Embed Size (px)
Citation preview
Seminars in Ophthalmology, 24, 149–155, 2009Copyright C© Informa Healthcare USA, Inc.ISSN: 0882-0538 print / 1744-5205 onlineDOI: 10.1080/08820530902802013
The Boston Ocular Surface Prosthesisas a Novel Drug Delivery System for
BevacizumabMira Lim
Massachusetts Eye and EarInfirmary, Boston, Massachusetts,
USA
Deborah S. Jacobs, PerryRosenthal, and Karen
G. CarrasquilloBoston Foundation for Sight, Boston,
Massachusetts, USA
ABSTRACT
Corneal neovascularization causes deterioration of visual acuity and increases surface irregularities.Various techniques have been employed to help control the progression of corneal neovasculariza-tion; bevacizumab is a medication that targets the specific pathway of corneal neovascularization.The Boston Ocular Surface Prosthesis (BOSP) is a large diameter contact lens that aids in maintainingcorneal surface integrity and may serve as a delivery system for topical bevacizumab. This paperreviews five patients who were treated with topical bevacizumab in their BOSP. All patients demon-strated improvement in their visual acuity and clinical exam. No adverse reactions were noted.
Keywords: corneal neovascularization, bevacizumab, scleral lens
INTRODUCTION
The cornea is an avascular organ. This avascularity con-tributes to its optical clarity and is maintained througha constant equilibrium among angiogenic and antian-giogenic factors.1 If the cornea undergoes inflamma-tion or infection the balance may be tipped in favor ofangiogenesis, leading to lipid deposition, scarring, de-creased vision, and an increased risk of graft failure.2,3
Various approaches towards controlling corneal neo-vascularization have been reported including: topicalcorticosteroids, cryotherapy, nonsteroidal antiinflam-matory agents, and photodynamic therapy.4,5,6 Suc-cess with these treatments varies depending on thelocation and degree of corneal neovascularization. Fur-thermore, these treatments may have deleterious sideeffects. Until recently, there have been no agents thatspecifically target the pathway of angiogenesis itself.
Address correspondence to: Mira Lim, MD, 243 CharlesStreet, Ophthalmic Education, Boston, MA 02114, USA. E-mail:mira [email protected]
Many factors contribute to the process of cornealneovascularization; among the leading angiogenicfactors are a group of vascular endothelial growthfactors (VEGF), which have been shown to beupregulated in instances of corneal inflammationand neovascularization.7,8,9,10 Bevacizumab is a re-combinant, humanized, monocolonal antibody thatbinds to and deactivates VEGF; it was FDA ap-proved in 2004 as a treatment for patients withmetastatic colorectal cancer. It has revolutionizedtreatment for wet age-related macular degeneration,when administered off-label by intra-vitreal injec-tion, and it is now being explored for other ar-eas of ocular angiogenesis.11,12,13,14,15 In particular,bevacizumab has been demonstrated to have in-hibitory effects on corneal neovascularization in thelaboratory setting when applied both topically andsubconjunctivally.16,17,18,19 Miltiades and colleaguesnoted regression mostly of smaller branches of neo-vascularization in the rabbit cornea, suggesting be-vacizumab is effective mostly on newly developingcorneal neovascularization.20
149
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Col
orad
o on
12/
09/1
1Fo
r pe
rson
al u
se o
nly.

M. Lim et al.
Subconjunctival injections of bevacizumab have re-cently been studied clinically in small case settingswith overall promising results.21,22,23 Topical adminis-tration of bevacizumab for corneal neovascularizationwas first reported in the clinical setting by DiStafenoand Kim in 2007; results showed clinical regressionof corneal neovascularization with no demonstrableside effects.24 This regression was subsequently ver-ified by additional reports from various groups.25,26
Uy et al. have demonstrated improvement in cornealneovascularization as well as patient comfort in their2 patients with Stevens Johnson syndrome.27 Kimet al. recently treated 10 eyes with topical beva-cizumab, and although initial regression of vesselswas observed, a 2-month follow-up demonstrated ad-verse effects such as epithelial breakdown and stromalthinning.28
The Boston Ocular Surface Prosthesis (BOSP) lensis a large diameter, rigid, gas permeable lens thatvaults over the corneal surface, bathing the entirecornea in oxygenated artificial tears. The BOSP iscustom-designed for each patient using CAD-CAMtechnology. It made with a high Dk fluoro-siliconeacrylate polymer, providing for oxygen transmissionto the cornea. The device was originally designed forthe treatment of ectasia and irregular astigmatismincluding cases after keratoplasty and keratorefractiveprocedures.29 This device has also been used withgreat success in treating patients with ocular surfacedisease, such as chronic ocular graft versus host disease(cGVHD), neurotrophic corneas, dry eye syndrome,and Stevens-Johnson syndrome.30 An additionalbenefit of the BOSP is its potential for drug delivery.Patients with non-healing corneal ulcers or persistentepithelial defects (PED), for example, are able tocombine topical antibiotics with saline in the BOSPreservoir, providing a continuous, dilute dose of thedrug for the duration the patient wears the lens. TheBoston Foundation for Sight sees many patients withocular surface disease and concomitant corneal neo-vascularization. Given the recently published reportsof success with corneal neovascularization and topicalbevacizumab, we decided to study the effects of topicalbevacizumab delivered via the BOSP. In this paper wereport 5 patients who were treated in this manner.
PATIENTS AND METHODS
Patients already fitted with the BOSP who had withcorneal neovascularization that might be responsive totopical therapy were identified from our clinic popu-lation at episodic visits from 2006 to the present. Afterreview of the potential risks and benefits of off-labeluse of topical bevacizumab, along with alternatives,
treatment was undertaken. Written informed consentfor the off-label use of bevacizumab was obtained. Thepatients were instructed to continue wearing the lensas usual, on a full-time daily wear basis, with nightlyremoval and disinfection. The prescribed dosage regi-men was: one drop of 1% bevacizumab, compoundedin sterile saline non-preserved, to be instilled eachmorning in the fluid reservoir of the BOSP. This reser-voir was then filled with non-preserved, buffered, ster-ile saline and the scleral lens inserted as usual. Thelens was removed, emptied, and cleaned, and the fluidreservoir was reconstituted after 6 hours with a seconddrop of bevacizumab, and the lens worn for an addi-tional 6–10 hours unless otherwise specified. All topicaland systemic medications were continued. Data col-lected included best-corrected visual acuity, slit lampexam, and slit-lamp photography at each visit. Patientswere monitored at 1 week, 1 month, 2 month, and 3months. In order to decrease the potential for systemicabsorption, punctal plugs or cautery were performedon all patients with patent punctae. After three months,dosage was tapered and discontinued except in case2. Retrospective medical record review of the patientstreated reveals that there were 2 females and 3 malesaged 26–65 years old with a range of indications forBOSP wear (Table 1).
Patient 1
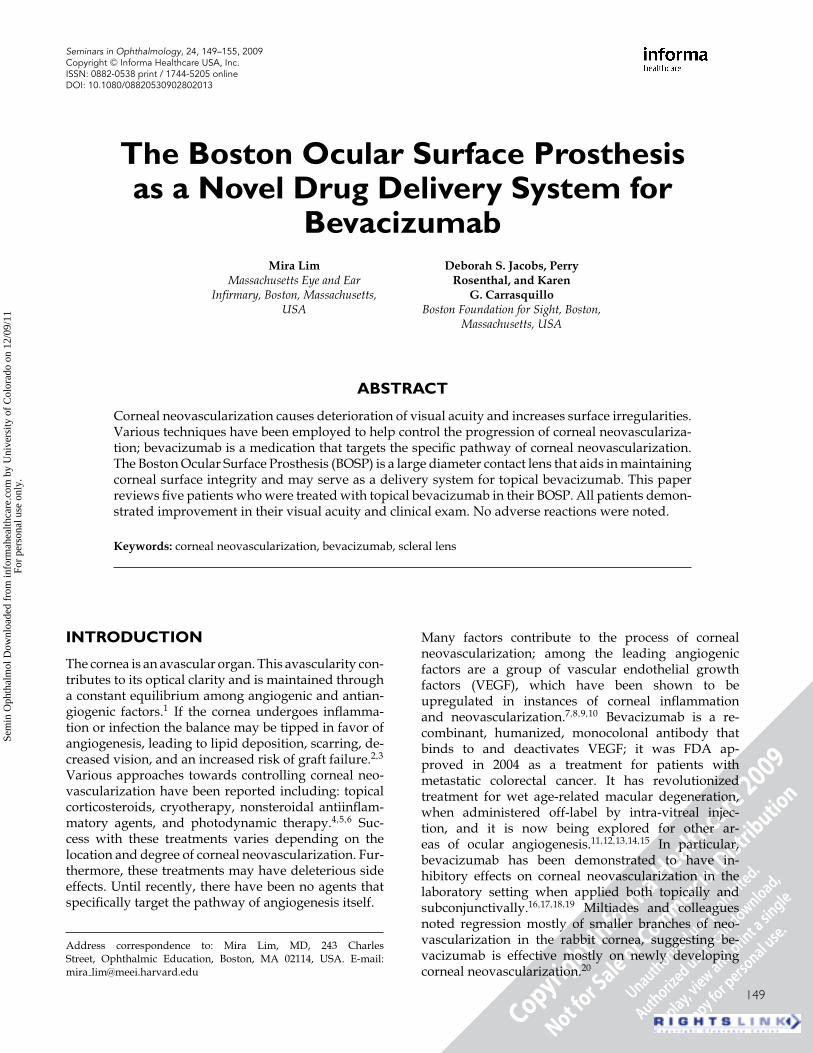
A 62-year-old man with herpes simplex virus neu-rotrophic keratitis in the left eye was initially fittedwith a BOSP for a persistent epithelial defect (PED)6 months after PK #2 in 1997. He healed with pan-nus and haze. A third penetrating keratoplasty wasundertaken in 2005 for visual rehabilitation, and theBOSP wear was resumed at 2 weeks post-operative.One year after surgery the patient had a stable ocularsurface and vision of 20/25. Eight months later, rapidprogression of inferior neovascularization was noted.Four months later, at 2 years after surgery, vascularpannus impinged on the visual axis reducing acuity toCount Fingers vision. Topical bevacizumab treatmentwas prescribed as above. One month after initiatingtreatment, marked regression of pannus and improve-ment in vision was noted, with a plateau of vision to20/40 at 3 and 10 months (Figure 1). Bevacizumab fre-quency was tapered to once daily and finally discon-tinued at 7 months. Vision remained at 20/40 whileoff bevacizumab for 17 months. There were no adverseocular or systemic effects.
Patient 2
A 30-year-old woman with Stevens-Johnson syndromeat age 12 secondary to Tegretol began wearing the
150
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Col
orad
o on
12/
09/1
1Fo
r pe
rson
al u
se o
nly.
Topical Bevacizumab in Boston Ocular Surface Prosthesis
Table 1. Patient demographics for topical bevacizumab/BOSP
Patient Age(yrs)/Gender Eye(s) Diagnosis Other topical medications
1 65/Male Left PED/HSV neurotrophic keratitis Predforte, Vigamox, Restasis2 30/Female Left Vascularized nodule/Stevens-Johnson
syndromeTimoptic, Xalatan, Alphagan, Acular,
serum drops3 35/Male Right PED/Limbal stem cell deficiency Timoptic, Lotemax4 61/Female Right PED/Sterile Melt Predforte, Artificial tears, Erythromycin
ointment5 26/Male Both Neovascular pannus and scar/Familial
dysautonomiaArtificial tears
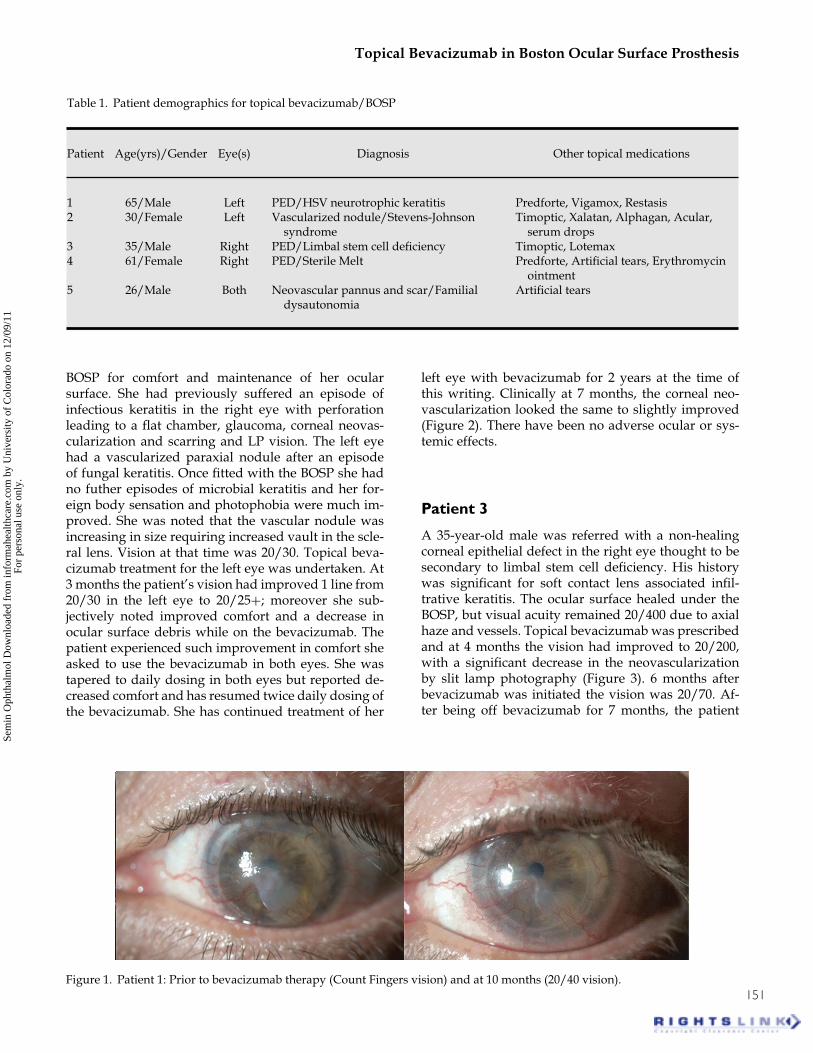
BOSP for comfort and maintenance of her ocularsurface. She had previously suffered an episode ofinfectious keratitis in the right eye with perforationleading to a flat chamber, glaucoma, corneal neovas-cularization and scarring and LP vision. The left eyehad a vascularized paraxial nodule after an episodeof fungal keratitis. Once fitted with the BOSP she hadno futher episodes of microbial keratitis and her for-eign body sensation and photophobia were much im-proved. She was noted that the vascular nodule wasincreasing in size requiring increased vault in the scle-ral lens. Vision at that time was 20/30. Topical beva-cizumab treatment for the left eye was undertaken. At3 months the patient’s vision had improved 1 line from20/30 in the left eye to 20/25+; moreover she sub-jectively noted improved comfort and a decrease inocular surface debris while on the bevacizumab. Thepatient experienced such improvement in comfort sheasked to use the bevacizumab in both eyes. She wastapered to daily dosing in both eyes but reported de-creased comfort and has resumed twice daily dosing ofthe bevacizumab. She has continued treatment of her
left eye with bevacizumab for 2 years at the time ofthis writing. Clinically at 7 months, the corneal neo-vascularization looked the same to slightly improved(Figure 2). There have been no adverse ocular or sys-temic effects.
Patient 3
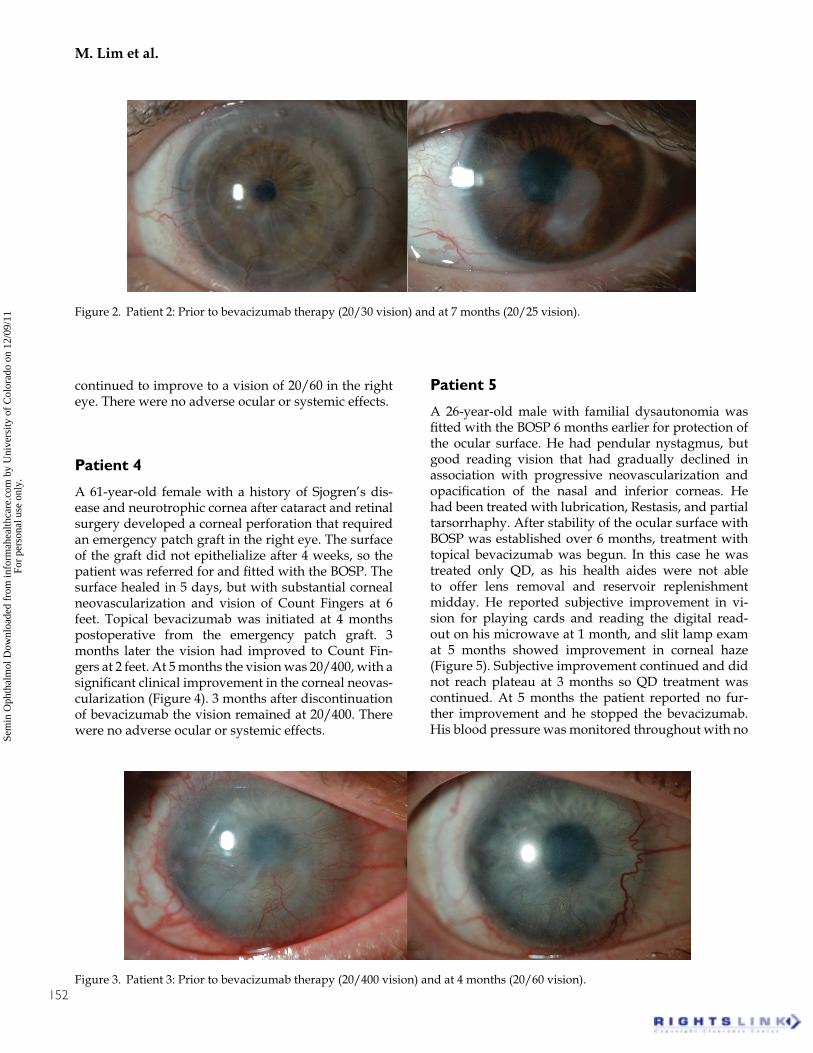
A 35-year-old male was referred with a non-healingcorneal epithelial defect in the right eye thought to besecondary to limbal stem cell deficiency. His historywas significant for soft contact lens associated infil-trative keratitis. The ocular surface healed under theBOSP, but visual acuity remained 20/400 due to axialhaze and vessels. Topical bevacizumab was prescribedand at 4 months the vision had improved to 20/200,with a significant decrease in the neovascularizationby slit lamp photography (Figure 3). 6 months afterbevacizumab was initiated the vision was 20/70. Af-ter being off bevacizumab for 7 months, the patient
Figure 1. Patient 1: Prior to bevacizumab therapy (Count Fingers vision) and at 10 months (20/40 vision).151
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Col
orad
o on
12/
09/1
1Fo
r pe
rson
al u
se o
nly.
M. Lim et al.
Figure 2. Patient 2: Prior to bevacizumab therapy (20/30 vision) and at 7 months (20/25 vision).
continued to improve to a vision of 20/60 in the righteye. There were no adverse ocular or systemic effects.
Patient 4
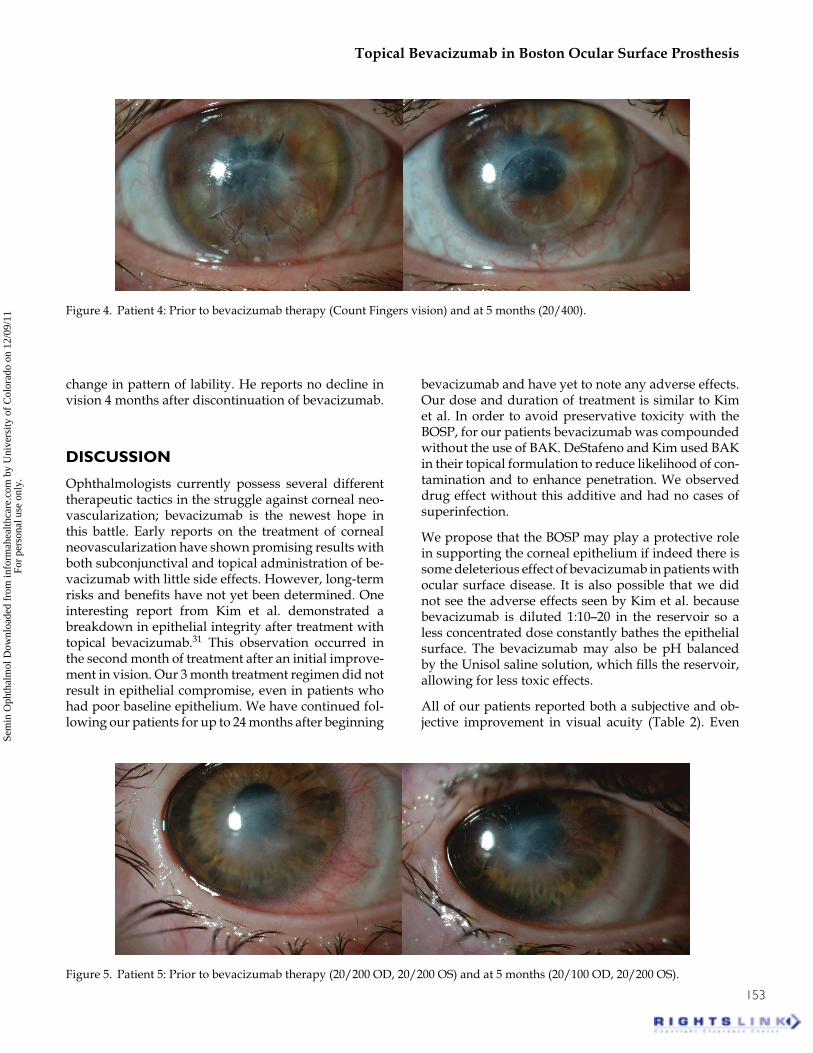
A 61-year-old female with a history of Sjogren’s dis-ease and neurotrophic cornea after cataract and retinalsurgery developed a corneal perforation that requiredan emergency patch graft in the right eye. The surfaceof the graft did not epithelialize after 4 weeks, so thepatient was referred for and fitted with the BOSP. Thesurface healed in 5 days, but with substantial cornealneovascularization and vision of Count Fingers at 6feet. Topical bevacizumab was initiated at 4 monthspostoperative from the emergency patch graft. 3months later the vision had improved to Count Fin-gers at 2 feet. At 5 months the vision was 20/400, with asignificant clinical improvement in the corneal neovas-cularization (Figure 4). 3 months after discontinuationof bevacizumab the vision remained at 20/400. Therewere no adverse ocular or systemic effects.
Patient 5
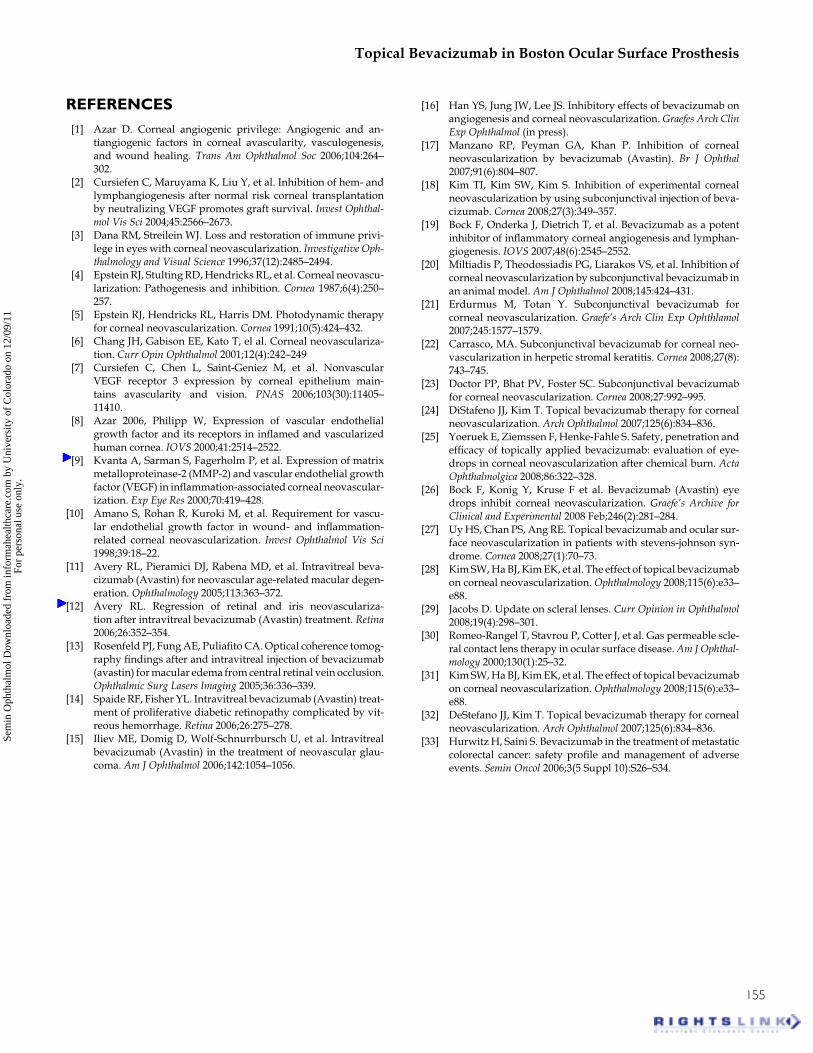
A 26-year-old male with familial dysautonomia wasfitted with the BOSP 6 months earlier for protection ofthe ocular surface. He had pendular nystagmus, butgood reading vision that had gradually declined inassociation with progressive neovascularization andopacification of the nasal and inferior corneas. Hehad been treated with lubrication, Restasis, and partialtarsorrhaphy. After stability of the ocular surface withBOSP was established over 6 months, treatment withtopical bevacizumab was begun. In this case he wastreated only QD, as his health aides were not ableto offer lens removal and reservoir replenishmentmidday. He reported subjective improvement in vi-sion for playing cards and reading the digital read-out on his microwave at 1 month, and slit lamp examat 5 months showed improvement in corneal haze(Figure 5). Subjective improvement continued and didnot reach plateau at 3 months so QD treatment wascontinued. At 5 months the patient reported no fur-ther improvement and he stopped the bevacizumab.His blood pressure was monitored throughout with no
Figure 3. Patient 3: Prior to bevacizumab therapy (20/400 vision) and at 4 months (20/60 vision).152
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Col
orad
o on
12/
09/1
1Fo
r pe
rson
al u
se o
nly.
Topical Bevacizumab in Boston Ocular Surface Prosthesis
Figure 4. Patient 4: Prior to bevacizumab therapy (Count Fingers vision) and at 5 months (20/400).
change in pattern of lability. He reports no decline invision 4 months after discontinuation of bevacizumab.
DISCUSSION
Ophthalmologists currently possess several differenttherapeutic tactics in the struggle against corneal neo-vascularization; bevacizumab is the newest hope inthis battle. Early reports on the treatment of cornealneovascularization have shown promising results withboth subconjunctival and topical administration of be-vacizumab with little side effects. However, long-termrisks and benefits have not yet been determined. Oneinteresting report from Kim et al. demonstrated abreakdown in epithelial integrity after treatment withtopical bevacizumab.31 This observation occurred inthe second month of treatment after an initial improve-ment in vision. Our 3 month treatment regimen did notresult in epithelial compromise, even in patients whohad poor baseline epithelium. We have continued fol-lowing our patients for up to 24 months after beginning
bevacizumab and have yet to note any adverse effects.Our dose and duration of treatment is similar to Kimet al. In order to avoid preservative toxicity with theBOSP, for our patients bevacizumab was compoundedwithout the use of BAK. DeStafeno and Kim used BAKin their topical formulation to reduce likelihood of con-tamination and to enhance penetration. We observeddrug effect without this additive and had no cases ofsuperinfection.
We propose that the BOSP may play a protective rolein supporting the corneal epithelium if indeed there issome deleterious effect of bevacizumab in patients withocular surface disease. It is also possible that we didnot see the adverse effects seen by Kim et al. becausebevacizumab is diluted 1:10–20 in the reservoir so aless concentrated dose constantly bathes the epithelialsurface. The bevacizumab may also be pH balancedby the Unisol saline solution, which fills the reservoir,allowing for less toxic effects.
All of our patients reported both a subjective and ob-jective improvement in visual acuity (Table 2). Even
Figure 5. Patient 5: Prior to bevacizumab therapy (20/200 OD, 20/200 OS) and at 5 months (20/100 OD, 20/200 OS).
153
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Col
orad
o on
12/
09/1
1Fo
r pe
rson
al u
se o
nly.

M. Lim et al.
Table 2. Visual acuity before and after bevacizumab treatment
Duration patient hasPatient Vision prior Last recorded vision been off Bevacizumab Comments
1 Count Fingers 20/40 1.5 years No recurrence noted2 20/30 20/25 still using in both eyes, left
eye has been treated for14 months
Attempted taper to QD, butreports improved comfort anddecreased discharge with BID
3 20/400 20/60 7 months No recurrence noted4 Count Fingers 20/400 5 months No recurrence noted5 20/200 OD, 20/200 OS 20/100 OD, 20/200 OS 4 months No recurrence noted
though our Stevens-Johnson patient did not receive asignificant improvement in vision, she opted to con-tinue treatment due to a noted improvement in ocularsurface comfort and decreased discharge. Uy and col-leagues have also reported this phenomenon in theirStevens-Johnson population. This suggests that tar-geting VEGF can have anti-inflammatory as well asanti-angiogenic properties. Miltiades et al. reported re-gression of smaller, newer branches of corneal neovas-cularization and no change with the larger vessels. Wefound similar results in our study; old corneal neovas-cularization did not seem as responsive to the treat-ment as newer vessels. These results differ from otherreports, which showed a decrease in both old and newangiogenesis.32 We specifically targeted patients whohad a recent drop in vision due to corneal neovascu-larization, so this may be why we saw such results. Inthese 5 patients who continued to wear the BOSP fortheir ocular surface disease, the effect of bevacizumabtreatment was durable with no recurrence of visu-ally significant vessels 4–24 months after cessation oftreatment.
Subconjunctival injection of bevacizumab has beenshown to be a successful delivery method againstcorneal neovascularization; however, topical ap-plication is likely to be a more appealing optionto patients. Subconjunctival delivery also carriespotential complications such as subconjunctival hem-orrhage, thinning/erosion of underlying sclera andeven intraocular penetration. If topical administrationis chosen, the BOSP may represent a novel method ofdelivering the drug in a safe manner over a prolongedperiod time. Furthermore, bevacizumab itself is a verylarge molecule; this may prevent its full absorptionif only topical administration is used. The BOSP, bymaintaining a fluid volume against the cornea, mayimprove the bio-availability of the large bevacizumabmolecule. The BOSP also provides the additional
benefit of epithelial protection in a likely alreadytenuous environment. Regression of corneal neovas-cularization can improve visual quality for patientswho are not amenable to surgical therapy, for examplethose in whom grafts are likely to fail or maintenanceof the graft is too burdensome. It may also improvethe success of grafts if future surgery is undertaken.
Systemic bevacizumab has been shown to cause hy-pertension and an increased rate of thrombosis inpatients with metastatic colorectal carcinoma.33 For-tunately, systemic side effects in our study and inother studies were not noted. Even our patient withfamilial dysutonomia, whose volatile blood pressurewas measured regularly, did not demonstrate anysystemic adverse effect. Regardless, punctal plugs orcautery should be used to decrease chance of sys-temic absorption when bevacizumab is administeredtopically.
Controlled studies and long-term follow-up are re-quired to determine the optimal dose and duration oftopical bevacizumab therapy for corneal neovascular-ization. The role of the BOSP in enhancing deliveryand/or protecting the corneal surface warrants furtherinvestigation. The clinical impact in these first five pa-tients shows great promise.
Declaration of interest
The authors have no proprietary or financial interestin the Boston Ocular Surface Prosthesis. Drs. Jacobs,Rosenthal, and Carrasquillo are salaried, full-time em-ployees of the Boston Foundation for Sight, a 501(c)3non-profit. Their salaries are fixed, with no volume orproductivity incentive, and are determined by the com-pensation committee of the Foundation’s independentboard of directors.
154
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Col
orad
o on
12/
09/1
1Fo
r pe
rson
al u
se o
nly.
Topical Bevacizumab in Boston Ocular Surface Prosthesis
REFERENCES[1] Azar D. Corneal angiogenic privilege: Angiogenic and an-
tiangiogenic factors in corneal avascularity, vasculogenesis,and wound healing. Trans Am Ophthalmol Soc 2006;104:264–302.
[2] Cursiefen C, Maruyama K, Liu Y, et al. Inhibition of hem- andlymphangiogenesis after normal risk corneal transplantationby neutralizing VEGF promotes graft survival. Invest Ophthal-mol Vis Sci 2004;45:2566–2673.
[3] Dana RM, Streilein WJ. Loss and restoration of immune privi-lege in eyes with corneal neovascularization. Investigative Oph-thalmology and Visual Science 1996;37(12):2485–2494.
[4] Epstein RJ, Stulting RD, Hendricks RL, et al. Corneal neovascu-larization: Pathogenesis and inhibition. Cornea 1987;6(4):250–257.
[5] Epstein RJ, Hendricks RL, Harris DM. Photodynamic therapyfor corneal neovascularization. Cornea 1991;10(5):424–432.
[6] Chang JH, Gabison EE, Kato T, el al. Corneal neovasculariza-tion. Curr Opin Ophthalmol 2001;12(4):242–249
[7] Cursiefen C, Chen L, Saint-Geniez M, et al. NonvascularVEGF receptor 3 expression by corneal epithelium main-tains avascularity and vision. PNAS 2006;103(30):11405–11410.
[8] Azar 2006, Philipp W, Expression of vascular endothelialgrowth factor and its receptors in inflamed and vascularizedhuman cornea. IOVS 2000;41:2514–2522.
[9] Kvanta A, Sarman S, Fagerholm P, et al. Expression of matrixmetalloproteinase-2 (MMP-2) and vascular endothelial growthfactor (VEGF) in inflammation-associated corneal neovascular-ization. Exp Eye Res 2000;70:419–428.
[10] Amano S, Rohan R, Kuroki M, et al. Requirement for vascu-lar endothelial growth factor in wound- and inflammation-related corneal neovascularization. Invest Ophthalmol Vis Sci1998;39:18–22.
[11] Avery RL, Pieramici DJ, Rabena MD, et al. Intravitreal beva-cizumab (Avastin) for neovascular age-related macular degen-eration. Ophthalmology 2005;113:363–372.
[12] Avery RL. Regression of retinal and iris neovasculariza-tion after intravitreal bevacizumab (Avastin) treatment. Retina2006;26:352–354.
[13] Rosenfeld PJ, Fung AE, Puliafito CA. Optical coherence tomog-raphy findings after and intravitreal injection of bevacizumab(avastin) for macular edema from central retinal vein occlusion.Ophthalmic Surg Lasers Imaging 2005;36:336–339.
[14] Spaide RF, Fisher YL. Intravitreal bevacizumab (Avastin) treat-ment of proliferative diabetic retinopathy complicated by vit-reous hemorrhage. Retina 2006;26:275–278.
[15] Iliev ME, Domig D, Wolf-Schnurrbursch U, et al. Intravitrealbevacizumab (Avastin) in the treatment of neovascular glau-coma. Am J Ophthalmol 2006;142:1054–1056.
[16] Han YS, Jung JW, Lee JS. Inhibitory effects of bevacizumab onangiogenesis and corneal neovascularization. Graefes Arch ClinExp Ophthalmol (in press).
[17] Manzano RP, Peyman GA, Khan P. Inhibition of cornealneovascularization by bevacizumab (Avastin). Br J Ophthal2007;91(6):804–807.
[18] Kim TI, Kim SW, Kim S. Inhibition of experimental cornealneovascularization by using subconjunctival injection of beva-cizumab. Cornea 2008;27(3):349–357.
[19] Bock F, Onderka J, Dietrich T, et al. Bevacizumab as a potentinhibitor of inflammatory corneal angiogenesis and lymphan-giogenesis. IOVS 2007;48(6):2545–2552.
[20] Miltiadis P, Theodossiadis PG, Liarakos VS, et al. Inhibition ofcorneal neovascularization by subconjunctival bevacizumab inan animal model. Am J Ophthalmol 2008;145:424–431.
[21] Erdurmus M, Totan Y. Subconjunctival bevacizumab forcorneal neovascularization. Graefe’s Arch Clin Exp Ophthlamol2007;245:1577–1579.
[22] Carrasco, MA. Subconjunctival bevacizumab for corneal neo-vascularization in herpetic stromal keratitis. Cornea 2008;27(8):743–745.
[23] Doctor PP, Bhat PV, Foster SC. Subconjunctival bevacizumabfor corneal neovascularization. Cornea 2008;27:992–995.
[24] DiStafeno JJ, Kim T. Topical bevacizumab therapy for cornealneovascularization. Arch Ophthalmol 2007;125(6):834–836.
[25] Yoeruek E, Ziemssen F, Henke-Fahle S. Safety, penetration andefficacy of topically applied bevacizumab: evaluation of eye-drops in corneal neovascularization after chemical burn. ActaOphthalmolgica 2008;86:322–328.
[26] Bock F, Konig Y, Kruse F et al. Bevacizumab (Avastin) eyedrops inhibit corneal neovascularization. Graefe’s Archive forClinical and Experimental 2008 Feb;246(2):281–284.
[27] Uy HS, Chan PS, Ang RE. Topical bevacizumab and ocular sur-face neovascularization in patients with stevens-johnson syn-drome. Cornea 2008;27(1):70–73.
[28] Kim SW, Ha BJ, Kim EK, et al. The effect of topical bevacizumabon corneal neovascularization. Ophthalmology 2008;115(6):e33–e88.
[29] Jacobs D. Update on scleral lenses. Curr Opinion in Ophthalmol2008;19(4):298–301.
[30] Romeo-Rangel T, Stavrou P, Cotter J, et al. Gas permeable scle-ral contact lens therapy in ocular surface disease. Am J Ophthal-mology 2000;130(1):25–32.
[31] Kim SW, Ha BJ, Kim EK, et al. The effect of topical bevacizumabon corneal neovascularization. Ophthalmology 2008;115(6):e33–e88.
[32] DeStefano JJ, Kim T. Topical bevacizumab therapy for cornealneovascularization. Arch Ophthalmol 2007;125(6):834–836.
[33] Hurwitz H, Saini S. Bevacizumab in the treatment of metastaticcolorectal cancer: safety profile and management of adverseevents. Semin Oncol 2006;3(5 Suppl 10):S26–S34.
155
Sem
in O
phth
alm
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Col
orad
o on
12/
09/1
1Fo
r pe
rson
al u
se o
nly.