is common to all areas of nursing and has been
shown to be enhanced by removal of traditional nurses'
uniform in favour of ordinary clothes or more casual
uniform (Glasper & Miller, 1992). The abandoning of
nurses' uniforms removes a barrier to communication,
thus nurturing the development of a bene®cial relationship
(Coombes & Heilman, 1993). This phenomenon was ®rst
highlighted in psychiatric nursing and continues to be
used in the mental health ®eld, although questions have
been raised about the validity of the research techniques
used to study this (Smith, 1990). There seems to be a
degree of agreement among healthcare professionals that
communication is improved by the absence of uniform,
and that uniform acts as a barrier to effective communi-
cation (Castledine, 1987; Tiffany & Sparrow, 1987;
Davies, 1995). The effect of uniform on communication
is also recognized by clients of healthcare; Leventon (1989)
regards it as a barrier to effective communication, which
fosters dependency on a uniform per se rather than
establishing con®dence through a relationship with the
professional beneath the uniform.
A separate question was included on the questionnaire
about speci®c uniform preferences. The majority of the total
sample preferred polo shirts (57%). However a signi®cant
minority (32%) preferred the old style of uniform.
Implications for nursing
Following analysis of the results, nursing staff in COPD
changed their uniform to polo shirts, with different
colours of shirt denoting different grades of staff. This
decision was considered consistent with the ®ndings of the
study.
The need for families to identify nurses could be
perceived as simply related to stereotypical images.
However, as previously discussed, the interviews revealed
that this seemed more related to issues of communication.
This supported the ®ndings of a number of key workers
(Castledine, 1987; Tiffany & Sparrow, 1987; Coombes &
Heilman, 1993; Davies, 1995). There was a strong
consensus that all nurses should wear the same kind of
clothing. If children's nurses decide to wear polo shirts
this means that there is potential for the stereotype to
change (Stewart et al., 1979) and for this to become the
new uniform in the eyes of the public. The stereotype of
the nurse consists of an authority ®gure ®rst and
foremost, and an approachable ®gure second (Sparrow,
1991). Our ®ndings indicate that families reverse this
view, and prefer nurses to be approachable ®rst and
authority ®gures second. Again this may imply that there
is a potential for the image of the nurse, as represented by
uniform, to be changed, thus in¯uencing the stereotype
(Stewart et al., 1979). This is echoed in our results by the
need for nurses to create an informal situation through
what they wear.
It has been suggested by some of the nurses in this
study, and elsewhere, that a casual style of uniform leads
parents to feel insecure. Our results seem to refute this
notion and may even suggest the opposite view, that a
more casual style of uniform can actually instil con®dence
in families. These conclusions would support Leventon's
(19895 ) view that uniform hinders the development of a
con®dent relationship. Participants in this study were
concerned that the image of children's nurses should be a
friendly one and this would seem to be closely linked with
issues of approachability.
There has been a general change in the uniform of
children's nurses in recent years, based on the rationale that
it is important to produce a more child friendly environ-
ment. Many children's wards have adopted a casual style of
uniform including polo shirts, use of child-orientated
materials in uniform or wearing ordinary clothes. This
mood of change, however, has not been captured by the
media, which is generally recognized as a major factor in
forming stereotypes. The media still present the nurse in
traditional uniform in advertising, the press and popular
television programmes. Until the media recognize the
changing uniforms and roles of nurses, other forms of direct
education are needed in order to help the public update their
schemata in relation to nurses' uniforms, nurses and the
environment of care in which they work (Kucera &
Nieswiadomy, 1991). It is the responsibility of every nurse
to present to the public a professional, therapeutic and
supportive image that is projected by behaviour rather than
relying on the nature of the uniform that is worn.
References
Bamford O. & Sparrow S. (1990) Nursing development units: a
virtue in uniformity. Nursing Times 86(41), 46±48.
Barrett T.G. & Booth I.W. (19947 ) Sartorial eloquence: does it exist
in the paediatrician±patient relationship? British Medical Journal
309(6970), 1710±1712.
Bischof R.O. (1995) White coats in the care of children. Lancet
345(8952), 777±778.
Brennan W., Scully W., Tarbuck P. & Young C. (1995) Nurses'
attire in a special hospital: perception of patients and staff.
Nursing Standard 9(31), 35±38.
Casey A. (1988) A partnership with child and family. Senior Nurse
8(4), 8±9.
Castledine G. (1987) The uniform farce. Geriatric Nursing and Home
Care 7(5), 10.
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
Users' experiences of care Children's nurses and uniform 81

Cauthen N.R., Robinson I.E. & Krauss H.H. (1971) Stereotypes: a
review of the literature 1926-1968. Journal of Social Psychology
84, 103±125.
Coombes S. & Heilman J. (1993) A uniform with uniformity.
Canadian Nurse 89(8), 61±62.
Davies P. (1995) Uniforms: cap in hand. Nursing Standard 9(29), 50.
Department of Health (1996) Patient's Charter: Services for Children
and Young People. Department of Health, London.
Dring S. (1987) Uniform views. Nursing Times 83(25), 19.
Franzoi S.L. (1988) A picture of competence. American Journal of
Nursing 88(8), 1109±1112.
Glaser B.G. & Strauss A. (1967) The Discovery of Grounded
Theory: Strategies for Qualitative Research. Aldine Publishing
Co, Chicago.
Glasper A. & Miller S. (1992) Newly clothed wards. Nursing Times
88(14), 34±36.
Glasper A., Miller S. & Payne S. (1991) Coming out. Paediatric
Nursing 5(5), 5±7.
Hawkey B. & Clarke M. (1990) Dress sense or nonsense? Nursing
Times 86(3), 28±29.
Joseph N. (1986) Uniforms and Nonuniforms: Communication
Through Clothing. Greenwood Press, New York.
Joseph N. & Alex N. (1972) The uniform: a sociological perspective.
American Journal of Sociology 77(4), 719±730.
Kucera K.A. & Nieswiadomy R.M. (1991) Nursing attire: the
public's preference. Nursing Management 22(10), 68±70.
Leventon S. (1989) A uniform barrier. Nursing Times 85(15), 64.
Livingstone M. (1995) Nursing uniform preferences of parents and
children in a paediatric setting. British Journal of Nursing 4(7),
390±395.
MacFarlane M.E. (1990) The professional nurse: with or without a
uniform. Canadian Journal of Nursing Administration 3(3), 14±17.
Marr J. & Matthews T. (1993) Change of a dress. Nursing Standard
7(49), 48±49.
Meyer D. (1992) Children's responses to nursing attire. Pediatric
Nursing 18(2), 157±160.
Nightingale K. (1983) The uniform approach. Nursing Times 79(47),
22±23.
Rowland W. (1994) Patients' perceptions of nurses' uniforms.
Nursing Standard 8(19), 32±36.
Smith D. (1990) Worn out. Nursing Times 86(3), 32±35.
Sparrow S. (1991) An exploration of the role of the nurses' uniform
through a period of non-uniform wear on an acute medical ward.
Journal of Advanced Nursing 16, 116±122.
Stewart R.A., Powell G.E. & Chetwynd S.J. (1979) Person,
Perception and Stereotyping. Saxon House, Farnborough.
Tiffany R. & Sparrow S. (1987) The uniform question. Nursing
Times 83(15), 40±41.
Ó 2000 Blackwell Science Ltd, Journal of Clinical Nursing, 9, 71±82
82 S. Campbell et al.