Embed Size (px)
Citation preview

The Classification of Pancreatic
Neuroendocrine Neoplasms: WHO 2017
Günter Klöppel, N. Volkan Adsay, Carlo Capella, Anne
Couvelard, Ralph H. Hruban, David S. Klimstra, Paul
Komminoth, Stefano La Rosa, Jean-Yves Scoazec, Nobuyuki
Ohike, Robert Y. Osamura, Aurel Perren, and Guido Rindi

Definition: “Neoplasm”
Overarching term to encompass all of the pancreatic
entities with significant neuroendocrine differentiation
(tumors, carcinomas, mixed carcinomas)

Classification of Pancreatic Neuroendocrine
Neoplasms (WHO 2004)
Microadenoma (<0.5 cm)
Well differentiated endocrine tumor
Benign behavior: confined to pancreas, <2 cm, non-angioinvasive, </= 2
mitoses per 10 HPF, </= 2% Ki67-positive cells
Uncertain behavior: confined to pancreas >/= 2 cm, >2 mitoses per 10 HPF,
> 2% Ki67-positive cells, OR angioinvasive
Well differentiated endocrine carcinoma
Low grade malignant: invasion of adjacent organs or metastases
Poorly differentiated endocrine carcinoma
High grade malignant: >10 mitoses per 10 HPF
Kloppel et al. Ann NY Acad Sci 2004; 1014: 13-27

Classification of Pancreatic Neuroendocrine
Neoplasms (WHO 2004): Issues
Combined staging (organ-confined, size) and grading (proliferative rate)
parameters
Used both “tumor” and “carcinoma” to refer to the same entity
Changed diagnosis with disease progression
Used “carcinoma” for both well and poorly differentiated neoplasms
Provided no prognostic stratification for advanced disease
“Benign behavior” and “uncertain behavior” were NOT!

2006 ENETS Grading of GEP-NETs
Grade Mitoses Ki-67 Index
G1 <2 / 10 H.P.F. < 2%
G2 2-20 / 10 H.P.F. 3-20%
G3 >20 / 10 H.P.F. >20%
Poorly Differentiated (High Grade ) Neuroendocrine Carcinoma

Pancreatic NETs:
Overall Survival by Grade
Rindi et al., J Natl Cancer Inst 2012; 104: 764

TX Primary tumor cannot be assessed
T0 No evidence of primary tumor
T1 Tumor limited to the pancreas and size </= 2 cm
T2 Tumor limited to the pancreas and size > 2 cm
T3 Tumor extends beyond the pancreas but without
involvement of the celiac axis or SMA
T4 Tumors involves the celiac axis or the SMA (unresectable
primary tumor)
TNM Staging System for Pancreatic
Neuroendocrine Neoplasms (AJCC/UICC 2009)
T – PRIMARY TUMOR

Classification of
Pancreatic Neuroendocrine Neoplasms
(WHO 2010)
Well differentiated
Well differentiated neuroendocrine tumor, Grade 1 (NET G1)
Well differentiated neuroendocrine tumor, Grade 2 (NET G2)
Poorly differentiated
Poorly differentiated neuroendocrine carcinoma, Grade 3 (NEC G3)
TNM should be performed in all cases

WHO Grading of GEP-NETs (2010)
Grade Mitoses Ki-67 Index
G1 <2 / 10 H.P.F. < 2%
G2 2-20 / 10 H.P.F. 3-20%
G3 >20 / 10 H.P.F. >20%
High Grade (Poorly Differentiated) Neuroendocrine Carcinoma
Virchows Archiv 2007, 451:757-762
Neuroendocrinology 2008, 87:1-64

WHO Grading of GEP-NETs:
Provisions
Count mitoses in 50 high power fields
Assess Ki67 based on counting 2000 (500) cells
Assess Ki67 in “hot spots”
If mitotic rate and Ki67 are discordant, assign higher
grade

What about G2 / G3 discordance??
(well differentiated tumor vs. poorly
differentiated carcinoma)

Ki67 = 45%
Mitotic rate = 8 / 10 HPF
Well Differentiated PanNET
Mitotic rate = 12 / 10 HPF
Ki67 = 55%

Poorly Differentiated Neuroendocrine Carcinoma
Chromogranin Ki67

Mitoses <1/10 HPF Mitoses 13/10 HPF
Progression of Low Grade to High Grade Neuroendocrine Tumor

Ki67 = 2%
G1
Ki67 = 45%
G3
Tang et al., Clin Cancer Res 2016; 22: 1011

Poorly Differentiated Neuroendocrine Carcinoma of Pancreas

Gene Small Cell Large Cell
NEC
W.D.
PanNET
Ductal ACa Small Cell
Lung CA
KRAS 25% 33% 0% >90% 0-10%
CDKN2A 11% 50% 0% 80-95% 0-10%
TP53 100% 90% 4% 75% 80%
SMAD4 0% 10% 0% 55% 0%
RB1 89% 50% 0% 13% 90%
DAXX/ATRX 0% 0% 43% 0%
MEN1 0% 0% 44% 0% 0%
mTOR genes 15% 1%
Genetics of Neuroendocrine Neoplasms
of the Pancreas
Yachida et al., Am J Surg Pathol 2012; 36: 173
Jiao et al., Science 2011; 331: 1199

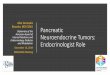
Predictive and prognostic factors for treatment and
survival in 305 patients with advanced gastrointestinal
neuroendocrine carcinoma (WHO G3)
• Reviewed clinical data on advanced stage G3 NECs, 2000-2009
• Ki67 > 20%
• 252 patients received chemotherapy (platinum-based)
• Median survival = 11 mos.
• Response rate = 31%
• Stable disease rate = 33%
Ki67 < 55% predicted a lower response rate (15% vs 42%, p < 0.001)
Ki67 < 55% predicted a better survival (14 vs 10 months, P < 0.001)
Sorbye et al., Ann Oncol 2013; 24: 152-60

Conclusion:
G3 NETs with Ki67 20-55%
may be well differentiated
biologically!!
(“Well Differentiated PanNET with
an Elevated Proliferative Rate”)

Basturk et al., Am J SurgPathol 2015; 39: 683-690
Survival of High Grade Neuroendocrine
Neoplasms of the Pancreas

Are all G3 Neuroendocrine
Neoplasms the Same?
NO!
Small cell carcinoma vs. Large cell NE carcinoma
Large cell NE carcinoma vs. G3 well differentiated NET
NEC G3 vs. NET G3

Well differentiated NE tumor*
Grade Mitoses Ki-67 Index
G1 <2 / 10 HPF <2%
G2 2-20 / 10 HPF 3-20%
G3** >20 / 10 HPF >20%
*Organoid architecture, “well
differentiated” cytology, absence of non-
neuroendocrine carcinoma components,
may have components of G1 or G2,
usually strong immunoexpression of
general NE markers
**mitoses usually <20/HPF; Ki 67 >20%
but usually <50%
Poorly differentiated NE carcinoma*
Grade Mitoses Ki-67 Index
G3** >20 / 10 HPF >20%
*Small cell carcinoma and large cell NE
carcinoma; less organoid architecture,
classic cytology of small cell and large cell
NE CA, absence of G1 or G2 NE
components, may have non-
neuroendocrine carcinoma components,
less diffuse immunoexpression of general
NE markers
**mitoses >20/10 HPF; Ki67 >20% and
usually >50%
Grading of Pancreatic Neuroendocrine Neoplasms: Proposal

Classification of Pancreatic
Neuroendocrine Neoplasms (WHO 2017)

Determining the Ki67 Labeling Index of NETs
Courtesy of Dr. Laura H. Tang

Ki67 Cutpoints
Grade Ki67 2010 Ki67 2017
G1 <2% <3%
G2 3-20% 3-20%
G3 >20% >20%

What about the G1/G2 cut-point??
Several studies have suggested 5% stratifies outcome better than 3%
HOWEVER:
Statistical basis for defining cut-point is complex
Not all studies support the same cut-point
Currently no significant treatment change for G1 vs. G2
Changes in grading parameters confound historical data interpretation
THERFORE:
Keep G1/G2 cut-point the same
Recommend reporting actual Ki67 index

0 10 20 30 40 50 60 70 80 90 100
Ki67%
WDNET
PDNEC
G3
G3 G2 G1

How to distinguish G3 NEC (esp. large
cell NE carcinoma) from G3 NET?

G3 NET Large Cell NEC
Pancreatic G3 NE Neoplasms

How to distinguish G3 NEC (esp. large
cell NE carcinoma) from G3 NET?
• Clinical clues
• History of well differentiated NET?
• Octreotide scan positive?
• FDG-PET positive?
• Morphologic clues
• Lower grade component?
• Non-neuroendocrine component?
• Mitotic rate?
• Molecular clues
• Status of TP53, RB1, DAXX, ATRX, MEN1

Well Differentiated PanNETs (G1-3)
Exhibit a Different Molecular Phenotype from
Poorly Differentiated NECs (G3)
TP53 Rb DAXX /
ATRX MEN1
WD-
PanNET
4% 0 43% 44%
PD-
PanNEC
56% 72% 0 0
Yachida et al., Am J Surg Pathol 2012; 36: 173
Jiao et al. Science 2011; 331: 1199

DAXX
Rb p53
Tang et al., Am J Surg Pathol 2016; 40: 1192
WD-NET PD-NEC PD-NEC
p53 Rb

Initial Consensus
Immunohistochemical
Abnormalities
Other Histologic
Components Confirmed Classification
WD-NET G1/G2 WD-NET WD-NET
WD-NET DAXX G1/G2 WD-NET WD-NET
WD-NET ATRX G1/G2 WD-NET WD-NET
WD-NET G1/G2 WD-NET WD-NET
WD-NET DAXX G1/G2 WD-NET WD-NET
WD-NET G1/G2 WD-NET WD-NET
Ambiguous G1/G2 WD-NET WD-NET
Ambiguous G1/G2 WD-NET WD-NET
Ambiguous DAXX G1/G2 WD-NET WD-NET
Ambiguous ATRX G1/G2 WD-NET WD-NET
Ambiguous DAXX G1/G2 WD-NET WD-NET
Ambiguous G1/G2 WD-NET WD-NET
Ambiguous ATRX WD-NET
Ambiguous DAXX G1/G2 WD-NET WD-NET
Ambiguous DAXX G1/G2 WD-NET WD-NET
Ambiguous G1/G2 WD-NET WD-NET
Ambiguous G1/G2 WD-NET WD-NET
Ambiguous G1/G2 WD-NET WD-NET
Ambiguous G1/G2 WD-NET WD-NET
Ambiguous p53/Rb PD-NEC
Ambiguous p53/SMAD4 Ductal adenocarcinoma PD-NEC
Ambiguous p53/Rb PD-NEC
Ambiguous p53/Rb PD-NEC
Ambiguous p53 PD-NEC
Ambiguous Undetermined
PD-NEC-LCC DAXX G1/G2 WD-NET WD-NET
PD-NEC-LCC Rb PD-NEC
PD-NEC-LCC Ductal adenocarcinoma PD-NEC
PD-NEC-SCC p53 Ductal adenocarcinoma PD-NEC
PD-NEC-SCC Rb PD-NEC
PD-NEC-SCC p53/Rb Ductal adenocarcinoma PD-NEC
PD-NEC Rb PD-NEC
PD-NEC p53 PD-NEC
Classification of 33 High Grade Pancreatic Neuroendocrine Neoplasms by Secondary Evidence
Tang et al., Am J Surg Pathol 2016; 40: 1192
18/19 (95%)
morphologically
ambiguous high grade
pancreatic
NEneoplasms
successfully classified
19/33 (58%) of
high grade (G3)
pancreatic NE
neoplasms were
morphologically
ambiguous

0 50 100 1500
25
50
75
100
Months
Pe
rc
en
t s
urv
iva
l
WD-NET
PD-NEC
p<0.0001
Disease Specific Survival of High Grade Pancreatic Neuroendocrine Neoplasms
(N=20)
(N=12)
Tang et al., Am J Surg Pathol 2016; 40: 1192

Somatostatin Receptor (SSTR2)
Immunohistochemistry

Pancreatic Neoplasms with Mixed
Differentiation
Neuroendocrine (usually poorly differentiated) plus a non-
neuroendocrine component
Mixed ductal neuroendocrine carcinoma
Mixed acinar neuroendocrine carcinoma
Each component >30%
Previous terms
Mixed exocrine-endocrine carcinoma, MEEC (2004)
Mixed adenoneuroendocrine carcinoma, MANEC (2010)
Mixed neuroendocrine non-neuroendocrine neoplasm, MiNEN

Comparison of WHO Classifications of
Pancreatic Neuroendocrine
Neoplasms, 1980-2017