Embed Size (px)
Citation preview
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 1 of 26
This document contains information specific to the State of Florida. Please refer to the Provider Reference Guide for general information regarding plan administration. Table of Contents
1.1 Covered Benefits - Molina Healthcare of Florida – Options Plus (Medicare) Plan 001........................................................... 2
1.2 Covered Benefits - Molina Healthcare of Florida (MMA 20 and Under) .................................................................................. 3
1.3 Covered Benefits - Molina Healthcare of Florida (MMA 21 and Older) ................................................................................... 9
1.4 Covered Benefits - Molina Healthcare of Florida (DSNP – QMB+, FBDE, SLMB+) (Medicare) ........................................... 15
1.5 Covered Benefits - Molina Healthcare of Florida (DSNP – QMB) (Medicare) ...................................................................... 19
1.6 Covered Benefits - Molina Healthcare of Florida (LTC) ........................................................................................................ 20
1.7 Covered Benefits - Molina Healthcare of Florida (Comprehensive) ...................................................................................... 21
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 2 of 26
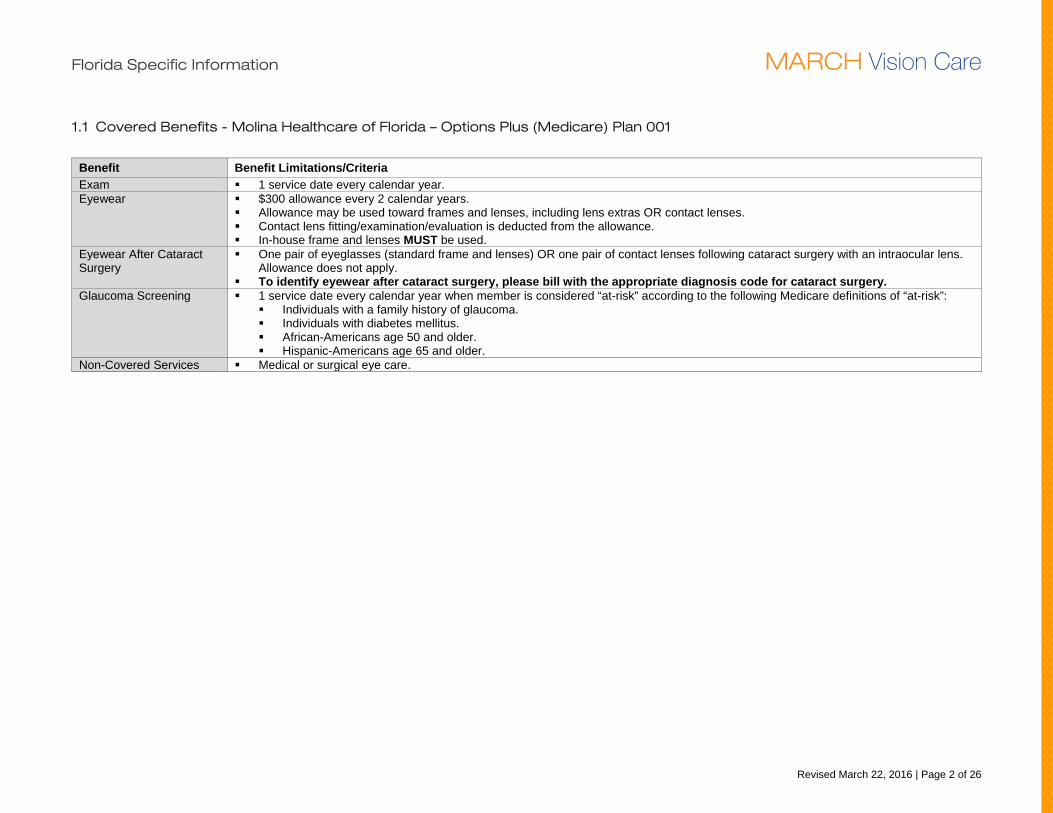
1.1 Covered Benefits - Molina Healthcare of Florida – Options Plus (Medicare) Plan 001
Benefit Benefit Limitations/Criteria Exam 1 service date every calendar year. Eyewear $300 allowance every 2 calendar years.
Allowance may be used toward frames and lenses, including lens extras OR contact lenses. Contact lens fitting/examination/evaluation is deducted from the allowance. In-house frame and lenses MUST be used.
Eyewear After Cataract Surgery
One pair of eyeglasses (standard frame and lenses) OR one pair of contact lenses following cataract surgery with an intraocular lens. Allowance does not apply.
To identify eyewear after cataract surgery, please bill with the appropriate diagnosis code for cataract surgery. Glaucoma Screening 1 service date every calendar year when member is considered “at-risk” according to the following Medicare definitions of “at-risk”:
Individuals with a family history of glaucoma. Individuals with diabetes mellitus. African-Americans age 50 and older. Hispanic-Americans age 65 and older.
Non-Covered Services Medical or surgical eye care.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 3 of 26
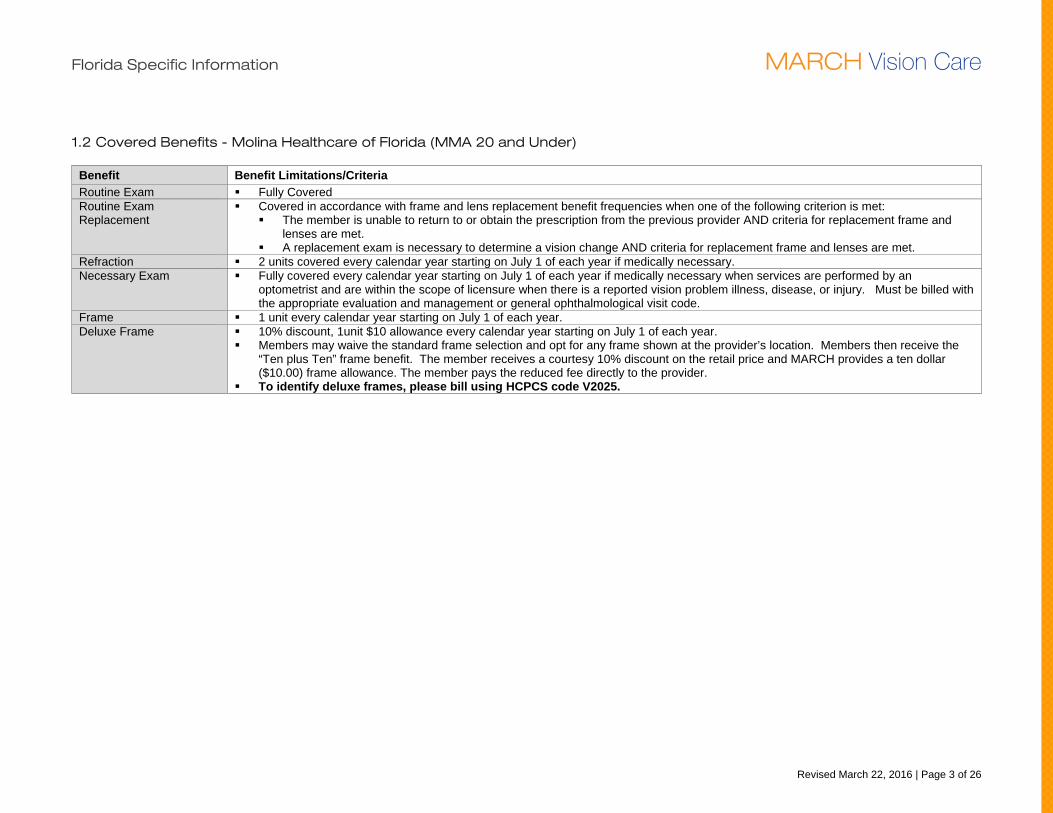
1.2 Covered Benefits - Molina Healthcare of Florida (MMA 20 and Under)
Benefit Benefit Limitations/Criteria Routine Exam Fully Covered Routine Exam Replacement
Covered in accordance with frame and lens replacement benefit frequencies when one of the following criterion is met: The member is unable to return to or obtain the prescription from the previous provider AND criteria for replacement frame and
lenses are met. A replacement exam is necessary to determine a vision change AND criteria for replacement frame and lenses are met.
Refraction 2 units covered every calendar year starting on July 1 of each year if medically necessary. Necessary Exam Fully covered every calendar year starting on July 1 of each year if medically necessary when services are performed by an
optometrist and are within the scope of licensure when there is a reported vision problem illness, disease, or injury. Must be billed with the appropriate evaluation and management or general ophthalmological visit code.
Frame 1 unit every calendar year starting on July 1 of each year. Deluxe Frame 10% discount, 1unit $10 allowance every calendar year starting on July 1 of each year.
Members may waive the standard frame selection and opt for any frame shown at the provider’s location. Members then receive the “Ten plus Ten” frame benefit. The member receives a courtesy 10% discount on the retail price and MARCH provides a ten dollar ($10.00) frame allowance. The member pays the reduced fee directly to the provider.
To identify deluxe frames, please bill using HCPCS code V2025.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 4 of 26
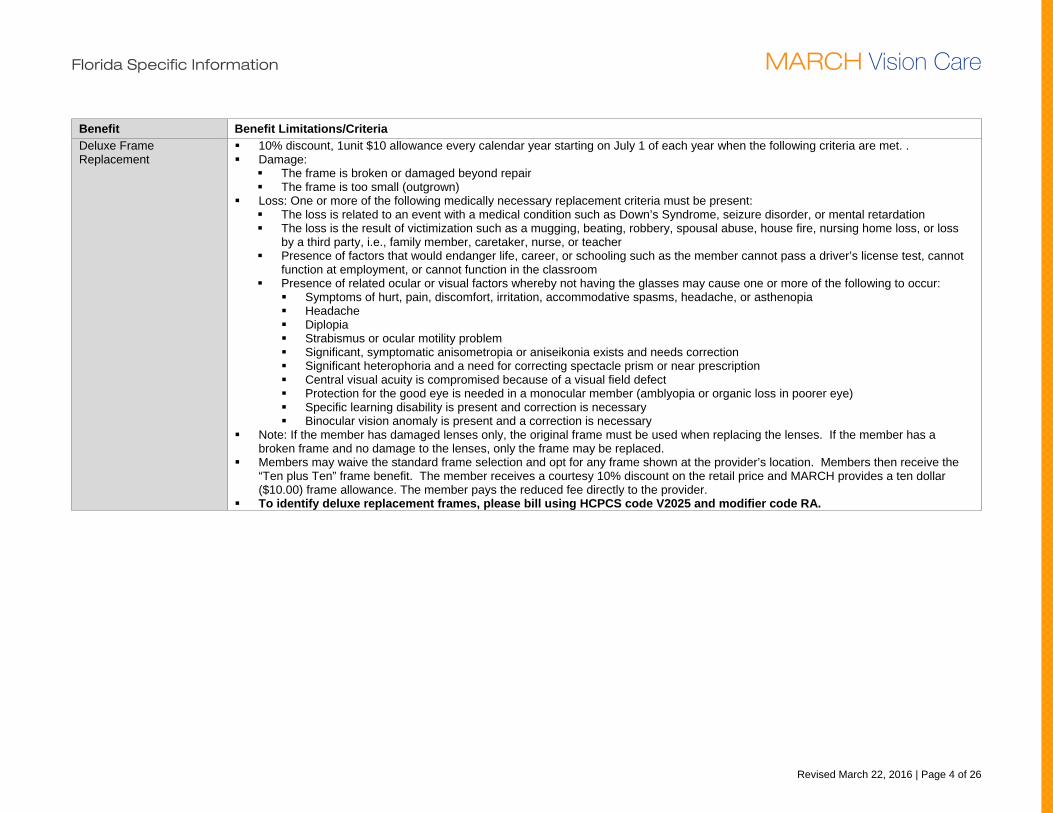
Benefit Benefit Limitations/Criteria Deluxe Frame Replacement
10% discount, 1unit $10 allowance every calendar year starting on July 1 of each year when the following criteria are met. . Damage:
The frame is broken or damaged beyond repair The frame is too small (outgrown)
Loss: One or more of the following medically necessary replacement criteria must be present: The loss is related to an event with a medical condition such as Down’s Syndrome, seizure disorder, or mental retardation The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary Binocular vision anomaly is present and a correction is necessary
Note: If the member has damaged lenses only, the original frame must be used when replacing the lenses. If the member has a broken frame and no damage to the lenses, only the frame may be replaced.
Members may waive the standard frame selection and opt for any frame shown at the provider’s location. Members then receive the “Ten plus Ten” frame benefit. The member receives a courtesy 10% discount on the retail price and MARCH provides a ten dollar ($10.00) frame allowance. The member pays the reduced fee directly to the provider.
To identify deluxe replacement frames, please bill using HCPCS code V2025 and modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 5 of 26
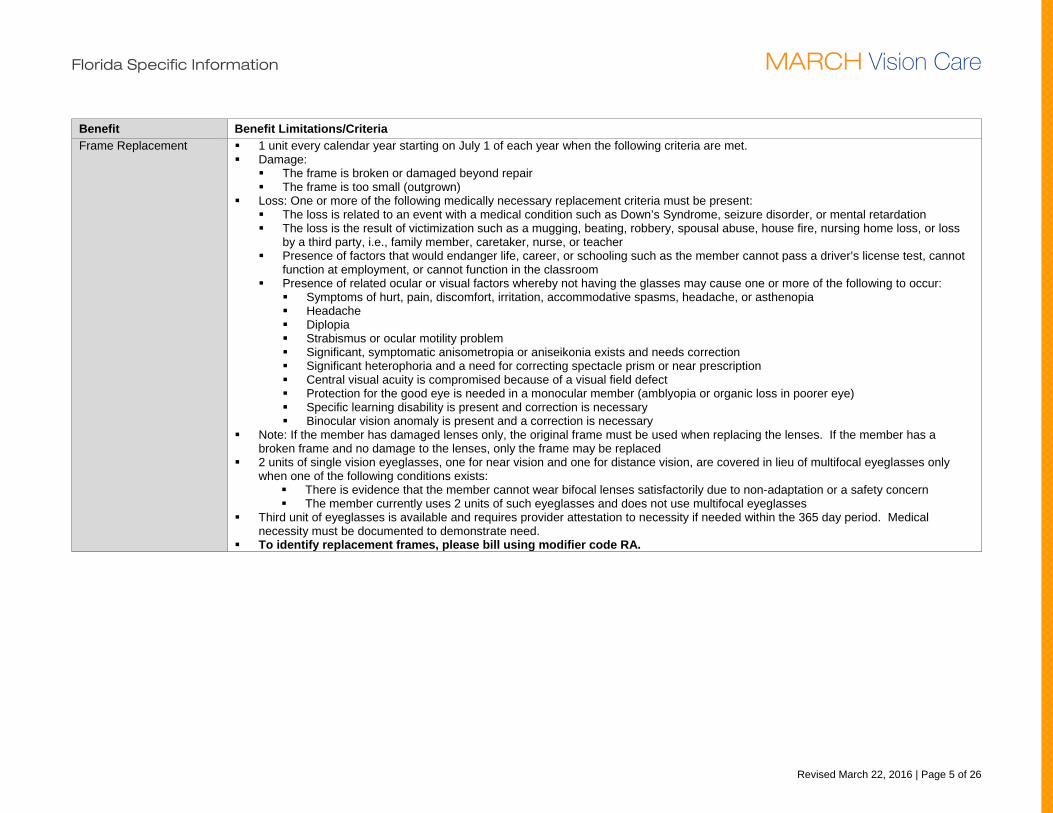
Benefit Benefit Limitations/Criteria Frame Replacement 1 unit every calendar year starting on July 1 of each year when the following criteria are met.
Damage: The frame is broken or damaged beyond repair The frame is too small (outgrown)
Loss: One or more of the following medically necessary replacement criteria must be present: The loss is related to an event with a medical condition such as Down’s Syndrome, seizure disorder, or mental retardation The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary Binocular vision anomaly is present and a correction is necessary
Note: If the member has damaged lenses only, the original frame must be used when replacing the lenses. If the member has a broken frame and no damage to the lenses, only the frame may be replaced
2 units of single vision eyeglasses, one for near vision and one for distance vision, are covered in lieu of multifocal eyeglasses only when one of the following conditions exists:
There is evidence that the member cannot wear bifocal lenses satisfactorily due to non-adaptation or a safety concern The member currently uses 2 units of such eyeglasses and does not use multifocal eyeglasses
Third unit of eyeglasses is available and requires provider attestation to necessity if needed within the 365 day period. Medical necessity must be documented to demonstrate need.
To identify replacement frames, please bill using modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 6 of 26
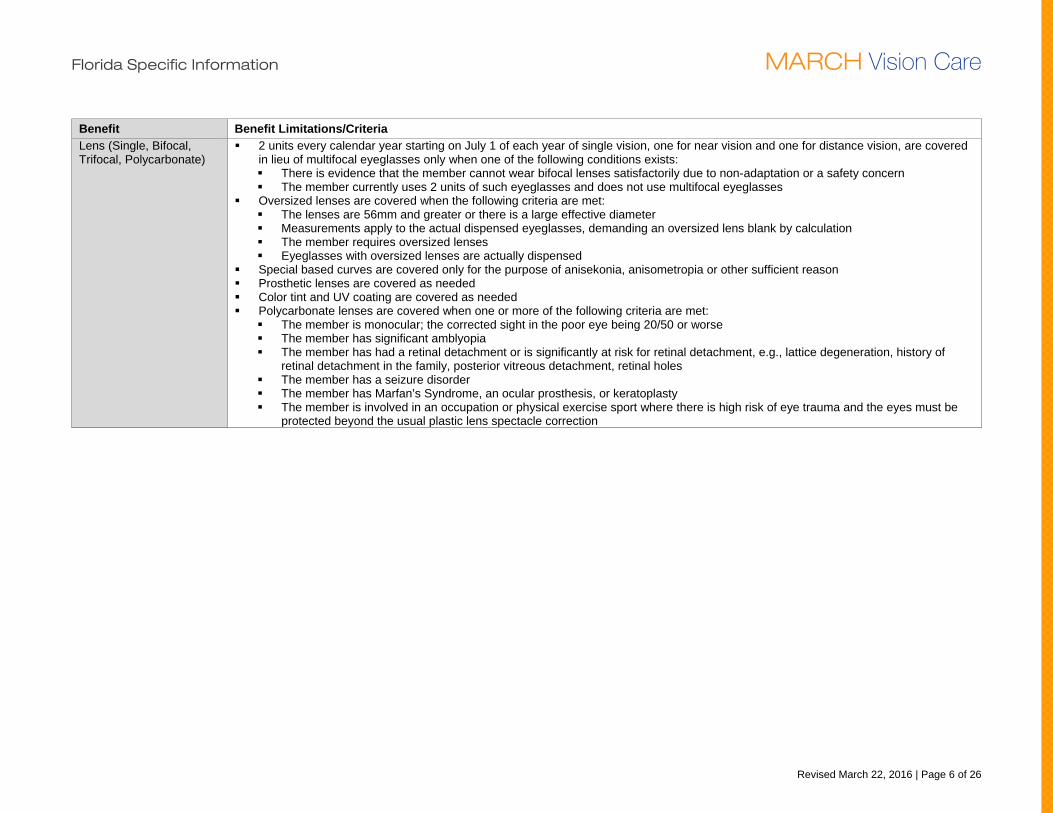
Benefit Benefit Limitations/Criteria Lens (Single, Bifocal, Trifocal, Polycarbonate)
2 units every calendar year starting on July 1 of each year of single vision, one for near vision and one for distance vision, are covered in lieu of multifocal eyeglasses only when one of the following conditions exists: There is evidence that the member cannot wear bifocal lenses satisfactorily due to non-adaptation or a safety concern The member currently uses 2 units of such eyeglasses and does not use multifocal eyeglasses
Oversized lenses are covered when the following criteria are met: The lenses are 56mm and greater or there is a large effective diameter Measurements apply to the actual dispensed eyeglasses, demanding an oversized lens blank by calculation The member requires oversized lenses Eyeglasses with oversized lenses are actually dispensed
Special based curves are covered only for the purpose of anisekonia, anisometropia or other sufficient reason Prosthetic lenses are covered as needed Color tint and UV coating are covered as needed Polycarbonate lenses are covered when one or more of the following criteria are met:
The member is monocular; the corrected sight in the poor eye being 20/50 or worse The member has significant amblyopia The member has had a retinal detachment or is significantly at risk for retinal detachment, e.g., lattice degeneration, history of
retinal detachment in the family, posterior vitreous detachment, retinal holes The member has a seizure disorder The member has Marfan’s Syndrome, an ocular prosthesis, or keratoplasty The member is involved in an occupation or physical exercise sport where there is high risk of eye trauma and the eyes must be
protected beyond the usual plastic lens spectacle correction
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 7 of 26
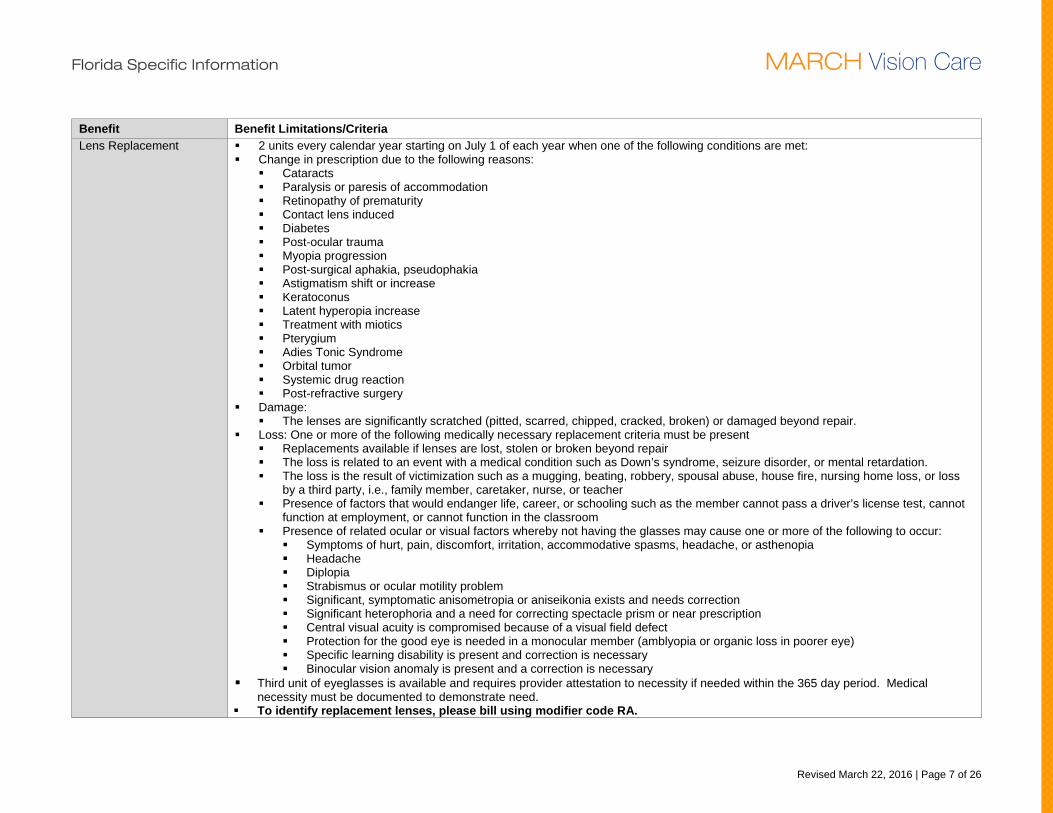
Benefit Benefit Limitations/Criteria Lens Replacement 2 units every calendar year starting on July 1 of each year when one of the following conditions are met:
Change in prescription due to the following reasons: Cataracts Paralysis or paresis of accommodation Retinopathy of prematurity Contact lens induced Diabetes Post-ocular trauma Myopia progression Post-surgical aphakia, pseudophakia Astigmatism shift or increase Keratoconus Latent hyperopia increase Treatment with miotics Pterygium Adies Tonic Syndrome Orbital tumor Systemic drug reaction Post-refractive surgery
Damage: The lenses are significantly scratched (pitted, scarred, chipped, cracked, broken) or damaged beyond repair.
Loss: One or more of the following medically necessary replacement criteria must be present Replacements available if lenses are lost, stolen or broken beyond repair The loss is related to an event with a medical condition such as Down’s syndrome, seizure disorder, or mental retardation. The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary Binocular vision anomaly is present and a correction is necessary
Third unit of eyeglasses is available and requires provider attestation to necessity if needed within the 365 day period. Medical necessity must be documented to demonstrate need.
To identify replacement lenses, please bill using modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 8 of 26
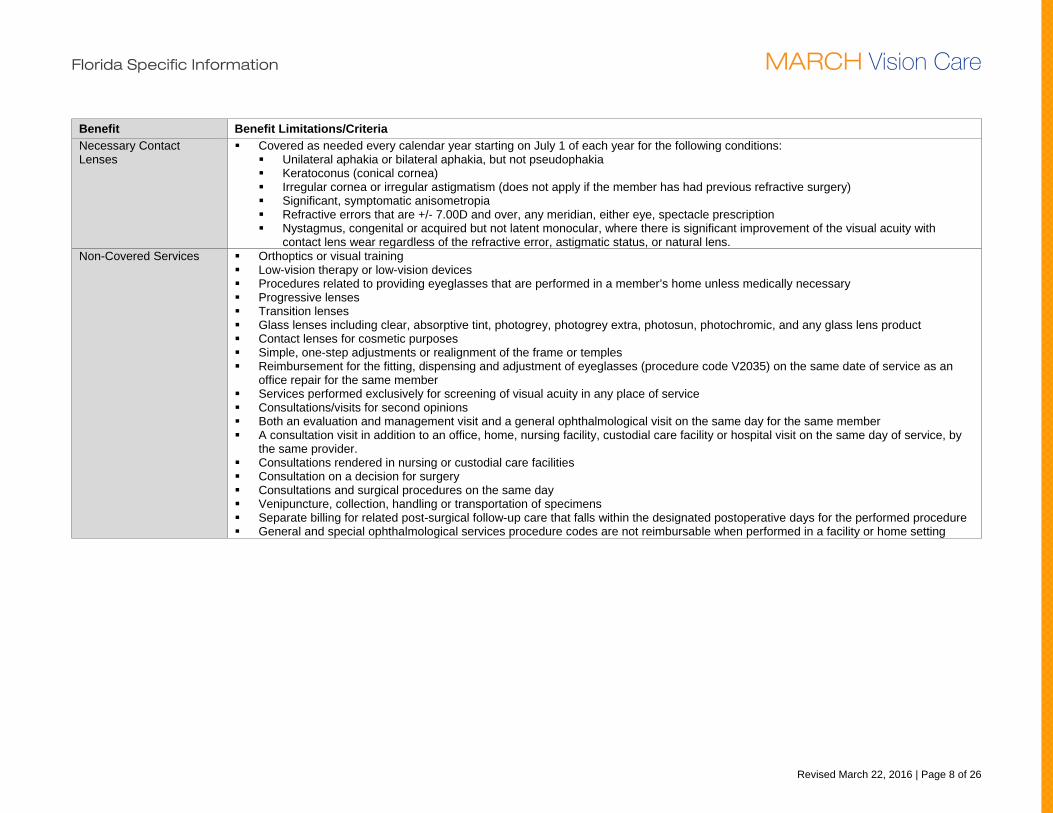
Benefit Benefit Limitations/Criteria Necessary Contact Lenses
Covered as needed every calendar year starting on July 1 of each year for the following conditions: Unilateral aphakia or bilateral aphakia, but not pseudophakia Keratoconus (conical cornea) Irregular cornea or irregular astigmatism (does not apply if the member has had previous refractive surgery) Significant, symptomatic anisometropia Refractive errors that are +/- 7.00D and over, any meridian, either eye, spectacle prescription Nystagmus, congenital or acquired but not latent monocular, where there is significant improvement of the visual acuity with
contact lens wear regardless of the refractive error, astigmatic status, or natural lens. Non-Covered Services Orthoptics or visual training
Low-vision therapy or low-vision devices Procedures related to providing eyeglasses that are performed in a member’s home unless medically necessary Progressive lenses Transition lenses Glass lenses including clear, absorptive tint, photogrey, photogrey extra, photosun, photochromic, and any glass lens product Contact lenses for cosmetic purposes Simple, one-step adjustments or realignment of the frame or temples Reimbursement for the fitting, dispensing and adjustment of eyeglasses (procedure code V2035) on the same date of service as an
office repair for the same member Services performed exclusively for screening of visual acuity in any place of service Consultations/visits for second opinions Both an evaluation and management visit and a general ophthalmological visit on the same day for the same member A consultation visit in addition to an office, home, nursing facility, custodial care facility or hospital visit on the same day of service, by
the same provider. Consultations rendered in nursing or custodial care facilities Consultation on a decision for surgery Consultations and surgical procedures on the same day Venipuncture, collection, handling or transportation of specimens Separate billing for related post-surgical follow-up care that falls within the designated postoperative days for the performed procedure General and special ophthalmological services procedure codes are not reimbursable when performed in a facility or home setting
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 9 of 26
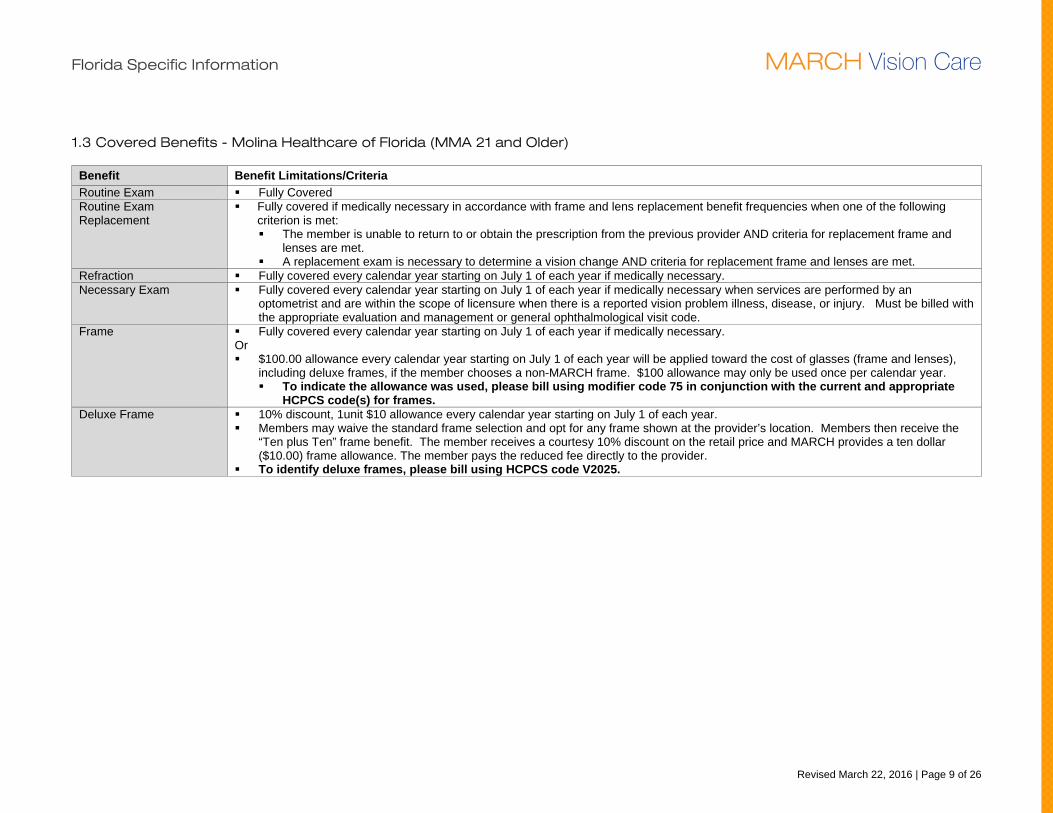
1.3 Covered Benefits - Molina Healthcare of Florida (MMA 21 and Older)
Benefit Benefit Limitations/Criteria Routine Exam Fully Covered Routine Exam Replacement
Fully covered if medically necessary in accordance with frame and lens replacement benefit frequencies when one of the following criterion is met: The member is unable to return to or obtain the prescription from the previous provider AND criteria for replacement frame and
lenses are met. A replacement exam is necessary to determine a vision change AND criteria for replacement frame and lenses are met.
Refraction Fully covered every calendar year starting on July 1 of each year if medically necessary. Necessary Exam Fully covered every calendar year starting on July 1 of each year if medically necessary when services are performed by an
optometrist and are within the scope of licensure when there is a reported vision problem illness, disease, or injury. Must be billed with the appropriate evaluation and management or general ophthalmological visit code.
Frame Fully covered every calendar year starting on July 1 of each year if medically necessary. Or $100.00 allowance every calendar year starting on July 1 of each year will be applied toward the cost of glasses (frame and lenses),
including deluxe frames, if the member chooses a non-MARCH frame. $100 allowance may only be used once per calendar year. To indicate the allowance was used, please bill using modifier code 75 in conjunction with the current and appropriate
HCPCS code(s) for frames. Deluxe Frame 10% discount, 1unit $10 allowance every calendar year starting on July 1 of each year.
Members may waive the standard frame selection and opt for any frame shown at the provider’s location. Members then receive the “Ten plus Ten” frame benefit. The member receives a courtesy 10% discount on the retail price and MARCH provides a ten dollar ($10.00) frame allowance. The member pays the reduced fee directly to the provider.
To identify deluxe frames, please bill using HCPCS code V2025.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 10 of 26
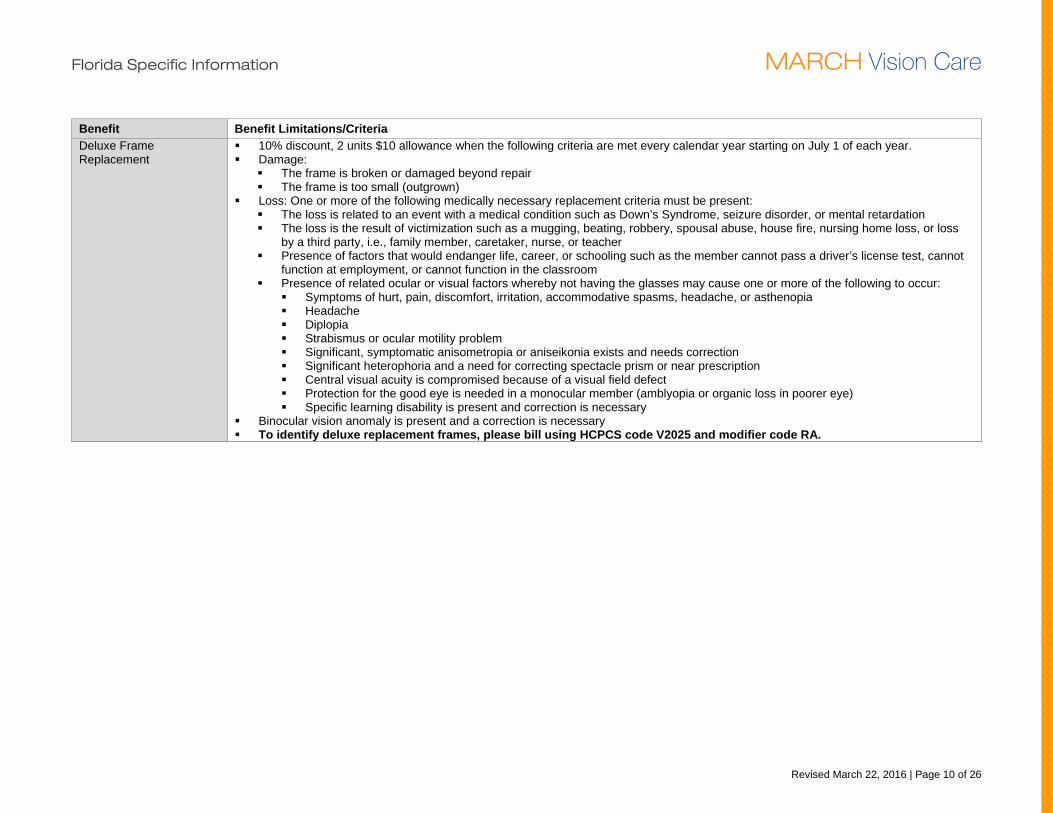
Benefit Benefit Limitations/Criteria Deluxe Frame Replacement
10% discount, 2 units $10 allowance when the following criteria are met every calendar year starting on July 1 of each year. Damage:
The frame is broken or damaged beyond repair The frame is too small (outgrown)
Loss: One or more of the following medically necessary replacement criteria must be present: The loss is related to an event with a medical condition such as Down’s Syndrome, seizure disorder, or mental retardation The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary
Binocular vision anomaly is present and a correction is necessary To identify deluxe replacement frames, please bill using HCPCS code V2025 and modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 11 of 26
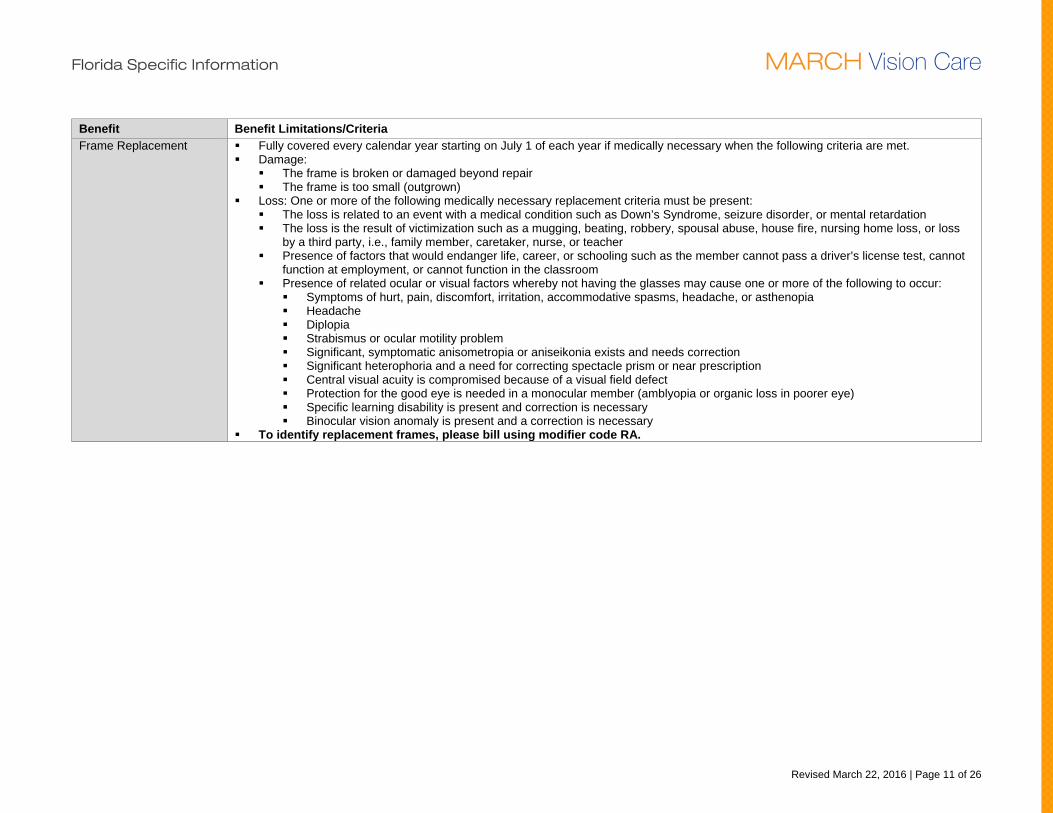
Benefit Benefit Limitations/Criteria Frame Replacement Fully covered every calendar year starting on July 1 of each year if medically necessary when the following criteria are met.
Damage: The frame is broken or damaged beyond repair The frame is too small (outgrown)
Loss: One or more of the following medically necessary replacement criteria must be present: The loss is related to an event with a medical condition such as Down’s Syndrome, seizure disorder, or mental retardation The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary Binocular vision anomaly is present and a correction is necessary
To identify replacement frames, please bill using modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 12 of 26
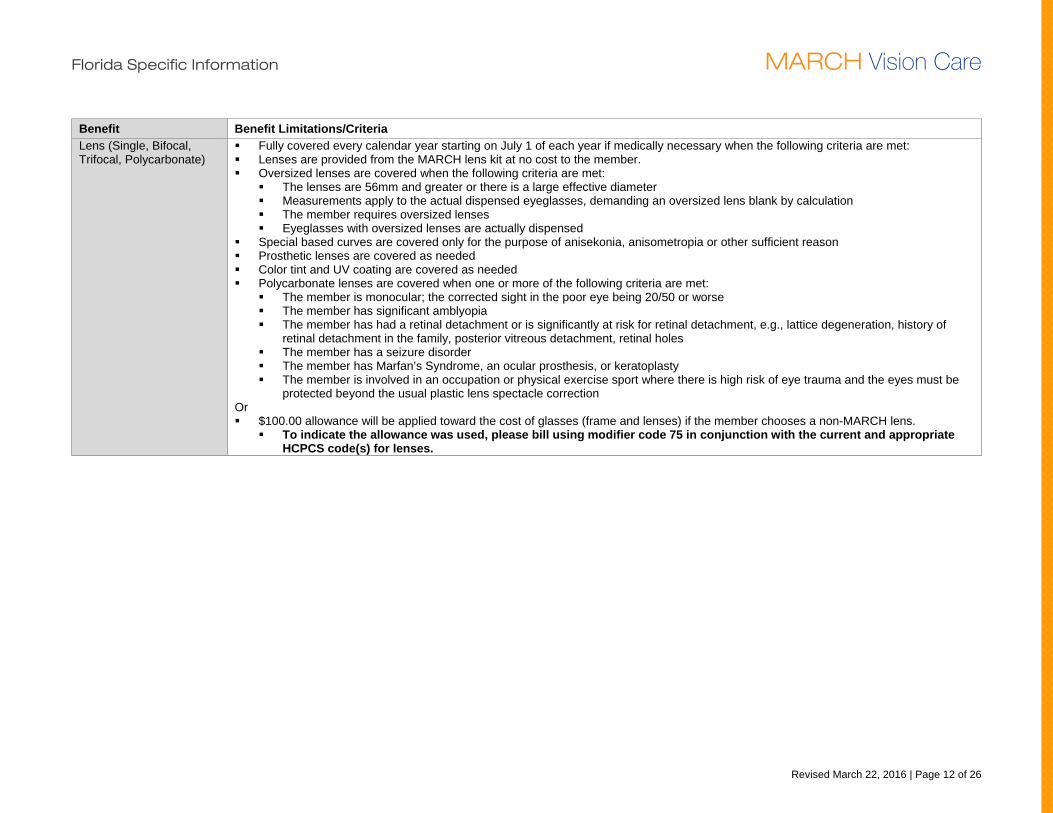
Benefit Benefit Limitations/Criteria Lens (Single, Bifocal, Trifocal, Polycarbonate)
Fully covered every calendar year starting on July 1 of each year if medically necessary when the following criteria are met: Lenses are provided from the MARCH lens kit at no cost to the member. Oversized lenses are covered when the following criteria are met:
The lenses are 56mm and greater or there is a large effective diameter Measurements apply to the actual dispensed eyeglasses, demanding an oversized lens blank by calculation The member requires oversized lenses Eyeglasses with oversized lenses are actually dispensed
Special based curves are covered only for the purpose of anisekonia, anisometropia or other sufficient reason Prosthetic lenses are covered as needed Color tint and UV coating are covered as needed Polycarbonate lenses are covered when one or more of the following criteria are met:
The member is monocular; the corrected sight in the poor eye being 20/50 or worse The member has significant amblyopia The member has had a retinal detachment or is significantly at risk for retinal detachment, e.g., lattice degeneration, history of
retinal detachment in the family, posterior vitreous detachment, retinal holes The member has a seizure disorder The member has Marfan’s Syndrome, an ocular prosthesis, or keratoplasty The member is involved in an occupation or physical exercise sport where there is high risk of eye trauma and the eyes must be
protected beyond the usual plastic lens spectacle correction Or $100.00 allowance will be applied toward the cost of glasses (frame and lenses) if the member chooses a non-MARCH lens.
To indicate the allowance was used, please bill using modifier code 75 in conjunction with the current and appropriate HCPCS code(s) for lenses.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 13 of 26
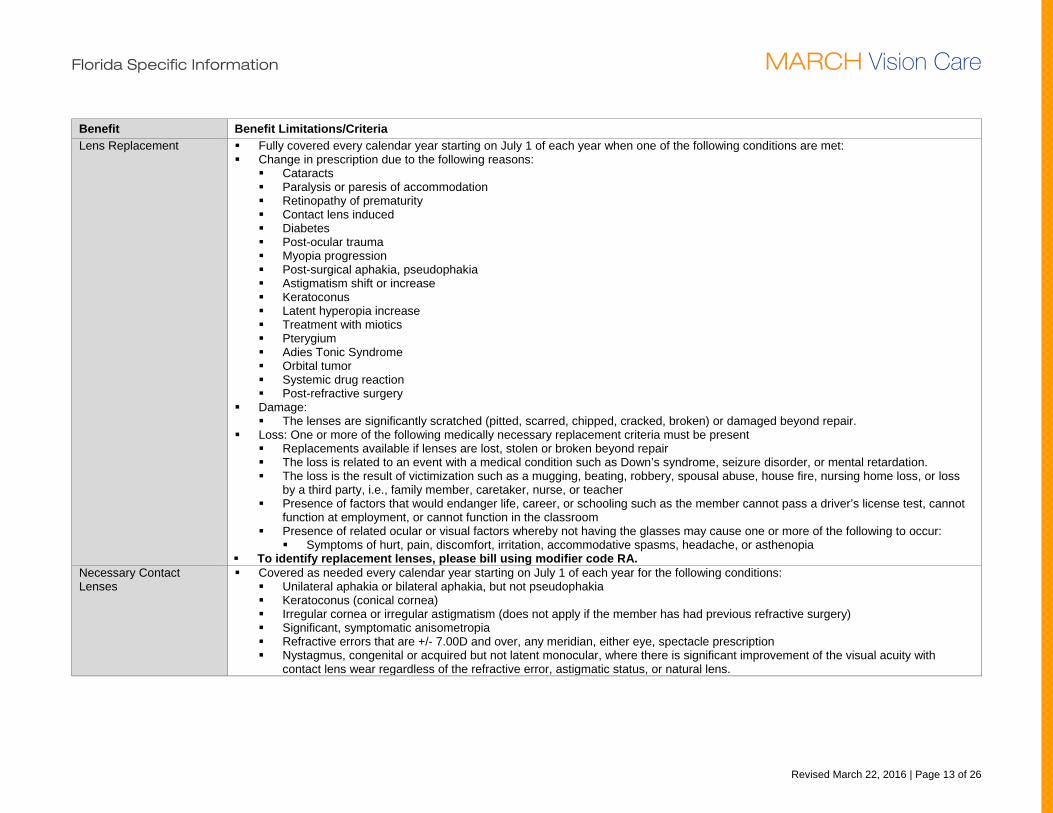
Benefit Benefit Limitations/Criteria Lens Replacement Fully covered every calendar year starting on July 1 of each year when one of the following conditions are met:
Change in prescription due to the following reasons: Cataracts Paralysis or paresis of accommodation Retinopathy of prematurity Contact lens induced Diabetes Post-ocular trauma Myopia progression Post-surgical aphakia, pseudophakia Astigmatism shift or increase Keratoconus Latent hyperopia increase Treatment with miotics Pterygium Adies Tonic Syndrome Orbital tumor Systemic drug reaction Post-refractive surgery
Damage: The lenses are significantly scratched (pitted, scarred, chipped, cracked, broken) or damaged beyond repair.
Loss: One or more of the following medically necessary replacement criteria must be present Replacements available if lenses are lost, stolen or broken beyond repair The loss is related to an event with a medical condition such as Down’s syndrome, seizure disorder, or mental retardation. The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia To identify replacement lenses, please bill using modifier code RA.
Necessary Contact Lenses
Covered as needed every calendar year starting on July 1 of each year for the following conditions: Unilateral aphakia or bilateral aphakia, but not pseudophakia Keratoconus (conical cornea) Irregular cornea or irregular astigmatism (does not apply if the member has had previous refractive surgery) Significant, symptomatic anisometropia Refractive errors that are +/- 7.00D and over, any meridian, either eye, spectacle prescription Nystagmus, congenital or acquired but not latent monocular, where there is significant improvement of the visual acuity with
contact lens wear regardless of the refractive error, astigmatic status, or natural lens.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 14 of 26
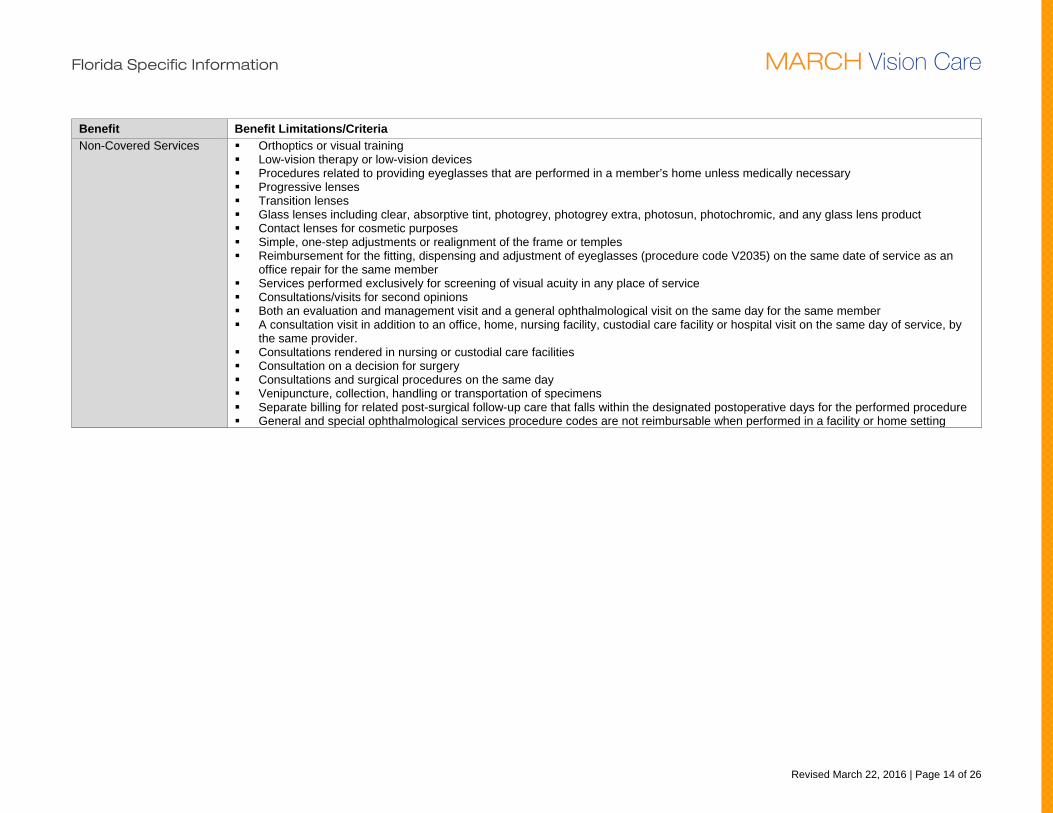
Benefit Benefit Limitations/Criteria Non-Covered Services Orthoptics or visual training
Low-vision therapy or low-vision devices Procedures related to providing eyeglasses that are performed in a member’s home unless medically necessary Progressive lenses Transition lenses Glass lenses including clear, absorptive tint, photogrey, photogrey extra, photosun, photochromic, and any glass lens product Contact lenses for cosmetic purposes Simple, one-step adjustments or realignment of the frame or temples Reimbursement for the fitting, dispensing and adjustment of eyeglasses (procedure code V2035) on the same date of service as an
office repair for the same member Services performed exclusively for screening of visual acuity in any place of service Consultations/visits for second opinions Both an evaluation and management visit and a general ophthalmological visit on the same day for the same member A consultation visit in addition to an office, home, nursing facility, custodial care facility or hospital visit on the same day of service, by
the same provider. Consultations rendered in nursing or custodial care facilities Consultation on a decision for surgery Consultations and surgical procedures on the same day Venipuncture, collection, handling or transportation of specimens Separate billing for related post-surgical follow-up care that falls within the designated postoperative days for the performed procedure General and special ophthalmological services procedure codes are not reimbursable when performed in a facility or home setting
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 15 of 26
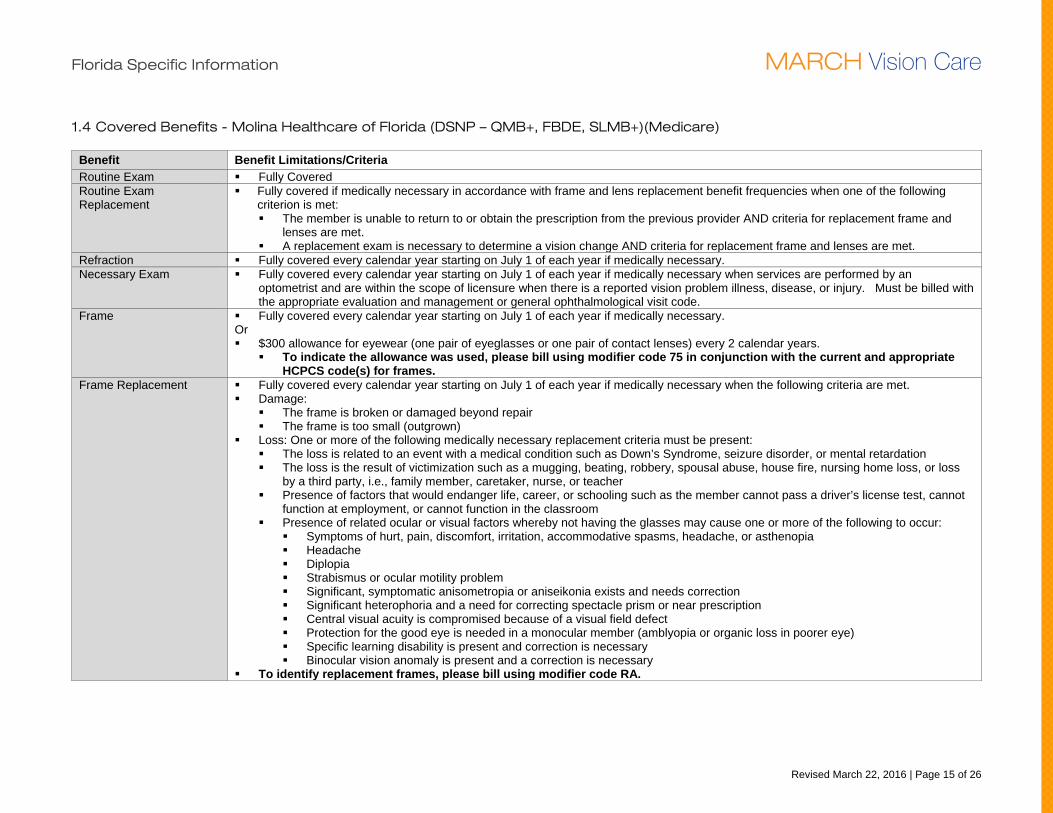
1.4 Covered Benefits - Molina Healthcare of Florida (DSNP – QMB+, FBDE, SLMB+)(Medicare)
Benefit Benefit Limitations/Criteria Routine Exam Fully Covered Routine Exam Replacement
Fully covered if medically necessary in accordance with frame and lens replacement benefit frequencies when one of the following criterion is met: The member is unable to return to or obtain the prescription from the previous provider AND criteria for replacement frame and
lenses are met. A replacement exam is necessary to determine a vision change AND criteria for replacement frame and lenses are met.
Refraction Fully covered every calendar year starting on July 1 of each year if medically necessary. Necessary Exam Fully covered every calendar year starting on July 1 of each year if medically necessary when services are performed by an
optometrist and are within the scope of licensure when there is a reported vision problem illness, disease, or injury. Must be billed with the appropriate evaluation and management or general ophthalmological visit code.
Frame Fully covered every calendar year starting on July 1 of each year if medically necessary. Or $300 allowance for eyewear (one pair of eyeglasses or one pair of contact lenses) every 2 calendar years.
To indicate the allowance was used, please bill using modifier code 75 in conjunction with the current and appropriate HCPCS code(s) for frames.
Frame Replacement Fully covered every calendar year starting on July 1 of each year if medically necessary when the following criteria are met. Damage:
The frame is broken or damaged beyond repair The frame is too small (outgrown)
Loss: One or more of the following medically necessary replacement criteria must be present: The loss is related to an event with a medical condition such as Down’s Syndrome, seizure disorder, or mental retardation The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary Binocular vision anomaly is present and a correction is necessary
To identify replacement frames, please bill using modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 16 of 26
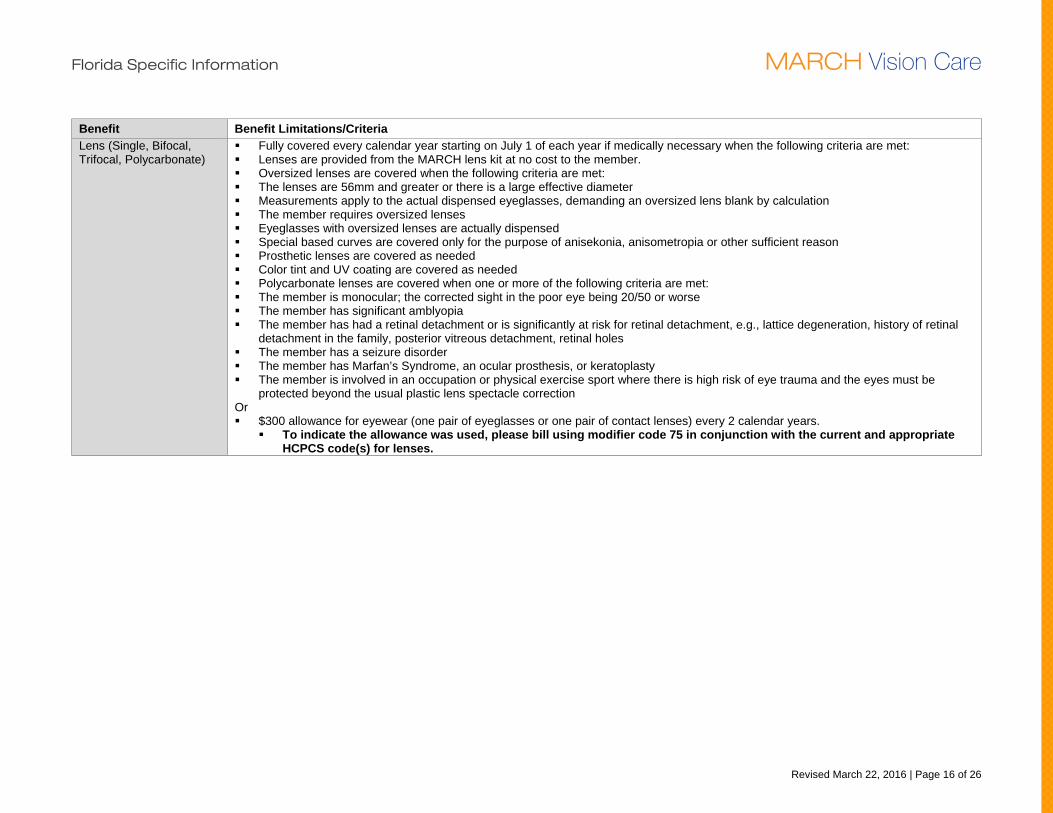
Benefit Benefit Limitations/Criteria Lens (Single, Bifocal, Trifocal, Polycarbonate)
Fully covered every calendar year starting on July 1 of each year if medically necessary when the following criteria are met: Lenses are provided from the MARCH lens kit at no cost to the member. Oversized lenses are covered when the following criteria are met: The lenses are 56mm and greater or there is a large effective diameter Measurements apply to the actual dispensed eyeglasses, demanding an oversized lens blank by calculation The member requires oversized lenses Eyeglasses with oversized lenses are actually dispensed Special based curves are covered only for the purpose of anisekonia, anisometropia or other sufficient reason Prosthetic lenses are covered as needed Color tint and UV coating are covered as needed Polycarbonate lenses are covered when one or more of the following criteria are met: The member is monocular; the corrected sight in the poor eye being 20/50 or worse The member has significant amblyopia The member has had a retinal detachment or is significantly at risk for retinal detachment, e.g., lattice degeneration, history of retinal
detachment in the family, posterior vitreous detachment, retinal holes The member has a seizure disorder The member has Marfan’s Syndrome, an ocular prosthesis, or keratoplasty The member is involved in an occupation or physical exercise sport where there is high risk of eye trauma and the eyes must be
protected beyond the usual plastic lens spectacle correction Or $300 allowance for eyewear (one pair of eyeglasses or one pair of contact lenses) every 2 calendar years.
To indicate the allowance was used, please bill using modifier code 75 in conjunction with the current and appropriate HCPCS code(s) for lenses.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 17 of 26
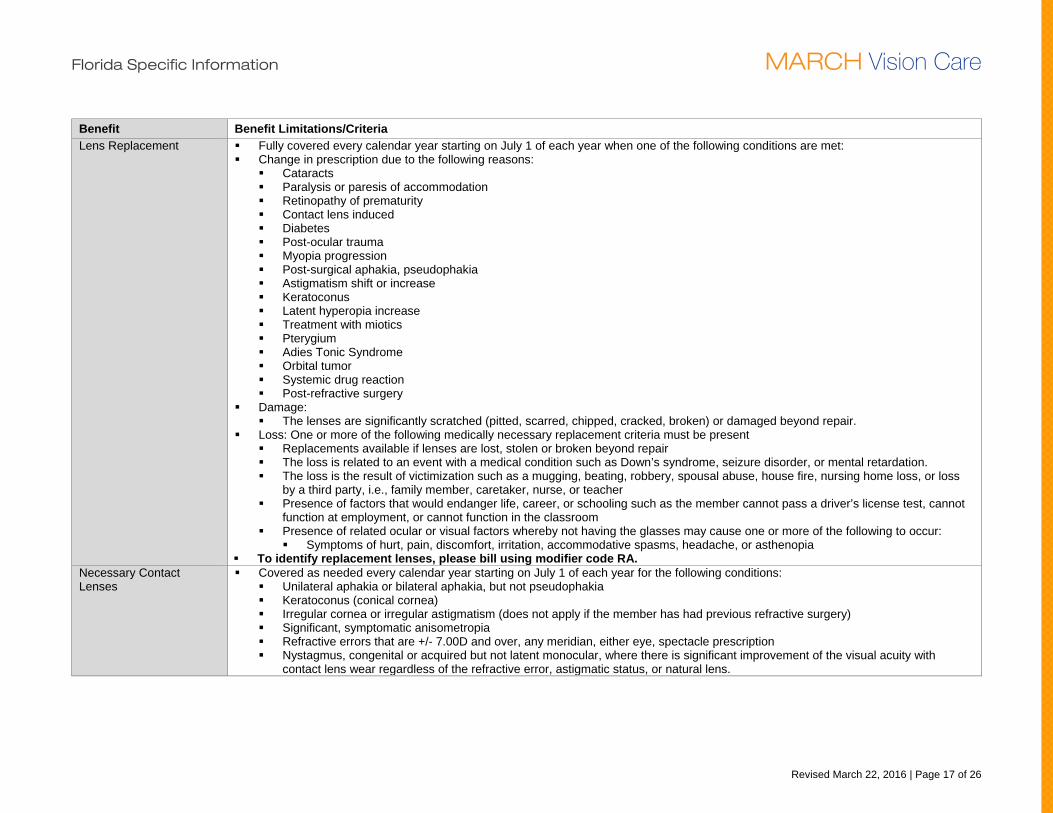
Benefit Benefit Limitations/Criteria Lens Replacement Fully covered every calendar year starting on July 1 of each year when one of the following conditions are met:
Change in prescription due to the following reasons: Cataracts Paralysis or paresis of accommodation Retinopathy of prematurity Contact lens induced Diabetes Post-ocular trauma Myopia progression Post-surgical aphakia, pseudophakia Astigmatism shift or increase Keratoconus Latent hyperopia increase Treatment with miotics Pterygium Adies Tonic Syndrome Orbital tumor Systemic drug reaction Post-refractive surgery
Damage: The lenses are significantly scratched (pitted, scarred, chipped, cracked, broken) or damaged beyond repair.
Loss: One or more of the following medically necessary replacement criteria must be present Replacements available if lenses are lost, stolen or broken beyond repair The loss is related to an event with a medical condition such as Down’s syndrome, seizure disorder, or mental retardation. The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia To identify replacement lenses, please bill using modifier code RA.
Necessary Contact Lenses
Covered as needed every calendar year starting on July 1 of each year for the following conditions: Unilateral aphakia or bilateral aphakia, but not pseudophakia Keratoconus (conical cornea) Irregular cornea or irregular astigmatism (does not apply if the member has had previous refractive surgery) Significant, symptomatic anisometropia Refractive errors that are +/- 7.00D and over, any meridian, either eye, spectacle prescription Nystagmus, congenital or acquired but not latent monocular, where there is significant improvement of the visual acuity with
contact lens wear regardless of the refractive error, astigmatic status, or natural lens.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 18 of 26
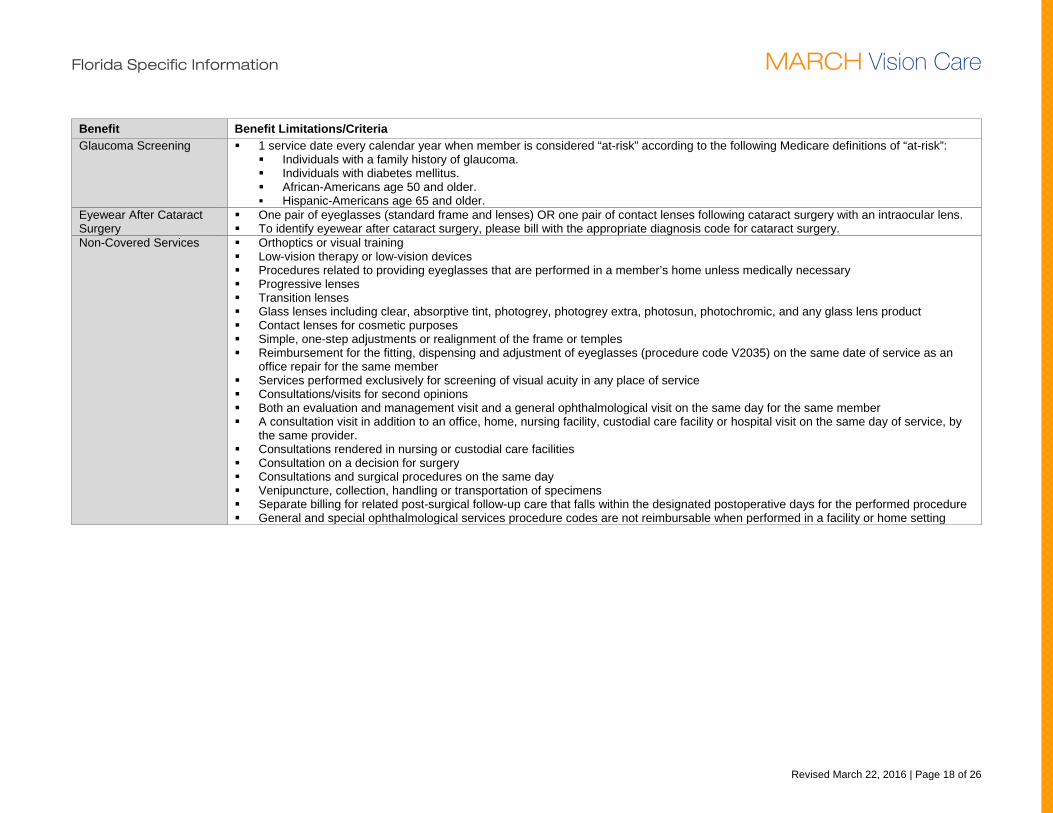
Benefit Benefit Limitations/Criteria Glaucoma Screening 1 service date every calendar year when member is considered “at-risk” according to the following Medicare definitions of “at-risk”:
Individuals with a family history of glaucoma. Individuals with diabetes mellitus. African-Americans age 50 and older. Hispanic-Americans age 65 and older.
Eyewear After Cataract Surgery
One pair of eyeglasses (standard frame and lenses) OR one pair of contact lenses following cataract surgery with an intraocular lens. To identify eyewear after cataract surgery, please bill with the appropriate diagnosis code for cataract surgery.
Non-Covered Services Orthoptics or visual training Low-vision therapy or low-vision devices Procedures related to providing eyeglasses that are performed in a member’s home unless medically necessary Progressive lenses Transition lenses Glass lenses including clear, absorptive tint, photogrey, photogrey extra, photosun, photochromic, and any glass lens product Contact lenses for cosmetic purposes Simple, one-step adjustments or realignment of the frame or temples Reimbursement for the fitting, dispensing and adjustment of eyeglasses (procedure code V2035) on the same date of service as an
office repair for the same member Services performed exclusively for screening of visual acuity in any place of service Consultations/visits for second opinions Both an evaluation and management visit and a general ophthalmological visit on the same day for the same member A consultation visit in addition to an office, home, nursing facility, custodial care facility or hospital visit on the same day of service, by
the same provider. Consultations rendered in nursing or custodial care facilities Consultation on a decision for surgery Consultations and surgical procedures on the same day Venipuncture, collection, handling or transportation of specimens Separate billing for related post-surgical follow-up care that falls within the designated postoperative days for the performed procedure General and special ophthalmological services procedure codes are not reimbursable when performed in a facility or home setting
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 19 of 26
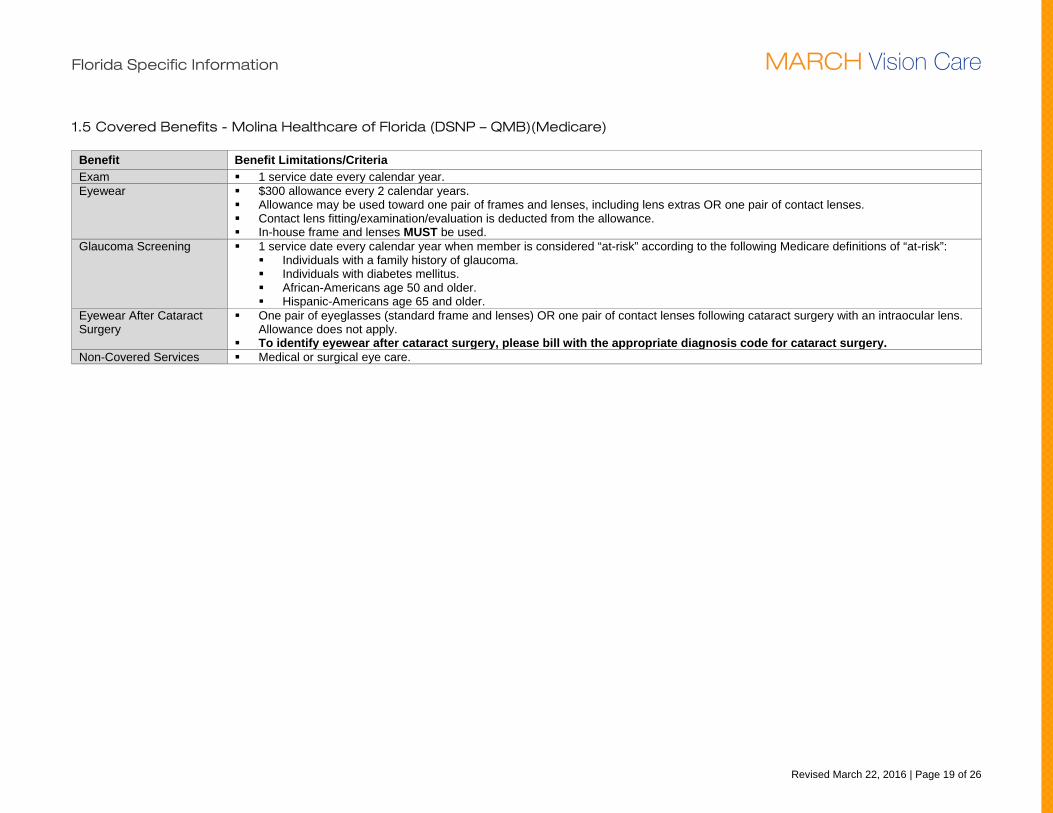
1.5 Covered Benefits - Molina Healthcare of Florida (DSNP – QMB)(Medicare)
Benefit Benefit Limitations/Criteria Exam 1 service date every calendar year. Eyewear $300 allowance every 2 calendar years.
Allowance may be used toward one pair of frames and lenses, including lens extras OR one pair of contact lenses. Contact lens fitting/examination/evaluation is deducted from the allowance. In-house frame and lenses MUST be used.
Glaucoma Screening 1 service date every calendar year when member is considered “at-risk” according to the following Medicare definitions of “at-risk”: Individuals with a family history of glaucoma. Individuals with diabetes mellitus. African-Americans age 50 and older. Hispanic-Americans age 65 and older.
Eyewear After Cataract Surgery
One pair of eyeglasses (standard frame and lenses) OR one pair of contact lenses following cataract surgery with an intraocular lens. Allowance does not apply.
To identify eyewear after cataract surgery, please bill with the appropriate diagnosis code for cataract surgery. Non-Covered Services Medical or surgical eye care.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 20 of 26
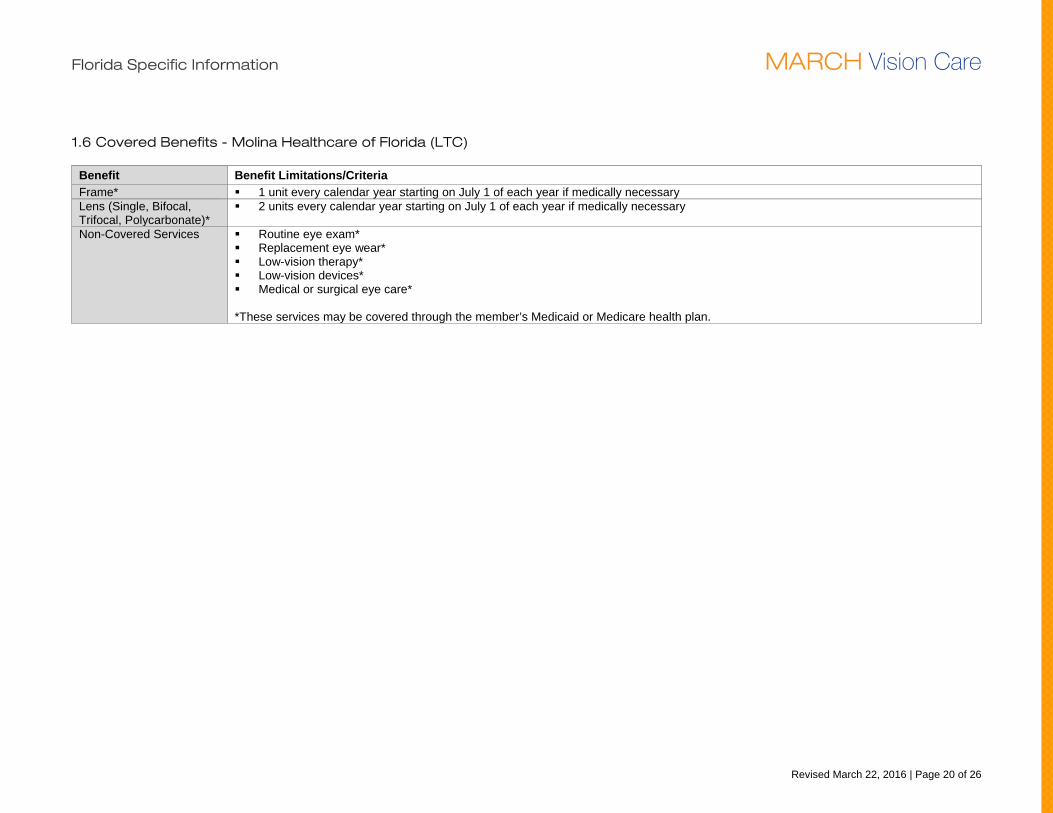
1.6 Covered Benefits - Molina Healthcare of Florida (LTC)
Benefit Benefit Limitations/Criteria Frame* 1 unit every calendar year starting on July 1 of each year if medically necessary Lens (Single, Bifocal, Trifocal, Polycarbonate)*
2 units every calendar year starting on July 1 of each year if medically necessary
Non-Covered Services Routine eye exam* Replacement eye wear* Low-vision therapy* Low-vision devices* Medical or surgical eye care* *These services may be covered through the member’s Medicaid or Medicare health plan.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 21 of 26
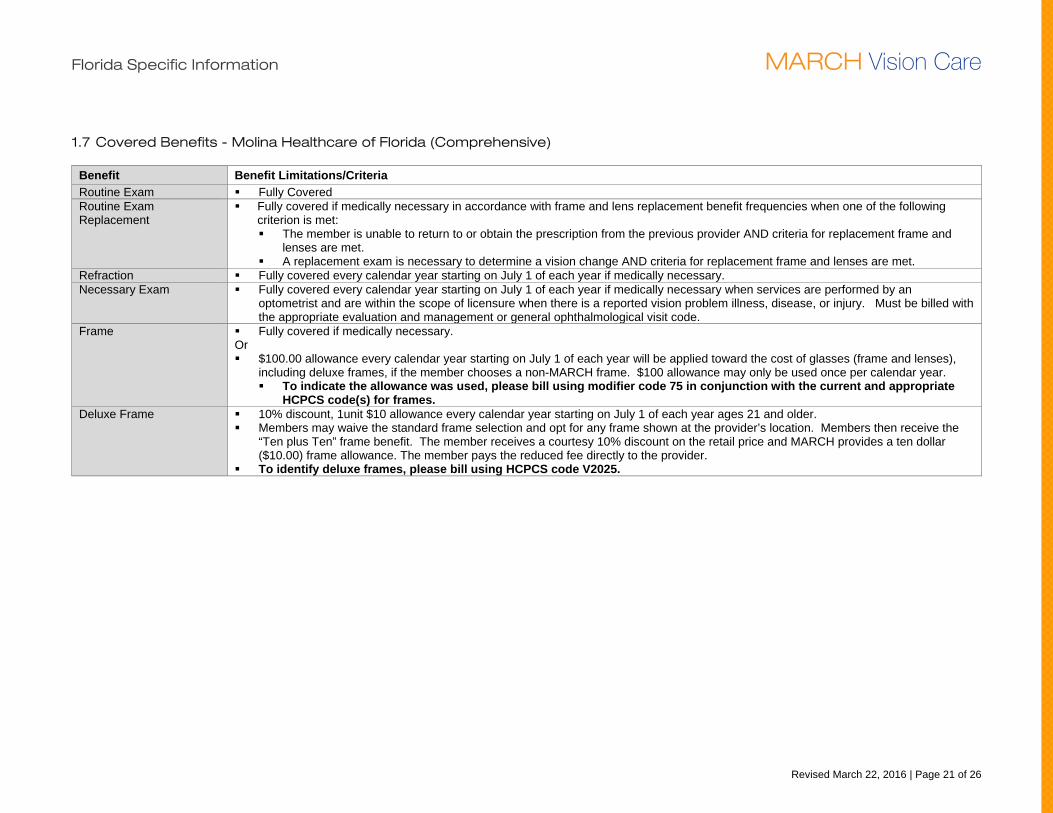
1.7 Covered Benefits - Molina Healthcare of Florida (Comprehensive)
Benefit Benefit Limitations/Criteria Routine Exam Fully Covered Routine Exam Replacement
Fully covered if medically necessary in accordance with frame and lens replacement benefit frequencies when one of the following criterion is met: The member is unable to return to or obtain the prescription from the previous provider AND criteria for replacement frame and
lenses are met. A replacement exam is necessary to determine a vision change AND criteria for replacement frame and lenses are met.
Refraction Fully covered every calendar year starting on July 1 of each year if medically necessary. Necessary Exam Fully covered every calendar year starting on July 1 of each year if medically necessary when services are performed by an
optometrist and are within the scope of licensure when there is a reported vision problem illness, disease, or injury. Must be billed with the appropriate evaluation and management or general ophthalmological visit code.
Frame Fully covered if medically necessary. Or $100.00 allowance every calendar year starting on July 1 of each year will be applied toward the cost of glasses (frame and lenses),
including deluxe frames, if the member chooses a non-MARCH frame. $100 allowance may only be used once per calendar year. To indicate the allowance was used, please bill using modifier code 75 in conjunction with the current and appropriate
HCPCS code(s) for frames. Deluxe Frame 10% discount, 1unit $10 allowance every calendar year starting on July 1 of each year ages 21 and older.
Members may waive the standard frame selection and opt for any frame shown at the provider’s location. Members then receive the “Ten plus Ten” frame benefit. The member receives a courtesy 10% discount on the retail price and MARCH provides a ten dollar ($10.00) frame allowance. The member pays the reduced fee directly to the provider.
To identify deluxe frames, please bill using HCPCS code V2025.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 22 of 26
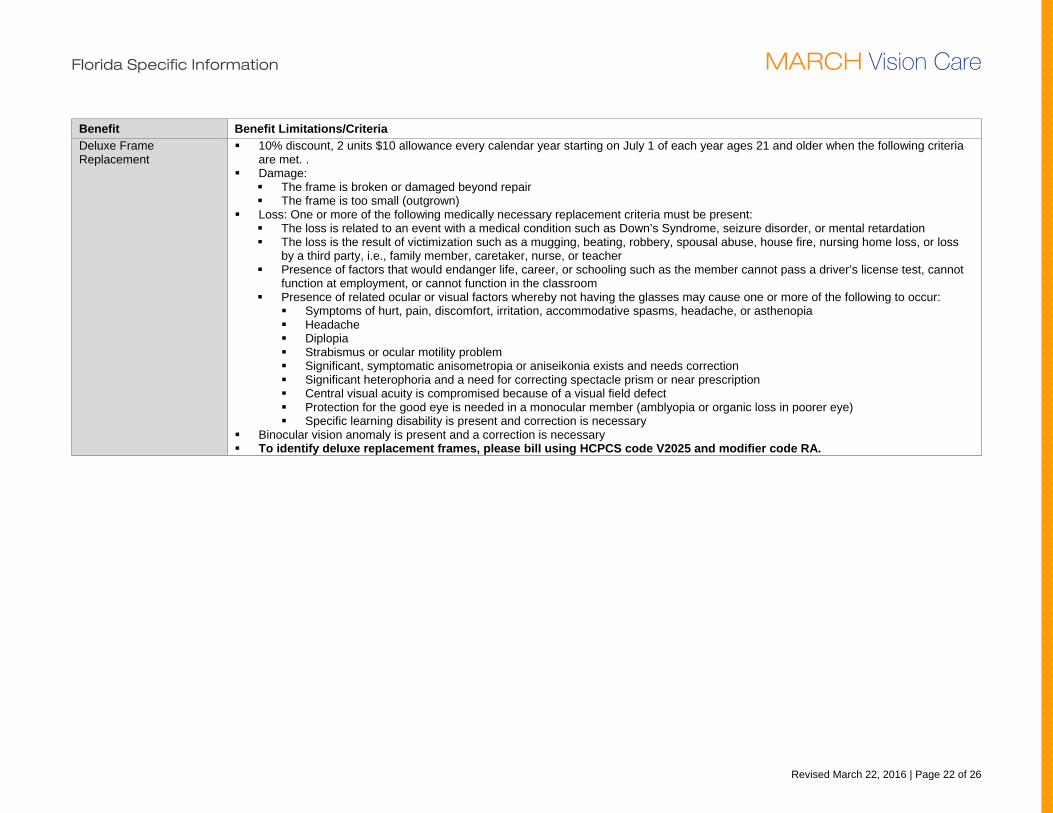
Benefit Benefit Limitations/Criteria Deluxe Frame Replacement
10% discount, 2 units $10 allowance every calendar year starting on July 1 of each year ages 21 and older when the following criteria are met. .
Damage: The frame is broken or damaged beyond repair The frame is too small (outgrown)
Loss: One or more of the following medically necessary replacement criteria must be present: The loss is related to an event with a medical condition such as Down’s Syndrome, seizure disorder, or mental retardation The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary
Binocular vision anomaly is present and a correction is necessary To identify deluxe replacement frames, please bill using HCPCS code V2025 and modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 23 of 26
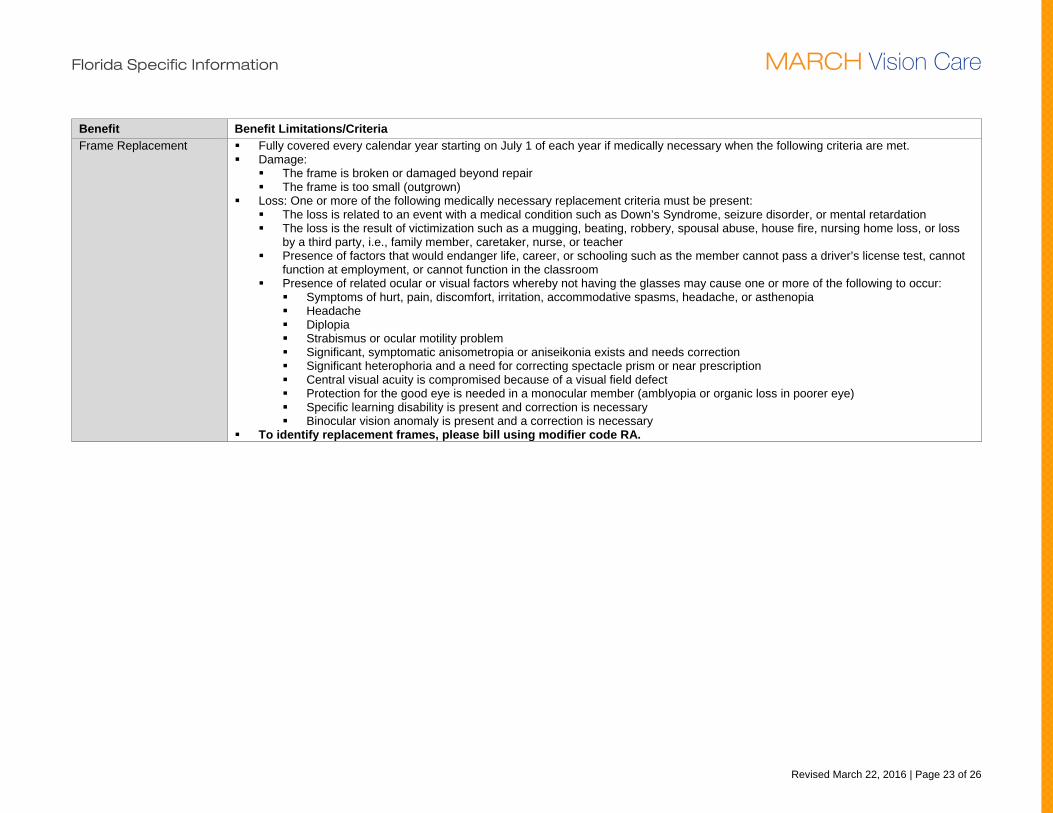
Benefit Benefit Limitations/Criteria Frame Replacement Fully covered every calendar year starting on July 1 of each year if medically necessary when the following criteria are met.
Damage: The frame is broken or damaged beyond repair The frame is too small (outgrown)
Loss: One or more of the following medically necessary replacement criteria must be present: The loss is related to an event with a medical condition such as Down’s Syndrome, seizure disorder, or mental retardation The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia Headache Diplopia Strabismus or ocular motility problem Significant, symptomatic anisometropia or aniseikonia exists and needs correction Significant heterophoria and a need for correcting spectacle prism or near prescription Central visual acuity is compromised because of a visual field defect Protection for the good eye is needed in a monocular member (amblyopia or organic loss in poorer eye) Specific learning disability is present and correction is necessary Binocular vision anomaly is present and a correction is necessary
To identify replacement frames, please bill using modifier code RA.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 24 of 26
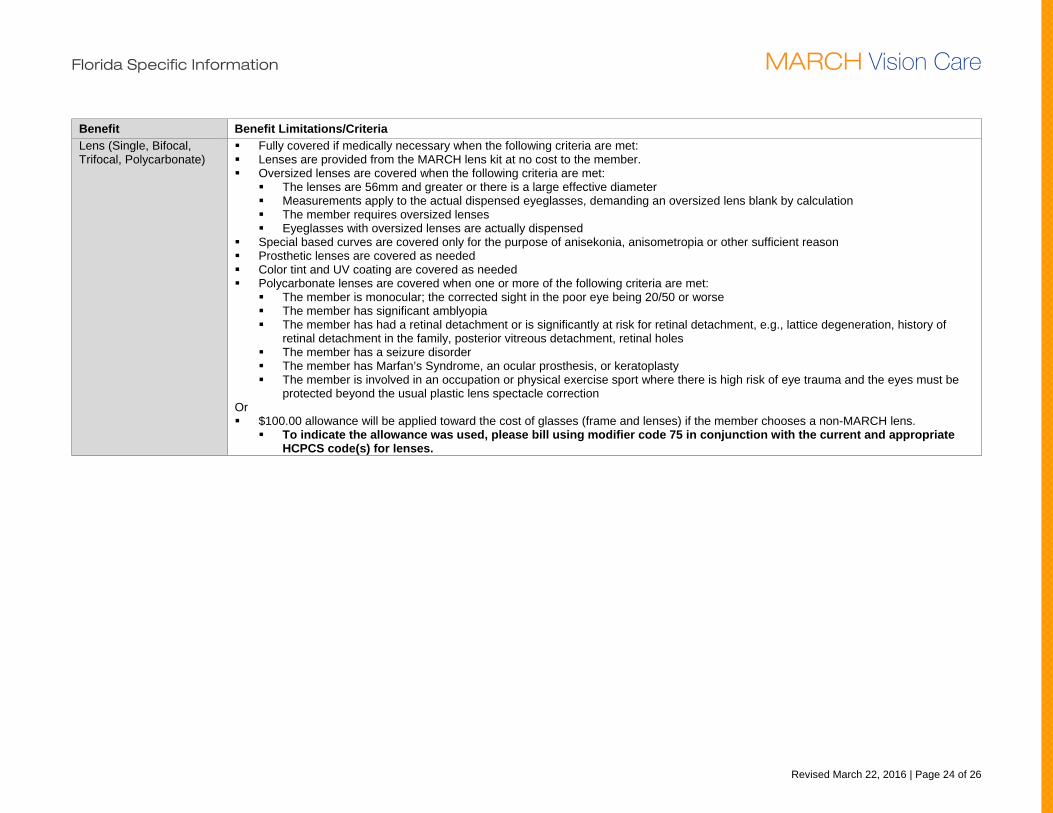
Benefit Benefit Limitations/Criteria Lens (Single, Bifocal, Trifocal, Polycarbonate)
Fully covered if medically necessary when the following criteria are met: Lenses are provided from the MARCH lens kit at no cost to the member. Oversized lenses are covered when the following criteria are met:
The lenses are 56mm and greater or there is a large effective diameter Measurements apply to the actual dispensed eyeglasses, demanding an oversized lens blank by calculation The member requires oversized lenses Eyeglasses with oversized lenses are actually dispensed
Special based curves are covered only for the purpose of anisekonia, anisometropia or other sufficient reason Prosthetic lenses are covered as needed Color tint and UV coating are covered as needed Polycarbonate lenses are covered when one or more of the following criteria are met:
The member is monocular; the corrected sight in the poor eye being 20/50 or worse The member has significant amblyopia The member has had a retinal detachment or is significantly at risk for retinal detachment, e.g., lattice degeneration, history of
retinal detachment in the family, posterior vitreous detachment, retinal holes The member has a seizure disorder The member has Marfan’s Syndrome, an ocular prosthesis, or keratoplasty The member is involved in an occupation or physical exercise sport where there is high risk of eye trauma and the eyes must be
protected beyond the usual plastic lens spectacle correction Or $100.00 allowance will be applied toward the cost of glasses (frame and lenses) if the member chooses a non-MARCH lens.
To indicate the allowance was used, please bill using modifier code 75 in conjunction with the current and appropriate HCPCS code(s) for lenses.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 25 of 26
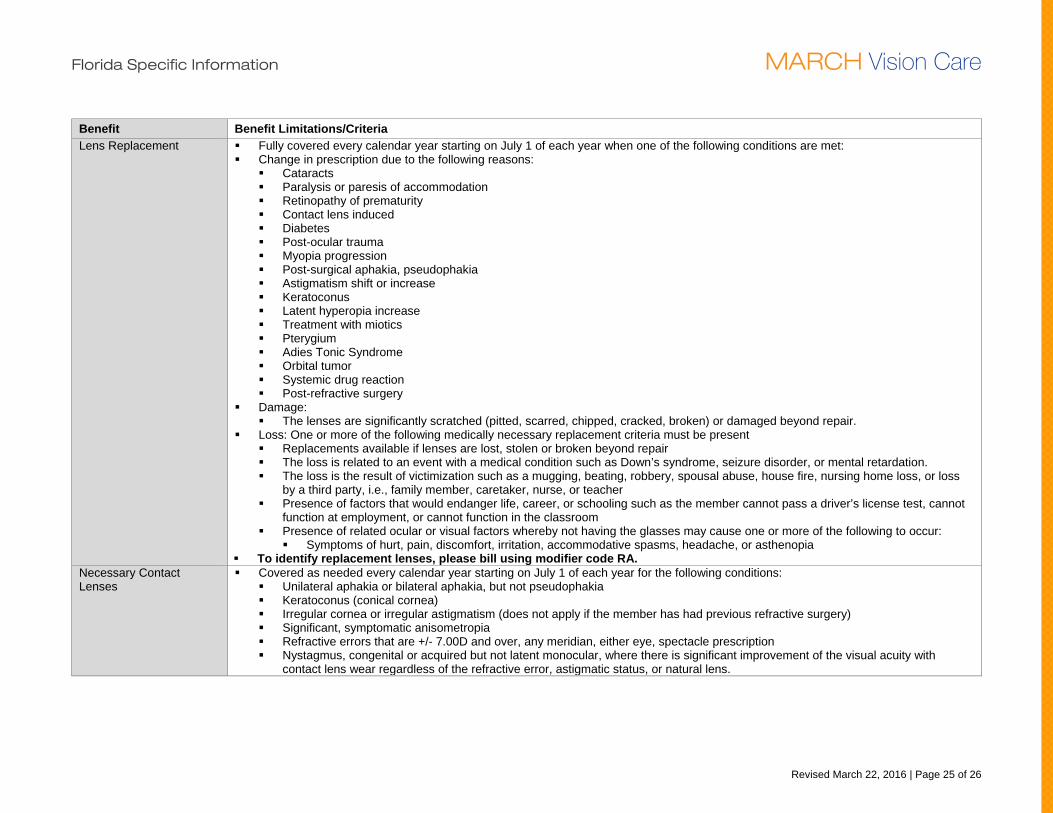
Benefit Benefit Limitations/Criteria Lens Replacement Fully covered every calendar year starting on July 1 of each year when one of the following conditions are met:
Change in prescription due to the following reasons: Cataracts Paralysis or paresis of accommodation Retinopathy of prematurity Contact lens induced Diabetes Post-ocular trauma Myopia progression Post-surgical aphakia, pseudophakia Astigmatism shift or increase Keratoconus Latent hyperopia increase Treatment with miotics Pterygium Adies Tonic Syndrome Orbital tumor Systemic drug reaction Post-refractive surgery
Damage: The lenses are significantly scratched (pitted, scarred, chipped, cracked, broken) or damaged beyond repair.
Loss: One or more of the following medically necessary replacement criteria must be present Replacements available if lenses are lost, stolen or broken beyond repair The loss is related to an event with a medical condition such as Down’s syndrome, seizure disorder, or mental retardation. The loss is the result of victimization such as a mugging, beating, robbery, spousal abuse, house fire, nursing home loss, or loss
by a third party, i.e., family member, caretaker, nurse, or teacher Presence of factors that would endanger life, career, or schooling such as the member cannot pass a driver’s license test, cannot
function at employment, or cannot function in the classroom Presence of related ocular or visual factors whereby not having the glasses may cause one or more of the following to occur:
Symptoms of hurt, pain, discomfort, irritation, accommodative spasms, headache, or asthenopia To identify replacement lenses, please bill using modifier code RA.
Necessary Contact Lenses
Covered as needed every calendar year starting on July 1 of each year for the following conditions: Unilateral aphakia or bilateral aphakia, but not pseudophakia Keratoconus (conical cornea) Irregular cornea or irregular astigmatism (does not apply if the member has had previous refractive surgery) Significant, symptomatic anisometropia Refractive errors that are +/- 7.00D and over, any meridian, either eye, spectacle prescription Nystagmus, congenital or acquired but not latent monocular, where there is significant improvement of the visual acuity with
contact lens wear regardless of the refractive error, astigmatic status, or natural lens.
Florida Specific Information MARCH Vision Care
Revised March 22, 2016 | Page 26 of 26
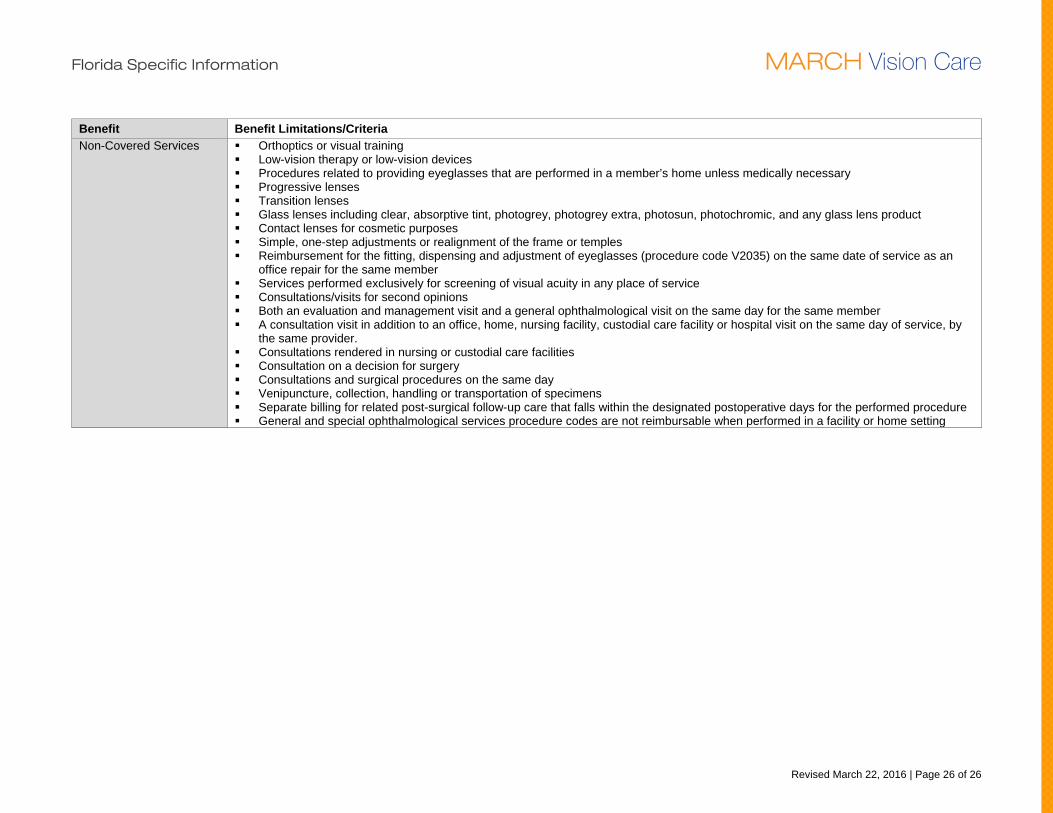
Benefit Benefit Limitations/Criteria Non-Covered Services Orthoptics or visual training
Low-vision therapy or low-vision devices Procedures related to providing eyeglasses that are performed in a member’s home unless medically necessary Progressive lenses Transition lenses Glass lenses including clear, absorptive tint, photogrey, photogrey extra, photosun, photochromic, and any glass lens product Contact lenses for cosmetic purposes Simple, one-step adjustments or realignment of the frame or temples Reimbursement for the fitting, dispensing and adjustment of eyeglasses (procedure code V2035) on the same date of service as an
office repair for the same member Services performed exclusively for screening of visual acuity in any place of service Consultations/visits for second opinions Both an evaluation and management visit and a general ophthalmological visit on the same day for the same member A consultation visit in addition to an office, home, nursing facility, custodial care facility or hospital visit on the same day of service, by
the same provider. Consultations rendered in nursing or custodial care facilities Consultation on a decision for surgery Consultations and surgical procedures on the same day Venipuncture, collection, handling or transportation of specimens Separate billing for related post-surgical follow-up care that falls within the designated postoperative days for the performed procedure General and special ophthalmological services procedure codes are not reimbursable when performed in a facility or home setting