Embed Size (px)
DESCRIPTION
by Prof Kwa (IMU)
Citation preview

TBL on Hypertension Therapeutics
Assoc Prof Dr Kwa Siew KimFamily Medicine Dept
IMU
April 2011 Semester 8

2
Pre-requisites
• Before you embark on this TBL, revisit the lectures on hypertension treatment in Phase 1
• You should also read up the latest 2008 Malaysian Clinical Practice Guidelines (CPG) on Management of Hypertension

3
Revision activity 1:
How would you classify hypertension?What are the co-morbidities that would
affect the management of hypertension?What are the common medications
prescribed for hypertension?What are the common side effects?

4
Revision activity 2:
How would you treat hypertension in the following special cases? children, elderly, pregnant women Chronic disease: hypertension, diabetes,
stroke, LVH, IHD, heart failure, renal disease, connective tissue disease, peripheral vascular disease
Accelerated/emergency hypertension

5
Background Reading
1. Clinical Practice Guidelines: Management of Hypertension. MOH/P/PAK/156.08 (GU). 3rd Edition Feb 2008. Ministry of Health Malaysia, Academy of Medicine of Malaysia, Malaysian Society of Hypertension. http://www.malaysianheart.org/section.php?sid=23&pb=Normal (accessed on 28.2.11)
2. D Gareth Beavers, Gregory YH Lip, Eoin O’Brien. ABC of Hypertension. 5th Ed. BMJ Books. Blackwell Publishing. (Available in the IMU library is the 5th Edition published in 2007)

6
0
10
20
30
40
50
60
1996 2006 2016
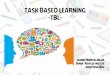
Prevalence of hypertension in Malaysians aged 30 years and above
42.6 %
29.9 %
14.4%
1986
?? ?

7
What does NHMS III show?
• Prevalence of hypertension has increased
• But there is little difference in the rate of awareness and rate of BP control in the hypertensive population
• Rate of blood pressure control remains poor (26%) although more diagnosed patients are prescribed with medication for hypertension

8
CVD Risk Factors
• Hypertension*• Diabetes mellitus*• Dyslipidemia*• Obesity* (BMI >30 kg/m2) * Components of the metabolic syndrome• Cigarette smoking• Physical inactivity• Microalbuminuria or estimated GFR <60 ml/min• Age (older than 55 for men, 65 for women)• Family history of premature CVD (men under age 55 or
women under age 65)

9
Benefits of Lowering BP
Average Percent Reduction
• Stroke incidence 35–40%
• Myocardial infarction 20–25%
• Heart failure 50%

10
State of HPT Management
• In general, management of hypertension is poor despite awareness and knowledge
• only 1/5 of hypertensive patients are identified
• 1/5 are treated
• 1/5 are treated to target

11
What is our objective?
• At the end of this session, students should be able to manage the hypertension in the primary care setting based on therapeutic guidelines

12
• Recognise the different co-morbidities with hypertension seen in primary care
• List the common groups of medication prescribed for hypertension
• Describe the mode of action of the drug groups and its side effects
• Discuss and provide answers to the clinical scenarios in “Clinical trigger”
• Summarise the learning issues in “Revision activity”
TBL-your tasks are to:

13
KEY MESSAGES: CLINICAL PRACTICE GUIDELINEON HYPERTENSION, 2008
1. Definition of hypertension: persistent elevation of BP of >140/90 mmHg
2. Prevalence of hypertension in Malaysians > 30 years was 42.6% in 2006
3. 64% of HPT in Malaysia undiagnosed. Do opportunistic BP at every encounter
4. Not treated or poorly treated HPT leads to increased cardiovascular, cerebrovascular and renal morbidity and mortality
5. BP of 120 to 139 over 80 to 89 mm Hg is defined as prehypertension and should be treated in certain high risk groups

14
KEY MESSAGES: CLINICAL PRACTICE GUIDELINE
ON HYPERTENSION, 2008
6. Lifestyle changes for all HPT/ prehypertension
7. Base drug treatment on global vascular risks 8. For new cases with no complications, first
line monotherapy includes all except BB9. Only 26% of Malaysians on treatment reach
target BP (<140/90 mmHg). 10. Combination therapy is often required to
achieve target and may be instituted early

SUMMARY OF SOME RECOMMENDATIONS
From 3rd Malaysian CPG

16
Measurement ofBlood Pressure
• mercury sphygmomanometer is the gold standard
• Take BP in both arms, use higher reading• Take lying and standing • systolic drop of >20 mmHg is considered a
significant postural drop• Home BP measurement useful to monitor control • empowers patient with BP control and may
improve compliance

17
HPT Emergencies
• systolic BP >210 and or diastolic BP >120
• admit
• Useful drugs are – Captopril– Nifedipine – Labetalol– Hydralazine, etc

18
Management of SevereHypertension
• Hypertensive urgencies– reduce BP slowly by 25% over 24 hours but
not lower than 160/90 mmHg
• Hypertensive emergencies– Reduce BP rapidly by 25% over 3 to 12 hours
but not lower than 160/90 mmHg
• NEVER give nifedipine sublingual

19
Hypertension and Diabetes Mellitus
• Rx when BP is persistently >130/80
• Target to <130/80
• If albuminuria, treat with ACEI even if BP normal
• Lower BP to <125/75 if proteinuria >1g/24 hours
• ACEI preferred to ARB unless cough

20
Hypertensionand Stroke
• BP most important predictor for stroke • CCB are better to protect against stroke
compared to diuretic and/or BB • ACEI + diuretic has been shown to reduce
stroke recurrence in both normotensive and hypertensive patients
• morbidity and mortality from further strokes significantly lower in patients receiving ARBs compared with CCBs
• In haemorrhagic stroke, avoid lowering BP in the first few days of accelerated hypertension or hypertensive emergencies

21
Hypertension in the Elderly• Target BP level same as for the young < 140/90• Those with high systolic hypertension can reduce
SBP to below 160 mmHg initially • Weight loss and salt reduction effective because of
their greater sensitivity to sodium intake• All 5 major classes of drugs (diuretics, BB, CCBs,
ACEIs and ARBs) reduce CVD events in elderly• But elderly more sensitive to diuretics and CCB• ACEI is drug of choice for those with concomitant
left ventricular systolic dysfunction, post myocardial infarction or diabetes mellitus.
• Standing BP should be measured to detect postural hypotension

22
Drug Classes in HPT
• Diuretics• ACEI / ARB• Calcium channel blockers• β blockers• α blockers• Combined α β blockers• Centrally-acting drugs-methyldopa, moxonidine • Direct renin inhibitor (Aliskiren)-new kid on the
block

23
Effective combination• ß-blockers +
diuretics
• ß-blockers + CCBs
• CCBs + ACEIs
• ACEIs + diuretics
• ACEI/ARBs + diuretics
• Benefits proven in the elderly (diuretics & CCB), cost-effective.
• Relatively cheap, appropriate for concurrent CHD.
• A p p r o p r i a t e f o r c o n c u r r e n t dyslipidaemias and diabetes mellitus.
• Appropriate for concurrent heart failure, diabetes mellitus and stroke.
• Appropriate for concurrent heart failure, left-ventricular hypertrophy and diabetes mellitus.

24
Choice of HPT drugs • Dyslipidaemia- ACEI & ARB, CCB• LVH- ARB/ACEI • Diabetes- ACEI & ARB, CCB, diuretics • Elderly- diuretics & CCB• Stroke- CCB (10 prevention) & ACEI (post stroke)• CHD & Angina- ß-blockers & long acting CCB• LV dysfunction & post MI- ß-blockers & ACEI• Heart failure- ACEI & diuretics (ß-blockers -
metoprolol, bisoprolol, carvedilol (alpha and beta))• Proteinuria- ACEI & ARB• Benign prostate enlargement- α blockers• HPT in pregnancy- methyldopa, labetalol

25
Some contraindications
• Diuretics: gout ?dyslipidaemia, ?diabetes
• ACEI/ARB: bilateral renal artery stenosis
• ß-blockers: asthma, PVD, ?DM ?dyslipidaemia
• Avoid using short acting CCB (nifedipine) in CHD and unstable angina
• Be careful about BP lowering immediately after stroke

26
Hypertension Cases for Discussion
• There are 2 OBAQ
• There are 6 cases for discussion
• Divide into your 2 groups
• Each group is to work through ALL cases
• You can use the references provided to guide you through the cases

27
Work through these: OBAQ 1
• A 28-year-old man is found to have a BP reading of between 130/82-139/88 mmHg
• This is confirmed on two further occasions
What is the most appropriate diagnosis?
A.Stage 3 Hypertension
B.Stage 2 Hypertension
C.Stage 1 Hypertension
D. Prehypertension
E. Normal

28
• A 70-year-old man is diagnosed with hypertension
• His BP reading is 186/74mm Hg
• He also has BPH
What is the most appropriate BP therapy?
A. Alpha blockers
B.Angiotensin Receptor Blockers
C.Angiotensin Receptor Inhibitors
D.Beta blockers
E.Thiazide diuretics
OBAQ 2

29
Case study 1 – Hypertension and the Elderly
• Mr. Ismail is a 72-year-old Malay man who has 3 repeated blood pressure reading of 180/80 mm Hg despite lifestyle changes. He is asymptomatic and does not have any end organ damage from hypertension.
Questions:• What condition does he have?• Would he benefit from pharmacological
treatment? Give reasons for your answer.• Which drug(s) is suitable?

30
Case study 2 – Hypertension and pregnancy
• 28-year-old primigravida who has a pre-pregnancy blood pressure reading of 100/60 mm Hg. Blood pressure reading at 24 weeks’ gestation is sustained at 130/82.
Question:• Does she have PIH?• For hypertension in pregnancy, which anti-
hypertensive drug(s) would you advise? Give reasons for your choice

31
Case 3: 57 years old Malay contractor • Severe hypertension started on Rx with atenolol 100
mg bd and nifedipine 20 mg tds • BP was uncontrolled at 190/110 mm Hg. • Started on hydrochlorothiazide 25 mg om 3 days ago• Sudden onset of right knee pain on waking up • On examination, BP is 170/100 mm Hg. Pulse is 54
beats per min. BMI 35 WC 110 cm• Right knee joint: red, swollen, hot, very tenderQuestions:What is the cause of his knee arthritis?How would you manage his hypertension?He develops angina. Would you offer him aspirin for
secondary prevention?

32
Case study 4 – Hypertension and Comorbid conditions
• Muthusamy is a 48-year-old smoker with gout, hypertension, dyslipidaemia and previous MI
• His wife is asthmatic and his son has eczema • He is on treatment with metoprolol 50 mg daily.
His blood pressure reading is between 140/90- 160/100 mm Hg
Questions:• Comment on his hypertension treatment.• What hypertensive drug(s) are suitable for him?

33
Case study 5 – ACEI
• Mr. Lim, a 52-year-old diabetic was prescribed ACEI for newly-diagnosed hypertension.
• His initial serum creatinine prior to treatment is 100 μmol/l
• One week later, his serum creatinine is 150 μmol/l
Questions: Explain why. What should you do?

34
Case study 6 – Hypertensive Urgencies
• Mr. Lim, a 52-year-old asymptomatic man was incidentally found to have BP of 190/112 mm Hg repeated three times
• He was treated with sublingual nifedipine and his BP dropped to 100/60 mmHg
• He then developed left-sided hemiplegiaQuestions:• What went wrong? Comment on his
hypertension management.

35