Embed Size (px)
Citation preview

1
RESPONSIVE BEHAVIOURSDRIVEN BY MEDICATION:
IMPROVING DEMENTIA CARETHROUGH RMMRS
Dr Andrew Stafford PhD
Director
Saturday 29th June 2019
2
Today’s presentation
Learning outcomes
By the end of this presentation you should be able to:• Describe the symptoms of responsive
behaviour • Discuss the role of medication in
contributing to responsive behaviour
Contents
• Prevalence and characteristics of responsive behaviours
• Case studies
In relation to this presentation, I declare that I have no real or perceived conflicts of interest.
1
2

3
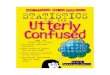
Dementia prevalence in Australia
doi:10.1093/gerona/glz032
0
10
20
30
40
50
60
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Home Care (n = 188,846) Long-term Aged Care (n = 348,311)
4
Responsive behaviour
• Changed behaviours exhibited by people with dementia living in long-term care are often referred to as behavioural and psychological symptoms of dementia (BPSD)
• Behavioural symptoms: e.g. physical aggression, screaming, restlessness, agitation, wandering, culturally inappropriate behaviours, sexual disinhibition, hoarding, cursing and shadowing.
• Psychological symptoms: e.g. anxiety, depressive mood, hallucinations and delusions
• Highly prevalent among people with dementia living in long-term care• Apathy (49%)• Depression (42%)• Agitation/aggression (40%)• Anxiety (39%)• Sleep disorders (39%)
Drugs & Aging 2019 36:125–136
3
4

5
Outcomes of responsive behaviour
• Source of significant distress and poor quality of life to both people living with dementia and their caregivers
• Negatively correlated with survival rates and acceleration of cognitive decline
• Medications widely utilised in managing responsive behaviour
• Limited effectiveness• Considerable risk of serious adverse
outcomes, even if only used for a short period of time
Front Neurol. 2012; 3: 73
6
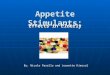
Outcomes of antipsychotic use in dementia
DOI: 10.1002/14651858.CD003476.pub2
If 1000 people were treated with an antipsychotic for 12 weeks:
91-200PEOPLE SHOW CLINICALLY SIGNIFICANT IMPROVEMENTS
10 ADDITIONAL DEATHS
18ADDITIONAL CEREBROVASCULAR EVENTS
58-94PEOPLE WITH DISTURBED GAIT
5
6

7
8
Approaches to managing responsive behaviour
Managing Behavioural and Psychological Symptoms of Dementia (BPSD) A Clinician’s Field Guide to Good Practice. 2014: UNSW
• Comprehensively assess, address potential underlying causes
• Introduce psychosocial methods, attend to environmental contributors (unless severe distress/ risk of harm)
• Involve all carers in the management plan
• Individually tailor interventions to the person. Identify the person behind the behaviour
• Monitor symptoms and review for a suitable period before considering pharmacological therapy
• Where pharmacological therapy is indicated, obtain informed consent
• Dosage should start low and go slow. Trial dose reduction after an appropriate period, e.g. three months
• Monitor for adverse events, as these can also present as BPSD
• Review and reassess BPSD symptoms and therapy regularly
7
8

9
Models for understanding behaviour
Biomedical model• Pathological changes to the brain in
dementia impair normal brain functions and cause behavioural symptoms
• Behaviours of concern are a part of dementia
ReBOC - Reducing Behaviours Of Concern. 2012; Adelaide, South Australia: Alzheimerís Australia SA Inc
10
Models for understanding behaviour (cont)
Unmet needs• A person may exhibit behaviours when
their needs are not met • Maslow’s hierarchy of needs is one way
of conceptualising the priority of needs, with the needs fundamental to survival being the foundation for higher order needs
ReBOC - Reducing Behaviours Of Concern. 2012; Adelaide, South Australia: Alzheimerís Australia SA Inc
9
10

11
Models for understanding behaviour (cont)
ABC model (antecedents, behaviour, consequences)• Focuses on triggers (antecedents) that
precede behaviours, with the subsequent consequences reinforcing the behaviour
ReBOC - Reducing Behaviours Of Concern. 2012; Adelaide, South Australia: Alzheimerís Australia SA Inc
12
Models for understanding behaviour (cont)
Progressively lowered stress threshold• Dementia lowers a person’s ability to
deal with daily stress and increases the susceptibility to environmental stressors.
• Accumulated stressors such as noise, temperature and light can contribute to behaviours
ReBOC - Reducing Behaviours Of Concern. 2012; Adelaide, South Australia: Alzheimerís Australia SA Inc
11
12

13
Case 1
• 78 yo man, 94kg• PMHx
• Alzheimer’s disease• Congenital deafness (rubella); has a
cochlear implant • Depression• Hypothyroidism• Osteoarthritis (back)• Squamous cell carcinoma (nose)
• Medication profile• Donepezil 10mg in the morning• Kenacomb® ointment twice daily to nose• Mirtazapine 45mg at night• Thyroxine 75microg in the morning• Paracetamol 1g twice daily
• Reviewed in December 2018• Recent change in behaviour; antipsychotic
treatment being considered
14
Case I – continued
• Historically always “pleasantly confused”• Over recent months significant increase in appetite
• Demanding more food at mealtimes, taking food from others’ plates• Persistent food seeking behaviour, particularly at night• Occasional episodes of pica• 10kg weight gain in previous two months
• Poor response to diversional strategies• Mirtazapine dose increased for several weeks to exclude depression as a potential
cause• No benefit, if anything the behaviour worsened
• GP considering commencing antipsychotic treatment to stop intrusive behaviour
13
14

15
Hyperphagia in Alzheimer’s disease
• Between a third and a half of people living with Alzheimer’s disease experience appetite changes
• Decreased appetite or anorexia most common• May occur at any stage of the condition, more common in latter stages
• Hyperphagia clinically manifests as an increase in food intake, active searching for food between meals, and loss of satiety
• May occur in isolation or with other behaviours, e.g. Klüver–Bucy syndrome (bilateral medial temporal lobe lesions)
• Associated with several adverse outcomes• Upper airway obstruction in the presence of dysphagia• Nutritional imbalance• Accidental poisoning because of judgement problems• Fall risk while searching for food at night• Aggression due to conflict with carers
Psychogeriatrics 2018; 18: 243–251
16
Hyperphagia in Alzheimer’s disease - management
• Medication is rarely implicated in causing/ exacerbating hyperphagia• Case report of dexamethasone, symptoms resolved upon its cessation• Appetite stimulants (e.g. mirtazapine, cyproheptadine) may exacerbate this behaviour and
should be reviewed
• Some evidence that topiramate alleviates hyperphagia associated with frontotemporal dementia
• Minimal role for antipsychotic treatment
• Non-pharmacological interventions preferred• Spaced retrieval training +/- Montessori activities potentially effective
Psychogeriatrics 2018; 18: 243–251. J Clin Nurs 2016; 26(20):3224–31
15
16

17
Case 1
• 78 yo man, 94kg• PMHx
• Alzheimer’s disease• Congenital deafness (rubella); has a
cochlear implant • Depression• Hypothyroidism• Osteoarthritis (back)• Squamous cell carcinoma (nose)
• Medication profile• Donepezil 10mg in the morning• Kenacomb® ointment twice daily to nose• Mirtazapine 45mg at night• Thyroxine 75microg in the morning• Paracetamol 1g twice daily
• Reviewed in December 2018• Recent change in behaviour; antipsychotic
treatment being considered
18
Case 2
• 93 yo man, 67kg• PMHx
• Alzheimer’s disease• Atrial fibrillation (AVR 2003)• Cataracts (bilateral, with IOLs)• GI bleed (2018)• Hypertension• Hiatus hernia• IHD (MI, CABG)• OA left knee• Prostate cancer (metastatic)• Type 2 diabetes
• Medication profile• Colecalciferol 25microg in the morning• Docusate/ senna 100/16mg twice daily• Enzalutamide 160mg in the morning• Leuprorelin 22.5mg every three months• Macrogol 13.12g two twice daily• Metoprolol 12.5mg twice daily• Pantoprazole 40mg twice daily• Paracetamol 500mg when required
• Reviewed in March 2019• Rapid decline, opinion on deprescribing
17
18

19
Case 2 - continued
• Hospitalised late 2018 with severe constipation• Found to have bone and liver metastases
• Administered zoledronic acid• Commenced on intensified laxative regimen• Anti-androgen therapy changed from bicalutamide to enzalutamide, leuprorelin maintained
• Significant decrease in functional ability and cognition following discharge• No longer able to dress or feed himself• Very confused, apathetic, minimally engaged with facility staff or family• GP considered that this change was most likely due to progression of overall frailty (prostate
cancer, dementia etc)
20
Enzalutamide
• An oral androgen-receptor inhibitor • Shown to significantly increase progression-free survival in castration-resistant
prostate cancer • Chemotherapy-naïve patients (PREVAIL study)• Previous treatment with docetaxel-based chemotherapy (AFFIRM study)
• Fatigue (39.1%), nausea (22.7%), and anorexia (14.8%) were the most commonly reported adverse effects in these trials
doi.org/10.2147/TCRM.S57509
19
20

21
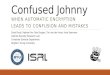
Enzalutamide and memory impairment
AMH 2019. Immunomodulators and antineoplastics / Hormonal antineoplastic drugs / Anti-androgens / Enzalutamide
22
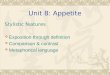
Enzalutamide and memory impairment
Prostate 2015; 75:836–844.
21
22

23
Key messages
• Responsive behaviours are a major cause of the morbidity and mortality associated with dementia
• Evaluation is crucial in developing an appropriate management plan for responsive behaviours
• Medications may cause or contribute to some responsive behaviours• A medication review may identify potentially reversible causes of some behaviours• Both common and uncommon adverse effects may adversely influence behaviour
23