Embed Size (px)
Citation preview
Basal Cell Basal Cell CarcinomaCarcinoma
Mark H. Tseng MDMark H. Tseng MDSUNY Downstate University HospitalSUNY Downstate University Hospital
June 17, 2005June 17, 2005
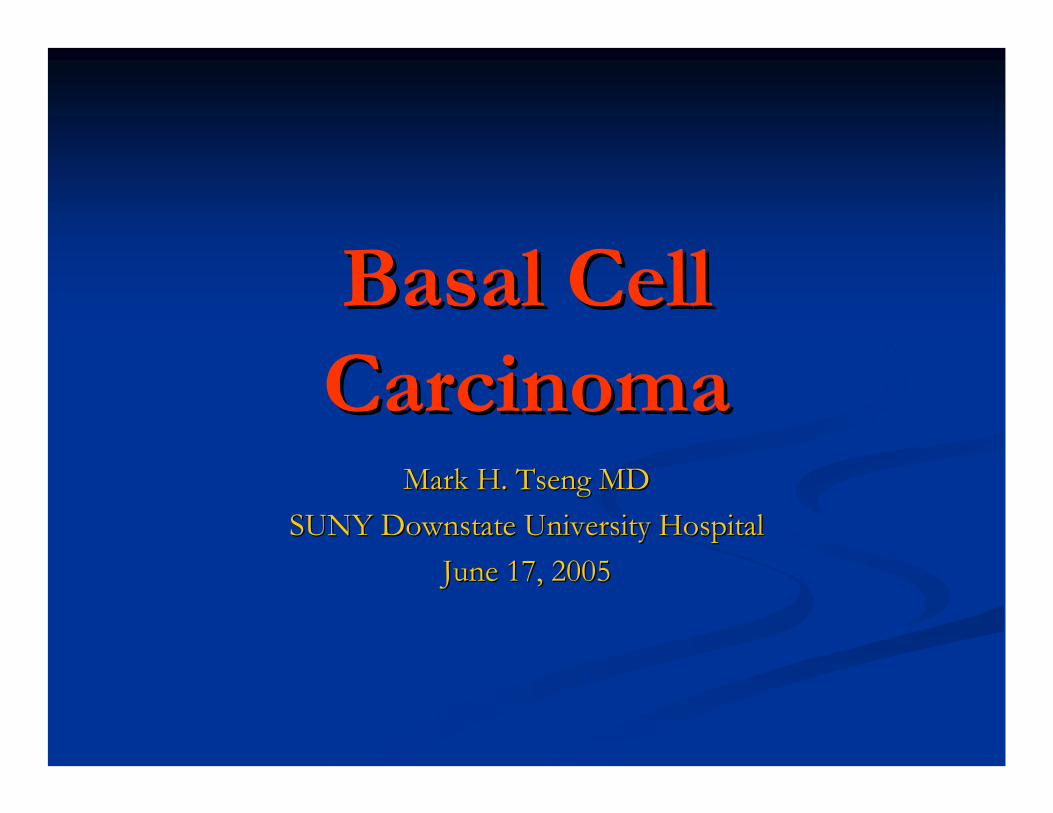
HistoryHistory
Discrete, raised, circular ulceration. Discrete, raised, circular ulceration.
HistoryHistory
Pt was admitted to xx Hospital in 2005 for Pt was admitted to xx Hospital in 2005 for bleeding. He was transfused 5 units of bleeding. He was transfused 5 units of blood. blood.
HistoryHistory
Pt arrived at SUNY Downstate on xx Pt arrived at SUNY Downstate on xx 2005. He was evaluated and biopsies of 2005. He was evaluated and biopsies of the margins was taken. Path came back the margins was taken. Path came back negative and surgery was scheduled.negative and surgery was scheduled.
HistoryHistory
PMH: NonePMH: NonePSH: TonsillectomyPSH: TonsillectomyFamily Family HxHx: None: NoneSocial Social HxHx: : ----Habits: Habits: --------------Allergies: NKDAAllergies: NKDAMEDS: MultivitaminsMEDS: Multivitamins
VitalsVitals
Temperature: 98.8FTemperature: 98.8FBlood Pressure: 120/73Blood Pressure: 120/73Heart Rate: 90Heart Rate: 90Respiratory Rate: 14Respiratory Rate: 14Saturation: 99% on room airSaturation: 99% on room air
Physical ExamPhysical Exam
General: Appears age appropriateGeneral: Appears age appropriateHEENT: large ulcer extending to HEENT: large ulcer extending to
left neck, friable, no active left neck, friable, no active bleeding.bleeding.
Chest: large left mass/ulcer approx. Chest: large left mass/ulcer approx. 3 feet x 3 feet extending from: 3 feet x 3 feet extending from: Anterior: chestAnterior: chestLateral: shoulderLateral: shoulderMedial: neckMedial: neckPosterior: Back Posterior: Back
Lung: CTA bilaterally, no wheezing, Lung: CTA bilaterally, no wheezing, no no ralesrales
Heart: S1S2Heart: S1S2Abdomen: soft, Abdomen: soft, ntnt, , ndnd, +, +bsbs
LABSLABS
5/3/05 pre5/3/05 pre--op: op: WbcWbc: 9 H/H: 10/33 : 9 H/H: 10/33 PltPlt: 408: 408Na: 136 K: 4.6 Na: 136 K: 4.6 ClCl: 101 HCO3: 23 BUN: 21: 101 HCO3: 23 BUN: 21CreaCrea: 1.1 Glucose: 69 Alb: 3.1 PT: 14.5 : 1.1 Glucose: 69 Alb: 3.1 PT: 14.5 INR: 1.2 PTT: 26INR: 1.2 PTT: 26
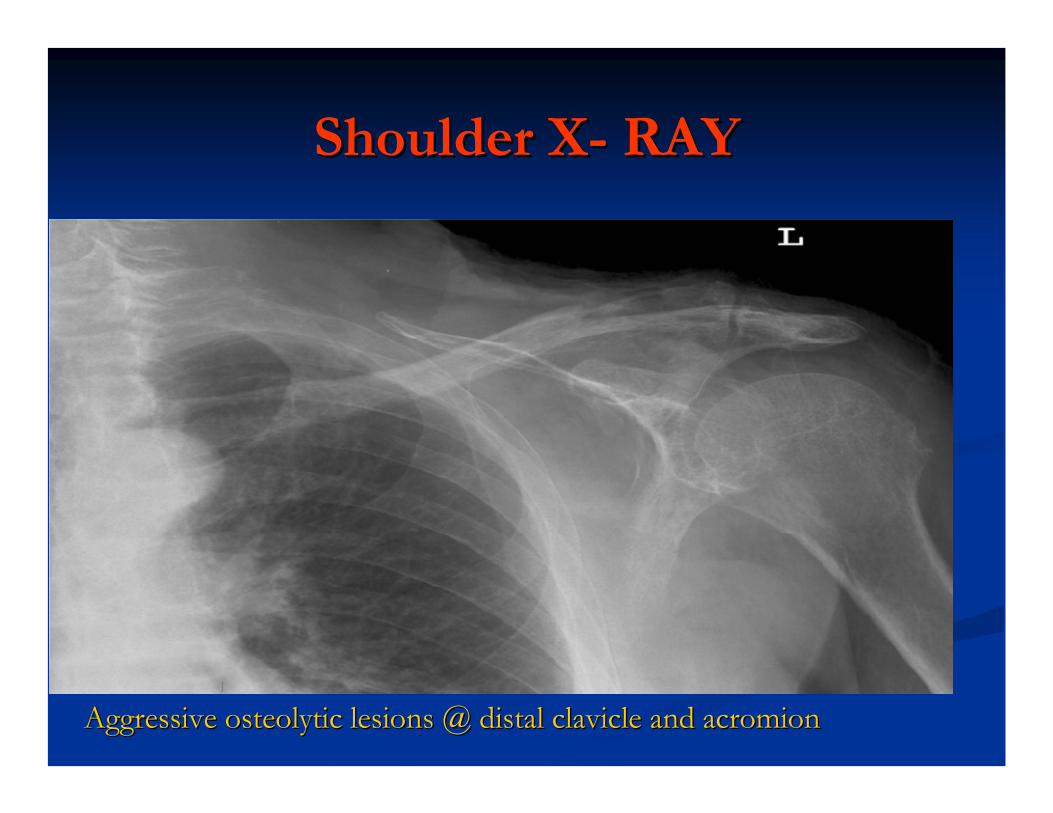
Shoulder XShoulder X-- RAYRAY
Picture1 Picture1 copy.pngcopy.png
Aggressive Aggressive osteolyticosteolytic lesions @ distal clavicle and lesions @ distal clavicle and acromionacromion
HistoryHistory
Because of the large area of ulceration, the depth Because of the large area of ulceration, the depth of invasion, and the vital structures involved. of invasion, and the vital structures involved.
A team of surgeon from various surgical specialties A team of surgeon from various surgical specialties were involved.were involved.
-- General SurgeryGeneral Surgery-- Plastic SurgeryPlastic Surgery-- Orthopedics SurgeryOrthopedics Surgery-- Vascular SurgeryVascular Surgery

Operating TeamOperating Team
Dr. Dr. BakshandehBakshandeh Dr. SchwartzmanDr. Schwartzman Dr. DeitchDr. Deitch
IntraIntra--opop
Taken to OR and Taken to OR and intubatedintubated..

IntraIntra--op: resectionop: resection
Incision through skin, Incision through skin, subQsubQ, fat, to level of fascia., fat, to level of fascia.
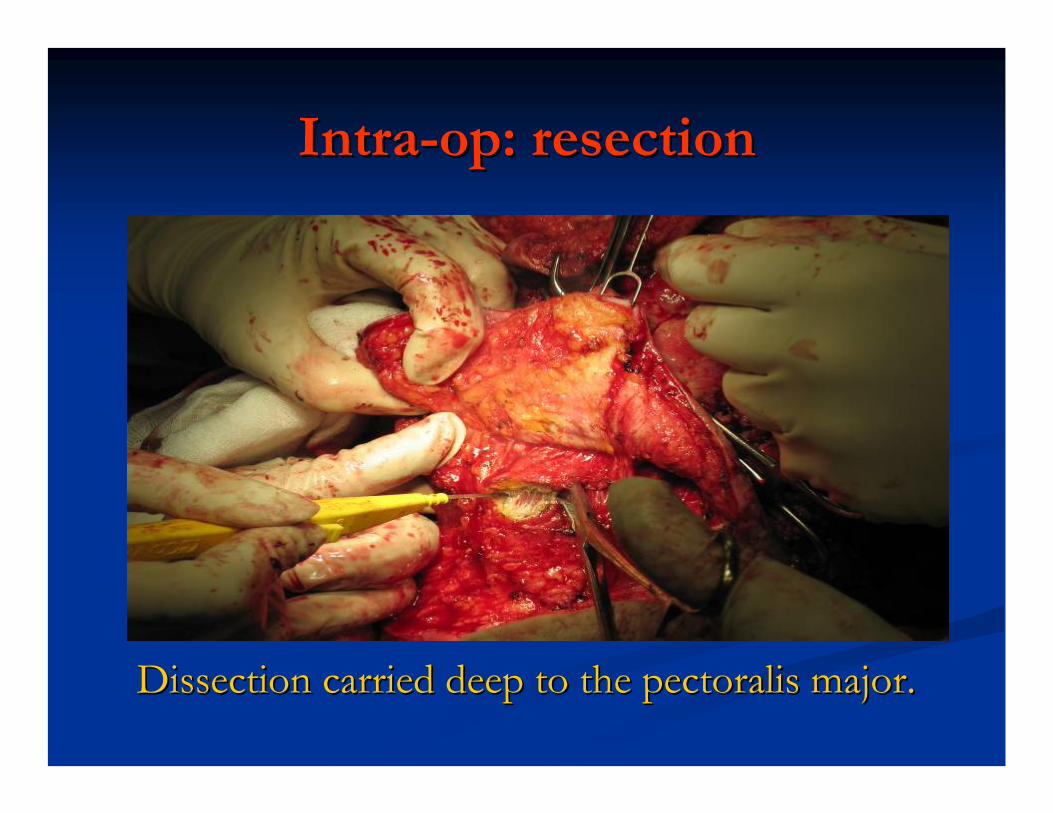
IntraIntra--op: resectionop: resection
Dissection carried deep to the Dissection carried deep to the pectoralispectoralis major.major.
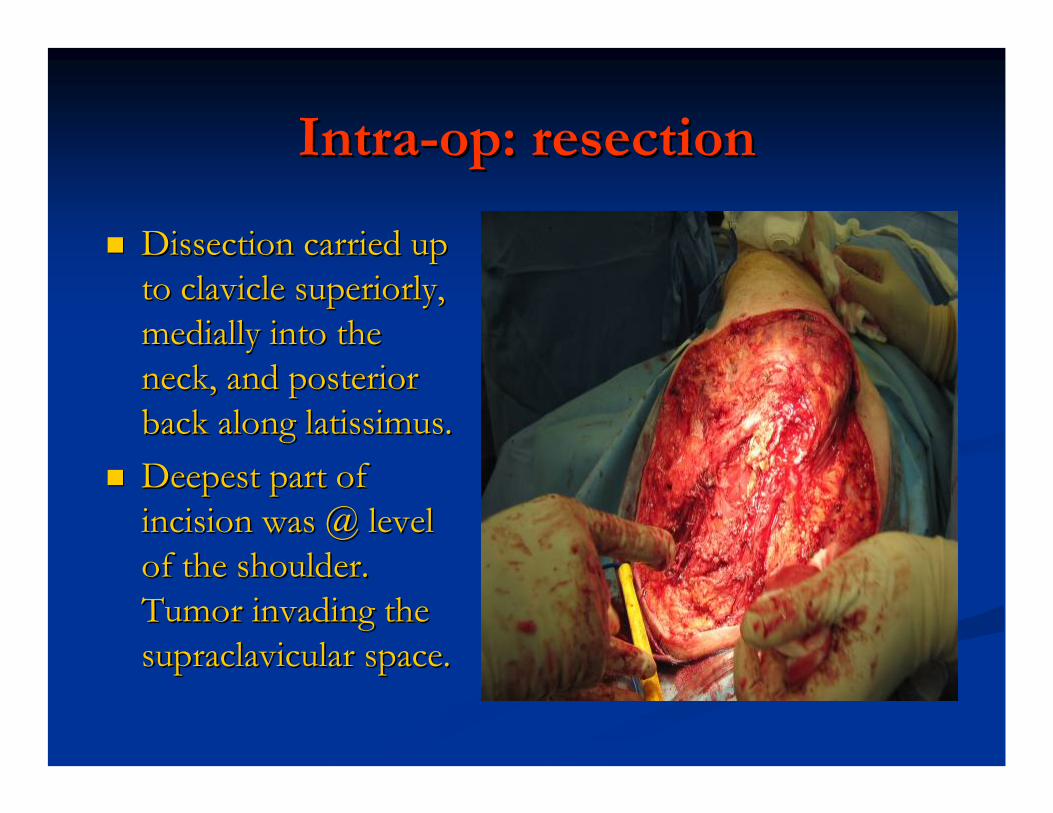
IntraIntra--op: resectionop: resection
Dissection carried up Dissection carried up to clavicle superiorly, to clavicle superiorly, medially into the medially into the neck, and posterior neck, and posterior back along back along latissimuslatissimus..Deepest part of Deepest part of incision was @ level incision was @ level of the shoulder. of the shoulder. Tumor invading the Tumor invading the supraclavicularsupraclavicular space.space.
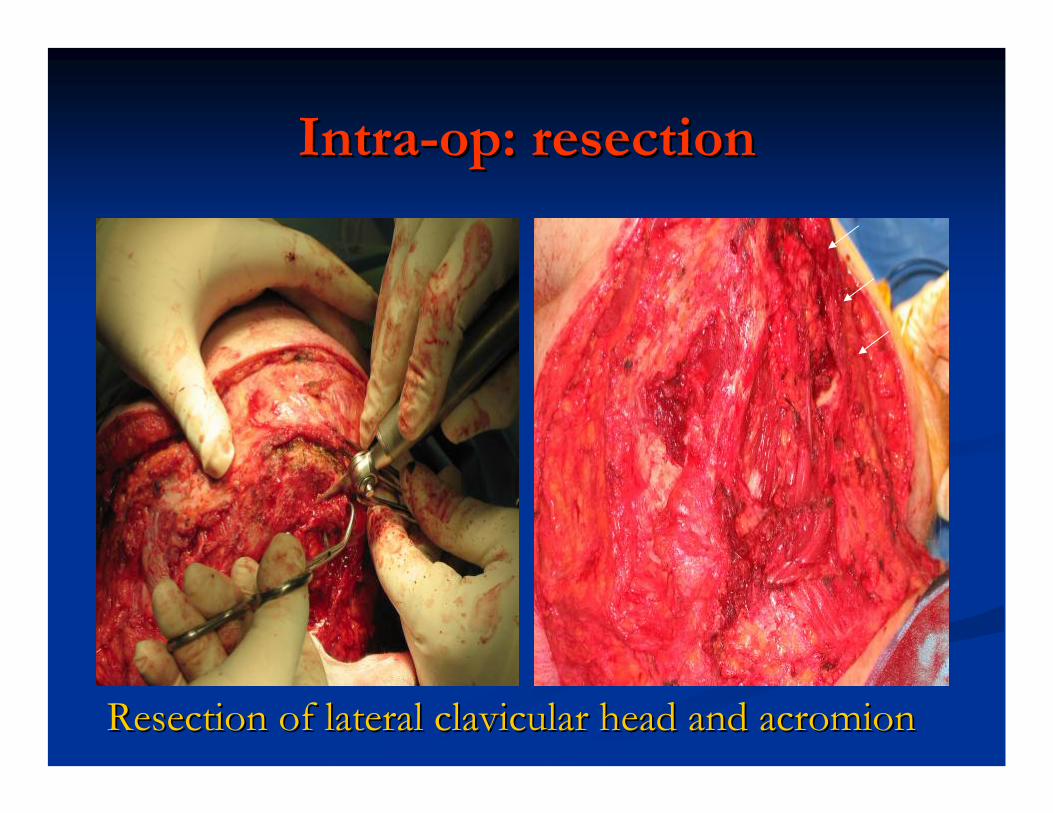
IntraIntra--op: resectionop: resection
Resection of lateral Resection of lateral clavicularclavicular head and head and acromionacromion
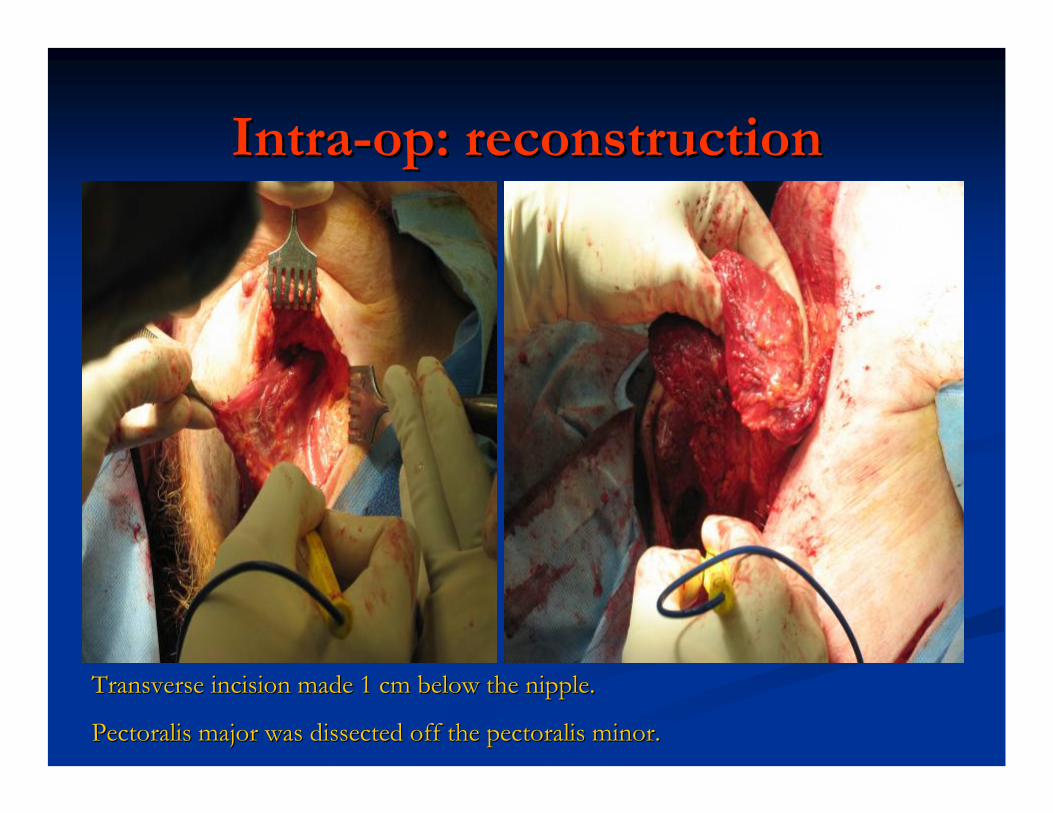
IntraIntra--op: reconstructionop: reconstruction
Transverse incision made 1 cm below the nipple.Transverse incision made 1 cm below the nipple.
PectoralisPectoralis major was dissected off the major was dissected off the pectoralispectoralis minor.minor.
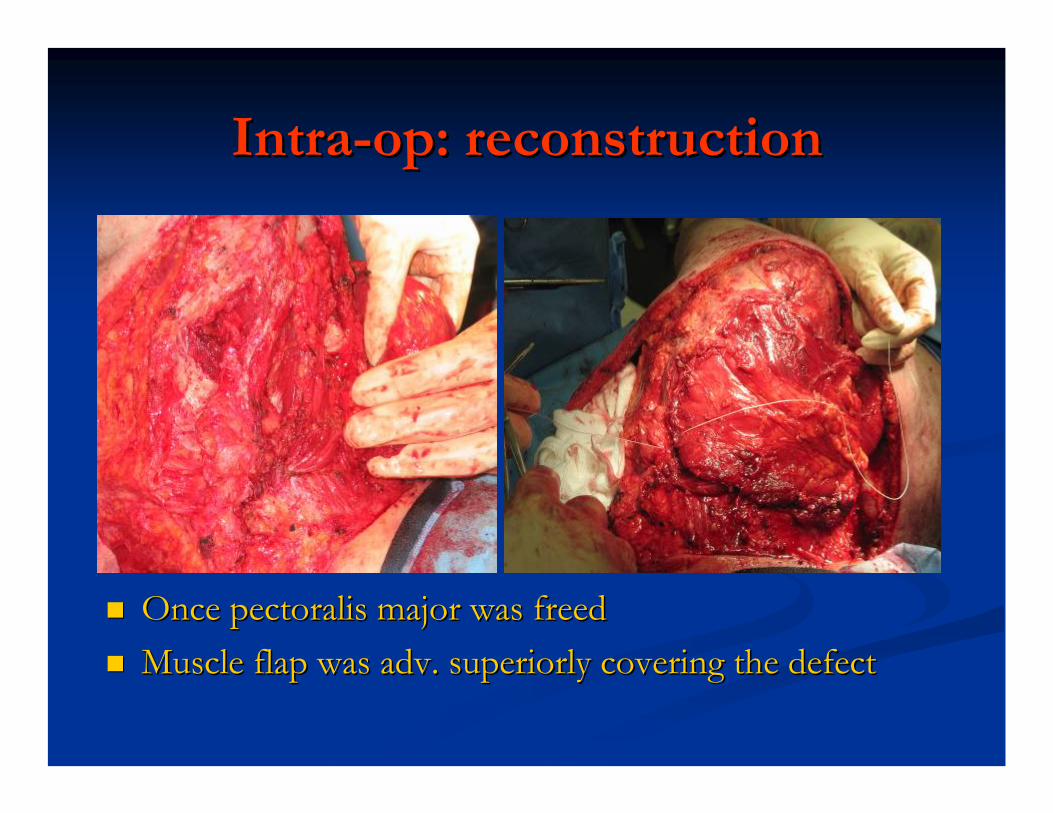
IntraIntra--op: reconstructionop: reconstruction
Once Once pectoralispectoralis major was freedmajor was freedMuscle flap was adv. superiorly covering the defectMuscle flap was adv. superiorly covering the defect
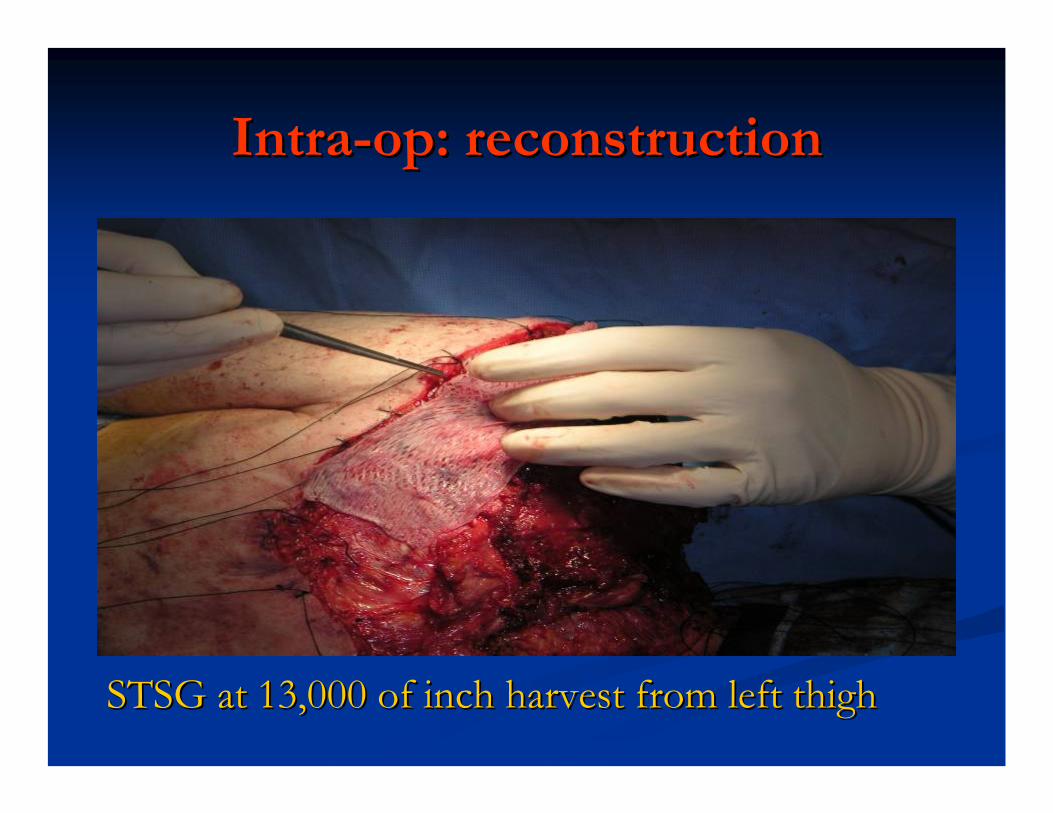
IntraIntra--op: reconstructionop: reconstruction
STSG at 13,000 of inch harvest from left thighSTSG at 13,000 of inch harvest from left thigh
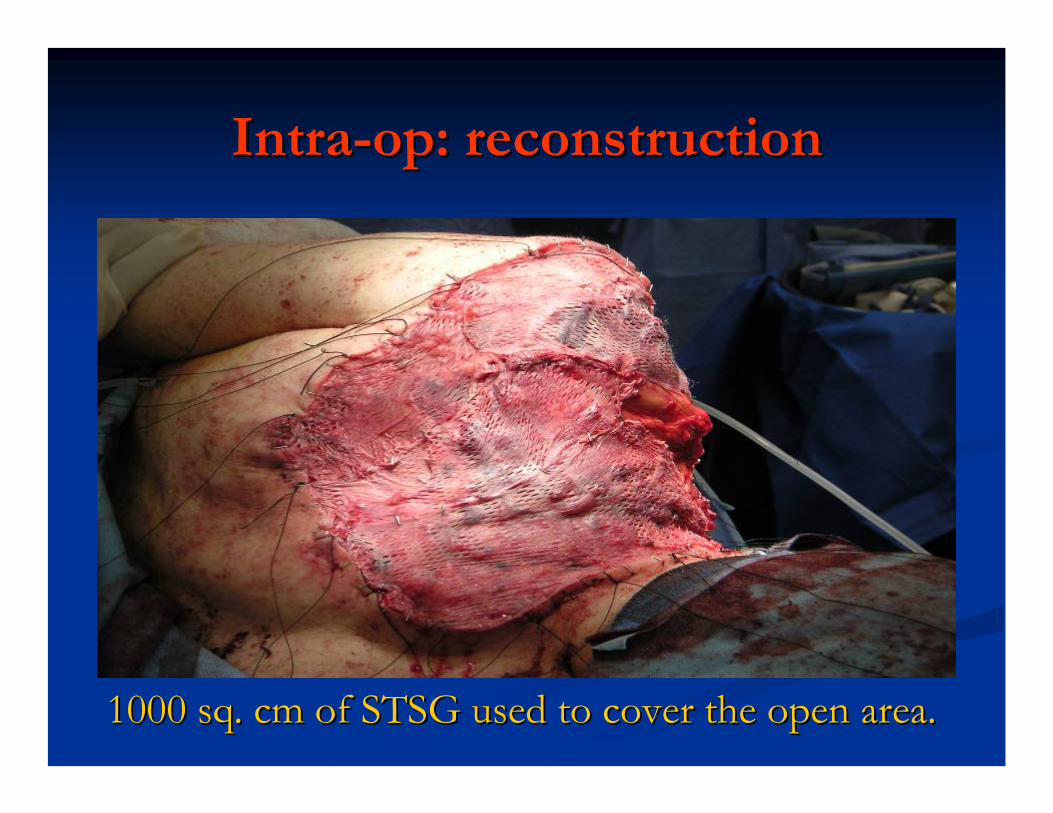
IntraIntra--op: reconstructionop: reconstruction
1000 sq. cm of STSG used to cover the open area.1000 sq. cm of STSG used to cover the open area.
Hospital courseHospital course
Immediate postImmediate post--op: op: extubatedextubated and and hemodynamicallyhemodynamically stable.stable.POD #1 Transfer to floorPOD #1 Transfer to floorPOD #9 Rehab was startedPOD #9 Rehab was startedPOD #14 Discharge POD #14 Discharge
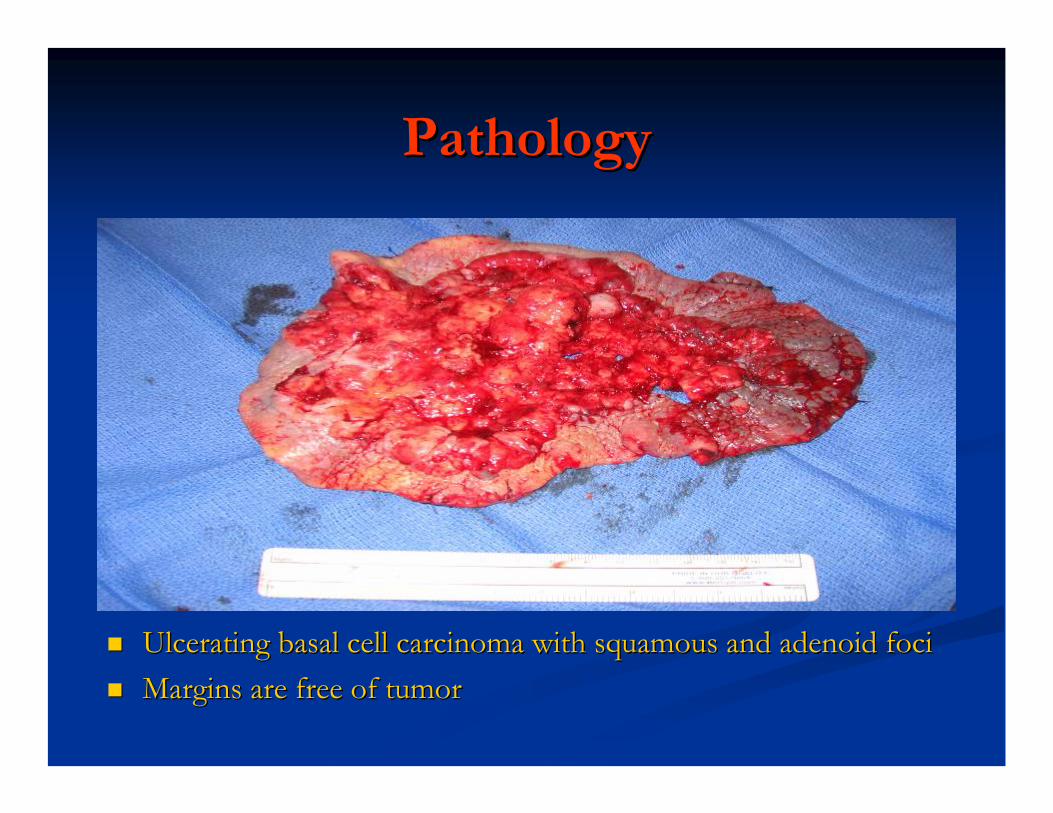
PathologyPathology
Ulcerating basal cell carcinoma with Ulcerating basal cell carcinoma with squamoussquamous and adenoid fociand adenoid fociMargins are free of tumorMargins are free of tumor
Basal Cell Carcinoma: Basal Cell Carcinoma: Overview and Overview and ManagementManagement
Mark H. Tseng MDMark H. Tseng MDSUNY Downstate University HospitalSUNY Downstate University Hospital
June 17, 2005June 17, 2005
OverviewOverview
IntroductionIntroductionEpidemiologyEpidemiology
IncidenceIncidenceRisk factorsRisk factors
Anatomy/HistologyAnatomy/HistologyClinical presentationClinical presentationDiagnosisDiagnosisTreatmentTreatmentPrognosisPrognosisConclusionConclusionReferencesReferences
IntroductionIntroduction
Most common skin cancer arising from the basal Most common skin cancer arising from the basal layer of epidermis and its layer of epidermis and its ppendagesppendagesLow Low metastaticmetastatic potientialpotientialLocally invasive, aggressive, and destructive to Locally invasive, aggressive, and destructive to skin and boneskin and bone
EpidemiologyEpidemiology
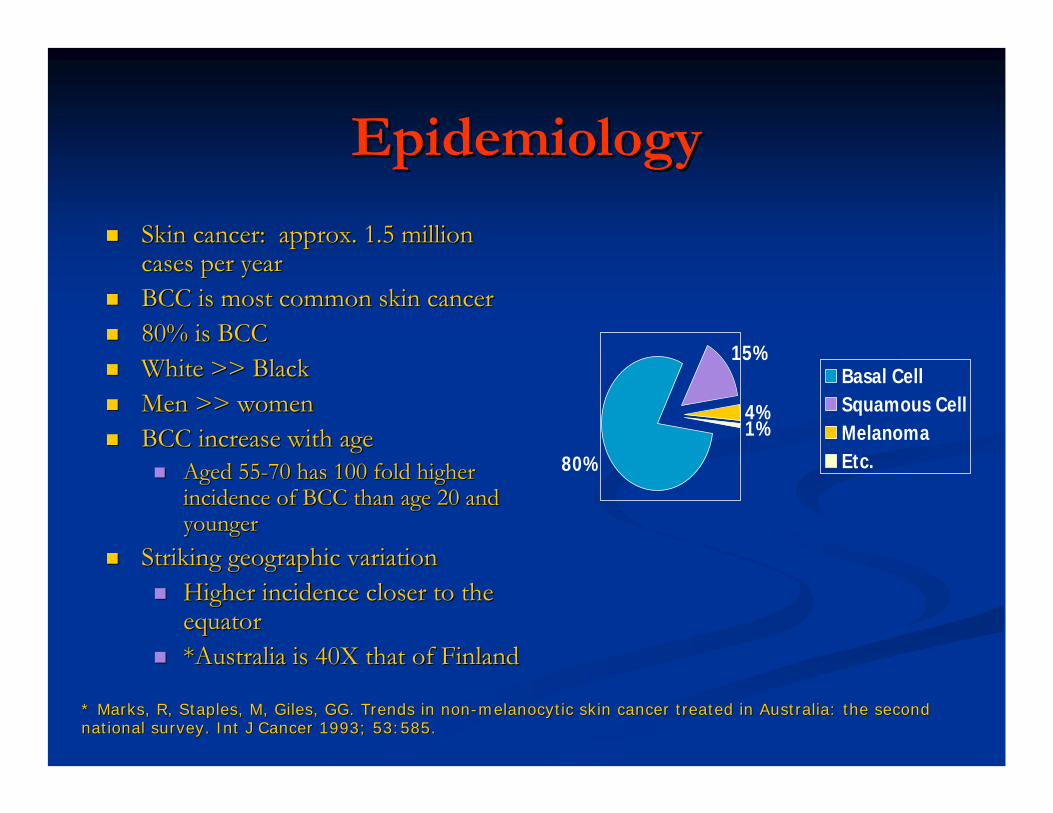
Skin cancer: approx. 1.5 million Skin cancer: approx. 1.5 million cases per yearcases per yearBCC is most common skin cancerBCC is most common skin cancer80% is BCC80% is BCCWhite >> Black White >> Black Men >> womenMen >> womenBCC increase with ageBCC increase with age
Aged 55Aged 55--70 has 100 fold higher 70 has 100 fold higher incidence of BCC than age 20 and incidence of BCC than age 20 and youngeryounger
Striking geographic variationStriking geographic variationHigher incidence closer to the Higher incidence closer to the equatorequator*Australia is 40X that of Finland*Australia is 40X that of Finland
80%
15%
4%1%
Basal CellSquamous CellMelanomaEtc.
* Marks, R, Staples, M, Giles, GG. Trends in non* Marks, R, Staples, M, Giles, GG. Trends in non--melanocyticmelanocytic skin cancer treated in Australia: the second skin cancer treated in Australia: the second national survey. national survey. IntInt J Cancer 1993; 53:585.J Cancer 1993; 53:585.
Risk Factors: EnvironmentalRisk Factors: Environmental
Sun exposure is the most important environmental cause of BCC.
Ultraviolet light – Sun ExposureIonizing radiation causes mutation of tumor suppressor genesUV B light: 280-320nm, UV A light 320-400nm
But, UVA rays pass deeper into the skin.
UVB radiation is thought to be the cause of melanoma and other types of skin cancer.
UVA radiation may cause skin damage that can lead to skin cancer and cause premature aging of the skin.
Amount of UV B exposure during childhood and adolescence is directly proportional to risk for BCC
Risk Factors: SunburnsRisk Factors: Sunburns
The Behavior Risk Factor Surveillance System The Behavior Risk Factor Surveillance System provided data showing nearly 32% of all adults provided data showing nearly 32% of all adults in the US report having had a sunburn in 1999.in the US report having had a sunburn in 1999.
More than 57% of adults age 18 to 29 reported More than 57% of adults age 18 to 29 reported having had a sunburn.having had a sunburn.
Over 40% of children are reported to have had Over 40% of children are reported to have had sunburns over the preceding year.sunburns over the preceding year.
Risk Factor: Sun exposureRisk Factor: Sun exposure
Childhood sun exposure is more important than Childhood sun exposure is more important than exposure during adult life.exposure during adult life.
*Canadian case control study*Canadian case control study226 men with BCC and 406 age226 men with BCC and 406 age--match controlsmatch controls
Aggressive sun protection before age 18 reduce Aggressive sun protection before age 18 reduce nonmelanomanonmelanoma skin cancer by 78%.skin cancer by 78%.The type, quantity and timing of sun exposure The type, quantity and timing of sun exposure necessary to increase the risk of BCC are not necessary to increase the risk of BCC are not clearly defined.clearly defined.
*Gallagher, *Gallagher, BajdikBajdik, CD, et al. Sunlight exposure, Basal cell carcinoma. Arch , CD, et al. Sunlight exposure, Basal cell carcinoma. Arch DermatolDermatol 1995; 131:157.1995; 131:157.
How can it be PREVENTED?How can it be PREVENTED?
For most of us, itFor most of us, it’’s too late !! But we can keep s too late !! But we can keep our kids from getting sunburns.our kids from getting sunburns.USE SUNSCREENUSE SUNSCREEN
*Large randomized trial evaluating sunscreen and beta*Large randomized trial evaluating sunscreen and beta--carotene (oral antioxidant) on prevention of BCC and SCC carotene (oral antioxidant) on prevention of BCC and SCC followed over 4 years.followed over 4 years.Users of sunscreen has 40% reduction in skin cancer over Users of sunscreen has 40% reduction in skin cancer over nonnon--usersusersBeta carotene failed to decrease incidence over placeboBeta carotene failed to decrease incidence over placebo..
*Green, A, Williams, G, *Green, A, Williams, G, NealeNeale, R, et al. Daily sunscreen application and , R, et al. Daily sunscreen application and betacarotenebetacarotenesupplementation in prevention of basalsupplementation in prevention of basal--cell and cell and squamoussquamous--cell carcinomas of the skin: a cell carcinomas of the skin: a randomisedrandomised controlled trial. Lancet 1999; 354:723.controlled trial. Lancet 1999; 354:723.
Risk FactorsRisk Factors
The following groups have the least melanin and The following groups have the least melanin and are at greatest risk for BCC:are at greatest risk for BCC:
fair complexion,fair complexion,light hair,light hair,blue/green eyes,blue/green eyes,inability to tan,inability to tan,history of multiple or severe sunburns,history of multiple or severe sunburns,frequent use of tanning beds, ladies!frequent use of tanning beds, ladies!Celtic ancestryCeltic ancestry
Risk FactorsRisk FactorsSmokingSmokingArsenicArsenicRadiation TherapyRadiation TherapyBurns, Scars, UlcersBurns, Scars, UlcersChronic Chronic immunosuppressionimmunosuppression
*Transplant patients*Transplant patientsIncidence is increased 10 fold in transplant patients compare toIncidence is increased 10 fold in transplant patients compare to nontransplantnontransplantpatientspatients
AlbinismAlbinismMutation of PTCH gene (tumor suppressor gene) on chromosome 9 inMutation of PTCH gene (tumor suppressor gene) on chromosome 9 inpatients with familial basal cell nevus syndrome.patients with familial basal cell nevus syndrome.Bazex'sBazex's syndrome (basal cell carcinomas, follicular syndrome (basal cell carcinomas, follicular atrophodermaatrophoderma, , hypotrichosishypotrichosis, and , and hypohidrosishypohidrosis or or hyperhidrosishyperhidrosis) ) Gorlin'sGorlin's syndrome (multiple basal cell carcinomas, pitting of the palms syndrome (multiple basal cell carcinomas, pitting of the palms and and the soles of the feet, the soles of the feet, mandibularmandibular cysts, spine and rib anomalies, calcification cysts, spine and rib anomalies, calcification of the of the falxfalx cerebricerebri, and cataracts ), and cataracts )
**HarteveltHartevelt, MM, , MM, BavinckBavinck, JN, , JN, KootteKootte, AM, et al. Incidence of skin cancer after renal , AM, et al. Incidence of skin cancer after renal transplantation in the Netherlands. Transplantation 1990; 49:506transplantation in the Netherlands. Transplantation 1990; 49:506..
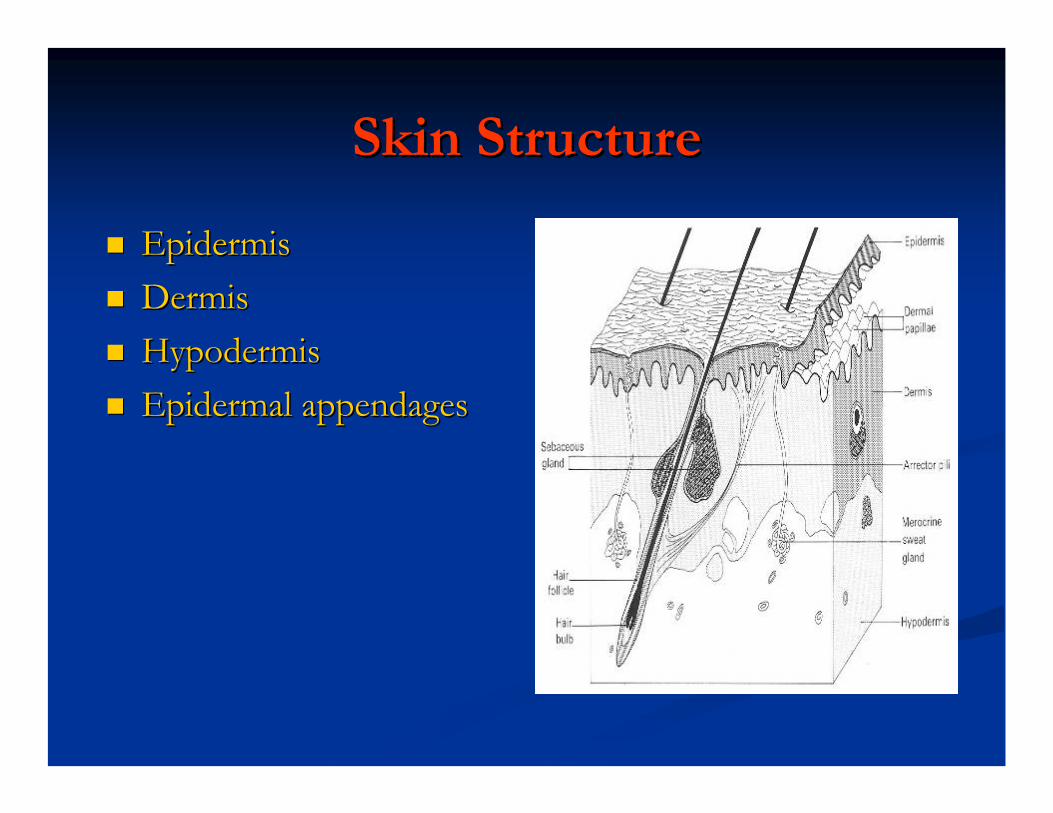
Skin StructureSkin Structure
EpidermisEpidermisDermisDermisHypodermisHypodermisEpidermal appendagesEpidermal appendages
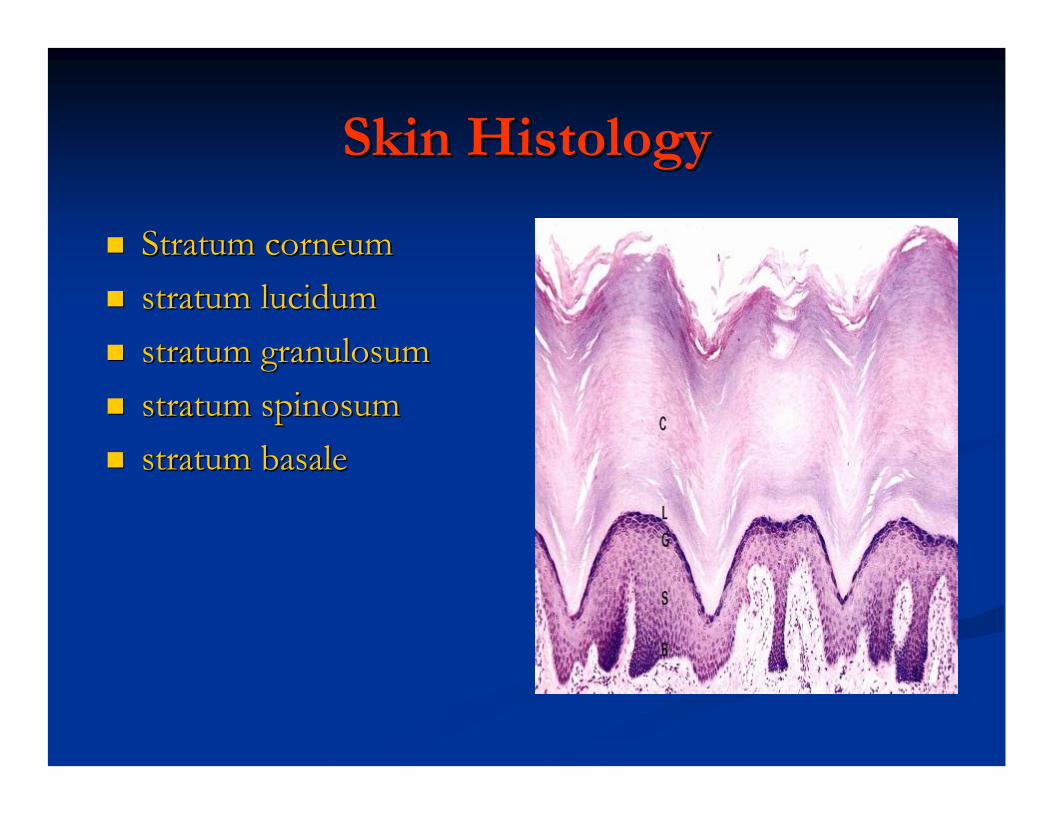
Skin HistologySkin Histology
Stratum Stratum corneumcorneumstratum stratum lucidumlucidumstratum stratum granulosumgranulosumstratum stratum spinosumspinosumstratum stratum basalebasale
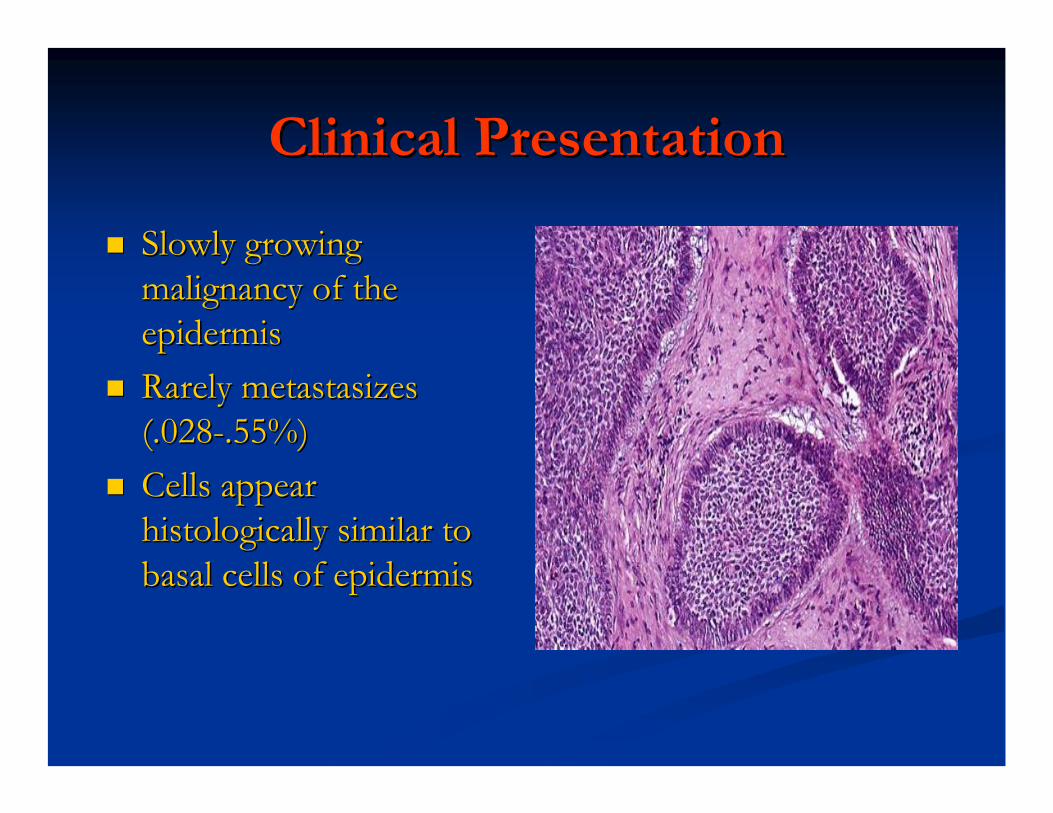
Clinical PresentationClinical Presentation
Slowly growing Slowly growing malignancy of the malignancy of the epidermisepidermisRarely metastasizes Rarely metastasizes (.028(.028--.55%).55%)Cells appear Cells appear histologicallyhistologically similar to similar to basal cells of epidermisbasal cells of epidermis
Clinical PresentationClinical Presentation
Distribution of BCC: Distribution of BCC: 70% on face70% on face25% on trunk25% on trunk5% on penis, vulva, or 5% on penis, vulva, or perianalperianal skinskin
Clinical subtypes (4)Clinical subtypes (4)NodularNodularSuperficialSuperficialPigmentedPigmentedMorpheaformMorpheaform
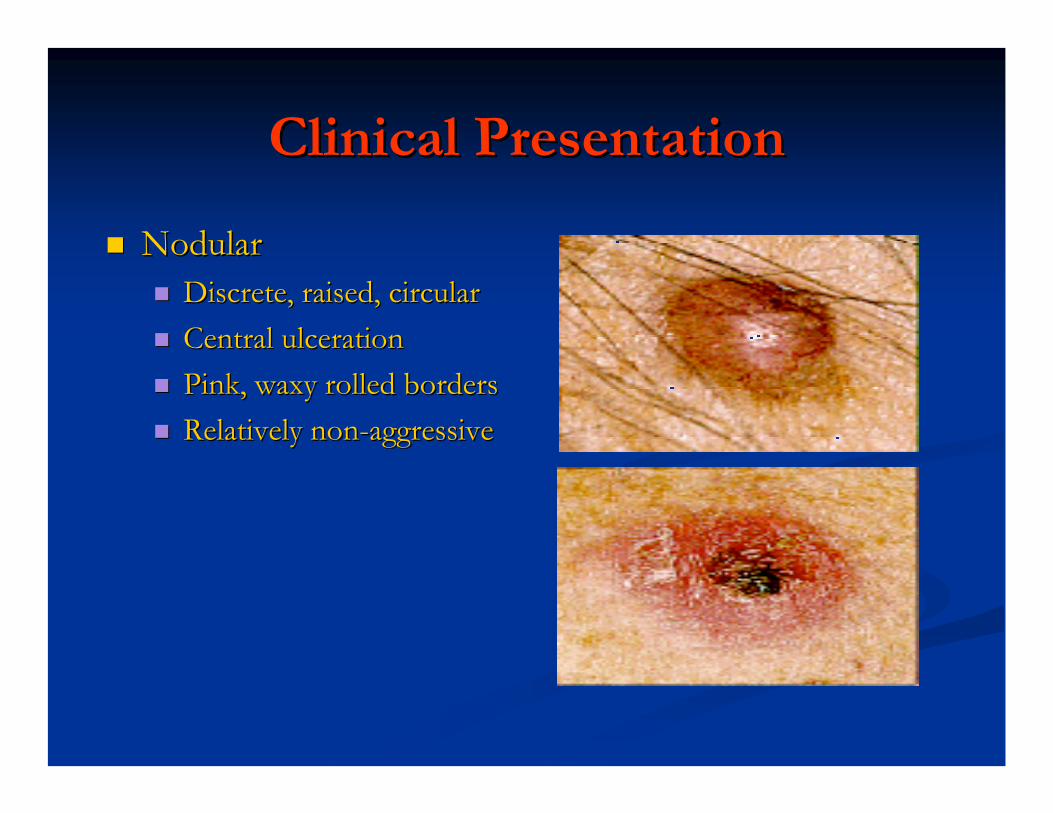
Clinical PresentationClinical Presentation
NodularNodularDiscrete, raised, circularDiscrete, raised, circularCentral ulcerationCentral ulcerationPink, waxy rolled bordersPink, waxy rolled bordersRelatively nonRelatively non--aggressiveaggressive
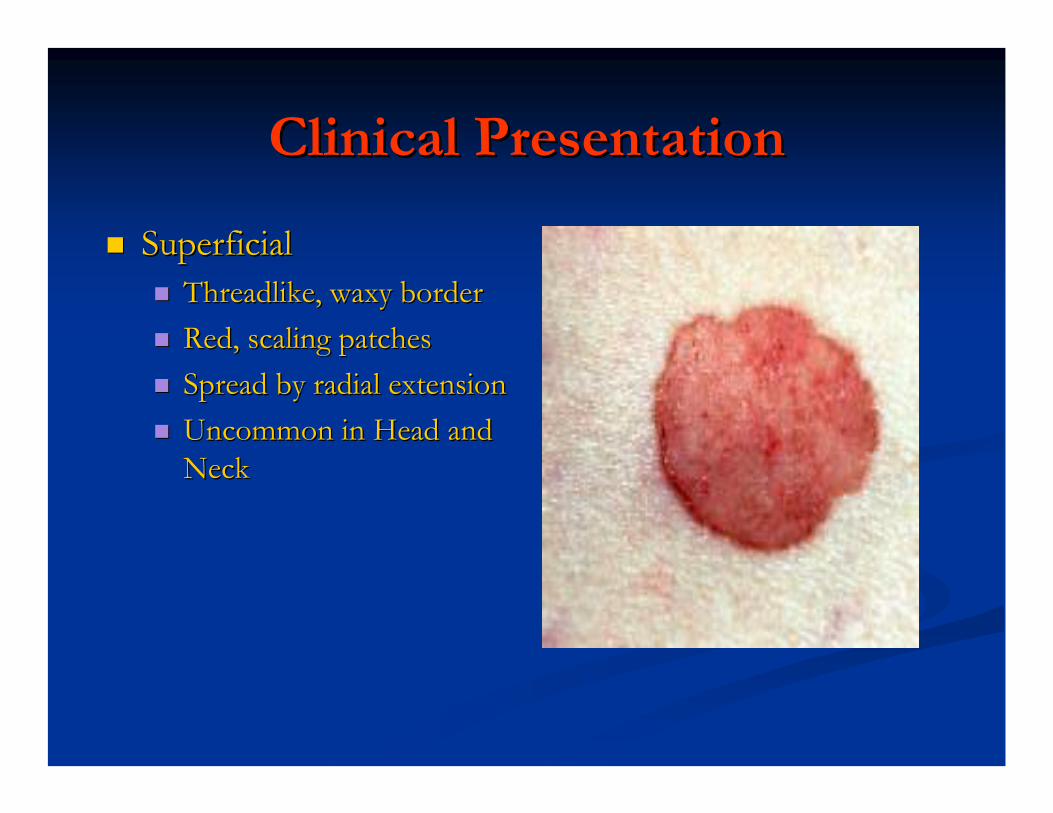
Clinical PresentationClinical Presentation
SuperficialSuperficialThreadlike, waxy borderThreadlike, waxy borderRed, scaling patchesRed, scaling patchesSpread by radial extensionSpread by radial extensionUncommon in Head and Uncommon in Head and NeckNeck
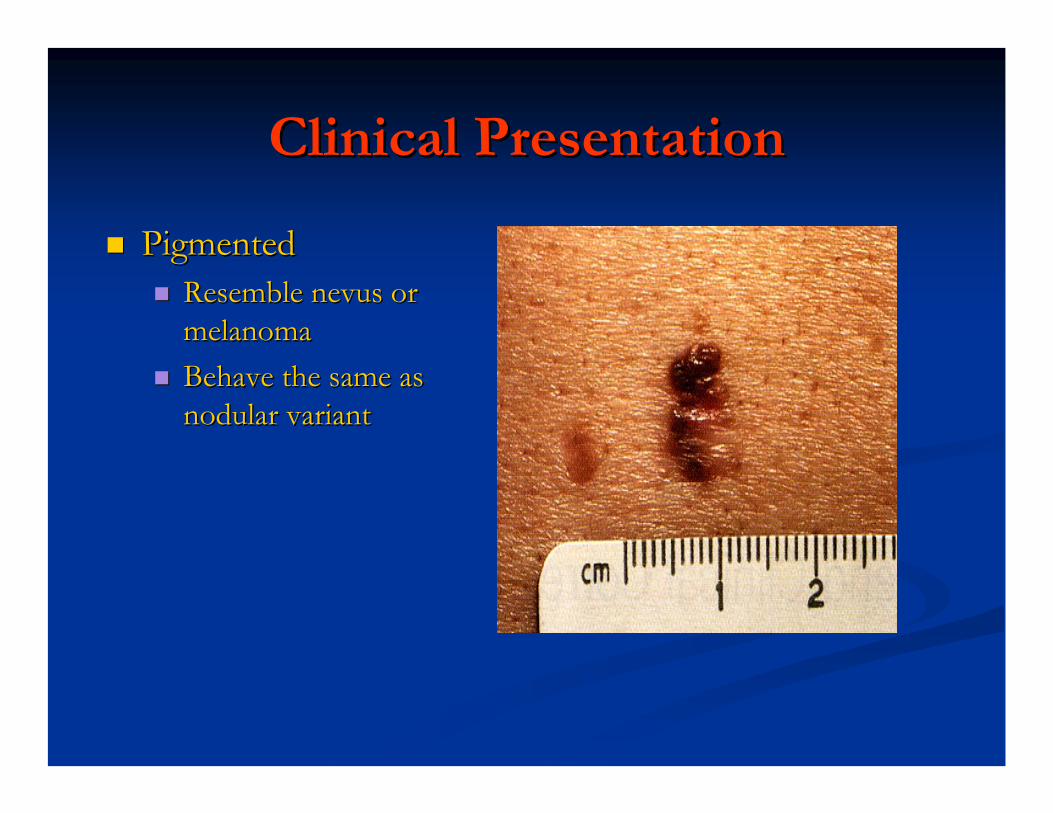
Clinical PresentationClinical Presentation
PigmentedPigmentedResemble nevus or Resemble nevus or melanomamelanomaBehave the same as Behave the same as nodular variantnodular variant
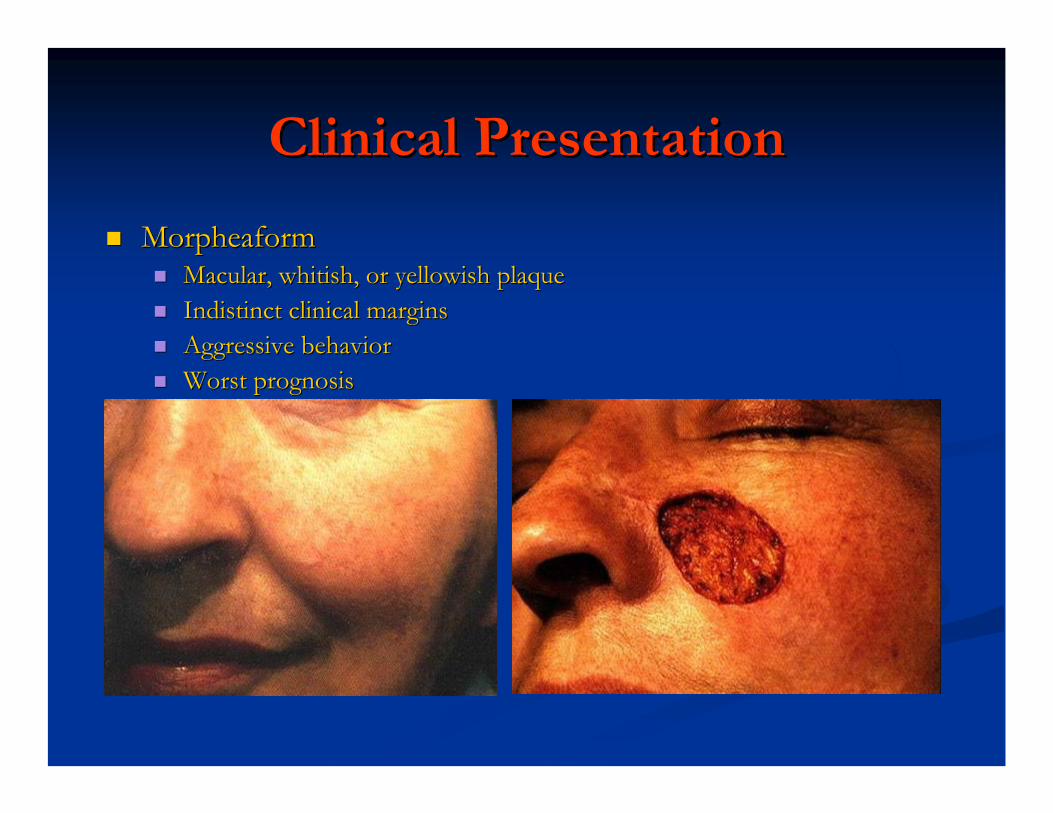
Clinical PresentationClinical Presentation
MorpheaformMorpheaformMacular, whitish, or yellowish plaqueMacular, whitish, or yellowish plaqueIndistinct clinical marginsIndistinct clinical marginsAggressive behaviorAggressive behaviorWorst prognosisWorst prognosis
Clinical PresentationClinical Presentation
HistologicHistologic Subtypes (4)Subtypes (4)SolidSolidCysticCysticAdenoidAdenoidKeratoticKeratotic ((BasosquamousBasosquamous))
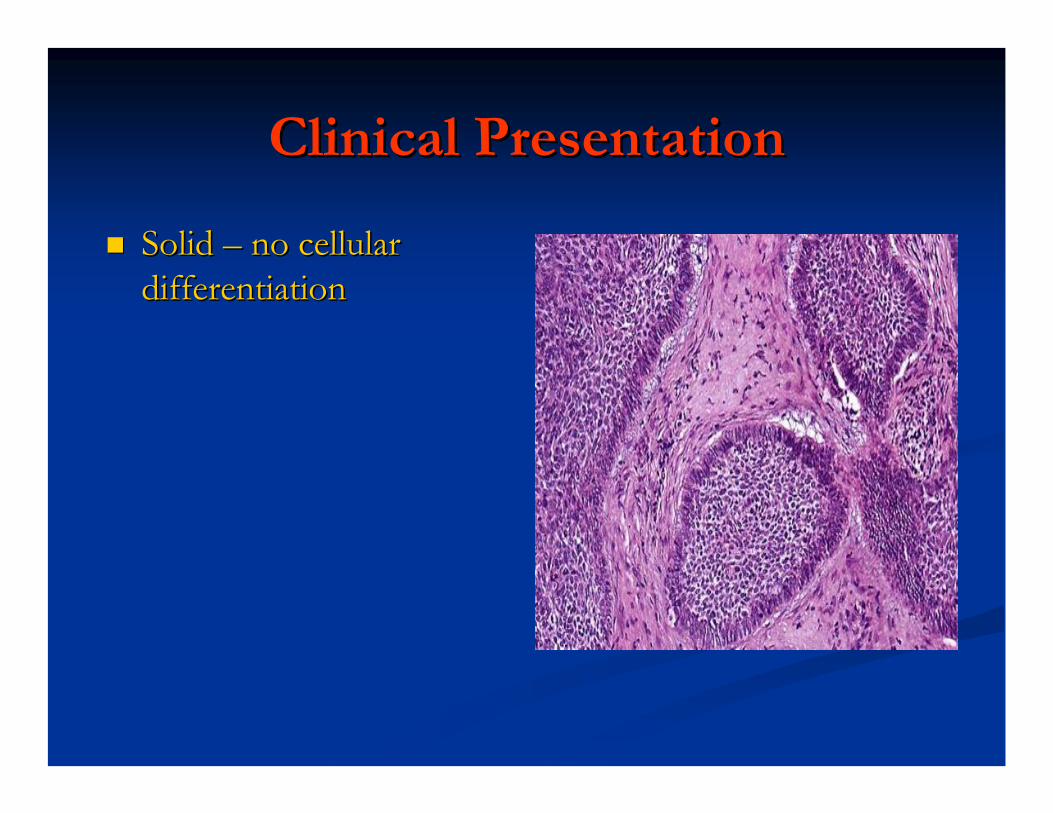
Clinical PresentationClinical Presentation
Solid Solid –– no cellular no cellular differentiationdifferentiation
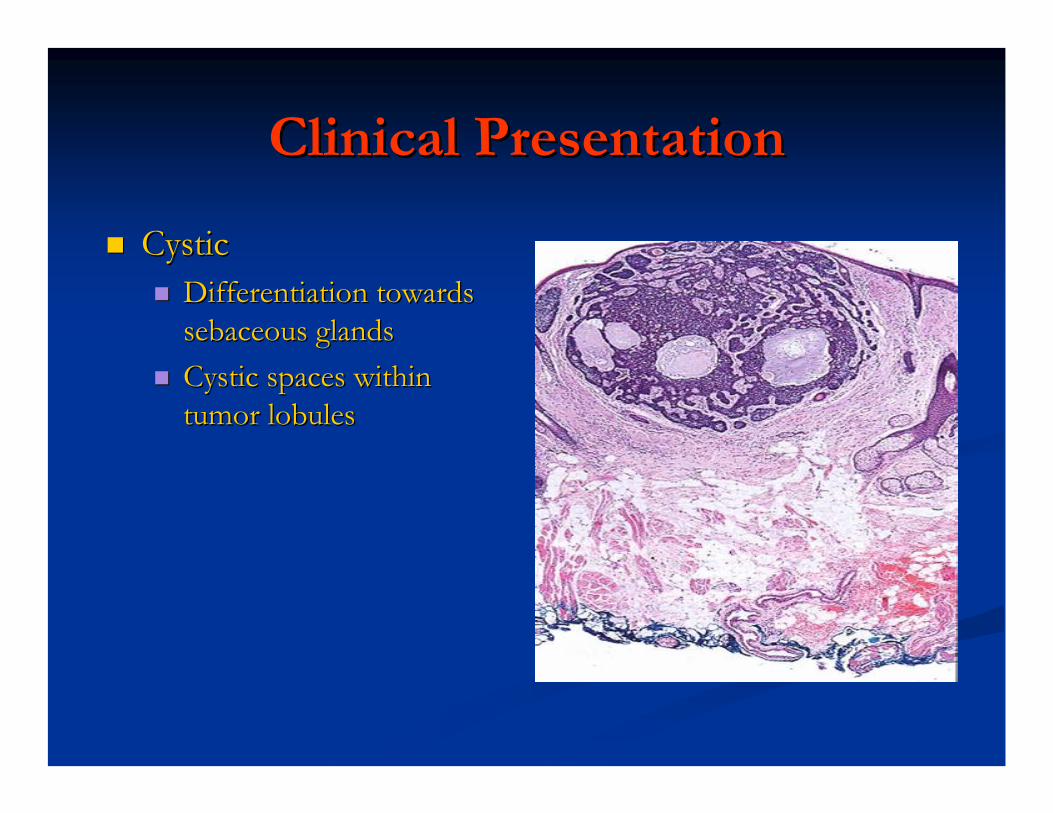
Clinical PresentationClinical Presentation
CysticCysticDifferentiation towards Differentiation towards sebaceous glandssebaceous glandsCystic spaces within Cystic spaces within tumor lobulestumor lobules
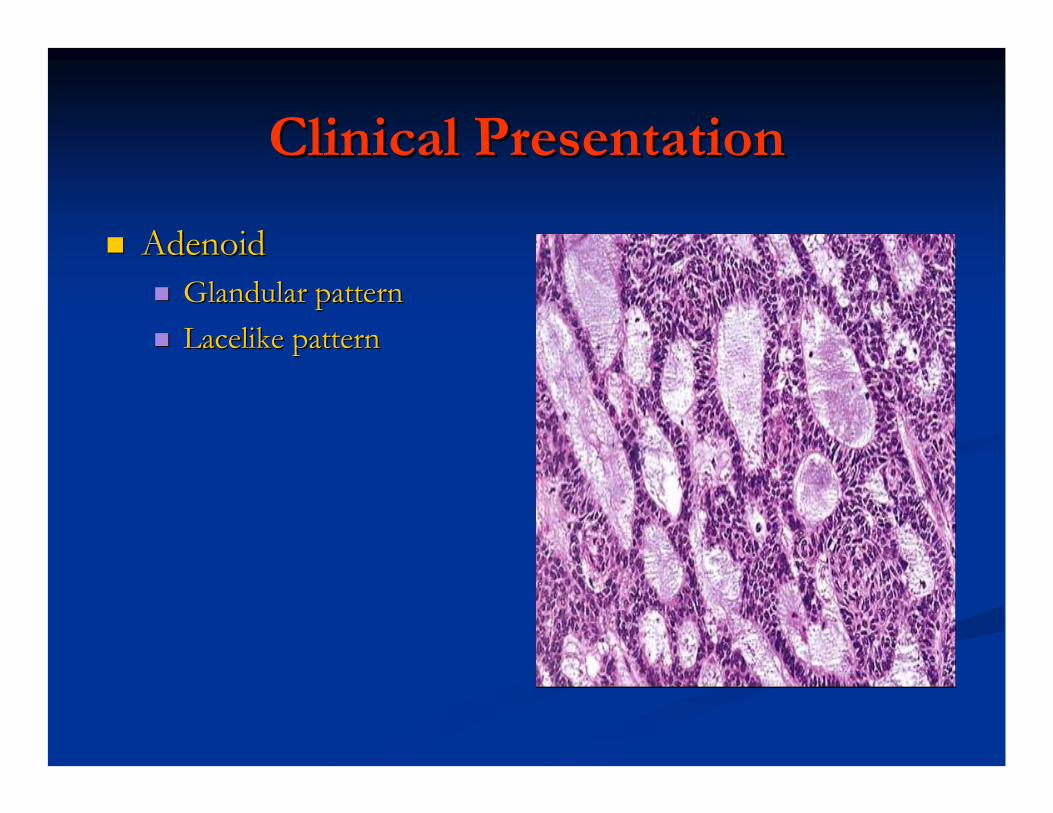
Clinical PresentationClinical Presentation
AdenoidAdenoidGlandular patternGlandular patternLacelike patternLacelike pattern
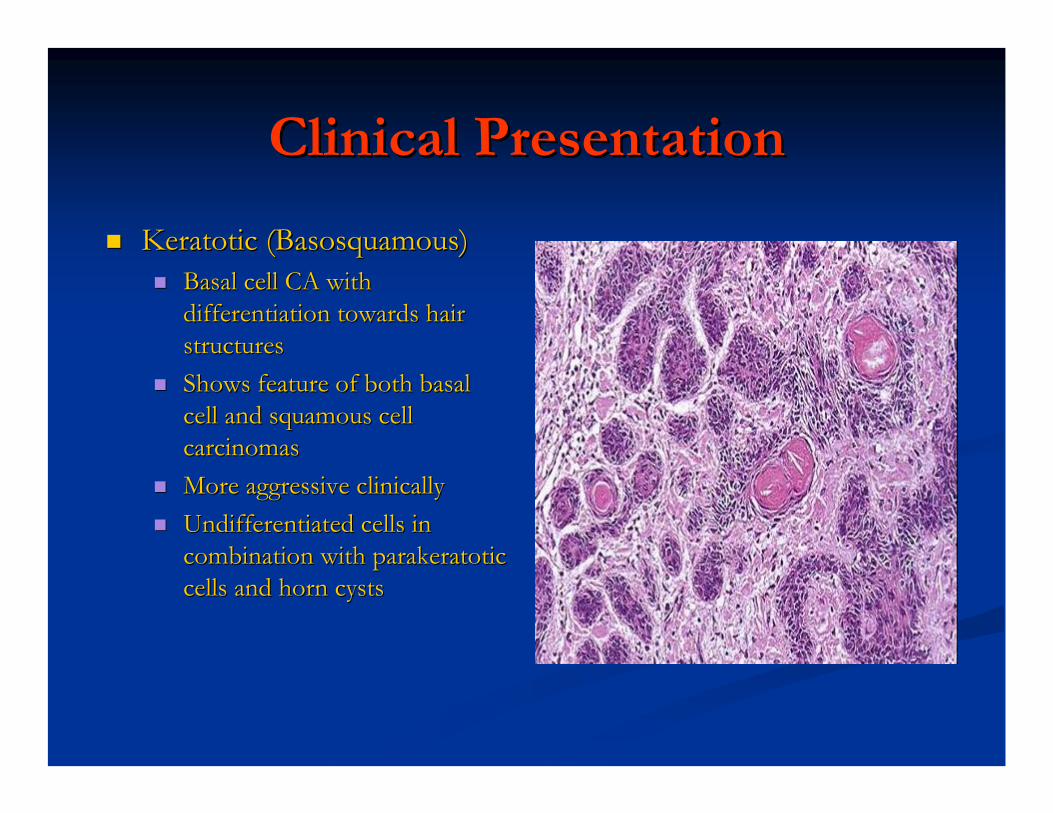
Clinical PresentationClinical Presentation
KeratoticKeratotic ((BasosquamousBasosquamous))Basal cell CA with Basal cell CA with differentiation towards hair differentiation towards hair structuresstructuresShows feature of both basal Shows feature of both basal cell and cell and squamoussquamous cell cell carcinomascarcinomasMore aggressive clinicallyMore aggressive clinicallyUndifferentiated cells in Undifferentiated cells in combination with combination with parakeratoticparakeratoticcells and horn cystscells and horn cysts
DiagnosisDiagnosis
Initial evaluation Initial evaluation involvesinvolves
Assessment of locationAssessment of locationPunch or Punch or excisionalexcisionalbiopsybiopsyStagingStaging
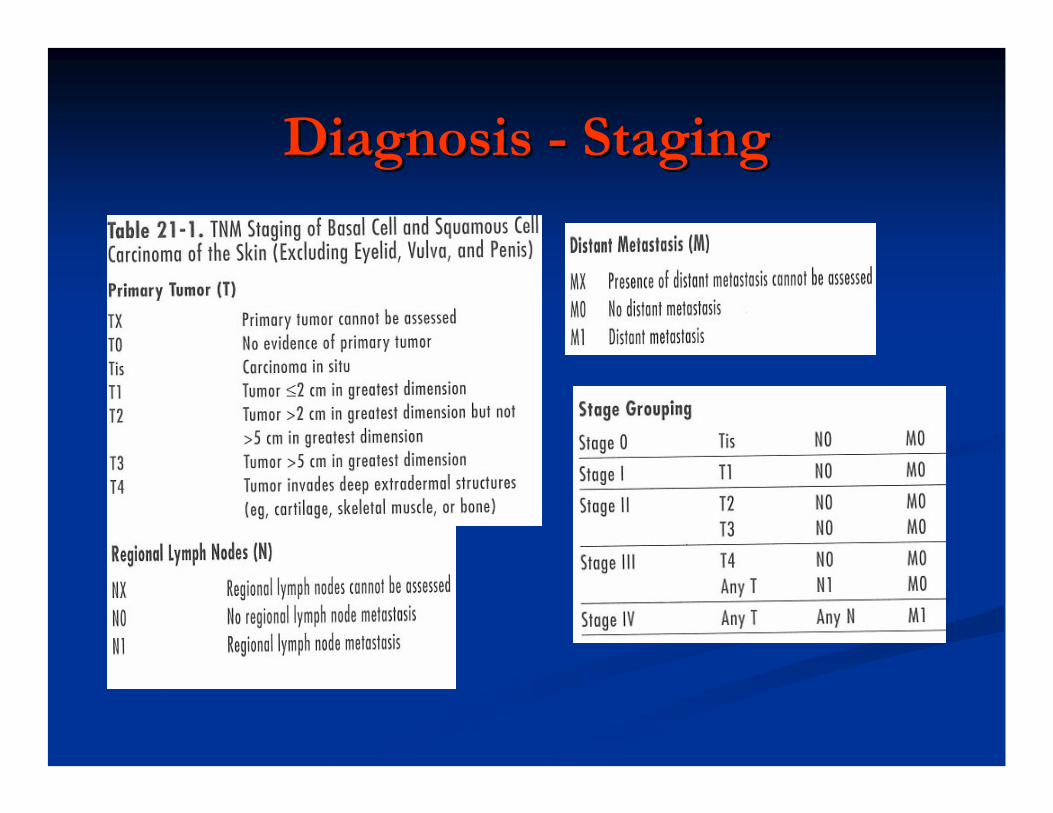
Diagnosis Diagnosis -- StagingStaging

Treatment: TechniquesTreatment: Techniques
Electrodessication and curettageElectrodessication and curettageCryosurgeryCryosurgeryRadiation therapyRadiation therapyPhotodynamic therapyPhotodynamic therapyExcisionalExcisional surgerysurgeryMohsMohs surgerysurgery
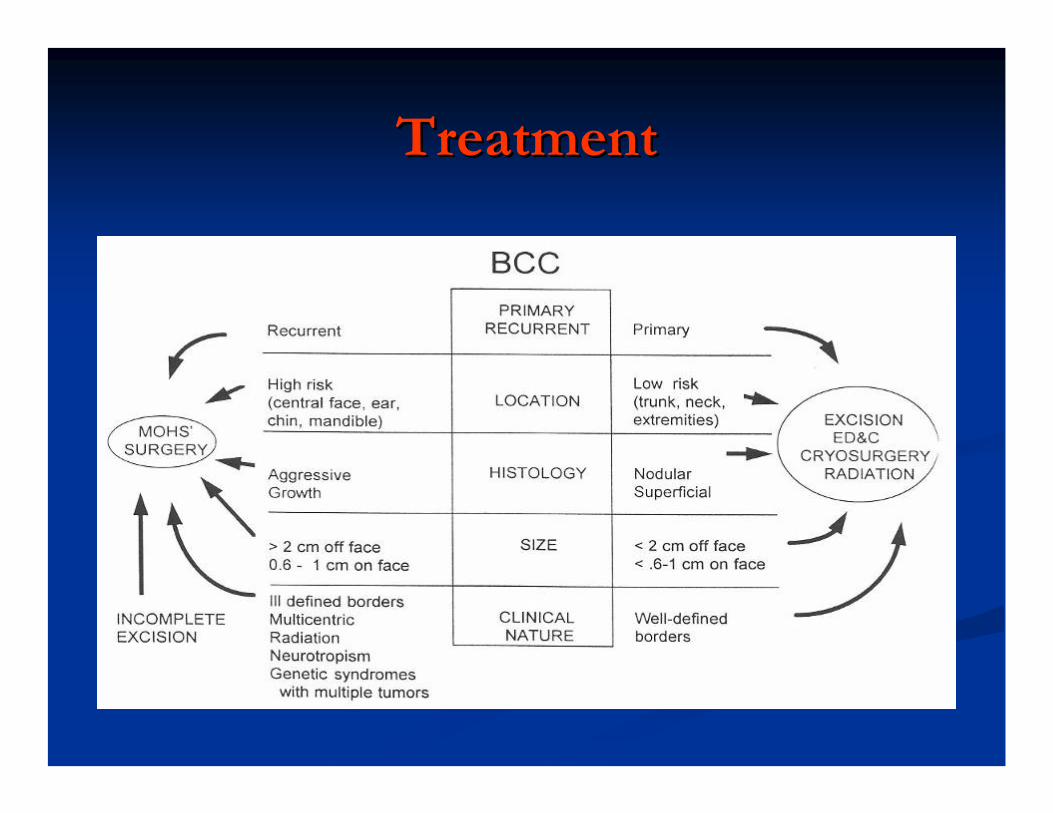
TreatmentTreatment
Treatment: Electrodessication Treatment: Electrodessication and Curettageand Curettage
Used to remove tumor by feel with small margin Used to remove tumor by feel with small margin of normal tissueof normal tissueReserved for Reserved for histologicallyhistologically and clinically and clinically favorable basal cell carcinomasfavorable basal cell carcinomas..Not used for Not used for squamoussquamous cell lesionscell lesions
Treatment: CryosurgeryTreatment: Cryosurgery
Uses liquid Nitrogen to kill tumor cellsUses liquid Nitrogen to kill tumor cellsTypical temperature of Typical temperature of --5050°°C .C .TissueTissue--sparing, but leave open woundsparing, but leave open woundHypopigmentationHypopigmentation and scarring may resultand scarring may resultLimited to favorable small lesions with wellLimited to favorable small lesions with well--defined bordersdefined borders
Treatment: Radiation TherapyTreatment: Radiation Therapy
Used extensively in the past, now sparinglyUsed extensively in the past, now sparinglyHigh cure rate (95%)High cure rate (95%)Does not allow surgical stagingDoes not allow surgical stagingCurrently Currently reserved for poor operative reserved for poor operative candidatescandidates, adjuvant in high risk malignancy , adjuvant in high risk malignancy Protracted treatment course, and expensiveProtracted treatment course, and expensiveRadiodermatitisRadiodermatitis, delayed carcinogenesis, delayed carcinogenesis
Treatment: Photodynamic TherapyTreatment: Photodynamic Therapy
Photosensitizing drug (Photosensitizing drug (porphyrinporphyrin, 5, 5--ALA) ALA) applied topically, orally or applied topically, orally or parenterallyparenterally and and localizes into tumor cellslocalizes into tumor cellsDrug is activated by exposure to light (laser)Drug is activated by exposure to light (laser)Efficacy is low (45%)Efficacy is low (45%)Side effects include local edema, Side effects include local edema, erythemaerythema, , blistering, ulcerationblistering, ulcerationUsed as palliationUsed as palliation
Treatment: Treatment: ExcisionalExcisional SurgerySurgery
Most often used by surgeons, especially for Most often used by surgeons, especially for larger lesionslarger lesionsCan be with cold steel or laserCan be with cold steel or laserCan allow reconstruction in the same sittingCan allow reconstruction in the same sittingFrozen sections decrease recurrence rateFrozen sections decrease recurrence rateCan be time consuming and inconvenientCan be time consuming and inconvenientIf more than 1/3 of a cosmetic facial unit is If more than 1/3 of a cosmetic facial unit is excised, better excised, better cosmesiscosmesis with removal of entire with removal of entire unitunit
MohsMohs SurgerySurgery
First described by Frederic E. First described by Frederic E. MohsMohs in 1941in 1941MohsMohs micrographic surgery (MMS)micrographic surgery (MMS)
Gold standard for treating highGold standard for treating high--risk skin cancersrisk skin cancersSeries of precise excision and microscopic evaluationSeries of precise excision and microscopic evaluation99% 5 year cure rate for BCC99% 5 year cure rate for BCCLowest recurrence rateLowest recurrence rateAdvantages: precision, excellent cure rate, better Advantages: precision, excellent cure rate, better cosmesiscosmesis because it spares normal tissuebecause it spares normal tissueDisadvantages: time consuming and expensiveDisadvantages: time consuming and expensive
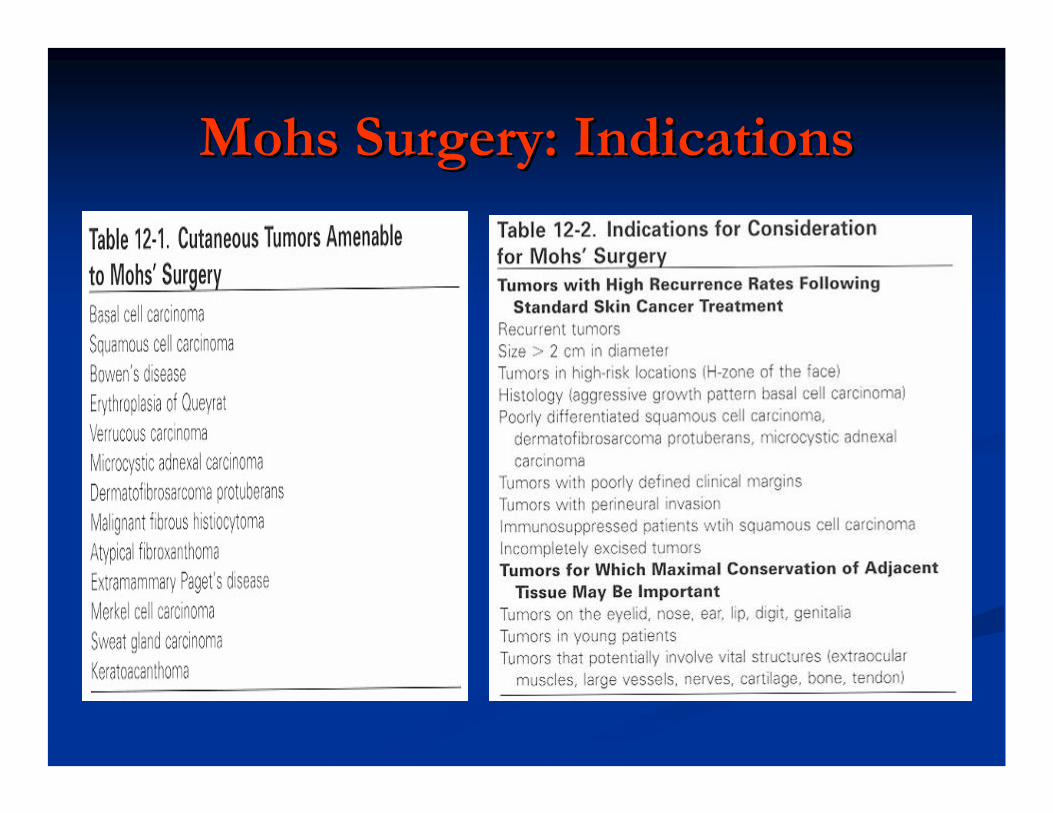
MohsMohs Surgery: IndicationsSurgery: Indications
Treatment: Recurrence RateTreatment: Recurrence Rate
All of the nonAll of the non--MohsMohs' modalities have roughly equal and ' modalities have roughly equal and excellent cure rates for BCC without highexcellent cure rates for BCC without high--risk risk prognostic factors prognostic factors Recurrence rates for tumors treated by Recurrence rates for tumors treated by MohMoh’’ssMicrographic Surgery appear to be lower at all points in Micrographic Surgery appear to be lower at all points in time and averages between 1time and averages between 1--2%. 2%. The key predictors of tumor recurrence are size and site The key predictors of tumor recurrence are size and site of the lesion, histology of tumor, and skill of the of the lesion, histology of tumor, and skill of the operatoroperatorThere is an increased risk of BCC recurrence regardless There is an increased risk of BCC recurrence regardless of treatment modality with increasing time.of treatment modality with increasing time.
PrognosisPrognosis
ExcellentExcellentSignificant morbidity and disfigurementSignificant morbidity and disfigurementPt with BCC are susceptible to other skin cancerPt with BCC are susceptible to other skin cancer
*40% over 3 years*40% over 3 yearsSlowSlow--growing tumorgrowing tumorMetastasis is rare: 0.1%Metastasis is rare: 0.1%
Usually deeply invasive or large ( 10 x 10 cm or greater )Usually deeply invasive or large ( 10 x 10 cm or greater )Fatal within eight monthsFatal within eight monthsRoutine Routine metastaticmetastatic workup is not recommend unless workup is not recommend unless symptoms supervenesymptoms supervene
**MarcilMarcil, I, Stern, RS. Risk of developing a subsequent , I, Stern, RS. Risk of developing a subsequent nonmelanomanonmelanoma skin cancer in patients with a history skin cancer in patients with a history of of nonmelanomanonmelanoma skin cancer: a critical review of the literature and metaskin cancer: a critical review of the literature and meta--analysis. Arch analysis. Arch DermatolDermatol 2000; 2000; 136:1524.136:1524.
ConclusionConclusion
BCC is the most common malignancyBCC is the most common malignancyRisk factors: sunlightRisk factors: sunlightUse sunscreenUse sunscreenMohMoh’’ss surgery is gold standardsurgery is gold standardHigh risk of developing a second BCCHigh risk of developing a second BCC
ReferencesReferences
Marks, R, Staples, M, Giles, GG. Trends in nonMarks, R, Staples, M, Giles, GG. Trends in non--melanocyticmelanocytic skin cancer treated in skin cancer treated in Australia: the second national survey. Australia: the second national survey. IntInt J Cancer 1993; 53:585.J Cancer 1993; 53:585.
Gallagher, Gallagher, BajdikBajdik, CD, et al. Sunlight exposure, Basal cell carcinoma. Arch , CD, et al. Sunlight exposure, Basal cell carcinoma. Arch DermatolDermatol1995; 131:1571995; 131:157
Green, A, Williams, G, Green, A, Williams, G, NealeNeale, R, et al. Daily sunscreen application and , R, et al. Daily sunscreen application and betacarotenebetacarotenesupplementation in prevention of basalsupplementation in prevention of basal--cell and cell and squamoussquamous--cell carcinomas of the cell carcinomas of the skin: a skin: a randomisedrandomised controlled trial. Lancet 1999; 354:723.controlled trial. Lancet 1999; 354:723.
HarteveltHartevelt, MM, , MM, BavinckBavinck, JN, , JN, KootteKootte, AM, et al. Incidence of skin cancer after renal , AM, et al. Incidence of skin cancer after renal transplantation in the Netherlands. Transplantation 1990; 49:506transplantation in the Netherlands. Transplantation 1990; 49:506..
MarcilMarcil, I, Stern, RS. Risk of developing a subsequent , I, Stern, RS. Risk of developing a subsequent nonmelanomanonmelanoma skin cancer in skin cancer in patients with a history of patients with a history of nonmelanomanonmelanoma skin cancer: a critical review of the literature skin cancer: a critical review of the literature and metaand meta--analysis. Arch analysis. Arch DermatolDermatol 2000; 136:1524.2000; 136:1524.
The EndThe End