Embed Size (px)
Citation preview

Dermatologic surgery
Surgical treatment of basal cell carcinoma of the nail unit
Ikue Shimizu1, MD, Philip R. Cohen2–4, MD, and Deborah F. MacFarlane2, MD
1Department of Dermatology, Texas Tech
University Health Sciences Center,
Lubbock, 2Department of Dermatology,
University of Texas MD Anderson Cancer
Center, Houston, 3University of Houston
Health Center, University of Houston,
Houston, and 4Department of Dermatology,
University of Texas Medical School at
Houston, Houston, TX, USA
Correspondence
Ikue Shimizu, MD
Department of Dermatology
Texas Tech University Health Sciences
Center
3601 4th Street MS 9400
Lubbock
TX 79430
USA
E-mail: [email protected]
Conflicts of interest: None.
Introduction
Basal cell carcinoma (BCC) has variable clinical and path-ologic presentations. However, nail unit involvement isexceedingly rare. We present an unusual case of two nailunit BCCs arising in a single patient, where treatmentwith Mohs micrographic surgery (MMS) followed bygranulation resulted in excellent nail regrowth.
Case report
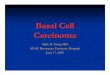
A 68-year-old woman with a medical history of breastcancer, renal cell cancer, follicular cell lymphoma, andnon-melanoma skin cancers presented to the dermatologyservice with a pruritic, pink plaque on the right fifth digit.This had initially been diagnosed – more than a decadeearlier – as dermatitis; however, there was no resolutionfollowing six months of topical steroid use. In theinterim, she also developed a tender, subungual mass onthe left thumb. There was a maternal family history ofskin cancers but no significant exposure to carcinogenicchemicals or digital trauma.On physical exam, a 2.0 9 1.5 cm plaque extended
from the distal interphalangeal joint to the fingertip on
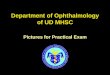
the right fifth digit (Fig. 1a). On the left thumb, a0.8 cm pink papule was noted beneath the nail plate(Fig. 1b). Biopsy revealed superficial BCC on the rightfifth digit and superficial and nodular BCC on the leftthumb.Both lesions were treated with MMS followed by gran-
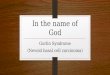
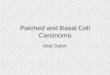
ulation. The right fifth digit required two stages of MMS(Fig. 2a); the left thumb required three stages (Fig. 2b,c).The postoperative outcome was excellent, and the patientwas pleased with the cosmetic and functional results(Fig. 3 a,b).
Discussion
BCC is the most prevalent skin cancer. However, it is therarest nail tumor.1,2 Including this patient, there are cur-rently 28 patients and 29 cases of nail unit BCC in the lit-erature.3 The thumb is the most commonly involved digit(13 cases), and fingers are more commonly involved thantoes. Clinical presentation is variable, ranging fromlesions mimicking periungual dermatitis to subungualmasses. The nonspecific appearance can delay diagnosis,and the differential diagnosis includes both malignant andbenign conditions. The pathogenesis is not entirely clear.
International Journal of Dermatology 2013, 52, 996–998 ª 2013 The International Society of Dermatology
996
Although BCC elsewhere is known to be related to ultra-violet radiation, nail unit BCC is infrequent despite digitsbeing relatively well exposed. Some have speculated about
the role of trauma,4,5 carcinogens (azo dyes6 andarsenic7), and chronic radiation exposure.8
As with all nail unit tumors, ruling out bony involve-ment with radiologic imaging is recommended beforetreatment. Surgical modalities are preferred to ensurecomplete clearance and margin confirmation. In the past,amputation was a common treatment for nail unit carci-nomas9 and is still performed today,10 though definitive,amputation confers significant morbidity. Excision withmargins and en bloc nail unit excision will preserve digitfunction. With the former, standard 3–4 mm marginsmay disrupt the matrix; some may opt for the latter tocompletely avoid dystrophic nail plate growth.Preserving the matrix whenever possible can prevent nail
plate loss or dystrophy. Matricectomy does not need to beperformed as long as margins are clear. In recent years,MMS has emerged as the option offering the best tissuepreservation for nail tumors. It is currently established asthe treatment of choice for nail unit squamous cell carci-noma without bony involvement due to high cure rates andmaximal preservation of tissue11–13; the same principlesapply to nail unit basal cell carcinoma. MMS has been usedfor 12 nail unit BCCs, including ours; no recurrences havebeen noted. Clear margins may be achieved with carefulorientation of the tissue specimen and knowledge of theunique histology and anatomy of the nail unit.As our case demonstrates, complicated repair is often
unnecessary as long as the matrix is intact. With diligentapplication of antibiotic ointment and an occlusive dress-ing, granulation will result in excellent functional andcosmetic outcome.9,11,14 While full-thickness skin graftsmay result in quicker healing, long-term outcome is
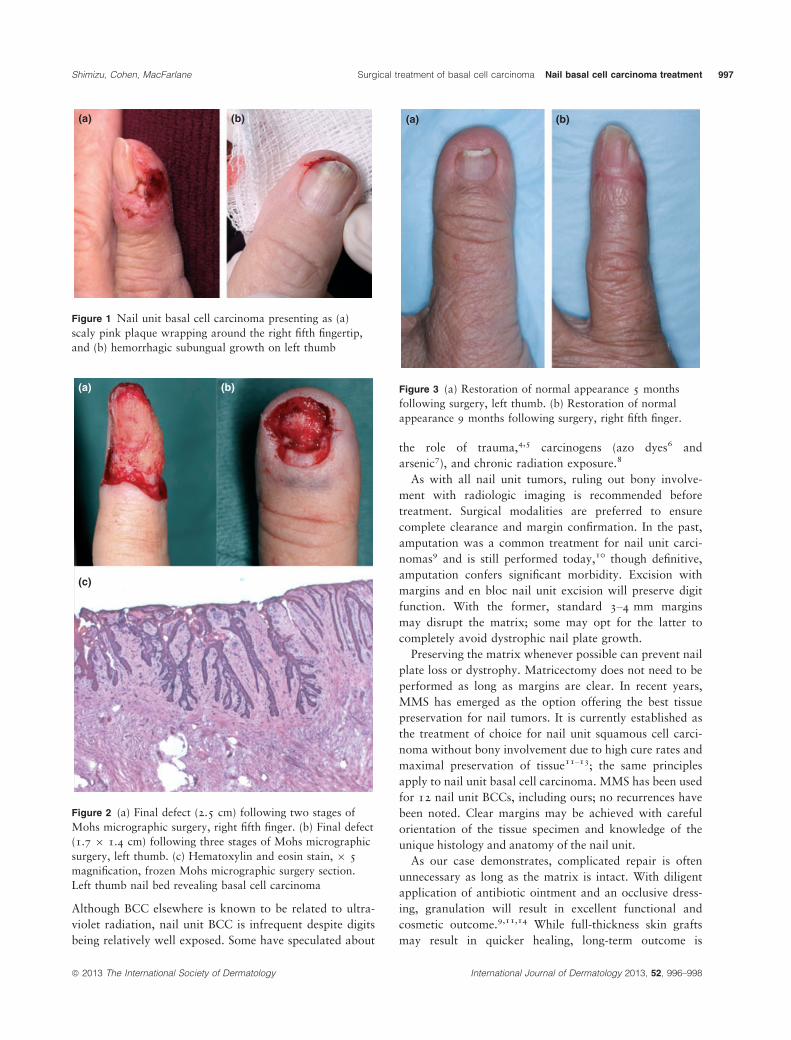
Figure 3 (a) Restoration of normal appearance 5 monthsfollowing surgery, left thumb. (b) Restoration of normalappearance 9 months following surgery, right fifth finger.
Figure 2 (a) Final defect (2.5 cm) following two stages ofMohs micrographic surgery, right fifth finger. (b) Final defect(1.7 9 1.4 cm) following three stages of Mohs micrographicsurgery, left thumb. (c) Hematoxylin and eosin stain, 9 5magnification, frozen Mohs micrographic surgery section.Left thumb nail bed revealing basal cell carcinoma
Figure 1 Nail unit basal cell carcinoma presenting as (a)scaly pink plaque wrapping around the right fifth fingertip,and (b) hemorrhagic subungual growth on left thumb
ª 2013 The International Society of Dermatology International Journal of Dermatology 2013, 52, 996–998
Shimizu, Cohen, MacFarlane Surgical treatment of basal cell carcinoma Nail basal cell carcinoma treatment 997

similar to granulation.4,15 Repair after partial or completenail unit excision may also include microsurgical nailtransfers, nail bed grafts, and a variety of locoregionalflaps.16,17
Nail unit BCC is a rare entity that, if diagnosed earlyand treated appropriately, results in a functional and nor-mal-appearing nail. It tends to be clinically nonspecific,and any non-resolving dermatitis or new nail unit growthneeds to be biopsied. MMS to preserve matrix followedby granulation can provide excellent results.
References
1 Grine RC, Parlette HL III, Wilson BB. Nail unit basal cellcarcinoma: a case report and literature review. J AmAcad Dermatol 1997; 37: 790–792.
2 Salasche SJ, Garland LD. Tumors of the nail. Derm Clin
1985; 3: 501–519.3 Bandyopadhyay D, Sen S. Periungual basal cell
carcinoma: a case report with review of literature. IndianJ Dermatol 2011; 56: 220–222.
4 Guana AL, Kolbusz R, Goldberg LH. Basal cellcarcinoma on the nailfold of the right thumb. Int JDermatol 1994; 33: 204–205.
5 Nelson LM, Hamilton CF. Primary carcinoma of the nailbed. Arch Dermatol 1970; 101: 63–67.
6 Engel E, Ulrich H, Vasold R, et al. Azo pigments and abasal cell carcinoma at the thumb. Dermatology 2008;216: 76–80.
7 Kim HJ, Kim YS, Suhr KB, et al. Basal cell carcinoma ofthe nail bed in a Korean woman. Int J Dermatol 2000;39: 397–398.
8 Serrano-Ortega S, Fernandez-Angel I, Dulanto-Campos E,et al. Basal cell carcinoma arising in professionalradiodermatitis of the nail. Br J Dermatol 2002; 147:628–629.
9 Zaiac MN, Weiss E. Mohs micrographic surgery of thenail unit and squamous cell carcinoma. Dermatol Surg
2001; 27: 246–251.10 Galeano M, Lentini M, Stagno DAlcontres F, et al.
Bowenoid basal cell carcinoma of the thumb: a casereport and review of the literature. Hand Surg 2002; 7:295–298.
11 Goldminz D, Bennett RG. Mohs micrographic surgery ofthe nail unit. J Dermatol Surg Oncol 1992; 18: 721–726.
12 Jellinek NJ. Primary malignant tumors of the nail unit.Adv Dermatol 2005; 21: 33–64.
13 Joyner KS, Wilson B, Wagner RF, et al. Marginalexcision of squamous cell carcinomas of the hand.Orthopedics 2008; 31: 79.
14 Martinelli PT, Cohen PR, Schulze KE, et al. Periungualbasal cell carcinoma: case report and literature review.Dermatol Surg 2006; 32: 320–323.
15 Forman SB, Ferringer TC, Garrett AB. Basal cellcarcinoma of the nail unit. J Am Acad Dermatol 2007;56: 811–814.
16 Mehrara BJ, Abood AA, Disa JJ, et al. Thumbreconstruction following resection for malignant tumors.Plast Reconstr Surg 2008; 121: 1279–1287.
17 Puhaindran ME, Cordeiro PG, Disa JJ, et al. Full-thickness skin graft after nail complex resection formalignant tumors. Tech Hand Up Extrem Surg 2011; 15:84–86.
International Journal of Dermatology 2013, 52, 996–998 ª 2013 The International Society of Dermatology
Nail basal cell carcinoma treatment Surgical treatment of basal cell carcinoma Shimizu, Cohen, MacFarlane998