Embed Size (px)
Citation preview

Supporting Residents Expressing Responsive Behaviours
at Home, Hospital, and LTC HNHB LHIN Behavioural Supports Ontario Strategy
Family Council Network Four (FCN-4) Regional Meeting June 29, 2017

Objectives • Background on BSO Strategy in HNHB LHIN and client
population • Discuss how BSO models support individuals across
care settings • Share case stories from the Team • Review how BSO Strategy is building LTC Champions • Share program data • Q & A
Source: BSO Kick off Presentation August 2011
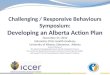
BSO Provincial Framework
Goals: Quality of Care & Quality of Life
Older people (& their caregivers) with cognitive impairments due to
mental health problems, addictions, dementia, or other neurological conditions that
exhibit, or are at risk of exhibiting, responsive
behaviours

Seniors with dementia are intensive users of health-care resources
People with dementia are: – Twice as likely to be hospitalized compared to seniors without
the disease – Twice as likely to visit emergency departments for potentially
preventable conditions – More than twice as likely to have alternate level of care days
when hospitalized – Nearly three times more likely to experience fall-related
emergency room visits Gill, et al. (2011). Health System Use by Frail Ontario Seniors. Institute for Clinical Evaluative Sciences.

Dementia • Dementia is an umbrella term for many brain disorders. Changes in a
person’s behaviour can be an indicator. • Dementia affects everyone differently, but it commonly diminishes
these abilities: • Language • Recognition • Memory (including knowledge of the disease) • Purposeful movement • Sensory perception • Reasoning
The Dementia Experience • We cannot understand the experience of a
person with dementia, but what we do know is that it can cause changes in memory, judgement, attention, mood, communication and language, and can significantly interfere with the person’s ability to do the things that matter to them and bring their life meaning

Normal Aging
Dementia
Presence of
Responsive Behaviours

What do Responsive Behaviours look like?
Verbally Responsive
Verbal Mutterings Swearing
Sounds that are Disruptive to Others
Throwing Objects Hurting Others
Disrobing
Verbal Complaints Physically responsive
Hurting Self
Hitting
Repetitive Sentences
Repetitive Behaviour Constant Requests for Attention
Agitation
Pacing
Wandering
Behaviours Have Meaning
Hiding Objects
Accusing

What do Responsive Behaviours often indicate?
a) an unmet need in a person, whether cognitive, physical, emotional, social, environmental or other
b) a response to circumstances within the social or physical environment that may be frustrating, frightening or confusing to a person.
Behaviours Have Meaning
• The most common trigger for the onset of responsive behaviours in anyone with a cognitive impairment is change in environment, including staff changes.
• As such, how Transitions are managed is essential to the quality of care and outcomes for individuals with cognitive impairment.
Margallo-Lana, M., Swann, A., O'Brien, J., Fairbairn, A., Reichelt, K., Potkins, D., … & Ballard, C. (2001). Prevalence and pharmacological management of behavioural and psychological symptoms amongst dementia sufferers living in care environments. International Journal of Geriatric Psychiatry, 16, 39–44. doi: 10.1002/1099-1166(200101)16:1<39::AID-GPS269>3.0.CO;2-F
Dementia and its link to Responsive Behaviours

Journey across the BSO continuum of care
BSO Connect
Community Outreach
Transitional Leads
LTC Mobile
Hospital Clinical Leads

Background of Funding • MOHLTC news release on August
18, 2016 announcing $10 million in new annual funding for Behavioural Supports Ontario
• The HNHB LHIN allocation is ≈ $1.1 M: – Long-Term Care: 0.7 M – Community/Hospital Sector: $0.3 M – Stabilization Funding (existing
resources): $0.1 M

HNHB LHIN Geographical Region
2 COT workers
2 COT workers
4 COT workers
3 COT workers
1 COT worker
BSO Funded Positions: 55 LTC Mobile Staff and Managers
13 COT staff and Manager 1 RH Responsive Behaviour Specialist
1 Connect staff 4 Clinical Leaders (serving 17 hospital sites)
1 Coordinator 1 Strategic Lead 2 Clinical Leaders
1 Clinical Leader
1 Clinical Leader
1RH RB Specialist
BSO Connect – Program Objectives • To provide a singular point of
entry for clients, caregivers, and providers to access services
• To ‘warmly connect’ clients to services
• To complete the feedback loop so clients do not ‘fall through cracks’
• Within I&R Department at HNHB LHIN
15

BSO Community Outreach Team – Program Objectives
• Provide ‘just in time’ care for clients and their families in community
• Educate caregivers (formal and informal) on triggers of behaviour and associated coping strategies
• Reduce inappropriate emergency visits
• Improve capacity within the host mental health mobile outreach teams
16

BSO LTC Transitional Leads– Program Objectives
• Supports future residents on “crisis list” in community and at “high risk” for a challenging transition into LTC
• Work with Community, Primary & Specialty care providers to stabilize individual as they wait for LTC bed offer
• Pre-admission meetings with LTC Homes and provide a Transitional Care Plan
• Support resident and LTC home staff well past admission 17
Transitional Care Plan developed and shared
with LTC Homes
Transitional Lead works with community , primary care, and
specialist care providers

BSO LTC Transitional Leads– In action
• Case study example
18

BSO LTC Mobile Team- Program Objectives Collaborating with LTC • Provide behaviour assessment • Identify triggers and strategies • Coach and model with staff Supporting Transitions & Episodic • Provision of transitional support to/from LTC for low to moderate risk transitions • Provision of episodic support as needed

BSO LTC Mobile Team– In action
• Case study example
20

BSO Clinical Leaders – Program Objectives • Consult with hospital inpatients who have
cognitive impairment and responsive behaviours
• Collaborate with the patient/family and the hospital team to: • Understand the triggers of the responsive
behaviours and develop personalized strategies to manage
• Share information between hospital, LTC and community to develop plans
• Educate hospital staff on population and their unique care needs

BSO Hospital Clinical Leads– In action
• Case study example
22
How BSO Teams work together • Community, LTC and Hospital teams coming together in
news ways • Educational opportunities for shared learning • Team meetings provide opportunity for creative problem
solving Goal is to ensure the BSO client’s ‘story’ and effective
behaviour strategies follow along with them on their healthcare journey

How do BSO Teams collaborate with LTC Homes • All BSO LTC programs collaborate regularly through
formal and informal ways – Coaching and modelling in peer to peer model – Shift Huddles on the unit – Responsive Behaviour (or similar) committees – Leadership/Management attend LHIN-LTC meetings – BSO Transitional lead program was developed with LTC
stakeholders – BSO Transitional Lead Oversight Committee

How is BSO Strategy building knowledgeable care teams?
• Unused BSO funds are directed toward education and training
• Since BSO began, LTC staff have been offered numerous education sessions to improve their knowledge and skills

BSO Enhanced Funding: Education Plan 2016-17
August 2016: Enhanced BSO
funding announced
January to March 2017: New positions
filled
Stakeholder consultation,
development & recruitment
Unspent staffing dollars allocated for education to support the BSO population.
Must be spent by March 31st, 2017

A multi-faceted approach to educating our teams and colleagues across sectors
Community Hospital Long-Term Care • Appointment of 1-2 Behavioural
Champions within LTCHs • 5 days’ training offered to
Leads • Opportunities to send additional
team members to training sessions
• Two full-day sessions targeted to front-line care providers
• Opportunities to send additional team members to training sessions
• Training of Mental Health First Aid for Seniors Coaches
• Four P.I.E.C.E.S. sessions planned in hospitals LHIN-wide
• U-First available for PSWs and Aides
BSO Staff • 5 day Mental Health Recovery Care Program • 1 day collaborative learning event for staff members from all BSO teams, PRCs and ICMs • Standardized patient experiential learning sessions
CORE
COM
PETE
NCIE
S

Report on Education Plan 2016-17 • A total of 63 education sessions delivered after funding announcement (a
total of 1150 participants: LTC and Community) • 773 LTC Sector RNs, RPNs, PSWs & Allied Health attended training (not unique number as some attended more than one training session) • 87% of LTCHs (75/86) assigned 1 to 2 Behavioural Leads/Champions for a
total of 120 unique staff • PIECES, Montessori Methods, Pain Assessment training, GPA, U-First, and
other sessions devoted to supporting residents with responsive behaviours

LTC Behavioural Leads/Champions
• A Community of Practice will be one method to keep the training alive for LTC Behavioural Champions
• 87% of LTCHs (75/86) assigned 1 to 2 Behavioural Leads/Champions for a total of 120 unique staff

Sustainability • LTCH leadership have been informed of their responsibilities re:
Behavioural Champions(s); Behavioural Champions are aware of the expectations in role
• A Community of Practice will be formed based upon the Provincial BSO Knowledge to Practice Process Framework. Members will include: – Behavioural Champions/Leads – PRCs – Geriatric Outreach Teams – BSO Transitional Leads – BSO LTC Mobile Team members – BSO Clinical Leaders – BSO Responsive Behaviour Specialist (Retirement Homes)

BSO Program Data: Long-Term Care Mobile Team
• # of family members supported: – July-September 2016 : 631 – October-December 2016: 471 – January-March 2017: 375
“The external team provides a great resource to the Home as the Mobile Team are dedicated to what they do, and are well trained and versed in managing and responding to behaviours.” – Laura, RN, Parkview Nursing Centre, Hamilton


BSO Program Data: Hospital Clinical Leader Program
“[The BSO Clinical Leader] worked to know Edward as a human being – his background, interests, and needs – the whole process was so well done. [Her] involvement has made a phenomenal difference.” - Beatrice, Spouse of patient served by BSO Clinical Leader
Between April 2016 – March 2017: • 21 patients were diverted from
more highly-resourced care settings and safely discharged to lesser resourced settings.
• 607 hospital staff received formal education about supporting patients who are BSO clients

BSO Program Data: Hospital Clinical Leader Program
Total of all HNHB LHIN Hospital Sites
2014-15 (Pre- BSO Clinical Leader Program)
2015-16 ( 1 Year Post-BSO
Clinical Leader Program
Implementation)
2016-17 (2 Years Post- BSO Clinical
Leader Program Implementation)
Average number of ALC days per patient with behaviours
46.2 days
31.2 days (↓32.5%)
22.8 days (↓26.9%)

Opportunities for Collaboration with Family Councils
• Residents and their families are at the centre of what we do!
• Let’s work together: – Education to Family Councils – Shared brainstorming on how to best
support residents and families

QUESTIONS
“ I am who I am, so help me continue to be me”

Feedback from LTC providers • “Over time I have seen BSO staff being increasingly collaborative offering
compliments and suggestions re: ways to enhance the brain storming and success of behaviour strategies.”
• “They are very supportive, flexible and they sit on some of our committees. They are a valuable part of our team.”
• “The RPN who attends our home is great and realistic”
• “Long term care mobile team is extremely helpful for the hospital. Communicate well with the team and give some great suggestions to manage behaviour”