Embed Size (px)
Citation preview

SUMMER EDITION AUGUST 2016
From ASCLS-IL!
Inside this issue: PRESIDENT’S 1 LETTER ASCLS VOICES 2 UNDER 40 2016 3-8 GRADUATES STUDENT 9-12 FORUM ARTICLES LRN ARTICLE 13-15 ASCLS 16-21 ANNUAL MEETING LABORATORY 22 CAREERS INFO FOR 23 PUBLICATION
ASCLS-IL
Insights LETTER FROM THE PRESIDENT MASIH SHOKRANI, PH.D. MT(ASCP)
“Moving ASCLS-IL Forward”
I am honored and excited to start my new position as the President of ASCLS-
IL. As someone who has worked on the bench as clinical laboratory scientist
(medical technologist) and now as an educator, I hope that I can bring various
aspects of the clinical lab together for a common cause.
The following objectives
are on my agenda as
President of the State
Society for this year:
● Increase membership. One way to achieve this objective will be to attract
more young professionals and recent graduates to join our state society and
to retain the current members.
● Increase engagement with the state and national
society. One way to achieve this objective would be to increase
attendance at the state and national meetings by making attendance to such meetings more affordable.
● Increase communication and collaboration between
laboratory professionals and educators. One way to achieve this objective
would be to take advantage of resources that are available to our
state society.
I understand that within my limited time as President, not all the objectives can be fully achieved, however, somewhere and sometimes we need to try. I just came back from a wonderful Annual Meeting of ASCLS which was held this year in Philadelphia and witnessed how much can be achieved when we commit ourselves responsibly to a common cause. I guess I could say, it is not too early to plan for next year’s Annual Meeting of ASCLS-IL that will be held in Peoria next April or for the ASCLS Annual Meeting in San Diego next summer. I would like to encourage everyone to attend at least one of these meetings next year.
The key to all of the above and more is
communication and to keep the lines of communication open. If
you have ideas to share with the laboratory professionals, please do
not hesitate to contact me and I will make sure to place it in ASCLS-IL
Insights. That’s why I have called to have a retreat next month in
Starved Rock State Park to brainstorm ideas for future plans. If any of you
are interested in attending that retreat or if you have ideas that you would like
to be discussed in that retreat, please do not hesitate to contact me. I
can be reached at [email protected]

PAGE 2 SUMMER 2016
ASCLS VOICES UNDER 40
Nicholas Moore, the President-Elect of ASCLS-IL, was recently honored as one of the inaugural recipients of the ASCLS Voices Under 40. This newest recognition program was developed by ASCLS to honor members who have shown exceptional commitment to ASCLS, the laboratory profession, and their community at a young age in their professional career. Candidates were selected based on their contributions to the profession as well as two professional references. Maribeth Flaws, ASCLS-IL President in 2013-2014, and Suzanne Zanto, ASCLS President in 2014-2015, supported Nicholas' nomination. Recipients were selected from their peers based on exemplifying commitment to the laboratory profession in the mid-point of their careers. Recipients were notified in late June, and received the award at the 84th ASCLS Annual Meeting in Philadelphia, PA. Outgoing ASCLS-IL President, Sheila Gibbons accepted the award on Nick’s behalf. Only 12 recipients were selected based on the rankings of their peers, the supporting nominations, and personal statement from each nominee. The 12 recipients will be featured in monthly spotlights by ASCLS during 2016-2017.
ASCLS-IL Board of Directors Officers President: Masih Shokrani President-Elect: Nick Moore Past- President: Sheila Gibbons Executive Secretary: Gilma Roncancio-Weemer Recording Secretary (2016-2018): Kate Bernhardt Treasurer (2015-2017): Amy Liu Board Member (2015-2017): Cheryl Hanson Board Member (2016-2018): Rebecca Gayeski

SUMMER 2016 PAGE 3
2016 GRADUATES: WELCOME TO THE PROFESSION FROM ASCLS-IL!
KANKAKEE COMMUNITY COLLEGE:
From left- to-right: Christy Favre, Julie Perry, Dominique Hammer,
Michelle Zborek, Randa Al-Talla, Jessica Kane, Stephanie Caldwell
ELGIN COMMUNITY COLLEGE:
From left-to-right: Heather Creegan, Victoria Weir, Kunal Patel, Estefania Illescas, Ann Ayers, Hemangi Patel

SUMMER 2016 PAGE 4
2016 GRADUATES: WELCOME TO THE PROFESSION FROM ASCLS-IL! CONT.
ILLINOIS CENTRAL COLLEGE:
From left-to-right: Anh Strow (Program Director,) Margaret Schwab,
Tyler Barlow, Melanie Paden, Michelle Colloton, Alyssa Harms,
Brandon Birdsell, and Brittany Eyster
SAINT JOHN’S HOSPITAL:
From left- to- right: Emily Springer, Paige Milhauser, Katie Golab,
Ali Zachman, Tori Baragiola, and Amy Kraning

VA HINES HOSPITAL:
SUMMER 2016 PAGE 5
Front, left- to- right: Nikita Patel Sue In Andrew Busch Ralica Raytchev Sydney Alonzo Florence DelCarlo Middle, left- to- right: Mireya Scheer Sammi Yerkes Donna Wray Nancy Fabbrini Brandy Kenny Nora Venckute Tricia Kessell Back, left- to- right: Michael Smalara Jordan Lopas Erik Blackowicz
2016 GRADUATES: WELCOME TO THE PROFESSION FROM ASCLS-IL! CONT.
OSF SAINT FRANCIS MEDICAL CENTER
From left-to-right: Marie Deter Keirston Creek Jacquelyn Lynn Kendra Hart Taylor Jacobs Suzanne Messer

SUMMER 2016 PAGE 6
2016 GRADUATES: WELCOME TO THE PROFESSION FROM ASCLS-IL! CONT.
NORTHSHORE UNIVERSITY HEALTH SYSTEM:
UNIVERSITY OF ILLINOIS AT SPRINGFIELD (no picture available)
Chuanyi Chu Jennifer Esquivel Alec Frazier Miranda Gorsuch Katie Grider Kylee Higgason Meryem Husen Magdalena Kurdi Colleen Kyle Ross Leclair Ashley Levickas Ryan Philyaw

SUMMER 2016 PAGE 7
2016 GRADUATES: WELCOME TO THE PROFESSION FROM ASCLS-IL! CONT.
ILLINOIS STATE UNIVERSITY (no picture available):
RUSH UNIVERSITY: Bachelor of Science in Medical Laboratory Science
December 2015 Jae Butler May 2016 Nimo Ahmed Jazmine Allen Sara Bartnick Laura Brazdziunaite Kiersten Cafcules Jason Clark Jessica Clary Colleen Gregory Yussuf Ibrahim Ahmed Jama Elona Joanidhi Haji Karshe Breanne Koszewski Kwan Lam Orlando Lara Muse Mohamed Munia Mustafa Alexa Neri Jacob Ngeno Amanuel Ogubagbir Angela Peterson Jeffrey Ramones Johanna Rutledge Michele Sabor Jon Shiroishi Chris Skelly Jacob Timms Brian Wambold Kelsey Young
From left- to- right, Front row : Sheida Behzadi-Teshnizi, Elsa Quintero, Jennifer Viteri, Lananh Pham
From left- to- right, Middle row : Hoai Nguyen, Alaa Halloon
From left- to- right, Back row : Laurel Meyers, Evgenia Barysheva, Marissa Gibson
Not pictured: Keyuri Patel, Patrycja Czarna

RUSH UNIVERSITY: Master of Science in Medical Laboratory Science
SUMMER 2016
2016 GRADUATES: WELCOME TO THE PROFESSION FROM ASCLS-IL! CONT.
NORTHERN ILLINOIS UNIVERSITY:
From left- to- right, Front row:
Nerjes Alsalman, Elaina
Analitis, Celine Fausto,
Kristi Mosher, Marie
Mohrbacher
From left- to- right, Middle
row: Courtney Booker, Michael
Conciatori, Juan Elias, Julia
Dale
From left- to- right, Back row :
Heidi Christian, Emily
Wysocki, Christina Dallas
From left- to- right: Emily Mackley, Kimberli Chrzan, Michele Burke, Michaela Dean, Heather Struthers,
Bailey Filbin, Peter Albright, Brooke Bausman, Natalie Davison, Katie Perkins, Caleb Bardy, Richard Keith,
Paige Elder, Nathan Sharp, Jennifer Wear, Merlyn Diaz, Katy Kirby, Deidra Hong, Jamie Phan, Reem
Alamoudi, Gina Pirroli, Gabriela Ortiz, Emily Piper, Linda Cassel, Melissa Watts, Amir Toghraee.
PAGE 8

THE SOUR TRUTH ABOUT LYME DISEASE
By: Reilly Steidle, Chair of ASCLS-IL Student Forum
Lyme disease (LD) is the number one reported vector borne illness in the United States1. LD is bacterial in
nature and generally caused by a spirochete called Borrelia burgdorferi but can also be caused by Borrelia
mayonii 2. B. burgdorferi has five known subspecies and over 100 strains in the US3, which makes these
bacteria difficult to remove from the body. LD is spread by being bit by an infected blacklegged tick (lxodes
scapularis or lxodes pacificus on the Pacific Coast). Ticks can attach to any part of a person or animal’s
body, but in humans, ticks are often found in hard-to-see areas such as the groin, armpits, and scalp. Immature
ticks are referred to as nymphs and often infect humans because they are very small (less than 2mm) and
therefore difficult to see. In a large majority of cases, the tick must be attached for 36 to 48 hours or more
before the bacteria that causes LD can be transmitted1.
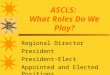
Cases of LD are growing exponentially and mostly being reported in the northeast and upper Midwestern United States. In 2008, 108 cases were reported to the Center for Disease Control (CDC) in Illinois alone, but in 2013 that number climbed to 337 cases1. Only 30,000 of the approximately 300,000 confirmed cases of LD are being reported to the CDC each year. The CDC has estimated that 25,000 people in the US become infected with LD every month and in 2014, 96% of confirmed cases were reported from 14 states1.
Fig. 1: Number of reported LD cases and how the disease has spread geographically in the US over 10 years1. The
figureon the left represents cases of LD reported to the CDC by county in 2004 and the figure on the right shows CDC
reported LD cases by county in 2014
Currently, the early symptoms of LD are recognized by a tick bite followed by the “bull’s eye”, Erythema
migrans (EM) rash. Other early symptoms occur within days of the bite and include: fever, chills, headache,
fatigue, muscle and joint aches, and swollen lymph nodes. If the patient is not treated, the symptoms may
advance to: severe headaches and neck stiffness, additional EM rashes on other areas of the body, arthritis with
severe joint pain and swelling (particularly the knees and other large joints), facial or Bell's palsy (loss of
muscle tone or droop on one or both sides of the face), intermittent pain in tendons, muscles, joints, and bones,
heart palpitations or an irregular heart beat (Lyme carditis), episodes of dizziness or shortness of breath,
inflammation of the brain and spinal cord, shooting pains, numbness, or tingling in the hands or feet, and
problems with short-term memory1. LD can be hard to recognize in the early stages because fewer than 50%
SUMMER 2016 PAGE 9

THE SOUR TRUTH ABOUT LYME DISEASE,CONT.
of patients with LD recall a tick bite or rash3. As many as 40% of LD patients end up with long term health
complications because the average patient sees over 5 doctors in nearly 2 years before receiving the proper
diagnosis and treatment3. Doxycycline, amoxicillin, or cefuroxime axetil are the most commonly used
antibiotics to treat LD. Patients with certain neurological or cardiac forms of the illness may require
intravenous treatment with drugs such as ceftriaxone or penicillin. The duration of the antibiotic therapy is
determined by the patient’s doctor1.
Table 13: Current two tier testing method sensitivity research data. ELISA is performed, and then confirmedby
Western blot. LD offers several complications in diagnosis and treatment. Diagnosis is complicated because without a
known tick bite or EM rash present, the patient or the physician may not recognize the symptoms as those of
LD. Testing is also difficult because LD can only be confirmed by two different lab tests that measure the
infection indirectly. This means the tests measure the patient's antibody response to the infection, not the
infection itself4. The common enzyme-linked immunosorbent assay (ELISA) test misses 35% of culture
proven LD and some studies indicate up to 50% of the patients receive false negative results3. This could be
due to the numerous strains of B. burgdorferi and lack of test sensitivity to each type. The CDC requires a
Western blot test be done as a confirmatory test for LD if the ELISA is positive. The Western blot for LD is
highly specific, so there are few false positives. However, the screening test (ELISA) is highly insensitive
and fails to accurately identify all of the patients who have LD. Research has shown that the two-tiered test
system misses roughly 54% of patients4. Evaluations of these methods can be seen in Table 1. The CDC
states that the Western blot test results have to have 5 out of 10 bands present to be positive for B.
burgdorferi antigens. Patients may display all the clinical symptoms of LD with less than 5 bands being
present, and what is considered a positive test varies across labs in the US4 because they do not all abide by
CDC guidelines. Also, there is not a test to prove that a patient’s body is fully rid of the bacteria, which
complicates deciding if the treatment was sufficient. Short treatment courses and delayed treatments have
approximately a 40% relapse rate because the spirochete is not fully out of the patient’s body3. Relapse is a
hallmark of what the CDC calls Post Treatment Lyme Disease Syndrome (PTLDS). PTLDS is a collection of
Sensitivity/Specificity of commercial two tier testing for convalescent/late stage Lyme disease in the US*
Study/Year Patients/Controls Sensitivity Specificity
Schmitz (1993) 25/28 66% 100%
Engstrom (1995) 55/159† 55% 96%
Ledue (1996) 41/53 44% 100%
Tilton (1997) 23/23 45% 100%
Trevejo (1999) 74/38 29% 100%
Bacon (2003) 106/559 67% 99%
Binnicker (2008) 35/5 49% 100%
Steere (2008) 76/86†† 18% 99%
TOTAL 435/951 46% 99%
*Limited to studies from the US that include negative controls; †Non-commercial ELISA and Western blot; †† Non-commercial ELISA
SUMMER 2016 PAGE 10

the more advanced symptoms discussed earlier and they can persist for months or years. There is no
approved treatment for PTLDS and many physicians treat these patients in ways similar to patients who have
fibromyalgia or chronic fatigue syndrome1.
In the future, expanding LD research could be done to aid in the development of new testing options and
more accurate diagnosis for patients. Test sensitivity is low for the ELISA and Western blot and could be
improved through the development of newer testing methodologies. The length of treatment and types of
antibiotics being used to treat LD are another target for evaluation and if altered could prevent more cases of
PTLDS from occurring. The statistics show that this vector borne illness is on the rise and with 300,000
cases1 every year, more should be done to give these patients a better diagnostic test and successful treatment
plan.
1. Post-Treatment Lyme Disease Syndrome. (2015, July 01). Retrieved July 22, 2016, from https://www.cdc.gov/lyme/postlds/index.html
2. Lyme disease. (n.d.). Retrieved July 22, 2016, from http://www.mayoclinic.org/diseases -conditions/lyme - disease/basics/definition/con-20019701 3. Lyme Disease Quick Facts. (n.d.). Retrieved July 22, 2016, from http://www.ilads.org/lyme/lyme- quickfacts.php 4. Lyme disease is a clinical diagnosis, based on your medical history, symptoms and exposure to ticks. (n.d.). Retrieved July 22, 2016, from https://www.lymedisease.org/lyme-basics/lyme-disease/diagnosis/
THE SOUR TRUTH ABOUT LYME DISEASE,CONT.
SUMMER 2016 PAGE 11

NEWEST TESTING FOR DIAGNOSIS OF SEPSIS
By: Martina Martin, Vice Chair of ASCLS-IL Student Forum
Procalcitonin, abbreviated PCT, is a string of 116 amino acids that are the precursor of calcitonin, a hormone secreted by the thyroid gland that regulates the body concentration of calcium and phosphate. When the body experiences an inflammatory response, typically to a bacterial infection, calcitonin peptides are broken down into complexes forming Procalcitonin. Based on this information, there are hypotheses among medical professionals that Procalcitonin could be used as an early indicator for the possible diagnosis of a bacterial infections causing systemic infections such as bacteremia and sepsis. Intensive Care Units (ICUs) and Emergency Departments (EDs) across the country are in the progress of, or have already added Procalcitonin to their laboratory testing panels. Procalcitonin testing is primarily ordered when a patient is exhibiting the major symptoms of sepsis including fever, elevated lactic acid, leukocytosis, tachycardia, etc. In the ED, where I am currently employed, Procalcitonin is automatically included on the testing panels for 3 sepsis criteria panel and our pneumonia panel. Procalcitonin is typically ordered in addition to blood cultures, lactic acid, and CBC for leukocyte count.
Currently, the main function of Procalcitonin testing from the ED is to establish a baseline reading for the patient in question pending probable admission to the ICUs. Reference ranges for Procalcitonin levels will vary from patient to patient; however, less than 0.05 is typically considered the normal valve indicating that the patient is at low risk for possible septicemia or bacteremia. There is an intermediate range between 0.5 and 2.0 that could indicate a possible inflammatory response. Between 2.0 and 10.0 is considered a likely systemic sepsis infection and greater than 10.0 is considered a severe sepsis.
In addition to testing in the EDs, Procalcitonin is also being used in the ICUs in order to monitor antimicrobial therapy progress. Because Procalcitonin levels are elevated with bacterial infection, as the antibiotics used to treat the infection begin killing the bacteria, the Procalcitonin levels will show a significant drop, indicating that the antimicrobial is treating the infection. This could potentially save ICUs many supplies of antibiotics including monetary funds. In the wake of the current antibiotic resistance crisis, Procalcitonin could prevent patients from being exposed to unnecessary or incorrect antimicrobial therapy.
In summary, Procalcitonin testing is on the rise in hospitals across the country in an effort to increase earlier detection of possible systemic bacterial infection. Procalcitonin could provide a partial solution for the current antibiotic resistance crisis.
Sources: https://www.healthcare.siemens.com/clinical-specialities/sepsis/siemens-inflamation-and infection-assays/what-is-pct http://www.hormone.org/hormones-and-health/what-do-hormones-do/calcitonin http://www.mayomedicallaboratories.com/test-catalog/Clinical+and+Interpretive/83169
SUMMER 2016 PAGE 12

“LRN’s MORPHOGENESIS IN PUBLIC HEALTH SAFETY”
By: Eleanor Wolfram, M.S.
The two words, “growth” and “development” are often confused by the general population as having the same meaning. But as laboratorians, we know from our biological science studies, that there are unique differences between these two terms. Biology defines “growth as an increase size” and mass of an organism. The term development is defined as “a process wherein an organism transforms itself from a lone cell into a more complicated multi-cellular organism”. (1) In other words, the word growth addresses how big or massive the organism is; while the term development speaks to the organism’s morphogenesis of structural and functional features. Laboratory Resource Network RN Matures at Methodical Pace Development is a fundamental maturation characteristic of all living organisms. And in a way, institutions, quality improvement projects, even your place of employment can be viewed as a breathing developing life form. An excellent example of a public health project that has been in the development stage for close to two decades is the Laboratory Resource Network (LRN). LRN is one of the Centers for Disease Control and Prevention’s (CDC) mechanisms for protecting the public health and safety of the nation’s population. The idea for the LRN left the drawing board and became operational seventeen years ago in August, 1999. According to the American Society for Microbiology (ASM), “LRN was established by the Department of Health and Human Services’ Center for Disease Control and Surveillance (CDC) in accordance with Presidential Decision Directive 39, which outlined national anti-terrorism policies and assigned specific missions to federal departments and agencies.” (2) Initially the only government agencies involved in this collaborative mandate included the CDC, the Association of Public Health Laboratories (APHL) and the Federal Bureau of Investigation (FBI). LRN Evolutionary Development Since its inception, the LRN creators have been singing a continuous melody that an effective and efficient surveillance task could be accomplished by linking local, federal, law enforcement, military, and international laboratories. It is noteworthy to mention that over the years, the LRN has developed several various surveillance arms and legs to its endeavor. As of July, 2016, in addition to the initial LRN players, namely APHL, CDC and the FBI, additional professional organizations and government agencies have joined in the quest for public safety. These vital entities include, but are not limited to: ASM, the American Association of Veterinary Laboratory Diagnosticians (AAVLD), the College of American Pathologists (CAP), the Department of Homeland Security (DHS), the Department of Defense (DOD), the Department of Energy (DOE), the Department of Justice (DOJ), the Environmental Protection Agency (EPA), the Food and Drug Administration (FDA) and the United States Department of Agriculture (USDA). (3) The ever growing LRN participants will ensure a strong and effective laboratory response infrastructure to swiftly assess biological and chemical adverse exposure which can be the result from terrorist acts.(4) In addition, the collaboration opened up a new chapter to address other endemic, pandemic and epidemic public health emergencies, such as the post September 11, 2001 anthrax bio-crime, the 2009 H1N1 influenza (swine flu) pandemic, the ever present threat of measles and influenza outbreaks, the Ebola epidemic and most recently, the mosquito spread of the Zika virus. Basic Epidemiology Skills As a result, local, national and global microscopic threats to human health, numerous questions are constantly being raised regarding how lab professionals can play vital roles in utilizing onsite tools and techniques to
SUMMER 2016 PAGE 13

“LRN’s MORPHOGENESIS IN PUBLIC HEALTH SAFETY”, CONT.
SUMMER 2016 PAGE 14
prevent and control biological and chemical crimes and nature-induced public health outbreaks. One answer that has emerged is that all laboratorians, at a minimum should receive basic education on the topic of epidemiology. Never-ending Search for Epidemiological Clues Epidemiology is the science of public health. This young science was formally birthed during the late the 1800s by British physician, John Snow. He uncovered the root cause (contaminated water pumps) of the cholera disease. Because of Dr. Snow’s genius approach to get to reveal the source of London’s devastating outbreak, he is deemed the Father of Epidemiology. But tracing further back into history, around 400 B.C., Hippocrates penned the initial epidemiological ideas by hypothesizing the association between health and environmental factors. Epidemiology which is another cousin of biological science has led to the discovery, treatment and even prevention (in some cases) of contagious diseases like smallpox, typhoid fever and polio among humans. In present day, epidemiologists include on their research list non-contagious lab studies of diseases like cancer and poisonings caused by environmental agents. Clinical laboratory science for the most part focuses on the diagnostic testing of individuals. Epidemiology lab science takes a wider scope, in that this discipline studies illnesses and diseases of populations. Lab workups for epidemiology cases attempt to determine what factors are associated with diseases, and what factors may protect people. Because CDC recognizes the unique opportunities that the science of epidemiology renders, CDC’s Office of Public Health Scientific Services (OPHSS), has created a division dedicated to epidemiological research and pursuits. This arm of OPHSS is titled the Center for Surveillance, Epidemiology and Laboratory Services (CSELS). According to the CDC’s website, “the mission of the CSELS is to provide scientific service, expertise, skills, and tools in support of CDC’s national efforts to promote health; prevent disease, injury and disability; and prepare for emerging health threats, including bioterrorism.” (5) CSELS supports the LRN process through epidemiological research, which includes but is not limited to disease surveillance and testing, genomics, and health informatics. Development Never Stops: Linking LRN, Epidemiology and Informatics Due to the technology boom, the world has clearly shifted from an “industrial” age into an “information” age. Personal and health data is deemed by many private and public entities as being more precious than gold. Epidemiology lab studies rely heavily on timely and efficient access to data, information and statistics that can reveal risk factors for illnesses and diseases. This seamless data source can be obtained from Laboratory Information Management systems (LIM) which automates health data exchange and delivery of data for diagnosis, treatment and prevention interventions. A new initiative, Laboratory Information Management Integration System (LIMSi) project was initiated in 2010. There is a widespread belief that this newest development will be the next generation in informatics to support LRN’s progress. According to APHL’s October 2012 report titled “Electronic Data Transfer Critical to LRN Success, “LIMSi optimizes information flow and system interoperability between CDC and participating LPN facilities. Though the success of the LIMSi initiative, participating LRN laboratories are able to maximize their IT capabilities and fully leverage the benefits of their investments. In addition, LRN laboratories can achieve PHIN interoperability, ultimately enhancing the LRN’s capability to maximize data in response to a public health emergency.” (6)

Conclusion LRN has experienced multiple developmental phases since its inception. And because of the complex world we live in, undoubtedly the 1990 LRN mandate will have more challenges well into its future. On a daily basis, both private and public entities uncover huge volumes of clinical laboratory data which is extremely valuable in uncovering public health diseases and bio/chemical crimes that can threaten the health and wellness of societies worldwide. Without question, the ongoing development of LRN will aid in helping local, national and global communities reap the benefits of epidemiological findings to preserve the future of humanity. References (1) “Growth vs. Development In Biology.” Difference Between Growth and Development in Biology. Difference Between.net. www.difference between.net./science/bioliogy/-science/differences-between-growth-and-development-biology. (2) Laboratory Response Network, American Society of Microbiology, www.ckinmicro.asm.org/index.php/lab-management/public-health/laboratory-response-network. (3)Laboratory Response Network (LRN) Partners and Other Related Sites, Centers for Disease Control and Prevention (CDC) website www.emergency.cdc.gov/lrn/partners.asp (4) Henchal, E. A., J. D. Teska, and J. W. Ezzell. 2000. Responding to biological terrorism: a role for the clinical laboratory. Clinical Laboratory News Volume 26, Pages 4-18. (5) Center for Surveillance, Epidemiology and Laboratory Science (CSELS). www.cdc.gov/ophss/csels/index.html. (6) Public Health Laboratory Informatics and the LRN-C APHL/publications/Documents/EH_2012)ct_Public-Health-Laboratory-Informatics-and-the-Laboratory-Response. www.aphl.org/About. October 2012. Valuable Reading “Sentinel Level Clinical Laboratory Protocols For Suspected Biological Threat Agents and Emerging Infectious Diseases” These guidelines were developed in collaboration between the Association of Public Health Laboratories (APHL), ASM and CDC. (Electronic Guidelines Updated Tuesday, May 10, 2016. www.asm.org.
Eleanor Wolfram, M.S., is a certified QA&C auditor
“LRN’s MORPHOGENESIS IN PUBLIC HEALTH SAFETY”, CONT.
SUMMER 2016 PAGE 15

Congratulation to members with anniversaries for their many years of service to ASCLS!!!
Congratulations to the Keys to the Future Award winners, Cheryl Hanson and Debbie Wollenberg, whose
names were displayed at the National Meeting!!! Outgoing ASCLS President: Barbara Snyderman
Incoming ASCLS President: Suzanne Campbell
ASCLS President Elect (2016 -2017): Deb Rodahl ASCLS-IL is a member of ASCLS Region VI Kim Von Ahsen (Iowa) is Region VI Director Demetra (Toula) Castillo is Region VI Secretary Lisa Bakken is Region VI Treasurer
Beckie Hetrick from KSCLS was the recipient of the Rho Sigma Award for the involvement and leadership
that she has brought to ASCLS and Region VI over the years.
Region VI has won Political Action Committee (PAC) for the past four years. Theresa Fruehling from
Region VI served as national PAC chair. The PAC was charged to get $2000 from each region and Region
VI surpassed those amounts to raise nearly $23,000 this past year Joan M. Albers, from Illinois, was recognized for 50 years of ASCLS membership at the National Meeting in Philadelphia, PA Wednesday evening, August 3rd, 2016
The ASCLS Annual Meeting will be held next year in San Diego, CA (July 30-August 4,,2017)
SUMMER 2016 PAGE 16
ASCLS ANNUAL MEETING 2016 IN PHILADELPHIA, PA
HIGHLIGHTS Prepared By: Masih Shokrani, ASCLS-IL President

SUMMER 2016 PAGE 17
2016 ASCLS ANNUAL MEETING (IN PICTURES)
The Annual Meeting of the American Society for Clinical Laboratory Science (ASCLS) was held this year in Philadelphia, PA from August 1-4. The meeting included various Educational Scientific Sessions, Committee Meetings, Clinical Lab Expo, Poster Presentations, Awards Ceremony & much more!
The incoming ASCLS President, Suzanne
Campbell (on the right), receives the President’s gavel from outgoing
ASCLS President Barbara Snyderman (on the left)
ASCLS Board of Directors. Pictured in the top row
second from right is Jim Flanigan, the new ASCLS Executive Vice President

Region VI group picture in Philadelphia
SUMMER 2016 PAGE 18
2016 ASCLS ANNUAL MEETING (IN PICTURES),CONT.
Region VI Events: ASCLS-IL is a member of ASCLS Region VI
Beckie Hetrick (middle) from KSCLS was the recipient of ASCLS Region VI Rho Sigma Award. Kim Von Ahsen (Iowa), Region VI Director, is on the left and Suzanne Campbell, ASCLS incoming President, is on the right.

SUMMER 2016 PAGE 19
2016 ASCLS ANNUAL MEETING (IN PICTURES),CONT.
Poster presentation: Kate Bernhardt, from Loyola University Medical Center (Maywood, IL)
Poster presentation: Masih Shokrani, from Northern Illinois University

Joan M. Albers, on the left, who was recognized for 50 years of ASCLS membership at the National Meeting in Philadelphia, PA with Sheila Gibbons, ASCLS-IL President (2015-2016)
On the left, Kate Bernhardt receives ASCLS Recognition Award for being ASCLS-IL Member of the Year the previous year from Sheila Gibbons, ASCLS-IL President (2015-2016)
SUMMER 2016 PAGE 20
2016 ASCLS ANNUAL MEETING (IN PICTURES),CONT.

SUMMER 2016 PAGE 21
2016 ASCLS ANNUAL MEETING (IN PICTURES),CONT.
ASCLS-IL Attends ASCLS House Of Delegates In The Annual Meeting
“Left- to- right”: Kate Bernhardt, Sheila Gibbons, Masih Shokrani, Demetra (Toula) Castillo, Sarah Chritz

LABORATORY CAREERS
SUMMER 2016 PAGE 22
Loyola University Medical Center has the following openings for ASCP- certified Medical Laboratory Scientists:
Blood Bank – PM shift & Midnight Shift Core Lab – Day & Midnight Shifts
For more information see loyolamedicine.org/jobs or contact Linda Leung – Blood Bank Manager ([email protected] ) or Cindy Blakemore – Core Lab Manager ([email protected]).
Advocate Lutheran General Hospital has a full-time, 3rd shift opening in the blood bank. Rotating holidays and weekends, start times flexible.
Contact: [email protected] or [email protected] for more details! Apply online at https://jobs.advocatehealth.com/job/park-ridge/lg-mls-

AMERICAN SOCIETY FOR CLINICAL LABORATORY–
SCIENCE - ILLINOIS
ASCLS-IL is an affiliate society of the American Society for Clinical Laboratory Science (ASCLS) and one of five states in ASCLS Region VI, which also includes Iowa, Kansas, Missouri and Nebraska. ASCLS serves as the voice of all clinical laboratory professionals, creating a vision for the advancement of the clinical laboratory practice field, and advocating the value and the role of the profession ensuring safe, effective, efficient, equitable, and patient centered health care.
Promoting the value of the profession to healthcare and the public
Uniting the profession to speak with one voice
Advocating on behalf of the profession
Promoting professional independence
Enhancing quality standards and patient safety
Ensuring workplace safety
Providing professional development opportunities
Promoting expanded roles and contributions of clinical laboratory professionals to the healthcare team
Increasing the diversity in the profession and expanding the voice and role of under-represented individuals and groups
Do you have examples/ideas of ways to promote the profession of Medical Laboratory Scientist? Ideas to increase ASCLS-IL membership? Are you interested in becoming more involved in ASCLS-IL? We are always looking for help and volunteers! Are you an educator? Are you a writer?
We are looking help for creating new student bowl questions!
Are you a great party planner?
We could use your help in planning the 2017 ASCLS-IL Annual Meeting!
Do you love talking to and meeting new people?
We could use your help in recruiting members to the association and
promoting the profession!
We’re on the web! www.asclsil.org
Like us on Facebook! www.facebook.com/
ASCLS.IL
We are always interested in articles for the newsletter
For any and all of the above, please feel free to contact the organization at:
[email protected] ASCLS-IL Insights Editors:
Editor-in-Chief: Masih Shokrani, Ph.D. MT(ASCP) - [email protected]
Copy Editor: Michelle Campbell, MLS(ASCP) - [email protected]
SUMMER 2016 PAGE 23