-
8/7/2019 Movement Disorders - Overview-1
1/117
SUMAIYA SALIM, M.D.
-
8/7/2019 Movement Disorders - Overview-1
2/117
Classification
y Hypokinesias - typified byslownessand/orpaucityofmovement, eg.
parkinsonism.
y Hyperkinesias - abnormalinvoluntarymovements,eg. chorea,
dystonia, myoclonus, stereotypes, tics,tremors.
-
8/7/2019 Movement Disorders - Overview-1
3/117
Hypokinesias
y Bradykinesia - slownessofmovement
andimpairedinitiation/paucityofmovement (akinesia).
y Rigidity- cogwheeling- increasedresistance topassive
movement.
y Posturalinstability- propulsion, retropulsion.
-
8/7/2019 Movement Disorders - Overview-1
4/117
Hyperkinesias- Chorea
y Chorea - continuous, abrupt, rapid, brief,unsustained,
irregular, random, DANCE-LIKE
movementswhichflowfrom one bodypart
toanother.Maybeincorporatedintosemipurposeful
activities.Motorimpersistance isacommonfeature -
difficultymaintainingsustainedcontractionssuchas
tongueprotrusion.
y Athetosis isacontinuousstream ofslow, sinuous,writhing
movements, typicallyofthehandsandfeet
y Ballism thrashing motions
-
8/7/2019 Movement Disorders - Overview-1
5/117
Hyperkinesias - Dystoniay Dystonia - involuntary, sustained
(tonic)or
intermittent (spasmodic, clonic), patterned,repetitive
musclecontractionswhichfrequentlycause twisting (torticollis),
flexingorextending(writerscramp, retrocollis),
andsqueezing(blepharospasm)orabnormalposture. Maybe
task-specific.
yFocal, segmental, generalized, multifocalandhemidystonia
-
8/7/2019 Movement Disorders - Overview-1
6/117
Hyperkinesias - Myoclonusy Lightning-like
movementssecondaryTO
y briefsuddencontractions (positive myoclonus)
y or muscleinhibition (negative myoclonus). Asterixis:one
typeofnegativemyoclonus
y Focal, segmental, multifocal, generalized.
y Cortical, brainstem (reticular), andspinal
-
8/7/2019 Movement Disorders - Overview-1
7/117
Hyperkinesias - Stereotypies
y Involuntaryorsemi-voluntary(unvoluntary)patterned, repetitive,
coordinated, rhythmic,
purposeless thoughseeminglypurposefulorritualistic movement,
postureorutterance.
y Examplesincludefoot tapping, bodyrocking,
orcomplexrituals.
-
8/7/2019 Movement Disorders - Overview-1
8/117
Hyperkinesias-Tics
y Relativelybrief, repetitive, nonrhythmic,y movements (motor
tics)y sounds (phonic/vocal tics).
y Premonitorysensations - maybelocalized (burning,tension,
tightness)orfeelingofanxiety, an urge
y Suppressible toadegree. suppressible yet irresistibley Simple
motor tics - sudden, brief, meaningless
movementsinvolveonlyonegroupofmuscles (eyeblinking, head
jerkingorshouldershrugging. simple
phonic tic can bealmost anysoundornoise (throatclearing,
sniffing, orgrunting)y Complex motor tic -
clusterofmovementsandapppear
coordinated. (pullingat clothes, touchingpeople). Vocal
echolalia, coprolalia
-
8/7/2019 Movement Disorders - Overview-1
9/117
Hyperkinesias -Tremorsy Involuntary, rhythmic,
oscillatorymovementsabout
a joint secondarytoalternatingorsynchronous
contractionsofantagonist muscles.y Rest - fullysupportedagainst
gravity.
y Action - duringvoluntarycontractions.
y Postural, Kinetic (initial, dynamic, terminalor
intention), task- orposition-specific, isometric.
-
8/7/2019 Movement Disorders - Overview-1
10/117
Anatomy - Basal Ganglia
y 6pairednuclei - caudatenucleus, putamen, globuspallidus,
nucleusaccumbens, subthalamicnucleus
andsubstantianigra.y lenticularnucleus - lenslike -
putamenandglobus
pallidus.
y GPiand SNr behaveassinglefunctionalunit.
-
8/7/2019 Movement Disorders - Overview-1
11/117
Anatomy - Basal Ganglia
y striatum - caudateandputamen - composedofstriosomes
(limbicsystem projectshere), matrix
(neocorticalfibersproject here).y putamen - motor -
receivesinput from
somatosensory, motorandpremotorareas.
y caudate - emotionalandcognitiveprocesses -
posteriorparietaland temporal, frontalassociationareasproject
here.
-
8/7/2019 Movement Disorders - Overview-1
12/117
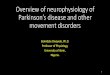
Anatomy - Basal Gangliay Functions to modulate
theamplitudeandvelocityof
movement andin thepreparationfor movement.
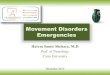
ySeediagramsforproposed basalgangliacircuitryinnormalsandin
Parkinsonsdisease
-
8/7/2019 Movement Disorders - Overview-1
13/117
Cortex
PrefrontalInsular
CingulateSensoryMotor
Suppl. MotorPremotor
PremotorPrefrontal
Striatum
D2 D1 ThalamusVA/VL
+ = excitatory
- = inhibitory
BrainstemSC
SNc
SNr
GPi
STN
GPe
-
+
+
+ -
-
--
-
-
+
++
+
+
+
Normal
-
8/7/2019 Movement Disorders - Overview-1
14/117
Cor ex
re ron ansu ar
Cingu a eensoryo or
upp o orre o or
re o orre ron a
riatu
2 1Thalamus
L
+ = excitatory
= inh ibitory
rainstemSC
SNc
SNri
STN
GPe
++
++++
+
++
+
+
+
Parkinsons isease
-
8/7/2019 Movement Disorders - Overview-1
15/117
Clinical Features/Cardinal Signs
y 1817: James Parkinson AnEssayon the Shaking Palsy
y
Diagnosis requires 2 of 3:y Bradykinesia
y Rigidity
y Tremor (primarily at rest)
y Othersigns: Maskedface, hypovolemic
speech,swallowingdifficulty, micrographia,
flexedposture,shufflinggait, start hesitancyandfreezing
-
8/7/2019 Movement Disorders - Overview-1
16/117
Onsety Insidious, unilateralprogressing to bilateral
-
8/7/2019 Movement Disorders - Overview-1
17/117
Classification of Parkinson Syndromes in a
Community
y Idiopathic PD ~ 85%ofall PS cases
y Neuroleptic-inducedparkinsonism (DIP)7% - 9%
y Vascularparkinson syndrome ~ 3%y PS due to MPTP, CO, Mn,
recurrent head traumais
extremelyrare
y Nonewcasesofpostencephalitic parkinsonism since
1960s
-
8/7/2019 Movement Disorders - Overview-1
18/117
Epidemiology of Parkinson Syndrome
y Incidence:
- 5-24/100000worldwide (USA/Canada 300/100000)-IncidenceofPS/PD
risingslowlywithagingpopulation
-
8/7/2019 Movement Disorders - Overview-1
19/117
Prevalence
y 57-371/100t. worldwide (USA/Canada 300/100t.)
y 35%-42%ofcasesundiagnosedat anytime
-
8/7/2019 Movement Disorders - Overview-1
20/117
Onset
y mean PS 61.6years; PD 62.4 years
y rare beforeage 30; 4-10%cases beforeage 40
-
8/7/2019 Movement Disorders - Overview-1
21/117
Pathology of Parkinsons Disease
y Markedstriatal DAdepletion
Striatal dopaminedeficiencysyndrome
y At death, DAloss > 90%
y
-
8/7/2019 Movement Disorders - Overview-1
22/117
-
8/7/2019 Movement Disorders - Overview-1
23/117
Parkinsons Disease Risk Factors
y Definite: Oldage
y Highlylikely: MZ co-twinwithearly-onset PD
y Probable: Positivefamilyhistoryy Possible:Herbicides,
pesticides, heavymetals,
proximitytoindustry, ruralresidence, wellwater,repeatedhead
trauma, etc.
y Possibleprotectiveeffect: Smoking
-
8/7/2019 Movement Disorders - Overview-1
24/117
Cause of PD
y Unknownin most cases;not acceleratedagingy GenesAD
inheritanceveryrare; mutationunknown
mutationofAlphasynucleingene (chromosome 4q)identifiedinonelarge
Italian (Contursi)and5 Greekautosomaldominant families
mutationofparkingeneinautosomal-recessive
juvenileparkinsonism
y EnvironmentMajorityofcases believedcaused
byenvironmentalfactor (s)
but noneidentifiedsofary Genesplusenvironment?
-
8/7/2019 Movement Disorders - Overview-1
25/117
Early Signs and Symptoms
y CardinalCharacteristics (Requires 2 of3):
y Resting tremor
yBradykinesia
y Rigidity
Andoftenassociatedwith Posturalinstability
-
8/7/2019 Movement Disorders - Overview-1
26/117
Early Signs and Symptoms
Others
y Micrographia
y
Maskedfacey SlowingofADLs
y Stooped, shufflinggait
y Decreasedarm swingwhenwalking
-
8/7/2019 Movement Disorders - Overview-1
27/117
Additional Signs and Symptoms
y Difficultyarisingfrom achair
y Difficultyturningin bed
y Hypophonicspeechy Sialorrhea
y Lossofthesenseofsmell
y Foot dystonia
-
8/7/2019 Movement Disorders - Overview-1
28/117
-
8/7/2019 Movement Disorders - Overview-1
29/117
Clues Suggesting Atypical Parkinsonism
y Earlyonset of, orrapidlyprogressing, dementia
y Rapidlyprogressivecourse
y Supranuclear gazepalsy(impairedverticalgaze,bradykinesia,
posturalinstability, frequent falls,incontinence)
y Upper motorneuronsigns (suggestiveofstrokes)
y Cerebellar signsdysmetria, ataxiay Urinaryincontinence
(NPH)
y Earlysymptomaticposturalhypotension
-
8/7/2019 Movement Disorders - Overview-1
30/117
Hereditary disorders associated with
parkinsonism
y Wilsonsdisease
y Huntingtonsdisease
y Dentatorubro-pallidoluysianatrophy(DRPLA)y
Machado-Josephdisease (SCA-3)
-
8/7/2019 Movement Disorders - Overview-1
31/117
Differential Diagnosis of PDy Drug-induced
y Toxin-induced
y Metabolicy Structurallesions (vascularparkinsonism, etc.)
y Hydrocephalus
y Infections
-
8/7/2019 Movement Disorders - Overview-1
32/117
Drug-Induced Parkinsonism
y Crucial toruleout, since most casesarereversible
y Careful medicationhistorylist drugnames
y Commonoffendingdrug types
y Antipsychotics :haloperidol, chlorpromazine,thioridizine,
perphenazine, risperidone, olanzapine
y Antiemeticsmetoclopramide, prochlorperazine
y Dopaminedepletorsmethyldopa, reserpine,
tetrabenaziney Combinationdrugse.g., Triavil (amitriptyline,
perphenazine)
y Treatment: Stopoffending medication
-
8/7/2019 Movement Disorders - Overview-1
33/117
Metabolic and Infectious Causes of
Parkinsonism
y Metabolicy Oftenreversible
y Hypo- orhyper-thyroidism
y Hypo- orhyper-parathyroidism
y Liverfailure
y Centralpontine myelinolysis
y Infectiousy Post-encephaliticy Creutzfeldt-Jakob disease
y Infectious masses
y HIV
-
8/7/2019 Movement Disorders - Overview-1
34/117
Toxin-induced Parkinsonism
y MPTP
y Carbon monoxide
y Manganesey Cyanide
-
8/7/2019 Movement Disorders - Overview-1
35/117
Structural Lesions Causing Parkinsonism
y Acuteorsubacuteonset
y Othersignshemiparesis, hyperreflexia, aphasia,
sensoryloss, seizuresy Brain tumor
y Infectious mass
y Aneurysm
-
8/7/2019 Movement Disorders - Overview-1
36/117
Vascular Parkinsonism
y Abrupt onset, usuallyunilateral
y Step-wiseornoprogression
y Othersignshemiparesis, aphasia, hyperreflexiay
Infarctsonneuroimaginghelpfulinconfirming
diagnosis
-
8/7/2019 Movement Disorders - Overview-1
37/117
Hydrocephalus-induced Parkinsonism
y Can becommunicatingorobstructive
y Normalpressurehydrocephalusidiopathic
y Clinical triad:y parkinsonism/gait disorder
y urinary/fecalincontinence
y dementia
-
8/7/2019 Movement Disorders - Overview-1
38/117
-
8/7/2019 Movement Disorders - Overview-1
39/117
Parkinsons Disease vs. Essential Tremory Essential tremorshould
be tremorwithnoothersigns
ofparkinsonism
y Bothcanhaveakineticandrest component
y Kinetic tremorcaninterferewith RAM
y Cogwheelrigiditycan befoundinET
-
8/7/2019 Movement Disorders - Overview-1
40/117
TreatmentOptions
y Preventive treatment -- Nodefinitiveavailable
y Symptomatic treatmenty
Pharmacologicaly Surgical
y Non-motor management
y Restorativeexperimentalonlyy Transplantationy Neurotrophic
factors
-
8/7/2019 Movement Disorders - Overview-1
41/117
Drug Classes in PD
y Dopaminergic agents
y Levodopa
y
Dopamineagonistsy COMT inhibitors
y MAO-Binhibitors
y Anticholinergics
y Amantadine
-
8/7/2019 Movement Disorders - Overview-1
42/117
Levodopa
y Most effectivedrugforparkinsonian symptoms
y First developedin thelate1960s;rapidlybecame
thedrugofchoicefor PDy Largeneutralaminoacid;requiresactive
transport
across thegut-bloodand blood-brain barriers
y Rapidperipheraldecarboxylation todopamine
without adecarboxylase inhibitor (DC
Is:carbidopa, benserazide)
y Sideeffects:nausea, posturalhypotension,dyskinesias,
motorfluctuations
-
8/7/2019 Movement Disorders - Overview-1
43/117
Diagram of LD Metabolism
-
8/7/2019 Movement Disorders - Overview-1
44/117
Levodopa-Induced Dyskinesiasy
Manifestationofexcessivedopaminergic
stimulationy Typicallylateeffect, andwithhigherdosesy
Narrowingoftherapeuticwindowy Rarein LD-naivepatientson DA
monotherapyy Most commonis peakdosedyskinesia
disappearswithdosereductiony Choreiform, ballisticanddystonic
movementsy Most patientsprefersomedyskinesiasover the
alternativeofakinesiaandrigidity
-
8/7/2019 Movement Disorders - Overview-1
45/117
Dopamine Agonists: Distinguishing Features
y Directlystimulatedopaminereceptorsy No metabolicconversion;
bypasses
nigrostriatalneuronsy Noabsorptiondelayfrom competitionwith
dietaryaminoacidsy Longerhalf-life thanlevodopay
Monotherapyoradjunct therapyy Maydelayorreduce motorfluctuations
&
dyskinesiasassociatedwithlevodopay Maybeneuroprotective
-
8/7/2019 Movement Disorders - Overview-1
46/117
DAs: Common Adverse Effects
y Nausea, vomitingy Dizziness, posturalhypotensiony Headachey
Dizzinessy Drowsiness & somnolencey Dyskinesiasy Confusion,
hallucinations, paranoiay Erythromelalgia;
pulmonary&retroperitonealfibrosis;pleuraleffusion &
pleuralthickening; Raynaudsphenomena. Maybe
morecommonwithergotoline DAs
-
8/7/2019 Movement Disorders - Overview-1
47/117
Apomorphine
y D1/D2 agonist
y Parenteraldelivery(s.c., i.v., sublingual,
intranasal,rectal)
y Rapid offperiodrescue 2-5 mgs.c.;peninjectionsystems
y Treatment ofunpredictable, frequent motorfluctuations
continuouss.c. infusionvia mini-pumpy SE:nausea, vomiting,
hypotension
trimethobenzamide 250 mg t.i.d.
domperidone 20 mg t.i.d.;not availablein U.S.
-
8/7/2019 Movement Disorders - Overview-1
48/117
-
8/7/2019 Movement Disorders - Overview-1
49/117
-
8/7/2019 Movement Disorders - Overview-1
50/117
Anticholinergics
y Dopaminergic depletion cholinergicoveractivityy
Initiallyusedin the1950sy Effective mainlyfor tremorandrigidityy
Commonagents (Start low, goslow):
y Trihexyphenidyl: 2-15 mg/day
y Benztropine:1-8 mg/dayy Ethopropazine:10-200 mg/day
y Sideeffects: Drymouth, sedation, delirium,confusion,
hallucinations, constipation, urinaryretention
-
8/7/2019 Movement Disorders - Overview-1
51/117
Amantadine
y Antiviralagent; PD benefit foundaccidentallyy Tremor,
bradykinesia, rigidity& dyskinesiasy Exact mechanism
unknown;possibly:
y enhancingreleaseofstoreddopamine
y inhibitingpresynaptic reuptakeofcatecholamines
y dopaminereceptoragonismy NMDAreceptor blockade
y Sideeffectsautonomic, psychiatricy 200-300 mg/day
-
8/7/2019 Movement Disorders - Overview-1
52/117
EarlyManagement of Parkinsons Disease
-
8/7/2019 Movement Disorders - Overview-1
53/117
Initial Therapy: Patient Considerationsy
Riskofacutedrugintolerance
y Riskoflong-term drug-relatedcomplications
yPolypharmacy
y Comorbidities, especiallydementia
y Patientslifestyle, responsibilities
y Cost ofmedications
y Functionalvs. chronologicalage
-
8/7/2019 Movement Disorders - Overview-1
54/117
Initial Therapy: The Elderly Patienty Shorter treatment
horizon
y Lowerriskoflong-term complications
y
Higherlikelihoodofcomorbiditiesy Levodopa:well tolerated,
effective
y Useadjunctive medicationscautiously
y Avoidsedating medications
-
8/7/2019 Movement Disorders - Overview-1
55/117
Initial Therapy: The Young Patient
y Long-term treatment horizon
y Increasedriskoflong-term complications
y
Increasedpatient responsibilitiesy Dopamineagonist
monotherapy
y Levodopa-sparingstrategies
y Putativeneuroprotectivestrategies
y Roleoflevodopaisnot adequatelydefined
:
-
8/7/2019 Movement Disorders - Overview-1
56/117
Complaint?
SymptomsSymptoms Clinical optionClinical option
No functional impairmentNo functional impairment Delay
TherapyDelay Therapy
Mild symptomsMild symptoms Amantadine, SelegilineAmantadine,
Selegiline
TremorTremor AnticholinergicAnticholinergic
DepressionDepression AntidepressantAntidepressant
AnxietyAnxiety AnxiolyticAnxiolytic
Functionally disablingFunctionally disabling
symptomssymptoms
Levodopa, DopamineLevodopa, Dopamine
agonist, COMT inhibitoragonist, COMT inhibitor
-
8/7/2019 Movement Disorders - Overview-1
57/117
Levodopa: Guidelines in Early PD
y Start lowandincreaseslowlyy Titratedosage toefficacy(~200-600
mg/day)y
Immediaterelease-morerapidonset-shorterdurationofbenefit-genericavailabley
Controlledrelease-longerdurationofbenefit-somepatientspreferlessfrequent
dosingy Acutesideeffects:nausea, dizziness, somnolence
-
8/7/2019 Movement Disorders - Overview-1
58/117
Dopamine Agonists: Guidelines in Early PD
y Effectiveas monotherapyy Lesssymptomatic benefit thanlevodopay
Maydelayneedforlevodopaapprox. 12 months
dataup to >3 yearshas beenpresentedy Start
lowandincreaseslowlyy Titrate toefficacy-bromocriptine7.5-30
mg/day-pergolide1.5-4.5 mg/day-pramipexole1.5-4.5 mg/day-ropinirole
3-24 mg/dayy Acute SEs:nausea, dizziness, somnolence, confusion
-
8/7/2019 Movement Disorders - Overview-1
59/117
Dopamine Agonists:Adjunctive Use with L-
dopa
y Bromocriptine, pergolide, pramipexole, ropinirole
y Agonist choiceis moreart thanscience
y Reducelevodopadosagewhenadding theagonist
y Failureofonedoesnot predict failureofanother
y Agonists
maybeswitchedeithergraduallyorrapidlytoacomparabledosage
-
8/7/2019 Movement Disorders - Overview-1
60/117
-
8/7/2019 Movement Disorders - Overview-1
61/117
Managing Early Complications:
AlteredMental States
y Confusion, sedation, dizziness, hallucinations,delusions
y
ReduceoreliminateC
NS-activedrugsoflesserpriorityanticholinergics sedatives
amantadine musclerelaxants
hypnotics urinaryspasmodics
y ReducedosageofDA, COMT inhibitor, or LD
-
8/7/2019 Movement Disorders - Overview-1
62/117
Late Complications
y Motor
-responsefluctuations, dyskinesias, dystonia, freezing,falls
y Behavioral/neuropsychological
-depression, sleepdisorders, psychosis
y Autonomic
-orthostatichypotension;hyperhidrosis, constipation,impotence,
urinaryincontinenceorretention
-
8/7/2019 Movement Disorders - Overview-1
63/117
LD Response Fluctuationsy Peripheralcauses:
-delayedgastricemptying
-dietaryprotein
-short plasmahalf-life
y Centralcauses:
-pulsatiledeliverytostriatalreceptors
-impairedstoragecapacity-alterationofDAreceptors
-
8/7/2019 Movement Disorders - Overview-1
64/117
Response Fluctuations: Treatment
y Increase LD dose
y Increase DCI dose
y
Adddopamineagonisty AddCOMT inhibitor
-reduce LD
-liverfunction monitoring
y Apomorphinerescue
-
8/7/2019 Movement Disorders - Overview-1
65/117
-
8/7/2019 Movement Disorders - Overview-1
66/117
Cognitive Assessment
y Memorydifficulties:11-29%ofPD patients
-Benignforgetfulness
-Delirium
-Alzheimersdisease-Otherdementias
y Evaluation
-Brainimaging
-Lumbarpuncture-EEG
-Bloodworkfor thyroidprofile, vitaminB12,
serology,chemistrypanel
-
8/7/2019 Movement Disorders - Overview-1
67/117
Psychosis
y Features Vividdreams/nightmares,
disorientation,hallucinations, delusional thought
y Simplifymedicalregimen Stopunnecessarynon-PD meds
Stop:anticholinergicdrugs, amantadine,selegiline, dopamineagonists,
COMT inhibitors
y Changefrom CR tostandard
carbidopa/levodopay Tryatypicalantipsychoticagentsy
Trylow-potencytraditionalantipsychotic
agents
-
8/7/2019 Movement Disorders - Overview-1
68/117
Anti-psychotic Agents
y Molindonelow-potencyneuroleptic; mayaggravate PD symptoms, but
cansometimesuse5-10 mgat HS
y Risperidone
D3 antagonist; D1/D2 agonist;aggravates PD at doses > 3
mg/d.y Olanzapine
D4 antagonist. D1/D2 inhibition > 10 mg/dy Quetiapine5-HT1-2
antagonist. Dosage 25 - 500 mg/d
y ClozapineD4 antagonist;noconfirmedaggravationofPD
orcausationofTDFatalagranulocytosisin 9 patients;weeklyCBC
-
8/7/2019 Movement Disorders - Overview-1
69/117
Depression
y Reportedin 30-90%ofPD patients
y Difficult todiscernfrom vegetativesymptoms
y Requiresinquiryintodepressionsymptoms
y Usuallyrespondsquicklyto medications
Tricyclicagents
Selectiveserotoninre-uptakeinhibitors
y
IfEC
T needed, will transientlyimprove PD symptoms
-
8/7/2019 Movement Disorders - Overview-1
70/117
Anxiety/Restlessness
y Primaryanxietydisorder: treat with benzodiazepines
-Associatedwith off-periodsorlow-levodopalevels:
adjust levodopadosingy Restless Leg Syndrome: benzodiazepines,
narcotics,
levodopa, dopamineagonists
-
8/7/2019 Movement Disorders - Overview-1
71/117
Sleep Disorders
y Insomnia
-carefulhistory
-difficultywithsleepinitiation: tricyclicagents,
benzodiazepines, diphenhydramine, chloralhydrate- treat
depression
-REM-behavioraldisorder:clonazepam
y Excessivedaytimesleepiness
-Correct poorsleepat night-Discontinueanticholinergics,
amantadine
-Reducedopamineagonist, levodopadosagesifpossible
-selegeline;caffeine; methylphenidate5-20 mgs/d
-
8/7/2019 Movement Disorders - Overview-1
72/117
Orthostatic Hypotension
y Light-headedness, dizziness, fatigue, shoulderorneckpain,
bloodpressuredropswhenstanding
y Taperanti-hypertensiveagents
y Tapernon-PD drugsy Increasesalt intake
y Compressionstockings
y Fludrocortisone (0.1-0.4 mg/d)
y Midodrine (2.5 - 20 mg/d)
-
8/7/2019 Movement Disorders - Overview-1
73/117
Urinary Incontinence/Frequencyy Ruleout urinarytract
infection
y Bladderevaluationfor
-detrusorhyperactivity
oxybutinin5 -30 mg/d;propanthaline7.5 - 15 mg/d
-detrusorhypoactivity
phenoxybenzamine;prazosin
y
Urinaryfrequency-avoidfluidpoolinginfeet
-DDAVP inhaler; tolterodine tartrate 2mghs to 2mg tid
-
8/7/2019 Movement Disorders - Overview-1
74/117
Sexual Dysfunction
y Medicalscreening
-depression, anxiety, iatrogeniccauses
y
Endocrinologicevaluation-prolactin, testosterone,
lutenizinghormone, thyroidscreen
y Urologicevaluation
-yohimbine, sildenafil
-
8/7/2019 Movement Disorders - Overview-1
75/117
Nausea
y Levodopa-related: takewith meals, addcarbidopa,
adddomperidone
y Otheranti-PD medications:same.
-Ifnoimprovement:withdrawnewest agent, re-initiateat
minimaldoses, slowlyincrease
-
8/7/2019 Movement Disorders - Overview-1
76/117
Excessive Sweating
y Usuallylevodoparelated, and maybeseenat
peakortroughdosedruglevels
-reducelevodopa
-adddopamineagonist orCOMT inhibitor
-addcarbidopa
-addBeta-blocker
The Surgical Treatment of Parkinsons
-
8/7/2019 Movement Disorders - Overview-1
77/117
The Surgical Treatment of Parkinsons
Disease
y Ablative
-thalamotomy
-pallidotomyy Electricalstimulation
-VIM thalamus, globuspallidusinternus, sub-thalamicnucleus
y Transplant-autologousadrenal, humanfetal,
xenotransplants,geneticallyengineered transplants
-
8/7/2019 Movement Disorders - Overview-1
78/117
Deep Brain Stimulation (DBS)
y Highfrequency, pulsatile, bipolarelectricalstimulation
y Stereotacticallyplacedinto target nucleus
y Can beactivatedanddeactivatedwithanexternalmagnet
y Exact physiologyunknown, but higherfrequencies
mimiccellularablation, not stimulation
-
8/7/2019 Movement Disorders - Overview-1
79/117
Adjustable Features
y Voltage (1-7volts)
y Pulsewidth (65-450 msec)
y
Frequency(130-180Hz)y Polarity
y Leadlocation (4 leads, each1.5 mm apart)
-
8/7/2019 Movement Disorders - Overview-1
80/117
-
8/7/2019 Movement Disorders - Overview-1
81/117
Cell Transplants
y Autologousadrenal transplants
-Noefficacy
y Allogenichumanfetal transplants
-Initialencouragingclinicalresults
y Xenogenicfetal transplant (porcineand bovine)
-Preliminaryresultspending
y
Geneticallyengineeredcells-Researchongoing
-
8/7/2019 Movement Disorders - Overview-1
82/117
Human Fetal Transplants
y Efficacy
-Encouragingpreliminaryresultsinyoung PD pts
-PET studiesconsistent withcellfunctioning
-Autopsies (2)showcellsurvival
y Problems
-4-10embryos
-
8/7/2019 Movement Disorders - Overview-1
83/117
Problems That May Respond to
-
8/7/2019 Movement Disorders - Overview-1
84/117
Problems That May Respond to
Nonpharmacological Approaches
y ADL difficultiesy Motor, balance, posture, gait, mobilityy
Speechandswallowing:hypophonia,
sialorrhea, dysphagiay Inadequatenutritiony Sleepdisturbancey
Autonomicdysfunction:painandconstipationy Skin breakdowny
Sexualdysfunctiony Depression
-
8/7/2019 Movement Disorders - Overview-1
85/117
Nonpharmacologic Treatments
y Patient/caregivereducation
y Physical therapy
y Exercise
y Occupational therapy
y Speech/language therapy
y Diet andnutrition
y Psychosocialinterventions
-
8/7/2019 Movement Disorders - Overview-1
86/117
Physical Therapy: Goals
y Maintainorincreaseactivitylevel
y Decreaserigidityand bradykinesia
y
Facilitate movement andflexibility;optimizegaity Maximizegross
motorcoordinationand balance
y Maximizeindependence, safety, function
-
8/7/2019 Movement Disorders - Overview-1
87/117
Physical Therapy: Features
y Exercise:e.g., walking (1+ mile/day), swimming,
golf,dancing
y Stretchingandstrengthening
y Exaggeratedorpatterned movements
y highstepping, weight shifting, repetition, verbalcues
y Mobilityaids, orthotics, adaptivefootwear
y Transfer techniques
-
8/7/2019 Movement Disorders - Overview-1
88/117
-
8/7/2019 Movement Disorders - Overview-1
89/117
Occupational Therapy: Features
y Patient andcaregivereducation
goalsofprogram
transfers, tasksimplification, positioning, etc.y
Homeexerciseprogram
y Homeandworkplace modifications
y Adaptiveequipment
y Upperextremitysplinting
Adaptive Equipment and
-
8/7/2019 Movement Disorders - Overview-1
90/117
Adaptive Equipment and
Environmental Modifications
y Customizefordisability, budgety Seating:wheelchairs, cushions,
lateralsupports,
etc.y Toilet andhygeine: tub/showerseat, grab bars,etc.
y Feeding:wide-handledutensils, sipcups, etc.y Clothing:velcro,
pullovers, shoehorns, etc.y Bed:rails, hospital bed, trapeze, etc.y
Equipment: bookholders, large-buttonphone,
keyholders, etc.y Considerdoorsills, throwrugs,
otherobstructions
-
8/7/2019 Movement Disorders - Overview-1
91/117
Speech and Communication Problems
y Maybeoneofthefirst symptomsofPD
y Characterized by:
-soft voiceandimprecisearticulation
-burstsofrapidspeechalternatingwithperiodsofsilence
-lossofinflection
y Can besignificant foremployment
y Dyskinesias mayworsen
-
8/7/2019 Movement Disorders - Overview-1
92/117
Speech-Language TherapyOptions
y Oftenunderutilized
y Earlytherapyespeciallyeffective
y
At-homeexercises; modificationofdailyactivitiesy
Emphasisoncontrolofrespirationandvoice
production
y Amplificationdevicesrarelyuseful
-
8/7/2019 Movement Disorders - Overview-1
93/117
Techniques to Improve Speech
y Increaseloudness
y Face thelistenerdirectly
y Emphasizekeywords
y Useshort sentences
y Range-of-motionexercisesfor musclesofspeech
y Breathingexercises
y Attendspeech therapy
-
8/7/2019 Movement Disorders - Overview-1
94/117
Nutritional Risk Factors
y Inactivity
y Foodpreparationproblems
y
Dyskinesiaandfeedingproblemsy Chewingandswallowingproblems
y Increased metabolicneeds
y Medication-relateddietaryrestrictions
y Drugsideeffects:anorexia, nausea, vomiting,constipation
y Depressionanddementia
-
8/7/2019 Movement Disorders - Overview-1
95/117
Dietary Recommendations
y Eat a balancediet, includingallfoodgroups
y Consumesufficient calories to maintainweight
y C
onsumeadequatefiberandfluids toavoidconstipation
y Takevitamin D andcalcium toprevent osteoporosis
y Reduceprotein to minimum dailyallowance
-concentrateinevening meal
-
8/7/2019 Movement Disorders - Overview-1
96/117
-
8/7/2019 Movement Disorders - Overview-1
97/117
-
8/7/2019 Movement Disorders - Overview-1
98/117
Miscellaneous Concerns
y Seborrheicdermatitis
-shampoosorlotionswithketoconazole, selenium,pyrithionezinc
y Driving
-assessregularlyforreactionspeed, judgment, mentalstatus
-retakedrivers test
-
8/7/2019 Movement Disorders - Overview-1
99/117
Education, Support and Counseling
y Patient/caregivereducation:newsletters,Webresources
y Support groups:patient, caregivers
-maybeappropriate towait fordisabilityprogression
-early-onset patients maydesireseparategroup
y Counseling
-bothpatient andcaregiver/family;assessneedsseparately
-anxiety, grief, guilt, anger, isolation, depression
-
8/7/2019 Movement Disorders - Overview-1
100/117
Community Resources
y Socialworkerintervention:
Social Securityoffice
Medicare, Medicaidy In-homeprograms
MealsonWheels, homevisiting, etc.
-
8/7/2019 Movement Disorders - Overview-1
101/117
-
8/7/2019 Movement Disorders - Overview-1
102/117
-
8/7/2019 Movement Disorders - Overview-1
103/117
Epidemiologyy Onset is typicallybetween theagesof25and
45years
(range 370years)withaprevalenceoftwo toeightcasesper100,000.
-
8/7/2019 Movement Disorders - Overview-1
104/117
Etiologyy HD iscaused byanincreasein thenumberof
polyglutamine (CAG)repeats (>40)in
thecodingsequenceoftheHuntingtongenelocatedon theshort arm
ofchromosome 4. Thegeneencodes
thehighlyconservedcytoplasmicproteinhuntingtin.
y Intraneuronalinclusionscontainingaggregatesof
ubiquitinand the mutant
proteinhuntingtinarefoundinnucleiofneuronsin thestriatum
andcerebralcortex.
-
8/7/2019 Movement Disorders - Overview-1
105/117
-
8/7/2019 Movement Disorders - Overview-1
106/117
-
8/7/2019 Movement Disorders - Overview-1
107/117
-
8/7/2019 Movement Disorders - Overview-1
108/117
-
8/7/2019 Movement Disorders - Overview-1
109/117
-
8/7/2019 Movement Disorders - Overview-1
110/117
PATHOLOGY AND PATHOGENESISy Impairedglucose metabolism in
thecaudatenucleus,
precedingvisibleatrophy
y excessofdopamine (incontrast to Parkinsondisease)
y disturbancesin the metabolism ofotherneurotransmitters
(norepinephrine, glutamicaciddecarboxylase,
cholineacetyltransferase, GABA,acetylcholine, andsomatostatin)
-
8/7/2019 Movement Disorders - Overview-1
111/117
CLINICAL FEATURESy The
mentaldisorderassumesseveralsubtleformslong
before the moreobviousdeteriorationofcognitivefunctions
becomesevident. Inapproximatelyhalfthe
cases, slight andoftenannoyingalterationsofcharacterare thefirst
toappear. Patients begin tofindfault witheverything,
tocomplainconstantly, and tonagother membersofthefamily
-
8/7/2019 Movement Disorders - Overview-1
112/117
CLINICAL FEATURESy Theabnormality of movement isat first slight
and
most evident in thehandsandface;often thepatient
ismerelyconsidered to befidgety, restless, or "nervous."
Slownessofmovement ofthefingersandhands, areducedrateoffinger
tapping, anddifficultyinperformingasequenceofhand
movementsareearlymotorsigns. Graduallytheseabnormalities
becomemorepronounceduntil theentire musculatureis
implicatedwithchorea.
-
8/7/2019 Movement Disorders - Overview-1
113/117
Diagnosisy It isnowpossible toconfirm orexclude thediagnosis
byanalysisofDNAfrom a bloodsample. Thepresenceofgreater than 39
to 42 CAG repeatsat theHuntington
locusessentiallyconfirmsitspresence
-
8/7/2019 Movement Disorders - Overview-1
114/117
Huntington's Disease: Treatmenty Treatment involvesa
multidisciplinaryapproachwith
medical, neuropsychiatric, social,
andgeneticcounselingforpatientsand theirfamilies
-
8/7/2019 Movement Disorders - Overview-1
115/117
Huntington's Disease: Treatmenty Dopamine-blockingagents
maycontrol thechorea but
aregenerallynot recommended becauseoftheirside-effect
profileandpotential toaggravate motor
symptoms, and because thechorea tends to
beself-limitedandisusuallynot disabling.
-
8/7/2019 Movement Disorders - Overview-1
116/117
Huntington's Disease: Treatmenty Depressionandanxietycan
begreaterproblems, and
patientsshould be treatedwithappropriateantidepressant
andantianxietydrugsand monitored
for maniaandsuicidalideations.y Psychosiscan be
treatedwithatypicalneuroleptics
suchasclozapine (50600 mg/d), quetiapine (50600mg/d),
andrisperidone (28 mg/d)
-
8/7/2019 Movement Disorders - Overview-1
117/117
Huntington's Disease: Treatmenty Thereisnoadequate treatment for
thecognitiveor
motordecline. Aneuroprotective therapythat
slowsorstopsdiseaseprogressionis the majorunmet medical
needinHD. Antiglutamateagents, bioenergetics,caspaseinhibitors,
inhibitorsofproteinaggregation,intracerebraldeliveryofneurotrophicfactors,
andtransplantationoffetalstriatalcellsareallareasofactiveresearch,
but nonehasasyet been
demonstrated tohaveadisease-modifyingeffect.