Embed Size (px)
Citation preview

ORIGINAL ARTICLE
The antibiofilm effects of ByotrolTM G32N. Govindji1, P. Wills2, M. Upton1, N. Tirelli3, S. Yeates2 and M. Webb1
1 School of Medicine, University of Manchester, Manchester, UK
2 Organic Materials Innovation Centre, School of Chemistry University of Manchester, Manchester, UK
3 School of Materials and School of Medicine, University of Manchester, Manchester, UK
Keywords
antimicrobials, biofilms, infection.
Correspondence
Michelle Webb, School of Medicine,
University of Manchester, Oxford Road,
Manchester, M13 9PL, UK.
E-mail: [email protected]
2013/1896: received 19 October 2012,
revised 17 January 2013 and accepted 20
January 2013
doi:10.1111/jam.12162
Abstract
Aim: The purpose of this study was to evaluate a commercial antimicrobial
formulation, ByotrolTM G32, as a potential coating for impeding biofilm
formation on medical devices such as urinary catheters.
Methods and Results: The antimicrobial activity of ByotrolTM G32 and its
individual constituents has been tested on planktonic and biofilm cultures of
uropathogenic bacteria. The ByotrolTM G32 formulation was superior with
MICs ranging from 3 lg ml�1 to 15 lg ml�1 for planktonic cultures and 3–20lg ml�1 for biofilms. Furthermore, ByotrolTM G32 was able to remove
established biofilms and act as an antibiofilm surface coating.
Conclusions: ByotrolTM G32 displays impressive antimicrobial activity both in
suspension and as a coating. Pretreating medical devices with ByotrolTM G32
may significantly impede biofilm formation and prolong the lifetime of the
device.
Significance and Impact of the study: Medical devices are indispensable in
health care. They are, however, a predisposing factor in infection. This research
has demonstrated that ByotrolTM G32 reduces bacterial growth and subsequent
biofilm formation. Application of ByotrolTM G32 as a medical device coating
could have a significant impact on the costs associated with device replacement
and patient morbidity and mortality.
Introduction
It is estimated that over half of all nosocomial infections
are associated with medical devices, such as artificial
heart valves, prosthetic devices, surgically implanted
devices, contact lenses, wound drainage tubes, dressings,
intrauterine contraception devices, sutures, intravenous
catheters and urinary catheters (Smith et al. 1991; Coster-
ton et al. 1999; Richards et al. 1999). Systemic and
chronic infections are a result of biofilm formation on
the surface of medical devices (Costerton et al. 1999).
Biofilms are organized multicellular communities of
bacteria attached to a surface and embedded in a protec-
tive polymer matrix. The biofilm phenotype is a ubiqui-
tous characteristic of bacteria that constitutes a protected
growth mode to facilitate survival in hostile environments
(Costerton et al. 1987, 1995, 1999). It offers increased
resistance to host defences and antimicrobials, and
consequently, biofilms are notoriously difficult to treat
and commonly manifest as chronic or recurrent infec-
tions (Patel 2005; Vuong et al. 2005; Anderson and
O’Toole 2008). The most effective method to impede
biofilm development is to avoid or reduce the initial
adhesion of bacteria to the surface. The nonspecific
attachment of bacteria to any surface is a key determi-
nant in subsequent biofilm formation; therefore, many
approaches have been adopted to prevent bacterial
attachment to surfaces of medical devices (Banerjee et al.
2011; Knetsch and Koole 2011). Currently, the most
widely used antimicrobial biomaterials are those that have
silver-modified coatings (Boswald et al. 1999; Davenport
and Keeley 2005). These are now routinely used in
wound management (Davenport and Keeley 2005; Silver
et al. 2006; Atiyeh et al. 2007), and while they can reduce
the risk of infection, they introduce a host of problems.
For example, the uptake of silver ions by bacterial cells
Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology 1285
Journal of Applied Microbiology ISSN 1364-5072

has resulted in the emergence of silver-resistant strains
(Silver 2003; Percival et al. 2005; Silver et al. 2006),
indeed silver-resistant Pseudomonas aeruginosa has been
isolated from burn patients who have been treated with
silver-coated wound dressings (Modak and Fox 1981).
Cationic compounds represent a suitable alternative as
they define a structurally diverse class of antimicrobials
(Banerjee et al. 2011). Such chemical diversity leads to a
broad spectrum of activity and different modes of action.
Furthermore, despite over a century of use, only trace
levels of cross-resistance have been observed in the clini-
cal environment (Gilbert and Moore 2005; Jaglic and
Cervinkova 2012). Antibiofilm coatings containing novel
cationic compounds could, therefore, have a significant
impact on the clinical setting.
ByotrolTM G32 is a successful commercial antimicrobial
hygiene product that is based on a novel proprietary mix-
ture of poly(hexamethylene biguanide) chloride (PHMB);
didecyldimethylammonium chloride (DDQ) and alkyl
(C12, 70%; C14, 30%) dimethyl benzyl ammonium chlo-
ride (BAC). In this study, we evaluated the in vitro
efficacy of ByotrolTM G32 for impeding biofilm formation.
Methods
Bacterial strains, media and growth conditions
The well-characterized laboratory strain Escherichia coli
K12 (XL1 blue phage) and clinical isolates of E. coli,
Klebsiella pneumoniae and Ps. aeruginosa obtained from
urinary tract infections and characterized by Vitek� 2
(BioM�erieux, Inc., Basingstoke, UK) were used in this
study. The staff at the Central Manchester Foundation
Trust, Clinical Sciences Building 2, Manchester, UK,
kindly provided the clinical isolates used in this study.
Stocks were stored at �80°C in 80% glycerol. Stock bac-
teria were cultured for 18 h on Luria–Bertani (LB) agar
plates every two weeks. Plates were stored at 4°C. Over-night cultures were prepared by inoculating LB broth
with several colonies from the working culture plates and
incubating for 18 h with shaking at 200 rev min�1. The
inoculum was standardized to 1 9 108 CFU ml�1 using
the Miles and Misra method for the determination of via-
ble cell counts. All cultures were incubated in an aerobic
atmosphere at 37°C.
ByotrolTM G32
The composition of ByotrolTM G32 (ByotrolTM Technology
Ltd., Daresbury, UK) is PHMB (poly(hexamethylene
biguanide) chloride); DDQ (didecyldimethylammonium
chloride) and BAC (alkyl (C12, 70%; C14, 30%) dimethyl
benzyl ammonium chloride).
Poly(hexamethylene biguanide) was obtained from
Arch Chemicals (Tradename-Vantocil TG) as a 20 wt%
solution in water. DDQ was obtained from Lonza
(Tradename - Lonza Bardac 2240) and received as a
40 wt% solution in water. BAC was obtained from Thor
(Tradename – Acticide BAC 50 mol l�1) and received as
a 50 wt% solution in water.
Determination of the minimum inhibitory concentration
The minimum inhibitory concentration (MIC) of
ByotrolTM G32 and its constituents was determined by
incubating increasing concentrations of each with 100 llof a 1 : 50 dilution of overnight cultures prepared in LB
in 96-well flat-bottomed nontissue culture–treated poly-
styrene microtitre plates (Greiner Bio-one Ltd., Glouces-
tershire, UK). Eight technical replicates were prepared on
each plate for each concentration of antimicrobial tested.
The microtitre plates were incubated under aerobic, static
conditions for 18 h at 37°C.Positive growth controls were prepared by inoculating
eight wells with 100 ll of 1 : 50 dilutions of bacteria and
100 ll sterile distilled water in which the antimicrobial
was prepared. Negative controls were prepared by dis-
pensing 100 ll LB broth and 100 ll sterile distilled water
into a further 8 wells. The microtitre plates were incu-
bated under aerobic, static conditions for 18 h at 37°C.After the incubation period, the optical density at
595 nm (OD595) of planktonic growth was measured to
quantify the MIC using a spectrophotometer (BMG Lab-
tech FLUOstar OPTIMA). The average optical density
(OD) from the eight negative control wells was sub-
tracted from the average OD from the eight technical
replicates of each concentration in the test wells. The
MIC is determined as the lowest concentration of antimi-
crobial that completely inhibits visual bacterial growth, or
an OD595 < 0�05.
Microtitre plate biofilm formation assay
After determining the MIC, the microtitre plate biofilm
formation assay was used according to the method by
Christensen et al. (1985). Briefly, excess media and any
planktonic cells were decanted from the microtitre plate,
and each well was washed with 200 ll sterile phosphate-
buffered saline (PBS) (Sigma-Aldrich Company Ltd.). The
plate was left in an inverted position to air dry overnight at
room temperature. Each well was stained with 150 ll 0�4%(w/v) crystal violet (Sigma-Aldrich Company Ltd.) at room
temperature for 10 min and washed with running tap
water until the excess stain was removed and the running
water appeared colourless. The plate was inverted and left
to dry overnight at room temperature. The biofilm density
1286 Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology
Preventing biofilm-related infections N. Govindji et al.

was quantified by solubilizing the ammonium crystal violet
stain with 200 ll 99�5% ethanol (Fisher Scientific UK Ltd.,
Loughborough, UK) and measuring the OD595 of solubi-
lized crystal violet in each well using a spectrophotometer
plate reader (BMG Labtech FLUOstar OPTIMA). The aver-
age OD from the eight negative control wells was sub-
tracted from the average OD from the eight technical
replicates of each concentration in the test wells.
Bright field microscopy
Eight-well glass chamber slides (Lab-TekTM Chamber
slideTM; Nunc, Fisher Scientific, Loughborough, UK) were
used to analyse biofilms by bright field microscopy. Each
slide had six increasing concentrations of antimicrobial
agent, one in each well. The concentration of antimicrobial
agent in each well was prepared by dispensing 150 ll of theantimicrobial agent and 150 ll of a 1 : 50 dilution of inoc-
ulum prepared from an overnight culture as described pre-
viously. The remaining two wells contained a positive
growth control prepared with 150 ll inoculum and 150 llwater, and a negative control with 150 ll media and 150 llwater. Slides were prepared in triplicate. After incubation,
the slides were washed with 1 ml PBS and immediately
stained with 0�4% crystal violet for 10 min. Excess stain
was washed with running water and left to dry in an
inverted position overnight. The chambers were removed
and microscopic images were collected on an Olympus
BX51 upright microscope using a 1009/1�30 UPlanFLN
objective. Images were captured using a CoolSnap HQ
camera (Photometrics) through MetaVue Software
(Molecular Devices). Images were then processed and anal-
ysed using ImageJ (http://rsb.info.nih.gov/ij).
Minimum Biofilm Eradication Concentration assay
This assay determines the effect of ByotrolTM G32 on
biofilm cells. 200 ll of a 1 : 100 dilution of an overnight
culture was dispensed into wells of a microtitre plate.
The Minimum Biofilm Eradication Concentration
(MBEC) assay is a modification of the method described
by Ceri et al. (1999). A lid with protruding pegs (trans-
ferable solid-phase screening system, Nunc) was placed
into the inoculated wells and incubated under static con-
ditions for 18 h. The lid carrying pegs were transferred to
a microtitre plate containing 200 ll sterile PBS, shaken
to remove any nonadhered bacterial cells and then placed
in a microtitre plate containing a concentration range of
each antimicrobial, which was prepared in the same man-
ner as described for the MIC assay and microtitre plate
biofilm production assay. The plates were incubated
under static conditions for 18 h. The pegs were then
placed in 200 ll PBS, shaken briefly and immediately
placed in 200 ll fresh sterile media and incubated for a
further 18 h to allow for regrowth of viable bacterial cells
on the pegs. After incubation, the OD595 of the plates
containing any planktonic growth was read. The pegs
were washed in 200 ll PBS and allowed to dry overnight
at room temperature before placing the pegs in 200 ll0�4% crystal violet for 15 min. The pegs were washed in
running water and left to air dry overnight at room tem-
perature. The biofilm density was quantified by solubiliz-
ing the ammonium crystal violet stain with 200 ll 99�5%ethanol and measuring the OD595 of solubilized crystal
violet using a spectrophotometer plate reader. The aver-
age OD from the eight negative control wells was sub-
tracted from the average OD from the eight technical
replicates of each concentration in the test wells.
Effect of pretreatment of glass chamber slides on biofilm
formation
The wells of a glass chamber slide were pretreated by
incubating overnight at 37°C with a 5 lg ml�1 and
1 mg ml�1 solution of ByotrolTM G32. After incubation,
excess ByotrolTM G32 was decanted and slides were
re-incubated for a further 18 h at 37°C to allow for evap-
oration of water. A 1 : 100 dilution of overnight cultures
of bacteria was prepared in LB broth, 100 ll of which
was added to pretreated slides and incubated for 8 h at
37°C. A minimum of four biological replicates were pre-
pared for each concentration. After the incubation per-
iod, the slides were washed with 1 ml PBS, stained with
250 ll crystal violet and solubilized with 300 ll ethanol.The OD595 measurements were determined as for the
microtitre plate biofilm formation assay.
Atomic force microscopy
Wells of a glass chamber slide were precoated with 300 llof a 1 mg ml�1 solution of ByotrolTM G32 overnight at
37°C. After incubation, excess ByotrolTM was decanted
and the slides were re-incubated for a further 18 h at
37°C to allow for evaporation of water.
Topographies were recorded using atomic force
microscopy (AFM) (PSIA Inc, XE100, Surrey, UK) in
noncontact mode. A commercial silicon cantilever (PSIA
Inc, 910M-NSC15) with a nominal spring constant of
about 40 N/m was used.
The glass slides with precoated ByotrolTM G32 were
secured to a metal disc using double sided tape and
installed on the AFM scanner. An area of 20 lm2 was
scanned. A scratch was made across the bottom of the
glass chamber using a 0�8 9 40 mm needle. The resulting
topography image of this scratch gives an indication of
the film thickness on the precoated glass slides.
Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology 1287
N. Govindji et al. Preventing biofilm-related infections

Results
ByotrolTM G32 as an antimicrobial
The antimicrobial activity of the ByotrolTM G32 formula-
tion and its individual constituents was tested on a
planktonic laboratory E. coli K12 strain and clinical
strains of E. coli, Kl. pneumoniae and Ps. aeruginosa, all
isolated from patients with urinary tract infections. For
the ByotrolTM G32 formulation, antimicrobial activity was
observed against all isolates (Fig. 1) with MICs ranging
from 3 lg ml�1 for the two E. coli isolates to 15 lg ml�1
for Kl. pneumoniae and Ps. aeruginosa. A comparison of
the MICs for the individual constituents of ByotrolTM
G32, displayed in Table 1, reveals that the G32 formula-
tion outperforms the individual constituents.
Next, the amount of biofilm produced by the remain-
ing viable planktonic cells after 18 h was determined by
crystal violet staining of the adhered bacterial cells.
Figure 2 illustrates that low concentrations of ByotrolTM
G32 (3–20 lg ml�1) reduce the biofilm development of
all isolates. To confirm these results, biofilms stained with
crystal violet were visualized by bright field microscopy
(Fig. 3). In this instance, bright field microscopy of
Table 1 The minimum inhibitory concentrations of ByotrolTM G32
and its individual components; poly(hexamethylene biguanide)
chloride (PHMB), didecyldimethylammonium chloride (DDQ) and
benzyl ammonium chloride (BAC) against Escherichia coli K12 and
clinical isolates of E. coli, Klebsiella pneumoniae and Pseudomonas
aeruginosa grown for 18 h
Minimum inhibitory concentration
(lg ml�1)
ByotrolTM G32 PHMB DDQ BAC
E. coli K12 3 15 20 60
E. coli clinical isolate 3 60 30 100
Kl. pneumoniae clinical isolate 15 100 100 200
Ps. aeruginosa clinical isolate 15 200 100 400
All data represent the mean of over 24 replicates, involving three
biological replicates for each strain.
1·00·80·6
0·20·0
0·4
1·5
1·0
0·5
0·0
1·00·80·6
0·20·0
0·4
0·50·4
0·10·0
0·20·3
Control 0·3 0·6 3 5 13 20 30
Control 0·3 0·6 3 5 13 20 30
Control 0·3 0·6 3 5 13 20 30
Control 0·3 0·6 3 5 13 20 30
ByotrolTM concentration (µg ml–1)
OD
595
nm
E. coli K12
E. coli
K. pneumoniae
P. aeruginosa
Figure 1 Minimum inhibitory concentrations determining the activity
of increasing concentrations of ByotrolTM G32 on planktonic bacterial
cells grown under static conditions for 18 h. All data represent the
mean of over 24 replicates, involving three biological replicates for
each strain. Error bars indicate the standard error of the mean.
0·6
0·4
0·2
0·0
2·0
1·5
1·0
0·5
0·0
0·3
0·1
0·0
0·2
0·4
0·3
0·1
0·0
0·2
Control 0·3 0·6 3 5 15 20 30
Control 0·3 0·6 3 5 15 20 30
Control 0·3 0·6 3 5 15 20 30
ByotrolTM concentration (µg ml–1)
Control 0·3 0·6 3 5 15 20 30
OD
595
nm
E. coli K12
E. coli
K. pneumoniae
P. aeruginosa
Figure 2 Effect of ByotrolTM G32 on biofilm development under static
conditions. Increasing concentrations of ByotrolTM G32 were incubated
with each bacterial strain at 37°C for 18 h, and the extent of biofilm
formation was determined by crystal violet staining. All data represent
the mean of over 24 replicates, involving three biological replicates
for each strain. Error bars indicate the standard error of the mean.
1288 Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology
Preventing biofilm-related infections N. Govindji et al.

bacterial cells stained with crystal violet was preferable to
fluorescence microscopy, as it avoided nonspecific bind-
ing of dyes to ByotrolTM G32, which we observed for the
standard fluorescent biofilm labelling dye FilmTracerTM
SYPRO� Ruby biofilm matrix stain (InvitrogenTM, Life
Technologies Ltd., Paisley, UK), and for the Live/Dead�
stain (InvitrogenTM). Figure 3 demonstrates that the num-
ber of adherent bacteria is substantially reduced in rela-
tion to the growth control, at concentrations of ByotrolTM
G32 as low as 3 lg ml�1, confirming the ability of Byo-
trolTM G32 to impede biofilm development. Consistent
with previous results, reducing Ps. aeruginosa biofilm
development required higher concentrations of ByotrolTM
G32. Furthermore, comparison to the minimum biofilm
inhibitory concentrations for the individual constituents
displayed in Table 2 reveals that again the G32 formula-
tion outperforms any of the individual constituents in its
ability to reduce the degree of bacterial growth.
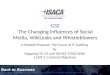
The impact that ByotrolTM G32 had on established bio-
films was also determined by performing the MBEC
assay. The results, which are presented in Fig. 4, show
that ByotrolTM G32 was effective against biofilms of E. coli
and Kl. pneumoniae; >50% of the biofilm was eradicated
at concentrations of 60 lg ml�1. Ps. aeruginosa was more
difficult to eradicate requiring 400 lg ml�1 to reduce the
biofilm mass by 50%.
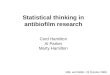
ByotrolTM G32 as a biofilm reducing device coating
ByotrolTM G32 was used to coat glass surfaces by incubat-
ing a solution at 37°C and then drying. Atomic force
microscopy was used to verify the extent of coating and
access surface morphology. Figure 5(a) shows the atomic
force micrographs of a glass surface coated with 5 lg ml�1
and 1 mg ml�1 ByotrolTM G32. A scratch drawn along the
surface allowed the depth of the coatings to be measured
(Fig. 5b). At a concentration of 5 lg ml�1, the coating
depth was measured as 20 nm. At a concentration of
1 mg ml�1, the surface is evenly coated and the depth of
the coating was measured as 60 nm (Fig. 5b). Biofilm
development on the coated surfaces was determined by
crystal violet staining of a biofilm grown for 8 h. On the
surface coated with 1 mg ml�1 ByotrolTM G32, no biofilm
development was observed for the two E. coli strains and
Control
E. c
oli
E. c
oli
K. p
neum
onia
eP.
aer
ugin
osa
0·3 µg ml–1 0·6 µg ml–1 13 µg ml–13 µg ml–1 20 µg ml–16 µg ml–1
ByotrolTM concentration (µg ml–1)
Figure 3 Bright field microscopy showing the effects of increasing concentrations of ByotrolTM G32 on biofilm formation. Bright field images
(1009 magnification) of Escherichia coli K12 and the clinical isolates of E. coli, Klebsiella pneumoniae and Pseudomonas aeruginosa grown for
18 h in the presence of increasing concentrations of ByotrolTM G32 and stained with crystal violet.
Table 2 The minimum biofilm inhibitory concentrations of ByotrolTM
G32 and its individual components; poly(hexamethylene biguanide)
chloride (PHMB), didecyldimethylammonium chloride (DDQ) and
benzyl ammonium chloride (BAC) against Escherichia coli K12 and
clinical isolates of E. coli, Klebsiella pneumoniae and Pseudomonas
aeruginosa grown for 18 h
Minimum biofilm inhibitory
concentration (lg ml�1)
ByotrolTM G32 PHMB DDQ BAC
E. coli K12 3 20 20 60
E. coli clinical isolate 5 60 30 100
Kl. pneumoniae clinical isolate 15 100 30 60
Ps. aeruginosa clinical isolate 20 400 100 400
All data represent the mean of over 24 replicates, involving three
biological replicates for each strain.
Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology 1289
N. Govindji et al. Preventing biofilm-related infections

Kl. pneumoniae, and Ps. aeruginosa biofilm development
was impeded by ~60%.
Discussion
Healthcare professionals, to support the care and treat-
ment of patients, increasingly use medical devices such as
catheters, shunts, orthopaedic implants and wound dress-
ings. While medical devices offer regained structure and
function to the body, they are a persistent source of
infection (Darouiche 2001; Van and Michiels 2005). Such
infections not only present profound economic burdens
for society but infections associated with the insertion of
a medical device lead to significant levels of morbidity
and are sometimes fatal (Polonio et al. 2001). Bacterial
communities known as biofilms play a central role in
device-associated infections (Costerton 2007; Hatt and
Rather 2008). Preventing biofilm formation is key to pro-
longing the lifetime of any medical device and reducing
infection-related complications.
The ability of many conventional antimicrobials to
inhibit biofilm formation has been assessed and some
success has been found with the use of heavy metals, par-
ticularly silver. Hydrogel-coated latex catheters impreg-
nated with silver on both the outer surface and lumen of
the catheter have shown some effectiveness, however,
only in the short-term (Bologna et al. 1999; Verleyen
et al. 1999), possibly because the main challenge of the
urinary catheter is the hugely mixed population of resis-
tant micro-organisms that form a biofilm and cause
infection, including bacteria, which display heavy metal
resistance (Woods et al. 2009). Therefore, silver may not
be an ideal inhibitor in the long term, as it may select for
organisms with silver resistance. Furthermore, there is
conflicting evidence in the literature as to the efficacy of
silver in the clinical environment (Johnson et al. 2006).
Here, we have studied the antimicrobial and biofilm
inhibitory properties of a proprietary hygiene product,
ByotrolTM G32, which is a commercial formulation based
upon a mixture of poly(hexylmethylbiguanide) chloride
(PHMB), didecyldimethylammonium chloride (DDQ)
and dimethyl benzyl ammonium chloride (BAC). PHMB
is a polymeric cationic antimicrobial agent, which for
many years has been used in the domestic, food and
medical industries (Gilbert and Moore 2005; Kim et al.
2011). BAC and DDQ are quaternary ammonium com-
pounds that have also been well studied as antimicrobial
agents and used in a wide variety of settings (Ioannou
et al. 2007). Although PHMB, DDQ and BAC all display
impressive antimicrobial activity, we demonstrate that
these constituents are synergistic in the ByotrolTM G32
formulation and present a much greater degree of
antimicrobial activity.
The microtitre plate biofilm formation assay demon-
strates a correlation between the MIC results for the inhi-
bition of planktonic cells and the inhibition of biofilm
forming cells, that is, the fewer the planktonic cells, the
fewer the number of viable cells that are able to form a
biofilm. However, the results from the microtitre plate
biofilm formation assay validates the activity of ByotrolTM
G32 against planktonic cells and therefore as an inhibitor
of early biofilm formation. Ps. aeruginosa is inherently
resistant to many antimicrobial agents due to surface fac-
tors such as its outer membrane impermeability and
active drug efflux mechanisms (Drenkard 2003; Trott
et al. 2007). The MIC for the planktonic cells of Ps. aeru-
ginosa is lower than the biofilm inhibition concentration,
which may be a result of fewer planktonic cells being
killed; therefore, perhaps a greater number of cells were
able to proliferate as a biofilm.
By comparison, ByotrolTM is least effective against
Ps. aeruginosa. This may be explained by the suggestion
that biocides, which have a broad spectrum of activity
4·0
3·0
2·0
1·0
0·0Control0·3 0·6 3 5 15 60 100 200 400 1000
Control0·3 0·6 3 5 15 60 100 200 400 1000
Control0·3 0·6 3 5 15 60 100 200 400 1000
Control 0·3 0·6 3 5 15 60 100 200 400 1000
0·4
0·3
0·2
0·1
0·0
0·8
0·6
0·4
0·2
0·0
3·02·52·01·51·00·50·0
E. coli K12
E. coli
K. pneumoniae
P. aeruginosa
OD
595
nm
ByotrolTM concentration (µg ml–1)
Figure 4 Minimum Biofilm Eradication Concentration assay to deter-
mine the biofilm eradication activity of ByotrolTM G32. The biofilms
were grown statically on a lid with protruding polystyrene pegs for
18 h and treated with ByotrolTM G32 for 18 h. The lid carrying pegs
were re-incubated in fresh media for a further 18 h. The extent of
remaining biofilm was determined by crystal violet staining. All data
represent the mean of 24 replicates, involving three biological repli-
cates for each strain. Error bars indicate the standard error of the
mean.
1290 Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology
Preventing biofilm-related infections N. Govindji et al.

and nonspecific targets, may cause nonspecific resistance
mechanisms, for example in Ps. aeruginosa, the hyperex-
pression of multidrug efflux pumps (Gilbert and McBain
2003). There may also be changes to the outer mem-
brane, which reduces the permeability of the membrane
to the biocide (McDonnell and Russell 1999; Gilbert
2005). However, the higher MIC of ByotrolTM for
Ps. aeruginosa compared to that of the other organisms
tested is likely to be due to increased tolerance rather
than resistance (Gilbert and McBain 2003).
Intervention at the early stages of biofilm development
and inhibiting planktonic cells before they are able to
attach to a surface is most desirable. For this reason, the
inhibition of viable planktonic bacteria to attach to the
surface was evaluated at 18 h with the microtitre plate
biofilm formation assay and 8 h for the pretreatment of a
glass surface, as these time points reflect the early stages
of biofilm formation.
Pretreatment of a surface with ByotrolTM G32 in this
study provided the preliminary data as to the efficacy of
ByotrolTM as an antimicrobial coating. AFM clearly shows
the deposition of a nonstructured thin film over the con-
centration range for ByotrolTM G32. Glass has a negative
zeta potential at pH 7 (Gu and Li 2000); therefore, we
propose that as PHMB is a positively charged polyelectro-
lyte, it strongly adheres to the surface through opposite
charge interaction (Borkovec and Papastavrou 2008) and
serves to enhance the weaker adhesion of both BAQ and
DDQ through the formation of a composite film.
To place these findings in a clinical context, the stabil-
ity and lifetime of this coating under the flow of urine
would also be an important factor in the success of Byo-
trolTM as a catheter coating. The more stable the coating,
the longer the lifetime of the catheter. That being the
case, any long-term toxicity associated with ByotrolTM
against uroepithelial cells would also need to be assessed.
It should be noted that PHMB and BAC, the compounds
demonstrating the highest antimicrobial activity in the
ByotrolTM formulation, are already widely used in the
environmental and clinical setting, including wound care
100
0 0
nm
20µM 10
020
µ M 10
0 20µM
100 20µM
10
1009080706050403020100
10090807060504030201000 1 2 3 4
Film
dep
th (
nm)
Film
dep
th (
nm)
Line distance (µm)0 1 2 3 4
Line distance (µm)
4·0
3·5
3·0
2·5
2·0
1·5
1·0
0·5
0·0U
E. coli K12
E. coli
K. pneumoniae
P. aeruginosa
C U C U C U C
(a)
(b)
(c)
Figure 5 The effects of ByotrolTM G32-coated
glass surfaces on biofilm development. (a) A
glass surface was coated with 5 lg ml�1 and
1 mg ml�1 ByotrolTM G32 for 18 h. A scratch
was made across the surface to indicate the
depth of the coatings (b) The film depth was
determined by measuring the distance across
the scratches in three distinct areas. ( )
Line1; ( ) Line2 and ( ) Line3. (c) Biofilms
of Escherichia coli K12 (black bars), and
clinical isolates of E. coli (grey bars), Klebsiella
pneumoniae (white bars) and Pseudomonas
aeruginosa (hashed bars), were grown
statically for 8 h at 37°C on uncoated glass
surfaces (Control) and glass surfaces coated
with 5 lg ml�1 and 1 mg ml�1 ByotrolTM
G32. The extent of biofilm formation was
determined by solubilization of crystal violet
used to stain adhered cells. The absorbance
values of solubilized stain represent the
mean of six biological replicates for each
strain. Error bars indicate the standard error
of the mean.
Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology 1291
N. Govindji et al. Preventing biofilm-related infections

dressings and ophthalmic solutions. In a clinical review,
PHMB was stated to have good clinical safety with no
known toxic risks (Gray et al. 2010), and even with long-
term use, BAC was stated to pose no clinical risk (Marple
et al. 2004). Therefore, although cytotoxicity testing
would need to be performed prior to a ByotrolTM-coated
catheter entering the clinical setting, it is probable that
ByotrolTM should be safe to use.
In conclusion, ByotrolTM G32 has the ability to reduce
bacterial growth as an antimicrobial in suspension, as a
coating, and is also able to disrupt an existing biofilm. It
may therefore hold great promise not only as an antimi-
crobial coating for medical devices but also as a sanitizing
agent for the removal of established biofilms.
Acknowledgements
We would like to thank Age UK for funding this research
and Byotrol Technology Ltd. for sample provision. The
microscopes used in this study were part of The Bioimag-
ing Facility at the University of Manchester, purchased
with grants from BBSRC, the Wellcome Trust and the
University of Manchester Strategic Fund.
References
Anderson, G.G. and O’Toole, G.A. (2008) Innate and induced
resistance mechanisms of bacterial biofilms. Curr Top
Microbiol Immunol 322, 85–105.
Atiyeh, B.S., Costagliola, M., Hayek, S.N. and Dibo, S.A.
(2007) Effect of silver on burn wound infection control
and healing: review of the literature. Burns 33, 139–148.
Banerjee, I., Pangule, R.C. and Kane, R.S. (2011) Antifouling
coatings: recent developments in the design of surfaces
that prevent fouling by proteins, bacteria, and marine
organisms. Adv Mater 23, 690–718.
Bologna, R.A., Tu, L.M., Polansky, M., Fraimow, H.D.,
Gordon, D.A. and Whitmore, K.E. (1999) Hydrogel/silver
ion-coated urinary catheter reduces nosocomial urinary
tract infection rates in intensive care unit patients: a
multicenter study. Urology 54, 982–987.
Borkovec, M. and Papastavrou, G. (2008) Interactions between
solid surfaces with adsorbed polyelectrolytes of opposite
charge. Curr Opin Colloid Interface Sci 13, 429–437.
Boswald, M., Lugauer, S., Regenfus, A., Braun, G.G., Martus, P.,
Geis, C., Scharf, J., Bechert, T. et al. (1999) Reduced rates
of catheter-associated infection by use of a new silver-
impregnated central venous catheter. Infection 27, S56–S60.
Ceri, H., Olson, M.E., Stremick, C., Read, R.R., Morck, D. and
Buret, A. (1999) The Calgary Biofilm Device: new
technology for rapid determination of antibiotic
susceptibilities of bacterial biofilms. J Clin Microbiol 37,
1771–1776.
Christensen, G.D., Simpson, W.A., Younger, J.J., Baddour,
L.M., Barrett, F.F., Melton, D.M. and Beachey, E.H.
(1985) Adherence of coagulase-negative staphylococci to
plastic tissue-culture plates - a quantitative model for the
adherence of staphylococci to medical devices. J Clin
Microbiol 22, 996–1006.
Costerton, J.W. (2007) The Biofilm Primer. Berlin, Heidelberg:
Springer-Verlag Berlin Heidelberg.
Costerton, J.W., Cheng, K.J., Geesey, G.G., Ladd, T.I., Nickel,
J.C., Dasgupta, M. and Marrie, T.J. (1987) Bacterial
biofilms in nature and disease. Annu Rev Microbiol 41,
435–464.
Costerton, J.W., Lewandowski, Z., Caldwell, D.E., Korber, D.R.
and Lappin-Scott, H.M. (1995) Microbial biofilms. Annu
Rev Microbiol 49, 711–745.
Costerton, J.W., Stewart, P.S. and Greenberg, E.P. (1999)
Bacterial biofilms: a common cause of persistent
infections. Science 284, 1318–1322.
Darouiche, R.O. (2001) Device-associated infections: a
macroproblem that starts with microadherence. Clin Infect
Dis 33, 1567–1572.
Davenport, K. and Keeley, F.X. (2005) Evidence for the use
of silver-alloy-coated urethral catheters. J Hosp Infect 60,
298–303.
Drenkard, E. (2003) Antimicrobial resistance of Pseudomonas
aeruginosa biofilms. Microbes Infect 5, 1213–1219.
Gilbert, P. (2005) Cationic antiseptics: diversity of action
under a common epithet. J Appl Microbiol 99, 12.
Gilbert, P. and McBain, A.J. (2003) Potential impact of
increased use of biocides in consumer products on
prevalence of antibiotic resistance. Clin Microbiol Rev 16,
189–208.
Gilbert, P. and Moore, L.E. (2005) Cationic antiseptics:
diversity of action under a common epithet. J Appl
Microbiol 99, 703–715.
Gray, D., Barrett, S., Battacharyya, M., Butcher, M., Enoch, S.,
Fumerola, S., Stephen-Haynes, J., Edwards-Jones, V. et al.
(2010) PHMB and its potential contribution to wound
management. Wounds UK 6, 40–46.
Gu, Y.G. and Li, D.Q. (2000) The zeta-potential of glass
surface in contact with aqueous solutions. J Colloid
Interface Sci 226, 328–339.
Hatt, J.K. and Rather, P.N. (2008) Role of bacterial biofilms in
urinary tract infections. Curr Top Microbiol Immunol 322,
163–192.
Ioannou, C.J., Hanlon, G.W. and Denyer, S.P. (2007) Action
of disinfectant quaternary ammonium compounds against
Staphylococcus aureus. Antimicrob Agents Chemother 51,
296–306.
Jaglic, Z. and Cervinkova, D. (2012) Genetic basis of resistance
to quaternary ammonium compounds - the qac genes and
their role: a review. Vet Med 57, 275–281.
Johnson, J.R., Kuskowski, M.A. and Wilt, T.J. (2006)
Systematic review: antimicrobial urinary catheters to
1292 Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology
Preventing biofilm-related infections N. Govindji et al.

prevent catheter-associated urinary tract infection in
hospitalized patients. Ann Intern Med 144, 116–126.
Kim, S.Y., Lee, H.S., Hyun, J.J., Seo, M.H., Yim, S.Y., Oh,
H.Y., Kim, H.S., Keum, B. et al. (2011) Comparison on
the efficacy of disinfectants used in automated endoscope
reprocessors: PHMB-DBAC versus orthophthalaldehyde.
Clin Endosc 44, 109–115.
Knetsch, M.L.W. and Koole, L.H. (2011) New strategies in the
development of antimicrobial coatings: the example of
increasing usage of silver and silver nanoparticles.
Polymers 3, 26.
Marple, B., Roland, P. and Benninger, M. (2004) Safety review
of benzalkonium chloride used as a preservative in
intranasal solutions: an overview of conflicting data and
opinions. Otolaryngol Head Neck Surg 130, 131–141.
McDonnell, G. and Russell, A.D. (1999) Antiseptics and
disinfectants: activity, action, and resistance. Clin Microbiol
Rev 12, 147–149.
Modak, S.M. and Fox, C.L. (1981) Sulfadiazine silver-resistant
Pseudomonas in Burns - New Topical Agents. Arch Surg
116, 854–857.
Patel, R. (2005) Biofilms and antimicrobial resistance. Clin
Orthop Relat Res, 4, 1–47.
Percival, S.L., Bowler, P.G. and Russell, D. (2005) Bacterial
resistance to silver in wound care. J Hosp Infect 60, 1–7.
Polonio, R.E., Mermel, L.A., Paquette, G.E. and Sperry, J.F.
(2001) Eradication of biofilm-forming Staphylococcus
epidermidis (RP62A) by a combination of sodium
salicylate and vancomycin. Antimicrob Agents Chemother
45, 3262–3266.
Richards, M.J., Edwards, J.R., Culver, D.H., Gaynes, R.P. and
System, N.N.I.S. (1999) Nosocomial infections in medical
intensive care units in the United States. Crit Care Med
27, 887–892.
Silver, S. (2003) Bacterial silver resistance: molecular biology
and uses and misuses of silver compounds. FEMS
Microbiol Rev 27, 341–353.
Silver, S., Phung, L.T. and Silver, G. (2006) Silver as biocides
in burn and wound dressings and bacterial resistance to
silver compounds. J Ind Microbiol Biotechnol 33, 627–634.
Smith, R.L., Meixler, S.M. and Simberkoff, M.S. (1991) Excess
mortality in critically ill patients with nosocomial blood-
stream infections. Chest 100, 164–167.
Trott, D.J., Moss, S.M., See, A.M. and Rees, R. (2007)
Evaluation of disc diffusion and MIC testing for
determining susceptibility of Pseudomonas aeruginosa
isolates to topical enrofloxacin/silver sulfadiazine. Aust Vet
J 85, 464–466.
Van, H.R. and Michiels, C.W. (2005) Role of bacterial cell
surface structures in Escherichia coli biofilm formation. Res
Microbiol 156, 626–633.
Verleyen, P., De Ridder, D., Van Poppel, H. and Baert, L.
(1999) Clinical application of the Bardex IC Foley
catheter. Eur Urol 36, 240–246.
Vuong, C., Kocianova, S., Voyich, J.M., Yao, Y.F., Fischer,
E.R., DeLeo, F.R. and Otto, M. (2005) A crucial role for
exopolysaccharide modification in bacterial biofilm
formation, immune evasion, and virulence (vol 279, pg
54881, 2004). J Biol Chem 280, 12064.
Woods, E.J., Cochrane, C.A. and Percival, S.L. (2009)
Prevalence of silver resistance genes in bacteria isolated
from human and horse wounds. Vet Microbiol 138,
325–329.
Journal of Applied Microbiology 114, 1285--1293 © 2013 The Society for Applied Microbiology 1293
N. Govindji et al. Preventing biofilm-related infections