Embed Size (px)
Citation preview

Bull. Org. mond. Sant) 1963, 28, 139-173Bull. Wid Hith Org.
Tests for Addiction (Chronic Intoxication)of Morphine Type
H. HALBACH, Dr.med. Dr.-Ing.' & NATHAN B. EDDY, M.D.2
A survey is presented of laboratory and clinical methods for the determination ofaddiction liability of substances with morphine-like effects. Since physical dependence isthe outstanding pharmacological criterion ofaddiction of morphine type, the procedures forits qualitative and quantitative assessment are described in detail.
CONTENTSPage
Introduction . . . . . . . . . . . . . . . . . . . . . 139
Tests for appraisal of physical dependence in animals . . . 140
Tests for addiction (abuse) liability in former addicts . . . . 150
Tests for development of tolerance and physical dependenceunder clinical conditions . . . . . . . . . . . . . . . 156
Tests for detection of drug use and recidivism . . . . . . 159
Discussion and summary . . . . . . . . . . . . . . . . 161
Resum . . . . . . . . . . . . . . . . . . . . . . . 163
References . . . . . . . . . . . . . . . . . . . . . . 164
Annexes . . . . . . . . . . . . . . . . . . . . . . 166
INTRODUCTION
In its seventh report, the WHO Expert Committeeon Addiction-Producing Drugs (1957) definedaddiction as follows:" Drug addiction is a state of periodic or chronic intoxica-tion produced by the repeated consumption of a drug(natural or synthetic). Its characteristics include:
(1) an overpowering desire or need (compulsion) tocontinue taking the drug and to obtain it by any means;
(2) a tendency to increase the dose;(3) a psychic (psychological) and generally a physical
dependence on the effects of the drug;(4) detrimental effect on the individual and on society."
I Chief, Addiction-Producing Drugs, World HealthOrganization, Geneva, Switzerland.
2 Consultant to the National Institutes of Health,Bethesda, Md., USA, and to the World Health Organiza-tion.
The purpose of this definition was to aid in thecharacterization of substances which have been orshould be subjected to international narcoticscontrol. Some of the characteristics in the defini-tion, the first and last particularly, are demonstrableonly through prolonged experience and are, in partat least, based upon impressions rather than uponquantitative data: tolerance and physical dependencecan be measured quantitatively.
Expressing themselves in more strictly pharma-cological terms, Himmelsbach & Small (1937) saidthat addiction embraced three intimately relatedbut distinct phenomena-tolerance, habituationand physical dependence. They were speakingof the opiates, morphine and morphine derivatives,but the statement applies to all synthetic substanceswith morphine-like effect. Tolerance, the gradualdecrease in an effect developing during the repeatedadministration of a drug, is measurable to the extent
1222 - 139 -

H. HALBACH & N. B. EDDY
that quantitative methods are available for investi-gating the effect in question. It can occur with a widevariety of substances, whether or not morphine-like.Habituation is a psychic dependence, adaptationand mental conditioning to the repetition of aneffect manifested by craving for and efforts to bringabout continuation of the drug's administration.Its possibility in animals has been claimed (Krueger,Eddy & Sumwalt, 1941b) and denied (Lindesmith,1937). Currently efforts are being made to proveits development and measure it quantitatively.Physical dependence is an essential characteristic ofopiate addiction. It is the distortion of physiologicalprocesses which results from prolonged administra-tion of a drug and which requires the presence of anadequate amount of an addicting drug in the bodyfor the maintenance of physical equilibrium. Phy-sical dependence is demonstrated bythe appearance ofa characteristic syndrome of abstinence phenomena.
Until comparatively recently the only means ofjudging over-all addiction liability was the generalimpression from prolonged clinical experience, andunder these circumstances years might elapse beforea reasonably accurate appraisal was attained. Theestablishment of the Addiction Research Centerat the Public Health Service Hospital for addicts atLexington, Ky., USA, led to the development of atleast semi-quantitative measurement of morphine-like properties as they related to addiction. Also theunequivocal demonstration of withdrawal pheno-mena in animals, proving the universality amongspecies of physical dependence as a pharmacologicalconsequence, stimulated efforts to measure it quanti-tatively. Therefore, there are now available testsapplicable to animals and to man which permit anearly estimate of the relative risk of abuse and ofaddiction to be expected under clinical conditions.In addition the production of nalorphine and othermorphine antagonists and the discovery of theirability to precipitate an abstinence syndrome whenphysical dependence exists has made possible earlydetection of physical dependence and developingaddiction under usual clinical conditions.In this report we propose to describe these tests
for addiction under four heads: appraisal of physicaldependence in animals; determination of addiction(abuse) liability in former addicts; measurement ofthe development of tolerance and physical depend-ence under clinical conditions; and detection of druguse and recidivism. Our purpose is to assess therelative importance, reliability and interpretation ofthe tests and to stimulate their broader application.
TESTS FOR APPRAISAL OF PHYSICAL DEPENDENCEIN ANIMALS
Since the abstinence symptoms on which theassessment of physical dependence is based occuron a high level of physiological organization, theexperimental object used is as a rule the wholeanimal. However, the occurrence of abstinencephenomena has also been shown in objects of alower level of organization, such as tissue-cultures.Semura (1933), Sanjo (1934), Nakazawa (1937), andSasaki (1938) observed the development of toleranceto the growth-inhibiting effects of morphine andcertain of its derivatives in cultures of fibroblastsand iris epithelial tissue, and furthermore, as a con-sequence of the withdrawal of these drugs, eitherrestoration of growth or damaging effects. Thecurative effect of morphine and its derivatives onthe latter was also described and the more abrupt thewithdrawal, the more pronounced were the abstin-ence signs (Kubo, 1939). However, these findingsdid not lead to the development of methods ofevaluation (Heubner et al., 1952); nor has this beenthe case with certain reactions in isolated organswhich might be interpreted as signs of abstinenceon the basis of a physical dependence, such as theinhibitory effect of the withdrawal of morphine onthe rabbit's heart (Wada, 1928) or the stimulationproduced in the same way in preparations of intes-tines (Abe, 1930; Fujita, 1931; see also Paton, 1957).A more intimate analysis of these phenomena mightdisclose some parallelism between the physicaldependence reactions of single cells, tissues, andisolated organs on the one hand and of the wholeanimal organism on the other.For practical purposes there are at present avail-
able physical dependence tests in various animalspecies with a varying degree of reliability, that is,comparability to what happens in man.
MiceAfter prolonged administration of morphine and
analgesics with morphine-like effect mice do notappear to react to their abrupt withdrawal withsymptoms which are sufficiently regular and distinctfor an assessment of physical dependence. In thehope of finding a correlation between tolerance tothe toxic effects of morphine and morphine-likesubstances and their addiction liability, it has beenrepeatedly examined whether mice can acquire atolerance to the toxic (lethal) effects of such drugs bytheir chronic administration in increasing doses.From an extensive survey of the literature and from
140

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
her own experiments, Fichtenberg (1951) concludedthat mice do not, or not nearly so easily as severalother species, become tolerant to the toxic effects ofmorphine. Mercier and associates (1957) found thatmice acquired no tolerance to the LD50 of heroin,oxycodone, or pethidine, and only a partial andincomplete tolerance to that of morphine, methadoneand levorphanol. However, in the latter cases thedevelopment of tolerance was not uniform and wasdifficult to compare because of different regimens ofadministration.
In view of the failure to establish a correlationbetween addiction liability and tolerance to the toxiceffects, the relation between the tolerance of mice tothe analgesic properties of the substance in questionand its addicting properties has been investigated.Using a modification of Woolfe & MacDonald'stest (hot plate; licking response) Jacob and associates(1958) examined a benzodioxane derivative (3570 CT)which had, in mice, half the analgesic activity ofmorphine. When given in equi-analgesic dosestolerance developed to the analgesic effect of bothsubstances. However, when tested in monkeys (formethod, see page 148 of this report) 3570 CT did notproduce evidence of physical dependence. Con-tinuous administration by means of subcutaneousimplantation of morphine (base) seemed to favourthe development of tolerance to various morphineeffects (such as sedation, analgesia, Straub reaction)and also the development of physical dependence, asshown by the unmasking action of nalorphine; butthe symptoms of nalorphine-induced withdrawalwere not uniform enough for an evaluation of physi-cal dependence (Maggiolo & Huidobro, 1961).
Correlations have also been sought between theStraub tail-reaction in mice and addiction liabilityin man. While the low tendency of mice to developtolerance to the effects of morphine refers also to thetail reaction (see Krueger, Eddy & Sumwalt, 1941a),Shemano &Wendel (1960; also personal communica-tion, 1962) believe that the determination of a" Straub index" in mice might be useful for initialscreening for potential addiction liability in man.They reported that, when drugs were administeredintravenously, the wider the dosage separationbetween drug-induced Straub tail-reaction anddeath, the greater was the probability of highaddiction liability. Compounds with a narrowdosage separation are likely to be minimally ormildly addicting. The degree of separation wasexpressed by the Straub index (LD50/ED60 Straubreaction). A statistically significant rank-order
correlation (0.75 (P < 0.01)) was found betweenthe Straub index and the "estimated " addictionliability in man in a series of drugs, including, interalia, phenazocine, hydromorphone, heroin, mor-phine, methadone, pethidine, codeine, dextro-propoxyphene and nalorphine. For most of thedrugs tested, a similar correlation was noted betweenaddiction liability and " analgesic index " in mice(LD5O/ED5O analgesic effect), but a specific exception(apomorphine) throws doubt on the interchange-ability of the indices.
Rats
Joel & Ettinger (1926) reported on the occurrenceof withdrawal phenomena in rats and their relief bythe re-administration of morphine. On the basis ofBarlow's (1932) observation that increased irritabilitywas a measurable and rather constant response ofrats to the sudden interruption of chronic morphineadministration, Himmelsbach and associates (1935)developed a method for the assessment of physicaldependence. The drugs tested in this way (morphine,codeine, heroin) were administered every 24 hoursfor five to six weeks and then abruptly withheld.Eddy & Himmelsbach (1936), applying in principlethe same method, found that desomorphine had tobe given at shorter intervals in order to produce asignificant response with regard to physical depend-ence. According to Stanton (1936) the signs follow-ing abrupt withdrawal, after four weeks of morphineinjections, reached a peak within two to four daysof withdrawal. Fichtenberg (1951) reported thatrats tolerant to 50 mg of morphine subcutaneouslyper 100 g body-weight became agitated and aggres-sive on the second and third days after discontinua-tion of morphine, with loss of weight, either tem-porary with recovery or continuing until death.
Motivated by the irregular results of withdrawalexperiments with rats, Mercier & Sestier (1954) meas-ured the development oftolerance and physical depen-dence by means of a discriminatory training test(choice between green and red drinking-water, withelectrical punishment for the latter). The discrimi-natory performance was totally abolished by a singlesubcutaneous dose of80mg ofmorphine perkg and, asa result of tolerance, reappeared during continuingadministration of increasing morphine doses of upto 120 mg/kg daily. Thirty-six to forty-eight hoursafter the abrupt withdrawal of morphine the dis-criminatory performance was seriously disturbed,but not completely abolished. Concomitant symp-toms appearing after the same interval were increased
141

H. HALBACH & N. B. EDDY
motor activity, aggressiveness, squeaking, and hor-ripilation. All signs disappeared, generally withinfour days. With heroin, oxycodone, pethidine,levorphanol and methadone, also, the disturbanceof the acquired behaviour could be demonstratedand so could its re-establishment as a sign of toler-ance (Mercier & Mercier, 1957). After abrupt ces-sation of these drugs, impairment of the performanceor other symptoms could, however, not be observedequally well in all cases (possibly because of con-siderable divergences in the dosages exceeding theequi-analgesic dose ratio).
In the course of experimentation in the AddictionResearch Center, Lexington, on the conditioning ofdrug-seeking behaviour, the effects of sudden with-drawal were studied by Wikler & Martin (personalcommunication, 1962) in rats tolerant to large dosesof morphine (200 mg/kg/day and 320 mg/kg/day,subcutaneously and intraperitoneally). Sudden with-drawal of morphine was followed by rapid subsi-dence of the locomotor hyperactivity, hyperthermiaand elevated oxygen consumption rates character-istic of morphine-tolerant animals. These variablesapproached normal levels between the 8th and 12thhours of abstinence, but during this time the animalsbegan to exhibit a marked increase in the frequencyof spontaneously occurring episodes of repetitiveshaking of the skin of the entire body (" wet dog "phenomenon). During the next 12-16 hours, theseepisodes increased in frequency, and the rats becamemore irritable, showed more grooming activity anddiarrhoea, and began to lose weight; concomitantly,body temperature and oxygen consumption rate fellfurther towards normal or even slightly subnormallevels. These signs reached peak intensity betweenthe 24th and 48th hours of abstinence and subsidedthereafter. However, from the 4th day of abstinenceonwards, for a period as yet undetermined, " wetdog" counts, body temperature, metabolic rateand total daily water intake were slightly higherin the formerly addicted rats than in the controlanimals.
In rats stabilized on a single dose of 200 mg/kg/dayof morphine intraperitoneally, increased " wet dog "frequency and other signs of acute abstinence,similar to those described above, were noted beforeadministration of the daily dose of morphine. If,however, the rats were permitted to drink an aqueoussolution of etonitazene instead of water during theinterval between two daily doses of morphine, theacute pre-injection abstinence syndrome was sup-pressed to a degree depending on the concentration
of etonitazene in the solution. With concentrationsof 20 and 40 ,ug/ml of etonitazene, all signs ofmorphine abstinence were suppressed but signsresembling those of chronic morphine intoxication(increased locomotor activity, hyperthermia andelevated oxygen consumption) were manifest.
Since the symptoms of spontaneous withdrawal inrats have not always been sufficiently uniform andregular to form the basis of a reliable test method,the nalorphine-precipitated withdrawal syndrome inrats has been examined, apparently with betterresults.
According to Hanna (1960) the demonstration ofnalorphine-induced withdrawal signs in rats (ofabout 250 g in weight) required the previous admi-nistration, conveniently by the intraperitoneal routeand at intervals not exceeding four hours, of verylarge doses of morphine, beginning with 90 mg/kg,with daily increases of 18 mg/kg until a dosage of360 mg/kg every 4 hours was reached. This dosage,which caused weight loss and sometimes death,was maintained for 5 days. 10-20 mg of nalorphineper kg, given intraperitoneally 30 minutes after thelast morphine injection, produced within a fewminutes increased motor activity and hyperexcita-bility, with brief convulsions in some animals. Thesymptoms subsided after about two hours. AsHanna remarked, the requirement of very largedoses of morphine " may or may not be of value inthe evaluation of physical dependence liability ofnew compounds " in rats.Kaymakcalan & Woods (1956) compared the
symptoms of abrupt withdrawal from morphinewith those produced by nalorphine in morphine-tolerant rats, that is, in animals which had receivedmorphine sulfate twice daily, subcutaneously, indoses increasing from 20 mg/kg to 100 mg/kg andhad been maintained on the latter dose for 12-25days. In the course of the development of tolerance,morphine produced less sedation and, instead, moreand more central stimulation. While the abruptwithdrawal of morphine generally resulted in mildsedation only, the nalorphine-induced withdrawalsyndrome included a marked increase in intestinalactivity with corresponding results appearing withina few minutes and followed, after about 30 minutes,by sedation that was distinctly greater than thatafter abrupt withdrawal. The dose of nalorphine(10 mg/kg) was administered 2 or 12 hours after thelast dose of morphine; in the case of the longerinterval the withdrawal symptoms were perhapssomewhat more pronounced.
142

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
To avoid the risks of local irritation and infectionpresented by frequent injections of the large quan-tities of drug necessary for the production anddemonstration of physical dependence, Lister &Ettles (personal communication, 1961) have admi-nistered the test drug dissolved in drinking-water.Because of the usually unpleasant taste this is pos-sible only with very low drug concentrations, that is,with highly potent substances. The authors em-ployed a compound with 1500 times the analgesicpotency of morphine in an estimated initial dailydose of 10 ,ug for rats weighing 35-45 g, and increasedit within three weeks to 10 mg per rat per day. Then,a withdrawal syndrome was precipitated by admi-nistration of 3 mg of levallorphan per kg sub-cutaneously or intraperitoneally. The outstandingsign of withdrawal was stretching or writhing similarto that produced in rats and mice by the intra-peritoneal administration of local irritants. Theauthors related this symptom to the gastro-intestinalwithdrawal symptoms in man. By analogy withHimmelsbach's system for scoring the abstinencesyndrome (see Table 1, opposite), the authorsestablished the following scale for scoring antagonist-precipitated (by levallorphan as well as by nalor-phine) withdrawal symptoms in rats:
Signs
StretchingSqueal on touchingTeeth chatteringHypersensitivity to noiseDiarrhoeaSedationPtosisChewingPinna sensitivityEar twitchPilo-erectionScratching
Points
543322
2Il
25
With suitable dosage of the addicting compound,physical dependence developed within one week,and the optimal dose of levallorphan for precipita-tion of abstinence signs was 2-3 mg/kg.
Lister & Ettles also demonstrated that the symp-toms following precipitated withdrawal of theirvery potent compound could be suppressed, at leastpartially, by a moderate dose of the same compoundor by the administration of morphine or anotherpotent analgesic.
TABLE 1
SYSTEM FOR SCORING ABSTINENCE SYNDROMES a
D b H c
Signs (by day) (by hour)points limit points limit
Yawning 1 1 1 1
Lacrimation I I 1 1
Rhinorrhoea I 1 1 1
Perspiration I I 1 1
Mydriasis 3 3 3 3
Tremor 3 3 3 3
Gooseflesh 3 3 3 3
Anorexia (40% decrease incaloric intake) 3 3
Restlessness 5 5 5 5
Emesis (each spell) 5 5 5
Fever (for each 0.1'C riseover mean addiction level) 1 1 10
Hyperpnoea (for each resp./min. rise over mean addic-tion level) 1 1 10
Rise in a.m. systolic BP(for each 2 mm Hg overmean addiction level) 1 15 1 10
Weight loss (a.m.) (for eachlb. from last day of addic-tion) 1
a The total abstinence syndrome intensity per day or per houris the sum of the points scored in the " D " or " H " columns,respectively, with due attention to the limits.
b Kolb & Himmelsbach (1938).c Himmelsbach (1939).
A nalorphine-precipitated abstinence syndromehas also been demonstrated in rats tolerant tocodeine, a substance with a much lower addictionpotential than morphine (Kuhn- & Friebel, 1962).For eight weeks the animals received daily threesubcutaneous doses of codeine phosphate, beginningwith 10 mg/kg and rising, in three bi-weekly increases,to 22.2 mg/kg per dose. After eight weeks, the lastcodeine injection was followed, 30 minutes later, bythe subcutaneous injection of 20 mg of nalorphineper kg. The ensuing abstinence syndrome, with itspeak between 15 and 20 minutes after nalorphineadministration, comprised practically the samesymptoms as those observed by Lister & Ettles.These symptoms were classified by Kuhn & Friebelas follows:
143

H. HALBACH & N. B. EDDY
Signs
StretchingChewingTeeth chatteringSqueal on touchingPtosisDiarrhoeaSedationIncreased movementsScratching
Points
322221111
15
Ptosis, sedation, and scratching-but not themore distinctive signs-occurred also in animalswhich were challenged with nalorphine after havingreceived one single dose of codeine and, about halfas frequently, in the controls. However, the dif-ference in the total point score between these animalsand those that had received codeine for eight weekswas significant.
Rabbits
In rabbits, which have been used far less for studieson morphine and its congeners than the other speciesincluded in this survey, morphine affects the carbo-hydrate metabolism in a typical way (see Krueger,Eddy & Sumwalt, 1941c). The animal developstolerance to the hyperglycaemic effects of morphineand reacts to its withdrawal after chronic adminis-tration by a transitory hyperglycaemia. For racemicmethadone and isomethadone as well as for theirI-isomers, a-acetylmethadol, pethidine, alphaprodine,and levorphanol, the same changes were found tooccur (see Phatak & David, 1953). These authorsconcluded that the withdrawal hyperglycaemia,being seemingly related to the rate of developmentof tolerance to the hyperglycaemic effect, mightserve as an index of the addiction potential. How-ever, since physical dependence has so far not beenproven to be in immediate relation to tolerance, theusefulness of such a test would have to be examinedby its application to a large series of substances withknown physical dependence potency.
Cats
In cats, medium dosages of morphine and pharma-cologically related substances produce a peculiar stateof central excitation, marked by mydriasis, tachy-pnoea, and seemingly hallucinatory behaviour (seeSchaumann, 1957; Wikler, 1944). This reaction isquite specific and has been utilized in the charac-terization of morphine-like analgesics (Eddy &Himmelsbach, 1936). Akad (1952) examined for
morphine, heroin, hydromorphone, oxycodone,hydrocodone, codeine, dionine, methadone andpethidine the doses necessary to bring about the typi-cal excitation in cats. Although he did not relatethem to analgesic effects or otherwise, it would appearthat some relation might exist between them andanalgesic potency and, hence (see Eddy, Halbach &Braenden, 1956), physical dependence potency.Tavat & Akcasu (1956) extended Akad's investiga-tions to ketobemidone, levorphanol, dextrorphan,and levallorphan, using a simple device for recordingmotor activity. Relatively high doses of dextrorphanand levallorphan were without effect-in parallelto lack of addiction liability. Levallorphan antagon-ized or prevented the exciting effects of morphine.Cullumbine & Konop (1959) examined a few moresubstances-addicting and non-addicting-in thesame way with essentially the same results, includingthe demonstration of the preventive effect of theantagonists. They also noted exceptions to theparallelism between excitation in cats and addictionliability in men, for example, in the case of apo-morphine. They confirmed the rapid developmentof tolerance to the excitatory effects of these sub-stances (as already noted by Eddy & Himmelsbach,1936) and concluded that the relation studied,although not strict, was"... sufficiently close tosuggest that the cat injection test could be used toindicate the danger of inducing addiction. . ."The value of the cat excitation method as a pre-
liminary test would be improved by a check withspecific morphine antagonists; the neutralizingeffects of the latter in this respect have been describedby the aforementioned authors and earlier by Unna(1943), Hart & McCawley (1944), Wikler & Carter(1952), and Winter et al. (1954).
DogsAbstinence symptoms in dogs addicted to mor-
phine had already been observed and described bymany workers (see review by Schaumann, 1957)when the introduction of pethidine and methadoneinto clinical practice stimulated new trials using thisspecies for the evaluation of physical dependence tosubstances of morphine type.
Intact dogs. The morphine abstinence syndromein dogs as described by Plant & Pierce (1928), Tatum,Seevers & Collins (1929), Eddy & Reid (1934), andothers includes muscular rigidity, tremor, convul-sions, restlessness, yawning, salivation, lacrimation,rhinorrhoea, singultus, vomiting, diarrhoea, tachy-pnoea, pulse irregularities, hyperpyrexia, hydro-
144

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
philia, and loss of weight, with a peak 24-72 hoursafter abrupt withdrawal. The minimum dosageswhich the early authors considered necessary for thedevelopment of physical dependence signified byunmistakable abstinence symptoms were obviouslysometimes too high; Wikler (1946, 1948) describedthe appearance of a "mild, but characteristic"abstinence syndrome in dogs when treated with twodaily doses of 10 mg of morphine per kg duringperiods of 83-158 days.Under similar but not strictly comparable condi-
tions as to dosage and duration of addiction, Wikler& Frank (1947) found that in dogs the " methadoneabstinence syndrome appeared to be more rapid inonset, more severe and of shorter duration than thatof morphine ", while Winter & Flataker (1950)found it somewhat less severe, but of similar dura-tion.Two pethidine derivatives, piminodine and the
closely related 1-(2-phenylaminoethyl)-4-phenyl-piperidine-4-carboxylic acid ethyl ester, were com-pared with morphine by means of the abrupt with-drawal method in dogs (Woods et al., 1961). Theresults would indicate that the relative sensitivitiesof the dog with respect to physical dependence onsubstances of the morphine and pethidine groupresemble the situation in man, whereas, for example,monkeys are in this respect particularly sensitiveto the pethidine group. This would speak in favourof using dogs for predicting addiction liability inman. Nevertheless, so far as is known, no systematicattempts have been made to determine the value ofthe abrupt withdrawal method in dogs for thispurpose by extending the observations to a largernumber of morphine-like substances with a knownaddiction potential.By administration of nalorphine the demonstra-
tion of abstinence symptoms in dogs is made simplerand safer. After having ensured that nalorphine assuch produced only mild sedation, Carter & Wikler(1954) demonstrated the precipitation of character-istic withdrawal signs by subcutaneous administra-tion of 15 mg of nalorphine per kg in dogs addictedfor 7 days or longer to morphine (5-10 mg/kg every6 hours) or methadone (2-5 mg/kg every 6 hours).In its most complete form, the abstinence syndromeconsisted of restlessness, lacrimation, rhinorrhoea,yawning, salivation, vomiting, urination, markedtremors, and persistent digging, gnawing and rootingin the earth or sand, but considerable individualvariation, qualitative and quantitative, was observed.The symptoms appeared within 5-20 minutes and
became more severe as the addiction proceeded andwere more pronounced than those following theabrupt withdrawal of morphine or methadone aftercomparable periods of addiction. According toKaymakcalan & Woods (1954), 1.5 mg of nalor-phine per kg subcutaneously is sufficient to elicit thefull abstinence syndrome in morphine-addicted dogs.Carter & Wikler concluded that " by use of N-allylnormorphine and a large number of dogs, auseful rapid screening method for testing addiction-liability of analgesics with opiate-like actions maybe developed ". This conclusion would not appearto be invalidated by their finding (Carter & Wikler,1954, 1955) that neither spontaneous nor nalor-phine-precipitated abstinence symptoms occurredafter addiction to pethidine (possibly because of thelimitations imposed on dosage and frequency ofadministration by the toxic effects of the drug).A " normal " sensitivity of the dog (in relation towhat happens in man) to the physical dependenceproperties of piminodine and another pethidinederivative, as demonstrated by a typical abstinencesyndrome following abrupt withdrawal, has alsobeen found after nalorphine-induced withdrawal(Woods et al., 1961).For the purpose of testing it would be advantage-
ous if the period necessary for the development ofphysical dependence could be curtailed. In man(Wikler and associates, 1953; Fraser et al., 1961a)as well as in dogs (Wikler & Carter, 1953; Carter &Wikler, 1954), tolerance and physical dependencecan indeed be produced and demonstrated, parti-cularly when precipitated by specific morphineantagonists, in a measurable degree after a relativelyshort period of administration of morphine. Martin& Eades (1961) have shown that a single intravenousinfusion of morphine brings about tolerance andphysical dependence in a reproducible and measur-able way. They considered that " the reproducibilityand brevity of this method may recommend it forpreliminary screening of analgesic agents to identifythose that produce physical dependence ". Theprinciple of this method is as follows.
In beagle dogs (between 7 and 19 kg in weight)the following signs were measured every half-hour:pulse rate, respiratory rate, pupillary diameter, rectaltemperature, skin-twitch reflex (on pinching thesaddle area of the back), and hind-limb withdrawalreflex (following the roughly measurable squeezingof the left lateral digit). Nalorphine alone did notalter these signs significantly except for causing aslight miosis. The intravenous infusion of morphine
145

H. HALBACH & N. B. EDDY
sulfate at the rate of 3 mg/kg hourly producedwithin one to two hours the known effects andchanges in the 6 parameters. To 3 of them- namely,miosis and depression of the skin-twitch andwithdrawal reflexes-as well as to the behaviouraldepression, the animals developed a partial toleranceafter about three hours of infusion. Administrationof nalorphine (20 mg/kg) after almost eight hoursof morphine infusion produced, within five minutes,a striking reversal in the parameters measured, areversal of the behavioural depression, and othersymptoms of withdrawal.La Barre (1959) and Desmarez (1960) have
attempted to simplify the measurement of the stateof physical dependence by singling out and record-ing those withdrawal symptoms which manifestthemselves in changes of spontaneous motor activity.To this end the animal is kept in a spacious cage,fitted for automatic mobility recording, during theperiod of direct addiction or substitution andwithdrawal of either morphine or a test substance.The period of building up tolerance and physicaldependence to the addicting agent extends overseveral months, owing to the relatively low dosesand their small increments. With morphine, forexample, the daily dosages per dog (of 6-8 kg weight)were 10 mg subcutaneously for two months, 15 mgin the third month, 20 mg for the following threemonths, and then 40 or 50 mg (divided into twodoses daily) to accentuate the withdrawal effect.With this scheme tolerance to the sedative effectsof morphine develops within several days followingeach increase in dosage, but the sudden cessation ofmorphine during the first four to five months is notfollowed by a noteworthy increase in motor activity.This symptom appears clearly and with a statisticalsignificance only when the withdrawal is effectedafter at least four months' duration of this regimen.With animals thus made physically dependent on
morphine and using the recorded motor activity asthe parameter for physical dependence, two typesof tests can be carried out: (a) the suppression test,in which a single dose of the test substance is admini-stered eight to ten hours after withdrawal of mor-phine, and (b) the substitution test, in which thelast dose of morphine is replaced by the test sub-stance. If the test drug suppresses the increase inmotor activity in (a) or prevents it in (b) this isvalued as a strong argument in favour of its mor-phine-like addicting character-on the basis of theexperience that no substance is hitherto knownwhich produces these effects of suppression or
substitution without being itself capable of pro-ducing physical dependence, that is, addiction ofmorphine type (Eddy, Halbach & Braenden, 1956).In the view of the authors the results of these testsshould be confirmed by a " direct addiction" test,that is, chronic administration of the test substancein increasing doses (as in the scheme describedabove for morphine) with abrupt withdrawal andrelief of withdrawal symptoms by re-administrationof the test drug, with recording of motor activityduring all stages of the experiment.As to the dosage of the test drug, La Barre (per-
sonal communication, 1961) recommends its estab-lishment in relation to the LD1o0 (Knaffi-Lenz methodin guinea-pigs). The LD1oo of the test substance isdetermined and a fraction of this is used versus thesame fraction of the LD10o of morphine. To savetheir animals, the authors of this method prefer notto exceed one-fourth of the LD1oo.
Chordectomized (" spinal ") dogs. In the courseof research on neurophysiological mechanisms ofaddiction, Wikler has developed a method usingspinal dogs. With its distinct and readily reprodu-cible effects this method could also be, and on alimited scale has already been, used to screen drugsfor the presence and degree of physical dependenceproperties. Its relevant features, as described indetail by Wikler & Frank (1948), can be summarizedas follows.The experiments were made after recovery from
chordectomy between D-10 and D-12 and return ofthe reflexes to a stable level. Single doses of mor-phine (2-100 mg/kg) produced marked and typicalchanges in certain mechanically elicited and graphi-cally recorded hind-limb reflexes. Most promi-nent were the depression of the ipsilateral flexorand crossed extensor reflexes. During chronicadministration of morphine, tolerance developed toits depressing action on these reflexes, as manifestedby increased reflex responses between injections.Abrupt cessation of morphine was followed by theirfurther increase; 30 hours after withdrawal, rhythmicmovements of flexion and extension of the hind-limbs began and increased, and were accompaniedlater by the same withdrawal symptoms as seen inintact dogs, such as tachypnoea, tachycardia, risein temperature, yawning, lacrimation, rhinorrhoea,vomiting, and diarrhoea, reaching a peak at aboutthe same time (72nd to 90th hour) as the " running "movements. With methadone the same effectsappeared, but within a shorter sequence, and, as inthe intact dog, the abstinence syndrome of either
146

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
drug could be suppressed by the other. Thus thispreparation offers the elements essential for thedemonstration of physical dependence and enablesobjective recording of specific symptoms.While abstinence phenomena following abrupt
withdrawal appear in the spinal dog only after along period of addiction, they can be demonstratedby means of a single dose of nalorphine after two orthree days of addiction (Wikler & Carter, 1953). Theeffect of nalorphine alone on the ipsilateral flexorand crossed extensor reflexes was qualitatively thesame as that of morphine but quantitatively less.However, after pre-treatment with as little as 0.5 mgof morphine per kg every six hours for two orthree days, 15 mg of nalorphine per kg precipitateda typical abstinence syndrome resembling closelythat produced in spinal dogs by the abrupt with-drawal after weeks or months of addiction. Onset,intensity and duration of the nalorphine-inducedwithdrawal syndrome appeared to be related to theduration of addiction to morphine and the dose ofnalorphine, that is, the longer the animal had beenaddicted to morphine the smaller was the dose ofnalorphine necessary to produce a complete abs-tinence syndrome. This opens prospects for thequantitative testing of the physical dependencecapacity of unknown substances. Relevant in thisconnexion appear the observations by Wikler &Carter that the nalorphine-induced withdrawalsyndrome as measured by the reflex changes inspinal dogs was more intense than the abstinencesyndrome seen in the same animals after abruptwithdrawal; and further that, after subsidence ofthe reflex hyperactivity following withdrawal ofmorphine, nalorphine had the same depressingeffects on reflexes as before addiction to morphine.Interestingly, the impossibility of demonstrating inthe intact dog either spontaneous or nalorphine-induced abstinence symptoms following addictionto pethidine (Carter & Wikler, 1954, 1955) was alsoencountered in the spinal dog (Carter & Wikler,1955) and possibly for the same reason-namely,the limitations to dosage and frequency of applica-tion set by the toxic effects of pethidine.
Monkeys
Tatum, Seevers & Collins (1929) demonstrated theoccurrence of abstinence phenomena when mor-phine was abruptly withheld from monkeys whichhad received the drug daily. The starting dose wasonly 2 mg/kg and was increased by about 2 mg eachweek. Kolb & DuMez, beginning their experiments
in 1923 but not reporting them until 1931, mademore extensive observations on attempted addictionexperiments in monkeys, employing morphine,heroin and codeine. The drug was given in one dailydose for three months and twice daily thereafter,Sundays and holidays excepted. The dose of mor-phine was increased from 7 or 8 mg to 200 mg peranimal per day in eight to ten months. By theseventh month the withdrawal symptoms were sosevere after 40 hours of abstinence, that is, from theSaturday afternoon to the Monday morning dose,that an additional dose was given on Sundaymorning. They said that morphine "caused markeddependence, shown by a crouching posture, facialdistortion, hypersensitiveness, fall in temperature,and, in one case, death on withdrawal of the drug ".Monkeys made tolerant to large doses of morphine,heroin or codeine were tolerant to large doses of allthree drugs; the dependence produced by morphineor heroin was satisfied by the other drug, but notby codeine.
This was the background situation when metha-done came to general attention in 1946 and stimu-lated tremendous activity in the synthesis of com-pounds which might have morphine-like activity.Seevers and his associates tested many of these newcompounds in the monkey and in 1950 he proposeda programme to determine the value of this animalfor predicting addiction liability to the newersynthetic analgesics. The plan in the main was tocarry out in the monkey all of the proceduresemployed in man at the Addiction Research Centerin Lexington (single-dose administration, substitu-tion for morphine and direct addiction) and tocompare the results obtained with substances whichwere tested in both monkey and man. Seevers' pro-posal was incorporated into the research programmeof the Committee on Drug Addiction and Narcoticsof the National Research Council (USA) andthe work in this connexion of his laboratory at theUniversity of Michigan still continues under thesponsorship and support of the Committee.
It was shown early that results in the monkey withmany different chemical types were qualitatively likethose obtained in man and that when strong mor-phine-like properties were manifested in the monkeythis could be taken as a safe prediction of whatwould happen in man. From this earlier work therehas been developed a screening programme in whichmore than 350 agents have been tested and whichhas proved of very great value to all those interestedin the addiction liability, and hence the safety, of
147

148 H. HALBACH & N. B. EDDY
potentially valuable medicinal agents. It is thisscreening programme which will be described here.'
It has been demonstrated in animal and man thatany chemical substance capable of complete sup-pression of all of the specific signs of morphineabstinence is capable of creating physical depend-ence during chronic administration. Therefore, theprimary and principal objective of the screeningprocedure is to ascertain whether or not the testdrug is capable of complete suppression of allabstinence signs in the morphine-dependent monkey.If suppression is not complete the procedure deter-mines the degree to which the total spectrum ofsigns is affected. The abstinence suppression potencyis termed physical dependence capacity. Its deter-mination is initially qualitative but serves a range-finding function for the subsequent quantitativestudy of potency relative to morphine.
Physical dependence capacity is characterized as:High, when the drug produces complete suppres-
sion of all abstinence signs with doses which revealno other overt pharmacological effect;
Intermediate, when complete suppression of allabstinence signs is obtainable, but only with doseswhich elicit other pharmacological actions, mani-fested by such signs as stupor, ataxia, tremors, etc.;Low, when some suppression of abstinence signs
is induced, but attempts to produce more or com-plete suppression with larger doses is prevented bythe intervention of toxic effects such as coma, con-vulsions, etc.;
None, when the drug fails to produce any specificsuppression of the morphine abstinence signs.Non-specific depressants may obscure individualsigns.A colony of 50 to 100 monkeys (Macaca mulatta)
is maintained in a state of physical dependence by thesubcutaneous administration of 3 mg/kg of morphinesulfate every six hours without interruption. Aftera stabilization period of 60 days these monkeys canbe used for testing at weekly intervals.For testing, regular morphine injections are with-
held for 12-14 hours until abstinence signs of inter-
'We are indebted to Dr M. H. Seevers, Professor ofPharmacology, and to Dr Gerald A. Deneau, AssociateProfessor of Pharmacology. University of Michigan MedicalSchool. for permission to describe their methods. They arecurrently preparing for publication a series of reports onthis programme. A great deal of credit is also due to SamuelIrwin, Duncan McCarthy and Richard Burns, who havebeen closely associated with the development of the pro-cedures.
mediate intensity are present. If left untreated theabstinence signs increase in intensity progressivelyover the next several hours, but the administration ofmorphine or any drug with morphine-like physicaldependence capacity results in a partial or completesuppression of the signs of abstinence. If the dose ofthe test drug is in excess of that required to producecomplete suppression of the abstinence symptoms,typical signs of narcotic depression result.A pre-selected quantity of the test drug and
3 mg/kg of morphine sulfate are administered sub-cutaneously by someone other than the observer,each drug to two monkeys. The intensity of theabstinence signs or drug depression is graded justprior to and at intervals of 1/2, 1, 2, 3 ... 6 hoursafter administration, or until the monkeys havereturned to the pre-injection level of excitability. Ifthe dose of the test drug produces less effect than3 mg/kg of morphine, the dose is doubled for asubsequent test. This procedure is repeated until adose which is approximately equivalent to 3 mg/kgof morphine is determined or until side-effectsappear in such intensity as to preclude furthertesting. By this procedure it is ascertained whetherthe drug has high, intermediate, low, or no physicaldependence capacity.
Further testing is done with all drugs which havebeen found to have high or intermediate physicaldependence capacity. Its purpose is twofold: toextend the series of animals to confirm the originalestimate of physical dependence capacity, and todetermine accurately the potency of the test drugrelative to morphine. It must be stressed thatphysical dependence capacity and single-dose absti-nence suppression potency are not synonymous andmay not even parallel each other in relation to mor-phine. Only the former is of major predictivesignificance as it relates to addiction in man. Forexample, a compound of relatively low potency,20.0 mg/kg equivalent to 3.0 mg/kg of morphine,may have a high physical dependence capacity andin this respect be equal to morphine in its potentialas a drug of abuse, only requiring larger quantitiesto be effective.
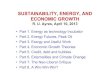
In the quantitative study five single-dose suppres-sion treatments are each administered to five mon-keys in a Latin square pattern at weekly intervals.These are X (the dose of the test drug which isapproximately equipotent to 3 mg/kg of morphine),1/2X, 2X and two controls, 3 mg/kg of morphinesulfate and a placebo (a saline injection). Theexperiment is conducted on a double-blind basis

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
FIG. I
TIME-EFFECT CURVES, OBTAINED FROM THE SAME FIVEMONKEYS IN SINGLE-DOSE SUPPRESSION TESTS, FOR A
TEST DRUG AT THREE DOSAGES (X2X, X, AND 2X),MORPHINE SULFATE (3 mg/kg) AND A PLACEBO a
a In all cases the average pre-inlection abstinence (with-drawal) severity was grade 3. The average maximum effect ofeach treatment is represented by the differences P to Q for 'AX,P to S for X, P to T for 2X, and P to R for morphine, and Is zerofor the placebo.
After Deneau & Seevers (1961).
FIG. 2
DOSE-RESPONSE CURVE OF THE TEST DRUG WHOSETIME-EFFECT CURVES ARE SHOWN IN FIG. I a
1/2X Y X 2XI/2X DOSE (mg/kg) Wo 2360
a The three points on the curve represent the effects P to Q,P to S and P to T in Fig. 1. A dose of Y is equivalent to 3 mg/kgof morphine sulfate.
After Deneau & Seevers (1961).
with respect to test drug versus morphine versusplacebo and from the peaks of the average time-effect curves which are obtained for each treatment(see Fig. I) a dose-effect curve (see Fig. 2) is estab-lished. The potency of the test agent relative tomorphine is determined from this curve.
In some cases the physical dependence potential ofa test drug is also investigated by chronic adminis-tration to monkeys which have not previouslyreceived narcotic analgesics. After the dose equi-potent to 3 mg/kg of morphine has been determinedby the single-dose suppression technique, this doseis administered for 31 days at intervals (usually twoto six hours) which correspond to its duration ofaction so that the monkeys are continuously underthe influence of the drug. If there is evidence ofwaning effect (tolerance) the individual dose isincreased. The development of physical dependenceis monitored on the 14th and 28th days of treatmentby administering 2 mg/kg of nalorphine. As in manthe administration of nalorphine precipitates anabstinence syndrome of one-half to four hours'duration, the severity of which corresponds to thedegree of physical dependence which has developed.On the 31st day of treatment drug administration isterminated abruptly and the monkeys are observedfor the following 7-14 days for signs of abstinence,graded according to the schema below.
In the single-dose suppression technique, effectivedoses of test drugs reduce the intensity of abstinencesigns more or less completely, or, having broughtabout complete suppression, may then producetypical signs of narcotic depression. In all of thetests described abstinence signs are graded, twogrades for each classification, according to Seevers'classification of abstinence signs (Deneau & Seevers,1961) and narcotic depression is graded (again twogrades for each classification) according to Irwin'sclassification of the effects of narcotic analgesics inthe monkey (Irwin, 1954). These classifications areas follows:
For abstinence signs:Mild (may be considered as of no significance by the
untrained observer): Apprehension, continual yawn-ing, rhinorrhoea, lacrimation, hiccup, shivering,perspiration on face, chattering, quarrelling andfighting;
Intermediate: Intention tremor, anorexia, pilomotoractivity, muscle twitching, rigidity and holding theabdomen (cramps);
Severe: Extreme restlessness, assumption of peculiarattitudes, vomiting, severe diarrhoea, erection and
IJ
149

150 H. HALBACH & N. B. EDDY
continued masturbation, inflammation of the eyelidsand conjunctiva (insomnia), continual calling andcrying, lying on the side with eyes closed, andmarked spasticity;
Very severe: Docility in the normally excitable animal,dyspnoea, pallor, strabismus, dehydration, weightloss, prostration, circulatory collapse, and occasion-ally death.
It will be noted that these signs fall into fourcategories of hyper-irritability: sympathetic, para-sympathetic, psychic (behavioural) and somatic(neuromuscular). Whereas morphine will suppressall signs of the syndrome evenly to an extent de-pendent upon the dose, many narcotic analgesicsfail to suppress one or another category of signs tothe same extent as the remainder of the syndrome.For this reason grades of abstinence intensity duringthe suppression test are assigned according to thebehavioural signs and not on the basis of the entireabstinence syndrome.For narcotic depression. The central nervous
system depression which is produced by narcoticanalgesics in the monkey is a combination of twofactors, referred to collectively as stupor: a de-creased awareness of, and diminished responsivenessto environmental stimuli, and a decrease in thedegree of apprehension, as indicated by alterationin behaviour, once his attention has been gained.The classification of stupor is:
Mild: Inattentive to ordinary movements and actionsof other monkeys within the cage and of the observeroutside the cage;
Intermediate: Attention gained by other monkeyswithin the cage only by strong threatening gesturesand attentive to the observer only when extra-ordinarily loud noises are made or the latch on thecage door is opened (a strong conditioned stimulus);
Severe: Responds only to such exteroceptive stimuli asshouting or clapping the hands loudly near its ear,or to being touched by other monkeys or the ob-server;
Very severe: Comatose and cannot be roused by anystimuli.
In the actual operation of the screening procedurea request for testing is made by the interested partyto the Executive Secretary of the Committee onDrug Addiction and Narcotics of the NationalResearch Council (USA). A sample of the drugis submitted to him, together with information as toits chemical identity, such pharmacological data asare available and the reason for interest in thecompound. He codes the compound and forwardsit to the pharmacology laboratory of the University
of Michigan Medical School under code number,suggesting a starting dose based upon the pharma-cological data. When the tests have been completedthe results are reported to the Executive Secretary,who transmits a copy to the producer and uponmutual agreement reveals the nature of the agentto the investigators. The results may be the deter-mining factor either in the abandonment of interestin the compound, should its physical dependencecapacity be high without compensating advantages,or in the decision to subject it to further laboratoryand clinical testing, including addiction liabilitytesting in man. In some unequivocal cases the testsin the monkey may also be the basis for a recom-mendation for narcotics control.
TESTS FOR ADDICTION (ABUSE) LIABtLITYIN FORMER ADDICTrS "
Given a new substance whose morphine-likeproperties and addiction liability are to be deter-mined, the investigators at the Addiction ResearchCenter at Lexington must assume responsibilitywith respect to the risks involved in carrying outtests in man. Accordingly, they have indicated that,prior to the initiation of tests, they wish to besupplied with information upon the general pharma-cology of the compound, including its toxicity andrelative potency, evidence that it has been admini-stered to man and that it may be a useful thera-peutic agent, its relative potency in man and someindication of the side-effects which it may produce.They request that the data on the general pharma-cology of the compound include information onacute and chronic toxicity, on relative potency withrespect to analgesic, antitussive and/or constipatingaction, on whether or not the actions of the drug areantagonized by one of the specific antagonists suchas nalorphine, on the rate and extent of dosageincrease in chronic administration in attempteddetermination of tolerance, on whether or nottolerance develops and cross-tolerance to morphinefor example, and on physical dependence capacityin monkeys and acute tolerance and physical de-pendence development in dogs. All such informa-tion is pertinent to the establishment of dosageschedules and to the safety of investigation of theagent in man.
1 We are indebted to Dr Harris Isbell, Director, toDr H. F. Fraser, Associate Director, and to their associatesat the Addiction Research Center for permission to describetheir methods, of which not all details have been publishedpreviously.

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
The subjects in the studies at Lexington are formeropiate addicts, male, coloured or white, in goodphysical condition, who are serving a sentence forviolation of the narcotic laws and who have volun-teered for the experiment.
Single-dose administration for the determination ofmorphine-like (euphorigenic) effectsStarting with small doses-their actual size is
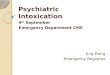
based upon previous experience with the drug-a new agent is administered by various routes,depending upon its solubility and other physicalproperties. The dose is then increased, two or threemen being given the drug at each dose level, until adefinite effect is obtained or signs indicative of im-pending toxicity are seen. Up to this point admini-stration is on a single-blind basis, the nature of thedrug being unknown only to the patient, who is,however, allowed to express his feelings about it incomparison with his previous drug experience. Anidea of relative potency thus having been arrived at,the next step is administration on a double-blindbasis, identity of drug and dose being unknown toboth patient and immediate observers. Two doselevels of the new agent are given at weekly intervalsin random order with two comparable doses of astandard of similar potency and a placebo ascontrols to a group of eight to twelve individuals.Administrations are continued until each individualin the group has reccived each of the medications.Certain objective measurements may be made beforeand at intervals after each dose, such as pupil size,respiratory rate and minute volume, blood pressureand body temperature, and both the patient and theobserver are required to fill out a " Single-doseattitude questionnaire" (see Annexes 1 and 2).It will be noted that both the subject and the observerare asked to check whether the agent seems to be anopiate (" dope ") or is like some other drug, thedegree of the patient's liking for the drug and thefrequency of opiate-like symptoms. The mean ofthe group for all observations with each medicationis determined and plotted for comparison with thestandard and the placebo. The results obtained in atypical experiment are illustrated in Fig. 3. Bothpatients and observers agreed very well in theirevaluation of the drugs and the frequency of opiate-like symptoms paralleled changes in pupillarydiameter.
Substitution for morphineFormerly a single dose of the agent under investi-
gation was given to individuals stabilized on mor-
phine, approximately 240 mg per day. The dosewas given 30 hours after abrupt discontinuance ofmorphine, when the withdrawal syndrome wasreaching its peak. The subsequent course of absti-nence intensity was compared with that to beexpected in otherwise untreated individuals. Amore adequate procedure has since been deviseda procedure that can be repeated on the sameindividual at weekly intervals because the abstinencesyndrome is never allowed to reach a seriouslydisturbing intensity. Thus double-blind cross-overobservations can be made comparing, in the sameindividual, one or more dose levels of one ormore experimental agents, a placebo and a stan-dard dose of morphine (Fraser & Isbell, 1960a,1960b).A group of 5-12 individuals is given morphine
subcutaneously regularly, the dose being built uprapidly to 240 mg per day and stabilized at that levelfor not less than 30 days. Beginning with the eveningdose (10 p.m.) and continuing through 24 hours acoded substance (experimental drug, placebo orstandard morphine dose given as an unknown) isadministered in place of the regular morphine doses.Beginning the next morning, 14 hours after the lastregular dose of morphine, observations are made atregular intervals, recorded and evaluated accordingto the Himmelsbach (1939) hourly score for abstin-ence phenomena (Table 1). The substitution pro-cedure is repeated at weekly intervals until eachindividual has received in random order at least onedose level of the experimental drug, a saline injectionas a placebo, the regular stabilization dose of mor-phine and perhaps one or more dose levels of oneor more other agents. The mean hourly Himmels-bach score for all patients for each agent is plottedand a comparison is made between the experimentalagent and morphine or placebo. If the drug isineffective as a morphine substitute, the graph ofabstinence phenomena intensity will coincide withthat obtained after the administration of a placebo.If it is morphine-like in some degree, the graph ofabstinence phenomena observed will approximateto that obtained after continuation of morphine as anunknown during the substitution period or will fallbetween the placebo and morphine graphs, depend-ing upon the effectiveness of the dose used as amorphine substitute (see Fig. 4). A more directand perhaps simpler comparison is obtained bysumming for each agent for each individual thehourly point scores and calculating the mean totalabstinence score for 24 hours (TAS-24). This score
2
151

H. HALBACH & N. B. EDDY
FIG. 3RESULTS OF SINGLE-DOSE ATTITUDE QUESTIONNAIRES, FILLED OUT BY PATIENTS AND OBSERVERS, AND DECREASEIN PUPILLARY DIAMETER AFTER SINGLE DOSES OF DIPHENOXYLATE (70 mg), CODEINE (140 mg) AND A PLACEBO a
.30 - oo-o_e-.1.2
.25 /P/0 0LtC D Mt >.25 T A ^ A *2 = +-o----LRS=io.2±2.62
1.5 _ 1L-.0 _/
m ~~~~~DIPHENOXYLATE WUWL TRS 2.4±1.13B: 0Ln.20 0 u .8
z~~~~~~~~~~.1- CODEINE
.-DEIN T.6= 1 .5t 2 5
0 TRS -1.9±1.23 u
I S~~~~~~~~~~~~~~0APLACEBO
.05 PLACEBO .2 AATRS=1.0±0.27
/TRS=0.0
1.75 -OPIATE SYMPTOMS DECREASE IN PUPILLARY DIAMETER
1.50 --3.0
/ D~~~IPHENOXYLATETRS= 13.6±3.61,1.25 5-2.5
ui ~ /E DIPHENOXYLATE
'n 1.00 *Z -2.0
CODEINE S>.75 ~TRS 15.2+3.28 15
CODE I
u 0 TRS 18.9±+ 3.32
.25 PLACEBO TRS 1.10.30 ..5 PLACEBO
~T -7 .7 .0
~~~~~~~~~~A /II
2 4 6 8 10 12 14 2 4 6 8 10 12 14
HOURS AFTER DRUG
WhO 2363
a The maximum number of positive answers hourly for identification as "dope" = 1.0; for positive attitude (liking) score = 4.0;and for frequency of opiate symptoms = 7.0. Each point on each curve represents the average of data obtained on 8 men, each ofwhom had diphenoxylate and codeine three times and the placebo once. The TRS values (total response scores for 14 hours) repre-sent the mean of the areas under the curves ± standard errors.
After Fraser & Isbell (1960c).
will be high (150 or more) for placebo substitutionand low (50 or less) for morphine continuation.
In many instances, especially if the 24-hoursubstitution does not completely suppress theappearance of abstinence phenomena, substitu-tion may be continued for 10 days. Individuals are
stabilized on morphine and substitution is begun as
in the 24-hour experiment. An attempt is made tosubstitute the new drug at such a dose and intervalof administration as to maintain the addiction; thatis, to prevent completely the appearance of abstin-ence phenomena which would have occurred as aresult of the cessation of morphine administration.Whether or not this is attained, one gets an impres-
POSITIVE ATTITUDE SCORE
152

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
FIG. 424-HOUR SUBSTITUTION OF PROPOXYPHENE FOR
MORPHINE a !~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~30
25 _
L)uzw L 20
X 5Oz 10V) Dz IL
Z 10
14 15 16 17 18 19 20 21 22 23 24HOURS OF ABSTINENCE
5
wHO 2361
a The total dose of propoxyphene was 2400 mg, given orallyin six doses of 400 mg each. In control experiments, using thesame subjects and the same schedule, placebo capsules orinjections of morphine were given. The subjects were told onlythat other drugs were being tested. Each point on the placeboand propoxyphene curves represents the average scores on thesame 11 subjects; each point on the morphine curve representsthe average score of 9 of these subjects. P signifies that thepoint Is significantly different from the corresponding point forthe placebo, and M that the point is significantly different fromthe corresponding point for morphine, indicating some sup-pressive effect on abstinence from morphine.
Reproduced, by permission, from Fraser & Isbell (1960a).
sion of the individual's satisfaction with the substi-tute. At the end of 10 days the substituted drug isreplaced by placebo, the change not being revealedto either patient or observer. Throughout the 10 daysof substitution and for a week of withdrawal (pla-cebo admpinistration), observations are made daily forsigns of abstinence and evaluated according to theKolb & Himmelsbach (1938) daily point score
(Table 1). The score during the withdrawal period iscompared with the abstinence syndrome after abruptwithdrawal of morphine, affording a qualitative andquantitative appraisal of the withdrawal symptomsafter the substituted drug.
It is possible to re-stabilize the individual on
morphine and subsequently to withdraw him abruptlyfor a comparative appraisal of his morphine absti-nence intensity; or, after re-stabilization, a second
10-day substitution with another agent can be carriedout if a direct comparison of two new agents in thesame individual is desired.
Direct addiction
If previous experience has shown a compound tobe significantly more or less effective than morphine,if it is a new chemical type, and particularly if itsintroduction into clinical practice is contemplated,a direct addiction experiment may be undertaken.Individuals previously addicted to morphine or arelated drug and free of drugs for some months aregiven the new agent regularly at an interval and doseand by a route deemed appropriate according toprevious experience. The dose is increased asrapidly as possible, avoiding, of course, cumulativeeffects and toxic reactions. The objective is toincrease the dose, if possible, by a schedule parallel-ing that leading to stabilization on morphine in theexperiments already described. The direct addictionattempt may be continued for 30, 60, or 90 daysor longer, and is followed by abrupt withdrawal;a comparison is then made with similar periodsof administration and withdrawal of morphine.During the latter part of such direct addictions, afew days before withdrawal, patients are challengedby administration of a small dose (3, 5 or 10 mg)of nalorphine. If signs of abstinence are preci-pitated by nalorphine, these are compared with thewithdrawal syndrome observed subsequently.
Recently a modification of the above procedurehas been tried, shortening the addiction period andaffording cross-over data on the same individuals(Fraser & Isbell, 1960b; Fraser et al., 1961b). Eightdrug-free former addicts were selected and to eachwas assigned in random order a coded medicationto be administered on a double-blind basis in as-cending dosage for a period of 18 or 19 days. Themedications were placebo capsules, morphinecapsules, codeine capsules, morphine for subcuta-neous injection and four experimental drugs, one incapsule form, the others for subcutaneous adminis-tration. The initial dosage (except of the placebo,of course) was usually that judged to be equivalentin effectiveness to morphine on the basis of 24-hoursubstitution; it was, however, sometimes less than theequivalent in order to avoid toxic reactions (Fraser etal., 1961b, p. 378, footnote 1). Since no difficulty isexperienced usually in increasing morphine dosagein former addicts to 240 mg a day in 18 days, sucha regimen of administration of morphine wasemployed and a schedule of increasing dosage for
m
o- -o 0P P
0 00 0MORPHINE
V 4,
153

H. HALBACH & N. B. EDDY
all other drugs was arranged which would parallelthat for morphine. Since tolerance to new agentsmay or may not develop as rapidly as tolerance tomorphine, patients were watched for depth of seda-tion and toxic reactions and the increasing dosageschedule was halted or modified as necessary.On the 19th or 20th day, the exact time being
known to the person preparing the drugs, but not tothe patient or the observer, a placebo (capsule orinjection according to which the patient had beenreceiving) was substituted and continued on thesame schedule for 10 days. Then each individual wasstarted on another of the series of medications, againassigned in random order, and the whole procedurewas repeated until each individual had received eachof the eight preparations.Throughout drug administration and placebo
substitution, the following observations were madethree times daily; rectal temperature, respiratoryrate, pulse rate, blood pressure and the usualobservations for abstinence signs according to theKolb & Himmelsbach scoring system. Caloricintake was measured daily; body-weight was re-corded each morning, and hours of sleep, hoursof inactivity (lying horizontally on bed, whether ornot asleep) and hours of initiative activity (off theward in various voluntary pursuits) were recordedat half-hour intervals daily. For each withdrawalperiod a total abstinence score for 10 days (TAS-10)was calculated. These scores for all drugs indivi-dually and as means for all patients were comparedwith the scores for placebo and all other drugs werecompared similarly with morphine and with eachother.At 7 p.m. on each day of the experiment each
patient completed a questionnaire dealing with thesubjective effects of the drug he was receiving, andconcurrently a separate questionnaire dealing withthe behavioural changes was completed by theobserver (see Annexes 3 and 4). These recorded suchthings as recognition of the drug as an opiate, thepatient's liking for it and inclination towards con-tinuation of its use, and judgement of its strength.The results of this experiment as revealed by the
chronic dosage attitude questionnaires are shown inFig. 5. All ratings of patients and observers weretabulated, but the figure is restricted to the para-meters: identified as " dope ", estimate of " strength,"and " would like to take drug daily ". The datawere analysed for statistical differences betweendrugs by the paired " t" test, using total responsesfor the first 18 days on each drug and a placebo.
An alternative short direct addiction test has beenemployed by Fraser and his associates which isespecially applicable to the evaluation of intra-venously administered drugs (Fraser et al., 1961a).A typical experiment employing this technique isdescribed as follows: In a single-blind study sixsubjects received drugs intravenously and onesubcutaneously becau;e all of his superficial veinswere sclerosed. A " sample " of a high dose of eachdrug was given at 3-day intervals-180 mg ofI-K-l (1-(p-chlorophenethyl-6,7-dimethoxy 2-methyl-1 ,2,3,4-tetrahydroisoquinoline), 180mg ofd-propoxy-phene, 120 mg of codeine and 30 mg of morphine-in randomized order. Each patient rated eachof these drugs on the single-dose attitude question-naire (see Annex 1) and after each had receivedall four sample doses he was asked to reviewhis response to each on the questionnaire and torate them in order of preference, 1 to 4. In this pre-ferential ballot morphine ranked first, d-propoxy-phene second, and codeine and I-K-1 equal and last.
It was explained to each subject that he wouldthen receive, in randomized order, all the sampledrugs which he elected to take in increasing dosesfor seven days, with a withdrawal period of threedays between each drug phase. However, after hisrating of the single doses, a subject could elect notto take any of them during the seven-day phase, totake one or more of them, or after starting anyparticular drug to stop at any time during the sevendays, go on to the next drug or discontinue entirelywithout penalty. At the end each subject was askedagain to rate the drugs in order of preference.The daily amounts of the drugs were as follows:
for I-K-1 and d-propoxyphene, 360 mg (divided intothree equal doses) on the first and second days and480, 600, 600, 720 and 720 mg (divided into fourequal doses) on the third to seventh days; for mor-phine, 60, 60, 80, 100, 100, 120 and 120 mg (dividedinto four equal doses); and for codeine, 240, 240,320, 400, 400, 480 and 480 mg (divided irnto fourequal doses). All drugs were administered intra-venously (with the one exception noted above)slowly over a 2-minute interval. Nalorphine (3 mg)or a placebo, on a randomized double-blind basis,was injected subcutaneously at 9 a.m., that is, threehours after the last dose of an experimental drug,on the sixth or seventh day of the test. Observationsfor abstinence signs were made also on the three daysbetween drug administrations.Morphine was definitely the preferred drug in
this series; it was taken by all the subjects, one dis-
154

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE 155
FIG. 5RESULTS OF CHRONIC DOSAGE ATTITUDE QUESTIONNAIRES: COMPARISON OF RATINGS OF PATIENTS ANDOBSERVERS IN A SHORT-TERM ADDICTION TEST (18-19 DAYS) INVOLVING SEVEN DRUGS AND A PLACEBO a
IDENTIFIED AS 0 DOPE OR OPIATESP A P A P A P A P A P A P A P A
°0oc 7 U U0~~~~~~
2 0 4 ~~~~~~~~~~~~~~~~~~~~c0hiK
IL w- 4 0
25 = e on m
0
hi o~~~~~~~~~~~~~~ NO2D
0 U) - u DONrT CARE2 hi~ ~~ ~~~~4d4 X t EYES
0 2 4 o
lO'~~~ 0 0 hiusi N hi .0
z ~ ~ ~ 2IP PATIENTS00 m"~~imr AsAIDES
0 -
WOULD LIKE TO TAKE DAILY"w0PA P A P A P A P A P A P A P A
taI0 75 u az 0~~K
Z- hi .4 -'")'z CL Z CY 0~~~~~~~'.",
wo m -Ob x b
9.)O* 0a A significant difference (P<0.05) between morphine subcutaneously and the other drugs, Including the placebo, Is shown by
the symbol"1 m ",between codeine orally and the other drugs by the symbol"1 c ", and between the placebo orally and the other drugsby the symbol p"p
R 1132 = diphenoxylate ; 7296A = d-3-methoxy-N-phenethylmorphinan.Reproduced, by permission, from Fraser et al. (1961 b).
continuing it, however, on the second day because ofnausea. d-Propoxyphene was taken by all thesubjects and by two of them for the whole period ofseven days; the average duration of administrationfor all subjects was 5.3 days. Even though five menidentified the drug as " dope ", five discontinuedd-propoxyphene for such reasons as pain at the siteof injection, nausea, loss of appetite, dizziness andnervousness. One patient took d-propoxypheneintravenously for seven days, but his veins becameprogressively occluded; successive injections of thehigher doses had to be given in different veins andas much as 45 minutes was spent locating a suitablevein. As to codeine, two patients elected not to
start the 7-day course of addiction and only threecompleted the course. Those taking codeine intra-venously complained that all they felt was a tem-porary pins-and-needles sensation. Although allthe subjects elected to take I-K-1 for the seven days,it was feasible to administer it to only two subjects(for 2.5 and 6.3 days, respectively) because it inducedsevere phlebitis and venous thrombosis. All pa-tients complained that with I-K-1 morphine-likeeffects were absent or very weak and there was painat the site of injection.
This short-term direct addiction technique has thefollowing advantages: The programme is less rigidin design than in the original long-term technique

H. HALBACH & N. B. EDDY
and permits the former addicts to make electionsamong drugs and on how long they wish to take anagent before trying another. Furthermore, as indi-cated above, it brings out rapidly differences amongdrugs respecting the quality of the subjective effectsand characteristics of a drug which determine itssuitability for intravenous administration-for ex-ample, its solubility and its local irritant and/orthrombotic properties. The primary deficiency ofthe method is that it does not evaluate adequatelythe degree of physical dependence. It does, however,give valuable information on the subject's immediatelike or dislike of a drug by his usually preferred routeof administration and, hence, on whether or not hewould be inclined to use it thus if it were availableto him.
TESTS FOR THE DEVELOPMENT OF TOLERANCE ANDPHYSICAL DEPENDENCE UNDER CLINICAL CONDITIONS
A direct attack upon the question of addictionliability in clinical practice was initiated about25 years ago under the auspices of the Commit-tee on Drug Addiction of the National ResearchCouncil (USA). Selected subjects with chronicpain were given morphine or another comparableanalgesic in an amount and at an interval justsufficient to control their pain. At 2- or 3-weekintervals the analgesic was withheld for a period upto 24 hours and careful hour-by-hour observationswere made for the appearance of abstinence pheno-mena. Recurrence of pain was the major difficultyand often made the period of withdrawal so shortthat no signs of abstinence could be expected (Eddy& Himmelsbach, 1936; Lee, 1942).The production of morphine antagonists, as
mentioned earlier, has made possible a new line ofattack. Wikler, Fraser & Isbell (1953) showed thatnalorphine would precipitate abstinence phenomenain subjects who had received 15-30 mg of morphinefour times daily for 3-7 days, or 10 mg of methadonefour times daily for 2-5 days, or 15 mg of heroinfour times daily for 2 days. Later.in the addictionperiod with any one of these drugs, the same dose ofnalorphine precipitated a more intense abstinencesyndrome. Indeed, later during continued metha-done administration, nalorphine precipitated absti-nence signs which exceeded in severity those whichensued after abrupt withdrawal of morphine follow-ing long periods of addiction to high doses of thatdrug. These observations implied that physicaldependence on morphine-like substances began to
develop very early, perhaps even with the first dose,and increased in intensity with continued adminis-tration. However, the results with methadoneindicated that the intensity of abstinence signs pre-cipitated by nalorphine was not necessarily a basisfor the prediction of the intensity of abstinence whichwould follow abrupt withdrawal, since withdrawalof methadone was followed by a slowly developingand relatively mild abstinence syndrome (Isbell etal., 1947). Nevertheless, if morphine or anothermorphine-like analgesic were given for chronic painand if nalorphine (or another specific antagonist)were given periodically during such administrationin fixed amount and in fixed relation to the last doseof the analgesic, followed by observation for charac-teristic abstinence symptoms, the appearance andintensity of such symptoms could be a measure of thetime required for, or the rate of development of,physical dependence. The procedure should beapplicable to any form of chronic administration.
Parenteral administration of potentially addictingagents
From a population of patients with inoperablecancer individuals are selected who have persistentpain of an intensity to warrant the application of anopiate. Their histories are scanned to select thosewith little previous narcotic experience and eachpatient is screened by an initial " allyl test" to ruleout already existing detectable physical dependence.A suitable patient is started on subcutaneousadministration of the medication, coded to providedouble-blind conditions. The patient remains on thatmedication throughout the study, other analgesicsbeing avoided entirely and, so far as possible, othersedatives. The initial dose is that determined pre-viously to be equivalent to 10 mg of morphine per60 kg of body-weight, but it is adjusted if necessaryby 10% increments within the first few days toprovide adequate relief in the individual patient.Repetition of the dose is based on the demand of thepatient because of the return of pain. The dose isincreased only as necessary to maintain adequaterelief. As a check on the adequacy of pain relief,with the first dose of coded medication and with asingle dose at weekly intervals, a careful record iskept of the degree of pain before and at hourlyintervals after medication. (See Eddy & Lee, 1959.)While the coded medication is continued, a record
is kept of the individual dose and the total amountof narcotic administered per day. From this recordand the weekly pain-relief scores a judgement is
156

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
made regarding the development of tolerance to theanalgesic effect of the drug. One must bear in mindthat advancing disease in these mainly terminalcases may cause some increase in pain, and in con-
sequence some increase in narcotic consumptionindependently of tolerance development.
Estimation of the development of physical de-pendence is based upon the periodic administrationof nalorphine, the " allyl test ". This test is per-
formed before coded medication is started andevery two weeks thereafter. In the alternate weeksa " placebo test " is carried out in like manner,
saline solution being injected in place of nalorphine.In each instance the test is begun two hours after a
dose of narcotic. Blood pressure, rectal temperature,respiratory rate and pupil size are determined andimmediately afterwards 1.0 mg of nalorphine hydro-chloride (or 0.5 ml of saline solution for the placebotest) is injected subcutaneously. At 5-minuteintervals up to 20 minutes blood pressure, tempera-ture, respiratory rate and pupil size are re-determinedand simultaneously the patient is observed for othercharacteristic abstinence signs. Unless the symptomsobserved are strikingly characteristic or severelydisturbing to the patient, 2.0 mg of nalorphinehydrochloride is injected 25 minutes after the firstdose and the observations are continued for at leastanother 20 minutes. Alternatively, each allyl testmay be performed with the administration of a
single dose of 3.0 mg of nalorphine hydrochloride.The decision to employ one or two doses of nalor-phine should be made initially and the procedureremain the same for all patients of a study group.
The signs looked for in each test and the numericalvalues assigned to them, both modified slightlyfrom the Himmelsbach hourly scoring system, areshown in Table 2. A limit of 10 points is set forchanges in systolic blood pressure but no limit foran increase in respiration or rise in temperature.The difference scored for blood pressure, respirationand temperature is the maximum observed after a
dose of nalorphine compared with the value beforeany nalorphine is given. The pupil size may bedetermined by comparison with a series of dotsdiffering one from another by 0.5 mm in diameteror, preferably, by photographing the pupil. A score
of 15 (the sum of the values for all signs observed)is judged to be significantly indicative of the presence
of physical dependence, provided that the score iscontributed to by some sign in addition to changesin blood pressure and respiratory rate. This condi-tion or restriction is necessary because lability of
TABLE 2
CRITERIA FOR PHYSICAL DEPENDENCE, AS USED IN THECLINICAL TEST FOR THE DEVELOPMENT OF TOLERANCE
AND PHYSICAL DEPENDENCE
Abstinence signs Symbol Numerical value
Systolic blood pressure BP 1 point for each 2 mm Hgmaximal rise, total not toexceed 10 points
Rectal temperature T I point for each 0.1°C rise
Respiratory rate R 1 point for each resp./min.increase
Yawning Y I point
Lacrimation La I point
Rhinorrhoea Rh 1 point
Sweating S 1 point
Gooseflesh G 3 points
Mydriasis My 3 points
Tremor Tr 3 points
Restlessness Re 5 points
Abdominal or othercramps C 5 points
Urge to defaecate D 5 points
Nausea Na 3 points
Emesis V 5 points for each act ofemesis
After Eddy, Lee & Harris (1959).
blood pressure and respiration may occasionally,under the conditions of the unusual procedure ofthe allyl test, produce wide non-specific fluctuations.In all cases a positive allyl test should be confirmedby another test giving the same or a greater score,two weeks or more later, before a definite con-clusion of physical dependence is reached.
Eddy, Lee & Harris (1959) have reported on theapplication of the procedures just described to astudy of addiction under clinical conditions. Theyhave, by this method, compared oxymorphone andanileridine with morphine and currently some otherold and new drugs are being compared in the sameway.
Schrappe and his associates (1959), believing thatthe Himmelsbach scoring system did not give anadequate quantitative representation of abstinencephenomena, have devised an alternative classifica-tion. They separate the abstinence signs into twogroups, specific and non-specific, as shown in thetabulation below:
157

H. HALBACH & N. B. EDDY
Abstinence symptoms of the first order (specific)
1. Shivering, feeling of cold, gooseflesh.2. Yawning, sneezing, cough, hiccup.3. Feeling of warmth, profuse sweating.4. Rhinorrhoea, lacrimnation, salivation.5. Diarrhoea.6. Colic, increased peristalsis, borborygmus, urge to
defaecate.7. Retching and vomiting.8. Extreme mydriasis (widening of the pupil by 3 mm
or more).9. Automatic movements, severe anxious turning,
psychomotor unrest.10. Muscular discomfort and pain.11. Burning sensations.
Abstinence symptoms of the second order (non-specific)1. Increase in body temperature of 0.3°C or more.2. Increase in respiratory frequency of three per minute
or more.3. Mydriasis (widening of the pupil by only 1 or 2 mm).4. Increase of systolic blood pressure of 10 mm or
more.5. Anxiety, inner unrest.6. Nausea.7. Headache, heart pain, palpitation, faintness.
Each of the non-specific signs is given a value ofone point; the specific signs are given a cumulativevalue based on 10 for the first to be observed. Theemphasis on the various abstinence phenomenadiffers in the Schrappe and Himmelsbach systemsand the former does not use a simple summation toarrive at the total abstinence score. Schrappe andhis associates used successive doses of nalorphine toprecipitate abstinence signs during continuingnarcotic administration and compared the syndromesthus produced with those occurring spontaneouslyafter abrupt withdrawal of morphine or methadone.
Oral administration of analgesic mixtures
Himmelsbach et al. (1940) showed that codeineadministered either subcutaneously or orally sup-ported previously established physical dependenceto morphine. Himmelsbach reviewed the literatureon addiction to codeine, cases of which continue toappear occasionally. Even the oral preparations ofcodeine of relatively low concentration are subjectto some abuse, and abuse of dihydrocodeinone oralpreparations is comparatively common (UnitedStates Bureau of Narcotics-personal communica-tion, 1960). However, specific information on the
degree and rate of development of physical depen-dence with oral administration of analgesic mixturesis only now being sought by a technique adaptedfrom that described above for parenteral administra-tion of analgesics. For the first report on this work,see Cass and associates (1961). The following is adescription of the procedure as modified for a con-tinuation of the study of this problem.
Hospitalized patients are selected for the studywho have persistent mild to moderate pain of adegree that warrants and is generally relieved by anoral analgesic mixture such as codeine plus APC(codeine phosphate 32.5 mg, aspirin 227.5 mg,acetophenetidin 162.5 mg, caffeine 32.5 mg) or itsequivalent. Background information is entered on aspecial record sheet (see Annex 5) and the patientbegins a control period of eight days, during whichhis analgesic medication, whatever it was previously,is changed to five grains of aspirin three cr four timesa day. A record sheet (see Annex 6) is filled out foreach of the control days to provide a baseline forthe degree of relief afforded by aspirin, the patient'sdaily complaints, etc. Also during this period ascreening allyl test is carried out and, if this test isnegative, the patient is assigned to a drug group.The assignment is based on the background informa-tion and the data obtained on the control days and isintended to make the several drug groups as homo-geneous as possible, since a number of drug mixtureswill be compared. The objective will be drug groupseach comprising about 25 persons, half males andhalf females. The medication is supplied in capsules,under code number, of course, to make the studydouble-blind, and is administered on a routine four-times-a-day schedule to those patients who getadequate pain relief on such a schedule and on apatient demand (p.r.n.) schedule to all others. Inthe latter group, the number of capsules per dose,the interval between doses and the total number ofcapsules per day are adjusted to the patient's needor demand, thus further simulating usual clinicalconditions and allowing psychic dependence andtolerance, if they develop, to play their roles intotal drug consumption. The medication for aparticular patient remains the same, but the code ischanged with the consumption of each 100 dosageunits. A record is kept for each patient each day(see Annex 7), showing total medication (number andtime of administration of dose units taken), whetherpain was present or absent at three interviewsduring the day, and patient's complaints (side-effects), if any.
158

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
To check for the development of physical de-pendence an allyl test (nalorphine hydrochloride,3 mg subcutaneously) will be carried out once amonth, also on a double-blind basis. To effect this,nalorphine and saline solution are provided inidentically appearing ampoules, each ampoulecarrying a different code number, and tests arecarried out on successive days using two codedampoules, one of which contains nalorphine andthe other saline. The tests are carried out as des-cribed in the section on parenteral administrationand the data are recorded (see Annex 8) and evalu-ated by the modified Himmelsbach score (Table 2).The daily record sheets and the allyl or placebo
test results are reviewed by a person not directlyassociated with the patients, so that the narcoticmedication can be stopped and a withdrawal periodinstituted, by substitution of APC capsules undercode number for the specific analgesic mixture, assoon as a significant degree of physical dependenceis demonstrated. During this withdrawal periodobservations will be made three times a day for thefirst three days and then daily through ten days forthe spontaneous appearance of withdrawal signs,according to the Kolb & Himmelsbach daily scoringsystem (Table 1).
In the initial study by Cass and his associates,results were reported on 63 patients who receivedtheir medication on a rigid four-times-a-day sche-dule. The drugs employed were codeine plus APC,ethoheptazine plus aspirin, oxycodone plus a modi-fied APC, and dextropropoxyphene. The experimentwas terminated in each case after not more than90 days of specific medication followed by a 10-daywithdrawal period. The authors said:" On periodic administration of Nalline (nalorphine),some signs of addiction were demonstrated with allproducts, but these symptoms were neither consistent,progressive or clear-cut. Upon withdrawal, some symp-toms suggestive at least of physical dependence wereobserved with all drugs except ethoheptazine. All fourdrugs demonstrated analgesic effectiveness."
In the current continuation of the study themedications are APC alone, codeine phosphate plusAPC, methadone hydrochloride plus APC, andlevorphanol tartrate plus APC. These were deli-berately selected on the basis of previous experienceto provide a range in the development of physicaldependence as a background for inclusion in thestudy later of new substances, concerning whichnothing is known of their addictiveness whenadministered orally under clinical conditions.
TESTS FOR DETECTION OF DRUG USE AND RECIDIVISM
The diagnosis of addiction or of return to drugsby an individual who has undergone treatment orincarceration for violation of the narcotic laws isnot easy in the absence of definite signs of abstinence.This problem has been discussed at length in areport, entitled " What to do with a drug addict? ",by Isbell (1952) to the Council on Pharmacy andChemistry of the American Medical Association.The report points out that there are no pathogno-monic physical signs of addiction and commentson various aspects of the situation and devicesemployed by addicts that need to be borne inmind if one is not to be misled. Since complete orpartial tolerance to many of the effects of morphineand allied drugs develops during the course ofaddiction, addicts will not show the same effects asmight be expected in persons not addicted. Constric-tion of the pupil and signs of sedation are not likelyto appear unless a dose of the addicting drug hasbeen received recently. Superficially tolerant addictswill appear to be physically and mentally normalunless they have been without drugs for some timeand signs of abstinence are beginning to appear.The most important findings are the presence ofold and recent needle marks. These should be soughtover the veins in the antecubital spaces, the deltoidregion, the abdomen, the anterior surfaces of thethighs and along the veins of the legs and hands.Long scars or tattooing over superficial veins isextremely suggestive, especially if fresh needle marksare present. Also suggestive are multiple abscessesor old abscess scars. Addicts using either pethidineor methadone are likely to have induration andinflammation of large areas of the skin, particularlyover the deltoid region and the anterior surface ofthe thigh. An important feature may be that nophysical findings are present which satisfactorilyexplain the serious symptoms detailed by the pa-tient. A complete physical examination as part ofthe diagnostic procedure is imperative.A definitive diagnosis of addiction to morphine or
similar drugs depends upon the demonstration ofthe characteristic signs of abstinence following com-plete and abrupt withdrawal of drugs. To prove thepresence of physical dependence, the addict must beisolated in an environment so well controlled thatthere is no possibility of his obtaining any narcoticdrugs other than those prescribed. If such an en-vironment is available, isolation of the addict andwithholding of all narcotics will prove the presenceor absence of dependence on these drugs. Detection
159

1H.: HALBACH & N. B. EDDY
requires, of course, familiarity with the signs ofabstinence and at best the procedure is prolongedand difficult for patient, physician and attendants.The precipitation of an abstinence syndrome bynalorphine or another specific opiate antagonist andthe utility of such a procedure in experimentalclinical designs have been described above. Asearly as the report to the Council that has beenquoted above, the possibility of the use of nalor-phine for diagnosis was suggested and a little laterits use for this purpose was described more explicitly(Isbell, 1953). As mentioned later, however, thereare certain basic requirements for the safety andinterpretation of this test.When these requirements have been met, a 3-mg
dose of nalorphine is given subcutaneously. Ifsigns of abstinence have not appeared in 20 minutes,an additional 5-mg dose is given and, if a definiteabstinence syndrome does not appear after 20 moreminutes, a final dose of 8 mg is administered. Ifabstinence has not become evident within 20 minutesafter the final injection, the patient is not addictedand can be released after the direct effects of nalor-phine have worn off, usually in less than six hours.If signs of abstinence appear after any of the doses ofnalorphine the individual has been taking morphineor an allied drug at sufficiently short intervals and insufficient amounts to produce physical dependence,and therefore is addicted. Obviously this method ofdiagnosing addiction requires familiarity with thesigns and symptoms of nalorphine-induced abstin-ence. Within two or three minutes after the adminis-tration of nalorphine an addicted person experiencesa sensation of heat in the back or abdomen spreadingover the body. There follow abdominal cramps andfrequently defaecation. The patient becomes appre-hensive and restless, perspires profusely and yawnsfrequently. Lacrimation and rhinorrhoea appearand increase in degree. The patient complains ofchilly sensations and recurring waves of goosefleshare observed. Vomiting is likely to occur. Thepatient may become quite hostile and antagonistic.Respiratory rate and minute volume increase andthe blood pressure is sharply elevated. The pupilsare dilated. These symptoms constitute a full-blown abstinence syndrome, which may begin infive minutes, reach peak intensity in 20, start todecline in 60 minutes and disappear after threehours. The symptoms are relieved, but not easily,by the administration of morphine.A negative nalorphine test does not exclude the
possibility that the person has been taking occa-
sional doses of narcotics, nor does it prove that hewas not actively addicted a week before the test wasdone. A positive test, as just described, can have butone meaning. However, efforts have been made touse a much milder reaction, even dilatation of thepupil alone, as presumptive evidence of the use ofnarcotics and this aspect of the procedure requiresfurther discussion.
Terry & Braumoeller (1956) reported upon theuse of nalorphine for the detection of addiction,relying upon changes in pupil size for a definitiveresult. They mentioned other withdrawal symptoms,but said:" The observation of gross withdrawal symptoms shouldnot be depended upon for a diagnosis but should beavoided if possible. To some degree patients themselvescan control withdrawal symptoms. The pupillary res-ponse alone is an accurate, sufficient, and sensitive indexof narcotic addiction or of occasional use, or of theabsence of narcotics."
The authors reported upon the use of the nalor-phine test in 454 patients suspected of taking anopiate. They used a single dose of 3 mg. A card withblack dots was used to measure the size of the pupil,the authors believing this to be accurate to 0.5 mmof diameter. According to the authors' interpreta-tion," If the person tested has not been using opiates thediameter of the pupil is reduced by 0.5 mm. In a personwho has been using opiates occasionally but who is notaddicted, the pupils will remain unchanged in size. In aperson who is addicted the diameter of the pupils willincrease by from 0.5 to 2 mm, the amount of increasedepending upon the degree of addiction."
Other localities in the USA have been employingthe nalorphine test for the detection of addictionand in some it has been made a condition of proba-tion that the individual report periodically for sucha test to determine whether or not there has beena return to drugs. It is now generally believed thatthe dose of nalorphine in these tests should notexceed 3 mg, but there is not general agreement onthe reliance to be placed on pupillary changes aloneor on the desirability or necessity for other evidence.There is a strong feeling that a positive finding-definite pupillary dilatation-could be used as apresumptive basis for holding an individual, butthat confirmation of such results should be soughtby immediate urinalysis. Urinalysis should be donein the cases showing equivocal results (slight dilata-tion or no change in pupil size) after nalorphine.Such analysis is cumbersome and time-consuming
160

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
and attention is being given to simplification.Cochin & Daly (1962), for example, have describeda method employing thin-layer chromatography thatis rapid and accurate in its differentiation of opiatesin the urine and attention is being given to theapplication of gas chromatography to this problem.The proponents of the nalorphine test for detecting
drug addiction and relapse are strongly of theopinion that it is a deterrent to relapse where it hasbeen used as a condition of probation. The testhas value and me-rits wider application, but it needsto be carried out under better conditions and withprecautions which have not always been observed.Isbell (personal communication, 1961) has outlinedthe requisite conditions for the nalorphine test asfollows: It should always be performed by a phy-sician who has studied the technique, is aware of theobservations to be made, the precautions to befollowed and the interpretation of the reaction.Before the test is done the patient should be given acomplete physical and mental examination, whichwill yield information on the history of addiction,the presence or absence of needle marks, miosis, etc.,the presence or absence of serious organic diseaseand the patient's competence to sign a consent form.The test is contra-indicated in any person who hasserious organic disease, whatever the nature of thatdisease may be. The consent of the patient should beobtained in writing, after the test and its purposehave been explained to him. This explanation shouldinclude the possibility of severe reactions, theirhazards and possible medico-legal implications. Ifthe pa:ient is under legal age or is mentally incom-petent, c)nsent must be obtained from a parent orlegal guardian. The test should be done in a clinicor hospital where there are adequate facilities forcare of the patient in the case of a severe reactionand it should not be done unless there are facilitiesfor putting the patient to bed before, during andafter the test and resuscitative equipment is at hand,including epinephrine and/or other stimulants,infusion sets with normal saline and plasma ex-panders, mechanical respirators and aspirators andinjectable forms of morphine and barbiturates. Thedose of nalorphine should not exceed 3 mg initiallyand additional doses should not be given except bypersons with considerable experience. There shouldalways be present two professional observers-twophysicians or a physician and a nurse-each ofwhom will make observations independently.
Isbell's recommendations have been in large partaccepted by the State of California Department of
Public Health, which has published a guide explain-ing the purpose and application of the test, themanner in which it is to be carried out and the cri-teria for determining that the test is positive (Stateof California Department of Public Health, 1961).This guide says with respect to the test:" The procedure recommended here is intended to serveonly as a guide to physicians performing the syntheticopiate-antagonist test as an adjunct to the diagnosis ofopiate usage. The procedure is not recommended as anaid in detection of obvious addiction to opiates. As inany clinical circumstance, the results of a single test orprocedure do not constitute a diagnosis."
This is a statement worthy of emphasis, becauseoften the impression has been given that the nalor-phine test or even a small degree of pupillary dilata-tion occurring in the test is all that is needed for apositive diagnosis, whereas the test may give somefalse positives and false negatives when checked byurinalysis and other evidence. Mason & Shepherd(1962) have reviewed tests performed on 154 casesin Illinois, USA, one of the States that authorizesthe use of the nalorphine test as a check on return todrug use of individuals on probation. They reportedthat in 59.1 % of the cases the result of the test wasunequivocal, 37.0% negative and 22.1 % positive.In 28.6% the test was equivocal, 11.7% negativeand 16.9% positive according to further analysis.There were 15 (9.6%) false positives and 4 (2.6%)false negatives. All of the nalorphine tests werechecked by urinalyses, but in these only morphine(by indirection heroin and codeine also) was lookedfor. Very probably this raised the number of appa-rent false positives, since the nalorphine test isstrongly positive when methadone is the drug usedand may be positive when the individual has beentaking pethidine or a related addicting substance.
DISCUSSION AND SUMMARY
The many procedures which have been described,both laboratory and clinical, have been devisedpartly to learn more about the phenomena of toler-ance and physical dependence and partly as attemptsat predicting the risks or relative safety for clinicalpractice of new agents possessing in some degreeone or more of morphine's clinically useful proper-ties. Undoubtedly much has been and can be learnedby these methods that is pertinent to their first pur-pose. Some comments are in order with respect tothe degree of attainment of the second objective.What happens in man is, of course, our real
concorn, but human material for abuse and addic-
161

H. HALBACH & N. B. EDDY
tion liability testing is not readily available. TheAddiction Research Center at Lexington is the onlyplace in the world where tests of this nature aregoing on and very few studies (to our knowledge lessthan half a dozen) of the development of toleranceand physical dependence in man under carefullycontrolled conditions are in progress. An animalmethod, therefore, which could be relied upon notto give false positive results would be very valuable.Negative results in animal experiments may beencouraging but are at present not conclusive andare not likely to be.The method of Shemano & Wendel for predicting
the probability of addiction on the basis of a relation-ship between the dose producing a Straub tail-reaction and the dose with a lethal effect in themouse is simple and economical of time and material,particularly since it does not require any period ofrepeated administration. However, a Straub tail-reaction has been described in the action of sub-stances which are not at all morphine-like and areknown not to produce tolerance or physical depend-ence. The authors report the highest Straub indexfor apomorphine, though they point out that itsability to produce physical dependence has neverbeen tested. The practicability and reliability of themethod with respect to other false positives, if theapomorphine result is a false positive, will needconfirmation through extension to a much widerseries of compounds to establish confidence in itspredictive value as a screening procedure.The several procedures which have been developed
in experiments on the rat have demonstrated thatthis animal can become physically dependent onmorphine and related substances. Also an abstin-ence syndrome, not unrelated to that seen in man,can appear after abrupt withdrawal of chronicallyadministered morphine and, more particularly andmore characteristically, following administration ofnalorphine or another opiate antagonist duringchronic morphinization. Attempts have been madeto quantify the components of the nalorphine-precipitated syndrome. Confirmation and refine-ment of this quantitative evaluation may yield apreliminary screening test for substances withphysical dependence liability of morphine type, atleast for positive results. Again negative resultscannot be considered more than suggestive. Alsoit should be borne in mind that continuity of admi-nistration, seven days a week without interruption, atan around-the-clock interval consonant with theduration of action of the drug, is essential for the
full development of physical dependence and quan-titative comparisons, whatever the experimentalsubject, small or large animal (Seevers, 1958).The investigators at the Addiction Research
Center in Lexington have pointed out similarities inthe behaviour of dog and man during chronicadministration and withdrawal of morphine, andparticularly the comparability of results with similaradministration and withdrawal of pethidine and itsderivatives. They have reported that the demonstra-tion of physical dependence can be made morerapidly and definitely by the use of nalorphine toprecipitate abstinence signs and Martin & Eades(1961) claim.d very recently that a single intravenousinfusion of morphine brought about, in a matter ofhours, reproducible and measurable tolerance andphysical dependence. Spinal dogs, too, have beenshown to exhibit characteristic and reproduciblewithdrawal signs spontaneously and after the use ofnalorphine. However, these various procedures asapplied to the dog have not yet been investigatedsystematically by extending the observations to alarge number of morphine-like substances of knownaddiction potential in man to determine their pre-dictive value in screening. In addition, maintenanceof spinal dogs in good physical condition is beset bymajor technical difficulties.La Barre's method of measuring motor activity
in the dog during addiction to morphine or a testsubstance and withdrawal or substitution of apotentially addicting agent is relatively simple andobjective. The limited number of substancesstudied so far by this method does not allow ex-tensive comparison to be made with the resultsobtained by other methods and in other species,including man. Also the limitation that has beenimposed on dosage in direct addictions and insubstitutions may increase very greatly the likelihoodof false negatives in comparison with tests in themonkey or man. In both of these species the ten-dency has been to push dosages upward until theappearance of signs of toxicity, unless positiveresults have been obtained at lower dose levels. Itshould be advantageous to include in La Barre'smethod the nalorphine abstinence precipitationtechnique and to attempt determination of dosageequivalence in terms of intensity of withdrawalphenomena and completeness of substitution ofone agent for another, as well as to remove thelimitation on dosage increase.
Seevers and his associates have demonstratedrepeatedly the qualitative similarity in the results
162

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
obtained in suppression of the morphine abstinencesyndrome in the monkey and in man and havewarned of the hazard of quantitative predictions.In the single-dose abstinence suppression tests themonkey is more sensitive than man to pethidinederivatives and less sensitive than man to benzo-morphan derivatives (substances related to phena-zocine). Nevertheless, observations in the monkeyhave now been extended to the largest series ofcompounds of related and diverse structure and theresults are subject to the greatest number of com-parisons with the results in man. The single-doseabstinence suppression technique in the monkey isproving of practical value in that it discourages thecontinuation of work with new compounds whichshow high physical dependence capacity and en-courages the development of compounds which havelow physical dependence capacity, and demons-trates the presence or absence of morphine-like pro-perties in new agents not yet sufficiently well knownfor trial in man.From the work in monkeys and the study of
addiction liability in man no substance has yet beenfound which will significantly suppress (to the extentthat codeine does, for example) morphine abstin-ence phenomena, or which will substitute for mor-phine in an established addiction, maintaining theaddiction and preventing the appearance of abstin-ence symptoms, which will not itself produce ad-diction (physical dependence). Therefore, ability tosubstitute for morphine, suppressing the abstinencesyndrome and sustaining the addiction, defines acompound as addicting just as certainly as producingan addiction.
All of the observations at the Addiction ResearchCenter in Lexington are made on individuals whohave been or are currently addicted to an opiate,and the question must arise of the validity for clinicalpractice of conclusions and predictions based onwork with such a population. All of the proceduresat Lexington are designed to push the dosage ifnecessary to the limits of safety, to determine thesubjective and objective reactions of the subjects tothe agent tested in comparison with their reactionsto known drugs given to the same subject in a cross-
over design, and to determine the likelihood of theseindividuals using the drug if it were available tothem. In other words, these tests determine thepatient's ability to identify the compound tested as" dope " (morphine- or heroin-like) or as beinglike some other agent of his experience, the subject'sliking for or attitude towards the new drug, and, if adirect addiction experiment is done, the rate anddegree of development of tolerance and physicaldependence, again in comparison with morphineand perhaps other known agents. The tests at leastprovide direct evidence on the likelihood of abuse,one of the criteria for narcotics control, and maymeasure directly addiction liability. It is significantthat predictions made as a result of work at Lex-ington have been confirmed whenever the agent inquestion has entered into extensive clinical use.The more recent additions to the series of tests
devised at the Addiction Research Center merit afinal word. Reference is made particularly to (a) the24-hour substitution procedure, which reduces thediscomfort to which the subject may be exposed andpermits extensive cross-over observations withpositive and negative controls; (b) the short-term,20-day, direct addiction experiment, which is time-saving and again permits cross-over observations;and (c) the very short, 7-day, intravenous drugadministration, which gives an opportunity for thepatient to express his likes or dislikes and his pre-ference for one drug over another.The final test in which the physician is likely to
have the most confidence is the experience of clinicalpractice. Before nalorphine, this was so tima-consuming and impressionistic as to be of no im-mediate value. The working out of techniques formonitoring, by periodic nalorphine injection,narcotic analgesic medication for chronic painwithout seriously disturbing the patient, makespossible the accumulation of data on tolerance andphysical dependence and comparison of one agentwith another in the same environment. The methodrequires painstaking and long-continued observa-tion, but where groups of suitable patients areavailable results of practical importance for thephysician's guidance can be obtained.
ReSUMIPendant longtemps. seules des observations de cas
reels de toxicomanie permettaient de se rendre comptedes effets toxicomanogenes des opiaces ainsi que dessubstances analgesiques a effet morphinique. Actuelle-ment, des methodes ont ete elaborees, applicables A
l'animal et a l'homme, permettant d'estimer le risque detoxicomanie qu'implique l'emploi de ces substances.Le critere sur lequel sont fondes les tests est la depen-
dance physique (toxicomanie). Les animaux de choix,pour ces epreuves, par ordre croissant d'analogie avec les
163

164 H. HALBACH & N. B. EDDY
r6actions de 1'homme, sont le rat, le chien et surtout lesinge. Les auteurs evaluent les divers tests et esquissentcertains developpements ou perfectionnements possibles.
Mais pour etablir de fa9on certaine le pouvoir toxico-manogene de produits inconnus, l'observation surl'homme reste indispensable. On trouve dans cet article ledetail des modalites d'observation, et des tentativesd'evaluation quantitative approximative de l'effet dessubstances a 1'etude.La mise au point d'antagonistes specifiques de la mor-
phine (du type de la nalorphine) grace auxquels le syn-drome d'abstinence peut etre precocement decele acontribue pour une large part 'a la precision des tests per-mettant de mettre en evidence le pouvoir toxicomanogene,
et a beaucoup accelere l'obtention des resultats. L'utilisa-tion de ces antagonistes, en particulier, a permis l'observa-tion clinique de l'apparition de 1'effet toxicomanogene, etde la tolerance, au cours de traitements prolonges par dessubstances morphinomimetiques.
Les travaux sur les singes, de meme que les observationssur l'homme, ont montre qu'une substance qui supprimele syndrome d'abstinence du au retrait de la morphine, ouqui, substituee a la morphine, entretient la toxicomanie,est elle-meme toxicomanogene. C'est pourquoi, la capa-cite d'une substance de remplacer la morphine ensupprimant le syndrome d'abstinence ou d'entretenirla toxicomanie, permet de la qualifier de toxico-manogene.
REFERENCES
Abe, K. (1930) Jap. J. med. Sci. (Part IV. Pharmacol.),4, 78
Akad, S. (1952) Bull. Narcot., 4, No. 1, p. 10Barlow, 0. W. (1932) J. Amer. med. Ass., 99, 986Carter, R. L. & Wikler, A. (1954) Fed. Proc., 13, 342Carter, R. L. & Wikier, A. (1955) Fed. Proc., 14, 325Cass, L. J., Laing, J. T. & Frederik, W. S. (1961) Curr.
ther. Res., 3, 289Cochin, J. & Daly, J. (1962) Experientia (Basel), 18, 294Cullumbine, H. & Konop, T. S. (1959) Canad. J. Bio-
chem., 37, 1075Deneau, G. A. & Seevers, M. H. (1961) Committee onDrug Addiction and Narcotics, National ResearchCouncil (USA), Minutes of twenty-third meeting,Addendum 1
Desmarez, J. J. (1960) Ann. Soc. roy. Sci. mid. nat. Brux.,13, 125
Eddy, N. B., Halbach, H. & Braenden, 0. J. (1956) Bull.Wld Hlth Org., 14, 353
Eddy, N. B. & Himmelsbach, C. K. (1936) Publ. HlthRep. (Wash.), Suppl. 118
Eddy, N. B. & Lee, L. E., jr (1959) J. Pharmacol. exp.Ther., 125, 116
Eddy, N. B., Lee, L. E., jr & Harris, C. A. (1959) Bull.Narcot., 11, No. 1, p. 3; Bull. Wld Hlth Org., 20, 1245
Eddy, N. B. & Reid, J. G. (1934) J. Pharmacol. exp. Ther.,52, 468
Fichtenberg, D. G. (1951) Bull. Narcot., 3, No. 3, p. 19Fraser, H. F. & Isbell, H. (1960a) Bull. Narcot., 12,No. 1, p. 9
Fraser, H. F. & Isbell, H. (1960b) Bull. Narcot., 12,No. 2, p. 15
Fraser, H. F. & Isbell, H. (1960c) Committee on DrugAddiction and Narcotics, National Research Council(USA), Minutes of twenty-first meeting, Addendum 2,p. 24
Fraser, H. F. et al. (1961a) Clin. Pharmacol. Ther., 2, 287Fraser, H. F. et al. (1961b) J. Pharmacol. exp. Ther., 133,
371
Fujita, Y. (1931) Jap. J. med. Sci. (Part IV. Pharmacol.),5, 39
Hanna, C. (1960) Arch. int. Pharmacodyn., 124, 326Hart, E. R. & McCawley, E. L. (1944) J. Pharmacol. exp.
Ther., 82, 339Heubner, W. et al. (1952) J. Mt Sinai Hosp., 19, 47Himmelsbach, C. K. (1939) J. Pharmacol. exp. Ther., 67,239
Himmelsbach, C. K., Gerlach, G. H. & Stanton, E. J.(1935) J. Pharmacol. exp. Ther., 53, 179
Himmelsbach, C. K. & Small, L. F. (1937) Publ. HithRep. (Wash.), Suppl. 125
Himmelsbach, C. K. et al. (1940) Publ. Hlth Rep. (Wash.),Suppl. 158
Irwin, S. (1954) Diss. Abst., 14, 686Isbell, H. (1952) J. Amer. med. Ass., 149, 1220Isbell, H. (1953) Merck Rep., AprilIsbell, H. et al. (1947) J. Amer. med. Ass., 135, 888Jacob, J., Blozovski, M. & Echinard-Garin, P. (1958)
Therapie, 13, 17Joel, E. & Ettinger, A. (1926) Arch. exp. Path. Pharmak.,
115, 334Kaymakcalan, S. & Woods, L. A. (1954) Fed. Proc.,
13, 373Kaymakcalan, S. & Woods, L. A. (1956) J. Pharmacol.
exp. Ther., 117, 112Kolb, L. & DuMez, A. G. (1931) Publ. H!th Rep.
(Wash.), 46, 698Kolb, L. & Himmelsbach, C. K. (1938) Amer. J. Psychiat.,
94, 759Krueger, H., Eddy, N. B. & Sumwalt, M. (1941a) Publ.
Hlth Rep. (Wash.), Suppl. 165, p. 699Krueger, H., Eddy, N. B. & Sumwalt, M. (1941b) Publ.
Hlth Rep. (Wash.), Suppl. 165, p. 733Krueger, H., Eddy, N. B. & Sumwalt, M. (1941c) Publ.
Hlth Rep. (Wash.), Suppl. 165, p. 741Kubo, T. (1939) Arch. exp. Zellforsch., 23, 253Kuhn, H. F. & Friebel, H. (1962) Med. exp. (Basel),
6, 301

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE 165
La Barre, J. (1959) Bull. Narcot., 9, No. 4, p. 10Lee, L. E., jr (1942) J. Pharmacol. exp. Ther., 75, 161Lindesmith, A. R. (1937) The nature of opiate addiction
(Dissertation, Private Edition. University of ChicagoLibraries)
Maggiolo, C. & Huidobro, F. (1961) Acta physiol. lat.-amer., 11, 70
Martin, W. R. & Eades, C. G. (1961) J. Pharmacol. exp.Ther., 133, 262
Mason, C. C. & Shepherd, H. G. (1962) Amer. J. clin.Path., 37, 176
Mercier, M. J., Etzensperger, P. & Chatain, R. A. (1957)Ann. pharm. franc., 15, 701
Mercier, J. & Mercier, E. (1957) Ann. pharm. fran9., 15,106
Mercier, J. & Sestier, M. R. (1954) Ann. pharm. franV.,12, 458
Nakazawa, Y. (1937) Jap. J. med. Sci. (Part IV. Pharma-col.), 10, 191
Paton, W. (1957) Brit. J. Pharmacol., 12, 119Phatak, N. M. & David, N. A. (1953) Curr. Res. Anesth.,
32, 242Plant, 0. H. & Pierce, I. H. (1928) J. Pharmacol. exp.
Ther., 33, 329Sanjo, K. (1934) Folia pharmacol. jap., 17, 219Sasaki, M. (1938) Arch. exp. Zellforsch., 21, 289Schaumann, 0. (1957) Handbutch der experimentellen
Pharmakologie. XII: Morphin und morphinahnlicheVerbindungen, Berlin, Springer-Verlag, p. 217
Schrappe, O., Burchard, J. M. & Gehiken, K. (1959)Arch. Psychiat. Nervenkr., 199, 19
Seevers, M. (1958) Fed. Proc., 17, 1175Semura, S. (1933) Folia pharmacol. jap., 17, 34Shemano, J. & Wendel, H. (1960) Pharmacologist, 2, 97
Stanton, E. J. (1936) J. Pharmacol. exp. Ther., 56, 252State of California Department of Public Health (1961)Recommended procedure for narcotic use testing ofprobationers and parolees. A guide to physicians,Berkeley, California State Printing Office
Tatum, A. L., Seevers, M. H. & Collins, K. H. (1929)J. Pharmacol. exp. Ther., 36, 447
Tavat, S. & Akgasu, A. (1956) Arch. int. Pharmacodyn.,108, 92
Terry, J. G. & Braumoeller, F. L. (1956) Calif. Med., 85,299
Unna, K. (1943) J. Pharmacol. exp. Ther., 79, 27Wada, A. (1928) Jop. J. med. Sci. (Part IV. Pharmacol.),
2, 68Wikler, A. (1944) J. Pharmacol. exp. Ther., 80, 176Wikier, A. (1946) Fed. Proc., 5, 213Wikler, A. (1948) Amer. J. Psychiat., 105, 329Wikler, A. & Carter, R. L. (1952) Fed. Proc., 11, 402Wikler, A. & Carter, R. L. (1953) J. Pharmacol. exp.
Ther., 109, 92Wikler, A. & Frank, K. (1947) Fed. Proc., 6, 384Wikier, A. & Frank, K. (1948) J. Pharmacol. exp. Ther.,
94, 382Wikier, A., Fraser, H. F. & Isbell, H. (1953) J. Pharmacol.
exp. Ther., 109, 8Winter, C. A. & Flataker, L. (1950) J. Pharmacol. exp.
Ther., 98, 305Winter, C. A. et al. (1954) J. Pharmacol. exp. Ther., 111,
152Woods, A. L. et al. (1961) Toxicol. appl. Pharmacol., 3,
358World Health Organization, Expert Committee on
Addiction-Producing Drugs (1957) Wld Hlth Org.techn. Rep. Ser., 116, 9

166 H. HALBACH & N. B. EDDY
Annex I
SINGLE-DOSE ATTITUDE QUESTIONNAIRE (PATIENTS' RATINGS)
Name: ................. No. .............
.. Dose: ..........Medication:
Date:
Time:
Questions to be answered by you about the effects of this drug. In answering all questions check only sensations which youhave experienced since your last examination by the aide. If the words listed are not satisfactory for describing your feelings, pleasewrite in other words or make comments.
Hour: 1 2 3 4 5 6 7 8 9 10
No No No No No No No No No No1. Do you feel the medicine?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
2. This drug is most like what drug listed below (check one)?
(a) A blank (water) ............................... ......... (d) Marihuana (reefer)
(b) " Dope" (opiates) (e)" Goof balls " (barbiturate-like)..
(c) Cocaine ................. . ............................. (f) Benzedrine (" Benny ") .... ....................
(g)Other (please name) ..............................................................
3. Check each sensation which you feel:
(a) Normal (no change) ................ ... ... ................ (g) "Pleasant sick"
(b) " Turningof stomach .. .................. ........................ ............ (h) " Drive " ............................................................................
(c) Skin itchy ......... .......(i) Sleepy ....... ..............................
(d) Relaxed ....Nerv.................................................. ) N
(e) " Coasting " ......... . ........... (k) Drunken ..
(f) " Soap-box" (loquacious; tendency to brag) Other (pleasedescribe)................................................
4. Your liking for this drug is most nearly described by which of the following?
(a ) Not a ........ ........................... ... (d) A lot ..................... .......................
(b) Slight ..... ... .................... (e) An awful lot ...... ..............................
(c)Moderate ......... .............................. .......... (f) ther (pleasedescribe).
ments : ......... .......................... ...................

167TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
Annex 2
SINGLE-DOSE ATTITUDE QUESTIONNAIRE (OBSERVERS' RATINGS)
........ No..... Date:
Medication: ...... Dose: .. Time:.
In answering all questions check only the items of behaviour observed since your last examination. If the words listed are notsatisfactory, please insert others which you consider more appropriate or make comments.
Hour: 1 2 3 4 5 6 7 8 9 10
No No No No No No No No No No1. Any evidence of drug effects?
Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes
2. Behaviour is most like that seen after (check one):
(a) A blank .......... ........................................ (d) Marihuana (reefer) ................. ......
(b) " Dope " (opiates or potent synthetic (e) " Goof balls" (barbiturates) b
analgesics) ..(f).Benzedrine Benny ").............................(f).Benzedrine.(".Benn(c) Cocaine ................................................(g) Other (please name).
3. Check each item which you think the patient shows:
(a) Norm al (no change) ....... (g) Vomiting .........................................................................
(b) Scratching .............................................. (h) "Nodding. .
(c)Red eyes .....................................(............ Sleepy .........................
(d) Relaxed .............................................. (j)N ervous
(e)"Coasting" . . . .......... ..........( k)Drun ken .................................................
(f) " Soap-box " (loquacious; tendency to brag) ..................... (/) Other (please describe)
4. How much do you think the patient liked the effects of this drug during the past hour?
(a (d A lot ................
(b) Slightly . . . .............. (e) An awful lot ..
(c) Moderately . ... (f) Other (please describe) . .
5. Pupils: ................................................ .............. ................ ... ................... .................... ............................................ ............ ........ ........
. o ents : ................ ...........................
................................................................................................................. .I........i...................................................... ..........................................................
Initials of aide: ...................................................

168 H. HALBACH & N. B. EDDY
Annex 3
CHRONIC DOSAGE ATTITUDE QUESTIONNAIRE FOR OPIATES (PATIENTS' RATINGS)
Nameof patient: ...................................................................................................................
Answer all questions according to how this drug is affecting you today.Date:.
1.Hasthisdrugproduced any effect on you? Yes ................. ..................... Noo.....
2.Does this drug feel like an opiate (" dope ") ? Yes ........ ........................... No ......... .......
If so, which of the drugs given below is this drug most nearly like, and how strong do you think it is ?It Is most nearly like (check one):
(a) Heroin ...................................... ......... (c) Codeine .......... ................... ..... .......
(b)Morphine ................................................................................ (d) Other "dope"-like drug (pleasename)I think the strength of this drug is (check one):
(a) No effect ................................................ (d) Average . ............
(b) Very weak ......................... (e) Strong .. . . ... ..
(c) Weak..... . ............................ (f) Very strong ...................
(g) Overdose..........................................................................................
3. Is the feeling from this drug like that from one of the drugs given below?Yes .No.
It is most nearly like (check one):
(a)Ablank(water) ................................................ . (d) "Goof balls"(barbiturate-like) ..........................................
(b)Marihuana (reefer) ................................................................. (e) Alcohol (whiskeyor beer) ............................. ............
(c)Cocaine ............................................... . . (f) Benzedrine ("Benny")(g)Other(please name) .................................................................
I think the strength of this drug Is (check one):
(a)Noeffect .......................................................... (d) AverageVery weak .... . . (e) Strong
(c)Weak ..................................................... (f) Very strong.....................................................
(g) Overdose ...................................................................................
4.Would you like to take this drug every day? Yes ...........No.......................................... Don't care ...... ........
5.Doesthisdrugmake you feel bad? Yes .......................................
If so, does it make you feel so badly that you would stop taking it ifyou were not on a test? Yes . No
. escri bebriefly themost important effects of this drug on you:
......................................................................................................................................I........I............................................................................
7 Are you "1 kicking a habit " ? Yes No

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
Annex 4
CHRONIC DOSAGE ATTITUDE QUESTIONNAIRE FOR OPIATES (OBSERVERS' RATINGS)
Name of patient ....... ................................................................................... at ..........................................
Answer all questions according to how this drug Is affecting this patient today.
1. Is this drug affecting the behaviour of this patient in any way? Yes .No
2.Doesthis patient show behaviour resembling that seen after opiates? Yes .................No.............................. .................
If so, indicate from your observations of the patient's behaviour the drug listed below which induces behaviour most nearlyresembling that of the patient. Also describe the potency of this drug in inducing opiate-like behaviour.Behaviour is most nearly like that seen after (check one):
(a) Heroin . . ............................................(c)Codeine .
(b) Morphine . . . (d) Other opiate (please name)........................ ...
The potency of this drug In Inducing behavioural changes Is (check one):(a) No effect .......... (d) Average .
(b) Very weak .......... (e) Strong .
(c) Weak ......... (f) Very strong .
(g) Overdose.
3 Is the behaviour after this drug like that after one of the drugs listed below?Yes .No.
Behaviour is most nearly like that seen after (check one):(a)A blank .......... ...............................((d)"olGoof ballsa" (barbiturates)b.....(b)Marihuana (reefer) .................................. .(f) Alcohol..............
(c) Cocaine ................. ........ (f) Benzedrinee(("Bennyy").(g)Other (please name) ................................................................
The potency of this drug In inducing behavioural changes Is (check one):(a) No effect ........... (d) Average .
(b) Very weak. ......... (e) Strong .
(c) Weak .. ......... (f) Very strong .
(g) Overdose.
4. Do you think this patient would like to take this drug every day?Yes.No .Doesn't care.
5. Do you think this drug makes this patient uncomfortable? YesY.No..If the answer is " yes " to this question, do you think he dislikes itsufficiently to voluntarily stop taking it if he were not on an experi-mental test? YesY.No..
6. Describebriefly themostimportant effects of this drug in this patient: ............................................................................................................
7. Is this patient " kicking a habit " ? Yes .. No.
Initials of aide: ..................................................
169

H. HALBACH & N. B. EDDY
Annex S
PATIENT'S INITIAL DATA SHEET
Name: ............. Hosp. No. ...... Date: ...... ..................... ..
Patient No Med. Code Card No..
Age: . Sex: .Weight:.
Diagnosisandgeneral condition: .......................................................................................... ............................................................................................
Mental state: ..................................... ....................................................................................................... ...................................................................
..........................................................................................................................................................................................
Nature or origin of pain:,
........................................................................................
Current treatment for pain: Kind: ......................
Dose: .....F...........................Fr..................... Frequency: ........................... ............................... .... ............ ...
Has codeine or other narcotic analgesic been used for this patient within
three months? Yes No
If yes, give details:
...................................................................................................................................... ..........................................................................................................
Does this patient require laxative medication? Yes No
If yes, g ive details :
....................................................................................................................
Does this patient require any other regular medication? Yes No .......................
If yes, give details:
............ ............... ............ ..... ... ............. ............... ........ ........ ..
170

171TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
Annex 6
DAILY RECORD: CONTROL PERIOD
Name:............
Patient No. ... .....
Analgesic medication:
Aspirin Dose: 5 gri
Aspirin 5 grn
Aspirin 5 grn
.. Date: ......... .
Control day:.
sins
ains
ains
Time:
Time: ........ .........
Time: ... ...................
Pain relief ' (circle figure which applies):Morning: 8 a.m. 0 1 2 3 4Afternoon: 12 noon 0 1 2 3 4 Average ......... .................
Evening: 4 p.m. 0 1 2 3 4
Side-effects (complaints) 2 (circle figure which applies):8 a.m. 12 noon 4 p.m.
Nausea 0 1 2 3 0 1 2 3 0 1 2 3Vomiting 0 1 2 3 0 1 2 3 0 1 2 3Nervousness 0 1 2 3 0 1 2 3 0 1 2 3Drowsiness 0 1 2 3 0 1 2 3 0 1 2 3Mental dullness 0 1 2 3 0 1 2 3 0 1 2 3Lightheadedness, faintness 0 1 2 3 0 1 2 3 0 1 2 3Unsteadiness 0 1 2 3 0 1 2 3 0 1 2 3Dizziness 0 1 2 3 0 1 2 3 0 1 2 3Euphoria 0 1 2 3 0 1 2 3 0 1 2 3Other (explain) 0 1 2 3 0 1 2 3 0 1 2 3
Constipation 0 +Bowel movement 0 +Laxative required 0 +
0 = moderately severe pain; patient claims no relief from medication.1 very little relief from medication.2 = slight to moderate pain; moderate relief attributed to medication.3= very little paln.4 = no pain; comfortable in this respect, whether or not on account of medication.
'0 = not present; I = slight; 2= moderate; 3 = severe.

H. HALBACH & N. B. EDDY
Annex 7
DAILY RECORD: STUDY PERIOD
Name:............... Date:.
Patient No..
Coded med.No..
Studyday
Analgesic medication:
Units: Time: Units:. Time: ... ..
Pain relief I (circle figure which applies):Morning: 8 a.m. 0 1 2 3 4
Afternoon:12 noon 0 1 2 3 4 Average ....................................Evening: 4 p.m. 0 1 2 3 4
Side-effects (complaints) 2 (circle figure which applies):8 a.m. 12 noon 4 p.m.
Nausea 0 1 2 3 0 1 2 3 0 1 2 3Vomiting 0 1 2 3 0 1 2 3 0 1 2 3Nervousness 0 1 2 3 0 1 2 3 0 1 2 3Drowsiness 0 1 2 3 0 1 2 3 0 1 2 3Mental dullness 0 1 2 3 0 1 2 3 0 1 2 3Lightheadedness, faintness 0 1 2 3 0 1 2 3 0 1 2 3Unsteadiness 0 1 2 3 0 1 2 3 0 1 2 3Dizziness 0 1 2 3 0 1 2 3 0 1 2 3Euphoria 0 1 2 3 0 1 2 3 0 1 2 3Other (explain) 0 1 2 3 0 1 2 3 0 1 2 3
Constipation 0 +Bowel movement 0 +Laxative required 0 +
' 0= moderately severe pain; patient claims no relief from medication.I = very little relief from medication.2 = slight to moderate pain; moderate relief attributed to medication.3= very little pain.4 = no pain; comfortable in this respect, whether or not on account of medication.
'0= not present; I = slight; 2- moderate; 3= severe.
172

TESTS FOR ADDICTION (CHRONIC INTOXICATION) OF MORPHINE TYPE
Annex 8
ALLYL OR PLACEBO TEST RECORD SHEET
Code No. of solution injected:
......... Study day: ...........................................................................
Time of last preceding coded drug given:
Blood pressure:
Control ........
10 min........
20 min..........
30 min........
40 min. ....
Respiratory rate:
Control .....
10 min.......
20 min.
30 min......
40 min-.
Points
-...I..........I.........
Points
Rectal temperature:
Control ....-.... ....
10 min......................
20 m in....
30 min....... ...
40 min. ... ..
Pupll size:
Control. .. ....
10 min. ............................................
20 min. ............................................
30 in. ...
40 min. .........................................
Other signs (circle as observed):
Yawning
Lacrimation
Rhinorrhoea
Sweating
Gooseflesh
Tremor
Restlessness
Abdominal or other cramps
Urge to defaecate
Nausea
Emesis
Points
Total score:
Remarks:
173
Nam e:
Patient No...........................
Test No..............................
Date:..
.......... Time:
Points ....
0
0
0
0
0
0
0
0
0
0
+
+