Embed Size (px)
Citation preview
Surgical Management of Movement
Disorders
January 24, 2011Rita NguyenPreceptor: Dr. Kiss

Overview• Historical perspective
• Pathophysiology of Movement Disorders
• Selecting patients for surgery
• Surgical Targets
• Aspects of Surgery
• Imaging
• Frame v. Frameless
• Localizing the Target
• Neurophysiological Verification
• IPG
• Complications
• Outcomes
• Future Directions: Growth Factors, Genes, Cell Transplants
• Hemifacial Spasm: Management and Outcome
A brief history of surgery...
• 1953: Cooper. Accidental choroidal artery injury suppressed patient’s tremor. Subsequently performed ligation surgeries on eight patients.1
• 1955: Hassler. Thalomotomy more effective than pallidotomy.2
• 1950s - 1960s: Development of stereotaxy leads to a variety of lesioning procedures in the basal ganglia and thalamus.
• mid-1960s: Advent of L-dopa leads to decrease in surgery fo Parkinson’s Disease. Surgery limited to thalamotomy and pallidotomy for tremor and dystonia.
• late 1980s: Renewed interest in surgery for PD.
A brief history of stimulation...
• 1809. Rolando. Electrical impulses can modify functional outcome in certain brain regions.3
• 1960. Hassler. High-frequency electric stimulation of the pallidum decreases tremor. 4
• 1967. Bechtereva (Russia). Chronic DBS of the thalamus, striatum, and palldum is beneficial in movement disorders.5
• 1980s. Published reports of use of DBS for treatment of movement disorders
• Over the past 20 years, DBS has become the neurosurgical standard of care for Parkinson’s Disease, dystonia, and essential tremor.
What can you treat?
•Parkinson’s Disease
•Dystonia
•Essential Tremor
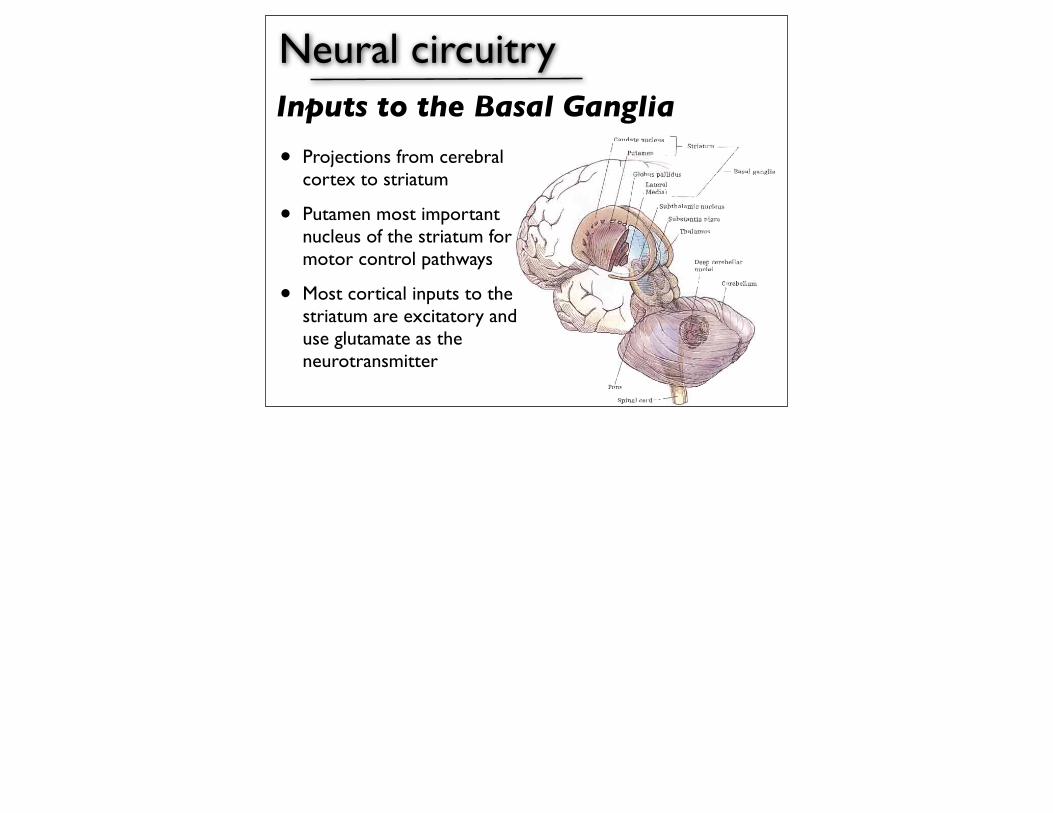
Neural circuitry
• Projections from cerebral cortex to striatum
• Putamen most important nucleus of the striatum for motor control pathways
• Most cortical inputs to the striatum are excitatory and use glutamate as the neurotransmitter
Inputs to the Basal Ganglia
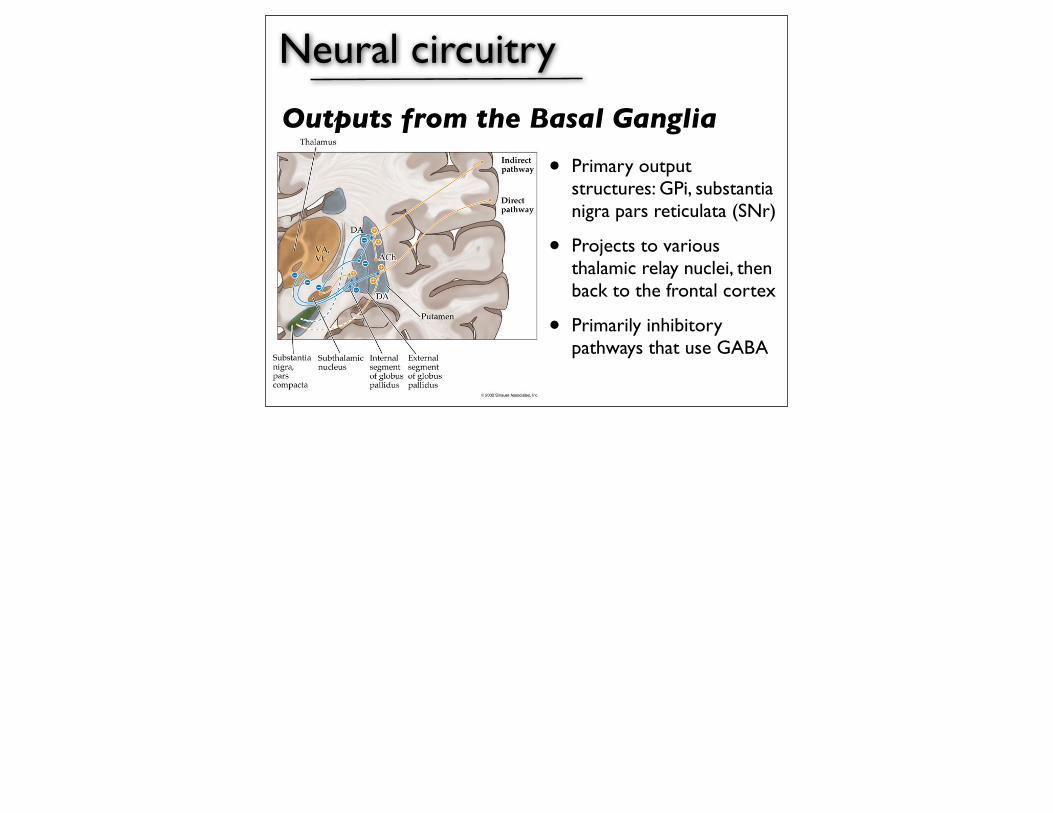
Neural circuitry
• Primary output structures: GPi, substantia nigra pars reticulata (SNr)
• Projects to various thalamic relay nuclei, then back to the frontal cortex
• Primarily inhibitory pathways that use GABA
Outputs from the Basal Ganglia
Neural circuitry
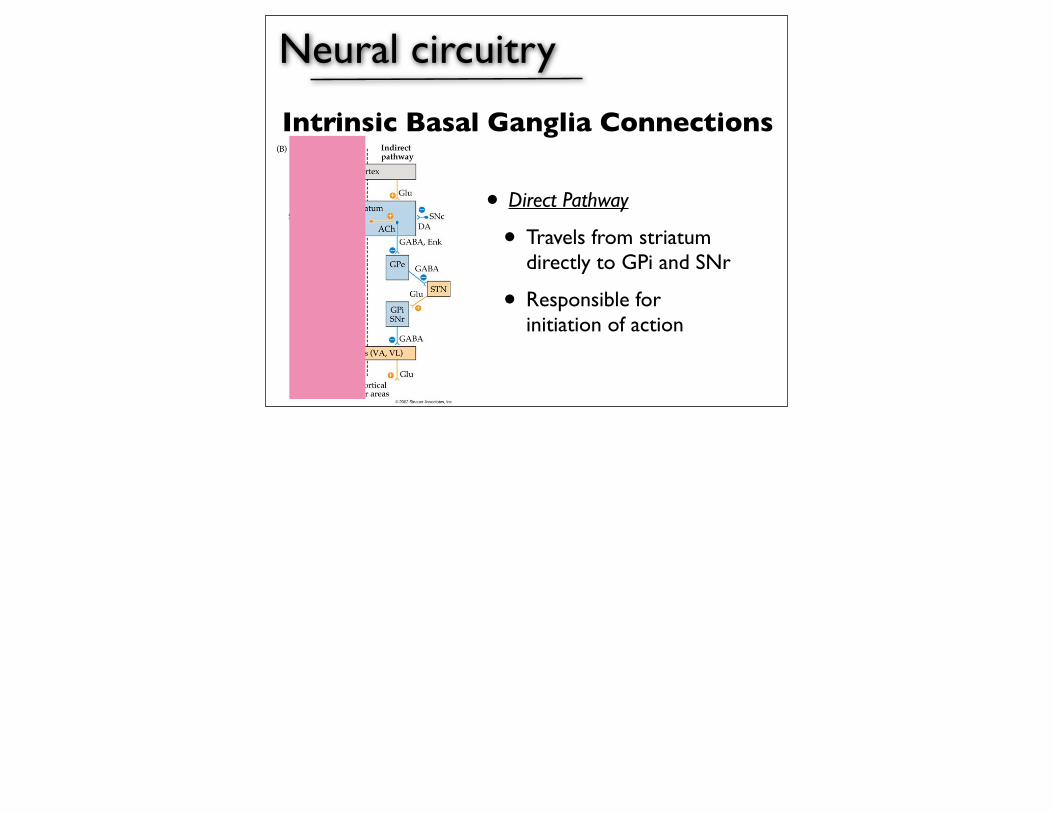
• Direct Pathway
• Travels from striatum directly to GPi and SNr
• Responsible for initiation of action
Intrinsic Basal Ganglia Connections
Neural circuitry
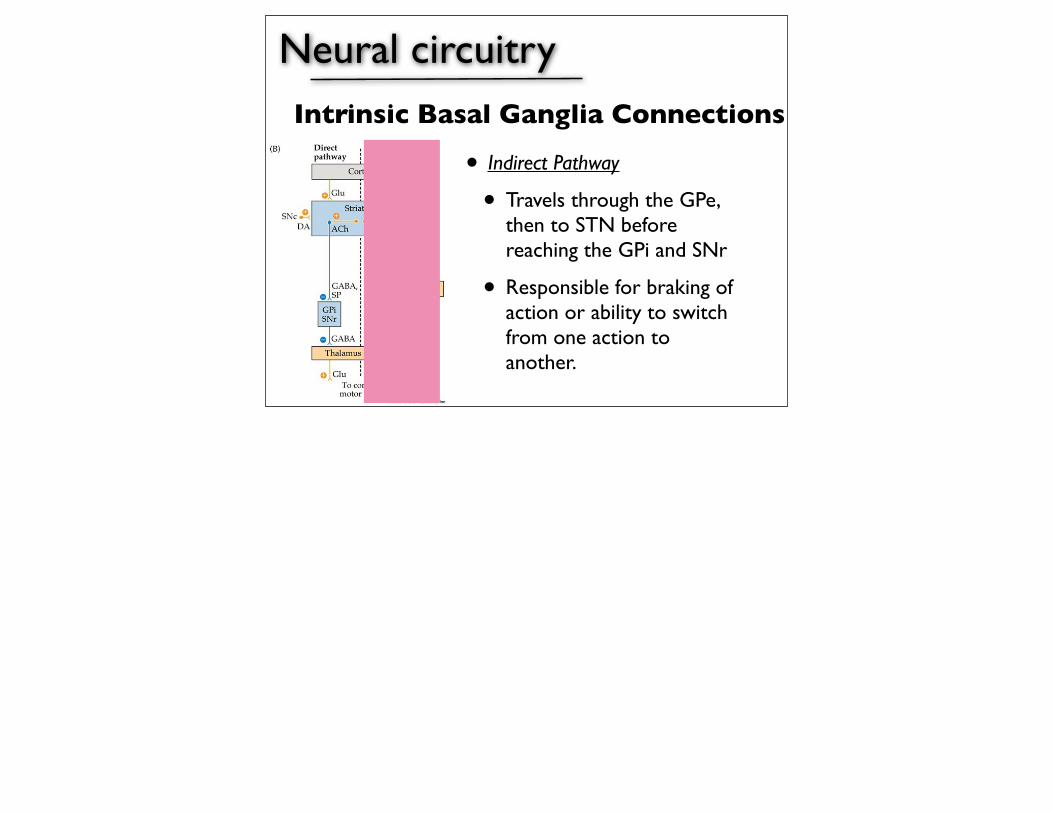
• Indirect Pathway
• Travels through the GPe, then to STN before reaching the GPi and SNr
• Responsible for braking of action or ability to switch from one action to another.
Intrinsic Basal Ganglia Connections
Neural circuitry
• Dopamine is one of the most powerful neurotransmitters influencing the motor circuit. Dopamine can either have an excitatory of inhibitory role on striatal neurons, depending on the subtype:
• D1 receptors: excitatory; direct pathway
• D2 receptors: inhibitory; indirect pathway
• In general, dopaminergic inputs to the striatum reduce basal ganglia output
Pathophysiology of PD
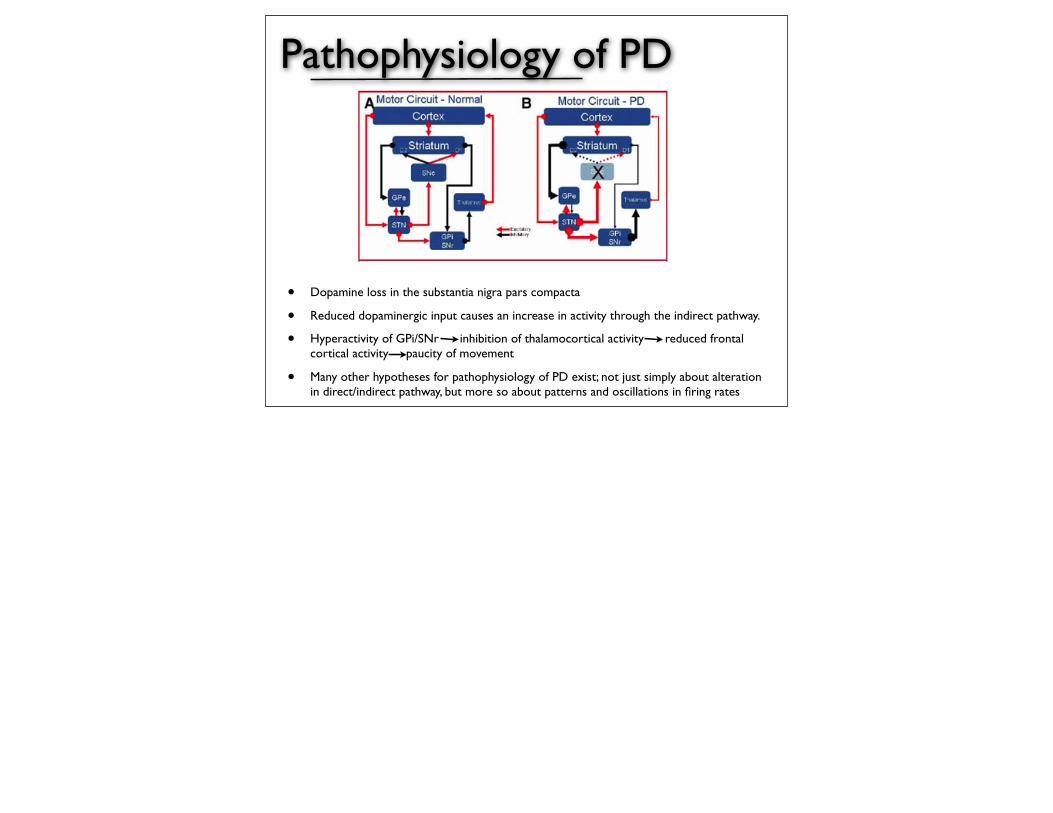
• Dopamine loss in the substantia nigra pars compacta
• Reduced dopaminergic input causes an increase in activity through the indirect pathway.
• Hyperactivity of GPi/SNr inhibition of thalamocortical activity reduced frontal cortical activity paucity of movement
• Many other hypotheses for pathophysiology of PD exist; not just simply about alteration in direct/indirect pathway, but more so about patterns and oscillations in firing rates
Pathophysiology of Dystonia
dystonic as well as hemiballistic movements, suggeststhat the widened receptive fields and altered patterns ofneuronal activity present in these disorders may providea more critical contribution to the pathophysiologicalmechanism(s) underlying their development than thechange in mean discharge rate. Alternatively, the reduc-tion in mean discharge rate that occurs in GPi in patientswith dystonia could in itself lead to the development ofaltered receptive fields and patterns of neuronal activityin the thalamus, whereas a further reduction or removalof pallidal input by means of pallidotomy may lead to animprovement or normalization of such activity. In asense, a window for the development of altered patternsand phasic responses of thalamic neuronal activity mayexist, which is dependent on the mean discharge rate ofneurons in GPi. Similarly, given previous reports ofchanges in discharge pattern of neurons in GPi depen-dent on their level of membrane polarization, increasedinhibitory input from the striatum could also underlie thealtered patterns of neuronal activity in GPi observed inpatients with dystonia. Thus altered patterns of neuronal
activity may be transmitted throughout the pallido-thalamo-cortical circuit or develop at different siteswithin the circuit, depending on local neuron or networkproperties.A model for dystonia based on these data is presented
in Figure 3A–C. Figure 3A, represents the normal state,Figure 3B a dystonic patient at rest, and Figure 3C, adystonic patient during movement. Although this is asimplified view of the anatomic connections and changesin neuronal activity in the subcortical-cortical circuitryunder each condition, the model depicts the observed andsuggested changes in neuronal activity in the neuronalnetwork mediating the development of dystonic move-ments.The exact relationship between the observed changes
in neural activity (rate, pattern, synchronicity, and re-sponse to phasic inputs) in the pallidum and the devel-opment of dystonia or to the development of phenotypi-cally or etiologically different types of dystonia (i.e.,segmental vs. generalized, primary vs. secondary) re-mains unclear. It is logical that focal changes in the re-
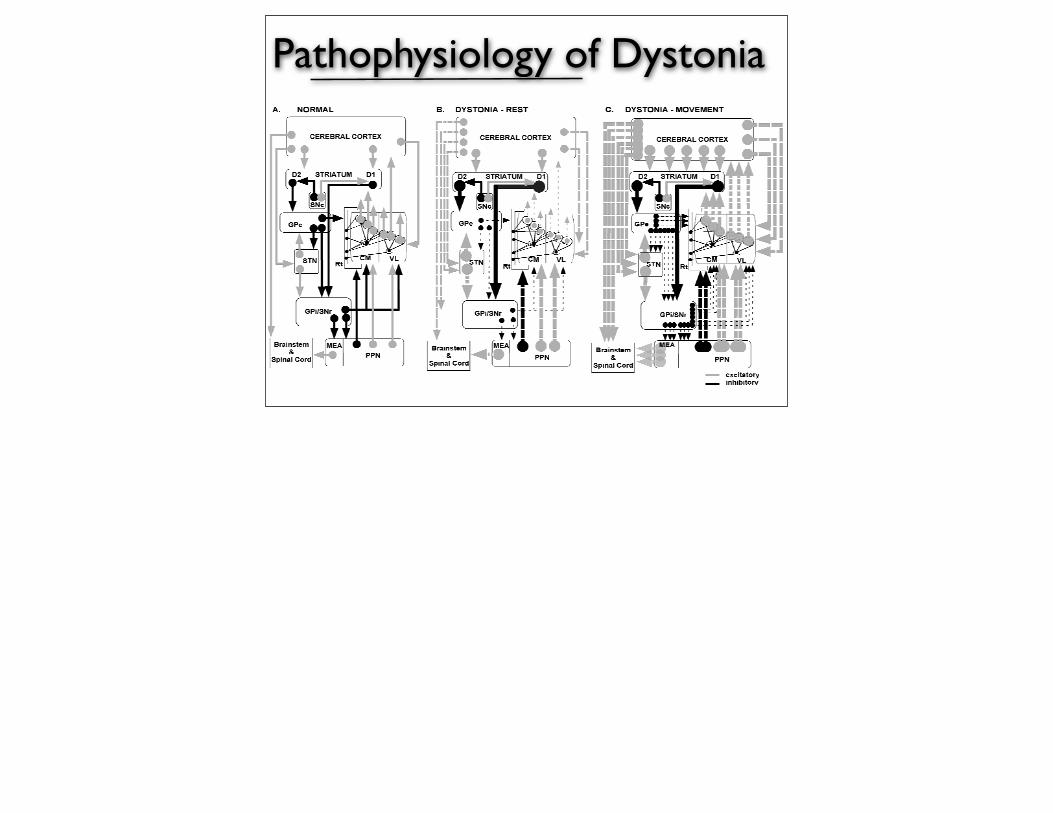
FIG. 3. Model for primary dystonia. Abbreviations are the same as in Figure 1 with the following additions: CM, centromedian; VL, motor thalamus;Rt, reticular nucleus of the thalamus; PPN, pedunculopontine nucleus; MEA, midbrain extrapyramidal area. Multiple lines of different lengths exitinga nucleus represent asynchronous neuronal activity; multiple broken lines of different lengths illustrate altered patterns of asynchronous neuronalactivity; whereas multiple broken lines of the same length illustrate altered patterns of synchronous activity. The width of the lines depicts the amountof neuronal activity. Consistent with previous reports, thalamic and pallidal activity is reduced at rest. During movement, pallidal activity is furtherreduced, leading to an increase in thalamic activity and the development of uncontrolled synchrony throughout the subcortical-cortical network. Thisreduction leads to a disruption in cortical and brainstem output and the disordered movement that occurs in dystonia. This model is not encompassingof the changes in TMS and spinal reflexes, nor does it completely attempt to fully depict the changes in intrathalamic circuitry that contribute to thesechanges. This is left for further speculation. Modification of the present model will occur as new data concerning the neuronal activity changes inthalamus neurons under the above conditions becomes available.
PATHOPHYSIOLOGY OF DYSTONIA S57
Movement Disorders, Vol. 17, Suppl. 3, 2002
Pathophysiology of Dystonia
• Multiple lines of different lengths exiting a nucleus represent asynchronous neuronal activity; multiple broken lines of different lengths illustrate altered patterns of asynchronous neuronal activity; whereas multiple broken lines of the same length illustrate altered patterns of synchronous activity.
• The width of the lines depicts the amount of neuronal activity.
• Consistent with previous reports, thalamic and pallidal activity is reduced at rest.
• During movement, pallidal activity is further reduced, leading to an increase in thalamic activity and the development of uncontrolled synchrony throughout the subcortical-cortical network.
• This reduction leads to a disruption in cortical and brainstem output and the disordered movement that occurs in dystonia.
Pathophysiology of Essential Tremor
• Does not necessarily involve the usual basal ganglia circuit.
• Related to olivocerebellar circuits in which axons from the cerebellum synpases on thalamic neurons
• VIM - affects excitability of the cerebellothalamocortical pathway.
Surgical Patient Selection
• Age
• Medically refractory
• Medically fit for surgery
• Committed to long-term follow-up re: programming, medication adjustments
• Neuropsychological assessment
• Exclude patients with severe cognitive dysfunction.
and include 1 to 5 V, 90 µs pulse width, and 130 Hz fre-quency. The larger the difference between clinical improve-ment thresholds and side-effects thresholds, the better thetherapeutic window of stimulation for the patient. Duringmacrostimulation, the patient is monitored for symptomaticimprovement such as tremor, rigidity, and bradykinesia.Dyskinesias may appear during stimulation and are gener-ally a positive predictor of the efficacy of chronic stimulation(157, 290). The importance of side-effect determinationshould be underscored, especially for patients in whom thetherapeutic efficacy is unclear or situations in which thepatient’s cooperation is hampered (30, 31, 330).
Once the DBS electrode is implanted at the final location, itmust be secured to the burr hole at the cranium. Continuousfluoroscopy is helpful to monitor the potential for electrodedisplacement. Anchoring and securing the lead can be achievedby various techniques depending on the surgeon’s preferenceand expertise. These include securing the lead to the craniumwith ligature embedded in dental cement or using mini-platesand screws, DBS manufacturer-provided plastic burr hole ringand cap, or the Medtronic Stim-Loc anchoring device(Medtronic). Once secured, the distal end of the DBS lead isattached to an extension wire or to a connector that will protectthe contacts. The distal tip is tunneled subcutaneously to theparietal/occipital region. The excess lead can be coiled around
the burr hole device or placed along the path of tunneling toserve as strain relief.
Implantation of the Pulse GeneratorThe second stage of the DBS procedure is implantation of
the implantable pulse generator (IPG), also referred to as the“neurostimulator,” and placement of the extension lead thatconnects the DBS lead to the IPG. Currently, there are twotypes of available IPGs: single channel (Medtronic Soletra)for one DBS lead, and dual channel (Medtronic Kinetra) fortwo leads. This is the last step of surgery, and it is performedunder general anesthesia. This step can be performed thesame day or in a delayed or staged fashion.
The patient is placed in a supine position, with the headturned to the opposite side of the intended site of IPG implan-tation. In brief, an infraclavicular subcutaneous pocket is cre-ated for the IPG, and the proximal end of the DBS electrode isexposed in the parietal region. A subcutaneously implantedextension wire is tunneled from the parietal region to the infr-aclavicular pocket, thus connecting the DBS electrode to theIPG pocket in the chest. The most common location for theIPG placement is infraclavicular, and it is typically marked 1to 2 cm below the clavicle and 4 cm away from the midline or2 cm from the lateral manubrial border. However, certainpatients may require placement in other locations due to body
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC821
C
FIGURE 16. A, the two commercially available electrodes each have four contactsof 1.5 mm in height and 1.27 mm in diameter and differ only in the spacingbetween contacts, as illustrated in B. C, the placement of the DBS lead, connectors,and implantable pulse generator (IPG) in a human. (A and C obtained fromwww.medtronic.com; B, printed with permission from Wiley-Liss).
BA
Surgical Patient Selection: PD6
• Idiopathic PD
• Patients with atypical parkinsonism (supranuclear palsy, nigrostrial degeneration) respond less favorably.
• Improvement with L-dopa.
• Exception: tremor.
• Extremity symptoms: tremor, rigidity, freezing, dystonia, bradykinesia
• Axial symptoms do now show marked improvement (posture, balance, gait, speech)
Surgical Patient Selection: Dystonia6
• Primary idiopathic dystonia: no discernible etiological factor responsible for onset
• Secondary dystonia: preexisting, identifiable brain insult such as perinatal hypoxia, stroke, trauma, toxin exposure, infectious sequelae. Surgery is less effective.
• Cervical dystonia.
• Appendicular symptoms
• Tardive dystonia
Surgical Patient Selection: ET6
• Resting tremor
• Distal postural tremor
• Intention/action tremor less amenable to treatment
• Head, neck, and lower-extremity tremors more difficult to treat vs upper-extremity tremors.
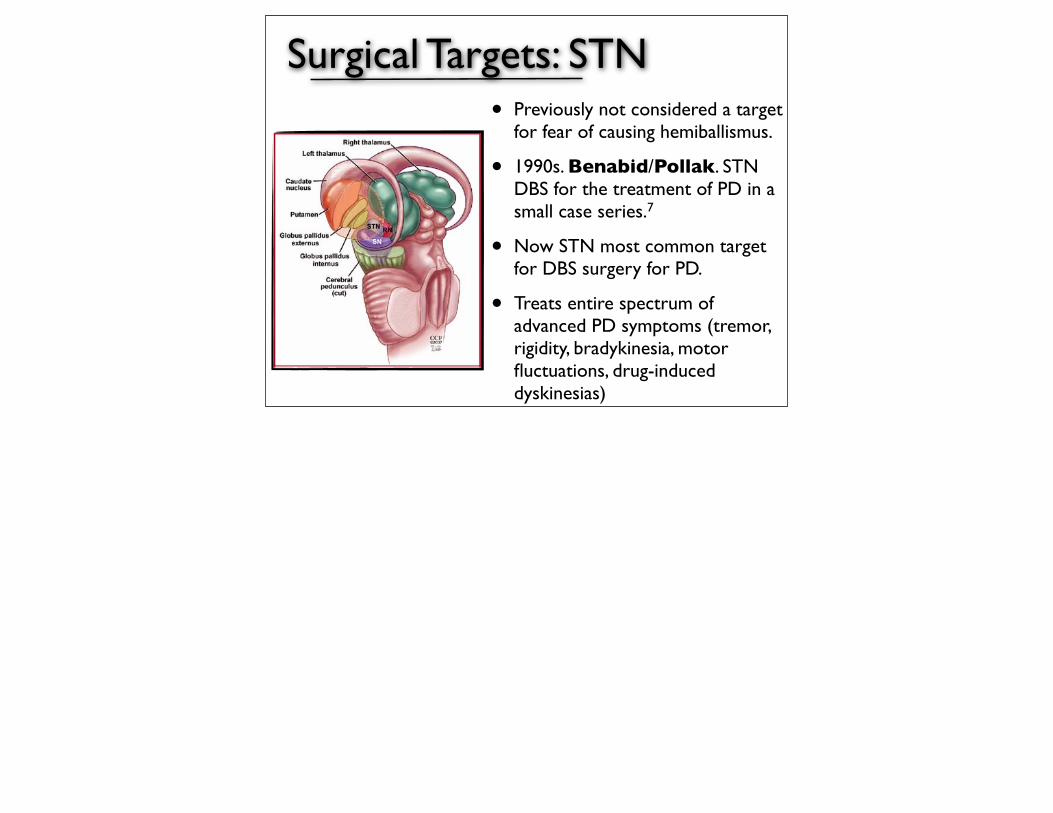
Surgical Targets: STN• Previously not considered a target
for fear of causing hemiballismus.
• 1990s. Benabid/Pollak. STN DBS for the treatment of PD in a small case series.7
• Now STN most common target for DBS surgery for PD.
• Treats entire spectrum of advanced PD symptoms (tremor, rigidity, bradykinesia, motor fluctuations, drug-induced dyskinesias)
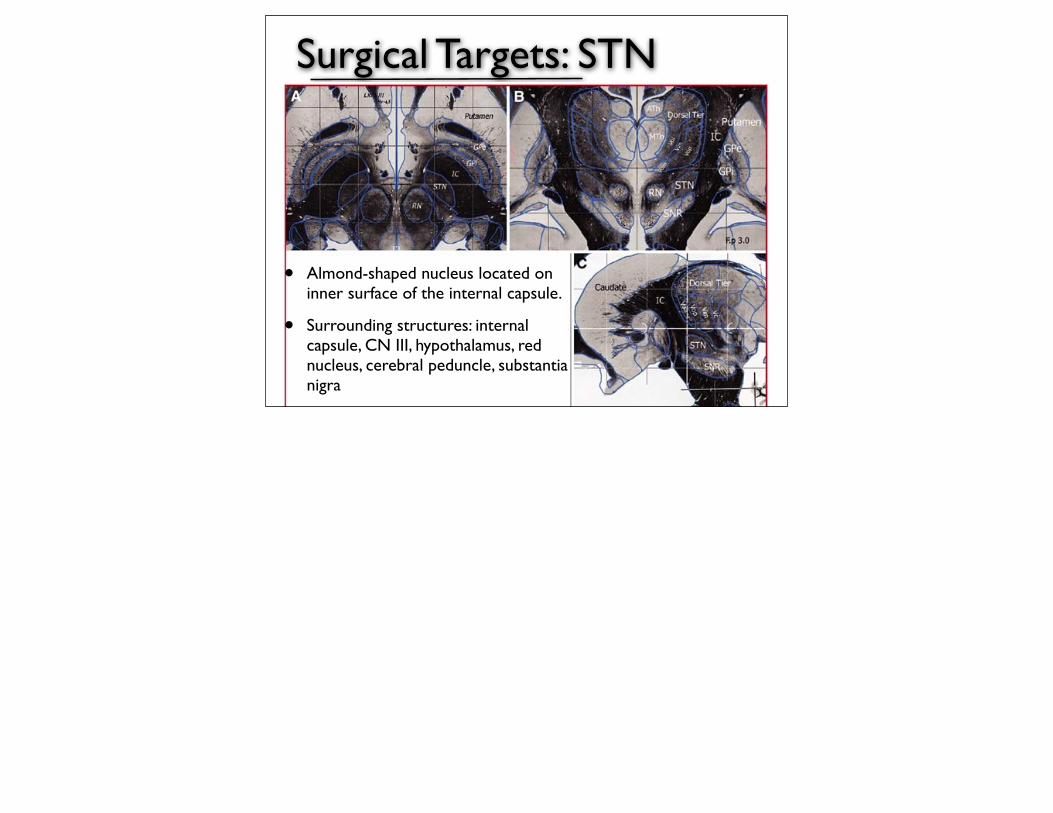
Surgical Targets: STN
• Almond-shaped nucleus located on inner surface of the internal capsule.
• Surrounding structures: internal capsule, CN III, hypothalamus, red nucleus, cerebral peduncle, substantia nigra
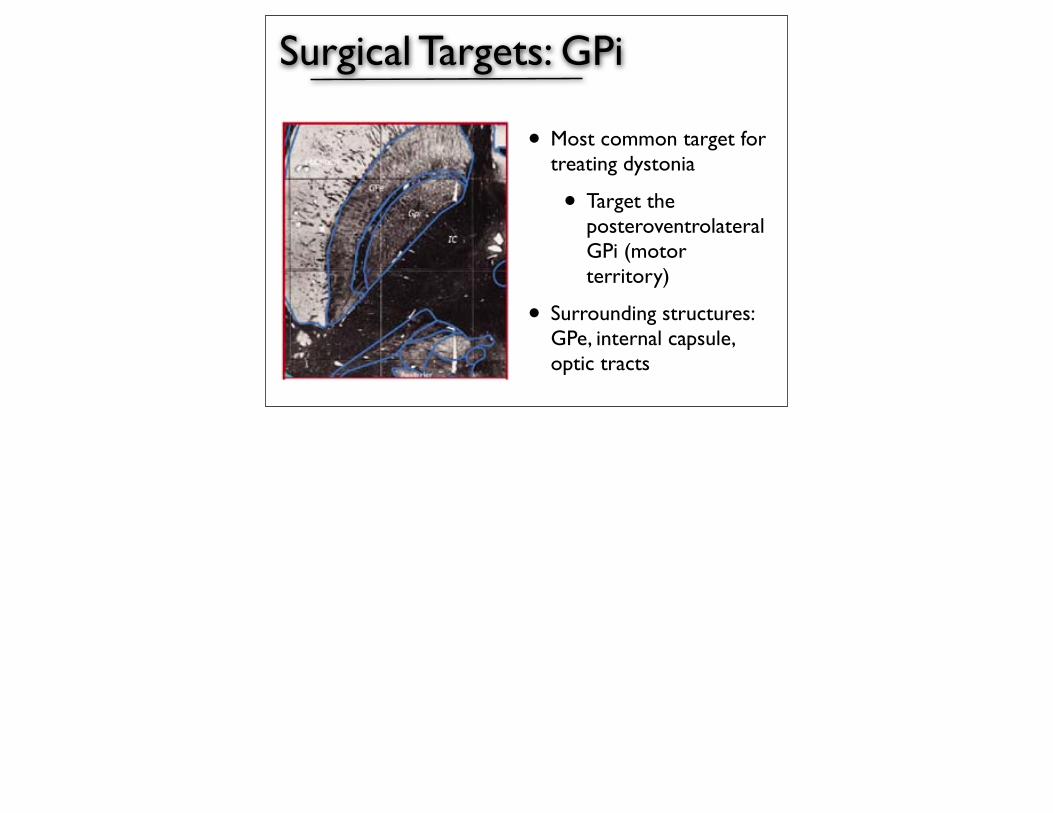
Surgical Targets: GPi
• Most common target for treating dystonia
• Target the posteroventrolateral GPi (motor territory)
• Surrounding structures: GPe, internal capsule, optic tracts
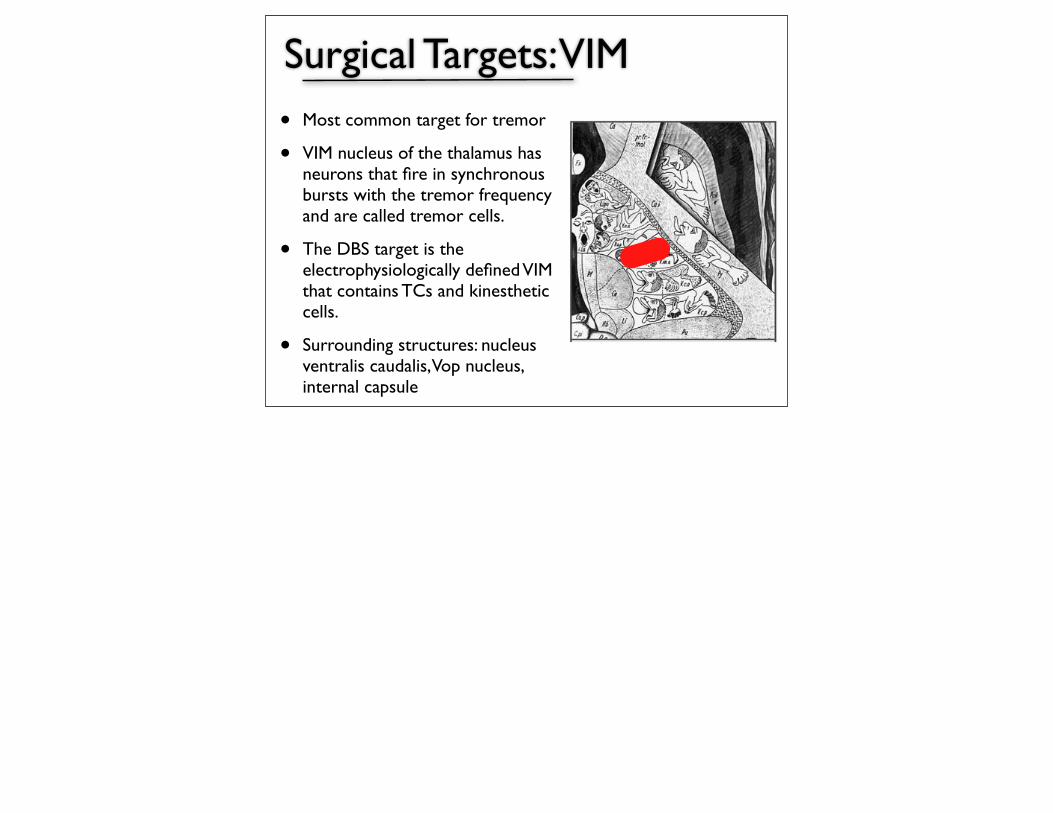
Surgical Targets: VIM
• Most common target for tremor
• VIM nucleus of the thalamus has neurons that fire in synchronous bursts with the tremor frequency and are called tremor cells.
• The DBS target is the electrophysiologically defined VIM that contains TCs and kinesthetic cells.
• Surrounding structures: nucleus ventralis caudalis, Vop nucleus, internal capsule
Aspects of Surgery
• Basic components of DBS
• Stereotactic anatomic targeting
• Physiologic target verification
• DBS lead implantation
• Implantable pulse generator/power-source placement
• Programming
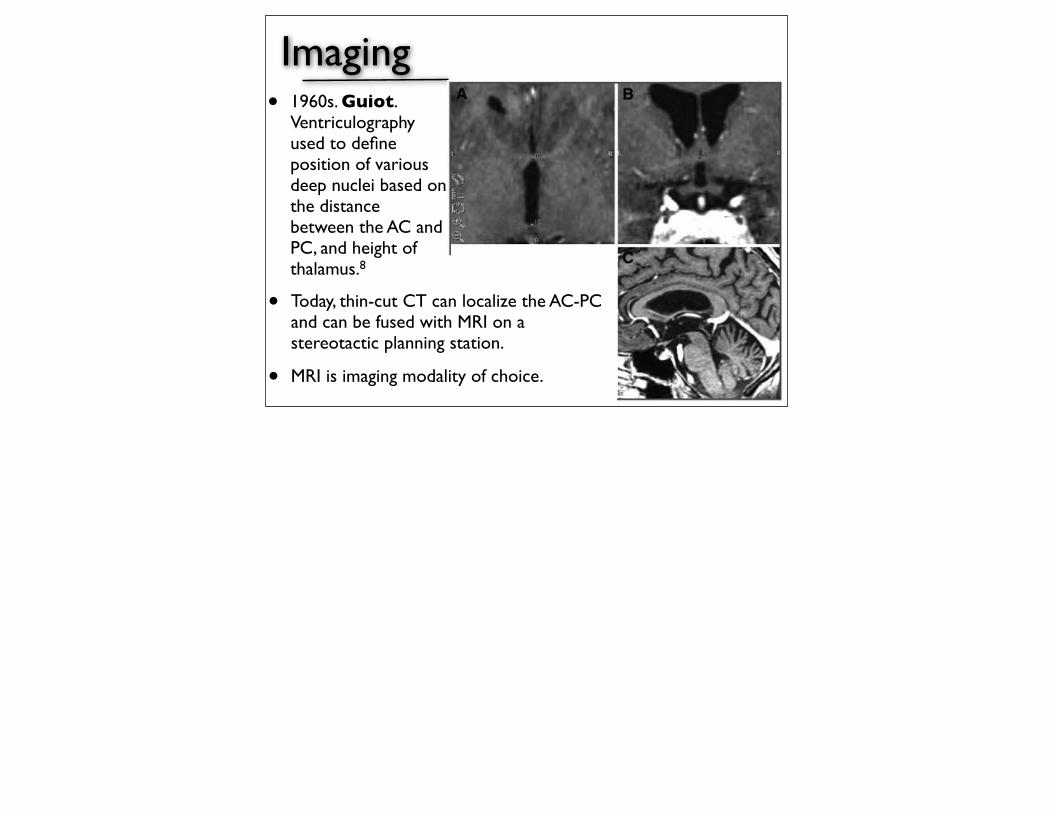
Imaging
• Today, thin-cut CT can localize the AC-PC and can be fused with MRI on a stereotactic planning station.
• MRI is imaging modality of choice.
• 1960s. Guiot. Ventriculography used to define position of various deep nuclei based on the distance between the AC and PC, and height of thalamus.8

Headframes
• Frame
• Gold standard: proven precision and reliability.
• Leksell, Cosman-Roberts-Wells
• Frame should be placed parallel to a line extending from lateral canthus to tragus, to approximate a parallel with the AC-PC line.

Headframes• Frameless• Frame-based fiducials replaced by
small screws that are visible on CT, which are secured to patient’s cranium prior to surgery.
• Pre-operative images loaded into neuronavigation, and fiducials are registered.
• Advantages: increased efficiency of surgical planning and imaging acquisition before the day of surgery, increased patient comfort with less immobilization of head and neck.

Finding the target• Indirect Targeting and Brain Atlases
• Use AC-PC coordinates to determine location of targets based on average anatomic differences with respect to the AC, PC, and MCP
• Standardized brain atlas used to locate the x, y, and z coordinates in relation to the MCP. Can be modified using neuronavigation software to fit patient’s anatomy.
• Stereotactic atlases are limited in the fact that they are derived from a small number of brains, resulting in significant variability.
Finding the target
•Direct Targeting
•Direct visualization of target nuclei using patient’s MRI
Neurophysiological Verification
• Neurophysiological techniques are necessary to refine lead positioning within a target and to optimize clinical outcome and minimize stimulation-related side effects.
• Physiological techniques:
• Microelectrode recording
• Macrostimulation
• DBS lead stimulation

Microelectrode recording
• Microelectrodes with a tip diameter between 20 - 40 um.
• Can record single units as well as deliver stimulation ( < 100 uA)
• A hydraulic or electrical microdrive advances the electrode
• Allows for delineation of the physiological signature of various nuclei and white matter tracts.
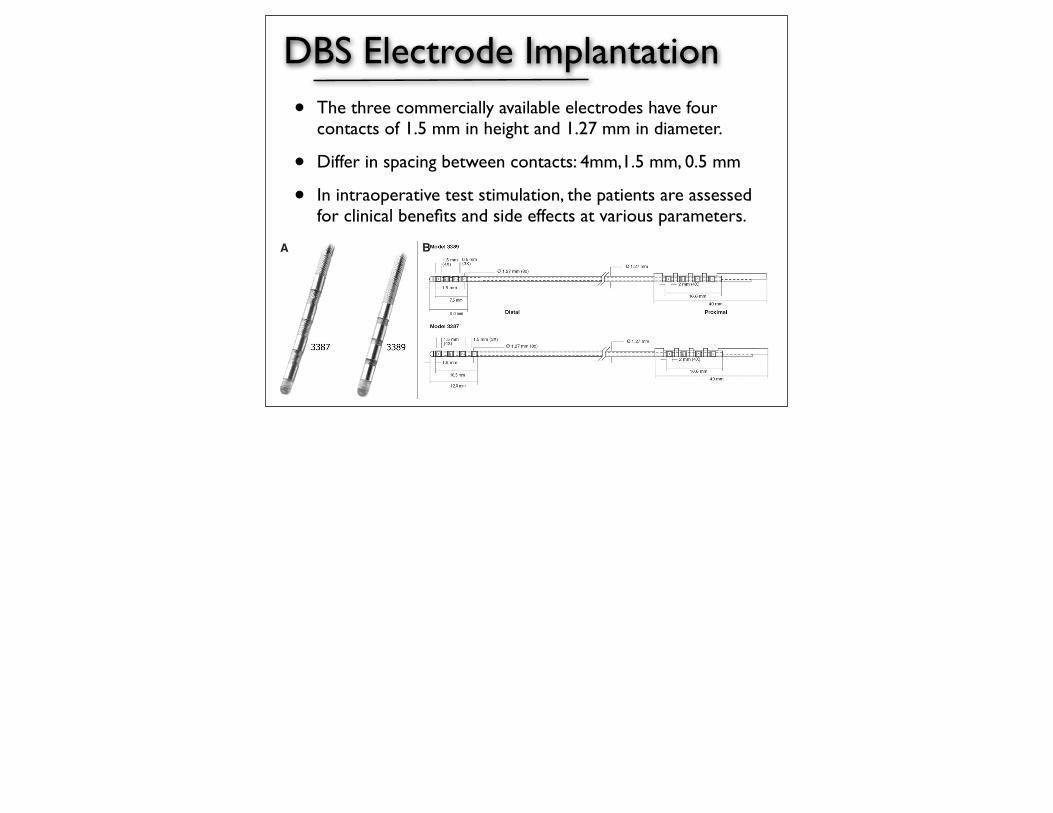
DBS Electrode Implantation• The three commercially available electrodes have four
contacts of 1.5 mm in height and 1.27 mm in diameter.
• Differ in spacing between contacts: 4mm,1.5 mm, 0.5 mm
• In intraoperative test stimulation, the patients are assessed for clinical benefits and side effects at various parameters.
and include 1 to 5 V, 90 µs pulse width, and 130 Hz fre-quency. The larger the difference between clinical improve-ment thresholds and side-effects thresholds, the better thetherapeutic window of stimulation for the patient. Duringmacrostimulation, the patient is monitored for symptomaticimprovement such as tremor, rigidity, and bradykinesia.Dyskinesias may appear during stimulation and are gener-ally a positive predictor of the efficacy of chronic stimulation(157, 290). The importance of side-effect determinationshould be underscored, especially for patients in whom thetherapeutic efficacy is unclear or situations in which thepatient’s cooperation is hampered (30, 31, 330).
Once the DBS electrode is implanted at the final location, itmust be secured to the burr hole at the cranium. Continuousfluoroscopy is helpful to monitor the potential for electrodedisplacement. Anchoring and securing the lead can be achievedby various techniques depending on the surgeon’s preferenceand expertise. These include securing the lead to the craniumwith ligature embedded in dental cement or using mini-platesand screws, DBS manufacturer-provided plastic burr hole ringand cap, or the Medtronic Stim-Loc anchoring device(Medtronic). Once secured, the distal end of the DBS lead isattached to an extension wire or to a connector that will protectthe contacts. The distal tip is tunneled subcutaneously to theparietal/occipital region. The excess lead can be coiled around
the burr hole device or placed along the path of tunneling toserve as strain relief.
Implantation of the Pulse GeneratorThe second stage of the DBS procedure is implantation of
the implantable pulse generator (IPG), also referred to as the“neurostimulator,” and placement of the extension lead thatconnects the DBS lead to the IPG. Currently, there are twotypes of available IPGs: single channel (Medtronic Soletra)for one DBS lead, and dual channel (Medtronic Kinetra) fortwo leads. This is the last step of surgery, and it is performedunder general anesthesia. This step can be performed thesame day or in a delayed or staged fashion.
The patient is placed in a supine position, with the headturned to the opposite side of the intended site of IPG implan-tation. In brief, an infraclavicular subcutaneous pocket is cre-ated for the IPG, and the proximal end of the DBS electrode isexposed in the parietal region. A subcutaneously implantedextension wire is tunneled from the parietal region to the infr-aclavicular pocket, thus connecting the DBS electrode to theIPG pocket in the chest. The most common location for theIPG placement is infraclavicular, and it is typically marked 1to 2 cm below the clavicle and 4 cm away from the midline or2 cm from the lateral manubrial border. However, certainpatients may require placement in other locations due to body
SURGERY FOR MOVEMENT DISORDERS
NEUROSURGERY VOLUME 62 | NUMBER 2 | FEBRUARY 2008 SUPPLEMENT | SHC821
C
FIGURE 16. A, the two commercially available electrodes each have four contactsof 1.5 mm in height and 1.27 mm in diameter and differ only in the spacingbetween contacts, as illustrated in B. C, the placement of the DBS lead, connectors,and implantable pulse generator (IPG) in a human. (A and C obtained fromwww.medtronic.com; B, printed with permission from Wiley-Liss).
BA
DBS Electrode Implantation
• Methods to secure electrode:
• Plates and screws
• Plastic burr hole ring and cap
• Medtronic Stim-Loc anchoring device
• Distal tip is tunneled subperiosteally to the parietal/occipital region.
Implantation of the Pulse Generator
• Usually implanted in subcutaneous infraclavicular pocket.
• Tunneled extension wire connects DBS electrode to IPG
• Available IPGs:
• Medtronic Soletra: single channel for one DBS lead
• Medtronic Kinetra: dual channel for two leads
• Medtronic Activa: dual channel, rechargeable
Complications
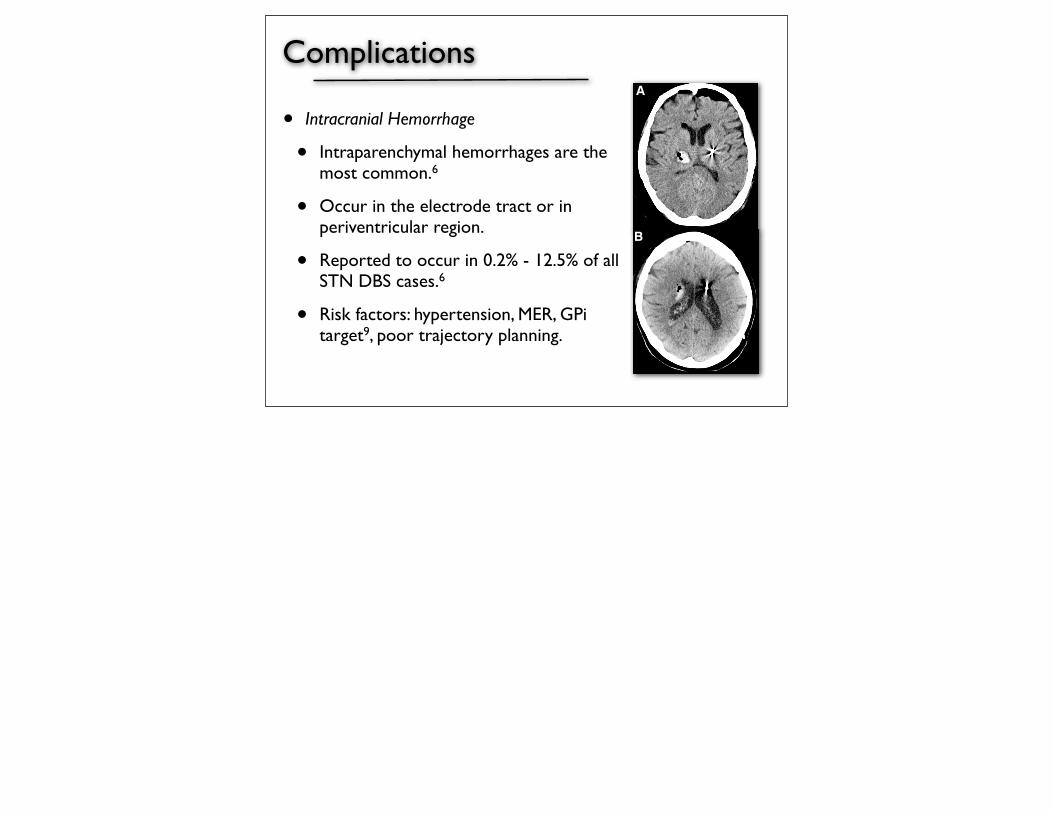
• Intracranial Hemorrhage
• Intraparenchymal hemorrhages are the most common.6
• Occur in the electrode tract or in periventricular region.
• Reported to occur in 0.2% - 12.5% of all STN DBS cases.6
• Risk factors: hypertension, MER, GPi target9, poor trajectory planning.
A
B

Complications
• Infections
• Infection rates vary from 1% - 5%6
• IPG most commonly infected site
• If hardware is not affected, can be treated with antibiotics.
• May require hardware removal.

Complications
• Hardware-related
• Most common: 2.7% - 50%6
• Includes electrode fracture, extension wire failure, lead migration, skin erosion, IPG malfunction, pain over the pulse generator.
Complications
• Stimulation-related
• Related to programming of the DBS system.
• Include dyskinesias, worsening of axial symptoms, speech dysfunction, ocular symptoms.

Outcomes: PD
original article
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 355;9 www.nejm.org august 31, 2006896
A Randomized Trial of Deep-Brain Stimulation for Parkinson’s Disease
Günther Deuschl, M.D., Ph.D., Carmen Schade-Brittinger, Paul Krack, M.D., Ph.D., Jens Volkmann, M.D., Ph.D., Helmut Schäfer, Ph.D., Kai Bötzel, M.D., Ph.D., Christine Daniels, M.D., Angela Deutschländer, M.D.,
Ulrich Dillmann, M.D., Ph.D., Wilhelm Eisner, M.D., Ph.D., Doreen Gruber, M.D., Wolfgang Hamel, M.D., Jan Herzog, M.D.,
Rüdiger Hilker, M.D., Ph.D., Stephan Klebe, M.D., Manja Klo!, M.D., Jan Koy, M.D., Martin Krause, M.D., Andreas Kupsch, M.D., Ph.D.,
Delia Lorenz, M.D., Stefan Lorenzl, M.D., Ph.D., H. Maximilian Mehdorn, M.D., Ph.D., Jean Richard Moringlane, M.D., Ph.D.,
Wolfgang Oertel, M.D., Ph.D., Marcus O. Pinsker, M.D., Heinz Reichmann, M.D., Ph.D., Alexander Reu!, M.S.,
Gerd-Helge Schneider, M.D., Alfons Schnitzler, M.D., Ph.D., Ulrich Steude, M.D., Ph.D., Volker Sturm, M.D., Ph.D., Lars Timmermann, M.D.,
Volker Tronnier, M.D., Ph.D., Thomas Trottenberg, M.D., Lars Wojtecki, M.D., Elisabeth Wolf, M.D., Werner Poewe, M.D., Ph.D.,
and Jürgen Voges, M.D., Ph.D., for the German Parkinson Study Group, Neurostimulation Section
From Christian Albrechts University, Kiel (G.D., P.K., J.V., C.D., W.H., J.H., S.K., D.L., H.M.M., M.O.P.); Philipps University, Marburg (C.S.-B., H.S., W.O., A.R.); Ludwig Maximilians University, Munich (K.B., A.D., S.L., U.S.); Homburg University, Homburg (U.D., J.R.M.); Charité Hospital, Humboldt University, Berlin (D.G., A.K., G.-H.S.,T.T.); Cologne University, Cologne, (R.H., V.S., J.V.); Heidelberg University, Heidelberg (M.Klo!, M.Krause, V.T.); Dresden Uni-versity, Dresden (J.K., H.R.); and Heinrich Heine University, Dusseldorf (A.S., L.T., L.W.) — all in Germany; and Innsbruck Medical University, Innsbruck, Austria (W.E., E.W., W.P.). Address reprint requests to Dr. Deuschl at the Department of Neur-ology, Universitätsklinikum Schleswig-Holstein, Campus Kiel, Christian Albrechts University, Schittenhelmstrasse 10, 24105 Kiel, Germany, or at [email protected].
N Engl J Med 2006;355:896-908.Copyright © 2006 Massachusetts Medical Society.
A BS TR AC T
BACKGROUNDNeurostimulation of the subthalamic nucleus reduces levodopa-related motor com-plications in advanced Parkinson’s disease. We compared this treatment plus med-ication with medical management.
METHODSIn this randomized-pairs trial, we enrolled 156 patients with advanced Parkinson’s disease and severe motor symptoms. The primary end points were the changes from baseline to six months in the quality of life, as assessed by the Parkinson’s Disease Questionnaire (PDQ-39), and the severity of symptoms without medication, accord-ing to the Unified Parkinson’s Disease Rating Scale, part III (UPDRS-III).
RESULTSPairwise comparisons showed that neurostimulation, as compared with medication alone, caused greater improvements from baseline to six months in the PDQ-39 (50 of 78 pairs, P = 0.02) and the UPDRS-III (55 of 78, P<0.001), with mean improvements of 9.5 and 19.6 points, respectively. Neurostimulation resulted in improvements of 24 to 38 percent in the PDQ-39 subscales for mobility, activities of daily living, emotional well-being, stigma, and bodily discomfort. Serious adverse events were more com-mon with neurostimulation than with medication alone (13 percent vs. 4 percent, P<0.04) and included a fatal intracerebral hemorrhage. The overall frequency of ad-verse events was higher in the medication group (64 percent vs. 50 percent, P = 0.08).
CONCLUSIONSIn this six-month study of patients under 75 years of age with severe motor compli-cations of Parkinson’s disease, neurostimulation of the subthalamic nucleus was more effective than medical management alone. (ClinicalTrials.gov number, NCT00196911.)
The New England Journal of Medicine Downloaded from www.nejm.org at YASER UNIVERSITY OF CALGARY on November 27, 2010. For personal use only. No other uses without permission.
Copyright © 2006 Massachusetts Medical Society. All rights reserved.
original article
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 355;9 www.nejm.org august 31, 2006896
A Randomized Trial of Deep-Brain Stimulation for Parkinson’s Disease
Günther Deuschl, M.D., Ph.D., Carmen Schade-Brittinger, Paul Krack, M.D., Ph.D., Jens Volkmann, M.D., Ph.D., Helmut Schäfer, Ph.D., Kai Bötzel, M.D., Ph.D., Christine Daniels, M.D., Angela Deutschländer, M.D.,
Ulrich Dillmann, M.D., Ph.D., Wilhelm Eisner, M.D., Ph.D., Doreen Gruber, M.D., Wolfgang Hamel, M.D., Jan Herzog, M.D.,
Rüdiger Hilker, M.D., Ph.D., Stephan Klebe, M.D., Manja Klo!, M.D., Jan Koy, M.D., Martin Krause, M.D., Andreas Kupsch, M.D., Ph.D.,
Delia Lorenz, M.D., Stefan Lorenzl, M.D., Ph.D., H. Maximilian Mehdorn, M.D., Ph.D., Jean Richard Moringlane, M.D., Ph.D.,
Wolfgang Oertel, M.D., Ph.D., Marcus O. Pinsker, M.D., Heinz Reichmann, M.D., Ph.D., Alexander Reu!, M.S.,
Gerd-Helge Schneider, M.D., Alfons Schnitzler, M.D., Ph.D., Ulrich Steude, M.D., Ph.D., Volker Sturm, M.D., Ph.D., Lars Timmermann, M.D.,
Volker Tronnier, M.D., Ph.D., Thomas Trottenberg, M.D., Lars Wojtecki, M.D., Elisabeth Wolf, M.D., Werner Poewe, M.D., Ph.D.,
and Jürgen Voges, M.D., Ph.D., for the German Parkinson Study Group, Neurostimulation Section
From Christian Albrechts University, Kiel (G.D., P.K., J.V., C.D., W.H., J.H., S.K., D.L., H.M.M., M.O.P.); Philipps University, Marburg (C.S.-B., H.S., W.O., A.R.); Ludwig Maximilians University, Munich (K.B., A.D., S.L., U.S.); Homburg University, Homburg (U.D., J.R.M.); Charité Hospital, Humboldt University, Berlin (D.G., A.K., G.-H.S.,T.T.); Cologne University, Cologne, (R.H., V.S., J.V.); Heidelberg University, Heidelberg (M.Klo!, M.Krause, V.T.); Dresden Uni-versity, Dresden (J.K., H.R.); and Heinrich Heine University, Dusseldorf (A.S., L.T., L.W.) — all in Germany; and Innsbruck Medical University, Innsbruck, Austria (W.E., E.W., W.P.). Address reprint requests to Dr. Deuschl at the Department of Neur-ology, Universitätsklinikum Schleswig-Holstein, Campus Kiel, Christian Albrechts University, Schittenhelmstrasse 10, 24105 Kiel, Germany, or at [email protected].
N Engl J Med 2006;355:896-908.Copyright © 2006 Massachusetts Medical Society.
A BS TR AC T
BACKGROUNDNeurostimulation of the subthalamic nucleus reduces levodopa-related motor com-plications in advanced Parkinson’s disease. We compared this treatment plus med-ication with medical management.
METHODSIn this randomized-pairs trial, we enrolled 156 patients with advanced Parkinson’s disease and severe motor symptoms. The primary end points were the changes from baseline to six months in the quality of life, as assessed by the Parkinson’s Disease Questionnaire (PDQ-39), and the severity of symptoms without medication, accord-ing to the Unified Parkinson’s Disease Rating Scale, part III (UPDRS-III).
RESULTSPairwise comparisons showed that neurostimulation, as compared with medication alone, caused greater improvements from baseline to six months in the PDQ-39 (50 of 78 pairs, P = 0.02) and the UPDRS-III (55 of 78, P<0.001), with mean improvements of 9.5 and 19.6 points, respectively. Neurostimulation resulted in improvements of 24 to 38 percent in the PDQ-39 subscales for mobility, activities of daily living, emotional well-being, stigma, and bodily discomfort. Serious adverse events were more com-mon with neurostimulation than with medication alone (13 percent vs. 4 percent, P<0.04) and included a fatal intracerebral hemorrhage. The overall frequency of ad-verse events was higher in the medication group (64 percent vs. 50 percent, P = 0.08).
CONCLUSIONSIn this six-month study of patients under 75 years of age with severe motor compli-cations of Parkinson’s disease, neurostimulation of the subthalamic nucleus was more effective than medical management alone. (ClinicalTrials.gov number, NCT00196911.)
The New England Journal of Medicine Downloaded from www.nejm.org at YASER UNIVERSITY OF CALGARY on November 27, 2010. For personal use only. No other uses without permission.
Copyright © 2006 Massachusetts Medical Society. All rights reserved.
• Unblinded trial with randomized-‐pairs design.• Compared DBS of STN vs best medical management; 156 paDents per arm.• Primary outcome measures: PDQ-‐39, UPDRS-‐III.• Pairwise comparison showed greater improvements in six months in DBS group .
• Conclusion: Neuros'mula'on of the STN more effec've than medical management alone in pa'ents < 75 years old with severe motor complica'ons of PD.

Outcomes: PD
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 362;22 nejm.org june 3, 2010 2077
original article
Pallidal versus Subthalamic Deep-Brain Stimulation for Parkinson’s Disease
Kenneth A. Follett, M.D., Ph.D., Frances M. Weaver, Ph.D., Matthew Stern, M.D., Kwan Hur, Ph.D., Crystal L. Harris, Pharm.D., Ping Luo, Ph.D.,
William J. Marks, Jr., M.D., Johannes Rothlind, Ph.D., Oren Sagher, M.D., Claudia Moy, Ph.D., Rajesh Pahwa, M.D., Kim Burchiel, M.D.,
Penelope Hogarth, M.D., Eugene C. Lai, M.D., Ph.D., John E. Duda, M.D., Kathryn Holloway, M.D., Ali Samii, M.D., Stacy Horn, D.O.,
Jeff M. Bronstein, M.D., Ph.D., Gatana Stoner, R.N., C.C.R.C., Philip A. Starr, M.D., Ph.D., Richard Simpson, M.D., Ph.D.,
Gordon Baltuch, M.D., Ph.D., Antonio De Salles, M.D., Ph.D., Grant D. Huang, Ph.D., and Domenic J. Reda, Ph.D.,
for the CSP 468 Study Group*
*The affiliations of authors are listed in the Appendix. A complete list of mem-bers of the Veterans Affairs Cooperative Studies Program (CSP) 468 study group is provided in the Supplementary Ap-pendix, available with the full text of this article at NEJM.org. Address reprint re-quests to Dr. Weaver at the Hines Vet-erans Affairs Hospital Center for Man-agement of Complex Chronic Care, 5000 S. 5th Ave., 151H, Hines, IL 60141, or at [email protected].
N Engl J Med 2010;362:2077-91.Copyright © 2010 Massachusetts Medical Society.
A bs tr ac t
BackgroundDeep-brain stimulation is the surgical procedure of choice for patients with ad-vanced Parkinson’s disease. The globus pallidus interna and the subthalamic nucle-us are accepted targets for this procedure. We compared 24-month outcomes for patients who had undergone bilateral stimulation of the globus pallidus interna (pallidal stimulation) or subthalamic nucleus (subthalamic stimulation).MethodsAt seven Veterans Affairs and six university hospitals, we randomly assigned 299 patients with idiopathic Parkinson’s disease to undergo either pallidal stimulation (152 patients) or subthalamic stimulation (147 patients). The primary outcome was the change in motor function, as blindly assessed on the Unified Parkinson’s Dis-ease Rating Scale, part III (UPDRS-III), while patients were receiving stimulation but not receiving antiparkinsonian medication. Secondary outcomes included self-reported function, quality of life, neurocognitive function, and adverse events.ResultsMean changes in the primary outcome did not differ significantly between the two study groups (P = 0.50). There was also no significant difference in self-reported func-tion. Patients undergoing subthalamic stimulation required a lower dose of dopamin-ergic agents than did those undergoing pallidal stimulation (P = 0.02). One compo-nent of processing speed (visuomotor) declined more after subthalamic stimulation than after pallidal stimulation (P = 0.03). The level of depression worsened after sub-thalamic stimulation and improved after pallidal stimulation (P = 0.02). Serious ad-verse events occurred in 51% of patients undergoing pallidal stimulation and in 56% of those undergoing subthalamic stimulation, with no significant between-group differences at 24 months.ConclusionsPatients with Parkinson’s disease had similar improvement in motor function after either pallidal or subthalamic stimulation. Nonmotor factors may reason-ably be included in the selection of surgical target for deep-brain stimulation. (ClinicalTrials.gov numbers, NCT00056563 and NCT01076452.)
The New England Journal of Medicine Downloaded from nejm.org at YASER UNIVERSITY OF CALGARY on January 15, 2011. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 362;22 nejm.org june 3, 2010 2077
original article
Pallidal versus Subthalamic Deep-Brain Stimulation for Parkinson’s Disease
Kenneth A. Follett, M.D., Ph.D., Frances M. Weaver, Ph.D., Matthew Stern, M.D., Kwan Hur, Ph.D., Crystal L. Harris, Pharm.D., Ping Luo, Ph.D.,
William J. Marks, Jr., M.D., Johannes Rothlind, Ph.D., Oren Sagher, M.D., Claudia Moy, Ph.D., Rajesh Pahwa, M.D., Kim Burchiel, M.D.,
Penelope Hogarth, M.D., Eugene C. Lai, M.D., Ph.D., John E. Duda, M.D., Kathryn Holloway, M.D., Ali Samii, M.D., Stacy Horn, D.O.,
Jeff M. Bronstein, M.D., Ph.D., Gatana Stoner, R.N., C.C.R.C., Philip A. Starr, M.D., Ph.D., Richard Simpson, M.D., Ph.D.,
Gordon Baltuch, M.D., Ph.D., Antonio De Salles, M.D., Ph.D., Grant D. Huang, Ph.D., and Domenic J. Reda, Ph.D.,
for the CSP 468 Study Group*
*The affiliations of authors are listed in the Appendix. A complete list of mem-bers of the Veterans Affairs Cooperative Studies Program (CSP) 468 study group is provided in the Supplementary Ap-pendix, available with the full text of this article at NEJM.org. Address reprint re-quests to Dr. Weaver at the Hines Vet-erans Affairs Hospital Center for Man-agement of Complex Chronic Care, 5000 S. 5th Ave., 151H, Hines, IL 60141, or at [email protected].
N Engl J Med 2010;362:2077-91.Copyright © 2010 Massachusetts Medical Society.
A bs tr ac t
BackgroundDeep-brain stimulation is the surgical procedure of choice for patients with ad-vanced Parkinson’s disease. The globus pallidus interna and the subthalamic nucle-us are accepted targets for this procedure. We compared 24-month outcomes for patients who had undergone bilateral stimulation of the globus pallidus interna (pallidal stimulation) or subthalamic nucleus (subthalamic stimulation).MethodsAt seven Veterans Affairs and six university hospitals, we randomly assigned 299 patients with idiopathic Parkinson’s disease to undergo either pallidal stimulation (152 patients) or subthalamic stimulation (147 patients). The primary outcome was the change in motor function, as blindly assessed on the Unified Parkinson’s Dis-ease Rating Scale, part III (UPDRS-III), while patients were receiving stimulation but not receiving antiparkinsonian medication. Secondary outcomes included self-reported function, quality of life, neurocognitive function, and adverse events.ResultsMean changes in the primary outcome did not differ significantly between the two study groups (P = 0.50). There was also no significant difference in self-reported func-tion. Patients undergoing subthalamic stimulation required a lower dose of dopamin-ergic agents than did those undergoing pallidal stimulation (P = 0.02). One compo-nent of processing speed (visuomotor) declined more after subthalamic stimulation than after pallidal stimulation (P = 0.03). The level of depression worsened after sub-thalamic stimulation and improved after pallidal stimulation (P = 0.02). Serious ad-verse events occurred in 51% of patients undergoing pallidal stimulation and in 56% of those undergoing subthalamic stimulation, with no significant between-group differences at 24 months.ConclusionsPatients with Parkinson’s disease had similar improvement in motor function after either pallidal or subthalamic stimulation. Nonmotor factors may reason-ably be included in the selection of surgical target for deep-brain stimulation. (ClinicalTrials.gov numbers, NCT00056563 and NCT01076452.)
The New England Journal of Medicine Downloaded from nejm.org at YASER UNIVERSITY OF CALGARY on January 15, 2011. For personal use only. No other uses without permission.
Copyright © 2010 Massachusetts Medical Society. All rights reserved.
ORIGINAL CONTRIBUTION
Bilateral Deep Brain Stimulation vsBest Medical Therapy for PatientsWith Advanced Parkinson DiseaseA Randomized Controlled TrialFrances M. Weaver, PhDKenneth Follett, MD, PhDMatthew Stern, MDKwan Hur, PhDCrystal Harris, PharmDWilliam J. Marks Jr, MDJohannes Rothlind, PhDOren Sagher, MDDomenic Reda, PhDClaudia S. Moy, PhDRajesh Pahwa, MDKim Burchiel, MDPenelope Hogarth, MDEugene C. Lai, MD, PhDJohn E. Duda, MDKathryn Holloway, MDAli Samii, MDStacy Horn, DOJeff Bronstein, MD, PhDGatana Stoner, RN, CCRCJill Heemskerk, PhDGrant D. Huang, PhDfor the CSP 468 Study Group
DEEP BRAIN STIMULATION ISthe surgical intervention ofchoice when Parkinson dis-ease (PD) motor complica-
tions are inadequately managed withmedications. Ideal candidates have fluc-tuating motor symptoms or medication-related adverse effects, few comorbidi-ties, and no cognitive or behavioral
For editorial comment see p 104.Author Affiliations and Members of the CSP 468Study Group are listed at the end of this article.Corresponding Author: Frances M. Weaver, PhD, Hines
VA Hospital, Center for Management of ComplexChronic Care, 5000 S Fifth Ave (151H), Hines, IL 60141([email protected]).
Context Deep brain stimulation is an accepted treatment for advanced Parkinsondisease (PD), although there are few randomized trials comparing treatments, and moststudies exclude older patients.
Objective To compare 6-month outcomes for patients with PD who received deepbrain stimulation or best medical therapy.
Design, Setting, and Patients Randomized controlled trial of patients who re-ceived either deep brain stimulation or best medical therapy, stratified by study siteand patient age (!70 years vs "70 years) at 7 Veterans Affairs and 6 university hos-pitals between May 2002 and October 2005. A total of 255 patients with PD (Hoehnand Yahr stage "2 while not taking medications) were enrolled; 25% were aged 70years or older. The final 6-month follow-up visit occurred in May 2006.
Intervention Bilateral deep brain stimulation of the subthalamic nucleus (n=60) orglobus pallidus (n=61). Patients receiving best medical therapy (n=134) were ac-tively managed by movement disorder neurologists.
Main Outcome Measures The primary outcome was time spent in the “on” state(good motor control with unimpeded motor function) without troubling dyskinesia,using motor diaries. Other outcomes included motor function, quality of life, neuro-cognitive function, and adverse events.
Results Patients who received deep brain stimulation gained a mean of 4.6 h/d ofon time without troubling dyskinesia compared with 0 h/d for patients who receivedbest medical therapy (between group mean difference, 4.5 h/d [95% CI, 3.7-5.4 h/d];P! .001). Motor function improved significantly (P! .001) with deep brain stimula-tion vs best medical therapy, such that 71% of deep brain stimulation patients and32% of best medical therapy patients experienced clinically meaningful motor func-tion improvements ("5 points). Compared with the best medical therapy group, thedeep brain stimulation group experienced significant improvements in the summarymeasure of quality of life and on 7 of 8 PD quality-of-life scores (P! .001). Neuro-cognitive testing revealed small decrements in some areas of information processingfor patients receiving deep brain stimulation vs best medical therapy. At least 1 seri-ous adverse event occurred in 49 deep brain stimulation patients and 15 best medicaltherapy patients (P! .001), including 39 adverse events related to the surgical pro-cedure and 1 death secondary to cerebral hemorrhage.
Conclusion In this randomized controlled trial of patients with advanced PD, deepbrain stimulation was more effective than best medical therapy in improving on timewithout troubling dyskinesias, motor function, and quality of life at 6 months, but wasassociated with an increased risk of serious adverse events.
Trial Registration clinicaltrials.gov Identifier: NCT00056563JAMA. 2009;301(1):63-73 www.jama.com
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 63
at University of Calgary on January 14, 2011jama.ama-assn.orgDownloaded from
ORIGINAL CONTRIBUTION
Bilateral Deep Brain Stimulation vsBest Medical Therapy for PatientsWith Advanced Parkinson DiseaseA Randomized Controlled TrialFrances M. Weaver, PhDKenneth Follett, MD, PhDMatthew Stern, MDKwan Hur, PhDCrystal Harris, PharmDWilliam J. Marks Jr, MDJohannes Rothlind, PhDOren Sagher, MDDomenic Reda, PhDClaudia S. Moy, PhDRajesh Pahwa, MDKim Burchiel, MDPenelope Hogarth, MDEugene C. Lai, MD, PhDJohn E. Duda, MDKathryn Holloway, MDAli Samii, MDStacy Horn, DOJeff Bronstein, MD, PhDGatana Stoner, RN, CCRCJill Heemskerk, PhDGrant D. Huang, PhDfor the CSP 468 Study Group
DEEP BRAIN STIMULATION ISthe surgical intervention ofchoice when Parkinson dis-ease (PD) motor complica-
tions are inadequately managed withmedications. Ideal candidates have fluc-tuating motor symptoms or medication-related adverse effects, few comorbidi-ties, and no cognitive or behavioral
For editorial comment see p 104.Author Affiliations and Members of the CSP 468Study Group are listed at the end of this article.Corresponding Author: Frances M. Weaver, PhD, Hines
VA Hospital, Center for Management of ComplexChronic Care, 5000 S Fifth Ave (151H), Hines, IL 60141([email protected]).
Context Deep brain stimulation is an accepted treatment for advanced Parkinsondisease (PD), although there are few randomized trials comparing treatments, and moststudies exclude older patients.
Objective To compare 6-month outcomes for patients with PD who received deepbrain stimulation or best medical therapy.
Design, Setting, and Patients Randomized controlled trial of patients who re-ceived either deep brain stimulation or best medical therapy, stratified by study siteand patient age (!70 years vs "70 years) at 7 Veterans Affairs and 6 university hos-pitals between May 2002 and October 2005. A total of 255 patients with PD (Hoehnand Yahr stage "2 while not taking medications) were enrolled; 25% were aged 70years or older. The final 6-month follow-up visit occurred in May 2006.
Intervention Bilateral deep brain stimulation of the subthalamic nucleus (n=60) orglobus pallidus (n=61). Patients receiving best medical therapy (n=134) were ac-tively managed by movement disorder neurologists.
Main Outcome Measures The primary outcome was time spent in the “on” state(good motor control with unimpeded motor function) without troubling dyskinesia,using motor diaries. Other outcomes included motor function, quality of life, neuro-cognitive function, and adverse events.
Results Patients who received deep brain stimulation gained a mean of 4.6 h/d ofon time without troubling dyskinesia compared with 0 h/d for patients who receivedbest medical therapy (between group mean difference, 4.5 h/d [95% CI, 3.7-5.4 h/d];P! .001). Motor function improved significantly (P! .001) with deep brain stimula-tion vs best medical therapy, such that 71% of deep brain stimulation patients and32% of best medical therapy patients experienced clinically meaningful motor func-tion improvements ("5 points). Compared with the best medical therapy group, thedeep brain stimulation group experienced significant improvements in the summarymeasure of quality of life and on 7 of 8 PD quality-of-life scores (P! .001). Neuro-cognitive testing revealed small decrements in some areas of information processingfor patients receiving deep brain stimulation vs best medical therapy. At least 1 seri-ous adverse event occurred in 49 deep brain stimulation patients and 15 best medicaltherapy patients (P! .001), including 39 adverse events related to the surgical pro-cedure and 1 death secondary to cerebral hemorrhage.
Conclusion In this randomized controlled trial of patients with advanced PD, deepbrain stimulation was more effective than best medical therapy in improving on timewithout troubling dyskinesias, motor function, and quality of life at 6 months, but wasassociated with an increased risk of serious adverse events.
Trial Registration clinicaltrials.gov Identifier: NCT00056563JAMA. 2009;301(1):63-73 www.jama.com
©2009 American Medical Association. All rights reserved. (Reprinted) JAMA, January 7, 2009—Vol 301, No. 1 63
at University of Calgary on January 14, 2011jama.ama-assn.orgDownloaded from
• Blinded assessment, randomized controlled trial• DBS (STN/GPi) versus best medical therapy; 255 paDents, 25% age >
70• Primary outcome measures: Time spent in on state (good motor
control with unimpeded motor funcDon) without troubling dyskinesia.
• DBS paDents gained a mean of 4.6 h/d versus 0 h/d for paDents with best medical therapy. Improvements in quality of life measurements.
• Conclusion: DBS more effec've than best medical therapy in improving on 'me without troubling dyskinesias, motor func'on, and quality of life at 6 months.
• Bilateral DBS STN versus bilateral DBS GPi; 299 paDents randomized.• Primary outcome: motor funcDon using UPDRS-‐III• No staDsDcally significant difference in UPDRS-‐III at 24 months
(sDmulaDon, no medicaDon). • NeurocogniDve funcDon with respect to processing speed index
decreased in paDents with STN DBS (mean difference 2.5, p = 0.03).• Beck Depression score worse for paDents undergoing STN (mean
difference 1.9, p = 0.02).• Use of dopaminergic medicaDons decreased in paDents undergoing
STN sDmulaDon. • SDmulaDon amplitudes and pulse widths lower on average for STN
DBS.• Conclusion: Pa'ents with PD had similar improvement in motor
func'on aHer either GPi or STN s'mula'on. Results of non-‐motor factors may help in selec'on of surgical target for individual pa'ents.
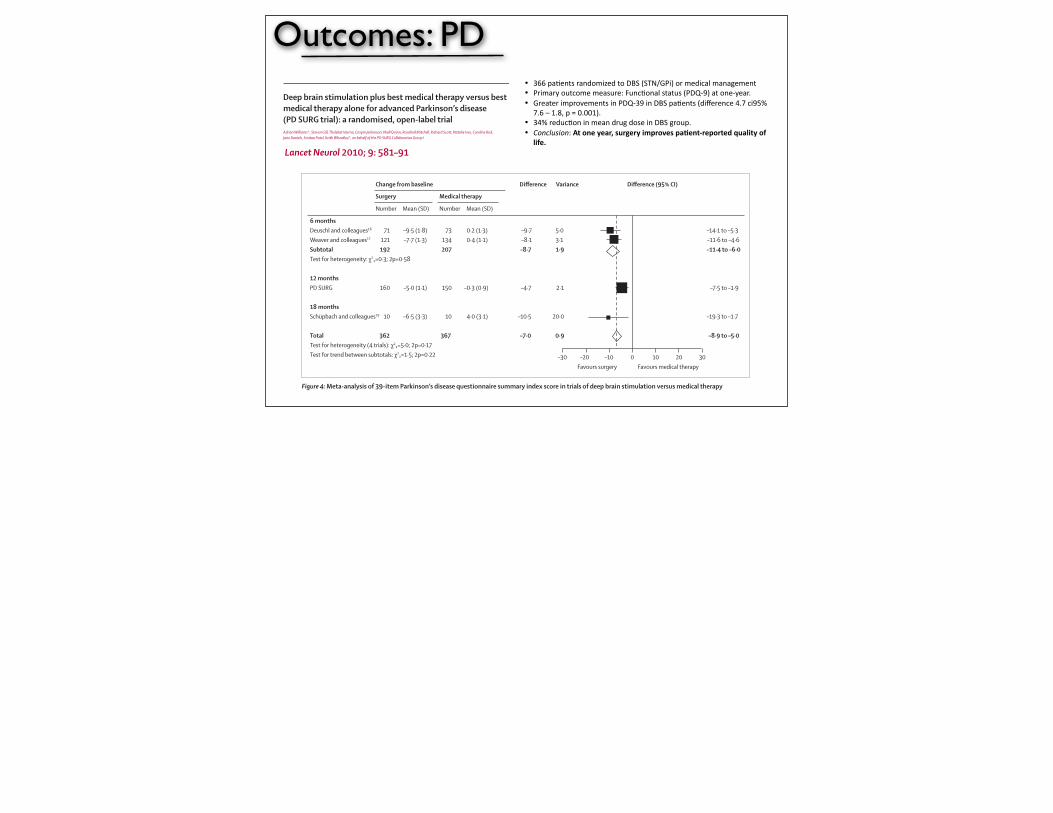
Outcomes: PD• 366 paDents randomized to DBS (STN/GPi) or medical management• Primary outcome measure: FuncDonal status (PDQ-‐9) at one-‐year.• Greater improvements in PDQ-‐39 in DBS paDents (difference 4.7 ci95%
7.6 – 1.8, p = 0.001). • 34% reducDon in mean drug dose in DBS group. • Conclusion: At one year, surgery improves pa'ent-‐reported quality of
life.
Articles
www.thelancet.com/neurology Vol 9 June 2010 581
Lancet Neurol 2010; 9: 581–91
Published OnlineApril 29, 2010DOI:10.1016/S1474-4422(10)70093-4
See Refl ection and Reactionpage 558
*Contributed equally
†Members listed at end of paper
Queen Elizabeth Hospital, Birmingham, Birmingham, UK (Prof A Williams MD, R Mitchell FRCS); Frenchay Hospital, Bristol, UK (Prof S Gill FRCS); Walton Centre for Neurology and Neurosurgery, Liverpool, UK (T Varma FRCS[Ed]); University of Oxford, Oxford, UK (Prof C Jenkinson DPhil); UCL Institute of Neurology, London, UK (Prof N Quinn MD); Russell Cairns Unit, John Radcliff e Hospital, Oxford, UK (R Scott PhD); and University of Birmingham, Birmingham, UK (N Ives MSc, C Rick PhD, J Daniels MSc, S Patel MSc, Prof K Wheatley DPhil)
Correspondence to:Natalie Ives, PD SURG Trial Offi ce, University of Birmingham Clinical Trials Unit, College of Medical and Dental Sciences, Robert Aitken Institute, University of Birmingham, Birmingham B15 2TT, [email protected]
Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson’s disease (PD SURG trial): a randomised, open-label trialAdrian Williams*, Steven Gill, Thelekat Varma, Crispin Jenkinson, Niall Quinn, Rosalind Mitchell, Richard Scott, Natalie Ives, Caroline Rick, Jane Daniels, Smitaa Patel, Keith Wheatley*, on behalf of the PD SURG Collaborative Group†
SummaryBackground Surgical intervention for advanced Parkinson’s disease is an option if medical therapy fails to control symptoms adequately. We aimed to assess whether surgery and best medical therapy improved self-reported quality of life more than best medical therapy alone in patients with advanced Parkinson’s disease.
Methods The PD SURG trial is an ongoing randomised, open-label trial. At 13 neurosurgical centres in the UK, between November, 2000, and December, 2006, patients with Parkinson’s disease that was not adequately controlled by medical therapy were randomly assigned by use of a computerised minimisation procedure to immediate surgery (lesioning or deep brain stimulation at the discretion of the local clinician) and best medical therapy or to best medical therapy alone. Patients were analysed in the treatment group to which they were randomised, irrespective of whether they received their allocated treatment. The primary endpoint was patient self-reported quality of life on the 39-item Parkinson’s disease questionnaire (PDQ-39). Changes between baseline and 1 year were compared by use of t tests. This trial is registered with Current Controlled Trials, number ISRCTN34111222.
Findings 366 patients were randomly assigned to receive immediate surgery and best medical therapy (183) or best medical therapy alone (183). All patients who had surgery had deep brain stimulation. At 1 year, the mean improvement in PDQ-39 summary index score compared with baseline was 5·0 points in the surgery group and 0·3 points in the medical therapy group (diff erence –4·7, 95% CI –7·6 to –1·8; p=0·001); the diff erence in mean change in PDQ-39 score in the mobility domain between the surgery group and the best medical therapy group was –8·9 (95% CI –13·8 to –4·0; p=0·0004), in the activities of daily living domain was –12·4 (–17·3 to –7·5; p<0·0001), and in the bodily discomfort domain was –7·5 (–12·6 to –2·4; p=0·004). Diff erences between groups in all other domains of the PDQ-39 were not signifi cant. 36 (19%) patients had serious surgery-related adverse events; there were no suicides but there was one procedure-related death. 20 patients in the surgery group and 13 in the best medical therapy group had serious adverse events related to Parkinson’s disease and drug treatment.
Interpretation At 1 year, surgery and best medical therapy improved patient self-reported quality of life more than best medical therapy alone in patients with advanced Parkinson’s disease. These diff erences are clinically meaningful, but surgery is not without risk and targeting of patients most likely to benefi t might be warranted.
Funding UK Medical Research Council, Parkinson’s UK, and UK Department of Health.
IntroductionParkinson’s disease is caused in part by loss of dopaminergic neurons in the substantia nigra pars compacta; the resultant abnormal neuronal oscillatory and synchronous activity between the subthalamic nucleus, globus pallidus pars interna, and cerebral cortex leads to increasing problems with tremor, rigidity, bradykinesia, and postural disturbances.1 Levodopa and other dopaminergic drugs relieve these movement disorders,2 but dyskinesia and motor fl uctuations develop after a few years.
Most neurosurgery for Parkinson’s disease has been done on the thalamus, globus pallidus pars interna, or subthalamic nucleus, using either lesioning or high frequency deep brain stimulation. In recent years, advances in imaging have increased the precision of surgical interventions; this and advances in the
understanding of basal ganglia physiology3–5 have meant that deep brain stimulation of the subthalamic nucleus has been preferred.6
In the late 1990s, there was little reliable evidence from randomised trials on the effi cacy and safety of surgery.7 Thus, we started the PD SURG trial with the aim of comparing the eff ect of surgery with best medical therapy in patients with advanced Parkinson’s disease. This report presents the results at 1 year’s follow-up.
MethodsPatientsPD SURG is a randomised, open-label trial. Patients with Parkinson’s disease for whom current medical therapy was not providing adequate symptomatic control were eligible. Inclusion criteria were diagnosis of Parkinson’s disease according to the UK Brain Bank
For the trial protocol see http://www.pdsurg.bham.ac.uk/investigators/documentation
Articles
www.thelancet.com/neurology Vol 9 June 2010 581
Lancet Neurol 2010; 9: 581–91
Published OnlineApril 29, 2010DOI:10.1016/S1474-4422(10)70093-4
See Refl ection and Reactionpage 558
*Contributed equally
†Members listed at end of paper
Queen Elizabeth Hospital, Birmingham, Birmingham, UK (Prof A Williams MD, R Mitchell FRCS); Frenchay Hospital, Bristol, UK (Prof S Gill FRCS); Walton Centre for Neurology and Neurosurgery, Liverpool, UK (T Varma FRCS[Ed]); University of Oxford, Oxford, UK (Prof C Jenkinson DPhil); UCL Institute of Neurology, London, UK (Prof N Quinn MD); Russell Cairns Unit, John Radcliff e Hospital, Oxford, UK (R Scott PhD); and University of Birmingham, Birmingham, UK (N Ives MSc, C Rick PhD, J Daniels MSc, S Patel MSc, Prof K Wheatley DPhil)
Correspondence to:Natalie Ives, PD SURG Trial Offi ce, University of Birmingham Clinical Trials Unit, College of Medical and Dental Sciences, Robert Aitken Institute, University of Birmingham, Birmingham B15 2TT, [email protected]
Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson’s disease (PD SURG trial): a randomised, open-label trialAdrian Williams*, Steven Gill, Thelekat Varma, Crispin Jenkinson, Niall Quinn, Rosalind Mitchell, Richard Scott, Natalie Ives, Caroline Rick, Jane Daniels, Smitaa Patel, Keith Wheatley*, on behalf of the PD SURG Collaborative Group†
SummaryBackground Surgical intervention for advanced Parkinson’s disease is an option if medical therapy fails to control symptoms adequately. We aimed to assess whether surgery and best medical therapy improved self-reported quality of life more than best medical therapy alone in patients with advanced Parkinson’s disease.
Methods The PD SURG trial is an ongoing randomised, open-label trial. At 13 neurosurgical centres in the UK, between November, 2000, and December, 2006, patients with Parkinson’s disease that was not adequately controlled by medical therapy were randomly assigned by use of a computerised minimisation procedure to immediate surgery (lesioning or deep brain stimulation at the discretion of the local clinician) and best medical therapy or to best medical therapy alone. Patients were analysed in the treatment group to which they were randomised, irrespective of whether they received their allocated treatment. The primary endpoint was patient self-reported quality of life on the 39-item Parkinson’s disease questionnaire (PDQ-39). Changes between baseline and 1 year were compared by use of t tests. This trial is registered with Current Controlled Trials, number ISRCTN34111222.
Findings 366 patients were randomly assigned to receive immediate surgery and best medical therapy (183) or best medical therapy alone (183). All patients who had surgery had deep brain stimulation. At 1 year, the mean improvement in PDQ-39 summary index score compared with baseline was 5·0 points in the surgery group and 0·3 points in the medical therapy group (diff erence –4·7, 95% CI –7·6 to –1·8; p=0·001); the diff erence in mean change in PDQ-39 score in the mobility domain between the surgery group and the best medical therapy group was –8·9 (95% CI –13·8 to –4·0; p=0·0004), in the activities of daily living domain was –12·4 (–17·3 to –7·5; p<0·0001), and in the bodily discomfort domain was –7·5 (–12·6 to –2·4; p=0·004). Diff erences between groups in all other domains of the PDQ-39 were not signifi cant. 36 (19%) patients had serious surgery-related adverse events; there were no suicides but there was one procedure-related death. 20 patients in the surgery group and 13 in the best medical therapy group had serious adverse events related to Parkinson’s disease and drug treatment.
Interpretation At 1 year, surgery and best medical therapy improved patient self-reported quality of life more than best medical therapy alone in patients with advanced Parkinson’s disease. These diff erences are clinically meaningful, but surgery is not without risk and targeting of patients most likely to benefi t might be warranted.
Funding UK Medical Research Council, Parkinson’s UK, and UK Department of Health.
IntroductionParkinson’s disease is caused in part by loss of dopaminergic neurons in the substantia nigra pars compacta; the resultant abnormal neuronal oscillatory and synchronous activity between the subthalamic nucleus, globus pallidus pars interna, and cerebral cortex leads to increasing problems with tremor, rigidity, bradykinesia, and postural disturbances.1 Levodopa and other dopaminergic drugs relieve these movement disorders,2 but dyskinesia and motor fl uctuations develop after a few years.
Most neurosurgery for Parkinson’s disease has been done on the thalamus, globus pallidus pars interna, or subthalamic nucleus, using either lesioning or high frequency deep brain stimulation. In recent years, advances in imaging have increased the precision of surgical interventions; this and advances in the
understanding of basal ganglia physiology3–5 have meant that deep brain stimulation of the subthalamic nucleus has been preferred.6
In the late 1990s, there was little reliable evidence from randomised trials on the effi cacy and safety of surgery.7 Thus, we started the PD SURG trial with the aim of comparing the eff ect of surgery with best medical therapy in patients with advanced Parkinson’s disease. This report presents the results at 1 year’s follow-up.
MethodsPatientsPD SURG is a randomised, open-label trial. Patients with Parkinson’s disease for whom current medical therapy was not providing adequate symptomatic control were eligible. Inclusion criteria were diagnosis of Parkinson’s disease according to the UK Brain Bank
For the trial protocol see http://www.pdsurg.bham.ac.uk/investigators/documentation
Articles
588 www.thelancet.com/neurology Vol 9 June 2010
seen in our trial is smaller than perhaps anticipated from the numerous small uncontrolled series that have suggested large eff ects of surgery.22,23
PD SURG, along with other reported randomised trials,16,17,19 shows benefi ts for surgery over best medical treatment in patients with advanced Parkinson’s disease, even when apomorphine is available, while also confi rming that there are risks associated with surgery. A meta-analysis of PDQ-39 summary index scores showed that the results of the trials are generally consistent with each other (test for heterogeneity, p=0·2; fi gure 4), although there is evidence of heterogeneity of treatment eff ect between the trials with 6 months of follow-up and PD SURG with 12 months of follow-up (test for interaction, p=0·04).
The PD SURG results at 1 year show smaller diff erences between the groups in the PDQ-39 summary index (4·7 points) than was seen in the two trials that reported results after 6 months (8·7 points).16,17 Although from a statistical perspective this diff erence is not substantial and might be a chance eff ect, it is worth considering potential alternative explanations based on diff erences in the trial designs. First, it is possible that there is a large immediate eff ect of surgery, whether real or in part related to an early so-called honeymoon eff ect,18 which gradually decreases over time. If the benefi ts of surgery are relatively transient, this would call into question the long-term value of surgery. Second, there might have been better drug treatment of Parkinson’s disease in the medical group of PD SURG than in the other two trials, because of the use of apomorphine in over one-third of patients in this group. Apomorphine is an eff ective drug in advanced Parkinson’s disease2 and can be given by continuous infusion to enable a more constant dose to be delivered to the patient, thereby smoothing out on–off periods and fl uctuations. However, apomorphine is expensive, and thus in the UK tends to be
used only when other drugs have failed to control the symptoms of Parkinson’s disease adequately; that is, it might be used in the same situations as surgery for patients with advanced Parkinson’s disease. Hence, a comparison of the eff ects of surgery plus medical therapy versus medical therapy, in a population of patients whose treatment could have included apomorphine (as in PD SURG), provides better evidence on the relative benefi ts of surgery than a comparison with medical therapy not including apomorphine. However, apomorphine is less widely used outside the UK, and was not reported as being widely used in the other trials.16,17 Administration of apomorphine is more complicated than for other Parkinson’s disease drugs, requiring infusion and monitoring. Nevertheless, because of its effi cacy, apomorphine use might become more common, and thus the results of PD SURG could have wider relevance in future. Optimisation of medical therapy might lead to a smaller comparative advantage for surgery. Nevertheless, surgery is still a valid treatment because patients would need to have only a one-off procedure (albeit with need for stimulator adjustment and replacement) rather than regular administration of an expensive drug. Whether technical aspects of the procedure, such as electrode location within the target site, are factors that could be improved are also important to consider.24,25
Substantially more patients in the surgery group had serious adverse events than did patients in the medical therapy group, confi rming that deep brain stimulation surgery for Parkinson’s disease is not without risks.26,27 Reporting of all serious adverse events, whether surgery related, disease related, or drug related, was mandatory in both the surgical and medical groups. Because a 6-month postoperation form that included serious adverse events was completed only in the surgical group, there could have been diff erential reporting of serious adverse events
Figure 4: Meta-analysis of 39-item Parkinson’s disease questionnaire summary index score in trials of deep brain stimulation versus medical therapy
6 monthsDeuschl and colleagues16 71 –9·5 (1·8) 73 0·2 (1·3) –9·7 5·0 –14·1 to –5·3Weaver and colleagues17 121 –7·7 (1·3) 134 0·4 (1·1) –8·1 3·1 –11·6 to –4·6Subtotal 192 207 –8·7 1·9 –11·4 to –6·0Test for heterogeneity: χ2₁=0·3; 2p=0·58
12 monthsPD SURG 160 –5·0 (1·1) 150 –0·3 (0·9) –4·7 2·1 –7·5 to –1·9
18 monthsSchüpbach and colleagues19 10 –6·5 (3·3) 10 4·0 (3·1) –10·5 20·0 –19·3 to –1·7
Total 362 367 –7·0 0·9 –8·9 to –5·0Test for heterogeneity (4 trials): χ2₃=5·0; 2p=0·17Test for trend between subtotals: χ2₁=1·5; 2p=0·22
Number Mean (SD) Number Mean (SD)
Surgery Medical therapy
Change from baseline Difference Variance Difference (95% CI)
–30 200–20 30Favours surgery Favours medical therapy
–10 10
Outcomes: Dystonia• ProspecDve study of 22 paDents undergoing bilateral GPi DBS for primary
dystonia.• Outcome measures: Movement score (Burke-‐Fahn-‐Marsden), global
disability, quality of life (SF-‐36), medicaDon use.• Decrease by 51% of BFM at 12 months (p < 0.001). StaDsDcally significant
improvements in all other domains. • Greatest motor improvement in neck, trunk, and limbs; facial movement
and speech were unchanged. • PaDents with phasic movement had greater improvements than those with
tonic posturing; post hoc analysis• Conclusions: Bilateral DBS of the GPi resulted in decrease in severity of
dystonia and func'onal disability and improved quality of life in pa'ents with generalized primary dystonia.
n engl j med
352;5
www.nejm.org february
3, 2005
The
new england journal
of
medicine
459
original article
Bilateral Deep-Brain Stimulation of the Globus Pallidus in Primary Generalized Dystonia
Marie Vidailhet, M.D., Ph.D., Laurent Vercueil, M.D., Jean-Luc Houeto, M.D., Ph.D., Pierre Krystkowiak, M.D., Alim-Louis Benabid, M.D., Ph.D., Philippe Cornu, M.D.,
Christelle Lagrange, Ph.D., Sophie Tézenas du Montcel, M.D., Ph.D., Didier Dormont, M.D., Ph.D., Sylvie Grand, M.D., Ph.D., Serge Blond, M.D.,
Olivier Detante, M.D., Bernard Pillon, Ph.D., Claire Ardouin, Ph.D., Yves Agid, M.D., Ph.D., Alain Destée, M.D., and Pierre Pollak, M.D., Ph.D., for the French Stimulation du Pallidum Interne dans la Dystonie (SPIDY) Study Group*
From the Department of Neurology, SaintAntoine Hospital, Paris (M.V.); INSERMUnité 289 (M.V.), the Department of Neu-rosurgery (P.C.), the Department of Neu-roradiology and UPR 640, Centre Nationalde la Recherche Scientifique Laboratoirede Neurosciences Cognitives et ImagerieCerebrale (D.D.), INSERM E007 and the De-partment of Neurology (B.P.), and the De-partment of Neurology, Centre d’Investi-gation Clinique, and INSERM Unité 289(Y.A.), Pitié–Salpêtrière Hospital, Paris; theDepartment of Biological and Clinical Neu-rosciences (L.V., A.-L.B., C.L., O.D., C.A.,P.P.) and the Magnetic Resonance Imag-ing Unit, Department of Neuroradiology(S.G.), Grenoble University Hospital, andINSERM Unité 318, Joseph Fourier Univer-sity (L.V., A.-L.B., P.P.), Grenoble; the De-partment of Neurology, University Hospi-tal, Poitiers (J.-L.H.); the Neurology andMovement Disorders Unit (P.K., A.D.) andthe Department of Neurosurgery (S.B.), LilleUniversity Hospital, Lille; Equipe Associée2683, University of Lille, Lille (P.K., A.D.);and the Department of Biostatistics, Univer-sity Hospital Pitié–Salpêtrière and INSERMUnité 535, Paul Brousse Hospital, Villejuif(S.T.M.) — all in France. Address reprintrequests to Dr. Vidailhet at the Depart-ment of Neurology, Saint Antoine Hospital,184 Faubourg Saint Antoine, 75571, ParisCEDEX 12, France, or at [email protected].
*Members of the French SPIDY StudyGroup are listed in the Appendix.
N Engl J Med 2005;352:459-67.
Copyright © 2005 Massachusetts Medical Society.
background
Severe forms of dystonia respond poorly to medical treatment. Deep-brain stimulationis a reversible neurosurgical procedure that has been used for the treatment of dysto-nia, but assessment of its efficacy has been limited to open studies.
methods
We performed a prospective, controlled, multicenter study assessing the efficacy andsafety of bilateral pallidal stimulation in 22 patients with primary generalized dysto-nia. The severity of dystonia was evaluated before surgery and 3, 6, and 12 months post-operatively during neurostimulation, with the use of the movement and disabilitysubscores of the Burke–Fahn–Marsden Dystonia Scale (range, 0 to 120 and 0 to 30,respectively, with higher scores indicating greater impairment). Movement scoreswere assessed by a review of videotaped sessions performed by an observer who wasunaware of treatment status. At three months, patients underwent a double-blind evalu-ation in the presence and absence of neurostimulation. We also assessed the patients’quality of life, cognition, and mood at baseline and 12 months.
results
The dystonia movement score improved from a mean (±SD) of 46.3±21.3 before sur-gery to 21.0±14.1 at 12 months (P<0.001). The disability score improved from 11.6±5.5before surgery to 6.5±4.9 at 12 months (P<0.001). General health and physical func-tioning were significantly improved at month 12; there were no significant changes inmeasures of mood and cognition. At the three-month evaluation, dystonia movementscores were significantly better with neurostimulation than without neurostimulation(24.6±17.7 vs. 34.6±12.3, P<0.001). There were five adverse events (in three patients);all resolved without permanent sequelae.
conclusions
These findings support the efficacy and safety of the use of bilateral stimulation of theinternal globus pallidus in selected patients with primary generalized dystonia.
abstract
The New England Journal of Medicine Downloaded from nejm.org at YASER UNIVERSITY OF CALGARY on January 14, 2011. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
n engl j med
352;5
www.nejm.org february
3, 2005
The
new england journal
of
medicine
459
original article
Bilateral Deep-Brain Stimulation of the Globus Pallidus in Primary Generalized Dystonia
Marie Vidailhet, M.D., Ph.D., Laurent Vercueil, M.D., Jean-Luc Houeto, M.D., Ph.D., Pierre Krystkowiak, M.D., Alim-Louis Benabid, M.D., Ph.D., Philippe Cornu, M.D.,
Christelle Lagrange, Ph.D., Sophie Tézenas du Montcel, M.D., Ph.D., Didier Dormont, M.D., Ph.D., Sylvie Grand, M.D., Ph.D., Serge Blond, M.D.,
Olivier Detante, M.D., Bernard Pillon, Ph.D., Claire Ardouin, Ph.D., Yves Agid, M.D., Ph.D., Alain Destée, M.D., and Pierre Pollak, M.D., Ph.D., for the French Stimulation du Pallidum Interne dans la Dystonie (SPIDY) Study Group*
From the Department of Neurology, SaintAntoine Hospital, Paris (M.V.); INSERMUnité 289 (M.V.), the Department of Neu-rosurgery (P.C.), the Department of Neu-roradiology and UPR 640, Centre Nationalde la Recherche Scientifique Laboratoirede Neurosciences Cognitives et ImagerieCerebrale (D.D.), INSERM E007 and the De-partment of Neurology (B.P.), and the De-partment of Neurology, Centre d’Investi-gation Clinique, and INSERM Unité 289(Y.A.), Pitié–Salpêtrière Hospital, Paris; theDepartment of Biological and Clinical Neu-rosciences (L.V., A.-L.B., C.L., O.D., C.A.,P.P.) and the Magnetic Resonance Imag-ing Unit, Department of Neuroradiology(S.G.), Grenoble University Hospital, andINSERM Unité 318, Joseph Fourier Univer-sity (L.V., A.-L.B., P.P.), Grenoble; the De-partment of Neurology, University Hospi-tal, Poitiers (J.-L.H.); the Neurology andMovement Disorders Unit (P.K., A.D.) andthe Department of Neurosurgery (S.B.), LilleUniversity Hospital, Lille; Equipe Associée2683, University of Lille, Lille (P.K., A.D.);and the Department of Biostatistics, Univer-sity Hospital Pitié–Salpêtrière and INSERMUnité 535, Paul Brousse Hospital, Villejuif(S.T.M.) — all in France. Address reprintrequests to Dr. Vidailhet at the Depart-ment of Neurology, Saint Antoine Hospital,184 Faubourg Saint Antoine, 75571, ParisCEDEX 12, France, or at [email protected].
*Members of the French SPIDY StudyGroup are listed in the Appendix.
N Engl J Med 2005;352:459-67.
Copyright © 2005 Massachusetts Medical Society.
background
Severe forms of dystonia respond poorly to medical treatment. Deep-brain stimulationis a reversible neurosurgical procedure that has been used for the treatment of dysto-nia, but assessment of its efficacy has been limited to open studies.
methods
We performed a prospective, controlled, multicenter study assessing the efficacy andsafety of bilateral pallidal stimulation in 22 patients with primary generalized dysto-nia. The severity of dystonia was evaluated before surgery and 3, 6, and 12 months post-operatively during neurostimulation, with the use of the movement and disabilitysubscores of the Burke–Fahn–Marsden Dystonia Scale (range, 0 to 120 and 0 to 30,respectively, with higher scores indicating greater impairment). Movement scoreswere assessed by a review of videotaped sessions performed by an observer who wasunaware of treatment status. At three months, patients underwent a double-blind evalu-ation in the presence and absence of neurostimulation. We also assessed the patients’quality of life, cognition, and mood at baseline and 12 months.
results
The dystonia movement score improved from a mean (±SD) of 46.3±21.3 before sur-gery to 21.0±14.1 at 12 months (P<0.001). The disability score improved from 11.6±5.5before surgery to 6.5±4.9 at 12 months (P<0.001). General health and physical func-tioning were significantly improved at month 12; there were no significant changes inmeasures of mood and cognition. At the three-month evaluation, dystonia movementscores were significantly better with neurostimulation than without neurostimulation(24.6±17.7 vs. 34.6±12.3, P<0.001). There were five adverse events (in three patients);all resolved without permanent sequelae.
conclusions
These findings support the efficacy and safety of the use of bilateral stimulation of theinternal globus pallidus in selected patients with primary generalized dystonia.
abstract
The New England Journal of Medicine Downloaded from nejm.org at YASER UNIVERSITY OF CALGARY on January 14, 2011. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
original article
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 355;19 www.nejm.org november 9, 20061978
Pallidal Deep-Brain Stimulation in Primary Generalized or Segmental DystoniaAndreas Kupsch, M.D., Reiner Benecke, M.D., Jörg Müller, M.D.,
Thomas Trottenberg, M.D., Gerd-Helge Schneider, M.D., Werner Poewe, M.D., Wilhelm Eisner, M.D., Alexander Wolters, M.D., Jan-Uwe Müller, M.D.,
Günther Deuschl, M.D., Marcus O. Pinsker, M.D., Inger Marie Skogseid, M.D., Geir Ketil Roeste, M.D., Juliane Vollmer-Haase, M.D., Angela Brentrup, M.D.,
Martin Krause, M.D., Volker Tronnier, M.D., Alfons Schnitzler, M.D., Jürgen Voges, M.D., Guido Nikkhah, M.D., Ph.D., Jan Vesper, M.D.,
Markus Naumann, M.D., and Jens Volkmann, M.D., for the Deep-Brain Stimulation for Dystonia Study Group*
From Charité Universitätsmedizin Berlin, Campus Virchow, Berlin (A.K., T.T., G.-H.S.); University of Rostock, Rostock (R.B., A.W.); Ernst Moritz Arndt University, Greifswald ( J.-U.M.); Christian Al brechts University, Kiel (G.D., M.O.P., J. Volkmann); Univer-sity of Münster, Münster ( J.V.-H., A.B.); University of Heidelberg, Heidelberg (M.K., V.T.); Heinrich Heine University, Düsseldorf (A.S.); University of Cologne, Cologne ( J. Voges); University of Freiburg, Freiburg (G.N., J. Vesper); and University of Würzburg, Würzburg (M.N.) — all in Germany; Medical University Innsbruck, Innsbruck, Austria ( J.M., W.P., W.E.); and University of Oslo, Oslo (I.M.S., G.K.R.). Address reprint requests to Dr. Volkmann at the Department of Neurology, Chris-tian Albrechts University, Schittenhelm-str. 10, D-24105 Kiel, Germany, or at [email protected].
* The members of the Deep-Brain Stimu-lation for Dystonia Study Group are listed in the Appendix.
N Engl J Med 2006;355:1978-90.Copyright © 2006 Massachusetts Medical Society.
A bs tr ac t
BackgroundNeurostimulation of the internal globus pallidus has been shown to be effective in reducing symptoms of primary dystonia. We compared this surgical treatment with sham stimulation in a randomized, controlled clinical trial.MethodsForty patients with primary segmental or generalized dystonia received an im-planted device for deep-brain stimulation and were randomly assigned to receive either neurostimulation or sham stimulation for 3 months. The primary end point was the change from baseline to 3 months in the severity of symptoms, according to the movement subscore on the Burke–Fahn–Marsden Dystonia Rating Scale (range, 0 to 120, with higher scores indicating greater impairment). Two investiga-tors who were unaware of treatment status assessed the severity of dystonia by re-viewing videotaped sessions. Subsequently, all patients received open-label neuro-stimulation; blinded assessment was repeated after 6 months of active treatment.ResultsThree months after randomization, the change from baseline in the mean (±SD) move-ment score was significantly greater in the neurostimulation group (−15.8±14.1 points) than in the sham-stimulation group (−1.4±3.8 points, P<0.001). During the open-label extension period, this improvement was sustained among patients orig-inally assigned to the neurostimulation group, and patients in the sham-stimulation group had a similar benefit when they switched to active treatment. The combined analysis of the entire cohort after 6 months of neurostimulation revealed substantial improvement in all movement symptoms (except speech and swallowing), the level of disability, and quality of life, as compared with baseline scores. A total of 22 adverse events occurred in 19 patients, including 4 infections at the stimulator site and 1 lead dislodgment. The most frequent adverse event was dysarthria.ConclusionsBilateral pallidal neurostimulation for 3 months was more effective than sham stimu-lation in patients with primary generalized or segmental dystonia. (ClinicalTrials.gov number, NCT00142259.)
Copyright © 2006 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at UNIVERSITY OF BRITISH COLUMBIA on December 15, 2008 .
original article
T h e n e w e ng l a nd j o u r na l o f m e dic i n e
n engl j med 355;19 www.nejm.org november 9, 20061978
Pallidal Deep-Brain Stimulation in Primary Generalized or Segmental DystoniaAndreas Kupsch, M.D., Reiner Benecke, M.D., Jörg Müller, M.D.,
Thomas Trottenberg, M.D., Gerd-Helge Schneider, M.D., Werner Poewe, M.D., Wilhelm Eisner, M.D., Alexander Wolters, M.D., Jan-Uwe Müller, M.D.,
Günther Deuschl, M.D., Marcus O. Pinsker, M.D., Inger Marie Skogseid, M.D., Geir Ketil Roeste, M.D., Juliane Vollmer-Haase, M.D., Angela Brentrup, M.D.,
Martin Krause, M.D., Volker Tronnier, M.D., Alfons Schnitzler, M.D., Jürgen Voges, M.D., Guido Nikkhah, M.D., Ph.D., Jan Vesper, M.D.,
Markus Naumann, M.D., and Jens Volkmann, M.D., for the Deep-Brain Stimulation for Dystonia Study Group*
From Charité Universitätsmedizin Berlin, Campus Virchow, Berlin (A.K., T.T., G.-H.S.); University of Rostock, Rostock (R.B., A.W.); Ernst Moritz Arndt University, Greifswald ( J.-U.M.); Christian Al brechts University, Kiel (G.D., M.O.P., J. Volkmann); Univer-sity of Münster, Münster ( J.V.-H., A.B.); University of Heidelberg, Heidelberg (M.K., V.T.); Heinrich Heine University, Düsseldorf (A.S.); University of Cologne, Cologne ( J. Voges); University of Freiburg, Freiburg (G.N., J. Vesper); and University of Würzburg, Würzburg (M.N.) — all in Germany; Medical University Innsbruck, Innsbruck, Austria ( J.M., W.P., W.E.); and University of Oslo, Oslo (I.M.S., G.K.R.). Address reprint requests to Dr. Volkmann at the Department of Neurology, Chris-tian Albrechts University, Schittenhelm-str. 10, D-24105 Kiel, Germany, or at [email protected].
* The members of the Deep-Brain Stimu-lation for Dystonia Study Group are listed in the Appendix.
N Engl J Med 2006;355:1978-90.Copyright © 2006 Massachusetts Medical Society.
A bs tr ac t
BackgroundNeurostimulation of the internal globus pallidus has been shown to be effective in reducing symptoms of primary dystonia. We compared this surgical treatment with sham stimulation in a randomized, controlled clinical trial.MethodsForty patients with primary segmental or generalized dystonia received an im-planted device for deep-brain stimulation and were randomly assigned to receive either neurostimulation or sham stimulation for 3 months. The primary end point was the change from baseline to 3 months in the severity of symptoms, according to the movement subscore on the Burke–Fahn–Marsden Dystonia Rating Scale (range, 0 to 120, with higher scores indicating greater impairment). Two investiga-tors who were unaware of treatment status assessed the severity of dystonia by re-viewing videotaped sessions. Subsequently, all patients received open-label neuro-stimulation; blinded assessment was repeated after 6 months of active treatment.ResultsThree months after randomization, the change from baseline in the mean (±SD) move-ment score was significantly greater in the neurostimulation group (−15.8±14.1 points) than in the sham-stimulation group (−1.4±3.8 points, P<0.001). During the open-label extension period, this improvement was sustained among patients orig-inally assigned to the neurostimulation group, and patients in the sham-stimulation group had a similar benefit when they switched to active treatment. The combined analysis of the entire cohort after 6 months of neurostimulation revealed substantial improvement in all movement symptoms (except speech and swallowing), the level of disability, and quality of life, as compared with baseline scores. A total of 22 adverse events occurred in 19 patients, including 4 infections at the stimulator site and 1 lead dislodgment. The most frequent adverse event was dysarthria.ConclusionsBilateral pallidal neurostimulation for 3 months was more effective than sham stimu-lation in patients with primary generalized or segmental dystonia. (ClinicalTrials.gov number, NCT00142259.)
Copyright © 2006 Massachusetts Medical Society. All rights reserved. Downloaded from www.nejm.org at UNIVERSITY OF BRITISH COLUMBIA on December 15, 2008 .
• 3 month randomized, double-‐blind, sham-‐controlled trial, followed by 3 or 6 months of open-‐label treatment, for a total of 6 months of sDmulaDon in 40 paDents.
• Outcome measures: Burke-‐Fahn-‐Marsden scale, SF-‐36, Beck Depression Inventory
• StaDsDcally greater improvements in all outcome measures at 3 months in the sDmulaDon group.
• Improvement sustained during the open-‐label extension, and paDents in the sham group had similar improvements.
• No changes in cogniDve status.• Conclusion: Bilateral DBS of GPi is effec've in reduc'on of movement
impairment and disability in pa'ents with primary generalized or segmental dystonia.
Outcomes: Essential Tremor
• Randomized, controlled trial of thalamotomy vs thalamic sDmulaDon.• 68 paDents with tremor (Parkinson’s, essenDal tremor, mulDple sclerosis).• Primary outcome measure: funcDonal outcome at six-‐month follow-‐up.• FuncDonal outcome improved in sDmulaDon group vs. thalamotomy group• PaDents with tremor due to essenDal tremor fared befer than paDents with tremor due to other diagnoses.
• Conclusion: Thalamic s'mula'on has fewer adverse effects and results in a greater improvement in func'on than thalamotomy in the treatment of tremor.
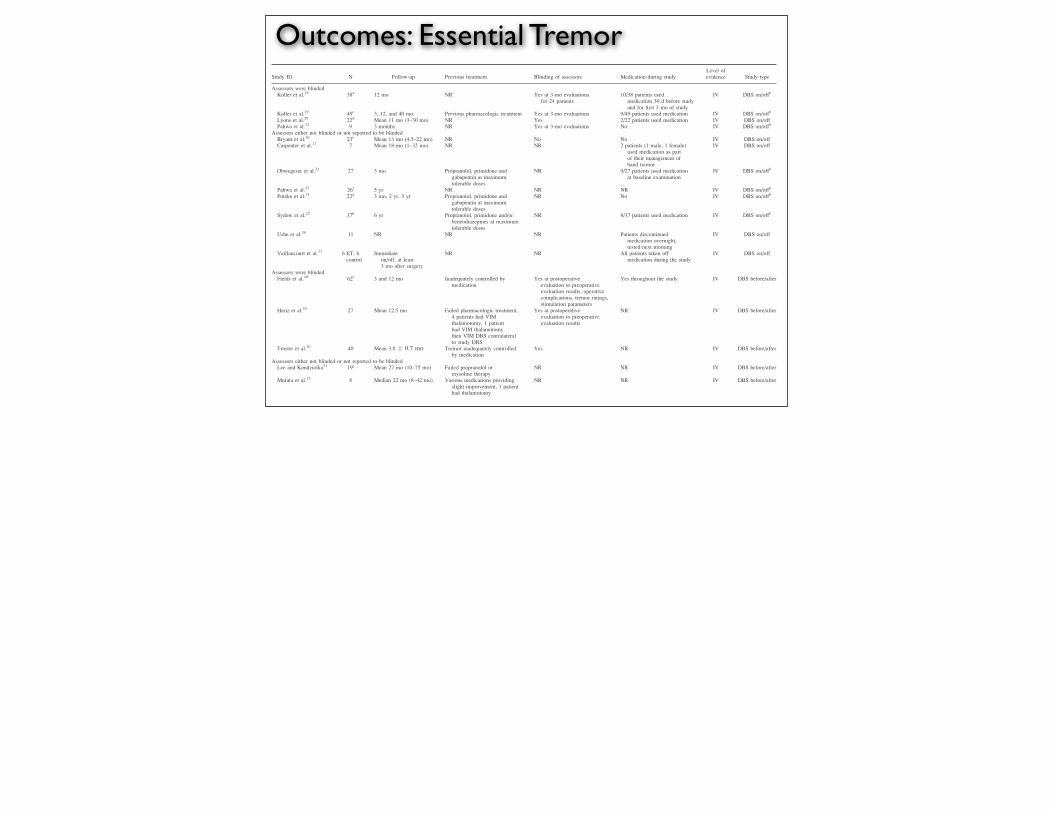
Outcomes: Essential TremorTABLE 3. Included studies
Study ID N Follow-up Previous treatment Blinding of assessors Medication during studyLevel ofevidence Study type
Assessors were blindedKoller et al.18 38a 12 mo NR Yes at 3-mo evaluations
for 24 patients10/38 patients used
medication 30 d before studyand for first 3 mo of study
IV DBS on/offb
Koller et al.19 49c 3, 12, and 40 mo Previous pharmacologic treatment Yes at 3-mo evaluations 9/49 patients used medication IV DBS on/offb
Lyons et al.20 22d Mean 11 mo (3–30 mo) NR Yes 2/22 patients used medication IV DBS on/offPahwa et al.22 9 3 months NR Yes at 3-mo evaluations No IV DBS on/offb
Assessors either not blinded or not reported to be blindedBryant et al.16 23e Mean 13 mo (4.5–22 mo) NR No No IV DBS on/offCarpenter et al.17 7 Mean 18 mo (1–32 mo) NR NR 2 patients (1 male, 1 female)
used medication as partof their management ofhand tremor
IV DBS on/off
Obwegeser et al.21 27 3 mo Propranolol, primidone andgabapentin at maximumtolerable doses
NR 9/27 patients used medicationat baseline examination
IV DBS on/offb
Pahwa et al.23 26f 5 yr NR NR NR IV DBS on/offb
Putzke et al.24 22g 3 mo, 2 yr, 3 yr Propranolol, primidone andgabapentin at maximumtolerable doses
NR No IV DBS on/offb
Sydow et al.25 37h 6 yr Propranolol, primidone and/orbenzodiazepines at maximumtolerable doses
NR 8/37 patients used medication IV DBS on/offb
Ushe et al.26 11 NR NR NR Patients discontinuedmedication overnight,tested next morning
IV DBS on/off
Vaillancourt et al.27 6 ET, 6control
Immediateon/off, at least3 mo after surgery
NR NR All patients taken offmedication during the study
IV DBS on/off
Assessors were blindedFields et al.28 62i 3 and 12 mo Inadequately controlled by
medicationYes at postoperative
evaluation to preoperativeevaluation results, operativecomplications, tremor ratings,stimulation parameters
Yes throughout the study IV DBS before/after
Hariz et al.29 27 Mean 12.5 mo Failed pharmacologic treatment,4 patients had VIMthalamotomy, 1 patienthad VIM thalamotomythen VIM DBS contralateralto study DBS
Yes at postoperativeevaluation to preoperativeevaluation results
NR IV DBS before/after
Troster et al.30 40 Mean 3.0 6 0.7 mo Tremor inadequately controlledby medication
Yes NR IV DBS before/after
Assessors either not blinded or not reported to be blindedLee and Kondziolka31 19j Mean 27 mo (10–75 mo) Failed propranolol or
mysoline therapyNR NR IV DBS before/after
Murata et al.32 8 Median 22 mo (8–42 mo) Various medications providingslight improvement, 1 patienthad thalamotomy
NR NR IV DBS before/after
aOriginally 38 patients at baseline, 22 at 6-mo follow-up, and 20 at 12-mo follow-up.bReported a presurgical baseline.cOriginally 49 patients at baseline, only 25 patients were evaluated with follow-up ‡2 yr.dOriginally 22 patients at baseline, 2 refused to switch stimulation to off.eOriginally 23 patients at baseline, only 16 completed the study.fOriginally 26 patients, only 23 patients remaining at 5 yr.gOriginally 22 patients, 18 at follow-up.hOriginally 37 patients at baseline, 18 lost to follow-up.iOriginally 62 patients, only 40 at 1-yr follow-up.jOriginally 19 patients, 18 at follow-up.
DBS, deep brain stimulation; NR, not reported; VIM, ventralis intermedius.
1553DEEPBRAIN
STIM
ULATIO
NFORESSE
NTIALTREMORMovem
entDisorders,
Vol.
25,No.
11,2010
Outcomes: Essential Tremor
• No randomized-controlled trials evaluating DBS soley for essential tremor.
• Based on a review of Level IV publications, DBS is safe and effective for treatment of essential tremor:
• Statistically significant improvements noted in all studies (on/off and pre/post studies) in tremor rating scores
• Bilateral stimulation more effective than unilateral stimulation
Deep Brain Stimulation for Essential Tremor:A Systematic Review
Eliana Della Flora, BMedPharmBiotech (Hons), GCPH,1
Caryn L. Perera, BA (Lib Info Mgt), Grad Cert EBP,1 Alun L. Cameron, BSc (Hons), PhD,1
and Guy J. Maddern, FRACS, PhD1,2,3*
1Australian Safety and Efficacy Register of New Interventional Procedures-Surgical (ASERNIP-S),Royal Australasian College of Surgeons, Stepney, South Australia, Australia
2Discipline of Surgery, University of Adelaide, Adelaide, South Australia, Australia3Department of Surgery, The Queen Elizabeth Hospital, Woodville, South Australia, Australia
Abstract: Deep brain stimulation (DBS) is a neurosurgicaltreatment, which has proven useful in treating Parkinson’sdisease. This systematic review assessed the safety and effec-tiveness of DBS for another movement disorder, essentialtremor. All studies concerning the use of DBS in patientswith essential tremor were identified through searching ofelectronic databases and hand searching of reference lists.Studies were categorized as before/after DBS or DBS stimu-lation on/off to allow the effect of the stimulation to be ana-lyzed separately to that of the surgery itself. A total of 430patients who had received DBS for essential tremor were
identified. Most of the reported adverse events were mild andcould be treated through changing the stimulation settings.Generally, in all studies, there was a significant improvementin outcomes after DBS compared with baseline scores. Inaddition, DBS was significantly better in testing when thestimulation was turned on, compared with stimulation turnedoff or baseline. Based on Level IV evidence, DBS is possiblya safe and effective therapy for essential tremor. ! 2010Movement Disorder SocietyKey words: deep brain stimulation; essential tremor; sys-
tematic review
Essential tremor (ICD-10 G25.0) is one of the mostcommon neurological disorders.1 A key feature of thisdisorder is kinetic tremor of the arms during voluntarymovement, which in severe cases can spread to otherbody parts or occur at rest.1,2 Patients may have signif-icant physical impairment and a markedly decreasedquality of life.
Among the general population, the prevalence ofessential tremor has been conservatively estimated atbetween 0.4% and 5%, although it is expected that thetrue prevalence is much higher due to the absence of uni-form methodology by which to diagnose the disorder.3–5
Existing Procedures
To date, no curative treatment exists for essentialtremor. Management of the disorder is focused on con-trolling the symptoms, with pharmacotherapy as theprimary therapy. However, it is estimated that between25% and 55% of patients will have medication-refrac-tory essential tremor.6 For these patients, surgicaloptions include stereotactic radiofrequency thalamot-omy, gamma knife thalamotomy, or deep brain stimu-lation (DBS).2,4,7 Thalamotomy is rarely conducted inAustralia because of its association with increasedmorbidity and mortality.8,9 This procedure is effectivein 73% to 93% of patients with medication-refractory
Guy J. Maddern, as corresponding author, had full access to all thedata in the study and had final responsibility for the decision to sub-mit for publication.
*Correspondence to: Guy J. Maddern, Australian Safety and Effi-cacy Register of New Interventional Procedures-Surgical (ASERNIP-S), Royal Australasian College of Surgeons, PO Box 553, Stepney,South Australia, 5069, Australia.E-mail: [email protected]
Potential conflict of interest: The authors report no conflicts of in-terest. The authors have no financial disclosures to make.
Received 28 September 2009; Revised 18 January 2010; Accepted22 March 2010
Published online 9 July 2010 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.23195
1550
Movement DisordersVol. 25, No. 11, 2010, pp. 1550–1559! 2010 Movement Disorder Society
Deep Brain Stimulation for Essential Tremor:A Systematic Review
Eliana Della Flora, BMedPharmBiotech (Hons), GCPH,1
Caryn L. Perera, BA (Lib Info Mgt), Grad Cert EBP,1 Alun L. Cameron, BSc (Hons), PhD,1
and Guy J. Maddern, FRACS, PhD1,2,3*
1Australian Safety and Efficacy Register of New Interventional Procedures-Surgical (ASERNIP-S),Royal Australasian College of Surgeons, Stepney, South Australia, Australia
2Discipline of Surgery, University of Adelaide, Adelaide, South Australia, Australia3Department of Surgery, The Queen Elizabeth Hospital, Woodville, South Australia, Australia
Abstract: Deep brain stimulation (DBS) is a neurosurgicaltreatment, which has proven useful in treating Parkinson’sdisease. This systematic review assessed the safety and effec-tiveness of DBS for another movement disorder, essentialtremor. All studies concerning the use of DBS in patientswith essential tremor were identified through searching ofelectronic databases and hand searching of reference lists.Studies were categorized as before/after DBS or DBS stimu-lation on/off to allow the effect of the stimulation to be ana-lyzed separately to that of the surgery itself. A total of 430patients who had received DBS for essential tremor were
identified. Most of the reported adverse events were mild andcould be treated through changing the stimulation settings.Generally, in all studies, there was a significant improvementin outcomes after DBS compared with baseline scores. Inaddition, DBS was significantly better in testing when thestimulation was turned on, compared with stimulation turnedoff or baseline. Based on Level IV evidence, DBS is possiblya safe and effective therapy for essential tremor. ! 2010Movement Disorder SocietyKey words: deep brain stimulation; essential tremor; sys-
tematic review
Essential tremor (ICD-10 G25.0) is one of the mostcommon neurological disorders.1 A key feature of thisdisorder is kinetic tremor of the arms during voluntarymovement, which in severe cases can spread to otherbody parts or occur at rest.1,2 Patients may have signif-icant physical impairment and a markedly decreasedquality of life.
Among the general population, the prevalence ofessential tremor has been conservatively estimated atbetween 0.4% and 5%, although it is expected that thetrue prevalence is much higher due to the absence of uni-form methodology by which to diagnose the disorder.3–5
Existing Procedures
To date, no curative treatment exists for essentialtremor. Management of the disorder is focused on con-trolling the symptoms, with pharmacotherapy as theprimary therapy. However, it is estimated that between25% and 55% of patients will have medication-refrac-tory essential tremor.6 For these patients, surgicaloptions include stereotactic radiofrequency thalamot-omy, gamma knife thalamotomy, or deep brain stimu-lation (DBS).2,4,7 Thalamotomy is rarely conducted inAustralia because of its association with increasedmorbidity and mortality.8,9 This procedure is effectivein 73% to 93% of patients with medication-refractory
Guy J. Maddern, as corresponding author, had full access to all thedata in the study and had final responsibility for the decision to sub-mit for publication.
*Correspondence to: Guy J. Maddern, Australian Safety and Effi-cacy Register of New Interventional Procedures-Surgical (ASERNIP-S), Royal Australasian College of Surgeons, PO Box 553, Stepney,South Australia, 5069, Australia.E-mail: [email protected]
Potential conflict of interest: The authors report no conflicts of in-terest. The authors have no financial disclosures to make.
Received 28 September 2009; Revised 18 January 2010; Accepted22 March 2010
Published online 9 July 2010 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/mds.23195
1550
Movement DisordersVol. 25, No. 11, 2010, pp. 1550–1559! 2010 Movement Disorder Society
Future Direction: Therapeutic Growth Factors
• GDNF reported to protect dopaminergic neurons from a variety of toxic insults in cell culture and rodent and primate models.10
•Gill. 2003. Intraputamenal injection of GDNF.11
•Slevin. 2006. Continuous GDNF infusion for one year.12
• International, multicenter, randomized placebo-controlled trial
• Sponsored by Amgen and Medtronic
• Abandoned after the sponsors reviewed safety and efficacy profile, which showed some patients developed anti-GDNF antibodies and some monkeys developed cerebellar lesions attributed to therapy
• Results at this point in the study did not show significant differences between the placebo and treatment groups with respect to the primary outcome measures.
Randomized Controlled Trial ofIntraputamenal Glial Cell Line–Derived
Neurotrophic Factor Infusionin Parkinson Disease
Anthony E. Lang, MD,1 Steven Gill, MD,2 Nik K. Patel, MD,2 Andres Lozano, MD,3 John G. Nutt, MD,4
Richard Penn, MD,5 David J. Brooks, MD,6 Gary Hotton, MD,6 Elena Moro, MD,1 Peter Heywood, MD,1
Matthew A. Brodsky, MD,4 Kim Burchiel, MD,4 Patrick Kelly, MD,7 Arif Dalvi, MD,5 Burton Scott, MD,8
Mark Stacy, MD,9 Dennis Turner, MD,9 V. G. Frederich Wooten, MD,10 William J. Elias, MD,10
Edward R. Laws, MD,10 Vijay Dhawan, PhD,11 A. Jon Stoessl, MD12 James Matcham,13
Robert J. Coffey, MD14 and Michael Traub, MD15
Objective: Glial cell line–derived neurotrophic factor (GDNF) exerts potent trophic influence on midbrain dopaminergicneurons. This randomized controlled clinical trial was designed to confirm initial clinical benefits observed in a small,open-label trial using intraputamenal (Ipu) infusion of recombinant human GDNF (liatermin). Methods:Thirty-four PDpatients were randomized 1 to 1 to receive bilateral continuous Ipu infusion of liatermin 15!g/putamen/day or placebo.The primary end point was the change in Unified Parkinson Disease Rating Scale (UPDRS) motor score in the practi-cally defined off condition at 6 months. Secondary end points included other UPDRS scores, motor tests, dyskinesiaratings, patient diaries, and 18F-dopa uptake. Results: At 6 months, mean percentage changes in “off” UPDRS motorscore were "10.0% and "4.5% in the liatermin and placebo groups, respectively. This treatment difference was notsignificant (95% confidence interval, "23.0 to 12.0, p # 0.53). Secondary end point results were similar between thegroups. A 32.5% treatment difference favoring liatermin in mean 18F-dopa influx constant (p # 0.019) was observed.Serious, device-related adverse events required surgical repositioning of catheters in two patients and removal of devicesin another. Neutralizing antiliatermin antibodies were detected in three patients (one on-study and two in the open-labelextension). Interpretation: Liatermin did not confer the predetermined level of clinical benefit to patients with PDdespite increased 18F-dopa uptake. It is uncertain whether technical differences between this trial and positive open-labelstudies contributed in any way this negative outcome.
Ann Neurol 2006;59:459–466
Current medical therapy for Parkinson’s disease (PD)involves dopaminergic replacement, which results insubstantial improvement, although long-term treat-ment is typically complicated by motor response fluc-tuations and dyskinetic movements. No currently avail-able treatment alters the progressive neurodegenerativecourse of PD.
Glial cell line–derived neurotrophic factor (GDNF),a member of the transforming growth factor-! super-
family, has potent neurotrophic effects particularly butnot exclusively on dopaminergic neurons.1 The humanGDNF gene has been cloned, and recombinant me-thionyl human GDNF (r-metHuGDNF, Liatermin;Amgen, Thousand Oaks, CA), a 30kDa disulfide-bonded homodimer displaying biological activity, hasbeen produced in Escherichia coli. GDNF has bothneuroprotective and neuroregenerative effects in rodentand nonhuman primate toxic models of PD, especially
From the 1Toronto Western Hospital and the University of Toronto,Toronto, Ontario, Canada; 2Frenchay Hospital, Bristol, United King-dom; 3Toronto Western Research Institute, Toronto, Canada; 4Ore-gon Health and Science University, Parkinson Center of Oregon,Portland, OR; 5University of Chicago, Chicago, IL; 6Imperial Col-lege, Hammersmith Hospital, London, United Kingdom; 7New YorkUniversity Medical Center, New York, NY; 8Duke Movement Dis-orders Clinic; 9Duke University, Durham, NC; 10University of Vir-ginia, Charlottesville, VA; 11North Shore Long Island Jewish ResearchInstitute, Manhasset, NY; 12University of British Columbia, Vancou-ver, British Columbia, Canada; 13Amgen Ltd., Cambridge, UnitedKingdom;
14Medtronic Inc., Minneapolis, MN; and 15Amgen Inc.,
Thousand Oaks, CA.
Received Aug 1, 2005, and in revised form Oct 3. Accepted forpublication Oct 6, 2005.
Published online Jan 20, 2006 in Wiley InterScience(www.interscience.wiley.com). DOI: 10.1002/ana.20737
Address correspondence to Dr Lang, Department of Medicine(Neurology), University of Toronto, Toronto Western HospitalMovement Disorders Center, 399 Bathurst Street, 7McL, Toronto,ON, Canada M5T 2S8. E-mail: [email protected]
ORIGINAL ARTICLES
© 2006 American Neurological Association 459Published by Wiley-Liss, Inc., through Wiley Subscription Services
Randomized Controlled Trial ofIntraputamenal Glial Cell Line–Derived
Neurotrophic Factor Infusionin Parkinson Disease
Anthony E. Lang, MD,1 Steven Gill, MD,2 Nik K. Patel, MD,2 Andres Lozano, MD,3 John G. Nutt, MD,4
Richard Penn, MD,5 David J. Brooks, MD,6 Gary Hotton, MD,6 Elena Moro, MD,1 Peter Heywood, MD,1
Matthew A. Brodsky, MD,4 Kim Burchiel, MD,4 Patrick Kelly, MD,7 Arif Dalvi, MD,5 Burton Scott, MD,8
Mark Stacy, MD,9 Dennis Turner, MD,9 V. G. Frederich Wooten, MD,10 William J. Elias, MD,10
Edward R. Laws, MD,10 Vijay Dhawan, PhD,11 A. Jon Stoessl, MD12 James Matcham,13
Robert J. Coffey, MD14 and Michael Traub, MD15
Objective: Glial cell line–derived neurotrophic factor (GDNF) exerts potent trophic influence on midbrain dopaminergicneurons. This randomized controlled clinical trial was designed to confirm initial clinical benefits observed in a small,open-label trial using intraputamenal (Ipu) infusion of recombinant human GDNF (liatermin). Methods:Thirty-four PDpatients were randomized 1 to 1 to receive bilateral continuous Ipu infusion of liatermin 15!g/putamen/day or placebo.The primary end point was the change in Unified Parkinson Disease Rating Scale (UPDRS) motor score in the practi-cally defined off condition at 6 months. Secondary end points included other UPDRS scores, motor tests, dyskinesiaratings, patient diaries, and 18F-dopa uptake. Results: At 6 months, mean percentage changes in “off” UPDRS motorscore were "10.0% and "4.5% in the liatermin and placebo groups, respectively. This treatment difference was notsignificant (95% confidence interval, "23.0 to 12.0, p # 0.53). Secondary end point results were similar between thegroups. A 32.5% treatment difference favoring liatermin in mean 18F-dopa influx constant (p # 0.019) was observed.Serious, device-related adverse events required surgical repositioning of catheters in two patients and removal of devicesin another. Neutralizing antiliatermin antibodies were detected in three patients (one on-study and two in the open-labelextension). Interpretation: Liatermin did not confer the predetermined level of clinical benefit to patients with PDdespite increased 18F-dopa uptake. It is uncertain whether technical differences between this trial and positive open-labelstudies contributed in any way this negative outcome.
Ann Neurol 2006;59:459–466
Current medical therapy for Parkinson’s disease (PD)involves dopaminergic replacement, which results insubstantial improvement, although long-term treat-ment is typically complicated by motor response fluc-tuations and dyskinetic movements. No currently avail-able treatment alters the progressive neurodegenerativecourse of PD.
Glial cell line–derived neurotrophic factor (GDNF),a member of the transforming growth factor-! super-
family, has potent neurotrophic effects particularly butnot exclusively on dopaminergic neurons.1 The humanGDNF gene has been cloned, and recombinant me-thionyl human GDNF (r-metHuGDNF, Liatermin;Amgen, Thousand Oaks, CA), a 30kDa disulfide-bonded homodimer displaying biological activity, hasbeen produced in Escherichia coli. GDNF has bothneuroprotective and neuroregenerative effects in rodentand nonhuman primate toxic models of PD, especially
From the 1Toronto Western Hospital and the University of Toronto,Toronto, Ontario, Canada; 2Frenchay Hospital, Bristol, United King-dom; 3Toronto Western Research Institute, Toronto, Canada; 4Ore-gon Health and Science University, Parkinson Center of Oregon,Portland, OR; 5University of Chicago, Chicago, IL; 6Imperial Col-lege, Hammersmith Hospital, London, United Kingdom; 7New YorkUniversity Medical Center, New York, NY; 8Duke Movement Dis-orders Clinic; 9Duke University, Durham, NC; 10University of Vir-ginia, Charlottesville, VA; 11North Shore Long Island Jewish ResearchInstitute, Manhasset, NY; 12University of British Columbia, Vancou-ver, British Columbia, Canada; 13Amgen Ltd., Cambridge, UnitedKingdom;
14Medtronic Inc., Minneapolis, MN; and 15Amgen Inc.,
Thousand Oaks, CA.
Received Aug 1, 2005, and in revised form Oct 3. Accepted forpublication Oct 6, 2005.
Published online Jan 20, 2006 in Wiley InterScience(www.interscience.wiley.com). DOI: 10.1002/ana.20737
Address correspondence to Dr Lang, Department of Medicine(Neurology), University of Toronto, Toronto Western HospitalMovement Disorders Center, 399 Bathurst Street, 7McL, Toronto,ON, Canada M5T 2S8. E-mail: [email protected]
ORIGINAL ARTICLES
© 2006 American Neurological Association 459Published by Wiley-Liss, Inc., through Wiley Subscription Services
Future Direction: Therapeutic Genes
1164 www.thelancet.com/neurology Vol 9 December 2010
Articles
Lancet Neurol 2010; 9: 1164–72
Published OnlineOctober 21, 2010
DOI:10.1016/S1474-4422(10)70254-4
See Refl ection and Reaction page 1142
Departments of Neurology (W J Marks Jr MD, J L Ostrem MD)
and Neurosurgery (P A Starr MD, P S Larson MD),
University of California San Francisco, San Francisco, CA,
USA; Ceregene, San Diego, CA, USA (R T Bartus PhD,
J Siff ert MD); Departments of Neurosurgery (N Boulis MD) and Neurology (J Vitek MD),
Cleveland Clinic, Cleveland, OH, USA; Departments of
Neurology (M Stacy MD) and Neurosurgery (D Turner MD),
Duke University, Durham, NC, USA; Departments of
Neurology (L Verhagen MD, J H Kordower PhD) and
Neurosurgery (R Bakay MD), Rush Medical University,
Chicago, IL, USA; Departments of Neurology (R Watts MD) and
Neurosurgery (B Guthrie MD), University of Alabama, Birmingham, AL, USA;
Departments of Neurology (J Jankovic MD) and
Neurosurgery (R Simpson MD), Baylor University, Houston, TX,
USA; Departments of Neurology (M Tagliati MD,
C W Olanow MD), Neurosurgery (R Alterman MD), and
Neuroscience (C W Olanow), Mount Sinai School of
Medicine, New York, NY, USA; Departments of Neurology
(M Stern MD) and Neurosurgery (G Baltuch MD), University of
Pennsylvania, Philadelphia, PA, USA; Department of
Neurology, University of Oregon, Portland, OR, USA
(J Nutt MD); CSD Biostatistics, San Diego, CA, USA
(C S Davis PhD); Department of Neurosurgery, University of
Toronto, Toronto, Canada (A Lozano MD); Department of
Neurology, University of Rochester, Rochester, NY, USA
Gene delivery of AAV2-neurturin for Parkinson’s disease: a double-blind, randomised, controlled trialWilliam J Marks Jr*, Raymond T Bartus*, Joao Siff ert, Charles S Davis, Andres Lozano, Nicholas Boulis, Jerrold Vitek, Mark Stacy, Dennis Turner, Leonard Verhagen, Roy Bakay, Raymond Watts, Barton Guthrie, Joseph Jankovic, Richard Simpson, Michele Tagliati, Ron Alterman, Matthew Stern, Gordon Baltuch, Philip A Starr, Paul S Larson, Jill L Ostrem, John Nutt, Karl Kieburtz, Jeff rey H Kordower, C Warren Olanow*
Summary Background In an open-label phase 1 trial, gene delivery of the trophic factor neurturin via an adeno-associated type-2 vector (AAV2) was well tolerated and seemed to improve motor function in patients with advanced Parkinson’s disease. We aimed to assess the safety and effi cacy of AAV2-neurturin in a double-blind, phase 2 randomised trial.
Methods We did a multicentre, double-blind, sham-surgery controlled trial in patients with advanced Parkinson’s disease. Patients were randomly assigned (2:1) by a central, computer generated, randomisation code to receive either AAV2-neurturin (5·4×10¹¹ vector genomes) injected bilaterally into the putamen or sham surgery. All patients and study personnel with the exception of the neurosurgical team were masked to treatment assignment. The primary endpoint was change from baseline to 12 months in the motor subscore of the unifi ed Parkinson’s disease rating scale in the practically-defi ned off state. All randomly assigned patients who had at least one assessment after baseline were included in the primary analyses. This trial is registered at ClinicalTrials.gov, NCT00400634.
Results Between December, 2006, and November, 2008, 58 patients from nine sites in the USA participated in the trial. There was no signifi cant diff erence in the primary endpoint in patients treated with AAV2-neurturin compared with control individuals (diff erence –0·31 [SE 2·63], 95% CI –5·58 to 4·97; p=0·91). Serious adverse events occurred in 13 of 38 patients treated with AAV2-neurturin and four of 20 control individuals. Three patients in the AAV2-neurturin group and two in the sham surgery group developed tumours.
Interpretation Intraputaminal AAV2-neurturin is not superior to sham surgery when assessed using the UPDRS motor score at 12 months. However, the possibility of a benefi t with additional targeting of the substantia nigra and longer term follow-up should be investigated in further studies.
Funding Ceregene and Michael J Fox Foundation for Parkinson’s Research.
Introduction Parkinson’s disease is a common neurodegenerative disorder characterised clinically by bradykinesia, rigidity, tremor, and gait dysfunction, and pathologically by degeneration of dopamine neurons in the substantia nigra pars compacta. Present therapies provide satisfactory disease control for most patients, particularly in the early stages. However, chronic levodopa treatment is associated with motor complications, does not control potentially disabling features such as falling and dementia, and fails to prevent disease progression.1 Thus, many patients suff er disability despite available medical and surgical treatments. More eff ective treatments that improve clinical disease control and slow progression are urgently needed.
Neurotrophic factors might improve neuronal function and protect against neurodegeneration. Glial-cell-derived neurotrophic factor (GDNF) protects dopamine neurons in in-vitro and animal models of Parkinson’s disease.2,3
Neurturin is a naturally occurring structural and functional analogue of GDNF4 that improved dopaminergic activity in aged monkeys5 and also protected dopamine neurons in animal models of Parkinson’s disease.6–9 Results from open-label trials have shown benefi ts of continuous
infusion of GDNF into the putamen in patients with advanced Parkinson’s disease.10,11 However, these results were not confi rmed in double-blind studies,12,13 possibly because the trophic factor was not adequately distributed throughout the target region.14,15
Gene delivery has the potential to provide diff use distribution and long-lasting expression of a therapeutic protein in one surgical procedure, and gene delivery of neurturin and GDNF provides long-term histological and behavioural benefi ts in primate models of Parkinson’s disease.5,9,16,17 Adeno-associated type-2 (AAV2)-neurturin is a vector that has been genetically engineered to express and secrete the human gene for neurturin.8 The AAV2 vector does not induce an infl ammatory reaction, has been used safely in clinical trials, and provides long-lasting transgene expression.18 An open-label, 12-month phase 1 trial of bilateral stereotactic intraputaminal injections of AAV2-neurturin in patients with advanced Parkinson’s disease showed that the treatment was safe, well tolerated, and associated with benefi ts in motor functions.19
We therefore aimed to assess the safety and effi cacy of stereotactic surgery with injections of AAV2-neurturin versus sham surgery in patients with advanced Parkinson’s disease in a double-blind, randomised trial.
1164 www.thelancet.com/neurology Vol 9 December 2010
Articles
Lancet Neurol 2010; 9: 1164–72
Published OnlineOctober 21, 2010
DOI:10.1016/S1474-4422(10)70254-4
See Refl ection and Reaction page 1142
Departments of Neurology (W J Marks Jr MD, J L Ostrem MD)
and Neurosurgery (P A Starr MD, P S Larson MD),
University of California San Francisco, San Francisco, CA,
USA; Ceregene, San Diego, CA, USA (R T Bartus PhD,
J Siff ert MD); Departments of Neurosurgery (N Boulis MD) and Neurology (J Vitek MD),
Cleveland Clinic, Cleveland, OH, USA; Departments of
Neurology (M Stacy MD) and Neurosurgery (D Turner MD),
Duke University, Durham, NC, USA; Departments of
Neurology (L Verhagen MD, J H Kordower PhD) and
Neurosurgery (R Bakay MD), Rush Medical University,
Chicago, IL, USA; Departments of Neurology (R Watts MD) and
Neurosurgery (B Guthrie MD), University of Alabama, Birmingham, AL, USA;
Departments of Neurology (J Jankovic MD) and
Neurosurgery (R Simpson MD), Baylor University, Houston, TX,
USA; Departments of Neurology (M Tagliati MD,
C W Olanow MD), Neurosurgery (R Alterman MD), and
Neuroscience (C W Olanow), Mount Sinai School of
Medicine, New York, NY, USA; Departments of Neurology
(M Stern MD) and Neurosurgery (G Baltuch MD), University of
Pennsylvania, Philadelphia, PA, USA; Department of
Neurology, University of Oregon, Portland, OR, USA
(J Nutt MD); CSD Biostatistics, San Diego, CA, USA
(C S Davis PhD); Department of Neurosurgery, University of
Toronto, Toronto, Canada (A Lozano MD); Department of
Neurology, University of Rochester, Rochester, NY, USA
Gene delivery of AAV2-neurturin for Parkinson’s disease: a double-blind, randomised, controlled trialWilliam J Marks Jr*, Raymond T Bartus*, Joao Siff ert, Charles S Davis, Andres Lozano, Nicholas Boulis, Jerrold Vitek, Mark Stacy, Dennis Turner, Leonard Verhagen, Roy Bakay, Raymond Watts, Barton Guthrie, Joseph Jankovic, Richard Simpson, Michele Tagliati, Ron Alterman, Matthew Stern, Gordon Baltuch, Philip A Starr, Paul S Larson, Jill L Ostrem, John Nutt, Karl Kieburtz, Jeff rey H Kordower, C Warren Olanow*
Summary Background In an open-label phase 1 trial, gene delivery of the trophic factor neurturin via an adeno-associated type-2 vector (AAV2) was well tolerated and seemed to improve motor function in patients with advanced Parkinson’s disease. We aimed to assess the safety and effi cacy of AAV2-neurturin in a double-blind, phase 2 randomised trial.
Methods We did a multicentre, double-blind, sham-surgery controlled trial in patients with advanced Parkinson’s disease. Patients were randomly assigned (2:1) by a central, computer generated, randomisation code to receive either AAV2-neurturin (5·4×10¹¹ vector genomes) injected bilaterally into the putamen or sham surgery. All patients and study personnel with the exception of the neurosurgical team were masked to treatment assignment. The primary endpoint was change from baseline to 12 months in the motor subscore of the unifi ed Parkinson’s disease rating scale in the practically-defi ned off state. All randomly assigned patients who had at least one assessment after baseline were included in the primary analyses. This trial is registered at ClinicalTrials.gov, NCT00400634.
Results Between December, 2006, and November, 2008, 58 patients from nine sites in the USA participated in the trial. There was no signifi cant diff erence in the primary endpoint in patients treated with AAV2-neurturin compared with control individuals (diff erence –0·31 [SE 2·63], 95% CI –5·58 to 4·97; p=0·91). Serious adverse events occurred in 13 of 38 patients treated with AAV2-neurturin and four of 20 control individuals. Three patients in the AAV2-neurturin group and two in the sham surgery group developed tumours.
Interpretation Intraputaminal AAV2-neurturin is not superior to sham surgery when assessed using the UPDRS motor score at 12 months. However, the possibility of a benefi t with additional targeting of the substantia nigra and longer term follow-up should be investigated in further studies.
Funding Ceregene and Michael J Fox Foundation for Parkinson’s Research.
Introduction Parkinson’s disease is a common neurodegenerative disorder characterised clinically by bradykinesia, rigidity, tremor, and gait dysfunction, and pathologically by degeneration of dopamine neurons in the substantia nigra pars compacta. Present therapies provide satisfactory disease control for most patients, particularly in the early stages. However, chronic levodopa treatment is associated with motor complications, does not control potentially disabling features such as falling and dementia, and fails to prevent disease progression.1 Thus, many patients suff er disability despite available medical and surgical treatments. More eff ective treatments that improve clinical disease control and slow progression are urgently needed.
Neurotrophic factors might improve neuronal function and protect against neurodegeneration. Glial-cell-derived neurotrophic factor (GDNF) protects dopamine neurons in in-vitro and animal models of Parkinson’s disease.2,3
Neurturin is a naturally occurring structural and functional analogue of GDNF4 that improved dopaminergic activity in aged monkeys5 and also protected dopamine neurons in animal models of Parkinson’s disease.6–9 Results from open-label trials have shown benefi ts of continuous
infusion of GDNF into the putamen in patients with advanced Parkinson’s disease.10,11 However, these results were not confi rmed in double-blind studies,12,13 possibly because the trophic factor was not adequately distributed throughout the target region.14,15
Gene delivery has the potential to provide diff use distribution and long-lasting expression of a therapeutic protein in one surgical procedure, and gene delivery of neurturin and GDNF provides long-term histological and behavioural benefi ts in primate models of Parkinson’s disease.5,9,16,17 Adeno-associated type-2 (AAV2)-neurturin is a vector that has been genetically engineered to express and secrete the human gene for neurturin.8 The AAV2 vector does not induce an infl ammatory reaction, has been used safely in clinical trials, and provides long-lasting transgene expression.18 An open-label, 12-month phase 1 trial of bilateral stereotactic intraputaminal injections of AAV2-neurturin in patients with advanced Parkinson’s disease showed that the treatment was safe, well tolerated, and associated with benefi ts in motor functions.19
We therefore aimed to assess the safety and effi cacy of stereotactic surgery with injections of AAV2-neurturin versus sham surgery in patients with advanced Parkinson’s disease in a double-blind, randomised trial.
• Neurturin: natural structural and funcDonal analogue of GDNF that improves dopaminergic acDvity in monkeys and protects dopamine neurons in animal models of Parkinson’s disease
• AAV2-‐neurturin a vector that has been geneDcally engineered to express and secrete the human gene for neurturin.
• In 58 paDents randomized for the study, there was no significant difference in primary outcome measures.
Safety and tolerability of putaminal AADCgene therapy for Parkinson disease
C.W. Christine, MDP.A. Starr, MDP.S. Larson, MDJ.L. Eberling, PhDW.J. Jagust, MDR.A. Hawkins, PhDH.F. VanBrocklin, PhDJ.F. Wright, PhDK.S. Bankiewicz, PhDM.J. Aminoff, MD
ABSTRACT
Background: In Parkinson disease (PD), the benefit of levodopa therapy becomes less marked overtime, perhaps because degeneration of nigrostrial neurons causes progressive loss of aromaticL-amino acid decarboxylase (AADC), the enzyme that converts levodopa into dopamine. In a pri-mate model of PD, intrastriatal infusion of an adeno-associated viral type 2 vector containing thehuman AADC gene (AAV-hAADC) results in robust response to low-dose levodopa without theside effects associated with higher doses. These data prompted a clinical trial.
Methods: Patients with moderately advanced PD received bilateral intraputaminal infusion ofAAV-hAADC vector. Low-dose and high-dose cohorts (5 patients in each) were studied usingstandardized clinical rating scales at baseline and 6 months. PET scans using the AADC tracer[18F]fluoro-L-m-tyrosine (FMT) were performed as a measure of gene expression.
Results: The gene therapy was well tolerated, but 1 symptomatic and 2 asymptomatic intracranialhemorrhages followed the operative procedure. Total and motor rating scales improved in bothcohorts. Motor diaries also showed increased on-time and reduced off-time without increased“on” time dyskinesia. At 6 months, FMT PET showed a 30% increase of putaminal uptake in thelow-dose cohort and a 75% increase in the high-dose cohort.
Conclusion: This study provides class IV evidence that bilateral intrastriatal infusion of adeno-associated viral type 2 vector containing the human AADC gene improves mean scores on theUnified Parkinson’s Disease Rating Scale by approximately 30% in the on and off states, but thesurgical procedure may be associated with an increased risk of intracranial hemorrhage and self-limited headache. Neurology® 2009;73:1662–1669
GLOSSARYAADC ! L-amino acid decarboxylase; AAV-hAADC ! adeno-associated viral type 2 vector containing the human AADC gene;DA ! dopamine; FMT ! [18F]fluoro-L-m-tyrosine; MPTP ! 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; MSN ! mediumspiny neurons; NS ! not significant; PD ! Parkinson disease; UPDRS ! Unified Parkinson’s Disease Rating Scale.
After initial improvement with levodopa, many patients with Parkinson disease (PD) eventu-ally require higher doses for benefit, and their condition is then often complicated by sideeffects such as motor fluctuations, dyskinesias, hallucinations, and autonomic symptoms. Thereason for the waning benefit of levodopa is unknown.
Peripherally administered levodopa is decarboxylated to dopamine (DA) by L-amino aciddecarboxylase (AADC), presumably within dopaminergic terminals in the striatum. One rea-son for the waning benefit of levodopa treatment may be that the conversion to DA is reduceddue to declining levels of AADC.1 We chose a strategy to restore dopaminergic function bydelivering the AADC gene directly into nondegenerating striatal neurons (the site of DA ac-tion) by means of an adeno-associated viral vector (AAV-hAADC), thereby eliminating theneed for the nigral neurons in DA synthesis. Potential advantages of this approach are that it
e-Pub ahead of print on October 14, 2009, at www.neurology.org.From the Departments of Neurology (C.W.C., K.S.B., M.J.A.), Neurological Surgery (P.A.S., P.S.L., K.S.B.), and Radiology and Biomedical Imaging(R.A.H., H.F.V.), University of California, San Francisco, CA; The Michael J. Fox Foundation for Parkinson’s Research (J.L.E.), New York, NY;Department of Molecular Imaging and Neuroscience, Lawrence Berkeley National Laboratory, and Helen Wills Neuroscience Institute (W.J.J.),University of California, Berkeley, CA; University of Pennsylvania School of Medicine (J.F.W.), Philadelphia, PA.
Disclosure: Author disclosures are provided at the end of the article.
Supplemental data atwww.neurology.org
Address correspondence andreprint requests to Dr. MichaelJ. Aminoff, UCSF Department ofNeurology, 505 Parnassus Ave.,Room 795-M, San Francisco, [email protected]
1662 Copyright © 2009 by AAN Enterprises, Inc.
Safety and tolerability of putaminal AADCgene therapy for Parkinson disease
C.W. Christine, MDP.A. Starr, MDP.S. Larson, MDJ.L. Eberling, PhDW.J. Jagust, MDR.A. Hawkins, PhDH.F. VanBrocklin, PhDJ.F. Wright, PhDK.S. Bankiewicz, PhDM.J. Aminoff, MD
ABSTRACT
Background: In Parkinson disease (PD), the benefit of levodopa therapy becomes less marked overtime, perhaps because degeneration of nigrostrial neurons causes progressive loss of aromaticL-amino acid decarboxylase (AADC), the enzyme that converts levodopa into dopamine. In a pri-mate model of PD, intrastriatal infusion of an adeno-associated viral type 2 vector containing thehuman AADC gene (AAV-hAADC) results in robust response to low-dose levodopa without theside effects associated with higher doses. These data prompted a clinical trial.
Methods: Patients with moderately advanced PD received bilateral intraputaminal infusion ofAAV-hAADC vector. Low-dose and high-dose cohorts (5 patients in each) were studied usingstandardized clinical rating scales at baseline and 6 months. PET scans using the AADC tracer[18F]fluoro-L-m-tyrosine (FMT) were performed as a measure of gene expression.
Results: The gene therapy was well tolerated, but 1 symptomatic and 2 asymptomatic intracranialhemorrhages followed the operative procedure. Total and motor rating scales improved in bothcohorts. Motor diaries also showed increased on-time and reduced off-time without increased“on” time dyskinesia. At 6 months, FMT PET showed a 30% increase of putaminal uptake in thelow-dose cohort and a 75% increase in the high-dose cohort.
Conclusion: This study provides class IV evidence that bilateral intrastriatal infusion of adeno-associated viral type 2 vector containing the human AADC gene improves mean scores on theUnified Parkinson’s Disease Rating Scale by approximately 30% in the on and off states, but thesurgical procedure may be associated with an increased risk of intracranial hemorrhage and self-limited headache. Neurology® 2009;73:1662–1669
GLOSSARYAADC ! L-amino acid decarboxylase; AAV-hAADC ! adeno-associated viral type 2 vector containing the human AADC gene;DA ! dopamine; FMT ! [18F]fluoro-L-m-tyrosine; MPTP ! 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; MSN ! mediumspiny neurons; NS ! not significant; PD ! Parkinson disease; UPDRS ! Unified Parkinson’s Disease Rating Scale.
After initial improvement with levodopa, many patients with Parkinson disease (PD) eventu-ally require higher doses for benefit, and their condition is then often complicated by sideeffects such as motor fluctuations, dyskinesias, hallucinations, and autonomic symptoms. Thereason for the waning benefit of levodopa is unknown.
Peripherally administered levodopa is decarboxylated to dopamine (DA) by L-amino aciddecarboxylase (AADC), presumably within dopaminergic terminals in the striatum. One rea-son for the waning benefit of levodopa treatment may be that the conversion to DA is reduceddue to declining levels of AADC.1 We chose a strategy to restore dopaminergic function bydelivering the AADC gene directly into nondegenerating striatal neurons (the site of DA ac-tion) by means of an adeno-associated viral vector (AAV-hAADC), thereby eliminating theneed for the nigral neurons in DA synthesis. Potential advantages of this approach are that it
e-Pub ahead of print on October 14, 2009, at www.neurology.org.
From the Departments of Neurology (C.W.C., K.S.B., M.J.A.), Neurological Surgery (P.A.S., P.S.L., K.S.B.), and Radiology and Biomedical Imaging(R.A.H., H.F.V.), University of California, San Francisco, CA; The Michael J. Fox Foundation for Parkinson’s Research (J.L.E.), New York, NY;Department of Molecular Imaging and Neuroscience, Lawrence Berkeley National Laboratory, and Helen Wills Neuroscience Institute (W.J.J.),University of California, Berkeley, CA; University of Pennsylvania School of Medicine (J.F.W.), Philadelphia, PA.
Disclosure: Author disclosures are provided at the end of the article.
Supplemental data atwww.neurology.org
Address correspondence andreprint requests to Dr. MichaelJ. Aminoff, UCSF Department ofNeurology, 505 Parnassus Ave.,Room 795-M, San Francisco, [email protected]
1662 Copyright © 2009 by AAN Enterprises, Inc.
Safety and tolerability of putaminal AADCgene therapy for Parkinson disease
C.W. Christine, MDP.A. Starr, MDP.S. Larson, MDJ.L. Eberling, PhDW.J. Jagust, MDR.A. Hawkins, PhDH.F. VanBrocklin, PhDJ.F. Wright, PhDK.S. Bankiewicz, PhDM.J. Aminoff, MD
ABSTRACT
Background: In Parkinson disease (PD), the benefit of levodopa therapy becomes less marked overtime, perhaps because degeneration of nigrostrial neurons causes progressive loss of aromaticL-amino acid decarboxylase (AADC), the enzyme that converts levodopa into dopamine. In a pri-mate model of PD, intrastriatal infusion of an adeno-associated viral type 2 vector containing thehuman AADC gene (AAV-hAADC) results in robust response to low-dose levodopa without theside effects associated with higher doses. These data prompted a clinical trial.
Methods: Patients with moderately advanced PD received bilateral intraputaminal infusion ofAAV-hAADC vector. Low-dose and high-dose cohorts (5 patients in each) were studied usingstandardized clinical rating scales at baseline and 6 months. PET scans using the AADC tracer[18F]fluoro-L-m-tyrosine (FMT) were performed as a measure of gene expression.
Results: The gene therapy was well tolerated, but 1 symptomatic and 2 asymptomatic intracranialhemorrhages followed the operative procedure. Total and motor rating scales improved in bothcohorts. Motor diaries also showed increased on-time and reduced off-time without increased“on” time dyskinesia. At 6 months, FMT PET showed a 30% increase of putaminal uptake in thelow-dose cohort and a 75% increase in the high-dose cohort.
Conclusion: This study provides class IV evidence that bilateral intrastriatal infusion of adeno-associated viral type 2 vector containing the human AADC gene improves mean scores on theUnified Parkinson’s Disease Rating Scale by approximately 30% in the on and off states, but thesurgical procedure may be associated with an increased risk of intracranial hemorrhage and self-limited headache. Neurology® 2009;73:1662–1669
GLOSSARYAADC ! L-amino acid decarboxylase; AAV-hAADC ! adeno-associated viral type 2 vector containing the human AADC gene;DA ! dopamine; FMT ! [18F]fluoro-L-m-tyrosine; MPTP ! 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; MSN ! mediumspiny neurons; NS ! not significant; PD ! Parkinson disease; UPDRS ! Unified Parkinson’s Disease Rating Scale.
After initial improvement with levodopa, many patients with Parkinson disease (PD) eventu-ally require higher doses for benefit, and their condition is then often complicated by sideeffects such as motor fluctuations, dyskinesias, hallucinations, and autonomic symptoms. Thereason for the waning benefit of levodopa is unknown.
Peripherally administered levodopa is decarboxylated to dopamine (DA) by L-amino aciddecarboxylase (AADC), presumably within dopaminergic terminals in the striatum. One rea-son for the waning benefit of levodopa treatment may be that the conversion to DA is reduceddue to declining levels of AADC.1 We chose a strategy to restore dopaminergic function bydelivering the AADC gene directly into nondegenerating striatal neurons (the site of DA ac-tion) by means of an adeno-associated viral vector (AAV-hAADC), thereby eliminating theneed for the nigral neurons in DA synthesis. Potential advantages of this approach are that it
e-Pub ahead of print on October 14, 2009, at www.neurology.org.From the Departments of Neurology (C.W.C., K.S.B., M.J.A.), Neurological Surgery (P.A.S., P.S.L., K.S.B.), and Radiology and Biomedical Imaging(R.A.H., H.F.V.), University of California, San Francisco, CA; The Michael J. Fox Foundation for Parkinson’s Research (J.L.E.), New York, NY;Department of Molecular Imaging and Neuroscience, Lawrence Berkeley National Laboratory, and Helen Wills Neuroscience Institute (W.J.J.),University of California, Berkeley, CA; University of Pennsylvania School of Medicine (J.F.W.), Philadelphia, PA.
Disclosure: Author disclosures are provided at the end of the article.
Supplemental data atwww.neurology.org
Address correspondence andreprint requests to Dr. MichaelJ. Aminoff, UCSF Department ofNeurology, 505 Parnassus Ave.,Room 795-M, San Francisco, [email protected]
1662 Copyright © 2009 by AAN Enterprises, Inc.
• L-‐amino acid decarboxylase (AADC): enzyme that converts levodopa into dopamine.
• 10 paDents received either high or low dose intraputaminal infusion of AAV-‐hAADC.
• StaDsDcally significant improvements in UPDRS raDng.• 30% increase of putaminal uptake of AADC in low dose group; 75% in high-‐dose.

Future Direction: Cell Transplantation
• Previous attempts at cell-based dopamine replacement therapy: implantation of adrenal medullary, fetal mesencephalic, and cultured human mesencephalic tissue grafts.6
• Bakay. 2004. Unilateral implantation of cultured, dopamine-producing hRPE cells attached to Spheramine microcarrier.13
• UDPRS scores improved by 34% at 6 month follow-up.
• Phase II clinical trials expected to be completed in late 2006, although no published studies as of yet.
Summary• DBS for movement disorders effective in
the treatment of Parkinson’s, dystonia, essential tremor
• Future areas of research include continued investigations into biotechnology, improvements in hardware design, and identifying new surgical targets for a variety of disorders.
Hemifacial Spasm
• Characterized by involuntary paroxysmal contractions of muscles innervated by the facial nerve.
• Affects women more than men, and usually appears in the 4th - 7th decade of life14.
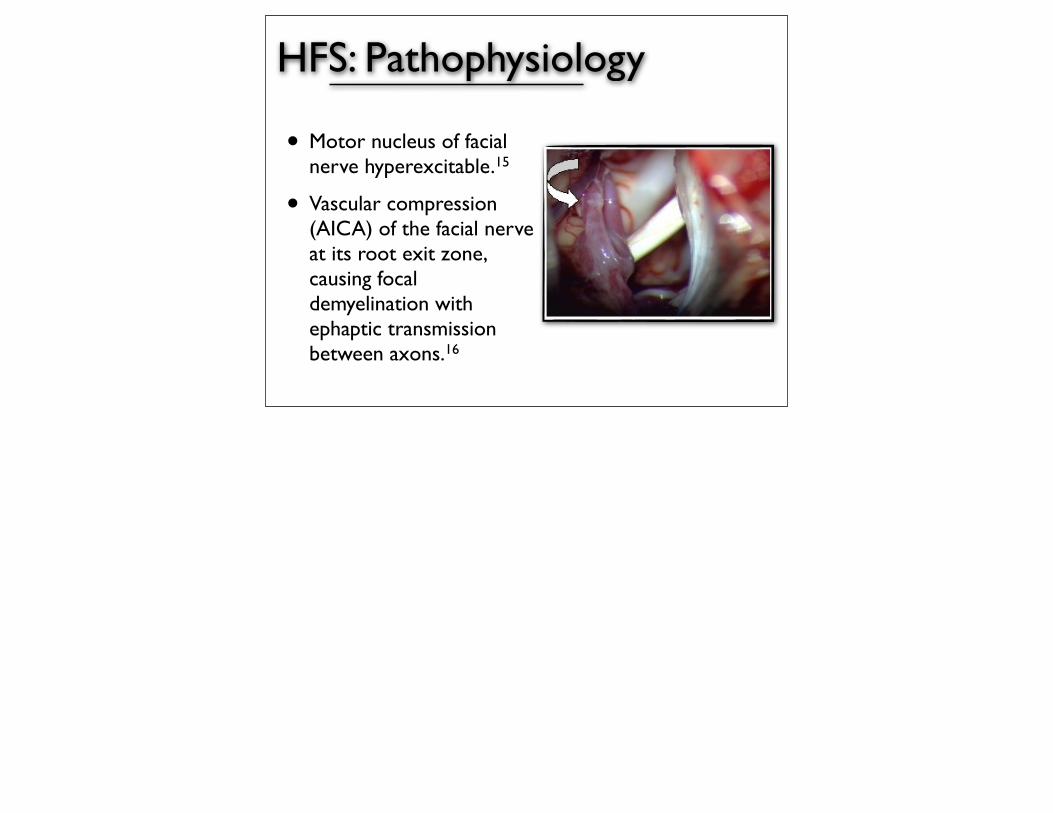
HFS: Pathophysiology
• Motor nucleus of facial nerve hyperexcitable.15
• Vascular compression (AICA) of the facial nerve at its root exit zone, causing focal demyelination with ephaptic transmission between axons.16
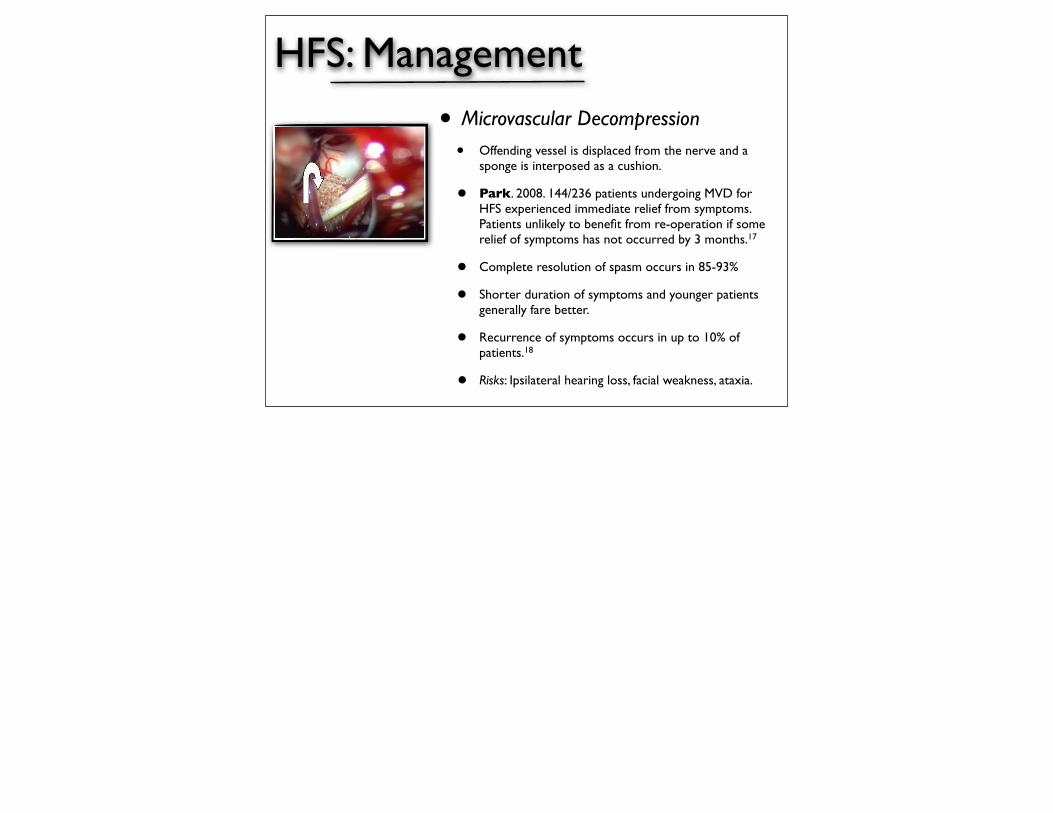
HFS: Management
• Microvascular Decompression
• Offending vessel is displaced from the nerve and a sponge is interposed as a cushion.
• Park. 2008. 144/236 patients undergoing MVD for HFS experienced immediate relief from symptoms. Patients unlikely to benefit from re-operation if some relief of symptoms has not occurred by 3 months.17
• Complete resolution of spasm occurs in 85-93%
• Shorter duration of symptoms and younger patients generally fare better.
• Recurrence of symptoms occurs in up to 10% of patients.18
• Risks: Ipsilateral hearing loss, facial weakness, ataxia.
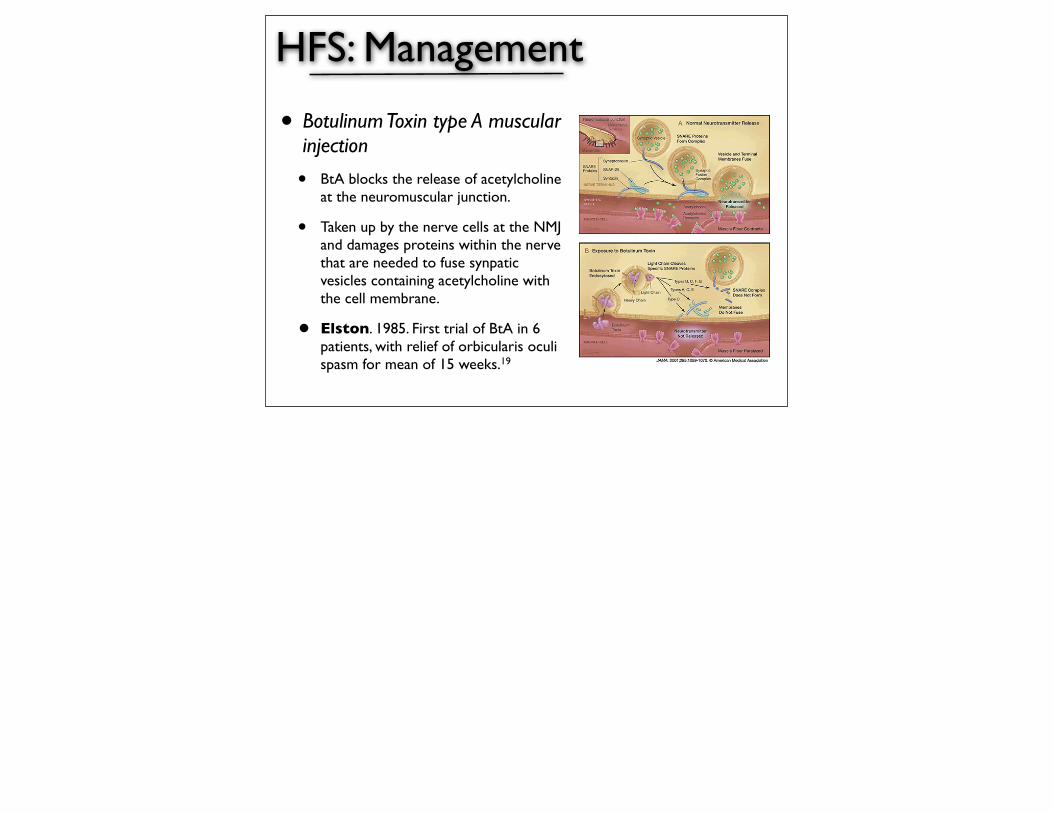
HFS: Management
• Botulinum Toxin type A muscular injection
• BtA blocks the release of acetylcholine at the neuromuscular junction.
• Taken up by the nerve cells at the NMJ and damages proteins within the nerve that are needed to fuse synpatic vesicles containing acetylcholine with the cell membrane.
• Elston. 1985. First trial of BtA in 6 patients, with relief of orbicularis oculi spasm for mean of 15 weeks.19

The effectiveness of botulinum toxin injections in 11 patients with hemifacial spasm was investigated in a prospective placebo-controlled blinded study. The patients were treated with four sets of injections to various facial mus- cles, selected by clinical evaluation. Three injections were with graded doses of toxin and one was with placebo. The order of injections was ran- dom and unknown to the patients. Results were scored both subjectively by patient assessment of symptoms and objectively by blinded review of vid- eotapes made one month after each injection. Subjective improvement oc- curred after 79% of injections with botulinum toxin, regardless of dose of toxin. Only 1 patient improved after placebo. Objective improvement was seen after 84% of injections with botulinum toxin. No patient showed objec- tive improvement after placebo injection. The most frequent side effect was facial weakness, seen after 97% of injections of botulinum toxin. Facial bruising (20%), diplopia (13O/0), ptosis (7%), and various other mild side ef- fects were seen less frequently. Botulinum toxin appears to be an effective and safe method of therapy for hemifacial spasm. 0 1992 John Wiley & Sons, Inc. Key words: hemifacial spasm botulinum toxin botox facial nerve
MUSCLE & NERVE 15:1045-1049 1992
TREATMENT OF HEMIFACIAL SPASM WITH BOTULINUM TOXIN DON M. YOSHIMURA, MD, MICHAEL J. AMINOFF, MD, FRCP, THOMAS A. TAMI, MD, and ALAN B. SCOTT, MD
Botulinum toxin is an effective therapy for a wide variety of muscle hyperactivity states and focal dystonias, including blepharo~pasm,~. '~ s asmodic tortiCollis,2,6,9, 17.19 spastic dysphonia,"."and oc- cupational cramps."18 In hemifacial spasm, a dis- order in which the muscles on one side of the face exhibit involuntary and repetitive contractions that have been attributed by some to vascular compression of the facial nerve, medical treatment is often unsatisfactory.8 A microvascular decom- pressive procedure may be helpful, but involves a direct operative approach. Several clinical trials have shown botulinum toxin to be highly effective for this condition with only minimal side ef- fects, 1.2,5,10,13,15 but these studies have generally been uncontrolled and most neurologists are un- familiar with them. Moreover, the manner in which botulinum toxin is given for hemifacial
From the Departments of Neurology (Drs. Yoshirnura and Aminoff) and Otolaryngology (Dr. Tarni), University of California at San Francisco, San Francisco, California; and Smith-Kettlewell Eye Research Institute, San Francisco, California (Dr. Scott).
Address reprint requests to Michael J Aminoff, MD, FRCP. Professor of Neurology, Room 794-M, Box 0114, School of Medicine. University of California, San Francisco, CA 94143-01 14
Accepted for publication February 9, 1992.
CCC 0148-639X/92/091045-05 $04 00 0 1992 John Wiley 8, Sons, Inc.
spasm, and the adverse effects that may occur with its use in this context, are not widely appreci- ated. Therefore, we decided to evaluate the effi- cacy of this approach to treating hemifacial spasm by a prospective, placebo-controlled, double- blinded trial, and to determine the nature and in- cidence of side effects both in this study group and in a larger group of patients followed as part of an open trial.
METHODS Eleven patients (8 women, 3 men) referred to the UCSF Movement Disorders Clinic with hemifacial spasm were studied. Their mean age was 50 years, with a range of 37 to 68 years. Mean duration of symptoms was 5.2 years, with a range of 1.5 to 12 years. Nine of the 11 patients had left-sided in- volvement, and 6 patients showed mild preinjec- tion facial weakness ipsilateral to the spasm. All patients had been treated with a wide variety of medications without success. One patient had un- dergone four surgical microvascular decompres- sive procedures without lasting benefit.
On entry into the study, patients were evalu- ated by each of us, the extent and severity of the hemifacial spasm and pattern of muscle involve- ment being determined clinically. This pattern usually included the following muscles: (1) fronta-
Hemifacial Spasm and Botox MUSCLE & NERVE September 1992 1045
The effectiveness of botulinum toxin injections in 11 patients with hemifacial spasm was investigated in a prospective placebo-controlled blinded study. The patients were treated with four sets of injections to various facial mus- cles, selected by clinical evaluation. Three injections were with graded doses of toxin and one was with placebo. The order of injections was ran- dom and unknown to the patients. Results were scored both subjectively by patient assessment of symptoms and objectively by blinded review of vid- eotapes made one month after each injection. Subjective improvement oc- curred after 79% of injections with botulinum toxin, regardless of dose of toxin. Only 1 patient improved after placebo. Objective improvement was seen after 84% of injections with botulinum toxin. No patient showed objec- tive improvement after placebo injection. The most frequent side effect was facial weakness, seen after 97% of injections of botulinum toxin. Facial bruising (20%), diplopia (13O/0), ptosis (7%), and various other mild side ef- fects were seen less frequently. Botulinum toxin appears to be an effective and safe method of therapy for hemifacial spasm. 0 1992 John Wiley & Sons, Inc. Key words: hemifacial spasm botulinum toxin botox facial nerve
MUSCLE & NERVE 15:1045-1049 1992
TREATMENT OF HEMIFACIAL SPASM WITH BOTULINUM TOXIN DON M. YOSHIMURA, MD, MICHAEL J. AMINOFF, MD, FRCP, THOMAS A. TAMI, MD, and ALAN B. SCOTT, MD
Botulinum toxin is an effective therapy for a wide variety of muscle hyperactivity states and focal dystonias, including blepharo~pasm,~. '~ s asmodic tortiCollis,2,6,9, 17.19 spastic dysphonia,"."and oc- cupational cramps."18 In hemifacial spasm, a dis- order in which the muscles on one side of the face exhibit involuntary and repetitive contractions that have been attributed by some to vascular compression of the facial nerve, medical treatment is often unsatisfactory.8 A microvascular decom- pressive procedure may be helpful, but involves a direct operative approach. Several clinical trials have shown botulinum toxin to be highly effective for this condition with only minimal side ef- fects, 1.2,5,10,13,15 but these studies have generally been uncontrolled and most neurologists are un- familiar with them. Moreover, the manner in which botulinum toxin is given for hemifacial
From the Departments of Neurology (Drs. Yoshirnura and Aminoff) and Otolaryngology (Dr. Tarni), University of California at San Francisco, San Francisco, California; and Smith-Kettlewell Eye Research Institute, San Francisco, California (Dr. Scott).
Address reprint requests to Michael J Aminoff, MD, FRCP. Professor of Neurology, Room 794-M, Box 0114, School of Medicine. University of California, San Francisco, CA 94143-01 14
Accepted for publication February 9, 1992.
CCC 0148-639X/92/091045-05 $04 00 0 1992 John Wiley 8, Sons, Inc.
spasm, and the adverse effects that may occur with its use in this context, are not widely appreci- ated. Therefore, we decided to evaluate the effi- cacy of this approach to treating hemifacial spasm by a prospective, placebo-controlled, double- blinded trial, and to determine the nature and in- cidence of side effects both in this study group and in a larger group of patients followed as part of an open trial.
METHODS Eleven patients (8 women, 3 men) referred to the UCSF Movement Disorders Clinic with hemifacial spasm were studied. Their mean age was 50 years, with a range of 37 to 68 years. Mean duration of symptoms was 5.2 years, with a range of 1.5 to 12 years. Nine of the 11 patients had left-sided in- volvement, and 6 patients showed mild preinjec- tion facial weakness ipsilateral to the spasm. All patients had been treated with a wide variety of medications without success. One patient had un- dergone four surgical microvascular decompres- sive procedures without lasting benefit.
On entry into the study, patients were evalu- ated by each of us, the extent and severity of the hemifacial spasm and pattern of muscle involve- ment being determined clinically. This pattern usually included the following muscles: (1) fronta-
Hemifacial Spasm and Botox MUSCLE & NERVE September 1992 1045
• ProspecDve placebo-‐controlled blinded study• 11 paDents randomly assigned to 4 sets of injecDons (low, intermediate or high dose BtA,saline)
• ObjecDve improvement observed in 84% ofinjecDons with BtA at 4 weeks.
• No paDent showed objecDve improvement aker placebo injecDon.
• Side effects: facial weakness, diplopia, ptosis

References1. Cooper IS: Ligation of the anterior choroidal artery for involuntary movements; parkinsonism. Psychiatr Q 27:317–319, 1953. 2. Hassler R. The influence of stimulations and coagulations in the human thalamus on the tremor at rest and its physiopathologic mechanism. In: Greenfield, Godwin J, Russell D, editors. Proceedings of the Second International Congress of Neuropathology. London. Amsterdam: Excerpta Medica; 1955. p. 637– 42.3. Finger S: Origins of Neuroscience. New York, Oxford University Press, 1994, p 39. 4. Hassler R, Riechert T, Mundinger F, Umbach W, Ganglberger JA: Physiological observations in stereotaxic operations in extrapyramidal motor disturbances. Brain 83:337–350, 1960.5. Bechtereva NP, Bondartchuk AN, Smirnov VM, Meliutcheva LA, Shandurina AN: Method of electrostimulation of the deep brain structures in treatment of some chronic diseases. Confin Neurol 37:136–140, 1975.6. Rezai et al. Surgery for Movement Disorders. Neurosurgery. 62 Suppl 2:809-38; discussion 838-9, 2008 Feb.7. Pollak P, Benabid AL, Gervason CL, Hoffmann D, Seigneuret E, Perret J: Long-term effects of chronic stimulation of the ventral intermediate thalamic nucleus in different types of tremor. Adv Neurol 60:408–413, 1993.8. Guiot G, Arfel G, Derome P, Kahn A: Neurophysiologic control procedures for sterotaxic thalamotomy [in French]. Neurochirurgie 14:553–566, 1968.9. Binder DK, Rau GM, Starr PA: Risk factors for hemorrhage during microelectrode-guided deep brain stimulator implantation for movement disorders. Neurosurgery 56:722–732, 200510. Airaksinen MS, Saarma M: The GDNF family: Signalling, biological functions and therapeutic value. Nat Rev Neurosci 3:383–394, 2002. 11. Gill SS, Patel NK, Hotton GR, O'Sullivan K, McCarter R, Bunnage M, Brooks DJ, Svendsen CN, Heywood P: Direct brain infusion of glial cell line-derived neurotrophic factor in Parkinson disease. Nat Med 9:589–595, 2003. 12. Slevin JT, Gash DM, Smith CD, Gerhardt GA, Kryscio R, Chebrolu H, Walton A, Wagner R, Young AB: Unilateral intraputaminal glial cell line-derived neurotrophic factor in patients with Parkinson disease: Response to 1 year each of treatment and withdrawal. Neurosurg Focus 20:E1, 2006.13. Bakay et al. Implantation of Spheramine in advanced Parkinson’s Disease. Frontiers in Bioscience. 9:592-602, 2004 Jan 1.14. Costa et al. Botulinum toxin type A therapy for hemifacial spasm (Review). Cochrane Database of Systematic Reviews. (1):CD004899, 2005.15. Cakmur R, Tataroglu C, Idiman F. Electrophysiologic observations on pathogenic mechanisms of hemifacial spasm: F-waves of the facial muscles and silent period evoked by transcranial magnetic stimulation. European Journal of Neurology 1999;6 Suppl:136.16. Hosoya T, Watanabe N, Yamaguchi K, Saito S, Nakai O. Three-dimensional-MRI of neurovascular compression in patients with hemifacial spasm. Neuroradiology 1995;37(5):350-2. 17. Park et al. Microvascular decompression for treating hemifacial spasm: lessons learned from a prospective study of 1,174 operations.Neurosurgical Review. 33(3):325-34; discussion 334, 2010 Jul.18. Payner et al. Recurrence of hemifacial spasm after microvascular decompression. Neurosurgery 13: 141-6, 1983.19. Elston JS. Botulinum toxin treatment of hemifacial spasm. Journal of Neurology, Neurosurgery and Psychiatry 1986;49:827-29.