Embed Size (px)
Citation preview

Hepatocellular Neoplasms Induced by Low-Number Pancreatic
Islet Transplants in Autoimmune Diabetic BB/Pfd Rats
Frank Dombrowski,1Chantal Mathieu,
2and Matthias Evert
1
1Institute of Pathology, Otto-von-Guericke-University Magdeburg, Magdeburg, Germany and 2Laboratories for Experimental Medicine andEndocrinology, Rega Institute, Catholic University Leuven, Leuven, Belgium
Abstract
It has been shown that combined high local hyperinsulinismand hyperglycemia after low-number islet transplantationinto the livers of streptozotocin-diabetic rats lead to thedevelopment of hepatocellular neoplasms but a substantialcocarcinogenic effect of genotoxic streptozotocin could not beruled out completely. Thus, we herein investigated this modelin BB/Pfd rats (n = 805; nine experimental groups), whichdevelop spontaneous autoimmune diabetes similar to humantype 1 diabetes. After low-number islet transplantation(n = 450), the liver acini downstream of the islets showinsulin-induced alterations: massive glycogen and/or fataccumulation, translocation of the insulin receptor, decreasein glucose-6-phosphatase activity, increase in expression ofinsulin-like growth factor (IGF)-I, IGF-II/mannose-6-phosphate receptor, insulin receptor substrate-1, Raf-1, andMek-1, corresponding to clear cell preneoplastic foci of alteredhepatocytes known from chemical hepatocarcinogenesis andidentical to that in streptozotocin-diabetic Lewis rats. After6 months, many altered liver acini progressed to other typesof preneoplasias often accompanied by an overexpression ofthe glutathione-S transferase (placental form), IGF-I receptor,and transforming growth factor (TGF)-A. After 12 to 15 and15 to 18 months, 52% and 100% of the animals showed oneor multiple hepatocellular adenomas or hepatocellular carci-nomas (HCCs), respectively. Conclusively, this study identifiescombined hyperinsulinism and hyperglycemia as a carcino-genic mechanism for the development of HCCs in diabeticrats. Hepatocarcinogenesis is independent from additionalgenotoxic compounds (i.e., streptozotocin), but is primarilytriggered by increased intracellular insulin signaling viapathways associated with cell growth and proliferation, suchas the Ras-Raf-mitogen-activated protein kinase pathwayand the IGF system, and secondarily involves other growthfactors, such as TGF-A. (Cancer Res 2006; 66(3): 1833-43)
Introduction
Recent clinical trials introducing new immunosuppressive regi-mens and improved islet preparation techniques have shown thattransplantation of islets of Langerhans into the liver of type 1 diabeticpatients could represent an alternative to exogenous insulin treatmentand allows for the normalization of metabolic control, which cannotbe achieved by administration of exogenous insulin alone (1–5).Although a few cases have been published in the English literature,
detailed histopathologic studies of the livers of long-term recipientshave not yet been conducted (5–8). Thus, little is known about theparacrine effects of insulin on the adjacent hepatocytes, which mayturn out to be of major clinical importance in the long term.On the other hand, diabetes mellitus has been identified as a risk
factor for hepatocellular carcinoma (HCC) in humans in WesternEurope and the United States (9–15). However, the mechanismsby which diabetes may contribute to the formation of HCCs inhumans are poorly understood. This led to a controversy aboutwhether diabetes mellitus itself or rather associated diseases, suchas obesity or hepatitis C, are mainly responsible for tumorinduction (11, 16, 17), and the need for experimental studiesrevealing the underlying mechanisms is emphasized (18).A possible explanation for the relationship of diabetes mellitus
and liver cancer is provided by our previous studies in an animalmodel of hormonally induced hepatocarcinogenesis in which intra-hepatic low number (i.e., 350-450 islets) pancreatic islet transplan-tation in streptozotocin-diabetic Lewis rats seemed to be theprimary trigger for carcinogenesis (19–26). Sole high number (i.e.,1,000-2,000 islets) transplantation in streptozotocin-diabetic Lewisrats, in which the h-cells of the grafts are not maximally stimulatedto secrete insulin and the resulting local hyperinsulinemia isrelatively slight, does not suffice to induce the carcinogenic process(19, 21). Carcinogenesis starts with hepatocellular alterations, which,on the one hand, correspond to known insulin effects and, onthe other hand, resemble the so-called clear cell focus (CCF) ofpreneoplastic hepatocytes, known from many other models of hepa-tocarcinogenesis (27). These alterations are reflected in an increasein glycogen and lipid storage, in an increase in cell-turnover, (i.e.,high proliferative activity and apoptotic elimination of preneoplastichepatocytes), as well as in characteristic alterations in the activitiesof key enzymes, in particular of the carbohydrate and fatty acidmetabolism (19–21, 23, 25). These include an up-regulation ofenzymes of glycolysis (hexokinase, glyceraldehyde-3-phosphatedehydrogenase, and pyruvate kinase), de novo lipid synthesis ( fattyacid synthase), and the pentose phosphate pathway (glucose-6-phosphate dehydrogenase), whereas key enzymes of gluconeogenesis(glucose-6-phosphatase), glycogenolysis (glycogen phosphorylase),and adenylate cyclase activity were down-regulated (20, 23). Insulineffects in the CCF also manifested in an overexpression of apoli-poprotein A-IV (25) and in an altered expression of proteins of theinsulin-like growth factor (IGF) pathway in the CCF, including IGF-Iand its binding proteins, such as IGF binding protein (IGFBP)-1 andIGFBP-4 (22). Moreover, we have recently shown strongly increasedinsulin signaling in CCF after islet transplantation, reflected in atranslocation of the insulin receptor and in an overexpression ofseveral insulin signal transduction proteins of the Ras-Raf-mitogen-activated protein kinase (MAPK) pathway, such as insulin receptorsubstrate-1 (IRS-1), Raf-1, and Mek-1 (24). In the beginning, the CCFwere always strictly confined to the liver acini located downstreamof the islets but gradually expanded into the neighborhood when
Requests for reprints: Frank Dombrowski, Institut fur Pathologie, UniversitatMagdeburg, Leipziger Strasse 44, D-39120 Magdeburg, Germany. Phone: 49-391-67-17869; Fax: 49-391-67-17952; E-mail: [email protected].
I2006 American Association for Cancer Research.doi:10.1158/0008-5472.CAN-05-2787
www.aacrjournals.org 1833 Cancer Res 2006; 66: (3). February 1, 2006
Research Article
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

undergoing neoplastic transformation (19, 21). After 15 to 22months, 86% and 19% of the animals developed at least onehepatocellular adenoma (HCA) or HCC, respectively (21).There are additional data obtained in other animal models that
showed that the phenotypes of preneoplasias can mimic responsesto insulin action (28), and Nehrbass et al. (29, 30) have shown thatIRS-1 overexpression is an early event in chemical hepatocarcino-genesis of rats, given p.o. N-nitrosomorpholine. From these studies,it can be concluded that increased insulin action or insulinomimeticeffects may constitute an interesting carcinogenic mechanism inthe development of HCC in rats and possibly also in humans.However, a serious drawback in the interpretation of the results
from the islet transplantation model was the administration of
streptozotocin to achieve diabetes. Streptozotocin is genotoxic andcarcinogenic in rats (31, 32). Okawa and Doi (33) have reported thedevelopment of hepatocellular and cholangiocellular tumors instreptozotocin-treated Sprague-Dawley rats, although a completehepatocarcinogenic potential in rats is not sufficiently proved by thisstudy in which only 16 animals were investigated. Nevertheless, atleast a significant cocarcinogenic contribution of streptozotocin hasto be taken into account. To finally exclude an influence of strep-tozotocin acting as an incomplete hepatocarcinogen in thisexperimental setting and for reasons of better comparability withthe situation in human diabetes mellitus, we thus investigated in thislong-term study the local influence and the carcinogenic potentialof insulin on the adjacent hepatocytes in a model of autoimmune
Table 1. Experimental design, preneoplastic foci, and hepatocellular neoplasms
Inbred BB/Pfd rats (n = 805)
Spontaneous autoimmune diabetes (n = 338)
Streptozotocin administration No
Islet transplantation Low-number (n = 450) High-number (n = 1,200) No
Spontaneous reestablishment of self-tolerance Yes No Yes No Not tested
Experimental group MG (n = 148) CG 1 (n = 42) CG 2 (n = 86) CG 3 (n = 22) CG 4 (n = 40)
Blood glucose (mean F SE; mmol/L) 11.6 F 0.7 19.9 F 0.9 4.7 F 0.2 16.2 F 1.1 20.4 F 0.8
Body weight at sacrifice (mean F SE; g) 288 F 5 262 F 9 348 F 9 282 F 15 254 F 6
Relative number/main type of foci
0-3
mo
p.t.
+++/CCF0
(15)
++/CCF0
(5)
00
(12)
00
(5)
00
(2)
3-6
mo
p.t.
+++/CCF0
(18)
++/CCF0
(4)
00
(8)
00
(1)
00
(8)
Relative no. animals bearing a
HCA/HCC (%)
6-9
mo
p.t.
+++/CCF0
(33)
++/CCF0
(13)
00
(11)
00
(2)
00
(5)
9-12
mo
p.t.
+++/MCF14/0
(51)
++/MCF0
(11)
00
(24)
00
(6)
00
(12)
No. investigated animals
(in parentheses)
12-15mo
p.t.
+++/MCF52/0
(25)
++/MCF29*/0(7)
+/CCF0/0
(22)
00/0
(6)
00/0
(8)
15-18mo
p.t.
+++/MCF83/50
c
(6)
++/MCF50/0
(2)
+/CCF11/0
(9)
00/0
(2)
00/0
(5)
NOTE: The number of foci was estimated semiquantitatively using three grades: +, single (sporadic) foci in single animals; ++, single number
of foci in every animal; +++, numerous foci in every animal. Yellow box, significantly more tumor-bearing animals than in CG 2–5 and CG 7–8.
Orange box, significantly more tumor-bearing animals than CG 5, 7, and 8 (others not tested).
Abbreviations: MG, main group; CG, control group; HCA, hepatocellular adenoma; HCC, hepatocellular carcinoma; CCF; clear-cell focus; MCF, mixedcell focus, p.t., post-transplantation.
*Significantly more HCA-bearing animals than in CG 2–5 and CG 7–8. All data refer to the right liver part and were tested using Fisher’s exact test and
accepted if P < 0.05.cSignificantly more HCC-bearing animals than in CG 2.
Cancer Research
Cancer Res 2006; 66: (3). February 1, 2006 1834 www.aacrjournals.org
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

diabetes, using autoimmune-diabetic BioBreeding (BB) rats. BB ratsbecame diabetic by an autoimmunologic disorder similar to humantype 1 diabetes mellitus (34), which is not completely understood butinvolves mutations of the lyp locus on chromosome 4, lymphopenia,and dysregulation of inflammatory cells, including eosinophils, mastcells, and lymphocytes, which, in turn, lead to insulitis and h-celldestruction (35–37). The Pfd substrain of BB rats is characterizedby the reestablishment of self-tolerance to the h-cells after previousdestruction of the h-cells in the pancreas (38, 39). Therefore, theseanimals tolerate the isologous islet grafts that were transplanted inthe course of the experiment without the use of immunosuppressionand its possible side effects on the hepatocytes. We also includedstreptozotocin-diabetic control groups of the BB strain to comparecarcinogenesis between these different types of diabetes inductionand with the Lewis rat model.
Materials and Methods
Animals. Eight hundred five animals were investigated in this study and
housed as described previously (21). Only nondiabetic littermates werepaired, which also served as islet donors. Spontaneous diabetes was defined
by a nonfasting blood glucose level higher than 22.2 mmol/L (400 mg/dL).
To avoid greater weight loss and to have normoglycemia by the time of
transplantation, the diabetic rats were treated with s.c. injections of insulin(Insulin Protraphan HM 40, NOVO, Mainz, Germany) as described
previously (21), a procedure that was immediately stopped after islet
transplantation.The spontaneous diabetic animals were finally subdivided into five
experimental groups according to whether the rats reestablished self-
tolerance (MG and CG 2) or not (CG 1 and CG 3) and according to the
modus of transplantation [low number (MG and CG 1), high-number (CG 2and CG 3), or no (transplantation CG 4)], resulting in one main group (MG)
and four control groups (CG 1-4; Table 1). CG 1 and CG 3 were composed of
animals that never developed self-tolerance or lost it again and rejected the
islet grafts during the experimental course.Rats not having developed autoimmune diabetes were left completely
untreated as normoglycemic controls (CG 5) or received a single i.v. injection
of streptozotocin (65 mg/kg). Two weeks later, they were again subdivided(CG 6-8) according to the respective transplantation procedure (Table 1).
All animals were inspected daily. Blood glucose and body weight were
measured monthly and also 1 and 3 days after transplantation, as well as
immediately before and 2 days after streptozotocin treatment. Animalsshowing a weight loss of more than one third of their maximal body weight
posttransplantation were given a s.c. insulin implant (Linplant, Linshin
Table 1. Experimental design, preneoplastic foci, and hepatocellular neoplasms (Cont’d)
Inbred BB/Pfd rats (n = 805)
No spontaneous diabetes (n = 467)
Streptozotocin administration No Diabetes induction by streptozotocin (65 mg/kg body weight)
Islet transplantation No Low number (n = 450) High number (n = 1,200) No
Spontaneous reestablishment of self-tolerance Tolerance never lost Tolerance never lost Tolerance never lost Tolerance never lost
Experimental group CG 5 (n = 165) CG 6 (n = 144) CG 7 (n = 118) CG 8 (n = 40)
Blood glucose (mean F SE; mmol/L) 5.0 F 0.1 10.8 F 0.6 4.2 F 0.1 17.8 F 0.6
Body weight at sacrifice (mean F SE; g) 328 F 7 296 F 6 367 F 7 289 F 8
Relative number/main type of foci
0-3
mo
p.t.
0
0
(15)
+++/CCF
0
(15)
0
0
(15)
0
0
(0)
3-6mo
p.t.
0
0(10)
+++/CCF
0(15)
0
0(15)
0
0(5)
Relative no. animals bearing a
HCA/HCC (%)
6-9mo
p.t.
0
0(33)
+++/CCF
0(35)
0
0(23)
0
0(7)
9-12mo
p.t.
0
0(50)
+++/MCF
15/0(39)
0
0(33)
0
0(12)
No. investigated animals(in parentheses)
12-15mo
p.t.
0
0/0(32)
+++/MCF54/0
(28)
+/CCF
0/0(20)
0
0/0(10)
15-18mo
p.t.
+/CCF
4/0(25)
+++/MCF75/25
(12)
+/CCF
8/0(12)
0
0/0(6)
HCA and HCC after Islet Transplantation
www.aacrjournals.org 1835 Cancer Res 2006; 66: (3). February 1, 2006
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

Canada, Scarborough, ON, Canada) to prevent death by diabetes. Animaltreatment was in line with the guidelines of the Society for Laboratory
Animal Service and the strict German Animal Protection Law.
Transplantation procedure. Animals were anesthetized (100 mg/kg
ketamin and 4 mg/kg xylazin) and islets of Langerhans were isolated from
nondiabetic littermates and transplanted into the liver via the portal vein as
described in detail previously (19). During infusion, the branch supplying
the left part of the liver (i.e., left lobe and left part of the middle lobe) was
clamped, thus making sure that the transplants were embolized only into
the right part of the livers (i.e., right lobe, right part of the middle lobe,
caudate lobe, and anterior and posterior papillary processus) and the left
part served as an intraindividual control. Ischemia for the left part lasted for
f1 minute. Rats of the MG, CG 1, and CG 6 received a low number (n = 450)
of islet grafts; CG 2, CG 3, and CG 7 animals received a high number
(n = 1,200) of islet grafts; and CG 4, CG 5, and CG 8 were not transplanted.Animal sacrifices and 5-bromo-2V-deoxyuridine application. Animals
were killed because of severe complications or were matched in time groups
(Table 1). Rats were anesthetized, the aorta was cannulated, the inferior
caval vein was cut, and the vessels were then rinsed for 2 minutes withRinger’s solution, mixed with 0.5% procain and 4% dextran, followed by
perfusion fixation using a cocktail of aqua dest containing 4% dextran,
0.5% glutaraldehyde, and 3% paraformaldehyde. All animals received a
single dose of BrdUrd i.p. (50 mg/kg) 1 hour before sacrifice as describedpreviously (21).
Tissue sampling and processing. After fixation, the livers were removed,
cut into slices (f0.5 mm), and examined with a stereomicroscope. All
macroscopic liver lesions and at least 10 additional slices, as well as specimens
from the heart, lung, kidneys, adrenal glands, small intestine and colon,
pancreas, spleen, thyroid gland,muscle, and pituitary glandwere embedded in
paraffin. Serial sections (2-3 Am) of the liver specimens were stainedwith H&E
and with the periodic acid-Schiff (PAS) reaction. Additional sections were
made for immunohistochemistry. The other organs were stained with H&E.
The morphologic classification of lesions was done as described
previously (21). Briefly, preneoplastic foci composed exclusively of glycogen-
and fat-storing cells were classified as CCF; a glycogen-depleted, exclusively
basophilic cell population as basophilic cell foci; and those with both cell
types as mixed cell foci. HCA extended beyond the original liver acini, were
sharply limited, and compressed the surrounding liver parenchyma. Tumors
being larger than 5 mm in diameter, exhibiting trabeculae thicker than three
cell layers in at least two separate areas, and showing a higher number of
mitotic figures, vascular invasion, or metastases were classified as HCC.
Insulinomas were diagnosed if they fulfilled the following criteria:
intrahepatic islet graft larger than 2 mm, immunohistochemical positivity
for insulin, mitotic activity of insulin-positive cells, and severe hypoglycemia
[blood glucose lower than 1.11 mmol/L (<20 mg/dL)].
For electron microscopy, appropriate tissue specimens of 2 � 2 mm size
were postfixed in OsO4 and embedded in Epon. Semithin sections were
stained according to Richardson et al. (40); ultrathin sections were stained
with uranyl acetate and lead citrate. The examination was done using a
Phillips (Einthoven, the Netherlands) CM10 electron microscope.For enzyme histochemistry, themiddle lobes of selected livers were removed
before fixation, cut into slices, and immediately frozen in �80jC cold iso-
pentane. Cryostat sections of 6 Am thickness were cut, stained according to
Benner et al. (41) for glucose-6-phospatase activity, and semiquantitavely
evaluated by comparison with the adjacent unaltered liver parenchyma. Addi-
tional sectionswere also stainedwith the PAS reaction and fat stain (Sudan red).
Immunohistochemistry. Paraffin sections were incubated with thefollowing primary polyclonal rabbit antibodies: anti-insulin receptor (A1314,0.5 mg/mL, kindly provided by Dr. J.W. Unger, Department of Anatomy,University of Munich, Munich, Germany), anti-IRS-1 (dilution: 1:50; UpstateBiotechnology, Inc., New York, NY), anti-Raf-1 (dilution 1:50; Santa CruzBiotechnology, Heidelberg, Germany), anti-Mek-1 (dilution 1:100; Santa CruzBiotechnology), anti-IGF-I (dilution 1:250; DSL, Webster, TX), anti-IGF-Ireceptor (Santa Cruz Biotechnology), anti-IGF-II/mannose-6-phosphate-receptor [purified from rat liver (42) and kindly provided by Dr. J.G. Scharf,Division of Gastroenterology and Endocrinology, Department of Medicine,University of Gottingen, Gottingen, Germany], anti-gluthathione S-transfer-
ase placental form (dilution 1:100, no pretreatment; Biogenex, San Ramon,CA), anti-TGF-a ( final concentration 10 Ag/mL; Oncogen Sciences, Cam-bridge, MA), as well as anti-insulin, antiglucagon, and antisomatostatin(dilution 1:200; all from DAKO, Hamburg, Germany). The anti-BrdUrdantibody (dilution 1:100; DAKO) was monoclonal. Negative controls withoutusage of the primary antibody were done in each run. Further details of thestaining procedures, including antigen retrieval methods, secondary anti-bodies, blocking of endogenous peroxidase, counterstaining, and mountingof the tissue sections, were described previously (21, 22, 24).
Results
Blood glucose and body weight. Spontaneous diabetesmanifested in f10% of male and in 2% of female 3- to 6-month-old rats. All animals of CG 4 (and also animals of CG 1 and CG 3)developed hyperglycemia (27-33 mmol/L), which was so severe thatinsulin depots had to be implanted to prevent death. Thus, bloodglucose of CG 4 was lowered to a mean of 20.4 mmol/L but wasstill higher than in untreated streptozotocin diabetic rats (CG 8:17.8 mmol/L). Animals after low-number transplantation persistedin a mild diabetic state as was intended (MG, mean blood glucose11.6 mmol/L). This was the result of previous autoimmunologicallyinduced self-destruction of the h-cells in the pancreas and thesubsequently transplanted and, owing to the reestablished self-tolerance now tolerated, low number of intrahepatic islet grafts.However, 22% of these animals failed to reestablish long-lasting self-tolerance and resumed h-cell destruction during the experimentalcourse, this time in the intrahepatic islet grafts, as revealed bypostmortem liver examination. The mean blood glucose level inthese animals was 19.9 mmol/L. They had to be excluded from theMG and formed CG 1. As expected, high-number transplantationinitially established normoglycemia in all animals but only 80%stayed normoglycemic owing to the reestablishment of self-tole-rance in these animals (CG 2, mean blood glucose: 4.7 mmol/L).Twenty percent resumed h-cell destruction in the islet grafts,proved by postmortem examination, and became diabetic again1 to 6 months posttransplantation. They had to be excluded fromCG 2 and formed CG 3 (mean blood glucose: 16.2 mmol/L).On average, the blood glucose level in the streptozotocin-treated
animals was 7% to 13% lower when compared with the corres-ponding autoimmune diabetic groups (Table 1) and they did notneed insulin implants. They also showed mild hyperglycemia afterlow-number transplantation (CG 6, mean blood glucose: 10.8mmol/L) and normoglycemia after high-number transplantation(CG 7, mean blood glucose: 4.2 mmol/L). Completely untreated ratswithout spontaneous diabetes stayed normoglycemic throughoutthe entire experiment (CG 5, mean blood glucose: 5.0 mmol/L).Single animals of the MG and CG 6 reached normoglycemia afterseveral months owing to hyperplasia of the islet grafts. The threeanimals that developed graft insulinomas (see below) were hypo-glycemic; the lowest blood glucose measured was 0.4 mmol/L.Body weight was inversely correlated with blood glucose; that is,
it was highest in normoglycemic animals of the CG 2, CG 5, and CG8, and lowest in the completely untreated diabetic animals of CG 4(Table 1).Intercurrent diseases and causes of spontaneous deaths.
Some rats were affected by other severe diseases that were notlocated in the liver and had no effect on hepatocarcinogenesis.When there were no complications of the diabetes, they wereequally distributed between the experimental groups. Theyincluded malignant lymphomas, pituitary gland adenomas, and,most frequently, a transmural eosinophilic inflammation of the
Cancer Research
Cancer Res 2006; 66: (3). February 1, 2006 1836 www.aacrjournals.org
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

colon and sometimes also the small intestine, leading to fibrosis,stenosis, and consecutive megacolon and massive obstipation asreported by Meehan et al. (43). These animals were usually killed intime to prevent further suffering and spontaneous deaths.Unfortunately, owing to this high morbidity, only a small numberof animals stayed alive for 15 to 18 months after transplantationand prolongation of the experiment exceeding 18 months was notpossible. As reported in previous studies (35, 44), some animals alsoshowed signs of an autoimmune enteropathy (i.e., decreased villousand enlarged crypt length) as well as an increase in the number ofintraepithelial lymphocytes; however, this was not the focus of ourstudy. We also observed several renal cell carcinomas showing astrong predilection for the diabetic groups, indicating diabetesmellitus to be a risk factor also for renal cell carcinomas. Therelationship between diabetes mellitus and renal carcinogenesiswill be investigated in detail in a future study.Macroscopy and stereomicroscopy of the livers. With the
exception of very few sporadic CCF in the control livers of late-stage animals, all focal liver alterations were observed in theright part of the livers of the MG, CG 6, and, to a lesser extent,of CG 1. This was the result of the transplantation procedure, asthe branches of the portal vein that supply the left liver part
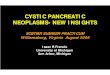
were clamped during infusion of the islets. Focal white lesionswere observed on the liver surface and on the cut surface ofliver slices, identified under a stereomicroscope as yellow-whiteliver acini draining the blood from the transplanted islet grafts(Fig. 1A). In the first 3 months, they were always confined to theanatomic borders of the respective liver acinus and limited bythe draining hepatic venules at the border to the adjacent acini(Fig. 1B). With increasing time, they expanded around thehepatic venules (Fig. 1C), extended into the neighboring liverparenchyma (Fig. 1D), and became inhomogenous in color andirregular in shape (Fig. 1E). Tumors of several millimeters in sizebegan to develop after 9 months (Fig. 1F-I).Light and electron microscopy of the liver parenchyma.
Light microscopy confirmed that in the first 3 months, thehepatocellular alterations were strictly limited to the liver acini,draining the blood from the transplanted islets. The hepatocytesat this stage were of uniformly clear cell morphology in the H&Estain and showed strong purple staining in the PAS reaction,resulting from a high amount of glycogen (Fig. 2A). Electronmicroscopy revealed that glycogen was deposited in a-particles inthe cytoplasm (Fig. 2E). In addition, these hepatocytes displayedan increase in fat storage in the form of single or multiple lipid
Figure 1. Stereomicroscopic aspects of unstainedliver slices. A to H, stepwise development fromaltered liver acini downstream of the transplantedislet (arrows ) in (A) to HCC (H ) in main group livers.Arrowheads, terminal hepatic venules. In (A and B),the borders of the liver acini are respected, but in(C and D) the altered tissue grows beyond. Theyellow-white color is the result of excessive glycogenand fat storage in the altered hepatocytes. Mixed cellfoci (E) developing later are irregular in color andshape as a result of admixed glycogen-rich andglycogen-poor hepatocytes. HCAs (F and G) showexpansive growth. The time course is as follows:A, 3 weeks; B, 3 months; C and D, 7 months; E, 9months; F, 14 months; G, 15 months; H, 16 months.The increasing size of the lesions is reflected by theincreasing length of the lower edge of the panel: 1.6mm in (A); 1.9 mm in (B ); 2.7 mm in (C ); 3 mm in (D );2.3 mm in (E); 4.6 mm in (F ); 4.6 mm in (G); and10.2 mm in (H ). I, a liver slice of CG1 at 14 monthsafter islet transplantation. All islets were rejected in thisanimal; nevertheless, some foci of altered hepatocytespersisted (small white spots ) and one HCA hasdeveloped. The lower edge represents 7.2 mm.
HCA and HCC after Islet Transplantation
www.aacrjournals.org 1837 Cancer Res 2006; 66: (3). February 1, 2006
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

vacuoles within the cytoplasm (Fig. 2B and E). These CCF werealso characterized by an increase in mitotic activity and inapoptotic elimination. In addition, they showed a mean 39-foldincrease in BrdUrd-positive nuclei when compared with the unal-tered liver parenchyma (Fig. 2C ; Table 2). Approximately 6 monthsposttransplantation, a subpopulation of altered hepatocytes losttheir glycogen and fat, now displaying a basophilic cytoplasm(Fig. 3C). In addition to the reduced glycogen content, these cellswere ultrastructurally characterized by abundant ribosomes andrough endoplasmic reticulum. In the beginning, these basophiliccells were intermingled with hepatocytes that retained the clear cellmorphology and such lesions were classified as mixed cell foci.However, some of the lesions gradually progressed to purebasophilic foci. Mixed cell foci and basophilic cell foci showed anincrease in mitotic activity and BrdUrd-labeled hepatocyte nucleiwhen compared with the adjacent unaltered liver tissue, albeit not
as strong as in CCF (Table 2). It is noteworthy that part of thepreneoplastic foci in the MG and CG 6 persisted, although therespective animals became normoglycemic and the insulinsecretion of the respective islet graft probably strongly decreased.Moreover, we also observed persistence of some preneoplasias inCG 1, although the islet grafts were rejected, became fibrotic, andthe h-cells completely vanished (Fig. 1I , 3G , and 4I).The first hepatocellular neoplasms developed after 9 months.
Most HCA and HCC in this study were composed of a mixedpopulation of clear and basophilic cells possibly originating frommixed cell foci. Some small HCA were purely clear cell. Purebasophilic or clear cell carcinomas were rare (Fig. 3D-F). They werefound to contain remnants of islet grafts in most cases. HCAs werecharacterized by expansive growth into the neighborhood withoutcytologic atypia. HCCs were highly differentiated, showed atrabecular growth pattern with trabecules thicker than three cell
Figure 2. Histochemical andimmunohistochemical alterations of liveracini downstream of transplanted isletsand HCCs in the main group. A, stronglypositive PAS reaction in the liver acinidownstream of the transplanted islet(arrow ) owing to increased glycogenstorage. Arrowheads, hepatic venules atthe border to the neighboring unalteredliver acini. Other altered liver acini showpredominant storage of fat droplets (B).Glycogen particles and fat droplets arealso visible using electron microscopy (E ).Glycogenosis in altered liver acini is dueto a strong decrease in the activity ofglucose-6 phosphatase (D, islet in thecenter). Increase in proliferative activityof the altered hepatocytes (and islet cells)is shown by BrdUrd immunostaining in (C ):left, islet; middle, altered acinus; rightthird of the panel, unaltered acinus.The insulin receptor (IR ) is translocatedfrom the cell membrane into thecytoplasm of the altered glycogen-storinghepatocytes (hyperinsulinemic acinus inthe left part of F ) and is increased inHCCs (I ). CCF are defined by their clearappearance in H&E stain (G ). As aconsequence of insulin action, IGF-I isup-regulated (H ). Signal transductionproteins IRS-1, Raf-1, and Mek-1are up-regulated in the altered acini(J , PAS; K , M , and N ) and are increasedin glycogen-storing HCCs (L ). Whereasall these phenomena are present a fewdays after transplantation, TGF-a isdetectable not earlier than 3 months aftertransplantation, beginning in acinar zone 3,and is stronger in mixed cell foci (O ).In addition to TGF-a, the placental form ofglutathione S-transferase (GST-P ) isalso strongly increased in glycogen-poorneoplasms, such as this HCA (P and Q).Time after transplantation and length of thelower edge of the panel: A, 3 weeks, 2.2mm; B, 3 weeks, 360 Am; C, 3 months,720 Am; D, 2 months, 2.2 mm; E, 1 month,10.6 Am; F, 1 month, 140 Am; G and H,3 months, 3.6 mm; I, 18 months, 560 Am;J and K, 4 months, 2.9 mm; L (sametumor as Fig. 1H ), 16 months, 1.1 mm;M and N, 1 month, 1.5 mm; O, 3 months,900 Am; P and Q, 14 months, 1.5 mm.A, B, and D, frozen sections; E, electronmicrograph of an ultrathin section; allothers are paraffin sections.
Cancer Research
Cancer Res 2006; 66: (3). February 1, 2006 1838 www.aacrjournals.org
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

layers in at least two separate areas, and showed mild to moderatecytologic atypia.In addition to the MG and CG 6, a significant increase in HCAs
was noted in the low-number-transplantation CG 1 (Table 1). Onesingle sporadic HCA occurring after 15 to 18 months also devel-oped in CG 2, CG 5, and CG 7. HCCs emerged only in the right partof the livers of the MG and CG 6 and did not develop before 15months after transplantation. BrdUrd labeling was stronglyincreased when compared with the unaltered parenchyma, rangingbetween a 36-fold increase in clear cell HCAs and an 80-foldincrease in basophilic HCCs (Table 2). Vascular invasion ormetastases were not observed. Between 15 and 18 months, 100%of the MG animals (6 of 6) and 83% of CG 6 animals (10 of 12)developed at least one hepatocellular neoplasm. Unfortunately, thediabetic BB/Pfd rats did not survive longer than 18 monthsposttransplantation as most HCCs had developed between 18 to 24months in the Lewis rats in previous studies. Some proliferativecholangiocellular lesions and cholangiomas, but no cholangiocel-lullar carcinomas, also developed in the draining area of the islets inthe MG and were more pronounced in the CG 6.In summary, the carcinogenic process was restricted to the right
liver part containing the islet grafts in animal groups that werediabetic and that received a low number of islets (i.e., MG, CG 1,and CG 6). Tumorigenesis was only weak in animals of CG 1, whichrejected most of their islet grafts (Fig. 4G-I) but was equally strongand showed no differences in the modus of progression in the MGand CG 6.Enzyme histochemistry and immunohistochemistry. Enzyme
and immunohistochemical results are given in detail in Table 2.The results were identical in autoimmune and streptozotocindiabetic BB/Pfd rats and were in line with previous results instreptozotocin diabetic Lewis rats (20–22, 24). Briefly, CCF werebiochemically characterized by alterations reflecting typical
insulin effects (i.e., overexpression of the fatty acid synthase anddown-regulation of the glucose-6-phophatase; Fig. 2D). Theinsulin receptor was translocated from the membrane into thecytoplasm (Fig. 2F), triggering increased intracellular signaling viathe Ras-Raf-MAPK pathway as reflected in the overexpression ofIRS-1, Raf-1, and Mek-1 (Fig. 2J, K, M , and N). Altered expressionswere also found for proteins of the IGF axis (Fig. 2G and H).Clear-cell HCAs and HCCs retained many of these alterationsbut additionally showed a moderate expression of the IGF-Ireceptor and TGF-a. Corresponding to the proportion of baso-philic cells, mixed cell foci, basophilic cell foci, and basophilictumors displayed not only a gradual normalization of theincreased insulin receptor signaling but also a strong overexpres-sion of TGF-a (Fig. 2O and P).Islet graft morphology. Islet grafts can already be identified
using a stereomicroscope (Fig. 1A and B). Histologically, they werefound within terminal portal venules (Fig. 2A and 3A-D) andconsisted of different types of endocrine cells, which were immu-nohistochemically discriminated using antibodies directed againstinsulin, glucagon, and somatostatin (Fig. 4E and F). They wererichly vascularized and sometimes showed small ductular pro-liferations at the border to the neighboring hepatocytes (Fig. 4A).Some islets displayed mild lymphocytic infiltration (Fig. 3A).Distinct differences were found regarding the ultrastructure ofa- and h-cells in the hyperglycemic animals but not in thenormoglycemic rats. The stimulated h-cells were enlarged, showedmassive hyperplasia of the rough endoplasmic reticulum and theGolgi complex, and were nearly completely degranulated (Fig. 4C).By contrast, the a-cells (and also the y-cells) were atrophic,were reduced in number, and stored many electron-dense secretiongranules (Fig. 4C). At later stages, islets were often observed in thecenter of small hepatocellular tumors that had originated from adownstream preneoplastic focus. In larger HCAs and in HCCs, the
Table 2. Expression of insulin-related proteins and BrdUrd index in preneoplasias and hepatocellular tumors
CCF MCF BCF cHCA bHCA cHCC bHCC
Insulin receptorMembranous #(=) = (#) = = = = =Intracytoplasmic " " (=) = (#) "" = (#) "" = (#)
IRS-1 "" " (=) = (#) "" = (#) "" = (#)Raf-1 "" " (=) = (#) "" = (#) "" = (#)Mek-1 "" " (=) = (#) "" = (#) "" = (#)IGF-I "" " = " = " # (=)IGF-I receptor = = = " (=) " (=) " (=) " (=)IGF-II/M6P receptor "" " " "" " "" "TGF-a = " "" " "" " ""GST-P = " (=) " " (=) "" " ""Glucose-6-phosphatase ## # N.D. N.D. N.D. N.D. N.D.Fatty acid synthase* "" N.D. N.D. N.D. N.D. N.D. N.D.Increase of BrdUrd
labeling indexc
39 F 4 15 F 6 25 F 3 36 F 4 68 F 5 65 F 4 80 F 6
NOTE: The intensity of the immunohistochemical variables in focal lesions was estimated semiquantitatively compared with unaltered liver tissue of thesame sections using the following grades: ##, strong decrease; #, decrease; = equal; ", increase; "", strong increase. If staining was not uniform in onelesion, the secondary pattern is given in parentheses.Abbreviations: BCF, basophilic cell focus; cHCA/cHCC, clear cell HCA/clear cell HCC; bHCA/bHCC, basophilic HCA/basophilic HCC; GST-P, glutathioneS-transferase (placental form); N.D., not determined.*Data obtained from a previous study (see ref. 23).cX-fold increase when compared with the adjacent unaltered liver tissue.
HCA and HCC after Islet Transplantation
www.aacrjournals.org 1839 Cancer Res 2006; 66: (3). February 1, 2006
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

integrity of the islets became disrupted and small clusters or singleislet cells were scattered within the tumor.In the few animals of the MG, CG 1, and CG 6, which became
normoglycemic after z10 months posttransplantation, the overallnumber of islets was reduced but the remaining islets wereconsiderably enlarged and consisted predominantly of large h-cells (Fig. 4J). In addition, we observed two and one insulinomasthat had originated 15 to 18 months after transplantation fromgrafts in the MG and CG 6, respectively (Fig. 4K and L). Noinsulinomas in the pancreas have emerged. The liver tissuesurrounding the insulinomas showed small areas of glycogenstorage; however, owing to the systemic hypoglycemia in theseanimals, this was not as pronounced and is much more variablethan in the CCF of hyperglycemic animals. Nevertheless, theseanimals had classic preneoplastic foci in other parts of the liver thatwere obviously progressed to a state in which they became
independent from the previously important hyperglycemia. Wedid not observe a topographic relation between insulinomas andhepatocellular tumors.
Discussion
In this experiment, we confirmed previous findings made instreptozotocin diabetic Lewis rats (19–25), showing that low-number transplantation of pancreatic islets into the liver exerts astrong carcinogenic influence on the downstream hepatocytes instreptozotocin diabetic BB/Pfd rats (CG 6-8). This study is the firstto show that the same carcinogenic process can be induced inspontaneously autoimmune diabetic BB/Pfd rats (MG and CG1),providing conclusive evidence that hepatocarcinogenesis in thismodel is a result of islet-derived factors and is independent fromstreptozotocin.
Figure 3. Histomorphology of alteredliver acini, hepatocellular neoplasms,and control livers. A, in CG 2, animalsstayed normoglycemic owing to the highnumber of transplanted islets; thus,no hepatocellular alterations emergeddownstream of the islets. At thetransplantation site, a few lymphocyteswere often visible (top right part of theislet in A), even when the transplants werenot rejected. B to F, stepwise developmentto a HCC in the MG, beginning with aslightly progressed CCF (B ), early mixedcell focus with areas of glycogen depletion(C ), early clear cell HCA (D ), largeclear cell HCA (E), and basophilic(glycogen-poor) HCC (F ). Arrows (B-D),islet grafts belonging to the respective liverlesion. In CG 1 (G and H), the transplantedislets were rejected after low-numbertransplantation, but the respectivehepatocellular lesions persisted; arrows,mononuclear cell infiltrate in the area of therejected islet. On serial sections of theseanimals, no vital islet epithelial cellswere present. G, mixed cell focus;H, a very early HCA with nodularexpansive growth and mitotic figures(arrowheads ). A to H, PAS reaction.Time after transplantation and length ofthe lower edge of the panel: A, 12 months,1.1 mm; B, 7 months, 1.8 mm; C, 7months, 1.5 mm; D, 14 months, 2.2 mm;E, 14 months, 720 Am; F, 18 months,900 Am; G, 8 months 720 Am; H,13 months, 720 Am.
Cancer Research
Cancer Res 2006; 66: (3). February 1, 2006 1840 www.aacrjournals.org
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

The sequence of hepatocellular alterations in the BB/Pfd rats,beginning with the early formation of CCF even a few days after islettransplantation and progressing partly via mixed cell foci andbasophilic cell foci to HCAs and HCCs, was qualitatively andquantitatively not different from our previous results (19–25). In thebeginning, CCF were always confined to the anatomic borders of theliver acini that drain the hyperinsulinemic blood from the isletgrafts. Moreover, all metabolic andmorphologic alterations, without
exception, are typical insulin effects, and we showed increasedintracellular insulin signaling in these cells via IRS-1 and the Ras-Raf-MAPK pathway. Thus, CCF must be interpreted as adaptivealterations resulting from increased insulin action, although minoradditional effects of other islet hormones cannot be ruled out. Thisis also corroborated by the fact that these alterations in preneo-plasias and the subsequent development into hepatocellular tumorsonly took place in the right part of the liver in which the islet
Figure 4. Morphology of transplanted islets (A-F ), islet grafts during rejection (G-I ), and development of insulinomas (J-L ). After high-number islet transplantation andresulting normogylcemia, the transplants remained more compact (CG2 in A ; CG7 not shown), whereas after low-number transplantation (MG in B-F ) the islet cellsintermingled with the liver parenchyma (B ). Activated h-cells showed degranulation and hyperplasia of smooth endoplasmic reticulum and Golgi fields in electronmicroscopy (C ). Note the atrophy of the a-cell, packed with electron-dense secret granules (top right part of C). D to F, the same lesion showing an islet graftsurrounded by a CCF of altered hepatocytes (E and F , insulin immunostain). In CG 1 (G and I ) and CG 3 (H ), mononuclear inflammatory infiltrates and rejection of theislets were visible. H, an insulin immunostain showing a few h-cells during rejection. I, a fibrotic scar marks the former place of a rejected islet in the center of aglycogenotic CCF (note strong PAS reactivity in the surrounding hepatocytes); thus, this CCF persists without depending on continuing insulin action. Insulinomasoccurred only in MG and CG 6. The h-cells of the transplanted islets in these groups proliferated until the animal became normoglycemic at 10 months or later.Then, single large islets were visible (J ). In single animals, these large islets continued to proliferate and secrete insulin, resulting in the formation of insulinomasand severe hypoglycemia (K and L show the same insulinoma). A, B, and G, semithin sections stained according to Richardson; C, electron micrograph of an ultrathinsection; D and K, unstained liver slices; E, F, H, and L, insulin immunostain; I and J, PAS stain. Time after transplantation and length of the lower edge of the panel:A, 13 months, 360 Am; B, 9 months, 360 Am; C, 5 months, 9.6 Am; D-F (same lesion), 11 months, D, 3.6 mm, E, 2.9 mm, F, 570 Am; G, 8 months, 360 Am;H, 1 month, 280 Am; I, 13 months, 360 Am; J, 13 months, 1.1 mm; K and L (same lesion), 14 months, K, 14.5 mm, L, 1.1 mm.
HCA and HCC after Islet Transplantation
www.aacrjournals.org 1841 Cancer Res 2006; 66: (3). February 1, 2006
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

grafts were transplanted. Similar to streptozotocin diabetic Lewisrats, preneoplastic CCF virtually did not develop in animals afterhigh-number islet transplantation, which fully compensates thediabetic state and establishes normoglycemia, illustrating thathyperglycemia is also of relevance for tumor development. However,even high-number islet transplantation in conjunction withnormoglycemia has at least cocarcinogenic potential, as it stronglypromotes hepatocarcinogenesis in Lewis rats, initiated by admin-istration of the hepatocarcinogen N-nitrosomorpholine (26),indicating a dose-dependent effect of insulin and glucose levels.Preneoplastic foci did not regress in late-stage animals of the MG orCG 6 that became normoglycemic or even hypoglycemic owing toexcessive insulin production by hyperplastic transplants or graftinsulinomas, which corroborates similar observations formerlymade in Lewis rats (45). However, a new and interesting finding wasthat CCF also did not regress in animals of CG 1, which showed arejection of islet grafts after several months of tolerance and localhyperinsulinism (Fig. 1I and 4I). These observations clearly indicatethat at this time point, the primary adaptive nature of these CCF hasalready changed and that neoplastic transformation no longerdepends on insulin action. In this context, the overexpression ofother tumorigenic growth factors or their receptors, such as TGF-a,which has been shown to promote hepatocarcinogenesis intransgenic mice (46, 47), in the late stage lesions and neoplasmsof the present model is interesting. The point of transformation ofthe purely adaptive alterations of the liver acini into genetically or,probably initially more likely, epigenetically fixated preneoplasiasthat did no longer spontaneously regress must lie between 3 and 12months after transplantation. The clarification of this importantbiological alteration and the underlying mechanisms is one of themost interesting aims for future studies.To the best of our knowledge, no detailed histopathologic
studies of human recipient livers in clinical islet transplantationhave been done nor has the occurrence of hepatocellular neo-plasms been reported. However, Hirshberg et al. (48) conducteda histopathologic study of livers in a nonhuman primate modeland showed glycogenotic CCF, which only developed in onesingle animal that was insufficiently treated by a too low num-ber of functioning islet grafts and that stayed hyperglycemic.Histologic reports in humans generally deal with the islet graftmorphology and do not describe the liver morphology in detail(8). However, there are a few recent single case reports or small
series of cases that describe focal, mostly steatotic, or glyco-genotic alterations in the livers of islet transplant recipientsthat are strikingly similar to our observations (5–7, 49). Themacroscopic descriptions and the histopathologic depictions ofthese alterations, as well as the clinical data (recurrence of hyper-glycemia, high fasting glucose levels) in these patients, are virtuallyidentical to the alterations seen in our rats, illustrating obvioussimilarities in the metabolic situation and its influence on thehepatocytes in our model and in a group of clinically transplantedpatients.The increased incidence of HCC in human diabetic patients
reported in epidemiologic and case-control studies is not wellunderstood. We suggest, although not always being clearly stated,that these patients are suffering from type 2 diabetes mellitus,which is usually characterized by hyperglycemia and hyper-insulinemia. On the one hand, the metabolic situation in thesepatients is similar to that in the altered liver acini of our modeland some researchers have indeed proposed that insulin andglucose may directly be involved in the carcinogenic process inhumans (11, 14). On the other hand, the occurrence ofhepatocellular CCF in human livers that resemble preneoplasticCCF known from a variety of animal models has been shown (50),and even indications for their involvement in human hepatocarci-nogenesis have been found (51). Therefore, our results may help tounderstand how the combination of insulin action with thediabetic state can alter the expression of growth factors and theirreceptors, intracellular signaling, enzyme activities, morphology,and proliferative activity of hepatocytes, thus inducing and/orpromoting hepatocarcinogenesis. In addition, they may also helpto explain the increase in HCC incidence in human type 2 diabeticpatients and warrant a careful observation of liver alterations inpatients having undergone clinical islet transplantation.
Acknowledgments
Received 8/5/2005; revised 10/14/2005; accepted 11/16/2005.Grant support: Deutsche Forschungsgemeinschaft (German Research Foundation)
grant Do622/1-5.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.
We thank Gabriele Becker, Jorg Bedorf, Danuta Chrobok, Mariana Dombrowski,Mathilde Hau-Liersch, Regine Landeck, and Claudia Miethke for technical assistance;Yvonne Fischer and Kurt Rudel for animal care; and Bernd Wusthoff for editing themanuscript.
References
1. Ricordi C, Strom TB. Clinical islet transplantation:advances and immunological challenges. Nat RevImmunol 2004;4:259–68.
2. Rother KI, Harlan DM. Challenges facing islettransplantation for the treatment of type 1 diabetesmellitus. J Clin Invest 2004;114:877–83.
3. Ryan EA, Lakey JRT, Paty BW, et al. Successful islettransplantation. Continued insulin reserve provideslong-term glycemic control. Diabetes 2002;51:2148–57.
4. Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplan-tation in seven patients with type 1 diabetes mellitususing a glucocorticoid-free immunosuppressive regi-men. N Engl J Med 2000;343:230–8.
5. Ryan ER, Lakey JRT, Rajotte RV, et al. Clinical outcomesand insulin secretion after islet transplantation with theEdmonton protocol. Diabetes 2001;50:710–9.
6. Eckhard M, Lommel D, Hackstein N, et al. Dissemi-nated periportal fatty degeneration after allogeneic
intraportal islet transplantation in a patient with type1 diabetes mellitus: a case report. Transplant Proc 2004;6:1111–6.
7. Bhargava R, Senior PA, Ackerman TE, et al. Prevalenceof hepatic steatosis after islet transplantation and itsrelation to graft function. Diabetes 2004;53:1311–7.
8. Sever CE, Demetris AJ, Zeng Y, et al. Islet cellallotransplantation in diabetic patients. Histologicfindings in four adults simultaneously receiving kidneyor liver transplants. Am J Pathol 1992;140:1255–60.
9. El-Serag HB, Tran T, Everhart JE. Diabetes increasesthe risk of chronic liver disease and hepatocellularcarcinoma. Gastroenterology 2004;126:460–8.
10. El-Serag HB. Hepatocellular carcinoma: recenttrends in the United States. Gastroenterology 2004;127:S27–34.
11. Caldwell SH, Crespo DM, Kang HS, Al-Osaimi AMS.Obesity and hepatocellular carcinoma. Gastroenterology2004;127:S97–103.
12. Adami HO, Chow WH, Nyren O, et al. Excess risk of
primary liver cancer in patients with diabetes mellitus.J Natl Cancer Inst 1996;89:317–8.
13. Wideroff L, Gridley G, Mellemkjaer L, et al. Cancerincidence in a population based cohort of patientshospitalized with diabetes mellitus in Denmark. J NatlCancer Inst 1997;89:1360–5.
14. Lagiou P, Kuper H, Stuver SO, Tzonou A, Trichopou-los D, Adami HO. Role of diabetes mellitus in theetiology of hepatocellular carcinoma. J Natl Cancer Inst2000;92:1096–9.
15. Davila JA, Morgan RO, Shaib Y, McGlynn KA, El-SeragHB. Diabetes increases the risk of hepatocellularcarcinoma in the United States: a population basedcase control study. Gut 2005;54:533–9.
16. Huo TI, Lee SD, Wu JC. Is diabetes a risk factor forhepatocellular carcinoma? Gastroenterology 2004;127:360–1.
17. El-Serag HB, Everhart JE. Reply to: Huo TI, Lee SD,Wu JC. Is diabetes a risk factor for hepatocellularcarcinoma? Gastroenterology 2004;127:361–2.
Cancer Research
Cancer Res 2006; 66: (3). February 1, 2006 1842 www.aacrjournals.org
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

18. Di Bisceglie AM. What every hepatologist shouldknow about endocrinology: obesity, diabetes, and liverdisease. Gastroenterology 2004;126:604–6.
19. Dombrowski F, Lehringer-Polzin M, Pfeifer U. Hyper-proliferative liver acini after intraportal islet transplan-tation in streptozotocin-induced diabetic rats. LabInvest 1994;71:688–99.
20. Dombrowski F, Filsinger E, Bannasch P, Pfeifer U.Altered liver acini induced in diabetic rats by portal veinislet isografts resemble preneoplastic hepatic foci intheir enzymic pattern. Am J Pathol 1996;148:1249–56.
21. Dombrowski F, Bannasch P, Pfeifer U. Hepatocellularneoplasms induced by low-number pancreatic islettransplants in streptozotocin diabetic rats. Am J Pathol1997;150:1071–87.
22. Scharf JG, Ramadori G, Dombrowski F. Analysis of theIGF axis in preneoplastic hepatic foci and hepatocellularneoplasms developing after low-number pancreatic islettransplantation into the livers of streptozotocin diabeticrats. Lab Invest 2000;80:1399–411.
23. Evert M, Schneider-Stock R, Dombrowski F. Over-expression of fatty acid synthase in chemically andhormonally induced hepatocarcinogenesis of the rat.Lab Invest 2005;85:99–108.
24. Evert M, Sun JP, Pichler S, Slavova N, Schneider-Stock R, Dombrowski F. Insulin receptor, insulinreceptor substrate-1, Raf-1, and Mek-1 during hormonalhepatocarcinogenesis by intrahepatic pancreatic islettransplantation in diabetic rats. Cancer Res 2004;64:8093–100.
25. Evert M, Schneider-Stock R, Dombrowski F. Apoli-poprotein A-IV mRNA overexpression in early preneo-plastic hepatic foci induced by low-number pancreaticislet transplants in streptozotocin-diabetic rats. PatholRes Pract 2003;199:373–9.
26. Dombrowski F, Jost C, Manekeller S, Evert M.Cocarcinogenic effects of islet hormones and N -nitro-somorpholine in hepatocarcinogenesis after intrahepatictransplantation of pancreatic islets in streptozotocin-diabetic rats. Cancer Res 2005;65:7013–22.
27. Bannasch P. Pathogenesis of hepatocellular carcino-
ma: sequential cellular, molecular, and metabolicchanges. Prog Liver Dis 1996;14:161–97.
28. Bannasch P, Klimek F, Mayer D. Early bioenergeticchanges in hepatocarcinogenesis: preneoplastic pheno-types mimic responses to insulin and thyroid hormone.J Bioenerg Biomembr 1997;29:303–13.
29. Nehrbass D, Klimek F, Bannasch P. Overexpression ofinsulin receptor substrate-1 emerges early in hepato-carcinogenesis and elicits preneoplastic hepatic glyco-genosis. Am J Pathol 1998;152:341–5.
30. Nehrbass D, Klimek F, Bannasch P, Mayer D. Insulinreceptor substrate-1 is over-expressed in glycogenoticbut not in amphophilic preneoplastic hepatic fociinduced in rats by N -nitrosomorpholine and dehydroe-piandrosterone. Cancer Lett 1999;140:75–9.
31. Bell RH, Jr., Hye WJ, Miyai K. Streptozotocin-inducedliver tumors in the Syrian hamster. Carcinogenesis 1984;5:1235–8.
32. Kazumi T, Yoshino G, Fujii S, Baba S. Tumorigenicaction of streptozotocin on the pancreas and kidney inmale Wistar rats. Cancer Res 1978;38:2144–7.
33. Okawa H, Doi K. Neoplastic lesions in streptozotocin-treated rats. Exp Anim 1983;32:77–84.
34. Mordes JP, Desemone J, Rossini AA. The BB rat.Diabetes Metab 1987;3:725–50.
35. Malaisse WJ, Courtois P, Scott FW. Insulin-dependentdiabetes and gut dysfunction: The BB rat model. HormMetab Res 2004;36:585–94.
36. Ramanathan S, Poussier P. BB rat lyp mutation andtype 1 diabetes. Immunol Rev 2001;184:161–71.
37. Hessner MJ, Wang X, Meyer L, et al. Involvement ofEotaxin, eosinophils, and pancreatic predisposition indevelopment of type 1 diabetes mellitus in thebiobreeding rat. J Immunol 2004;173:6992–7002.
38. Mathieu C, Kuttler B, Waer M, Bouillon R, Hahn HJ.Spontaneous reestablishment of self-tolerance in BB/Pfd rats. Transplantation 1994;58:349–54.
39. Kuttler B, Mathieu C, Waer M, Hahn HJ, Bouillon R.Lack of disease recurrence in diabetic BB/Pfd rats aftersyngeneic islet transplantation. Autoimmunity 1993;15:107–12.
40. Richardson KC, Jarrett L, Finke EH. Embedding inepoxy resins for ultrathin sectioning in electronmicroscopy. Stain Technol 1960;35:313–25.
41. Benner U, Hacker HJ, Bannasch P. Electron micro-scopical demonstration of glucose-6-phosphatase innative cryostat sections fixed with glutaraldehyde throughsemipermeable membranes. Histochemistry 1979;65:41–7.
42. Schmitz F, Bresciani R, Hartmann H, Braulke T.Effect of insulin-like growth factor II on uptake ofarylsulfatase A by cultured rat hepatocytes and Kupffercells. J Hepatol 1995;22:356–63.
43. Meehan CJ, Fleming S, Smith W, Baird JD. Idiopathicmegacolon in the BB rat. Int J Exp Pathol 1994;75:37–42.
44. Graham S, Courtois P, Malaisse WJ, Rozing J, ScottFW, Mowat AM. Enteropathy precedes type 1 diabetes inthe BB rat. Gut 2004;53:1437–44.
45. Dombrowski F, Klingmuller D, Pfeifer U. Insulinomasderived from hyperplastic intra-hepatic islet transplants.Am J Pathol 1998;152:1025–38.
46. Jhappan C, Stahle C, Harkins NR, Fausto N, Smith GH,Merlino GT. TGF-a overexpression in transgenic miceinduces liver neoplasia and abnormal development ofthe mammary gland and pancreas. Cell 1990;61:1137–46.
47. Lee GH, Merlino G, Fausto N. Development of livertumors in transforming growth factor a transgenicmice. Cancer Res 1992;52:5162–70.
48. Hirshberg B, Mog S, Patterson N, Leconte J, HarlanDM. Histopathological study of intrahepatic isletstransplanted in the nonhuman primate model usingEdmonton protocol immunosuppression. J Clin Endo-crinol Metab 2002;87:5424–9.
49. Sohn J, Siegelman ES, Osiason AW. Unusual patternsof hepatic steatosis caused by the local effect of insulinrevealed on chemical shift MR imaging. AJR Am JRoentgenol 2001;176:471–4.
50. Bannasch P, Haertel T, Su Q. Significance of hepaticpreneoplasia in risk identification and early detection ofneoplasia. Toxicol Pathol 2003;31:134–9.
51. Su Q, Bannasch P. Relevance of hepatic preneoplasiafor human hepatocarcinogenesis. Toxicol Pathol 2003;31:126–33.
HCA and HCC after Islet Transplantation
www.aacrjournals.org 1843 Cancer Res 2006; 66: (3). February 1, 2006
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from

2006;66:1833-1843. Cancer Res Frank Dombrowski, Chantal Mathieu and Matthias Evert RatsPancreatic Islet Transplants in Autoimmune Diabetic BB/Pfd Hepatocellular Neoplasms Induced by Low-Number
Updated version
http://cancerres.aacrjournals.org/content/66/3/1833
Access the most recent version of this article at:
Cited articles
http://cancerres.aacrjournals.org/content/66/3/1833.full#ref-list-1
This article cites 51 articles, 9 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/66/3/1833.full#related-urls
This article has been cited by 4 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerres.aacrjournals.org/content/66/3/1833To request permission to re-use all or part of this article, use this link
Research. on January 6, 2020. © 2006 American Association for Cancercancerres.aacrjournals.org Downloaded from