Embed Size (px)
Citation preview
PANCREATIC NEOPLASMS
Dr K Sreenath
Junior Resident, Dept of Surgery
RIMS Imphal
PANCREAS
Weighs between 75 and 125 g and measures 10 to
20 cm.
Lies in the retroperitoneum just anterior to the first
lumbar vertebrae
Divided into four portions, the head, neck, body
and tail.

PANCREAS ANATOMY
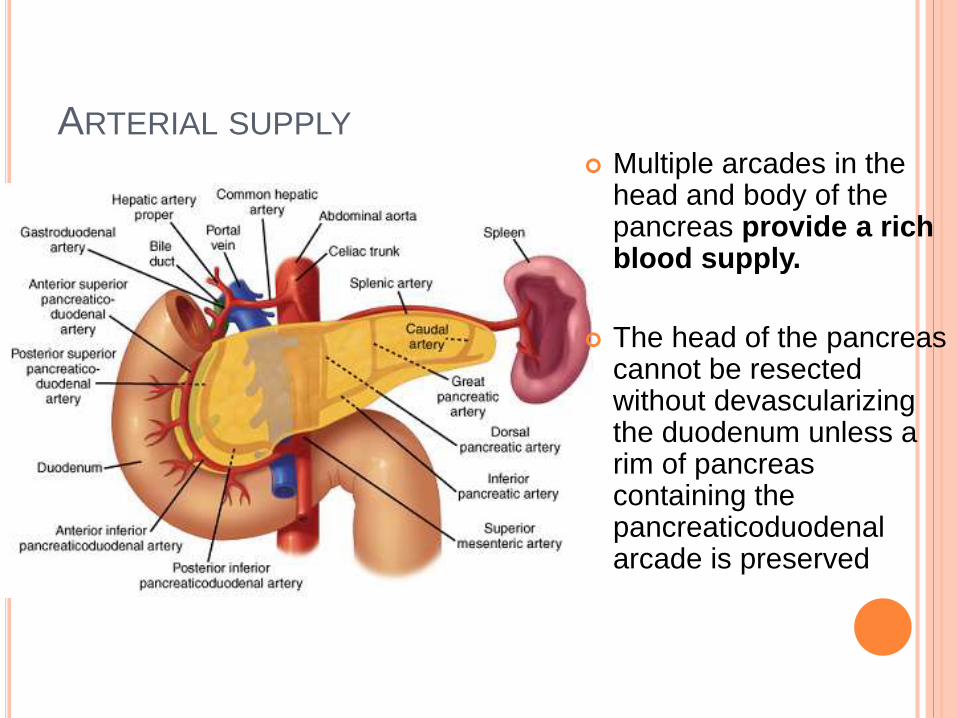
ARTERIAL SUPPLY
Multiple arcades in the head and body of the pancreas provide a rich blood supply.
The head of the pancreas cannot be resectedwithout devascularizingthe duodenum unless a rim of pancreas containing the pancreaticoduodenalarcade is preserved
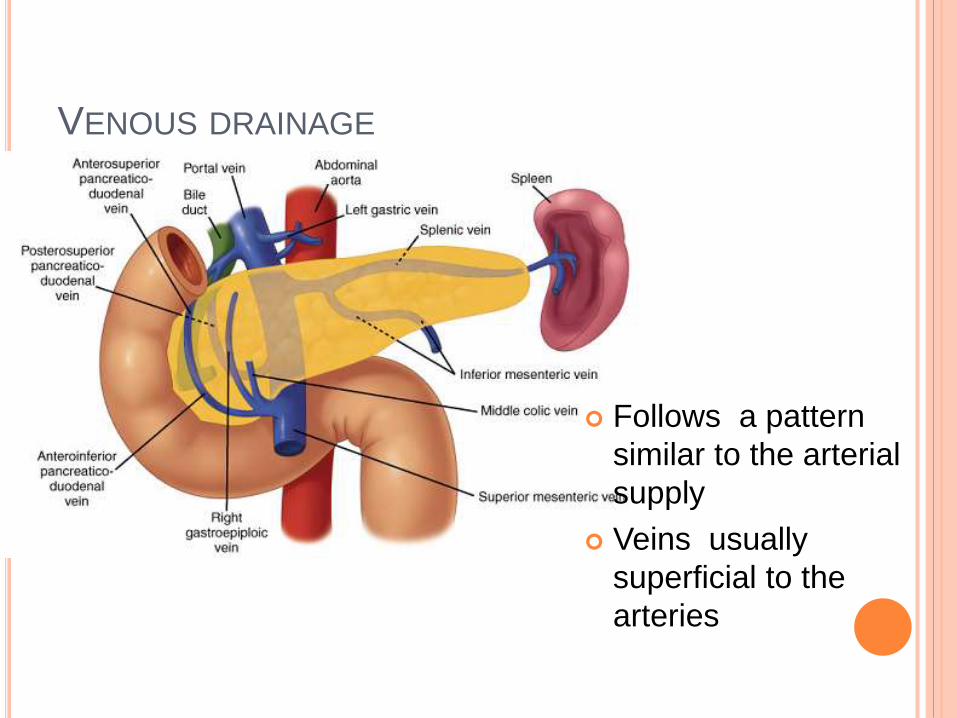
VENOUS DRAINAGE
Follows a pattern
similar to the arterial
supply
Veins usually
superficial to the
arteries
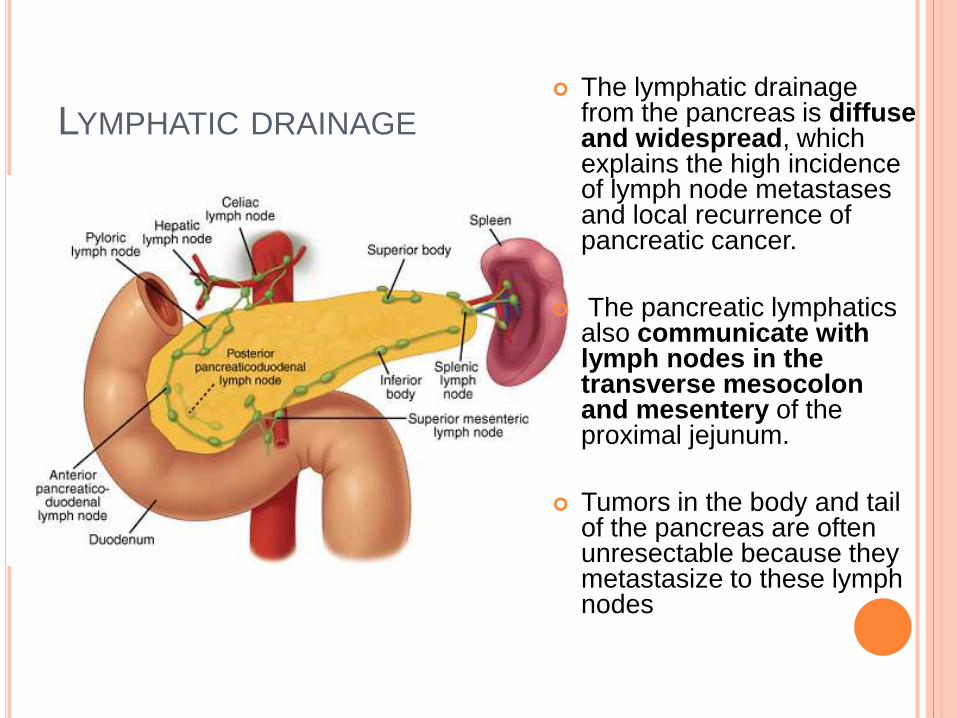
LYMPHATIC DRAINAGE
The lymphatic drainage from the pancreas is diffuse and widespread, which explains the high incidence of lymph node metastases and local recurrence of pancreatic cancer.
The pancreatic lymphaticsalso communicate with lymph nodes in the transverse mesocolonand mesentery of the proximal jejunum.
Tumors in the body and tail of the pancreas are often unresectable because they metastasize to these lymph nodes

INNERVATION
The pancreas has a rich supply of afferent sensory fibers that travel superiorly to the celiac ganglia.
Interruption of
these somatic fibers with a celiac plexus block can interfere with transmission of pancreatic pain
TYPES OF PANCREATIC NEOPLASMS
Neoplasms of exocrine pancreas
Cystic neoplasms account for <1% of
pancreatic cancers
Ductal adenocarcinoma >90% of pancreatic
cancers
Neoplasms of endocrine pancreas
Neuroendocrine tumors or islet-cell tumors,
rare
CARCINOMA EXOCRINE PANCREAS
MC – Ductal adenocarcinoma
Ninth most common cancer diagnosis
Fourth in cancer deaths
Men> women (1.3 : 1)
African Americans have a slightly higher risk
Mean age at diagnosis is 72 years
Incidence lowest in Middle East and in India
RISK FACTORS-ENVIRONMENTAL
Smoking
C/C Pancreatitis
Occuopational exposure
Diabetes
Obesity
Diet ( Rich in protein and fat)
Infectious - H pylori or HBV ?
Genetic
Alcohol , coffee and Radiation ..No Risk
(Maingot’s 12th edn p. 1188)
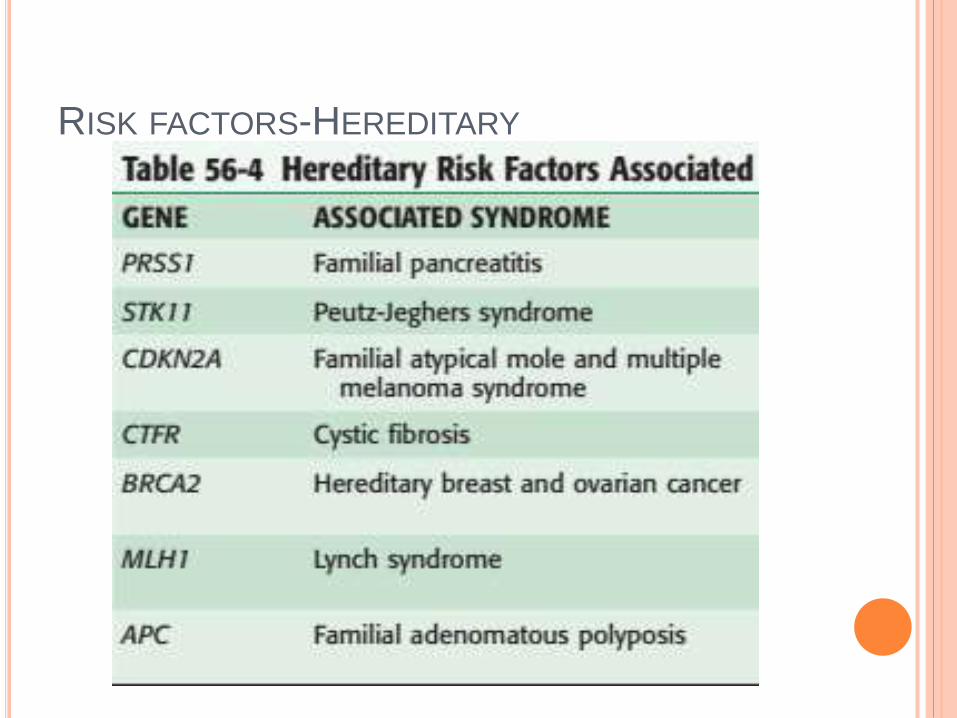
RISK FACTORS-HEREDITARY
PATHOGENESIS
Most cases are sporadic.
Sequential pathway has been observed in the development of PDAC from pancreatic intraepithelial neoplasia (PanIN) to invasive cancer.
Genes identified- PDX1, KRAS2, CDKN2A/p16, P53, and DPC4 (SMAD4).
KRAS2 oncogene is activated (by point mutation ) 95% of pancreatic cancers
Earliest event in tumorigenesis.

PanIN :
Progressive abnormality of the ductal epithelium from
columnar metaplasia (PanIN-1A) through carcinoma in
situ (PanIN-3).
PanIN-1A : Presence of columnar, mucin-producing ductal
epithelium
PanIN-1B : The development of papillary architecture
PanIN-2 : Evidence of nuclear atypia
PanIN-3 (carcinoma in situ): marked cytologic atypia,
complete loss of polarity
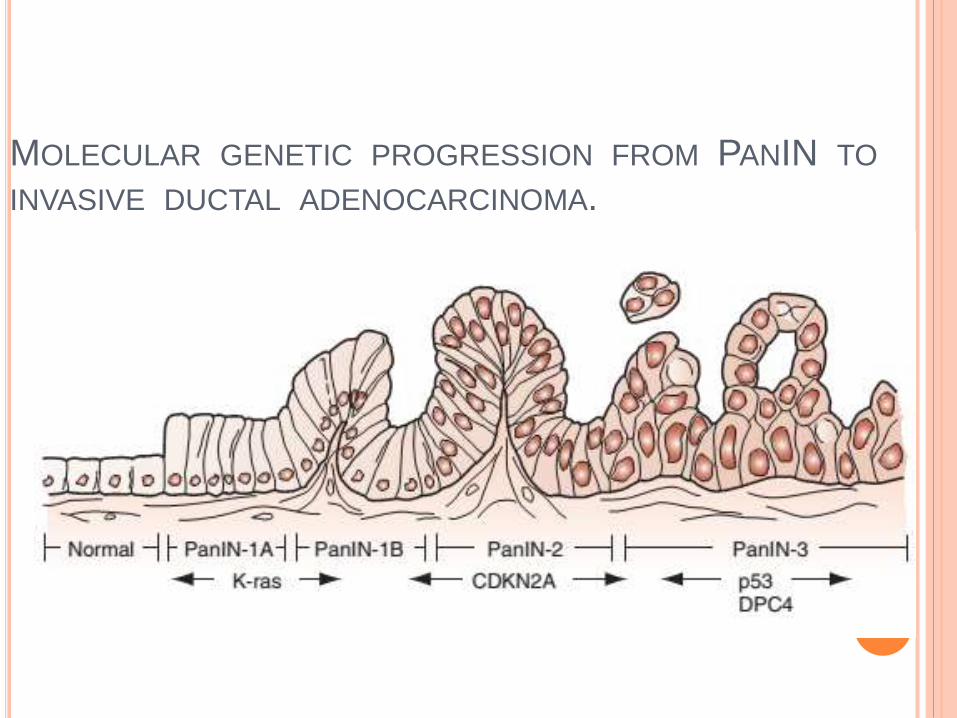
MOLECULAR GENETIC PROGRESSION FROM PANIN TO
INVASIVE DUCTAL ADENOCARCINOMA.
PERIAMPULLARY CARCINOMA
Adenocarcinomas of the
Head of the pancreas
Ampulla of Vater ,
Distal bile duct (cholangiocarcinoma),
Duodenum .
Less commonly, acinar cell carcinomas or
pancreatic endocrine neoplasms occur in the
periampullary region of the pancreas

CLINICAL PRESENTATION
CARCINOMA BODY AND TAIL
Late presentation
Pain and weight loss are more common
Rare
Poor prognosis
SIGNS
A palpable distended gallbladder (Courvoisier’s law)
Left supraclavicular node (Virchow’s node & Troisier’ssign )
Periumbilical lymphadenopathy may be palpable (Sister Mary Joseph’s node).
Peritoneal dissemination and perirectal tumor involvement may be palpable via digital rectal examination (Blumer’s shelf)
Migratory suprficial thrombophlebitis (Trousseau ‘s sign)
LABORATORY EVALUATION
Hepatic function evaluation
Coagulation profile
Nutritional assessment.
Tumor markers : CEA, CA19-9
CA19-9
Most sensitive most reliable tumor marker
for pretreatment evaluation and post-
treatment surveillance
IMAGING STUDIES
Ultrasound abdomen
Initial ivestigation
Multiphase Multidetector CT
- The imaging study of choice
- Three-phase (noncontrast, arterial,
and portal venous) CT scan with 3-
mm slices and coronal and 3 D
reconstruction
- Extension to SMA, Celiac axis, SMV-PV complex
and contiguous structures can be determined
- Metastasis can be asessed
- Resectability can be predicted
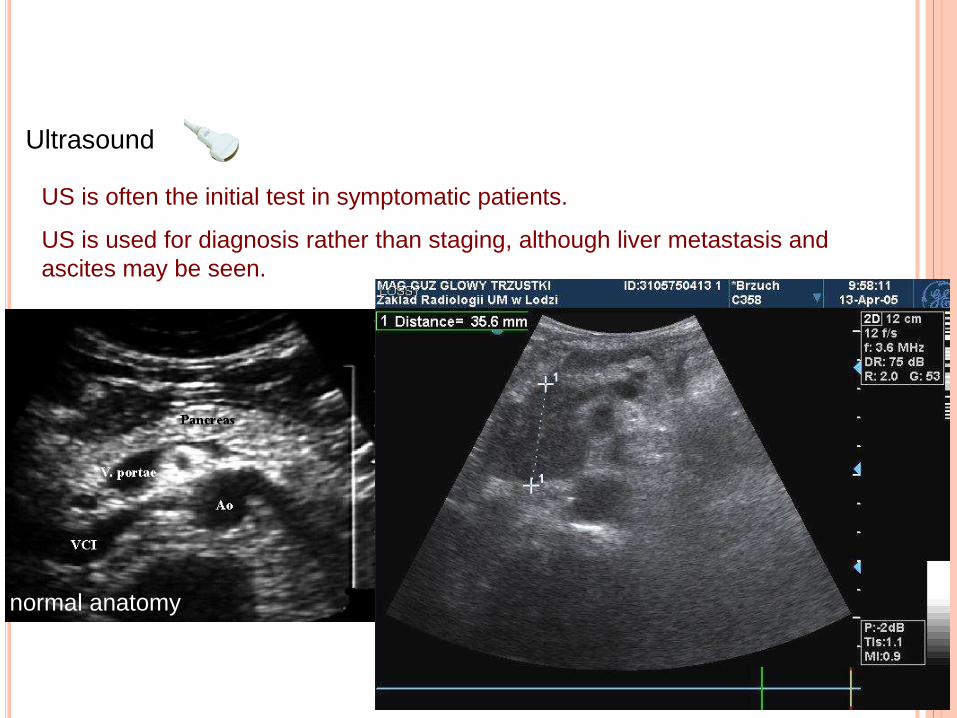
US is often the initial test in symptomatic patients.
US is used for diagnosis rather than staging, although liver metastasis and
ascites may be seen.
Ultrasound
normal anatomy
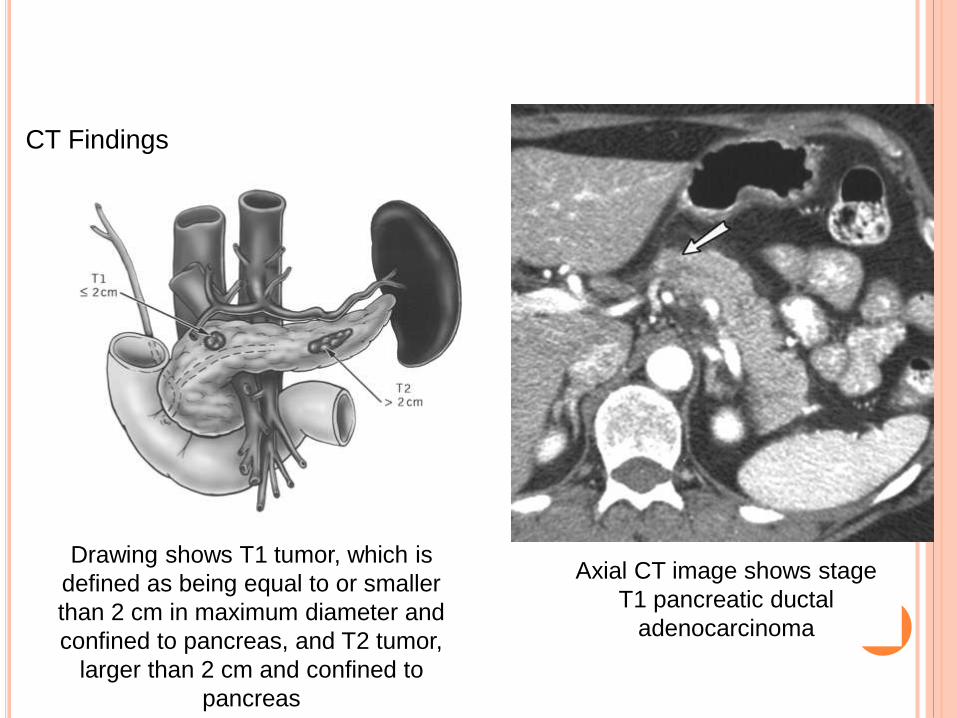
CT Findings
Axial CT image shows stage
T1 pancreatic ductal
adenocarcinoma
Drawing shows T1 tumor, which is
defined as being equal to or smaller
than 2 cm in maximum diameter and
confined to pancreas, and T2 tumor,
larger than 2 cm and confined to
pancreas

CT Findings
Drawing shows T3 tumor, defined as
tumor that may extend beyond
pancreas but without involvement of
celiac axis or superior mesenteric
artery.
Contrast-enhanced axial CT image shows T3 tumor that
has involved common bile duct, requiring a stent, and that
extends medially beyond confines of pancreatic head.
Tumor is separated from superior mesenteric vein (long
arrow) and superior mesenteric artery (short arrow) by fat
plane (type A relationship). Note that tumor involves
duodenum (arrowhead).

CT Findings
Drawing shows T4 tumor, defined as
primary tumor involving either
superior mesenteric artery or celiac
axis.
Contrast-enhanced axial CT image shows
pancreatic tumor (white arrows) engulfing
celiac axis. Short black arrow = splenic
artery, long black arrow = common
hepatic artery.
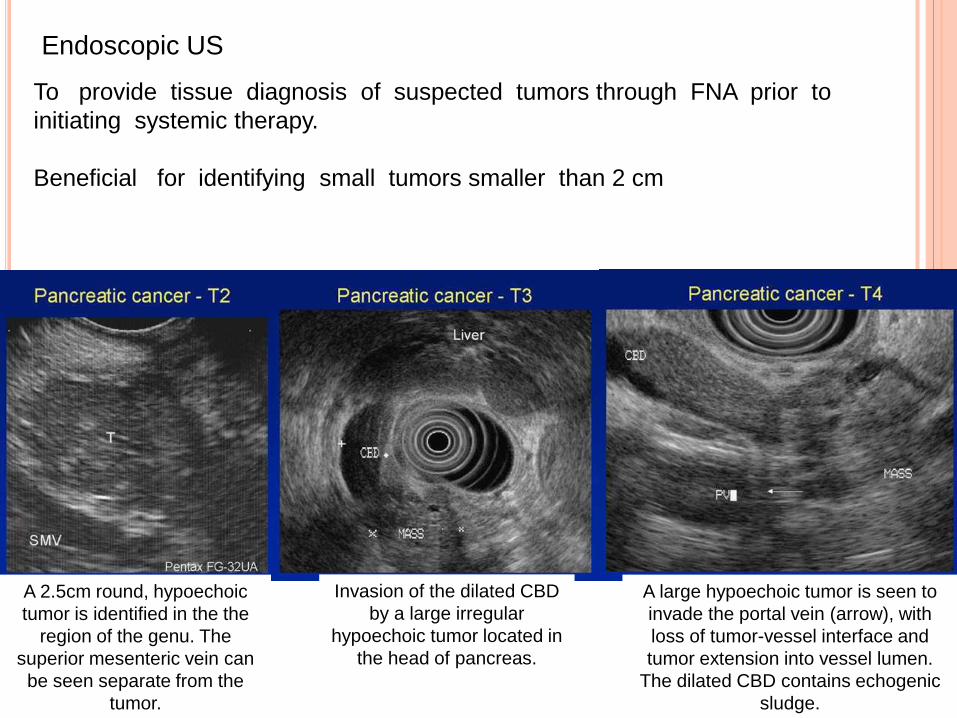
Endoscopic US
To provide tissue diagnosis of suspected tumors through FNA prior to
initiating systemic therapy.
Beneficial for identifying small tumors smaller than 2 cm
A 2.5cm round, hypoechoic
tumor is identified in the the
region of the genu. The
superior mesenteric vein can
be seen separate from the
tumor.
Invasion of the dilated CBD
by a large irregular
hypoechoic tumor located in
the head of pancreas.
A large hypoechoic tumor is seen to
invade the portal vein (arrow), with
loss of tumor-vessel interface and
tumor extension into vessel lumen.
The dilated CBD contains echogenic
sludge.
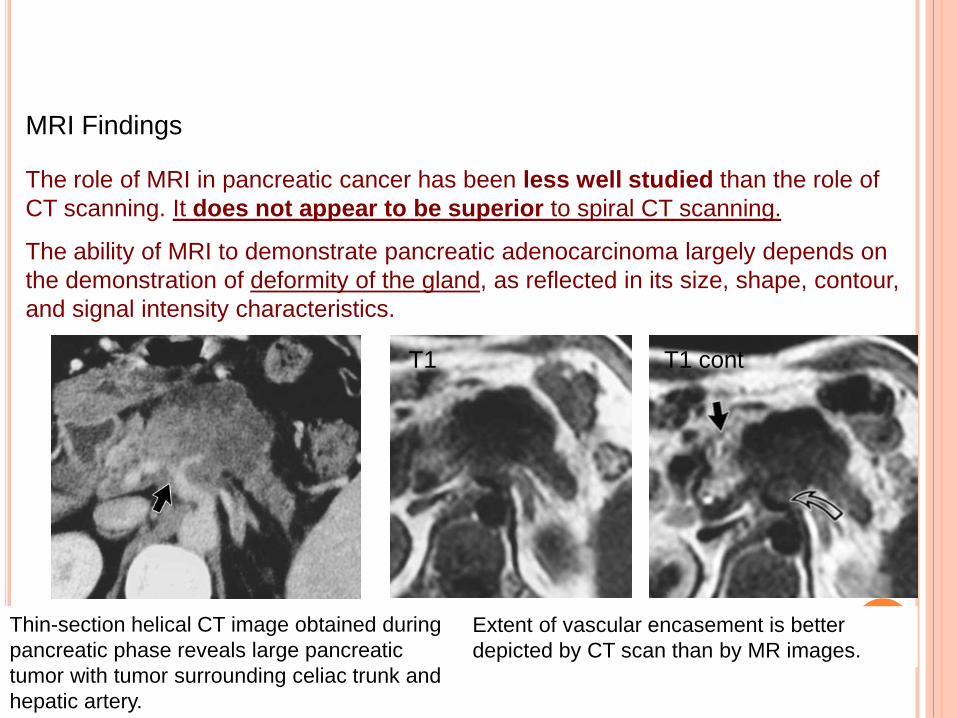
MRI Findings
The role of MRI in pancreatic cancer has been less well studied than the role of
CT scanning. It does not appear to be superior to spiral CT scanning.
The ability of MRI to demonstrate pancreatic adenocarcinoma largely depends on
the demonstration of deformity of the gland, as reflected in its size, shape, contour,
and signal intensity characteristics.
Thin-section helical CT image obtained during
pancreatic phase reveals large pancreatic
tumor with tumor surrounding celiac trunk and
hepatic artery.
Extent of vascular encasement is better
depicted by CT scan than by MR images.
T1 contT1
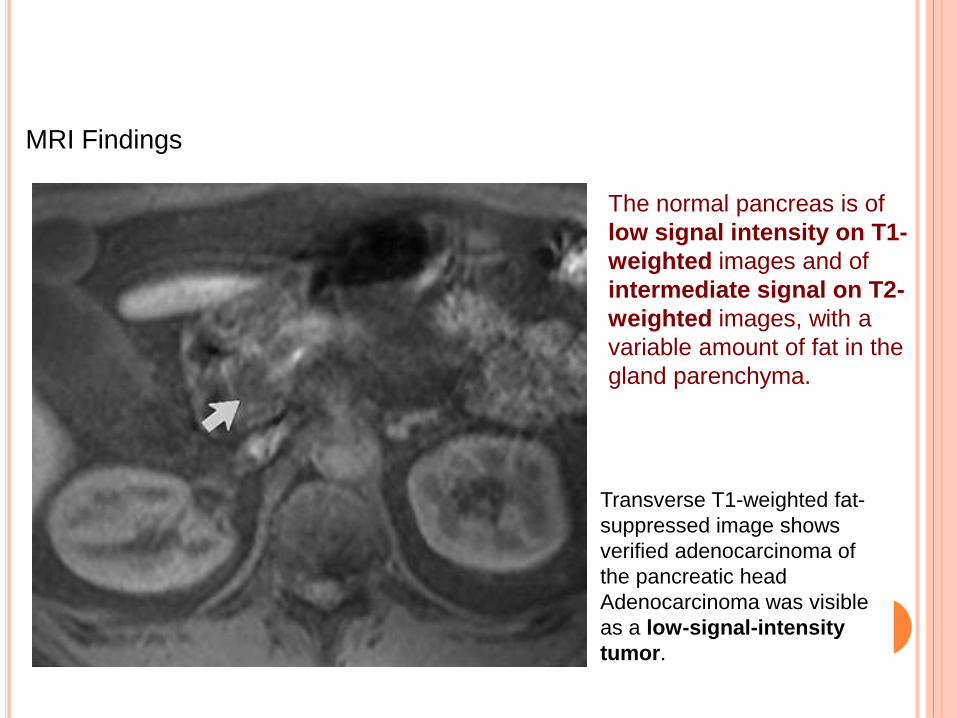
MRI Findings
Transverse T1-weighted fat-
suppressed image shows
verified adenocarcinoma of
the pancreatic head
Adenocarcinoma was visible
as a low-signal-intensity
tumor.
The normal pancreas is of
low signal intensity on T1-
weighted images and of
intermediate signal on T2-
weighted images, with a
variable amount of fat in the
gland parenchyma.

MRCP
Assessment of luminal pancreatobiliary anatomy
Usefull for cystic lesions of the pancreas
ERCP
- To perform a biopsy and palliate
jaundice (biliary stenting)
Signs
Abrupt block
PD encasement
Dubble duct sign
Scrambled egg appearance
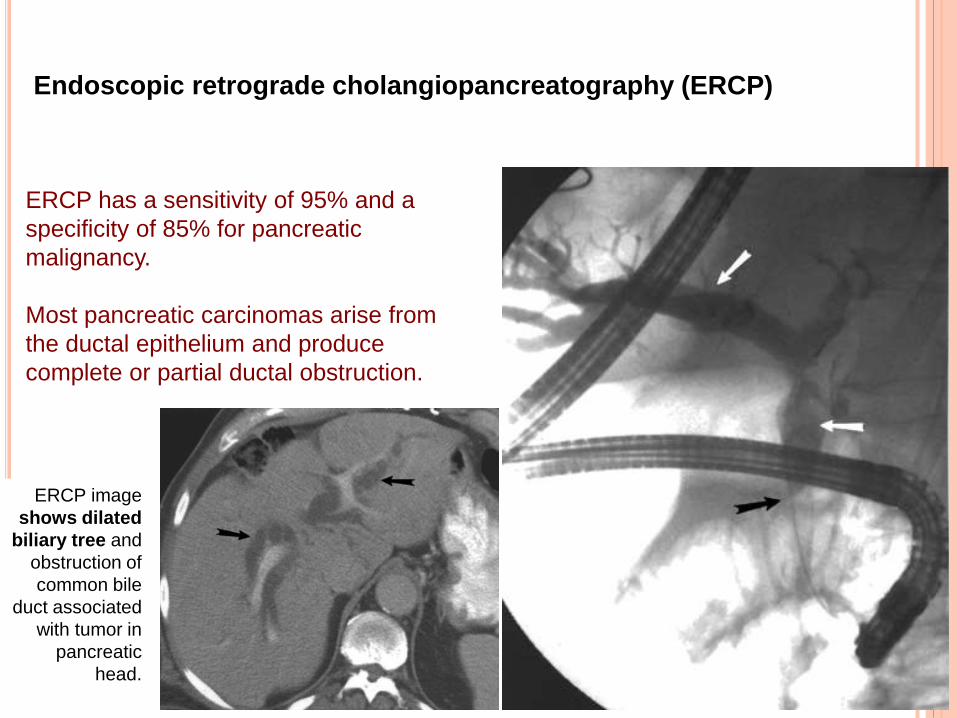
ERCP has a sensitivity of 95% and a
specificity of 85% for pancreatic
malignancy.
Most pancreatic carcinomas arise from
the ductal epithelium and produce
complete or partial ductal obstruction.
ERCP image
shows dilated
biliary tree and
obstruction of
common bile
duct associated
with tumor in
pancreatic
head.
Endoscopic retrograde cholangiopancreatography (ERCP)

ERCP image shows
slight narrowing of
pancreatic duct and
ductal dilatation.
Sphincterotomy was
performed, and
pancreatic stent was
placed.
Contrast-enhanced CT
scan fails to depict
tumor (arrow) around
stent in dilated common
bile duct.
Unenhanced T1-weighted MR
image shows inhomogeneity of
pancreatic head, but does not
show tumor.
Compared with other modalities, MRI appears to be more valuable for staging the
extent and spread of pancreatic carcinoma than for tumor detection of lesions
smaller than 2 cm.
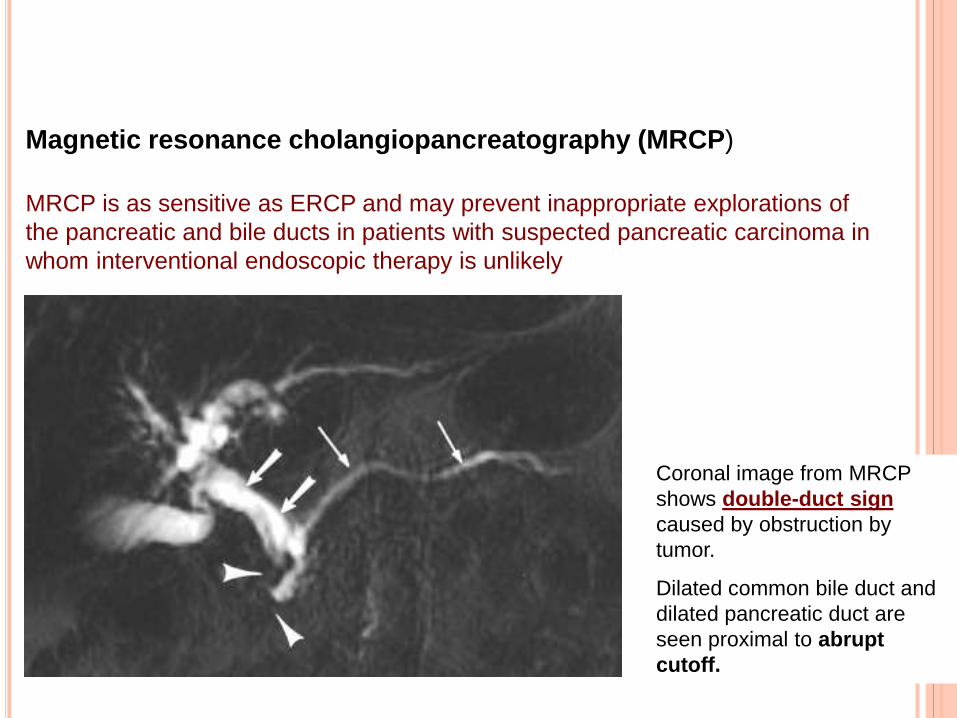
Magnetic resonance cholangiopancreatography (MRCP)
MRCP is as sensitive as ERCP and may prevent inappropriate explorations of
the pancreatic and bile ducts in patients with suspected pancreatic carcinoma in
whom interventional endoscopic therapy is unlikely
Coronal image from MRCP
shows double-duct sign
caused by obstruction by
tumor.
Dilated common bile duct and
dilated pancreatic duct are
seen proximal to abrupt
cutoff.
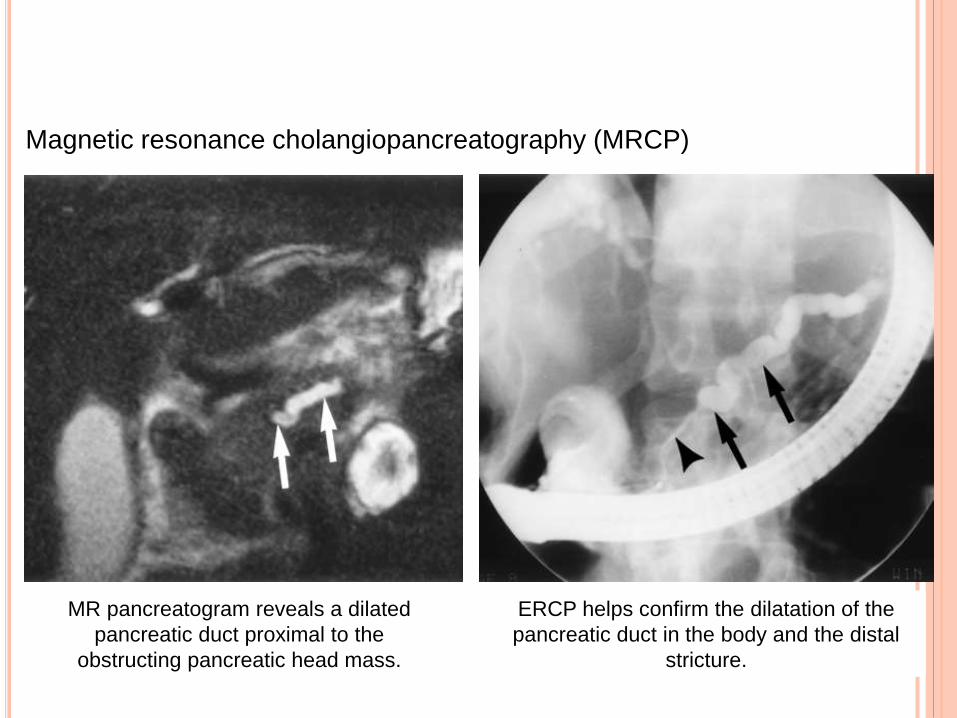
Magnetic resonance cholangiopancreatography (MRCP)
MR pancreatogram reveals a dilated
pancreatic duct proximal to the
obstructing pancreatic head mass.
ERCP helps confirm the dilatation of the
pancreatic duct in the body and the distal
stricture.
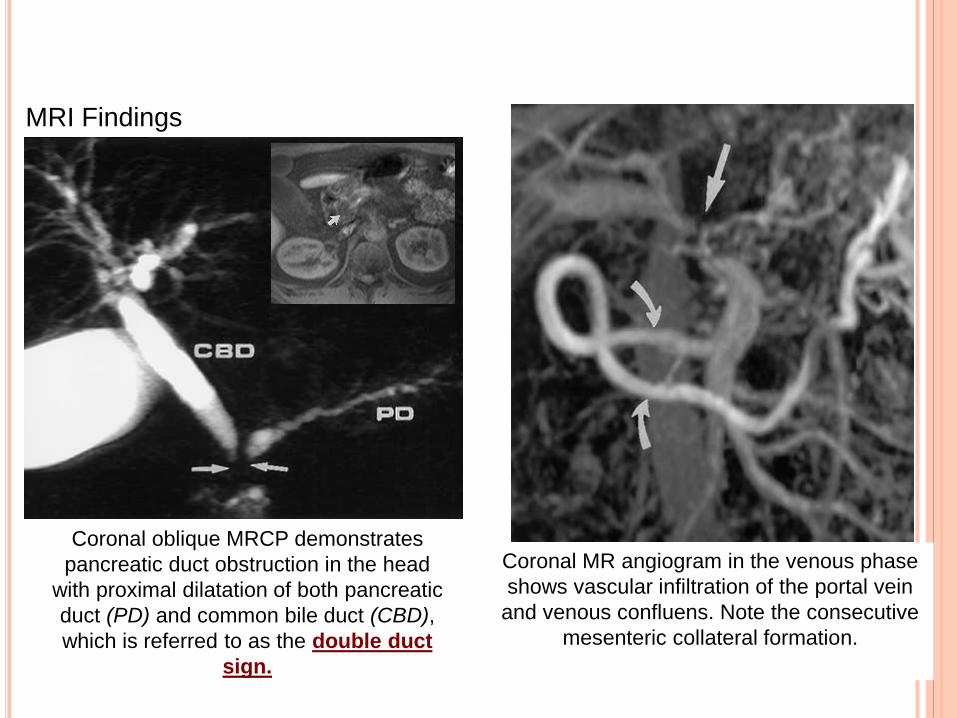
MRI Findings
Coronal oblique MRCP demonstrates
pancreatic duct obstruction in the head
with proximal dilatation of both pancreatic
duct (PD) and common bile duct (CBD),
which is referred to as the double duct
sign.
Coronal MR angiogram in the venous phase
shows vascular infiltration of the portal vein
and venous confluens. Note the consecutive
mesenteric collateral formation.
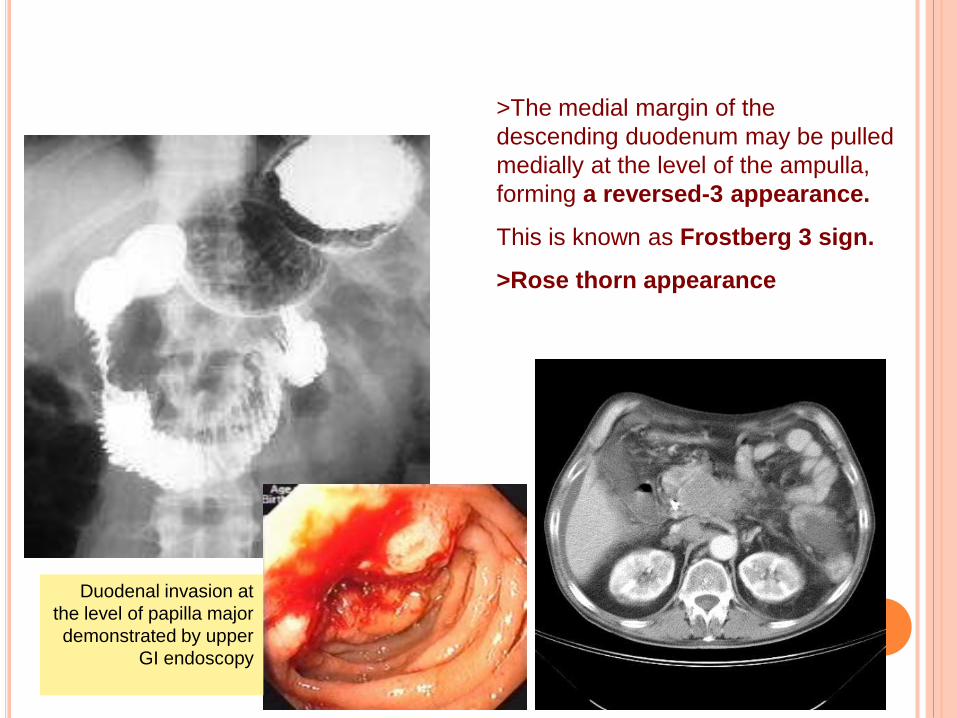
>The medial margin of the
descending duodenum may be pulled
medially at the level of the ampulla,
forming a reversed-3 appearance.
This is known as Frostberg 3 sign.
>Rose thorn appearance
Duodenal invasion at
the level of papilla major
demonstrated by upper
GI endoscopy

Upper GI barium studies may
reveal an extrinsic impression of
the mass on the posteroinferior
aspect of the antrum of the
stomach, widened C loop of
duodenum
This is known as antral pad
sign”.
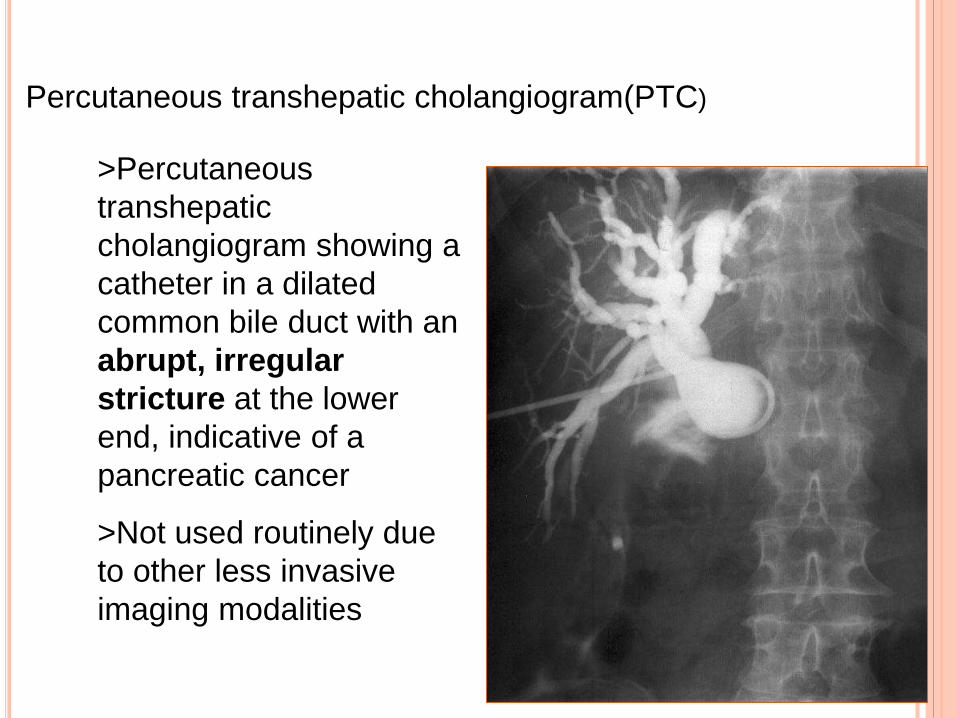
Percutaneous transhepatic cholangiogram(PTC)
>Percutaneous
transhepatic
cholangiogram showing a
catheter in a dilated
common bile duct with an
abrupt, irregular
stricture at the lower
end, indicative of a
pancreatic cancer
>Not used routinely due
to other less invasive
imaging modalities

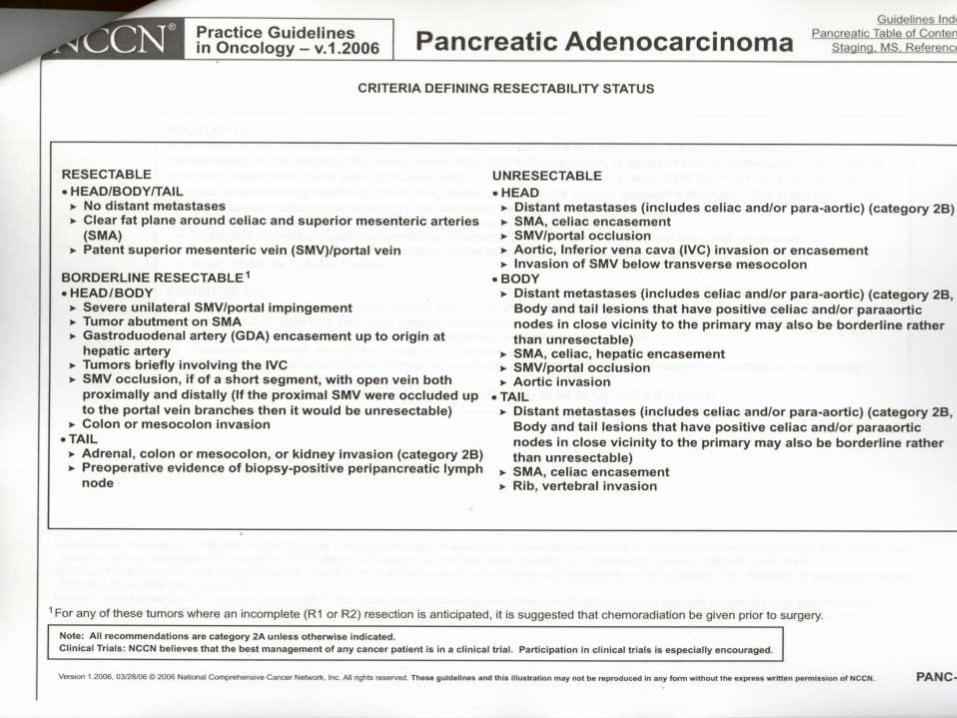
STAGING

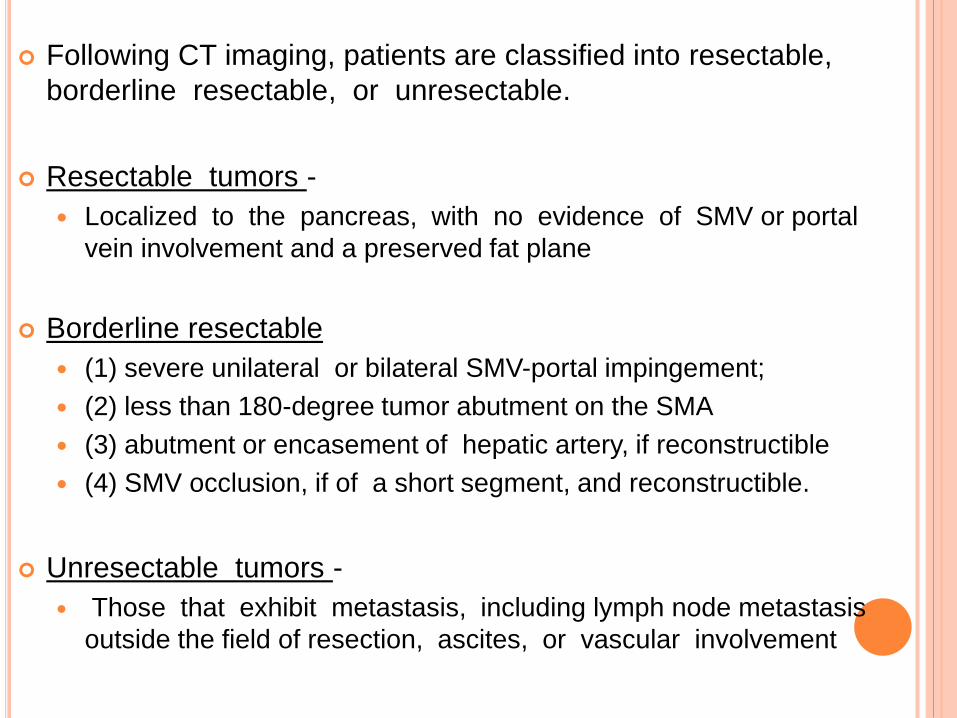
Following CT imaging, patients are classified into resectable,
borderline resectable, or unresectable.
Resectable tumors -
Localized to the pancreas, with no evidence of SMV or portal
vein involvement and a preserved fat plane
Borderline resectable
(1) severe unilateral or bilateral SMV-portal impingement;
(2) less than 180-degree tumor abutment on the SMA
(3) abutment or encasement of hepatic artery, if reconstructible
(4) SMV occlusion, if of a short segment, and reconstructible.
Unresectable tumors -
Those that exhibit metastasis, including lymph node metastasis
outside the field of resection, ascites, or vascular involvement
STAGING LAPROSCOPY
Indications
Large tumors (>3 cm)
Significantly elevated CA19-9 level (>100 U/mL)
Uncertain findings on CT
Body or tail tumors
PREOPERATIVE PREPARATION
Correction of anemia
Replenishment of glycogen store
Correction of dehydration
Injection of vitamin K
Adequate IV fluids and mannitol to ensure
adequate diuresis
Broad spctrum antibiotics 1-2 days prior
Enteral or parenteral nutrition
Pulmonary physiotherapy
Preoperative biliary drainage – contraversial
TREATMENTHead of the pancreas
> Pancreaticoduodenectomy is the
procedure of choice.
(Either Wipple’s or Traverso and Longmire)
> Laparoscopic Pancreaticoduodenectomy
Body and Tail of the Pancreas
Distal pancreatectomy and en
bloc splenectomy

PANCREATICODUODENECTOMY – 6 STEPS
1. A Cattell-Braasch maneuver
2. Extended Kocher maneuver
3. Portal dissection
4. Transect stomech
5. Transect jejunum
6. Transect pancreas and
complete retroperitoneal
dissection

PANCREATICODUODENECTOMY-
RECONSTRUCTIONS
1. End to side PJ
2. End to side HJ
3. End to side GJ
( antecolic)
STRUCTURES REMOVED
Distal stomach
Gall bladder
CBD
Head of Pancreas
Duodenum
Proximal jejunum
Regional lymphatics

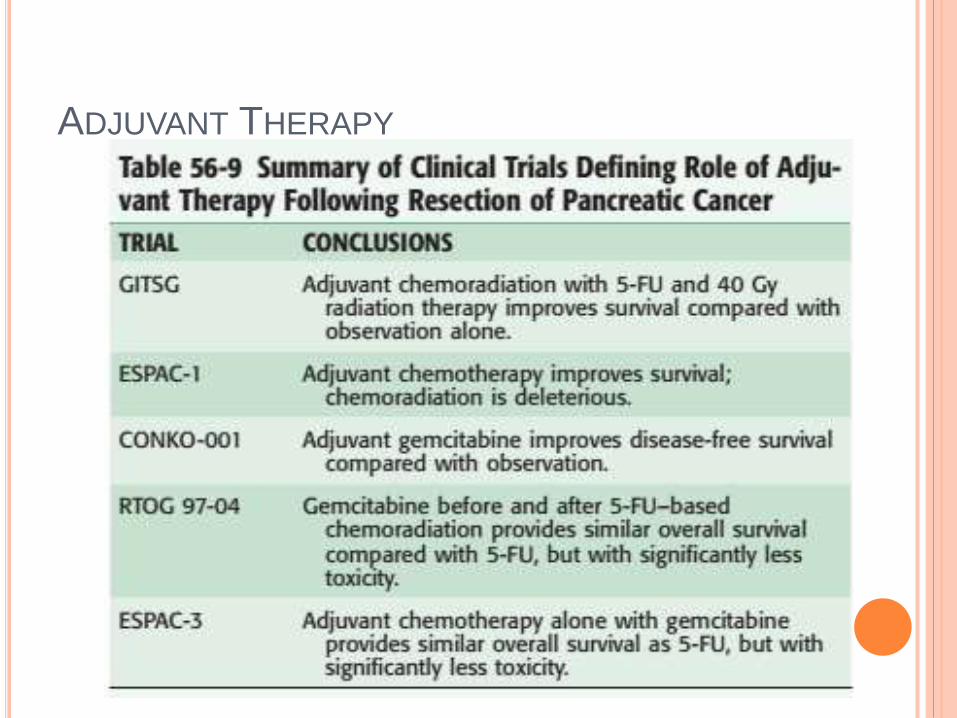
ADJUVANT THERAPY
PALLIATIVE THERAPY
Biliary Obstruction
ERCP with metal stent placement
Surgical biliary-enteric bypass (Roux-en-Y
hepaticojejunostomy)
Gastric Outlet Obstruction
Endoscopic luminal stenting
Double bypass consisting of a Roux-en-Y
hepaticojejunostomy and gastrojejunostomy
Pain Relief
NSAIDS or long acting opioids
Celiac nerve block
Neurolysis
RECENT ADVANCES
Immunotherapy
Allogenic tumor cell vaccine under phase 2 trial
Angiogenesis inhibitors
Becacizumab (anti VEGF) with gemcitabine under
phase 3 trial
K ras inhibitors
Tipifarnib ( farnesyl transferase inhibitor)- studied and
showed no improvement in outcome
EGFR inhibitors
EKB 569 and erlotinib
Erlotinib approved for treatment of unresectable
cancer( study by NCI of Canada)
CYSTIC NEOPLASMS OF THE PANCREAS
CYSTIC NEOPLASMS OF THE PANCREAS
Second most common exocrine pancreatic
neoplasm next to adenocarcinoma.
Types
Mucinous
Serous
IPMN
MUCINOUS CYSTIC NEOPLASM
Most common cystic neoplasms of the
pancreas.
Young women, Men are rarely affected.
Fifth decade.
Typically found in the body and tail of the
pancreas
Contain mucin-producing epithelium
Presence of mucin-rich cells and ovarian-like stroma
CT scan –
solitary , fine septations, surrounded by a rim of calcification
Predictors of malignancy
Eggshell calcification,
larger tumor size
mural nodule on cross-sectional imaging
EUS and cyst fluid analyses demonstrate
mucin-rich aspirate and
high CEA levels (>192 ng/mL)
low levels of amylase
Standard treatment - Pancreatic resection
SEROUS CYSTIC NEOPLASM
Predilection for the head of the pancreas
Vague abdominal pain and less frequently with weight
loss and obstructive jaundice
Large , wellcircumscribed masses.
Microscopy - multiloculated, glycogen-rich small cysts.

CT Scan-
Central calcification, with radiating septa giving the
sunburst appearance (10-20%)
Large (>4 cm) or rapidly growing, symptomatic lesion
Treatment is Resection
Small (<4 cm) , asyptomatic can be observed.
INTRADUCTAL PAPILLARY MUCINOUS
NEOPLASM
First described by Ohashi
Several names—
Mucin secreting carcinoma
Villous adenoma of the duct of Wirsung
Diffuse intraductal papillary adenocarcinoma
Intraductal cystadenoma
Mucinous duct ectasia, and
Intraductal papillary mucinous tumor.

Sixth to seventh decade of life.
Commonly in head region.
Wide spectrum
ranging from benign adenoma, borderline, carcinoma in
situ, and invasive adenocarcinoma.
Types-
Side branch or branch duct IPMN,
Main duct IPMNs,
Mixed -type IPMNs
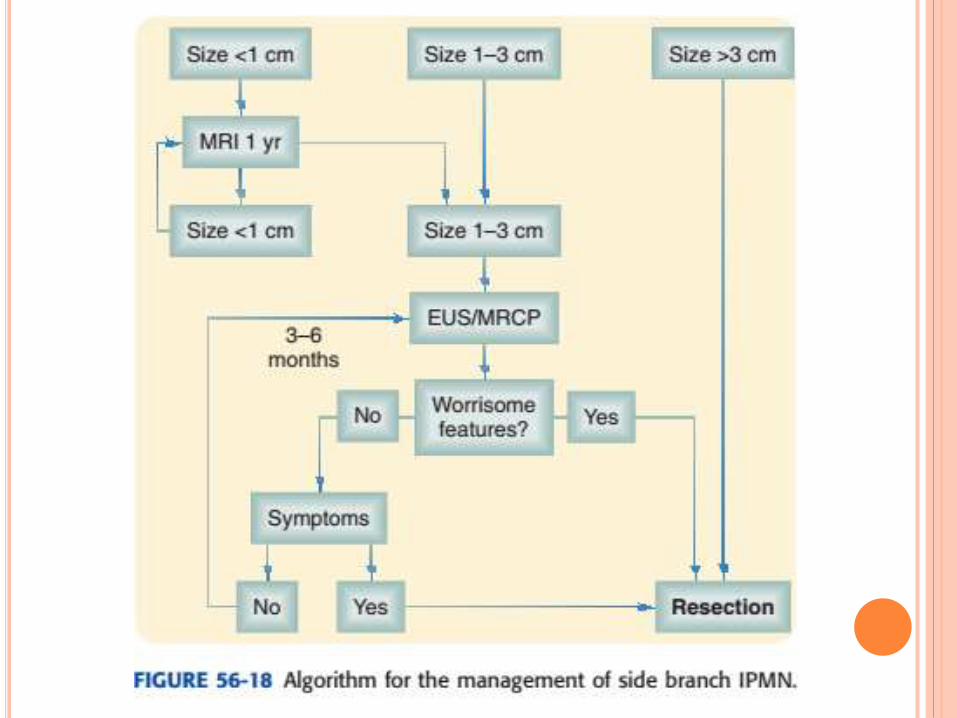
SIDE BRANCH IPMN
Involves dilation of the pancreatic duct side branches that communicate with but do not involve the main pancreatic duct.
Focal (involving a single side branch) or multifocal
Risk of malignant transformation directly related to the size of the cystic dilation
Others - mural nodules or general thickening of the cyst wall symptoms like jaundice, pain, and diabetes
Small (<1 cm) IPMNs:-
Surveillance with CT or MRI in 1 year
Asymptomatic cysts ,1 -3 cm:-
Imaging at 6 months followed by
annual evaluation if no change in size.
Cysts larger than 3 cm:-
Surgical resection (Partial
pancreatectomy)
Risk of invasive malignancy- 10% to 15%
MAIN DUCT IPMN
Abnormal cystic dilation of the main pancreatic duct with
columnar metaplasia
Endoscopy –
thick mucinous secretions oozing from patulous papilla
May be focal or diffuse
30% to 50% risk of harboring invasive pancreatic cancer at the
time of presentation.

Treatment- Surgical resection
(Risk of malignant transforamtion)
Predictors of malignancy-
Jaundice,
Elevated serum alkaline phosphatase
Mural nodules,
Diabetes
Main pancreatic duct diameter of 7 mm
Elevation of the CEA level is not predictive of invasive
malignancy
CT scans –
dilated main pancreatic duct, cysts of varying sizes,
and possibly mural nodules.
MRCP-
localization of mural nodules and pretreatment
classification of suspected side branch or main duct
types of IPMN
Aspirated fluid is typically viscous and clear, contains
mucin and columnar mucinous cells with variable atypia
Elevated CEA level (>192 ng/mL; log scale)

MIXED-TYPE IPMN
Side branch IPMN that has extended to involve the
main pancreatic duct
Risk of invasive malignancy at the time of
presentation (30% to 50%)
Surgical resection is indicated for the treatment


NEOPLASMS OF ENDOCRINE PANCREAS

Paul Langerhans medical student, in 1869
pale staining cells within the pancreas
Alpha (A) – Glucagon
Beta (B) – Insulin and amylin
Delta (D) – Somatostatin and
vasoactive intestinal
peptide (VIP)
F cells – Pancreatic
polypeptide (PP)
Gastrin-producing cells are normally present in the fetal pancreas only.
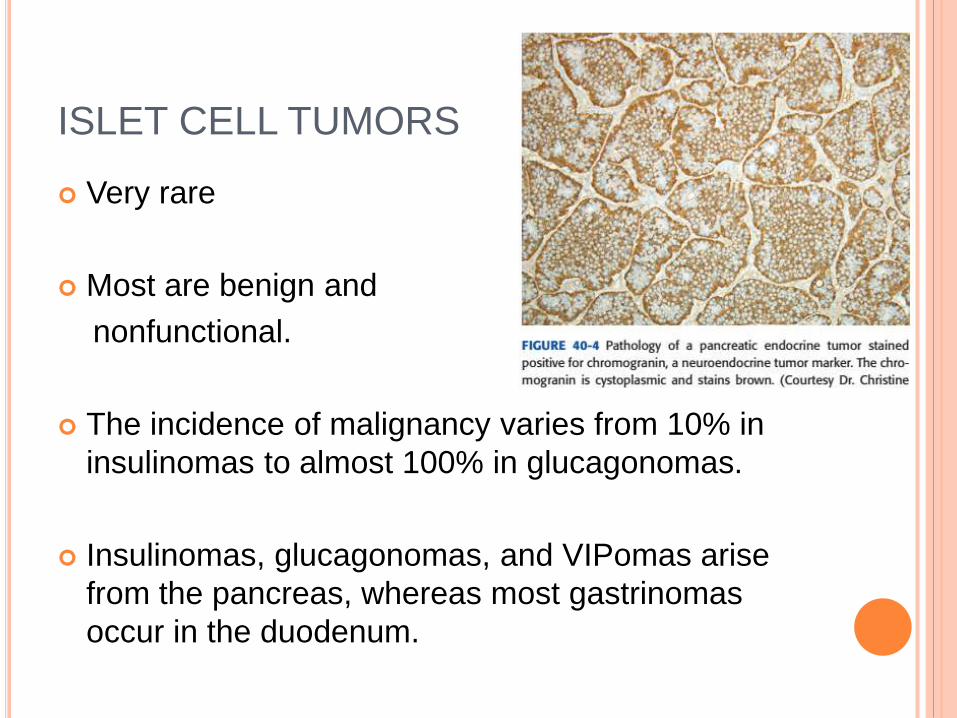
ISLET CELL TUMORS
Very rare
Most are benign and
nonfunctional.
The incidence of malignancy varies from 10% in
insulinomas to almost 100% in glucagonomas.
Insulinomas, glucagonomas, and VIPomas arise
from the pancreas, whereas most gastrinomas
occur in the duodenum.
MOLECULAR GENETICS
Distinct from that of pancreatic adenocarcinoma.
Transcriptional silencing is believed to play a
role in islet cell tumorigenesis.
Loss of heterozygosity (LOH) 11q is common in
functional pancreatic endocrine tumors
LOH 6q is associated with the development of
nonfunctional tumors.
INSULINOMA
Most common functioning tumor
Equal distribution in the head, body, and tail.
97% are located in the pancreas, remaining 3% are located in the duodenum, splenic hilum, or gastrocolicligament
Whipple’s triad
fasting-induced neuroglyopenic symptoms of hypoglycemia
low blood glucose levels (40 to 50 mg/dL),
relief of symptoms after the administration of glucose.
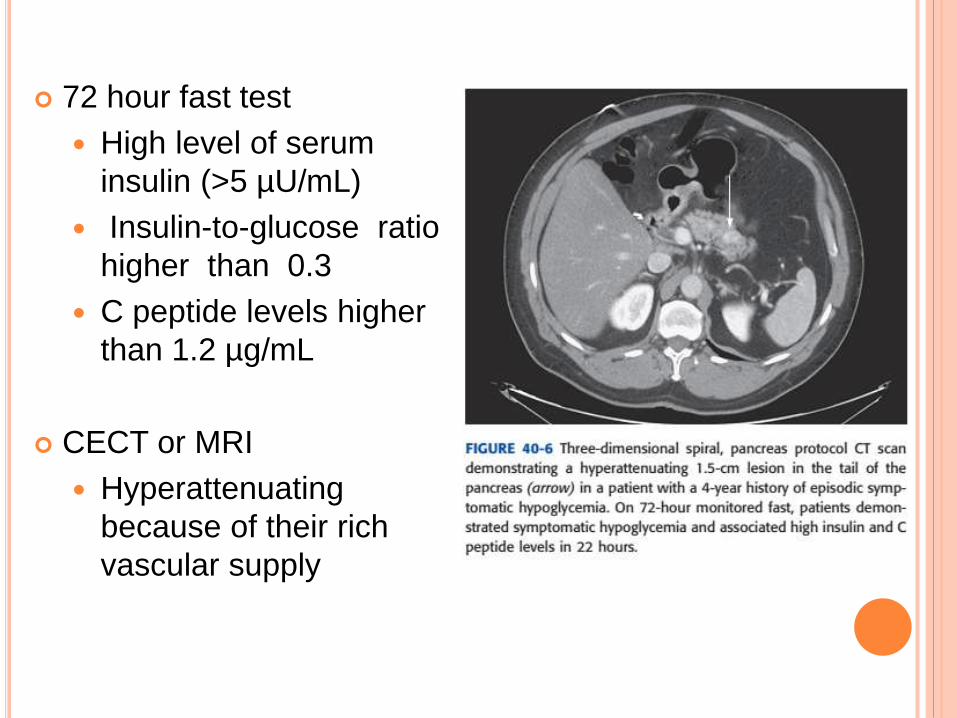
72 hour fast test
High level of serum
insulin (>5 µU/mL)
Insulin-to-glucose ratio
higher than 0.3
C peptide levels higher
than 1.2 µg/mL
CECT or MRI
Hyperattenuating
because of their rich
vascular supply
GASTRINOMA
Second most common functional pancreatic endocrine tumor
Cell of origin is not clear, because the normal adult pancreas has no gastrin-producing cells.
More common in men
Produce Zollinger-Ellison syndrome (ZES)
Hypergastrinemia , subsequent severe peptic ulceration, severe diarrhea.
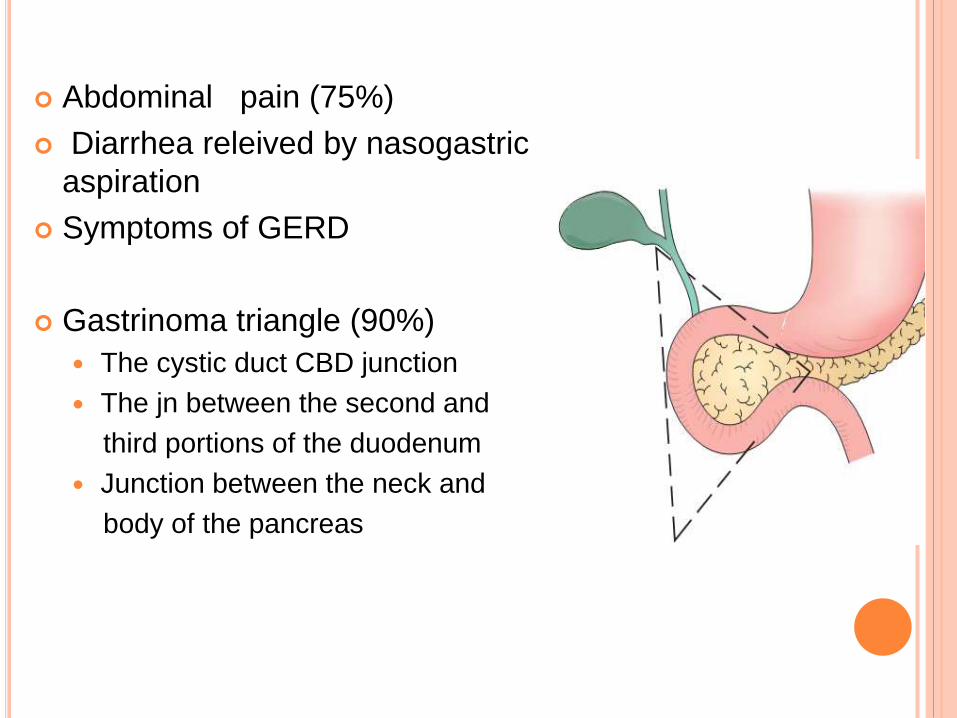
Abdominal pain (75%)
Diarrhea releived by nasogastric
aspiration
Symptoms of GERD
Gastrinoma triangle (90%)
The cystic duct CBD junction
The jn between the second and
third portions of the duodenum
Junction between the neck and
body of the pancreas

Presence of hypergastrinemia in the presence of
increased secretion of gastric acid.
An elevated serum gastrin level coupled with a pH
lower than 2 in the gastric aspirate
Fasting levels of gastrin. higher than 1000 pg/mL
(upper limit of normal of 100 pg/mL)
An increase of more than 200 pg/mL in the gastrin
value after administration of secretin
VIPOMAS
Release high levels of VIP
Verner-Morrison syndrome
Also known as WDHA syndrome (watery diarrhea,
hypokalemia, achlorhydria) or pancreatic cholera.
Solitory , larger than 3 cm ; 75% body and tail
Hypokalemia, hypomagnesemia, hypo or achlorhydria,
hypercalcemia.
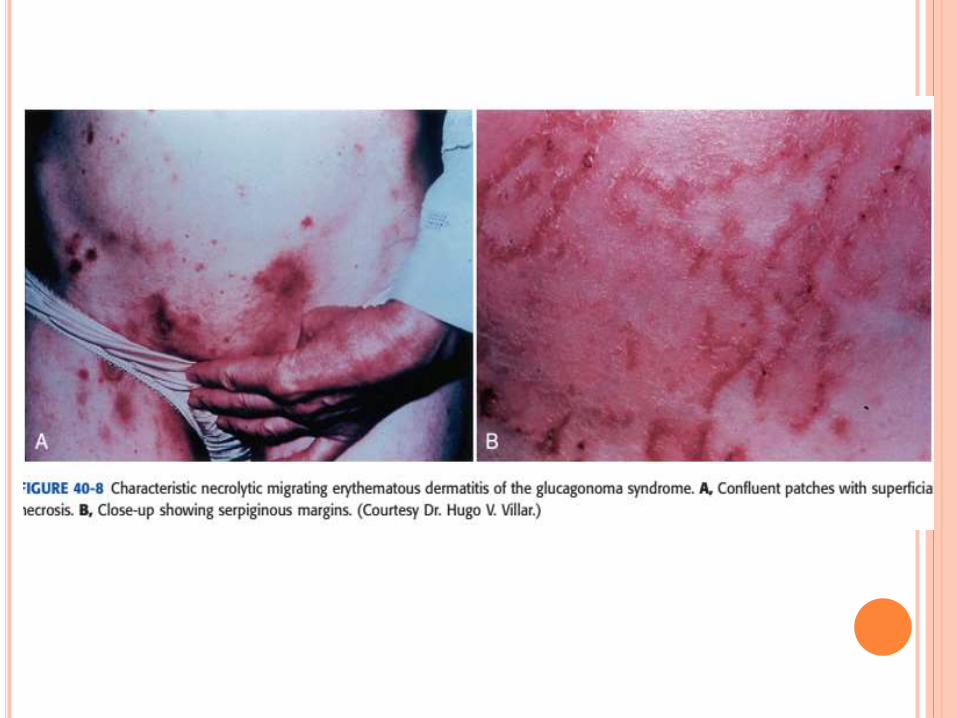
GLUCAGONOMAS
Very rare
Tend to be larger, averaging 5 to 10 cm in size
Most are malignant
Almost always arise in the pancreas and 65% to 75% are found in the body or tail.
A fasting glucagon level higher than 50 pmol/L is considered diagnostic.
The glucagonoma syndrome:
4Ds: diabetes, dermatitis, deep vein thrombosis, and depression
SOMATOSTATINOMAS
Usually solitary and 85% are larger than 2 cm.
Mostly at head of pancreas
Ninety percent are malignant
Steatorrhea , diabetes mellitus, hypochlorhydria, and gallstones
Fasting somatostatin level higher than 14 mol/liter
Associated with von Recklinghausen’s disease and pheochromocytomas
NONFUNCTIONAL NEUROENDOCRINE TUMORS
Defined as a pancreatic tumor of endocrine origin,
with no definable hormonal syndrome.
Late in seeking help hence most tumors are
malignant and metastasized at the time of
presentation
Identified by positive immunostaining for
chromogranin A or synaptophysin.
LOCALIZATION
Cross -sectional imaging with CT or MRI
first step in localization.
sensitivity is 71% to 82% and is directly related to
the size of the tumor.
vascular blush in the arterial phase is critical
lesions smaller than 1cm cannot be identified.
Endoscopic ultrasound (EUS)
Overall sensitivity of 93%
Greater sensitivity when compared with CT and MRI for
detecting tumors < 3 cm
Allows for fine-needle aspiration (FNA) of tumors

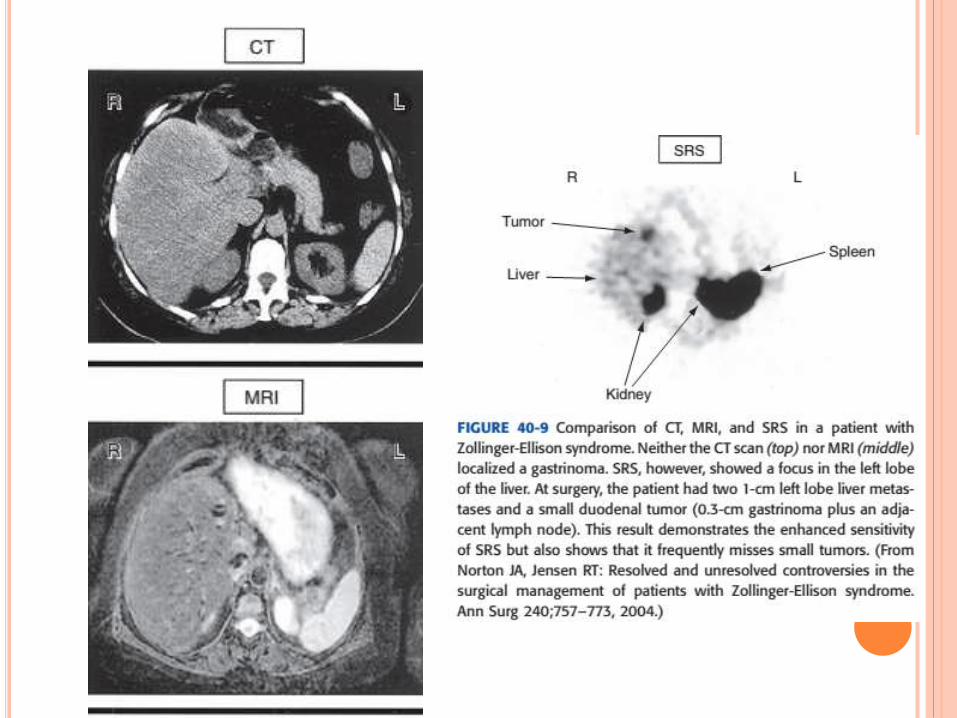
Somatostatin receptor scintigraphy (SRS)
Not useful for insulinoma
The sensitivity for SRS is over 80% for all pancreatic
endocrine tumors excluding insulinomas
It has an overall sensitivity of 80% to 100% and
specificity higher than 90% for gastrinomas.
SRS may not show the exact location of a tumor
indicates its vicinity within a few centimeters
Angiographic techniques and portal venous
sampling (sensitivity higher than 90%)
Blind exploration with intraoperative ultrasound


TREATMENT
The treatment of endocrine tumors is surgical.
(pancreatic head resection, distal pancreatic resection, or
enucleation.)
Performed by open or laparoscopic approaches
Insulinoma – Enucleation
Metastatic _ Streptozotocin, with or without 5-fluorouracil
Gastrinoma
Small well encapsulated _ Enucleation
Large unencapsulated _ Require segmental resection,
including distal pancreatectomy or
pancreaticoduodenectomy.
Radiation therapy and chemotherapy are ineffective.

VIPomas, glucagonomas, somatostatinomas, and
nonfunctional pancreatic endocrine tumors-
Resection is the treatment of choice for and
remains the only curative option.
Dacarbazine is uniquely effective against glucagonoma.

THANK YOU
![Pancreatic Neoplasms: A Diagnostic Dilemma€¦ · neoplasm and rarely contain calcification (Figure 8) [5]. Figure 8: (58 y/M) Adeno carcinoma appearing hypodense peripherally enhancing](https://img.pdfslide.us/doc/110x75/5f6d4c8a3fa4e442dc19c1cf/pancreatic-neoplasms-a-diagnostic-dilemma-neoplasm-and-rarely-contain-calcification.jpg)


![Neuroendocrine Neoplasms of the Pancreas: The Pathological …€¦ · neoplasm of the pancreas, accounting for approximately 1–2% of all pancreatic neoplasms [1, 2]. The incidence](https://img.pdfslide.us/doc/110x75/5f6d4c375d58c6724b1aebea/neuroendocrine-neoplasms-of-the-pancreas-the-pathological-neoplasm-of-the-pancreas.jpg)